")
Back to Journals » Infection and Drug Resistance » Volume 18
Rates of Multidrug-Resistant Gram-Negative Bacterial Infections in Hospitalized Non-Immunocompromised Pediatric Patients: A 9-Year Retrospective Study at a Lebanese Tertiary Medical Center
Authors Zakhour R, Khafaja S, Korman R , Boutros CF, El Zein Z, Chmaisse A, Haj M, Haddara A, El-Houry Z, Jbahi M, Chamseddine S, Bou Karroum S, Al Oweini D, Youssef YS, Youssef N, Nasser M, Fayad D, Abi Farraj F, El Nakib C, Isaac I, Lteif M, Araj GF, Dbaibo GS
Received 24 July 2024
Accepted for publication 16 December 2024
Published 20 January 2025 Volume 2025:18 Pages 363—376
DOI https://doi.org/10.2147/IDR.S488436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Ramia Zakhour,1,2,* Sarah Khafaja,1,2,* Rawan Korman,1,* Celina F Boutros,1 Zeinab El Zein,1– 3 Ahmad Chmaisse,1 Magda Haj,1 Amani Haddara,1 Zeina El-Houry,1 Malak Jbahi,1 Sarah Chamseddine,1 Samer Bou Karroum,1 Dana Al Oweini,1 Yolla Salama Youssef,1 Nour Youssef,1,2 Mayse Nasser,1 Danielle Fayad,1 Farida Abi Farraj,1 Clara El Nakib,1 Imad Isaac,1 Mireille Lteif,1 George F Araj,1,4 Ghassan S Dbaibo1– 3
1Center for Infectious Diseases Research (CIDR) and WHO Collaborating Center for Reference and Research on Bacterial Pathogens, American University of Beirut, Beirut, Lebanon; 2Department of Pediatrics and Adolescent Medicine, American University of Beirut Medical Center, Beirut, Lebanon; 3Division of Pediatric Infectious Diseases, Department of Pediatrics and Adolescent Medicine, American University of Beirut Medical Center, Beirut, Lebanon; 4Clinical Microbiology Laboratory, Department of Pathology and Laboratory Medicine, American University of Beirut Medical Center, Beirut, Lebanon
*These authors contributed equally to this work
Correspondence: Ghassan S Dbaibo, Center for Infectious Diseases Research (CIDR), Division of Pediatric Infectious Diseases, Department of Pediatrics and Adolescent Medicine, American University of Beirut Medical Center, Beirut, 1107, Lebanon, Email [email protected]
Introduction: Multidrug resistant (MDR) Gram-negative bacterial infections are considered a major public health threat. The objectives of this study were to describe the epidemiology, potential contributing factors, and antimicrobial resistance patterns associated with infections caused by MDR Gram-negative bacteria (GNB) in non-immunocompromised children and adolescents.
Methods: This was a retrospective observational study conducted at the American University of Beirut Medical Center (AUBMC) from 2009 to 2017. The study included non-immunocompromised patients 18 years of age or younger with infections caused by GNB isolated from a sterile site or nonsterile site in the setting of clinical infection.
Results: A total of 810 episodes of infection with GNB in 674 pediatric patients were identified. The most common pathogens were Enterobacterales followed by Pseudomonas. MDR GNB infections represented 47.8% of the episodes, with alarming MDR rates among Escherichia coli (64.3%), Klebsiella pneumoniae (59.1%) and Acinetobacter species (70.6%). Previous infection with the same organism during the previous 12 months, urinary catheter or cardiac catheterization in the past 30 days had high percentages of infections with MDR GNB. The carbapenem resistance rates were 1.7% in Enterobacterales, 19.8% in Pseudomonas species and 64.7% in Acinetobacter species.
Conclusion: High prevalence of infections with MDR GNB was detected in non-immunocompromised pediatric patients in Lebanon. This poses a significant threat to the pediatric population and underscores the importance of implementing antimicrobial stewardship programs and infection control policies, which are crucial to cope with the burden of these infections, especially in the presence of other ongoing challenges such as the current economic collapse and ongoing war leading to severe antimicrobial shortages.
Keywords: adolescents, antimicrobial resistance, children, gram-negative bacteria, multidrug resistance
Introduction
Antimicrobial resistance (AMR) is one of the leading growing health threats worldwide today, affecting the healthcare, veterinary and agriculture industries. The World Health Organization (WHO) designated AMR as one of the 10 threats to global health in 2019, thus requiring a global coordinated action plan. It has been estimated that by 2050, mortality from AMR could reach 10 million people annually.1,2
Among the leading pathogens contributing to the burden of AMR are multidrug-resistant (MDR) Gram-negative bacteria (GNB) due to their intrinsic resistance and rapid acquisition and spread of new resistance mechanisms.3 The WHO, in 2017, identified 12 bacterial priority pathogens with increasingly limited treatment options due to AMR, nine of which are GNB. They were classified into 3 categories (critical, high, and medium priority) according to the urgency to guide and promote research and development of new antibiotics. Among the critical priority pathogens are Acinetobacter baumannii carbapenem-resistant (CR), Pseudomonas aeruginosa CR and Enterobacterales, formerly Enterobacteriaceae [CR, extended spectrum beta-lactamase (ESBL)-producing].4 The Centers for Disease Control and Prevention (CDC) also included Acinetobacter CR and Enterobacterales CR among the urgent organisms that need immediate attention, while ESBL-producing Enterobacterales and MDR P. aeruginosa were categorized as serious organisms warranting close monitoring.5
In Middle Eastern countries, the dissemination of MDR organisms is a major area of concern driven by multiple predisposing factors including inappropriate use of antibiotics in humans and animals, over-the-counter availability of antibiotics, inadequate infection control measures and the ongoing population migration due to socio-economic conflicts and several war crises.6 GNB are significant contributors to healthcare-associated infections (HAI) among pediatric patients in these countries, with their prevalence and resistance profiles showing geographic variability among pediatric patient populations and institutions. A recent narrative review published in 2023 on the prevalence of HAI caused by GNB among pediatric patients in Middle Eastern countries reported varying rates of MDR GNB ranging from 0% to 100%.7 Local data from both adult and pediatric populations show a rise in the resistance of GNB in Lebanon, especially ESBL-producing and CR organisms.8 A study published in 2016, looking at device-associated infections in pediatric intensive care unit (PICU) patients ≤20 years of age in a tertiary care medical center in Beirut, reported that 80% of Klebsiella isolates and 67% of E. coli isolates were ESBL-producing organisms.9 Another study conducted by Hanna-Wakim et al on the epidemiology of urinary tract infections (UTI) in hospitalized patients <18 years of age, showed that 15% of E. coli and Klebsiella species were ESBL-producing organisms with a remarkable increase over time from around 7% in 2001 to almost 25% in 2011.10 In 2008, Lebanon witnessed the isolation of the first carbapenem-resistant Enterobacterales (CRE), marking the onset of a growing problem.11 Official national AMR data are scarce in Lebanon, with hospitals generating their own antimicrobial susceptibility data annually in the form of pamphlets. A compilation-based surveillance of AMR in Lebanon for the years 2015–2016 conducted in 13 hospitals distributed across different governorates of Lebanon showed that the resistance of Enterobacterales to third-generation cephalosporins and to carbapenems was 41% and 3%, respectively. Moreover, 30% of P. aeruginosa and 87% of Acinetobacter species were CR in this study.12
MDR GNB infections are of particular concern, especially in the pediatric patients who are naturally a vulnerable population depending on the immune system maturity, the presence of underlying comorbidities, and the use of invasive medical devices.7 The increasing use of antibiotics in infants and children and the selective pressure exerted by these agents on the human gut microbiota can result in a drastic change in children’s gut flora, thus acting as a major reservoir for organisms with novel resistance genes.13–16 Although pediatric patients seem to have lower mortality and morbidity associated with resistant infections when compared to adults,17,18 early initiation of appropriate therapy is crucial for increasing survival rates and decreasing morbidity from such infections. It is noteworthy that the treatment of MDR GNB infections poses a real challenge in the pediatric population, especially with the inability of the antibiotic development pipeline to keep up with the pace of rapid emergence of resistance mechanisms and the delayed time to approval of novel agents for the pediatric populations as compared to the adult.19 To overcome this challenge, it is essential to understand the true burden of MDR GNB infections, particularly in areas with limited surveillance data such as the Middle East and North Africa (MENA) region.2,7 For this purpose, the objectives of this study were to describe the epidemiology, potential contributing factors, and antimicrobial resistance pattern for infections with MDR GNB in non-immunocompromised children and adolescents.
Methods
This was a retrospective medical record review of children and adolescents aged 18 years or younger, who were hospitalized with, or developed during hospitalization, Gram-negative bacterial infections, from June 1st, 2009, to June 31st, 2017. The study was conducted at the American University of Beirut Medical Center (AUBMC), a tertiary care medical center located in Beirut, Lebanon. This study was approved by the Institutional Review Board (IRB) at AUBMC (IRB ID: BIO-2017-0298).
A list of all positive cultures yielding GNB was identified through the medical records department. The medical records of patients with positive cultures were reviewed according to the predefined inclusion and exclusion criteria.
Inclusion and Exclusion Criteria
The inclusion criteria comprised: 1 – Positive cultures for GNB collected from a sterile site or nonsterile site in the setting of clinical infection such as tracheal aspirate culture in the presence of clinical and radiographic findings suggestive of pneumonia, wound culture in the setting of surgical wound infection, or others; 2 – Cultures taken from non-immunocompromised patients 18 years of age or younger who were hospitalized during the study period. “Non-immunocompromised patients” refer to individuals whose immune system is fully functional and capable of building up an effective defense against infections, diseases, and external agents. These individuals do not have conditions, treatments, or other factors that weaken their immune response.20–25
To avoid duplication of isolates, cultures obtained on the same day or on different dates but related to the same episode of infection were excluded with only the first culture from each episode being considered, unless it was collected from different sites, or it yielded different organisms or same organisms with different antimicrobial resistance pattern. In cases where different organisms were identified from different sites during the same episode, they were regarded as distinct episodes.
The exclusion criteria were: 1 – Positive cultures for GNB reflecting colonization rather than true infection as per the treating physician; 2 – Incomplete charts; 3 – Episodes of infection with GNB in the outpatient setting; 4 – Cultures taken from immunocompromised patients including patients with hematological malignancies or solid tumors (active or in remission for less than 5 years), IEI, or those receiving long term (>30 days) or high dose (>1 mg per kilogram per day) steroids or other immunosuppressive drugs.24,25
Definitions and Classification
True infections, as opposed to colonization (asymptomatic carrier state), were defined by clinical, biological and imaging characteristics according to the definitions published by international societies on community or healthcare-associated pneumonia,26 bloodstream and catheter-related infections,27 urinary tract infections,28 and other community- and healthcare-associated infections.29,30 The classification of isolates into MDR and non-MDR GNB was based on a standardized international terminology, developed by a consortium of international experts convened through a collaborative effort between the European Centre for Disease Prevention and Control (ECDC) and the CDC. These experts described the acquired resistance profiles in Enterobacterales (other than Salmonella and Shigella), Pseudomonas aeruginosa and Acinetobacter species. MDR was defined as acquired non-susceptibility to at least one agent in three or more antimicrobial categories.31 Other organisms, not included in this definition, were categorized according to the reported result by our Clinical Microbiology Laboratory.32 Stenotrophomonas maltophilia is considered an intrinsically MDR organism.33
Bacterial Isolates, Identification, and Antimicrobial Susceptibility Testing
Isolates of GNB recovered from clinical samples submitted to the Clinical Microbiology Laboratory, Department of Pathology and Laboratory Medicine, AUBMC, were identified using the standard biomedical methods or the matrix-assisted laser desorption/ionization time of flight (MALDI-TOF) system (Bruker Daltonik, GmbH, Bremen, Germany) starting 2015. The antimicrobial susceptibility testing was performed using the disk diffusion test and interpreted according to the Clinical and Laboratory Standards Institute (CLSI) guidelines published each year. When requested by the medical team, the minimal inhibitory concentrations (MICs) of carbapenems, colistin and tigecycline were determined, using the E-test (PDM-Epsilometer, AB Biodisk, Solna, Sweden) in accordance with the manufacturer’s guidelines.
Data Collection
We collected data using a case report form, which included the following information: basic demographic and epidemiological characteristics (age, gender, nationality, and residence), underlying medical comorbidities, placement of invasive device or undergoing invasive procedure in the 30 days prior to infection, previous hospital or pediatric/neonatal intensive care unit (PICU or NICU) admission, surgical intervention or antibiotic use within the previous 12 months, history of previous infection or colonization with the same organism or any other MDR GNB. In addition, outcomes including length of hospital stay, PICU or NICU admission, the need for mechanical ventilation, recurrence of infection or resolution and mortality were recorded. Microbiological data including isolated organisms and antimicrobial resistance profiles were also documented.
Statistical Analysis
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) program, version 29.0 for Windows (IBM, Armonk, NY, USA). Simple descriptive statistics were used to describe organisms’ distribution, factors potentially contributing to MDR GNB infections, and antimicrobial resistance.
Results
During the study period from June 1st, 2009, to June 31st, 2017, a total of 1344 cultures taken from non-immunocompromised patients aged 18 years or younger fulfilled both inclusion and exclusion criteria. After the removal of duplicated cultures, the final analysis comprised 810 episodes in 674 patients. Among these episodes, a total of 893 GNB isolates were recovered. Notably, 387 episodes (47.8%) were associated with MDR GNB, corresponding to 335 patients.
Socio-Demographic, Clinical Characteristics, and Risk Factors
Table 1 highlights the main demographics and baseline characteristics. Both groups (MDR and non-MDR), were similar in terms of gender and age distribution, with a median age of 0.83 (interquartile range 0.25–8.25). Overall, infants less than 12 months of age accounted for approximately half of all GNB infections and of each group separately. MDR GNB infections were more prevalent among non-Lebanese patients. Patients with underlying comorbidities, particularly those with cardiovascular or neurological or renal diseases, were more likely to have MDR GNB infections.
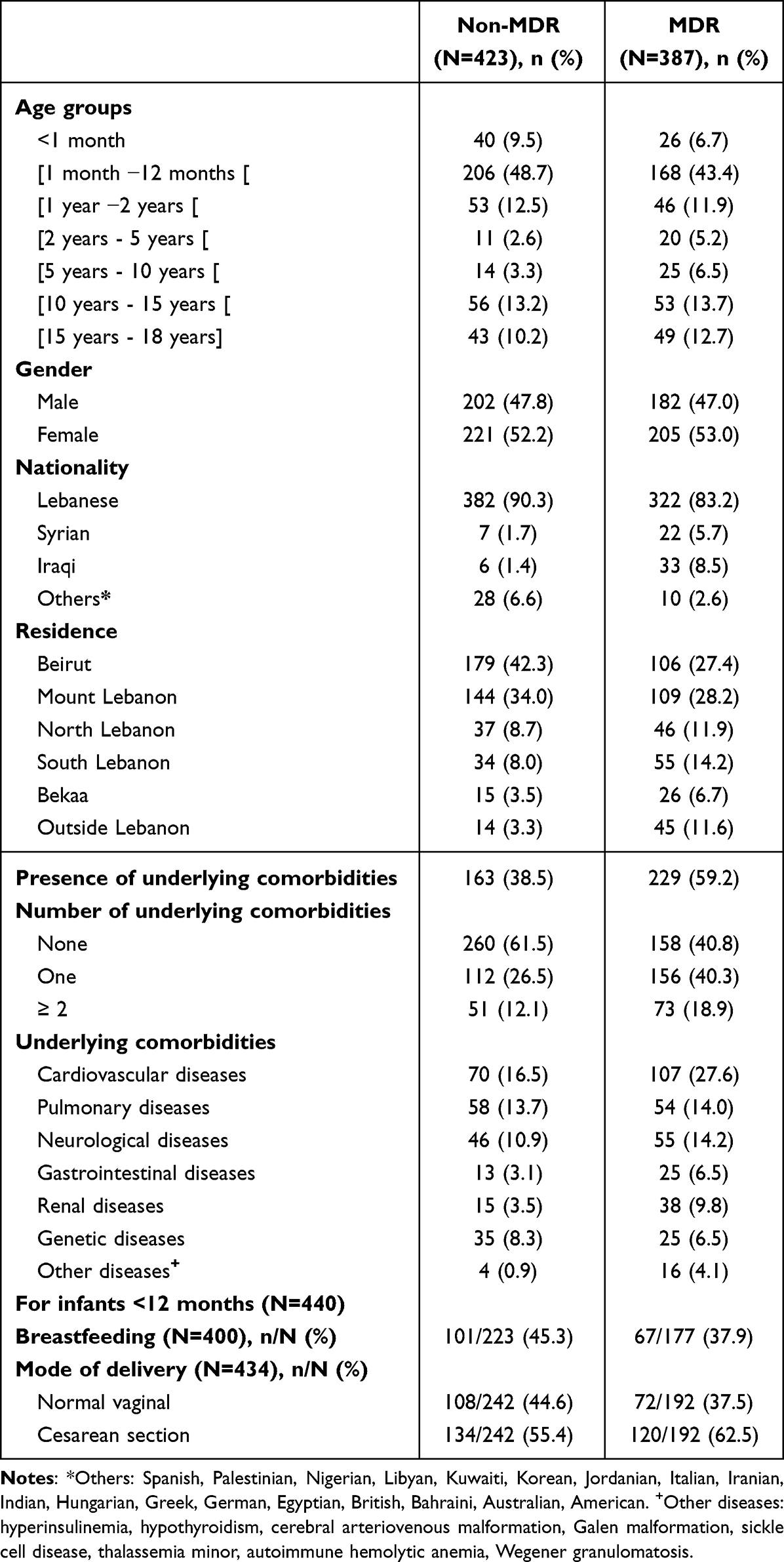 |
Table 1 Demographics and Baseline Characteristics of Pediatric Patients with MDR and Non-MDR GNB Infections |
In Table 2, we displayed the possible contributing factors for MDR GNB infections, patients with previous hospitalizations or previous PICU/NICU admission in the past 12 months had a higher risk of MDR GNB infections. Antibiotic use in the past 30 days or 12 months were associated with a higher risk of developing an MDR GNB infection. Moreover, MDR GNB group had higher frequency of previous infection with the same organism (25% vs 13.6%). Among the main factors observed attributed to MDR GNB episodes were the presence of a central line, feeding tube, or urinary catheter in the past 30 days. Furthermore, mechanical ventilation in the past 30 days increased the percentage of developing MDR GNB infection (33%).
 |
Table 2 Potential Contributing Factors Associated with MDR GNB Infections |
Outcome
As shown in Table 3, patients with MDR GNB infections had a long hospital stay duration (13.10 days). In addition, the need for PICU/NICU admission was high in the MDR group (49.4%).
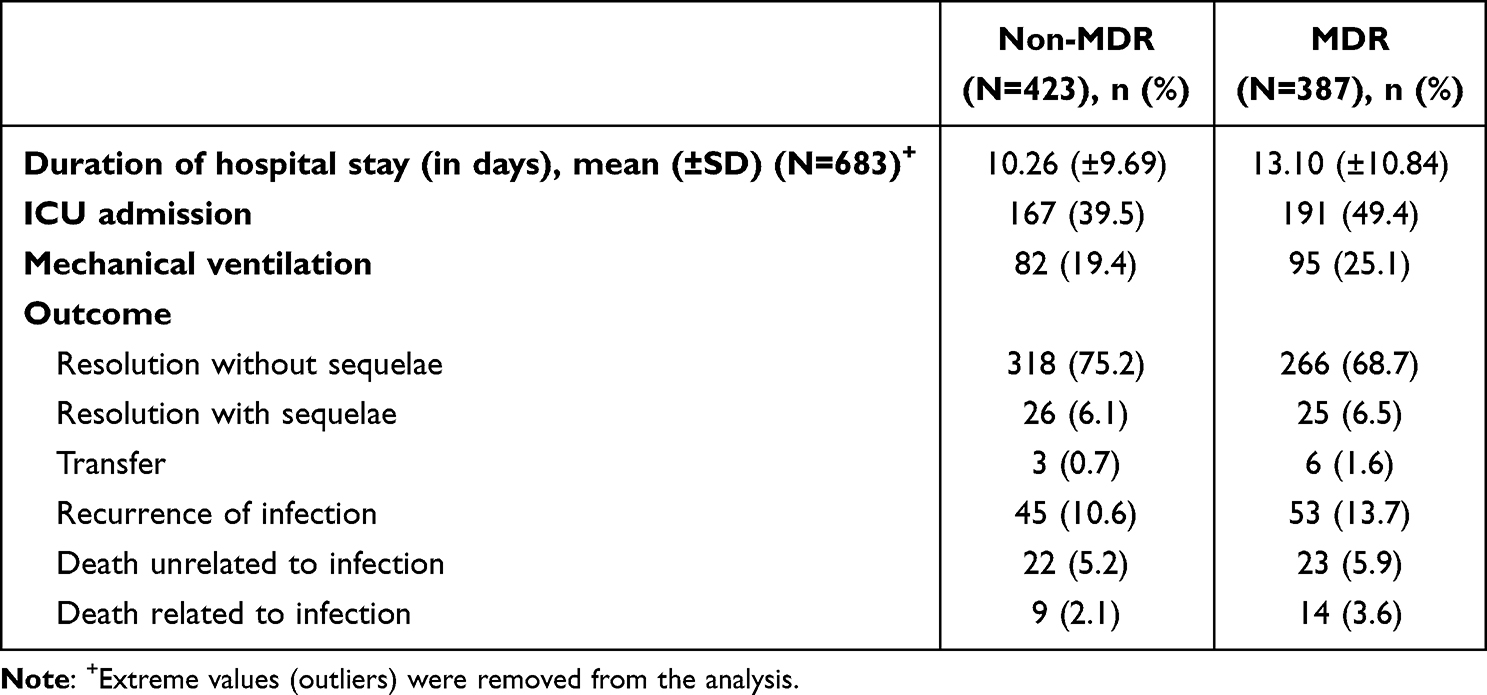 |
Table 3 Outcome |
Microbiology and Antibiotic Susceptibility
The frequency and phenotypic profiles of all isolated GNB are reported in Figures 1 and 1S. The most common isolated GNB were E. coli (38.9%), Pseudomonas species (19.3%) of which Pseudomonas aeruginosa was the most frequent (18%), and Klebsiella species (17.2%), including Klebsiella pneumoniae (16.1%). Among MDR GNB, Enterobacterales were the most frequent organisms, accounting for 83.1%. MDR phenotype was mainly identified in E. coli (223/347, 64.3%), Klebsiella species (91/154, 59.1%) [Klebsiella pneumoniae: 87/144 (60.4%)], and Acinetobacter species (24/34, 70.6%) [Acinetobacter baumannii: 24/29 (82.8%)].
 |
Figure 1 Distribution of the gram-negative bacterial isolates and the rate of their resistance phenotype in infected pediatric patients. The bar chart shows the count of each organism isolated from pediatric infections, with dark gray bars indicating multidrug-resistant (MDR) isolates and light gray bars representing non-MDR isolates. Escherichia coli (38.9%), Pseudomonas species (19.3%), and Klebsiella species (17.2%) are the most commonly isolated organisms. Less frequent isolates include Salmonella species, Enterobacter species, and others. The number of MDR and non-MDR isolates is displayed for each organism to highlight variations in resistance. *Other organisms: Campylobacter coli, Haemophilus influenzae, Moraxella catarrhalis, Morganella morganii, Neisseria meningitidis, Providencia rettgeri and Providencia stuartii. |
Over the 9-year study period, the rate of MDR GNB increased from 40% in 2009 to 56% in 2013 and then remained almost steady between 2014 and 2017, ranging between 45% and 47% (Figure 2). The identified organisms were mainly isolated from urine (n = 329, 36.8%), deep tracheal aspirate or sputum (n = 234, 26.2%), skin and soft tissue (n = 110, 12.3%), stool (n = 77, 8.6%) and blood (n = 72, 8.1%). The most common sources of MDR GNB were from urine (44.1%), respiratory samples (24.7%) and skin and soft tissue (14%) (Figure 3). E. coli was the most common organism isolated from the urinary tract, skin and soft tissue and intra abdominal infections, whereas P. aeruginosa was the most common cause of respiratory tract infections. As for bloodstream infections (BSI), Klebsiella species were the most common organisms followed by Pseudomonas species and E. coli (Supplementary material and Table 1S).
 |
Figure 2 Number of gram-negative bacterial isolates, their resistance phenotype, and percentage of multidrug resistance over the 9-year study period (N=893). The x-axis represents the years from 2009 to 2017 (to note that the included cultures were from June 1st to December 31st for the year 2009 and from January 1st to June 31st for 2017), and the y-axis is the number of organisms per year. The stacked bars indicate the number of non-MDR (light gray) and MDR (dark gray) GNB isolates per year. The line graph represents the annual percentage of MDR gram-negative bacteria, showing trends of multidrug resistance over time. |
 |
Figure 3 The distribution of MDR versus non-MDR gram-negative bacterial isolates by sample source. This bar chart displays the number of MDR (dark gray) and non-MDR (light gray) GNB isolates collected from various sample sources in pediatric patients. The most common sources of GNB isolates are urine (182 MDR, 147 non-MDR) and deep tracheal aspirate or sputum (102 MDR, 132 non-MDR). Blood samples had relatively fewer isolates (29 MDR and 43 non-MDR). Stool and other less common sample sources demonstrated lower total isolate counts, with non-MDR isolates being predominant across most sample types. The table below the chart provides the exact counts of MDR and non-MDR isolates for each sample type, highlighting the distribution of resistance across different infection sites. |
Antimicrobial susceptibility results for Enterobacterales, Pseudomonas species and Acinetobacter species are summarized in Figure 4. Overall, 43.1% of Enterobacterales displayed resistance to third-generation cephalosporins (3GC), 27.1% to fourth-generation cephalosporins (4GC), 24.4% to aminoglycosides, and 19% to fluoroquinolones. Resistance to carbapenems was 1.7% among Enterobacterales.
 |
Figure 4 Antimicrobial susceptibility patterns of select gram-negative bacteria. This figure illustrates the antimicrobial resistance and susceptibility profiles of three groups of gram-negative bacteria: (A) Enterobacterales (N=666), (B) Pseudomonas species (N=172), and (C) Acinetobacter species (N=34). The y-axis shows the percentage of isolates, and the x-axis categorizes various antimicrobial agents used in treatment. Each panel displays the resistance (dark gray) and susceptibility (light gray) percentages for various antimicrobial categories in pediatric isolates. Antimicrobial classes include BLI: β-lactamase inhibitors, 1GC: First generation cephalosporins, 2GC: Second generation cephalosporins, 3GC: Third generation cephalosporins, 4GC: Fourth generation cephalosporins, among others. Enterobacterales (Panel (A) shows high resistance rates to several classes, particularly penicillins, first, second and third-generation cephalosporins. Pseudomonas species (Panel (B) demonstrates notable resistance to carbapenems and fluoroquinolones, while Acinetobacter species (Panel (C) displays extensive resistance across multiple antibiotic classes, especially aminoglycosides and carbapenems. |
All tested Pseudomonas species showed 100% susceptibility to polymyxins, with a slightly reduced susceptibility to aminoglycosides (90.7%). Overall, in vitro resistance rates of these species were 19.8% to carbapenems, 15.7% to antipseudomonal 3GC, 9.9% to 4GC, and 13.6% to fluoroquinolones. Among MDR Pseudomonas species, high rates of resistance were observed against carbapenems (62.1%), fluoroquinolones (65.5%), antipseudomonal 3GC (86.2%), 4GC (58.6%) and monobactams (72.4%). On the other hand, these organisms showed lower rate of resistance to aminoglycosides (34.5%).
Regarding Acinetobacter species, high rates of resistance were observed against aminoglycosides (67.6%), carbapenems (64.7%), 4GC (67.6%), fluoroquinolones (66.7%) folate pathway inhibitors (70.6%) and tetracyclines (76.7%). Similar proportions were observed when dissecting them into species (Figure 2S). Tables 2S-5S (supplementary material) represent the analysis of antimicrobial resistance profiles of E. coli, Klebsiella species, Klebsiella pneumoniae, Pseudomonas aeruginosa and Acinetobacter baumannii.
Discussion
This study aimed to describe the frequency of MDR GNB infections in hospitalized non-immunocompromised patients 18 years of age or younger with infections caused by GNB, associated risk factors as well as the resistance profiles over a 9-year period.
The median age of children with GNB in our study was 0.83 (interquartile range 0.25–8.25). Similar median age was reported by previous studies on GNB BSI in children.34–36 In fact, this age group is at higher risk of UTI compared to older children and usually necessitates hospital admissions for appropriate management.37 Moreover, our medical center is a main referral center for children with congenital heart disease, many of whom undergo corrective surgeries within the first year of life, predisposing them to a higher risk of developing HAI such as central line-associated bloodstream infections, ventilator-associated pneumonia, surgical site infections and others. In addition, this younger age group might be overrepresented in our study due to the inclusion of inpatients only.
The factors predisposing children to infections with MDR organisms include previous infection or colonization with resistant organisms, recent travel to an area with high prevalence of resistant pathogens, prior exposure to broad-spectrum antibiotics, previous hospitalization, indwelling catheters or other foreign medical devices, household members with resistant bacteria, and underlying medical conditions.38–40 Our study revealed that previous infections with the same organism, cardiac catheterization in the past 30 days and urinary catheter in the past 30 days were contributing factors for infections with MDR GNB.
Our study did not demonstrate an association between MDR GNB and mortality, however a longer length of stay was noted among patients with MDR GNB infections. Comparable results were reported by other studies.34,41,42 In fact, initiating the appropriate antibiotics without any delay plays a major contributing factor towards decreasing mortality in these infections.34,41,42 Therefore, lack of data regarding the time of initiation of antimicrobial therapy may mask the true impact of MDR GNB infections on the outcome.
The most common GNB were E. coli (38.9%), Pseudomonas species (19.3%) and Klebsiella species (17.2%). This is in line with the results of other studies.34,36 In addition, GNB were mainly isolated in our study from urine, respiratory, skin and soft tissue, and blood samples. There are several studies showing E. coli as a significant pathogen causing UTI.10,43 A recent narrative review of healthcare-associated gram-negative bacterial infections among pediatric patients in Middle Eastern countries indicated that the prevalence of MDR GNB varied geographically with high rates of MDR reaching 100% in Egypt and Gulf Cooperation Council countries.7 This retrospective study showed that almost 48% of the GNB infections were MDR, with the highest rates of MDR detected among E. coli (64.3%), Klebsiella species (59.1%) and Acinetobacter species (70.6%) which are among the leading pathogens contributing to the burden of AMR as classified by the WHO and the CDC.1,5 A study on the epidemiology of resistant GNB BSI in patients younger than 19 years old, conducted by Geier et al between January 2014 and April 2016 at a Canadian pediatric tertiary care hospital, reported a lower rate of MDR GNB (25.8%)40 which could be explained by the use of different definition for MDR or more stringent AMS programs. Another prospective multicenter study conducted during a 2-year period in six different hospitals in Budapest found that 33.6% of all GNB were MDR with highest rates of E. coli, Enterobacter and Pseudomonas species.34 It is noteworthy to mention that the major resistance mechanism in Enterobacterales is the production of β-lactam hydrolysing enzymes such as ESBL, AmpC beta-lactamases and carbapenemases which confer resistance to the most important antimicrobial agents.12,38 Similarly to our findings, Moghnieh et al in their study on the antimicrobial susceptibility data of isolates from 13 local hospitals in Lebanon reported that 41% and 46% of Enterobacterales were resistant to third-generation cephalosporins and folate pathway inhibitors, respectively.12 In line with these findings, high resistance rates to penicillins (72.6%), penicillins with β-lactamase inhibitors (45.4%), 3GC (43.1%), 4GC (27.1), and aminoglycosides (24.4%) among Enterobacterales are reported in the current study. In addition, our data showed that 13.6% of Enterobacterales were resistant to fluoroquinolones. A previous study by Moghnieh et al reported higher resistance rates to fluoroquinolones among Enterobacterales and this disparity could be attributed to the inclusion of isolates from both pediatric and adult populations since the misuse of this class of antibiotics in adult patients, in particular, is rampant due to its availability over the counter in Lebanese pharmacies.12 In our study, resistance to carbapenems was 1.7% among Enterobacterales. This is particularly challenging as available treatment options in the pipeline are scarce and the development of new, broader-spectrum antibiotics remains relatively stagnant in the pediatric age group.12,38,44
P. aeruginosa is a GNB with great genetic plasticity, intrinsically resistant to most antibiotics via multiple mechanisms, including hyperproduction of enzymes, such as beta-lactamases and DNA-gyrases, active efflux pumps, and permeability changes.42,45 MDR and CR P. aeruginosa are significant threats globally, with MDR rates ranging between 15% and 30% in some geographical areas.46 Our study revealed that 16.8% and 19.8% of Pseudomonas species were MDR and CR respectively. A study conducted by Logan et al in children aged 1 to 17 years between 1999 and 2012, using data from the Surveillance Network Database-USA reported that MDR P. aeruginosa increased from 15.4% in 1999 to 26% in 2012, and CR P. aeruginosa increased from 9.4% in 1999 to 20% in 2012.45 The susceptibility percentages of Pseudomonas species to antipseudomonal 3GC, fluoroquinolones and carbapenems reported by our study are relatively similar to those reported by a compilation-based surveillance of AMR in Lebanon for the years 2015–2016 and by a study conducted in the United States (1999–2012).12,45 Nevertheless, MDR Pseudomonas species in our study showed lower resistance rates to antimicrobial agents compared to findings reported in a recent study conducted by Hafiz et al in Riyadh, Saudi Arabia, including pediatric and adult patients. In the latter study, the authors attributed the high resistance rate to the selective pressure exerted by the overuse of antibiotics, especially during COVID-19 pandemic.47
Acinetobacter baumannii is a Gram-negative coccobacillus, widely distributed in nature, with a remarkable ability to acquire antibiotic resistance and to cause persistent HAI with a high mortality rate.48 Our present study revealed that 70.6% of Acinetobacter species were MDR and their resistance rates to carbapenems, aminoglycosides, cephalosporins, fluoroquinolones, folate pathway inhibitors and tetracyclines were more than 65%. However, these isolates showed high sensitivity only to glycyclines (100%) and polymyxins (92.6%). Our results are consistent with the findings of a study conducted by Shi et al in the pediatric intensive care unit (PICU) of Shanghai Children’s Hospital in China from December 2014 to May 2018.48 In addition, previous studies evaluating the antimicrobial susceptibility patterns of bacterial isolates based on data retrieved from bacteriology laboratories of different hospitals distributed across different governorates of Lebanon showed high resistance rates of Acinetobacter species to most of the antimicrobial agents including carbapenems up to 87%, with blaOXA-48 being the predominantly detected carbapenemase gene, and high susceptibility to tigecycline (80%) and colistin (83%).12,49 Comparing the 2015–2016 Lebanese data to European surveillance data during the same period, the resistance rate to carbapenems among Acinetobacter species in our country was similar to results observed in Romania. However, these rates were higher than values in Spain and Italy while remaining lower than those reported in Croatia and Greece.12,50
The main strength of this study is that it offers scarcely available data about the epidemiology and resistance profiles of MDR GNB infections in the pediatric population in Lebanon and the region. Given its retrospective design, this study has several limitations including missing data and incomplete medical records. The single-center nature of this study limits the generalizability of the results. Furthermore, data on antimicrobial therapy and the time to initiation of appropriate therapy were not readily available and were thus not included in the analysis, this would have allowed us to analyze the impact of these factors on outcomes of the infectious episodes.
Our results highlight the importance of MDR GNB surveillance in the pediatric population to optimize antimicrobial therapy, avoid the spread and transmission of resistance genes, mitigate outbreaks and improve patient outcomes. In fact, vaccines are highly effective tools in combating AMR. However, MDR GNB classified as AMR priority pathogens by the WHO are associated with moderate or low feasibility of vaccine development.51 Consequently, the focus on alternative methods of control such as diagnostic tools, treatments and effective infection prevention is increasingly imperative. Screening and continuous monitoring through whole genome sequencing analysis can effectively limit the dissemination of drug-resistant isolates in hospitalized patients and can help physicians in selecting the optimal treatment.38 Additionally, and perhaps even more importantly, antimicrobial stewardship programs are crucial to decrease the burden of MDR GNB infections. In 2019, the World Health Organization provided guidance on how to implement an ASP in low- and middle-income countries.52 AUBMC had already launched its official ASP in 2017.53 A follow-up study looking at resistance rates following this implementation would be helpful in showing the value of such a program and encouraging other centers in our area of the world to implement them.
Conclusion
Infections with MDR GNB pose a significant growing threat to the pediatric population given the near-empty antibiotic pipeline. Therefore, the findings of our study shed light on the importance of several initiatives and prevention efforts including bacterial surveillance, antimicrobial stewardship programs and enhanced infection control measures. These efforts are crucial to minimize the burden of these infections, particularly in low- and middle-income countries and notably during this critical period of economic collapse exacerbated by the COVID-19 pandemic resulting in shortages in drugs and diagnostic tools.
Data Sharing Statement
Data is available upon request to the corresponding author at [email protected] due to privacy and ethical restrictions.
Ethical approval statement
This study was approved by the Institutional Review Board (IRB) at the American University of Beirut Medical Center (IRB ID: BIO-2017-0298) in line with the World Medical Association, Declaration of Helsinki in 2013. A waiver from obtaining consent from subjects was granted by IRB for this study since we were reviewing medical records retrospectively; all data collected were stripped of patient identifiers, and there is no risk to subjects.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Dr Ghassan Dbaibo reports grants, personal fees from Pfizer, personal fees from MSD, grants from Sanofi/Pasteur, outside the submitted work. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health Organization. Ten threats to global health in. Available from: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
2. Murray CJL, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
3. Koulenti D, Song A, Ellingboe A, et al. Infections by multidrug-resistant gram-negative bacteria: what’s new in our arsenal and what’s in the pipeline? Int J Antimicrob Agents. 2019;53(3):211–224. doi:10.1016/j.ijantimicag.2018.10.011
4. World Health Organization. WHO publishes list of bacteria for which new antibiotics are urgently needed. Available from: https://www.who.int/en/news-room/detail/27-02-2017-who-publishes-list-of-bacteria-for-which-new-antibiotics-are-urgently-needed.
5. CDC. AR threats report. Available from: https://www.cdc.gov/drugresistance/biggest-threats.html.
6. Dandachi I, Chaddad A, Hanna J, Matta J, Daoud Z. Understanding the epidemiology of multi-drug resistant gram-negative bacilli in the middle east using a one health approach. Front Microbiol. 2019;10:1941. doi:10.3389/fmicb.2019.01941
7. Al Dabbagh M, Alghounaim M, Almaghrabi RH, et al. A narrative review of healthcare-associated gram-negative infections among pediatric patients in Middle Eastern Countries. Infect Dis Ther. 2023;12(5):1217–1235. doi:10.1007/s40121-023-00799-w
8. El-Herte RI, Kanj SS, Matar GM, Araj GF. The threat of carbapenem-resistant Enterobacteriaceae in Lebanon: an update on the regional and local epidemiology. J Infect Public Health. 2012;5(3):233–243. doi:10.1016/j.jiph.2012.02.003
9. Ismail A, El-Hage-Sleiman AK, Majdalani M, Hanna-Wakim R, Kanj S, Sharara-Chami R. Device-associated infections in the pediatric intensive care unit at the American University of Beirut Medical Center. J Infect Dev Countries. 2016;10(6):554–562. doi:10.3855/jidc.7303
10. Hanna-Wakim RH, Ghanem ST, El Helou MW, et al. Epidemiology and characteristics of urinary tract infections in children and adolescents. Front Cell Infect Microbiol. 2015;5:45. doi:10.3389/fcimb.2015.00045
11. Matar GM, Cuzon G, Araj GF, et al. Oxacillinase-mediated resistance to carbapenems in Klebsiella pneumoniae from Lebanon. Clin Microbiol Infect. 2008;14(9):887–888. doi:10.1111/j.1469-0691.2008.02059.x
12. Moghnieh R, Araj GF, Awad L, et al. A compilation of antimicrobial susceptibility data from a network of 13 Lebanese hospitals reflecting the national situation during 2015–2016. Antimicrob Resist Infect Control. 2019;8(1):41. doi:10.1186/s13756-019-0487-5
13. Arrieta MC, Stiemsma LT, Amenyogbe N, Brown EM, Finlay B. The intestinal microbiome in early life: health and disease. Front Immunol. 2014;5:427. doi:10.3389/fimmu.2014.00427
14. Mitsou EK, Kirtzalidou E, Pramateftaki P, Kyriacou A. Antibiotic resistance in faecal microbiota of Greek healthy infants. Beneficial Microbes. 2010;1(3):297–306. doi:10.3920/BM2010.0007
15. Moore AM, Ahmadi S, Patel S, et al. Gut resistome development in healthy twin pairs in the first year of life. Microbiome. 2015;3:27. doi:10.1186/s40168-015-0090-9
16. Francino MP. Antibiotics and the human gut microbiome: dysbioses and accumulation of resistances. Front Microbiol. 2015;6:1543. doi:10.3389/fmicb.2015.01543
17. Chiotos K, Han JH, Tamma PD. Carbapenem-resistant Enterobacteriaceae infections in children. Curr Infect Dis Rep. 2016;18(1):2. doi:10.1007/s11908-015-0510-9
18. Logan LK. Carbapenem-resistant Enterobacteriaceae: an emerging problem in children. Clin Infect Dis. 2012;55(6):852–859. doi:10.1093/cid/cis543
19. Hawken SE, Snitkin ES. Genomic epidemiology of multidrug-resistant gram-negative organisms. Ann N.Y. Acad Sci. 2019;1435(1):39–56. doi:10.1111/nyas.13672
20. Center for Disease Control and Prevention. People who are immunocompromised. Available from: https://archive.cdc.gov/www_cdc_gov/coronavirus/2019-ncov/need-extra-precautions/people-who-are-immunocompromised.html.
21. Center for Disease Control and Prevention. 2007 Guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings- last update on September 2024. Available from: https://www.cdc.gov/infection-control/hcp/isolation-precautions/?CDC_AAref_Val=https://www.cdc.gov/infectioncontrol/guidelines/isolation/index.html#toc;https://www.cdc.gov/infection-control/media/pdfs/Guideline-Isolation-H.pdf.
22. Center for Disease Control and Prevention. Immunity Types. Available from: https://www.cdc.gov/vaccines/basics/immunity-types.html.
23. National Cancer Institute. immunocompromised. Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/immunocompromised.
24. Lemiale V, Mokart D, Resche-Rigon M, et al. Effect of noninvasive ventilation vs oxygen therapy on mortality among immunocompromised patients with acute respiratory failure: a randomized clinical trial. JAMA. 2015;314(16):1711–1719. doi:10.1001/jama.2015.12402
25. Russell L, Pène F, Martin-Loeches I. Multidrug-resistant bacteria in the grey shades of immunosuppression. Intensive Care Med. 2023;49(2):216–218. doi:10.1007/s00134-022-06968-8
26. Bradley JS, Byington CL, Shah SS, et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the pediatric infectious diseases society and the infectious diseases society of America. Clin Infect Dis. 2011;53(7):e25–e76. doi:10.1093/cid/cir531
27. Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the infectious diseases society of America. Clin Infect Dis. 2009;49(1):1–45. doi:10.1086/599376
28. Mattoo TK, Shaikh N, Nelson CP. Contemporary management of urinary tract infection in children. Pediatrics. 2021;147(2). doi:10.1542/peds.2020-012138
29. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the surgical infection society and the infectious diseases society of America. Clin Infect Dis. 2010;50(2):133–164. doi:10.1086/649554
30. Kreitmann L, Vasseur M, Jermoumi S, et al. Relationship between immunosuppression and intensive care unit-acquired colonization and infection related to multidrug-resistant bacteria: a prospective multicenter cohort study. Intensive Care Med. 2023;49(2):154–165. doi:10.1007/s00134-022-06954-0
31. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
32. CLSI. Performance standards for antimicrobial susceptibility testing.
33. Brooke JS. Stenotrophomonas maltophilia: an emerging global opportunistic pathogen. Clin Microbiol Rev. 2012;25(1):2–41. doi:10.1128/CMR.00019-11
34. Ivády B, Kenesei É, Tóth-Heyn P, et al. Factors influencing antimicrobial resistance and outcome of Gram-negative bloodstream infections in children. Infection. 2016;44(3):309–321. doi:10.1007/s15010-015-0857-8
35. Folgori L, Livadiotti S, Carletti M, et al. Epidemiology and clinical outcomes of multidrug-resistant, gram-negative bloodstream infections in a European tertiary pediatric hospital during a 12-month period. Pediatr Infect Dis J. 2014;33(9):929–932. doi:10.1097/INF.0000000000000339
36. Aizawa Y, Shoji T, Ito K, et al. Multidrug-resistant gram-negative bacterial bloodstream infections in children’s hospitals in Japan, 2010–2017. Pediatr Infect Dis J. 2019;38(7):653–659. doi:10.1097/INF.0000000000002273
37. Kathryn OB, Adrian E, Kerenza H, Christopher CB. Prevalence of urinary tract infection in acutely unwell children in general practice: a prospective study with systematic urine sampling. Br J Gen Pract. 2013;63(607):e156. doi:10.3399/bjgp13X663127
38. Moxon CA, Paulus S. Beta-lactamases in Enterobacteriaceae infections in children. J Infect. 2016;72:S41–S49. doi:10.1016/j.jinf.2016.04.021
39. Zaoutis TE, Goyal M, Chu JH, et al. Risk factors for and outcomes of bloodstream infection caused by extended-spectrum β-lactamase–producing Escherichia coli and Klebsiella species in children. Pediatrics. 2005;115(4):942–949. doi:10.1542/peds.2004-1289
40. Geier R, Liu S, Tilley P, et al. Epidemiology of antibiotic resistant gram-negative bacteremia in a hospital-based pediatric population. Pediatrics. 2018;142(1_MeetingAbstract):567. doi:10.1542/peds.142.1MA6.567
41. Lye DC, Earnest A, Ling ML, et al. The impact of multidrug resistance in healthcare-associated and nosocomial gram-negative bacteraemia on mortality and length of stay: cohort study. Clin Microbiol Infect. 2012;18(5):502–508. doi:10.1111/j.1469-0691.2011.03606.x
42. Labib JR, Ibrahim SK, Salem MR, Youssef MRL, Meligy B. Infection with gram-negative bacteria among children in a tertiary pediatric hospital in Egypt. Am J Infect Control. 2018;46(7):798–801. doi:10.1016/j.ajic.2017.12.008
43. Nagvekar V, Sawant S, Amey S. Prevalence of multidrug-resistant Gram-negative bacteria cases at admission in a multispeciality hospital. J Global Antimicrob Resist. 2020;22:457–461. doi:10.1016/j.jgar.2020.02.030
44. Aguilera-Alonso D, Escosa-García L, Saavedra-Lozano J, Cercenado E, Baquero-Artigao F. Carbapenem-resistant gram-negative bacterial infections in children. Antimicrob Agents Chemother. 2020;64(3). doi:10.1128/AAC.02183-19
45. Logan LK, Gandra S, Mandal S, et al. Multidrug- and carbapenem-resistant pseudomonas aeruginosa in children, United States, 1999-2012. J Pediatric Infect Dis Soc. 2017;6(4):352–359. doi:10.1093/jpids/piw064
46. Horcajada Juan P, Montero M, Oliver A, et al. Epidemiology and treatment of multidrug-resistant and extensively drug-resistant pseudomonas aeruginosa infections. Clin Microbiol Rev. 2019;32(4). doi:10.1128/cmr.00031-00019
47. Hafiz TA, Bin Essa EA, Alharbi SR, et al. Epidemiological, microbiological, and clinical characteristics of multi-resistant pseudomonas aeruginosa isolates in King Fahad Medical City, Riyadh, Saudi Arabia. Trop Med Infect Dis. 2023;8(4):205. doi:10.3390/tropicalmed8040205
48. Shi J, Sun T, Cui Y, et al. Multidrug resistant and extensively drug resistant Acinetobacter baumannii hospital infection associated with high mortality: a retrospective study in the pediatric intensive care unit. BMC Infect Dis. 2020;20(1):597. doi:10.1186/s12879-020-05321-y
49. Chamoun K, Farah M, Araj G, et al. Surveillance of antimicrobial resistance in Lebanese hospitals: retrospective nationwide compiled data. Inter J Infect Dis. 2016;46:64–70. doi:10.1016/j.ijid.2016.03.010
50. Sleiman A, Fayad AGA, Banna H, Matar GM. Prevalence and molecular epidemiology of carbapenem-resistant Gram-negative bacilli and their resistance determinants in the Eastern Mediterranean Region over the last decade. J Global Antimicrob Resist. 2021;25:209–221. doi:10.1016/j.jgar.2021.02.033
51. Frost I, Sati H, Garcia-Vello P, et al. The role of bacterial vaccines in the fight against antimicrobial resistance: an analysis of the preclinical and clinical development pipeline. Lancet Microbe. 2023;4(2):e113–e125. doi:10.1016/S2666-5247(22)00303-2
52. WHO. Antimicrobial stewardship programmes in health-care facilities in low-and middle-income countries: a WHO practical toolkit. Available from: https://www.who.int/publications/i/item/9789241515481.
53. AUB. Infectious diseases services and programs. Available from https://www.aub.edu.lb/fm/InternalMedicine/Pages/Infectious-Diseases-Services-and-Programs.aspx.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.