")
Back to Journals » Nature and Science of Sleep » Volume 17
Prevalence and Associative Analysis of Thyroid Dysfunction in Patients with Obstructive Sleep Apnea Hypopnea Syndrome: A Cross-Sectional Study
Authors Zhou P , Li H , Qiu J, Ye J, Guo J, Yao Y, Li H , Shi Y, Duan Y, Lv Y
Received 7 January 2025
Accepted for publication 4 June 2025
Published 23 June 2025 Volume 2025:17 Pages 1467—1475
DOI https://doi.org/10.2147/NSS.S515819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Valentina Alfonsi
Pinyi Zhou,1,* Hongmei Li,2,* Jingman Qiu,1 Jing Ye,1 Jingyu Guo,1 Yun Yao,1 Hongyan Li,1 Yanfen Shi,1 Yufan Duan,1 Yunhui Lv1
1Department of Sleep Medicine, The Affiliated Hospital of Kunming University of Science and Technology, The First People’s Hospital of Yunnan Province, Kunming, 650500, People’s Republic of China; 2Department of Neurology, The Affiliated Hospital of Kunming University of Science and Technology, The First People’s Hospital of Yunnan Province, Kunming, 650500, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pinyi Zhou, Department of Sleep Medicine, The Affiliated Hospital of Kunming University of Science and Technology, The First People’s Hospital of Yunnan Province, Kunming, 650500, People’s Republic of China, Email [email protected] Yunhui Lv, Department of Sleep Medicine, The Affiliated Hospital of Kunming University of Science and Technology, The First People’s Hospital of Yunnan Province, Kunming, 650500, People’s Republic of China, Email [email protected]
Objective: Obstructive sleep apnea-hypopnea syndrome (OSAHS) is closely associated with hypothyroidism. This study aimed to evaluate the prevalence and correlation of hypothyroidism in patients with OSAHS.
Methods: This investigation included a cohort of 1693 patients newly diagnosed with OSAHS, all of whom underwent polysomnography and thyroid function assessments.
Results: The study cohort comprised 1693 OSAHS patients (60.4% male). No significant differences in thyroid-stimulating hormone (TSH) or free thyroxine (FT4) levels were observed across OSAHS severity groups (p = 0.670 and p = 0.307). Notably, patients with overt hypothyroidism demonstrated significantly lower lowest oxygen saturation (LSpO2) levels than their euthyroid counterparts (p = 0.035). The analysis did not reveal any significant correlations between TSH/FT4 levels and the apnea-hypopnea index, mean oxygen saturation (MSpO₂), or LSpO₂. Nevertheless, TSH levels were positively correlated with female sex and age (p = 0.001), while no correlation was found with body mass index. After controlling for sex and age, TSH was positively correlated with apnea-hypopnea index (p = 0.002) and negatively correlated with both MSpO₂ and LSpO₂ (p = 0.001). In contrast, FT4 levels exhibited a negative correlation with apnea-hypopnea index (p = 0.016) and positive correlations with MSpO₂ and LSpO₂ (p = 0.030 and p = 0.018). The overall prevalence rates of hypothyroidism and overt hypothyroidism within the study population were determined to be 13.7% and 3.8%, respectively, with no significant differences observed across the severity categories of OSAHS (p = 0.166 and p = 0.193). Subclinical hypothyroidism was identified in 9.9% of the patients, with a notably lower prevalence in those with severe OSAHS compared to those with milder forms of the condition (p = 0.004).
Conclusion: In patients with OSAHS, 13.7% had hypothyroidism, with 3.8% being overt hypothyroidism and 9.9% being subclinical hypothyroidism. Thyroid function parameters are associated with the severity of OSAHS and are influenced by sex and age.
Keywords: sleep apnea, obstructive, hypothyroidism, prevalence, correlation
Introduction
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is a common sleep-related breathing disorder characterized by recurrent episodes of partial or complete obstruction of the upper airway during sleep, resulting in interruptions in breathing and hypoventilation.1 The prevalence of OSAHS is significant, affecting approximately 936 million individuals globally between the ages of 30 and 69, with an estimated 176 million cases reported in China, reflecting a prevalence rate of 23.6%.2 Recognized risk factors for OSAHS include obesity, advanced age, and male sex.3,4 OSAHS has the potential to result in functional deterioration or even failure of various organ systems.5
Hypothyroidism (HT), which includes both overt (OH) and subclinical (SCH) forms, is characterized by a hypometabolic state resulting from either absolute or relative deficiency of thyroid hormones.6 Recent studies indicate a bidirectional relationship between OSAHS and HT. A large cross-sectional study involving 5515 participants found a prevalence of 9.47% for HT in the general population of the United States, with regression analyses revealing significant associations between HT and sleep apnea.7 Notably, 25–30% of patients with primary HT also exhibit comorbid OSAHS,8,9 which can exacerbate the severity of the disease10 and increase cardiovascular morbidity and mortality.4,11 While the potential for OSAHS to induce thyroid dysfunction is theoretically plausible, current clinical evidence remains inconclusive regarding its role as a causative factor in the development of HT. Although SCH is more prevalent in populations with OSAHS, the clinical implications of this association on disease progression warrant further investigation.
This study aims to conduct a retrospective analysis of the prevalence of HT among patients diagnosed with OSAHS at a single medical center. Additionally, the study will compare the demographic characteristics and specific clinical data of patients exhibiting varying degrees of OSAHS alongside those with HT, thereby examining the relationship between HT and OSAHS.
Patients and Methods
This research was carried out at the Sleep Center of the First People’s Hospital of Yunnan Province. The study population consisted of patients who were initially diagnosed with OSAHS through polysomnography (PSG) using the Philips Respironics Alice 6 system at the aforementioned hospital between 2018 and 2021, and who also underwent thyroid function assessments. Eligible participants were individuals aged 18 years or older who satisfied the diagnostic and severity criteria for adult OSAHS as specified in the International Classification of Sleep Disorders, 3rd edition (ICSD-3).1 Exclusion criteria encompassed: 1) individuals with severe organic diseases, including heart failure, hepatic failure, or renal failure; 2) individuals with chronic respiratory conditions such as chronic obstructive pulmonary disease, bronchial asthma, or interstitial lung disease; 3) individuals with a history of thyroid disorders or newly diagnosed hyperthyroidism; 4) individuals with known autoimmune diseases; 5) pregnant individuals; and 6) individuals with incomplete data. This study received approval from the Institutional Review Board (IRB)/Ethics Committee of the First People’s Hospital of Yunnan Province (Approval No.: KHLL2023-KY002) and adhered rigorously to the ethical principles outlined in the Declaration of Helsinki. Given that the study utilized de-identified data obtained from existing electronic medical records and presented no more than minimal risk to participants, the requirement for informed consent was waived.
Study Design
This research utilized a retrospective descriptive design to gather data. The demographic characteristics, PSG parameters, and thyroid function indices of eligible patients were obtained through a review of medical records. In accordance with the laboratory testing standards implemented at our facility, which employs chemiluminescent immunoassay techniques, OH was defined as elevated thyroid-stimulating hormone (TSH) levels exceeding 4.2 mIU/L, in conjunction with decreased free thyroxine (FT4) levels below 12 pmol/L. Conversely, SCH was identified by elevated TSH levels while maintaining normal FT4 levels.
Statistical Analysis
Statistical analyses were performed utilizing the SPSS 26.0 software package. Normally distributed data are presented as the mean ± standard deviation (SD), with differences among the three groups assessed through one-way analysis of variance (ANOVA). The Least Significant Difference (LSD) method was employed when variances were homogeneous, while the Games-Howell method was applied in heterogeneous variances. Results are reported as the median (P25, P75) for skewed data, and intergroup comparisons were conducted using the Kruskal–Wallis H-test. Categorical data are expressed as the number of cases (percentage), with group comparisons executed via the Chi-square test. Spearman’s rho correlation coefficient was used to evaluate the correlation between continuous variables. A p-value of less than 0.05 was deemed indicative of statistically significant findings.
Results
From January 2018 to December 2021, a total of 2161 patients were screened, of which 1693 were ultimately incorporated into the study. The study cohort was comprised of 60.4% males, with a mean age of 49.4 ± 13.8 years, a body mass index (BMI) of 26.6 (23.9, 30.5) kg/m², and an apnea-hypopnea index (AHI) of 32.1 (16.1, 60.7). Figure 1 provides a summary of the patient flow throughout the study.
 |
Figure 1 The chart of patient flow through the study. Abbreviations: OSAHS, obstructive sleep apnea-hypopnea syndrome. |
Table 1 delineates the demographic characteristics and prevalence of thyroid disorders among patients categorized by OSAHS severity. The mean TSH level across the entire study cohort was 2.2 (1.4, 3.2) mIU/L, while the mean FT4 level was recorded at 14.3 ± 3.6 pmol/L. In the cohort with mild OSAHS, there was a notable predominance of female patients and a lower BMI. Conversely, the group with severe OSAHS exhibited a higher proportion of male patients and a greater incidence of hypertension. TSH and FT4 levels did not show significant variation among patients with differing severities of OSAHS. The prevalence of OH across all patients was found to be 3.8%, with no significant differences identified among the three OSAHS severity groups. In contrast, the prevalence of SCH was 9.9%, which was significantly elevated in patients with mild and moderate OSAHS compared to those with severe OSAHS. The overall prevalence of OH and SCH within the study population was 13.7%, with no significant differences noted among the three OSAHS severity categories.
 |
Table 1 Demographic Characteristics and Prevalence of Thyroid Disease Among All Patients Stratified by the Severity of OSAHS |
Table 2 delineates the demographic characteristics and clinical profiles of all patients categorized by thyroid function status (euthyroid, SCH, and OH). The groups classified as OH and SCH exhibited a notably higher prevalence of female patients and an older age demographic in comparison to the euthyroid group. Patients diagnosed with OH presented with more pronounced respiratory disturbances, as indicated by significantly elevated AHI scores and reduced lowest oxygen saturation (LSpO2) levels relative to those in the SCH group. Nevertheless, no statistically significant differences were identified in AHI or mean oxygen saturation (MSpO2) between patients with OH and the euthyroid controls.
 |
Table 2 Comparative Analysis of Demographic Characteristics and Clinical Parameters Stratified by Thyroid Function Status |
Table 3 illustrates the Spearman’s ρ correlations among demographic characteristics, thyroid function indices, and PSG parameters across the entire patient cohort. The AHI exhibited significant correlations with sex (r = −0.299; p = 0.001), age (r = −0.121; p = 0.001), and BMI (r = 0.380; p = 0.001), while no significant associations were found with thyroid function indices. TSH demonstrated significant correlations with sex (r = 0.193; p = 0.001) and age (r = 0.086; p = 0.001). FT4 was correlated with age (r = −0.094; p = 0.001) but not with sex. Following adjustments for sex and age differences, as presented in Table 4, TSH retained significant correlations with AHI (r = 0.075; p = 0.002), MSpO2 (r = −0.116; p = 0.001), and LSpO2 (r = −0.101; p = 0.001). Likewise, FT4 demonstrated significant associations with AHI (r = −0.059; p = 0.016), MSpO2 (r = 0.053; p = 0.030), and LSpO₂ (r = 0.057; p = 0.018). Furthermore, BMI exhibited a strong correlation with AHI (r = 0.350; p = 0.001) but did not show significant relationships with TSH or FT4.
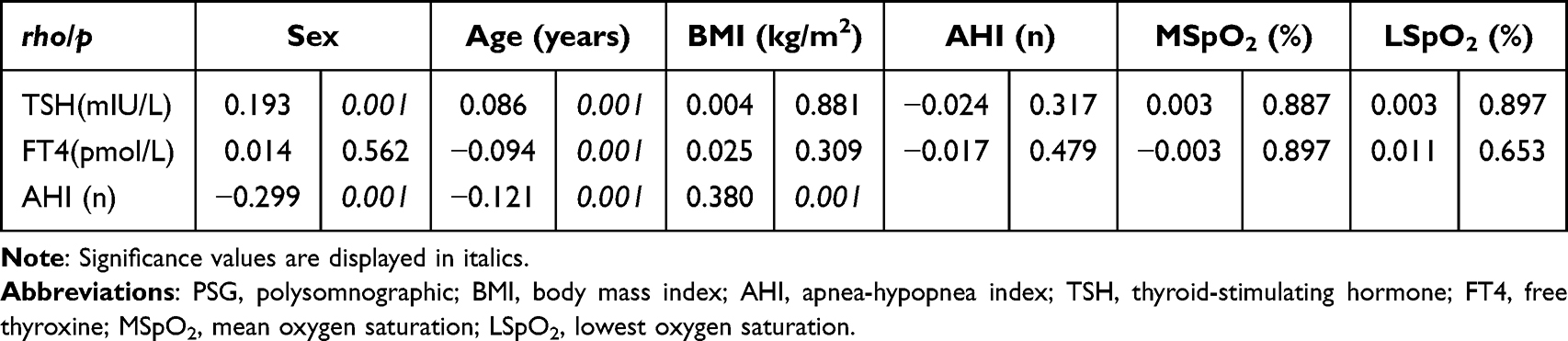 |
Table 3 Spearman’s ρ Correlations Between Demographic Characteristics, Thyroid Function Indicators, and PSG Parameters Among All Patients |
 |
Table 4 Partial Spearman’s ρ Correlations Between Thyroid Function Indices and PSG Parameters, Adjusted for Sex and Age |
Discussion
The findings of this study indicate a significant prevalence of HT among patients diagnosed with OSAHS. The majority of these cases were newly identified instances of OH and SCH in individuals without a previous history of thyroid surgery or current treatment with thyroid hormone therapy. Additionally, the relationship between HT and the severity of OSAHS was found to be moderated by factors such as sex and age.
The existing literature indicates significant variability in the prevalence of HT among patients with OSAHS. For example, a meta-analysis conducted by Zhang et al10 identified an overall prevalence of OH at 8.12 ± 7.13% and SCH at 11.07 ± 8.49% within this patient population. Additional clinical studies examining the prevalence of thyroid disorders in OSAHS cohorts have reported OH rates ranging from 1.97% to 10%, SCH rates between 7% and 12%, and newly diagnosed OH rates of 0.4% to 2%.12–15 These variations may be attributed to differences in the inclusion criteria for study populations, methodologies for assessing thyroid hormone levels, and standards for diagnosing OSAHS. In the current study, which excluded most conditions that could potentially influence thyroid function, the prevalence of HT among OSAHS patients was found to be 13.7%, with SCH at 9.9% and OH at 3.8%. Although non-OSAHS control groups were not included in this analysis, the prevalence of OH observed in this study was notably higher than that reported in the general population of China (3.7% compared to 1.03%).16 Furthermore, the overall prevalence of HT in this cohort surpassed that documented in the general population of the United States (13.5% versus 9.47%).7
Previous research has highlighted sex differences in the prevalence of HT and OSAHS, with females demonstrating a greater vulnerability to HT6,17 and males exhibiting a higher likelihood of developing OSAHS.5 The current study reveals a notably elevated prevalence of HT among female patients with OSAHS in comparison to their male counterparts, aligning with the findings of Bahammam et al12 and Wang et al.18 This phenomenon may be linked to sex-specific hormonal factors and the inherent predisposition of females to autoimmune conditions,19,20 although the existing evidence remains insufficient. Additionally, thyroid function plays a significant role in influencing PSG parameters in patients with OSAHS. Previous studies have shown that OH diminishes sex-related differences in PSG outcomes among OSAHS patients, while SCH is primarily associated with increased BMI in female patients relative to males.12 The influence of sex in OSAHS patients with concurrent hypothyroidism constitutes a vital yet underexplored domain of research.
Previous researchers have systematically delineated the bidirectional relationship between HT and OSAHS through comprehensive reviews.21 Thyroid hormones play crucial roles in glucose, lipid, and protein metabolism, facilitating mitochondrial oxidative processes, promoting pulmonary surfactant maturation, and regulating the transcription of genes encoding myofibrillar and calcium-regulatory proteins in muscle fibers.22 HT may induce or exacerbate OSAHS through several pathophysiological mechanisms: (1) deposition of mucopolysaccharides and proteins in the upper airway leading to pharyngeal narrowing;22,23 (2) impaired contractile function of pharyngeal and respiratory muscles24 coupled with neurological dysfunction, resulting in ventilatory impairment;22 (3) metabolic syndrome presenting primarily as obesity;11,25 and (4) attenuated ventilatory response to hypoxia and hypercapnia in the respiratory center, contributing to central apnea.10 Conversely, OSAHS may promote thyroid tissue damage and hypothyroidism through intermittent hypoxia, sleep deprivation, and sustained sympathetic activation, which collectively enhance oxidative stress and inflammatory responses.26,27 Pathophysiologically, HT progression would be expected to correlate with OSAHS severity. However, our study found no significant differences in thyroid function parameters (TSH and FT4) across varying OSAHS severity groups, aligning with findings by Ozcan et al13 and Bruyneel et al.14 This suggests that thyroid hormone levels may be modulated by multiple confounding factors.
To evaluate HT’s impact on OSAHS, we compared polysomnographic measures between OSAHS patients with and without HT. Our results demonstrated significantly higher AHI levels and more severe hypoxemia in OH patients. These findings contrast with Wang et al,18 who reported no differences in PSG parameters (AHI, MSpO2, LSpO2) between comparable groups - a discrepancy potentially attributable to their limited HT sample size (n=27) and failure to stratify OH and SCH subgroups.
The SCH-OSAHS relationship remains unclear. One study found no difference in OSAHS prevalence between SCH patients and controls, nor any correlation between TSH levels and respiratory disturbance indices.28 Intriguingly, our SCH patients exhibited milder OSAHS than euthyroid counterparts - a novel observation potentially mediated by sex and age factors. Furthermore, SCH’s transient nature29 may explain its modest clinical impact on OSAHS severity.
Spearman correlation analysis conducted on the entire cohort of study participants indicated an absence of significant associations between thyroid function parameters and polysomnographic measures. It is noteworthy that both TSH and the AHI exhibited significant correlations with sex and age. Upon adjusting for these confounding variables, significant correlations were identified between TSH/ FT4 and AHI, MSpO2, and LSpO2, thereby providing enhanced evidence for a pathophysiological connection between these conditions. These results imply that the onset of HT in patients with OSAHS may be linked to the extent of systemic hypoxia,30 while also underscoring the importance of sex and age as critical confounding factors in research pertaining to thyroid function and OSAHS. Conversely, several studies have documented a lack of significant correlations between TSH/FT4 levels and AHI or LSpO2.13,14,31 The discrepancies in findings may be attributed to methodological limitations, such as the failure to consider potential confounders (including sex, age, obesity, and comorbid chronic conditions) and insufficient sample sizes, which could introduce considerable bias. The metabolic disturbances associated with HT are known to promote obesity, a well-recognized risk factor for the exacerbation of OSAHS.25 In our study cohort, patients with OH displayed higher BMI values compared to euthyroid individuals (28.2±5.0 vs 27.6±5.6, P=0.859), although this difference did not achieve statistical significance.
The inherent limitations of this retrospective study hinder the evaluation of two essential clinical interactions: (1) the therapeutic effects of thyroid hormone replacement on the progression of OSAHS in patients with HT, and (2) the potential alterations in thyroid function following continuous positive airway pressure (CPAP) therapy in individuals with OSAHS. Prior research has indicated that patients with hypothyroidism receiving thyroid hormone supplementation experience significant reductions in apnea events, oxygen desaturation indices, and episodes of snoring and choking, with these improvements occurring independently of changes in body weight.9,32 Simultaneously, CPAP treatment has been linked to measurable enhancements in thyroid function among the majority of OSAHS patients,23,33 collectively suggesting indirect evidence of a bidirectional relationship between OSAHS and HT.
Moreover, studies investigating the prevalence and clinical significance of SCH within OSAHS populations encounter an additional methodological challenge: the potential transient nature of SCH as a physiological state that may resolve spontaneously under varying bodily conditions.29 This situation necessitates longitudinal studies to differentiate between persistent and transient cases of SCH, thereby ensuring the validity of the research findings. Additionally, while autoimmune thyroiditis is recognized as the primary cause of HT,6 emerging evidence suggests that shared immunopathological mechanisms—particularly those involving Th1/Th17 cell-mediated inflammatory pathways—may be implicated in both OSAHS and autoimmune thyroiditis.34,35 A large cross-sectional study involving 920 participants identified lymphocyte count as an independent predictor of OSAHS in conjunction with HT,36 thereby reinforcing the immunological connection between these conditions. Although our study excluded patients with diagnosed immune disorders, this exclusion criterion may be inadequate given the complexities associated with immune dysregulation. Future investigations should incorporate comprehensive immunophenotyping to reduce bias and clarify the specific mechanistic pathways that link immune markers to the comorbidity of OSAHS and HT.
Due to the absence of comprehensive sleep architecture data, this study did not include the sleep parameters of patients with OSAHS in the final analysis. Patients with OSAHS typically experience chronic sleep fragmentation, disrupted sleep architecture, and sleep deprivation as a result of recurrent nocturnal awakenings.5 Importantly, the synthesis and secretion of thyroid hormones exhibit distinct circadian rhythms,37 indicating that prolonged sleep deprivation may disrupt the secretion patterns of TSH and, in turn, impair thyroid function. Epidemiological studies have shown that night-shift workers have significantly elevated serum TSH levels and a higher risk of SCH compared to their day-shift counterparts, with this risk increasing in proportion to the duration of exposure to shift work.38 Furthermore, research by Yan et al39 has indicated that individuals with isolated TSH elevation report poorer nocturnal sleep quality compared to those with normal TSH levels. Mechanistic investigations have revealed that sleep deprivation leads to oxidative stress, which triggers an imbalance between autophagy and apoptosis in thyroid cells, ultimately compromising thyroid histology and function.40 Collectively, these findings highlight the clinically significant effects of disrupted sleep architecture on thyroid homeostasis, thereby necessitating systematic exploration in future research endeavors.
Conclusion
The current investigation reveals a notably increased prevalence of HT among patients with OSAHS, with a higher vulnerability observed in females compared to males, a finding that aligns with existing clinical epidemiological literature. A significant methodological advantage of this study is its large sample size and the thorough exclusion of confounding comorbidities. Our findings reinforce the clinically relevant association between the severity of OSAHS and thyroid dysfunction, highlighting the necessity for heightened awareness and proactive management by healthcare providers. However, several critical gaps in knowledge remain due to the limitations of the study. Future research should aim to: (1) clarify the natural progression of transient SCH, (2) investigate the pathogenesis of autoimmune thyroiditis, (3) assess disruptions in sleep architecture, and (4) analyze the therapeutic effects of both thyroid hormone replacement and CPAP treatments in OSAHS populations. A systematic examination of these areas will contribute to an evidence-based framework for enhancing clinical management for OSAHS patients with concurrent HT.
Abbreviations
OSAHS, obstructive sleep apnea-hypopnea syndrome; PSG, polysomnography; AHI, apnea hypopnea index; LSpO2, lowest oxygen saturation; MSpO2, mean oxygen saturation; BMI, body mass index; CPAP, continuous positive airway pressure; TSH, thyroid stimulating hormone; FT4, free thyroxine; HT, hypothyroidism; OH, overt hypothyroidism; SCH, subclinical hypothyroidism.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the First People’s Hospital of Yunnan Province (Approval No. KHLL2023-KY002). The requirement for informed consent was waived by the committee due to the retrospective nature of the study, which involved analysis of anonymized patient data without any intervention or additional risk. All data were de-identified before analysis and stored on a password-protected institutional server accessible only to the research team.
Acknowledgments
We thank all the participants and staff involved in this study.
Author Contributions
Pinyi Zhou (First Author): Conceptualization, Formal Analysis, Investigation, Writing - Original Draft, Writing - Review & Editing.
Hongmei Li: Investigation, Formal Analysis, Validation, Writing - Original Draft, Writing - Review & Editing.
Jingman Qiu: Investigation, Formal Analysis, Validation, Data Curation, Writing - Original Draft.
Jing Ye: Methodology, Investigation, Formal Analysis, Data Curation, Writing - Original Draft.
Jingyu Guo: Data Curation, Validation, Visualization, Writing - Original Draft.
Yun Yao: Investigation, Data Curation, Resources, Writing - Original Draft.
Hongyan Li: Formal Analysis, Validation, Data Curation, Writing - Original Draft.
Yanfen Shi: Conceptualization, Data Curation, Visualization, Writing - Review & Editing.
Yufan Duan: Writing - Original Draft, Investigation, Visualization, Writing - Review & Editing.
Yunhui Lv (Corresponding Author): Conceptualization, Formal Analysis, Supervision, Writing - Review & Editing, Funding Acquisition, Project Administration.
All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work. All authors reviewed and approved the final manuscript for submission to this journal.
Funding
This research was funded by [National Natural Science Foundation of China], Number: 1760022; Hanfang Expert Workstation in Yunnan Province, NO. 202105AF150022. Yunnan Province “Xing Dian Talent Support Program” Project, NO. XDYC-MY-2022-0013. Kunming Health Science and Technology Talent Cultivation Program and Medical Science and Technology Discipline Thousand Project Reserve Talents, NO. 2024-SW (Reserve-30).
Disclosure
The authors declare that there are no competing interests associated with the paper.
References
1. Medicine AAOS. International Classifi Cation of Sleep Disorders.
2. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/s2213-2600(19)30198-5
3. Fietze I, Laharnar N, Obst A, et al. Prevalence and association analysis of obstructive sleep apnea with gender and age differences - Results of SHIP-Trend. J Sleep Res. 2019;28(5). doi:10.1111/jsr.12770
4. Bauters FA, Hertegonne KB, De Buyzere ML, Joos GF, Chirinos JA, Rietzschel ER. Phenotype and risk burden of sleep apnea: a population-based cohort study. Hypertension. 2019;74(4):1052–1062. doi:10.1161/hypertensionaha.119.13452
5. Berry BR. Pathophysiology of obstructive sleep apnea. In: Fundamentals of Sleep Medicine. W.B. Saunders; 2012:263–279.
6. Chaker L, Bianco AC, Jonklaas J, Peeters RP. Hypothyroidism. Lancet. 2017;390(10101):1550–1562. doi:10.1016/s0140-6736(17)30703-1
7. Thavaraputta S, Dennis JA, Laoveeravat P, Nugent K, Rivas AM. Hypothyroidism and its association with sleep apnea among adults in the United States: NHANES 2007–2008. J Clin Endocrinol Metab. 2019;104(11):4990–4997. doi:10.1210/jc.2019-01132
8. Lin -C-C, Tsan K-W, Chen P-J. The relationship between sleep apnea syndrome and hypothyroidism. Chest. 1992;102(6):1663–1667. doi:10.1378/chest.102.6.1663
9. Jha A, Sharma SK, Tandon N, et al. Thyroxine replacement therapy reverses sleep-disordered breathing in patients with primary hypothyroidism. Sleep Med. 2006;7(1):55–61. doi:10.1016/j.sleep.2005.05.003
10. Zhang M, Zhang W, Tan J, Zhao M, Zhang Q, Lei P. Role of hypothyroidism in obstructive sleep apnea: a meta-analysis. Curr Med Res Opin. 2016;32(6):1059–1064. doi:10.1185/03007995.2016.1157461
11. Devdhar M, Ousman YH, Burman KD. Hypothyroidism. Endocrinol Metab Clinics North Am. 2007;36(3):595–615,v. doi:10.1016/j.ecl.2007.04.008
12. Bahammam SA, Sharif MM, Jammah AA, BaHammam AS. Prevalence of thyroid disease in patients with obstructive sleep apnea. Respir Med. 2011;105(11):1755–1760. doi:10.1016/j.rmed.2011.07.007
13. Ozcan KM, Selcuk A, Ozcan I, et al. Incidence of hypothyroidism and its correlation with polysomnography findings in obstructive sleep apnea. Europ Archiv Oto-Rhino-Laryngol. 2014;271(11):2937–2941. doi:10.1007/s00405-014-2962-1
14. Bruyneel M, Veltri F, Poppe K. Prevalence of newly established thyroid disorders in patients with moderate-to-severe obstructive sleep apnea syndrome. Sleep Breathing. 2018;23(2):567–573. doi:10.1007/s11325-018-1746-z
15. Kapur VK, Koepsell TD, deMaine J, Hert R, Sandblom RE, Psaty BM. Association of hypothyroidism and obstructive sleep apnea. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1379–1383. doi:10.1164/ajrccm.158.5.9712069
16. Shan Z, Chen L, Lian X, et al. Iodine status and prevalence of thyroid disorders after introduction of mandatory universal salt iodization for 16 years in china: a cross-sectional study in 10 cities. Thyroid. 2016;26(8):1125–1130. doi:10.1089/thy.2015.0613
17. Association CM, House CMJP, Practice CSoG, of EBoCJ, Association GPoCM, Disease EGoGPCoS. Guideline for primary care of hypothyroidism: practice version(2019). Chinese J General Practitioners. 2019;18(11):1029–1033.
18. Wang L, Fang X, Xu C, et al. Epworth sleepiness scale is associated with hypothyroidism in male patients with obstructive sleep apnea. Front Endocrinol. 2022;13:1010646. doi:10.3389/fendo.2022.1010646
19. Ren B, Zhu Y. A new perspective on thyroid hormones: crosstalk with reproductive hormones in females. Int J Mol Sci. 2022;23(5):2708. doi:10.3390/ijms23052708
20. Desai MK, Brinton RD. Autoimmune disease in women: endocrine transition and risk across the lifespan. Front Endocrinol. 2019;10:265. doi:10.3389/fendo.2019.00265
21. Zhou P, Tan W, Mei X, Shan X. Research progress of the relations between obstructive sleep apnea-hypopnea syndrome and hypothyroidism. Int J Respiration. 2022;42(15):1194–1200.
22. Lencu M, Petrulea M, Alexescu T, Lencu C. Respiratory manifestations in endocrine diseases. Med Pharm Rep. 2016;89(4):459–463. doi:10.15386/cjmed-671
23. Petrone A, Mormile F, Bruni G, Quartieri M, Bonsignore MR, Marrone O. Abnormal thyroid hormones and non-thyroidal illness syndrome in obstructive sleep apnea, and effects of CPAP treatment. Sleep Med. 2016;23:21–25. doi:10.1016/j.sleep.2016.07.002
24. Siafakas NM, Salesiotou V, Filaditaki V, Tzanakis N, Thalassinos N, Bouros D. Respiratory muscle strength in hypothyroidism. Chest. 1992;102(1):189–194. doi:10.1378/chest.102.1.189
25. Chanson P, Attal P. Endocrine aspects of obstructive sleep apnea. J Clin Endocrinol Metab. 2010;95(2):483–495. doi:10.1210/jc.2009-1912
26. Ryan S, Taylor CT, McNicholas WT. Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation. 2005;112(17):2660–2667. doi:10.1161/circulationaha.105.556746
27. Yu L-M, Zhang W-H, Han -X-X, et al. Hypoxia-induced ROS contribute to myoblast pyroptosis during obstructive sleep apnea via the NF-κB/HIF-1α signaling pathway. Oxid Med Cell Longev. 2019;2019:1–19. doi:10.1155/2019/4596368
28. Resta O, Carratù P, Carpagnano GE, et al. Influence of subclinical hypothyroidism and T4 treatment on the prevalence and severity of obstructive sleep apnoea syndrome (OSAS). J Endocrinol Invest. 2005;28(10):893–898. doi:10.1007/bf03345320
29. Zhang X, Zhang G, Wang S, Jin J, Zhang S, Teng X. The change in thyroid function categories with time in patients with subclinical hypothyroidism: a systematic review and meta-analysis. BMC Endocr Disord. 2024;24(1):224. doi:10.1186/s12902-024-01754-7
30. Zwillich C, Devlin T, White D, Douglas N, Weil J, Martin R. Bradycardia during sleep apnea. Characteristics and mechanism. J Clin Invest. 1982;69(6):1286–1292. doi:10.1172/jci110568
31. Bielicki P, Przybyłowski T, Kumor M, Barnaś M, Wiercioch M, Chazan R. Thyroid hormone levels and TSH activity in patients with obstructive sleep apnea syndrome. Adv Exp Med Biol. 2016;878:67–71. doi:10.1007/5584_2015_180
32. Wang P, Ma L, Lv Y, Shao D. The efficacy of thyroid hormone replacement therapy in patients with hypothyroidism and OSAHS: a Meta analysis. J Clin Otorhinolaryngol Head Neck Surg. 2017;31(17):1362–1366. doi:10.13201/j.issn.1001-1781.2017.17.017
33. Lu D, Li N, Yao X, Zhou L. Potential inflammatory markers in obstructive sleep apnea-hypopnea syndrome. Bosnian J Basic Med Sci. 2016. doi:10.17305/bjbms.2016.1579
34. Drugarin D, Negru S, Koreck A, Zosin I, Cristea C. The pattern of a T(H)1 cytokine in autoimmune thyroiditis. Immunol Lett. 2000;71(2):73–77. doi:10.1016/s0165-2478(99)00156-x
35. Nanba T, Watanabe M, Inoue N, Iwatani Y. Increases of the Th1/Th2 cell ratio in severe Hashimoto’s disease and in the proportion of Th17 cells in intractable Graves’ disease. Thyroid. 2009;19(5):495–501. doi:10.1089/thy.2008.0423
36. Fang X, Wang L, Xu C, et al. The association of lymphocyte with hypothyroidism in obstructive sleep apnea. BMC Pulm Med. 2024;24(1):60. doi:10.1186/s12890-024-02872-7
37. Shekhar S, Hall JE, Klubo-Gwiezdzinska J. The hypothalamic–pituitary–thyroid axis and sleep. Curr Opin Endocr Metab Res. 2021;17:8–14. doi:10.1016/j.coemr.2020.10.002
38. Moon S-H, Lee B-J, Kim S-J, Kim H-C. Relationship between thyroid stimulating hormone and night shift work. Ann Occupational Environm Med. 2016;28(1). doi:10.1186/s40557-016-0141-0
39. Yan Y, Li J, Tang H, et al. Elevated thyroid-stimulating hormone levels are associated with poor sleep: a cross-sectional and longitudinal study. Endocrine. 2021;75(1):194–201. doi:10.1007/s12020-021-02849-0
40. Li Y, Zhang W, Liu M, et al. Imbalance of autophagy and apoptosis induced by oxidative stress may be involved in thyroid damage caused by sleep deprivation in rats. Oxid Med Cell Longev. 2021;2021(1):1–10. doi:10.1155/2021/5645090
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Overweight/Obese Status Synergistically Worsens Nocturnal Time-to-Time Blood Pressure in Children with Obstructive Sleep Apnea
Wu Y, Geng X, Xu Z, Ni X
Nature and Science of Sleep 2022, 14:1261-1271
Published Date: 15 July 2022