")
Back to Journals » Infection and Drug Resistance » Volume 18
Prevalence and Clinical Implications of Pyrazinamide Resistance in Newly Diagnosed TB Patients in Uganda
Authors Ndawula C, Petra NP , Wasswa FB, Bazira J
Received 11 February 2025
Accepted for publication 26 March 2025
Published 29 March 2025 Volume 2025:18 Pages 1629—1635
DOI https://doi.org/10.2147/IDR.S491770
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Christopher Ndawula, Nalumaga Pauline Petra, Fredrickson B Wasswa, Joel Bazira
Department of Microbiology, Mbarara University of Science and Technology, Mbarara, 1410, Uganda
Correspondence: Joel Bazira, Email [email protected]
Background: Globally, 10.8 million people were diagnosed with tuberculosis during 2023 causing approximately 1.3 million deaths. This study aimed to assess the prevalence and characterization of pyrazinamide resistance by detecting the pncA gene among newly diagnosed Mycobacterium tuberculosis patients attending Bombo General Military Hospital, Central Uganda.
Methods: Cross-sectional study looking at newly diagnosed TB patients in Bombo General Military Hospital. The sputum samples were confirmed TB positive using GeneXpert PCR technology, DNA extraction using the CTAB method, DNA amplification, and finally gel electrophoresis for pncA gene detection.
Results: A total of 166 sputum-positive tuberculosis samples were analyzed. Males were 91/166 (55%), while 115 (70%) of the positive sputum samples were positive HIV status. The majority (96%) of the newly diagnosed Mycobacterium tuberculosis patients showed no detection of rifampicin resistance, while the rest 6/160 (4%) showed indeterminate rifampicin resistance. Of the 52 (31%) patients with positive pncA gene, 29 (56%) had HIV positive status 18 (34%) had unknown HIV status and 5 (10%) had negative HIV status. It was observed that only one patient 1 (2%) showed both rifampicin and pyrazinamide resistance and was a female patient aged 42 years of age with positive HIV status and positive pncA gene status.
Conclusion: This study reveals the important trends regarding drug resistance and its relationship with HIV status. The majority of patients (96%) did not exhibit rifampicin resistance, suggesting that multi-drug-resistant tuberculosis is not widespread among the newly diagnosed cases. The majority (56%) of the patients with the pncA gene mutation, were HIV-positive. This highlights the potential vulnerability of HIV-positive TB patients to multidrug resistance though the overall pyrazinamide resistance rate remains low.
Keywords: pncA gene, pyrazinamide resistance, tuberculosis, Uganda
Introduction
Tuberculosis (TB) remains the leading cause of morbidity and mortality worldwide as a result of the emergence of drug-resistant Mycobacterium tuberculosis.1 Drug-resistant tuberculosis is a very serious concern with over 500,000 estimated cases of multi-drug resistant TB/Rifampicin resistance in 2020.2 This is a result of a low treatment success rate with only 57% of the patients on conventional treatment regimens achieving success against a set target of 75%.1 Globally, 10.8 million were diagnosed with tuberculosis in 2023,3 and 10.6 million people were diagnosed with tuberculosis during the year 2022, from the estimates of 10.3 million in 2021 causing approximately 1.3 million deaths recorded in 2024.4 The gap between the incident rates and notified cases narrowed to an estimate of 3.1 million in 2022 down from 1.4 million in both years of 2020 and 2021 and then back to the pre-pandemic level of 2019.5
Mycobacterium tuberculosis is one of the communicable diseases that are still major ill health causes as well as a leading cause of death globally. During the previous coronavirus pandemic period, TB was ranked as the lead cause of death with a single infectious agent, putting it above Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome.6
Pyrazinamide (PZA) is one of the first-line anti-tuberculosis drugs that perform a critical role in the management of both drug-susceptible and multidrug-resistant tuberculosis, especially in the early stages of infection.7 The antibacterial activity of PZA requires an enzyme, known as pyrazinamide, which is a pncA gene encoded found in PZA-susceptible tubercle bacilli. The amidase converts the pyrazinamide to pyrazinoic acid (POA), which has antituberculosis properties. It has also been reported that the pyrazinamidase activity of a given strain of M. tuberculosis correlates with its susceptibility to PZA8 and any mutational changes within the pncA gene can lead to pyrazinamide resistance.9 However, resistance to pyrazinamide has emerged as a growing global concern, especially in regions with high TB burden and HIV co-infection.10
Recent studies show that pyrazinamide resistance is increasingly prevalent, with a global rate of approximately 11% to 58% in multi-drug resistant (MDR) TB cases.11,12 In sub-Saharan Africa, pyrazinamide resistance has been found to vary, but studies suggest a notable increase in areas with high TB and HIV co-infection rates.13 In Uganda, while the national TB program has focused on monitoring rifampicin and isoniazid resistance, there are limited data on the prevalence of pyrazinamide resistance, particularly in the context of newly diagnosed TB cases. This gap in data underscores the need for studies focusing on pyrazinamide resistance to better inform treatment strategies.
Pyrazinamide resistance is often linked to the pncA gene, which encodes for pyrazinamidase enzyme.14 There has been a high occurrence of pyrazinamide resistance among Mycobacterium tuberculosis patients on both standard and new drug regimens, which has indicated a higher demand for routine testing of pyrazinamide resistance through detection of the pncA gene.15
In Uganda, where HIV prevalence is high and TB is a significant public health concern, understanding the prevalence of pyrazinamide resistance and the role of pncA gene mutations is vital. HIV progression and treatment of TB are well documented, with HIV-positive patients being more susceptible to developing resistant strains due to their immunocompromised status. However, the interplay between pyrazinamide resistance and HIV co-infection in Uganda remains poorly understood.
Methods
Study Design and Setting
This study is a cross‐sectional and laboratory-based study that was conducted at the Department of Microbiology, Bombo General Military Hospital laboratory where sputum positive Mycobacterium tuberculosis samples were collected by simple random sampling technique as well as following the Clinical Laboratory Standard Institute guidelines, 2022 for sputum collection.
The study population comprised newly diagnosed sputum-positive clients confirmed with GeneXpert machine from patients attending the Outpatient department of Bombo General Military Hospital as the entry point into the hospital with the ages between 14 and 80 years.
Sample Size
The formulae of Kish and Leslie (1965) estimated the sample size using the prevalence of 12.8%.16 The sample size estimation was 166 positive sputum Mycobacterium tuberculosis patients confirmed using the GeneXpert machine.
Laboratory Procedures
Sample Processing
The sample processing was done under biosafety cabinet level 3 for the containment of microorganisms. The GeneXpert assay was employed in this study. This was done by transferring at least 1 mL of the suspended sputum into a conical, screw-capped tube having the Cepheid GeneXpert MTB/RIF Assay for Mycobacterium tuberculosis detection and rifampicin resistance identification. The GeneXpert MTB/RIF test was done for both MTB detection and Rifampicin resistance identification among collected samples before proceeding to molecular techniques.
pncA Gene Amplification
DNA extraction from sputum was done using Cetyltrimethylammonium bromide (CTAB).
The primers used included; forward primer pncA-F (50-GGCCCGATGAAGGTGTCGTA) and reverse primer pncA-R (50-CGGACGGATTTGTCGCTCACTAC). The pncA primers were designed according to the Mycobacterium tuberculosis reference sequence (GenBank accession number AL123456.3).
The PCR master mix was prepared as follows: 2.5µL 10x buffer, 0.5 µL dNTPs, 0.5 Taq polymerase, New England Bio-labs, 0.5µL forward (10µM), 0.5µL reverse (10µM), 3.0µL DNA template and 17.5µL RNAase-Free-H2O making up to 25.0µL final reaction volume.
PCR Amplification/Cycling
The PCR amplification was carried out in a conventional PCR Thermocycler (CLASSIC K960 Thermal Cycler), a pre-denaturation step at 98°C for 10 min, denaturation at 98°C for 15s, annealing at 61.2°C for 15s, extension at 72°C for 10s, and terminated with final extension at 72°C for 5 min for 40 cycles.17 Electrophoresis was run at 200V and 80mA for 1 hour. Bands were visualized using the Gene-Flash Trans-illuminator.
Data Analysis
The data were analyzed using STATA software version 17. Categorical variables have been expressed as numbers (n) and percentages (%). All tables have been constructed.
Results
Demographics of the Newly Diagnosed Mycobacterium tuberculosis Patients
A total of 166 sputum-positive Mycobacterium tuberculosis samples were analyzed. The majority (53%, n = 88) were adults aged 30–49 years, with a mean patient age of 36 years (range: 14–80 years). Males constituted 55% (n = 91) of the sample population, and 70% (n = 115) of positive sputum samples were HIV-positive.
Prevalence of Pyrazinamide Resistance Among Newly Diagnosed Mycobacterium tuberculosis Patients
The majority 160/166 (96%) of the newly diagnosed Mycobacterium tuberculosis patients showed no detection of the rifampicin resistance while the rest 6/160 (4%) showed indeterminate rifampicin resistance. Further, still, the data analyzed below reveal the pncA status gene shows more than two-thirds 114 (69%) of the patients did not have any mutations and therefore had no resistance to the Mycobacterium tuberculosis treatment while 2 (31%) of the patients showed resistance to the tuberculosis treatment (Table 1).
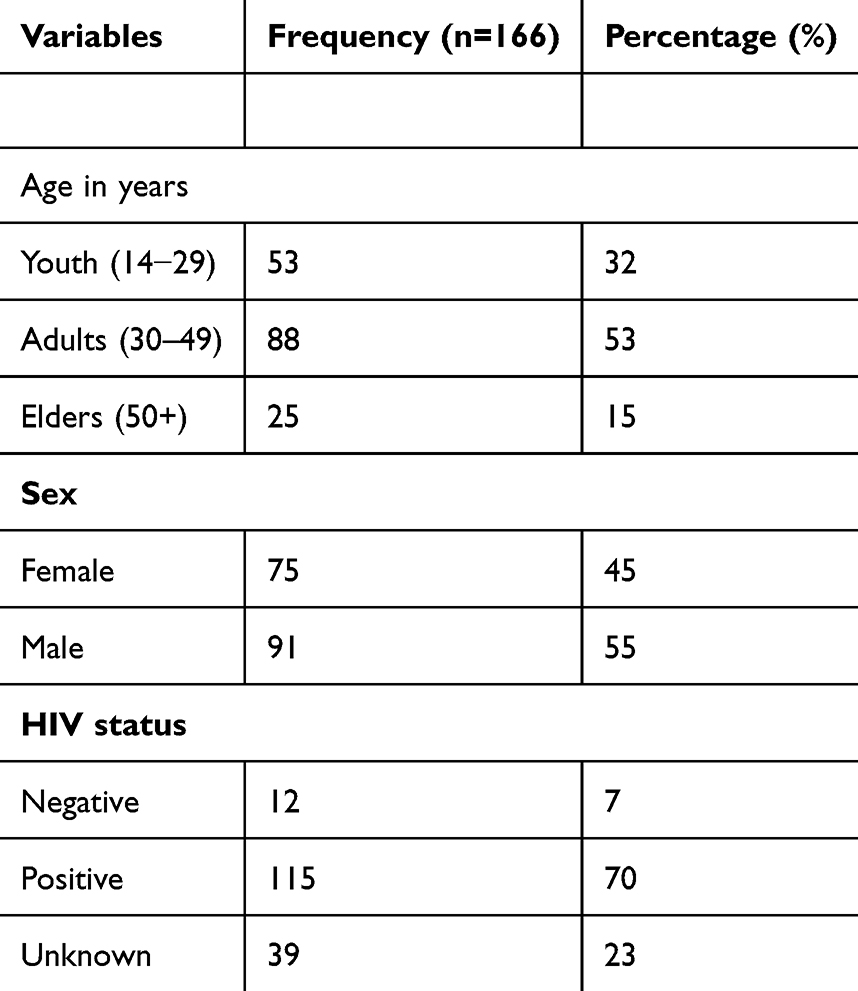 |
Table 1 Demographics of Newly Diagnosed Mycobacterium tuberculosis Patients in Bombo General Military Hospital |
Pyrazinamide Resistance Detection Among the Demographics of Newly Diagnosed MTB Patients
The newly diagnosed Mycobacteria tuberculosis patients with pyrazinamide resistance were mainly adults aged between 30 and 49 years. Pyrazinamide resistance was majorly detected in those who had a positive HIV status 29 (56%) (Table 2).
 |
Table 2 Shows Pyrazinamide Resistance Detection Across Demographics of New MTB Patients |
Prevalence of Pyrazinamide Resistance Among Newly Diagnosed MTB Patients
Majority 160/166 (96%) of the newly diagnosed Mycobacteria tuberculosis patients showed no detection of the rifampicin resistance, while the rest 6/160 (4%) showed indeterminate rifampicin resistance while using the GeneXpert machine. Further still, the pncA status gene showed more than two-thirds 114 (69%) of the patients were of a negative status indicating no resistance to the tuberculosis treatment. However, 52 (31%) of the patients showed resistance to the tuberculosis treatment.
The Proportion of Rifampicin Resistance in Pyrazinamide Resistance Among Newly Diagnosed MTB Patients
It was observed that only one patient (2%) showed co-existence of pyrazinamide resistance and rifampicin resistance. This was a middle-aged female newly diagnosed with pulmonary mycobacterium, with rifampicin resistance, indeterminate results on GeneXpert and positive HIV status.
Discussion
Pyrazinamide is a very important anti-tuberculosis drug that plays a key role in shortening MTB treatment therapeutic duration by killing the non-replicating persistent MTB hence making it a preferred drug in both susceptible and MDR-TB regimens.8,17–19 Excessive or increased acidic conditions can also lead to unreliable results of PZA susceptibility tests, hence the inaccurate susceptibility results of PZA leading to the improper treatment of TB and spread of PZA resistance.20
This study provides insight into the prevalence of pyrazinamide resistance among newly diagnosed TB patients in Uganda, highlighting key associations with HIV status. This study illustrated that pyrazinamide resistance is much higher among the youth than in the elderly. The above findings are similar to various research worldwide6,7,21,22 where the majority were within the age brackets of 30–59 years (60.2%) followed by age below 30 years. The age statistical findings in both studies are similar because of the similar population dynamics where the youths were the majority in both research areas as well as the majority that considered participating in the study.
The majority of the positive pncA gene were male 60% (31/52) which was similar to many other studies.9,17 The higher prevalence among males may reflect the military setting’s demographics, where men are overrepresented. A higher prevalence of the pncA gene 56% (29/52) among the HIV-positive patients was in agreement with similar findings in Uganda.23 Additionally, the high prevalence among HIV-positive patients highlights the need for integrated TB and HIV management strategies. However, our study showed a positive moderation association between the HIV status of patients and the presence of the PncA gene, which was contrary to many studies. Having one pncA gene and rifampicin resistance may be attributed to the small sample size used in this study research, hence not mimicking the actual data for the large population. Several studies such as in Pakistan,24 and China17 reported a higher prevalence in the sample population. This discrepancy may be due to differences in sample populations, prior TB treatment exposure, and local epidemiological factors.
The presence of pncA gene mutations as the primary mechanism of pyrazinamide resistance is well documented.9 The enzyme pyrazinamidase, encoded by pncA, is responsible for converting pyrazinamide into its active form, pyrazinoic acid (POA). Mutations in this gene disrupt enzymatic activity, leading to drug resistance.9 Given the high prevalence of HIV among TB patients in this study (70%), immunosuppression may contribute to increased genetic variability in M. tuberculosis, potentially facilitating the emergence of pncA mutations. Additionally, co-infection with HIV is associated with more rapid disease progression and altered drug pharmacokinetics, which could influence resistance patterns.10
These results emphasize the need for routine molecular testing for pncA mutations to enhance TB treatment strategies. Currently, pyrazinamide resistance is not considered in the standard TB diagnostic algorithms, yet its detection is crucial for optimizing therapy, particularly in MDR-TB cases.25 Incorporating pncA mutation screening into routine TB diagnostic workflows could help refine treatment regimens and prevent treatment failure. Furthermore, given the observed association between pncA mutations and HIV-positive status, targeted resistance testing in this high-risk group could improve patient outcomes.
The study sample was limited to newly diagnosed MTB patients, excluding those already undergoing treatment or on second-line regimens. This limits the generalizability of findings to the broader TB population. Lack of genotypic data on specific mutations within the pncA gene that could further explain resistance mechanisms. The study was conducted in a single facility (Bombo General Military Hospital), which may not represent the population dynamics and TB resistance patterns in other regions of Uganda.
Future studies should include a larger and more diverse sample size to capture resistance patterns in different TB populations, including patients on second-line treatment. Strengthen surveillance systems for TB drug resistance as well as incorporate advanced genotypic and phenotypic testing to identify specific pncA mutations and their role in pyrazinamide resistance to guide public health policies and optimize resource allocation.
Conclusion
This study reveals important trends regarding drug resistance and its relationship with HIV status. The majority of patients (96%) did not exhibit rifampicin resistance, suggesting that multi-drug-resistant tuberculosis is not widespread among the newly diagnosed cases.
However, despite the low prevalence of pyrazinamide resistance overall, with only 1 (2%) patient showing resistance to both rifampicin and pyrazinamide, there was a notable association between pyrazinamide resistance and HIV-positive status. The majority (56%) of the patients with the pncA gene mutation, which is associated with pyrazinamide resistance, were HIV-positive. This highlights the potential vulnerability of HIV-positive TB patients to multidrug resistance, even when the overall pyrazinamide resistance rate remains low. Furthermore, this research provided insights into pyrazinamide and rifampicin resistance, highlighting implications for diagnostic accuracy, initial drug regimens, and strategies to mitigate the global TB economic burden.
Data Sharing Statement
The datasets of the current study are available at the DC laboratory-Mbarara City, western Uganda, and the datasets will be shared with the corresponding author upon reasonable request.
Ethical Consideration
This study complies with the Declaration of Helsinki. Ethical clearance numbered MUST-2023-860 dated 23/10/2023 was obtained from MUST-Research Ethical Committee through Faculty Research committee (FRC), Mbarara University of Science and Technology and UPDF/JCOS/A16 dated 05/7/2023 from Joint Chief of Staff’s office, UPDF-HQ, Mbuya through Bombo general military hospital administration where permission was sought for sample collection. Informed consent was obtained from all the study participants before the study commencement.
Acknowledgment
Special thanks to, Dr Kabanda Hilton, Mr Kassaza Kennedy and Miss Tuhamize Barbra for professional guidance, DC laboratories, Chieftaincy of medical services-UPDF, Joint Chief of Staff – UPDF and the entire Department of medical microbiology, Bombo General Military Hospital Laboratory. Lastly, I extended my sincere gratitude towards Oyet Alphonse and Pafula Tanaba who contributed to the data collection.
The data does not include information that can be traced to the subjects’ privacy, such as medical record numbers, addresses, and contact information.
Author Contributions
All authors contributed significantly to the work reported, including research conceptualization, study design, execution, data collection, analysis, and interpretation. All authors contributed to the drafting and critical review of this article, gave final consent to the published version, and agreed to accept responsibility for all elements of the work.
Disclosure
The authors declare that there was no conflicts of interest in this work.
References
1. Andries K, Verhasselt P, Guillemont J, et al. A diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis. Science. 2005;307(5707):223–227. doi:10.1126/science.1106753
2. Chakaya J, Khan M, Ntoumi F, et al. Global tuberculosis report 2020–reflections on the global TB burden, treatment and prevention efforts. Inter J Infect Dis. 2021;113:S7–S12.
3. Goletti D, Meintjes G, Andrade BB, Zumla A, Lee SS. Insights from the 2024 WHO global tuberculosis report–more comprehensive action, innovation, and investments required for achieving WHO end TB goals. Inter J Infect Dis. 2025;150.
4. Goletti D, Al-Abri S, Migliori GB, et al. World tuberculosis day 2024 theme “yes! we can end TB” can be made a reality through concerted global efforts that advance detection, diagnosis, and treatment of tuberculosis infection and disease. Inter J Infect Dis. 2024;139:141. doi:10.1016/j.ijid.2023.11.035
5. Chakaya J, Petersen E, Nantanda R, et al. The WHO global tuberculosis 2021 report–not so good news and turning the tide back to end TB. Inter J Infect Dis. 2022;124:S26–S9.
6. Houben RM, Dodd PJ, Metcalfe JZ. The global burden of latent tuberculosis infection: a re-estimation using mathematical modelling. PLoS Med. 2016;13(10):e1002152. doi:10.1371/journal.pmed.1002152
7. Shi W, Chen J, Feng J, et al. Aspartate decarboxylase (PanD) as a new target of pyrazinamide in Mycobacterium tuberculosis. Emerging Microbes Infect. 2014;3(1):1–8. doi:10.1038/emi.2014.61
8. Steele MA, Des Prez RM. The role of pyrazinamide in tuberculosis chemotherapy. Chest. 1988;94(4):845–850. doi:10.1378/chest.94.4.845
9. Hirano K, Takahashi M, Kazumi Y, Fukasawa Y, Abe C. Mutation in pncA is a major mechanism of pyrazinamide resistance in Mycobacterium tuberculosis. Tubercle Lung Dis. 1998;78(2):117–122.
10. Heidary M, Shirani M, Moradi M, et al. Tuberculosis challenges: resistance, co-infection, diagnosis, and treatment. Eur J Microbiol Immunol. 2022;12(1):1–17. doi:10.1556/1886.2021.00021
11. Wang Z, Tang Z, Heidari H, et al. Global status of phenotypic pyrazinamide resistance in Mycobacterium tuberculosis clinical isolates: an updated systematic review and meta-analysis. J Chemother. 2023;35(7):583–595. doi:10.1080/1120009X.2023.2214473
12. Rajendran A, Palaniyandi K. Mutations associated with pyrazinamide resistance in Mycobacterium tuberculosis: a review and update. Current Microbiol. 2022;79(11):348. doi:10.1007/s00284-022-03032-y
13. Mvelase NR, Singh R, Swe Swe-Han K, Mlisana KP. Pyrazinamide resistance in rifampicin discordant tuberculosis. PLoS One. 2022;17(9):e0274688. doi:10.1371/journal.pone.0274688
14. Somoskovi A, Parsons LM, Salfinger M. The molecular basis of resistance to isoniazid, rifampin, and pyrazinamide in Mycobacterium tuberculosis. Respir Res. 2001;2(1):1–5. doi:10.1186/rr31
15. Dean AS, Auguet OT, Glaziou P, et al. 25 years of surveillance of drug-resistant tuberculosis: achievements, challenges, and way forward. Lancet Infect Dis. 2022;22(7):e191–e6. doi:10.1016/S1473-3099(21)00808-2
16. Whitfield MG, Soeters HM, Warren RM, et al. A global perspective on pyrazinamide resistance: systematic review and meta-analysis. PLoS One. 2015;10(7):e0133869. doi:10.1371/journal.pone.0133869
17. Li K, Yang Z, Gu J, Luo M, Deng J, Chen Y. Characterization of pncA mutations and prediction of PZA resistance in Mycobacterium tuberculosis clinical isolates from Chongqing, China. Front Microbiol. 2021;11:594171. doi:10.3389/fmicb.2020.594171
18. Zhang Y, Shi W, Zhang W, Mitchison D, Hatfull GF, Jacobs WR. Mechanisms of pyrazinamide action and resistance. Microbiology Spectrum. 2014;2(4):
19. Gopal P, Grüber G, Dartois V, Dick T. Pharmacological and molecular mechanisms behind the sterilizing activity of pyrazinamide. Trends Pharmacol Sci. 2019;40(12):930–940. doi:10.1016/j.tips.2019.10.005
20. Bwalya P, Yamaguchi T, Mulundu G, et al. Genotypic characterization of pyrazinamide resistance in Mycobacterium tuberculosis isolated from Lusaka, Zambia. Tuberculosis. 2018;109:117–122. doi:10.1016/j.tube.2017.12.007
21. Hou L, Osei-Hyiaman D, Zhang Z, Wang B, Yang A, Kano K. Molecular characterization of pncA gene mutations in Mycobacterium tuberculosis clinical isolates from China. Epidemiol Infect. 2000;124(2):227–232.
22. Zignol M, Dean AS, Alikhanova N, et al. Population-based resistance of Mycobacterium tuberculosis isolates to pyrazinamide and fluoroquinolones: results from a multicountry surveillance project. Lancet Infect Dis. 2016;16(10):1185–1192. doi:10.1016/S1473-3099(16)30190-6
23. Scorpio A, Lindholm-Levy P, Heifets L, et al. Characterization of pncA mutations in pyrazinamide-resistant Mycobacterium tuberculosis. Antimicrob Agents Chemother. 1997;41(3):540–543. doi:10.1128/AAC.41.3.540
24. Tahseen S, Khanzada FM, Rizvi AH, et al. Isoniazid resistance profile and associated levofloxacin and pyrazinamide resistance in rifampicin resistant and sensitive isolates/from pulmonary and extrapulmonary tuberculosis patients in Pakistan: a laboratory based surveillance study 2015-19. PLoS One. 2020;15(9):e0239328. doi:10.1371/journal.pone.0239328
25. Micheni LN, Kassaza K, Kinyi H, Ntulume I, Bazira J. Rifampicin and isoniazid drug resistance among patients diagnosed with pulmonary tuberculosis in southwestern Uganda. PLoS One. 2021;16(10):e0259221. doi:10.1371/journal.pone.0259221
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.