")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 18
Real-World Experience of Clascoterone Cream 1% in Acne Management: Case Series and Canadian Experience
Received 9 October 2024
Accepted for publication 30 December 2024
Published 20 January 2025 Volume 2025:18 Pages 161—167
DOI https://doi.org/10.2147/CCID.S498879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Elena Tay,1 Wei Jing Loo1– 3
1Western University, London, ON, Canada; 2DermEffects, London, ON, Canada; 3Probity Medical Research, Waterloo, ON, Canada
Correspondence: Wei Jing Loo, DermEffects, 1560 Hyde Park Road, London, ON N6H 5L5, Canada, Tel +1 519 472 2929, Email [email protected]
Abstract: Acne vulgaris is a globally prevalent dermatological condition associated with substantial physical and psychological burden. Although acne typically presents during adolescence, it is a chronic condition that also affects many adults. Despite the spectrum of treatments available for acne, limitations in tolerability and safety concerns can present challenges for the use of conventional medications in clinical practice. Clascoterone cream 1%, a topical androgen receptor inhibitor, was recently approved in Canada for the topical treatment of acne vulgaris. This case series included 10 patients with acne vulgaris who were treated with clascoterone cream 1% as monotherapy or part of a combination treatment program between August 2023 and May 2024. Clascoterone cream 1% was effective and well tolerated regardless of acne severity, age, gender, and ethnicity. Clascoterone led to clinical improvement when used as monotherapy, adjunctive treatment in combination with other topical or systemic agents or laser therapy, and as maintenance therapy to prevent relapse of acne. Moreover, clascoterone also helped to address other concerns in several patients, including hirsutism, hidradenitis suppurativa, retinoid-induced dermatitis, androgenetic alopecia, folliculitis, postinflammatory hyperpigmentation, and laser-induced acne flares. This early real-world clinical experience supports the effectiveness, tolerability, and versatility of clascoterone cream 1% for patients with acne across a variety of clinical and demographic characteristics.
Keywords: androgen, topical, therapy, efficacy, safety, tolerability
Introduction
Acne vulgaris is a common dermatological condition characterized by the formation of comedones, papules, pustules, and nodules primarily affecting sebum-rich areas including the face, chest, and back.1,2 Androgens play a key role in acne pathogenesis by stimulating production of sebum and proinflammatory cytokines as well as the proliferation and differentiation of sebocytes.2–4
Treatment of acne typically involves a multimodal approach tailored to the severity and subtype of acne lesions.1 Topical agents such as retinoids, benzoyl peroxide, and salicylic acid are commonly used to treat mild-to-moderate acne, whereas systemic therapies including oral antibiotics, hormonal agents (eg, spironolactone), and isotretinoin are reserved for moderate-to-severe cases.1 Clinicians may also use chemical peels, microdermabrasion, microneedling, and laser therapy for the treatment of refractory or scarring acne, although there is limited clinical evidence supporting the use of these procedures in acne therapy.1
Although a wide range of medications is available for the treatment of acne vulgaris, many are associated with side effects or have burdensome monitoring requirements that can limit their tolerability and use in a clinical setting.1 Additionally, systemic hormonal agents such as combined oral contraceptives and spironolactone, although available for acne treatment in select female patients, are associated with systemic adverse effects and are not suitable for use in male patients.5 Clascoterone cream 1%, a topical androgen receptor inhibitor, is a first-in-class therapy approved for the treatment of acne vulgaris in male and female patients ≥12 years old; it was first approved in the US in 2020 and is now available in Canada as of June 2023.6,7 In Phase 3 clinical trials, treatment with clascoterone cream 1% in patients with moderate-to-severe acne vulgaris resulted in significantly higher treatment success rates and a greater reduction in lesion counts compared with vehicle, and clascoterone had a safety profile similar to that of vehicle.8 In this case series, we share our real-world Canadian experience of clascoterone cream 1% in the management of acne vulgaris.
Materials and Methods
This study is a case series based on a retrospective chart review conducted in a medical dermatology clinic and was therefore exempt from research ethics board approval. Ten patients with acne vulgaris attending a private clinic in London, ON, Canada between August 2023 and May 2024 were included in this case series (Table 1). The information presented was obtained from a retrospective chart review of the patients’ medical records. For each patient, clinical characteristics (eg, acne subtype, location of acne, and morphology of lesions) were recorded at each follow-up assessment, and acne severity was assessed as clear, almost clear, mild, moderate, or severe. Reduction in severity of acne was determined by comparison with records from previous visits.
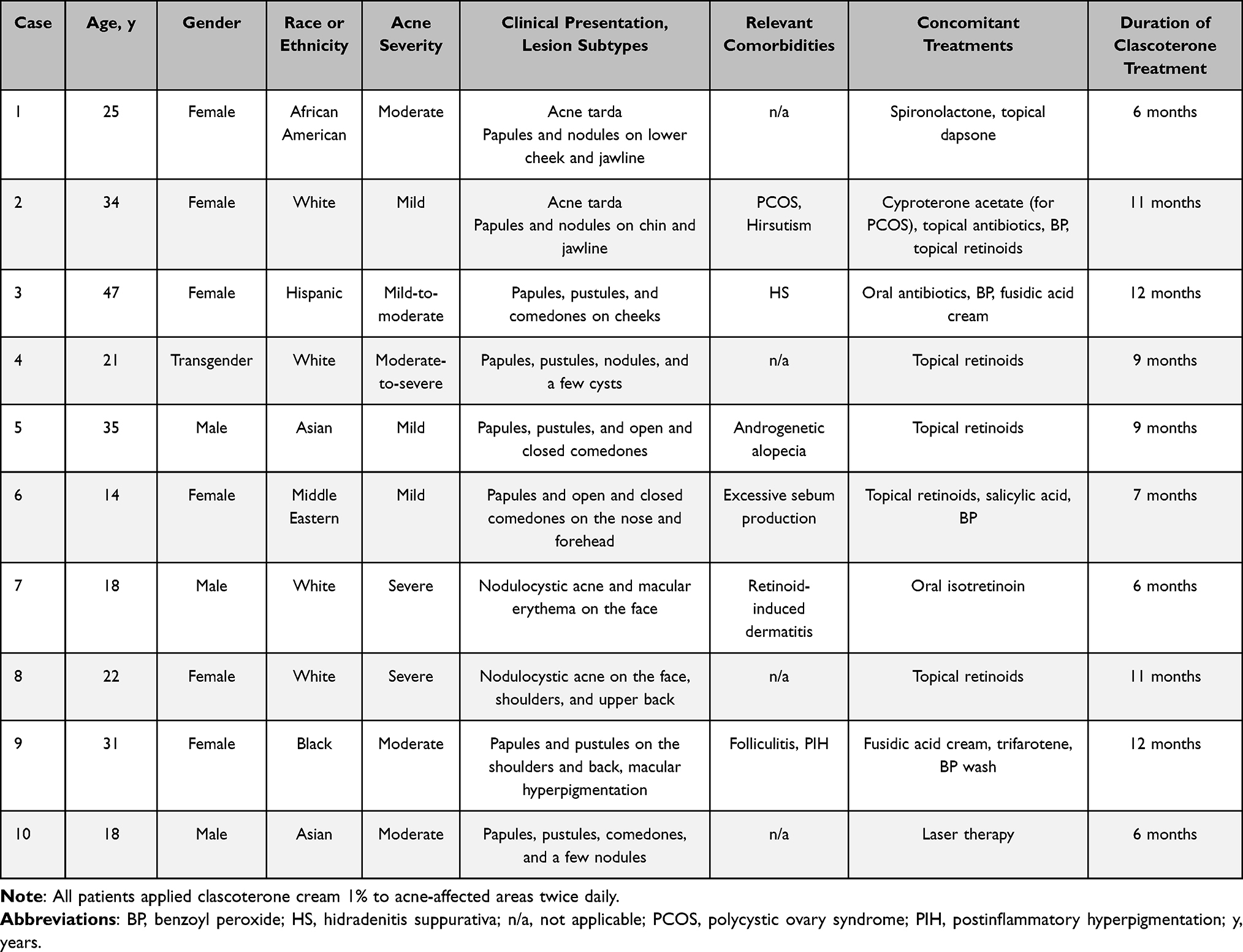 |
Table 1 Demographics and Clinical Characteristics of Patients Included in the Case Series |
Results
Case 1
A 25-year-old African American female with a history of troublesome hormonal acne, exacerbated during menstrual periods, sought treatment due to persistent papules and nodules predominantly located on her lower cheeks and jawline. Due to her inability to tolerate oral contraceptive pills because of migraines, she was initially prescribed adapalene 0.3%/benzoyl peroxide 2.5% by her family physician. Upon consultation with a dermatologist, a treatment plan was devised that included the initiation of spironolactone 50 mg once daily along with topical dapsone 5%. Minimal improvement was observed after 4 months of treatment, and the dosage of spironolactone was consequently increased to 100 mg daily. This led to better control of her acne but was accompanied by bothersome side effects such as dizziness and nocturia, prompting nocturnal awakenings to urinate. The decision was made to introduce clascoterone cream 1% twice daily to address the persistent acne, which allowed for a reduction in the spironolactone dosage to 50 mg to mitigate side effects. Over the course of 6 months, spironolactone was gradually tapered off, as the acne remained well controlled with clascoterone monotherapy. The patient experienced clear skin and expressed satisfaction with the outcome of her treatment regimen.
Case 2
A 34-year-old White female with polycystic ovary syndrome sought dermatological care for persistent acne despite cyproterone acetate treatment. She reported experiencing inflammatory papules and occasional nodules primarily clustered along her chin and jawline. Despite ongoing treatment with clindamycin 1%/benzoyl peroxide gel 5% and tretinoin gel microsphere 0.1% for over 7 months, her acne tarda remained poorly controlled. Clascoterone cream 1% twice daily was introduced in addition to the existing topical regimen. At follow-up 11 months later, control of her acne had improved notably following the addition of clascoterone. The patient also reported a reduction in symptoms of facial hirsutism, noting a decrease in the appearance of coarse, dark hairs that had been particularly evident on her chin. This multimodal approach led to excellent control of her acne and additionally addressed her facial hirsutism.
Case 3
A 47-year-old Hispanic female with a complex medical history—including a diagnosis of breast cancer 1 year prior for which she underwent a lumpectomy and initiated tamoxifen therapy—presented with concurrent acne and hidradenitis suppurativa (HS). Her acne presentation encompassed a combination of inflammatory and comedonal lesions distributed across her face; her HS was characterized by mild involvement, graded as Hurley Stage I, with 1 inflammatory nodule noted in the left axilla and 2 in the right groin. The patient’s condition was previously managed for 3 months with a combination of oral doxycycline 100 mg daily, benzoyl peroxide 5% acne wash, and fusidic acid 2% cream, which yielded only partial improvement. Given her medical history, adalimumab was deemed unsuitable due to concern regarding immunosuppression in the context of malignancy.
Because of the inadequate response to prior therapies and the contraindication to adalimumab, clascoterone cream 1% was incorporated into her treatment regimen. The patient was advised to apply clascoterone twice daily to both her facial acne and HS lesions. There was a remarkable resolution of both her acne and HS lesions following the addition of clascoterone, leading to marked improvement in her overall skin condition when she was seen for follow-up 1 year later. This tailored approach addressed the patient’s dermatological concerns while taking into consideration her underlying medical conditions and treatment limitations, resulting in successful management of both acne and HS.
Case 4
A 21-year-old White transgender individual who recently underwent female-to-male gender reassignment surgery and was receiving testosterone therapy presented with acne breakouts. Their family physician initiated treatment with minocycline, clindamycin 1%/benzoyl peroxide gel 5%, and a salicylic acid cleanser. However, they remained distressed by the persistent acne, prompting a referral to a dermatologist. During the consultation, they expressed concerns regarding the potential side effects of oral isotretinoin and declined this option. In response, a tailored treatment plan was devised, incorporating clascoterone cream 1% twice daily and tazarotene lotion 0.045% every other night. These medications were chosen to provide effective management while addressing the patient’s apprehension regarding systemic therapies. They experienced marked improvement in their acne following the initiation of clascoterone and tazarotene, with approximately 80% clearance noted at 9 months, and expressed satisfaction with the results.
Case 5
A 35-year-old Asian male with mild facial acne characterized by a combination of inflammatory and comedonal lesions was prescribed trifarotene cream 0.005%, which resulted in skin dryness and irritation. In response to these adverse effects, the frequency of trifarotene application was reduced to 3 times per week, and clascoterone cream 1% twice daily was added to the regimen. He achieved effective control of his acne, along with resolution of dryness and irritation, following this adjustment in treatment. During a follow-up appointment 9 months later, the patient noted that he was using clascoterone off-label on his scalp for androgenetic alopecia without medical direction. He reported stabilization of hair loss and some evidence of hair regrowth.
Case 6
A 14-year-old Middle Eastern female presented with acne vulgaris primarily concentrated on her nose and forehead, accompanied by complaints of oily skin due to excessive sebum production. Her skincare regimen included a 5% salicylic acid cleanser, along with adapalene 0.3%/benzoyl peroxide 2.5%. Despite these efforts, her acne persisted, and she continued to struggle with oily skin. In response to her concerns, clascoterone cream 1% twice daily was incorporated into her treatment regimen. The patient experienced a notable improvement in her acne 7 months later as well as decreased sebum production following the addition of clascoterone, leading to an overall improvement in her skin condition.
Case 7
An 18-year-old White male presented with severe nodulocystic acne that was unresponsive to systemic antibiotics and topical treatments. Due to the severity of his condition, he was initiated on treatment with isotretinoin 40 mg daily. However, he experienced prominent postinflammatory erythema, irritation, and dryness, particularly on his cheeks. To address these concerns and improve treatment tolerability, clascoterone cream 1% twice daily was introduced into his treatment regimen. The addition of clascoterone proved beneficial, as it helped alleviate the patient’s postinflammatory erythema, irritation, and dryness associated with isotretinoin therapy. Moreover, clascoterone served as an effective adjunctive treatment that enhanced the overall tolerability of isotretinoin. He completed a 6-month course of isotretinoin and maintained clear skin with topical clascoterone cream 1% twice daily.
Case 8
A 22-year-old White female presented with a history of acne conglobata and prior treatment failure with oral contraceptive pills, multiple courses of antibiotics, and various topical prescription creams. Following 6 months of treatment with isotretinoin 50 mg daily, she experienced substantial clearance of her acne lesions. However, due to concerns about potential relapse, she was hesitant to discontinue isotretinoin, especially considering her twin sister’s experience of relapsing twice after stopping isotretinoin therapy. To address the patient’s concerns, she was prescribed clascoterone cream 1% and tazarotene lotion 0.045% following discontinuation of isotretinoin. Eleven months post discontinuation, the patient’s acne remained well controlled, supporting the efficacy of clascoterone and tazarotene for preventing relapse of acne.
Case 9
A 31-year-old Black female presented with a combination of acne and folliculitis predominantly affecting her shoulders and back. She reported inadequate control of papules and pustules on her shoulders and back despite treatment with fusidic acid cream, trifarotene, and benzoyl peroxide wash. Clascoterone cream 1% was added to the patient’s existing topical regimen, resulting in a marked improvement in her acne and folliculitis as well as notable reduction in secondary postinflammatory hyperpigmentation on her back. The patient reported satisfactory control of symptoms without significant adverse effects on follow-up 1 year later.
Case 10
An 18-year-old Asian male presented with moderate acne vulgaris predominantly affecting his face. He reported poor control of acne with topical anti-acne treatments and doxycycline. Additionally, he was intolerant to isotretinoin due to side effects including dry chapped lips, extreme lethargy, and muscle aches. The patient underwent AviClear® laser therapy for acne, but experienced a severe acne flare consistent with “purging” after the first treatment session. Clascoterone cream 1% was added to his therapeutic regimen, mitigating the initial flares, and subsequent sessions were better tolerated. After completing 3 sessions of laser therapy with adjunctive clascoterone, he achieved clear skin. Clascoterone treatment for a total of 6 months played a crucial role in minimizing acne flares associated with laser therapy, contributing to the overall success of the treatment.
Discussion
This case series provides real-world evidence for the effectiveness, safety, and tolerability of clascoterone cream 1% for the management of acne vulgaris. Clascoterone was effective and well tolerated across all patients regardless of acne severity, age, gender, or ethnicity. In a few patients, the addition of clascoterone to the patient’s current treatment regimen, including topical agents, oral isotretinoin, and laser treatments, also helped to mitigate the side effects caused by other medications or laser devices, improving both the patient experience and treatment outcome. Thus, the addition of clascoterone to the acne treatment armamentarium either as a monotherapy or as an adjunctive treatment provides clinicians with increased flexibility to safely address the hormonal component of acne in male and female patients and regardless of the patient’s clinical or demographic characteristics.
Acne is a common adverse effect observed in transgender individuals receiving masculinizing hormone therapy.9 Treatment options for managing acne in transmasculine patients include topical agents (eg, benzoyl peroxide/topical antibiotics or retinoids), oral antibiotics, or isotretinoin in more severe cases.10 Systemic hormonal agents are typically not suitable for transmasculine patients receiving testosterone due to concerns regarding potential feminizing effects.10 Although the clinical trials of clascoterone did not specifically include transgender patients, the use of topical antiandrogens such as clascoterone has been proposed as a safe option for acne treatment in transmasculine patients due to the absence of systemic antiandrogen activity or systemic adverse effects.8,10,11 In the current case series, treatment with clascoterone cream 1% in a transgender patient led to marked improvement in their acne, underscoring the importance of a patient-centered approach in addressing dermatological concerns, particularly in the context of gender transition and related medical treatments.
The American Academy of Dermatology guidelines recommend a multimodal approach to therapy incorporating agents with multiple mechanisms of action to address the multifactorial pathogenesis of acne.1 In clinical studies, clascoterone cream 1% was evaluated as a monotherapy8; no clinical data are published on the efficacy and safety of concomitant usage of clascoterone cream 1% with other topical therapies, systemic medications, or laser devices for the treatment of acne. The findings from this case series demonstrate that clascoterone may also work well as an adjunct to other topical and systemic therapies as well as laser treatments, or as a maintenance therapy to prevent relapse of acne. The efficacy of clascoterone in preventing acne relapse following isotretinoin therapy underscores the importance of individualized maintenance therapy strategies for patients who have completed isotretinoin treatment, particularly those with a history of severe acne or concerns about relapse.
There is growing interest in the potential applications of clascoterone in other dermatological conditions.12–16 In previous reports, clascoterone cream 1% led to substantial reduction in the number and severity of lesions in patients with HS.12,14 Clascoterone may also benefit patients with androgenetic alopecia via competitive inhibition of dihydrotestosterone, a known pathogenic trigger in androgenetic alopecia, based on evidence from Phase 1 and Phase 2 studies.15,16 Phase 3 studies evaluating the efficacy and safety of clascoterone solution in patients with androgenetic alopecia are recruiting participants (www.clinicaltrials.gov NCT05910450/NCT05914805). In the current case series, adding clascoterone cream 1% to patients’ treatment regimens also helped to address other patient concerns in Cases 2, 3, 5, 6, and 9, highlighting its potential versatility in addressing multiple dermatologic concerns including hirsutism, HS, retinoid-induced dermatitis, androgenetic alopecia, folliculitis, and postinflammatory hyperpigmentation when used in combination with other topical agents. Thus, clascoterone warrants further consideration as a treatment option in other dermatological conditions.
Conclusions
Clascoterone cream 1% is a well tolerated and effective topical acne treatment regardless of acne severity and patient gender, race, or ethnic background. In clinical practice, clascoterone is highly versatile and can be used not only as monotherapy but also as an adjunctive therapy with other topical therapies, systemic agents, and laser devices, as well as maintenance therapy to prevent relapse of acne vulgaris.
Consent for Publication
All patients and/or a legal guardian, as applicable, provided consent for the publication of the cases.
Acknowledgments
Editorial assistance in the preparation of this manuscript was provided by Dana Lengel, PhD, of AlphaBioCom, a Red Nucleus company, and funded by Sun Pharma.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study. Medical writing and editorial support were funded by Sun Pharma.
Disclosure
WJL has served as an investigator, speaker, adviser/consultant, and/or received grants/honoraria from AbbVie, Allakos, Alumis, Amgen, AnaptysBio, Arcutis Biotherapeutics, Aslan, Bausch Health, BioJamp, Bristol Myers Squibb, Celgene Corporation, Celltrion, Concert Pharmaceuticals, Eli Lilly, Galderma, GSK, Incyte, Inmagene, Janssen, LEO Pharma, Medexus, Meiji Seika Pharma, Novartis, Numab, Pediapharm, Pfizer, Reistone, Sanofi, SkinCeuticals, Sun Pharma, Takeda, UCB, and Valeant. The authors report no other conflicts of interest in this work.
References
1. Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90(5):1006.e1001–1006.e1030. doi:10.1016/j.jaad.2023.12.017
2. Del Rosso JQ, Kircik LH, Stein Gold L, Thiboutot D. Androgens, androgen receptors, and the skin: from the laboratory to the clinic with emphasis on clinical and therapeutic implications. J Drugs Dermatol. 2020;19(3):30–35.
3. Baldwin H, Farberg A, Frey C, et al. Unmet needs in the management of acne vulgaris: a consensus statement. J Drugs Dermatol. 2023;22(6):582–587. doi:10.36849/JDD.7587
4. Cong TX, Hao D, Wen X, et al. From pathogenesis of acne vulgaris to anti-acne agents. Arch Dermatol Res. 2019;311(5):337–349. doi:10.1007/s00403-019-01908-x
5. Elsaie ML. Hormonal treatment of acne vulgaris: an update. Clin Cosmet Invest Dermatol. 2016;9:241–248. doi:10.2147/CCID.S114830
6. WINLEVI® (clascoterone cream 1%). Product Monograph. Brampton, Ontario: Sun Pharma Canada Inc; 2023.
7. WINLEVI® (clascoterone cream 1%). Full Prescribing Information. Cranbury, NJ: Sun Pharmaceutical Industries, Inc; 2023.
8. Hebert A, Thiboutot D, Stein Gold L, et al. Efficacy and safety of topical clascoterone cream, 1%, for treatment in patients with facial acne: two phase 3 randomized clinical trials. JAMA Dermatol. 2020;156(6):621–630. doi:10.1001/jamadermatol.2020.0465
9. Chu L, Gold S, Harris C, et al. Incidence and factors associated with acne in transgender adolescents on testosterone: a retrospective cohort study. Endocr Pract. 2023;29(5):353–355. doi:10.1016/j.eprac.2023.02.002
10. Radi R, Gold S, Acosta JP, et al. Treating acne in transgender persons receiving testosterone: a practical guide. Am J Clin Dermatol. 2022;23(2):219–229. doi:10.1007/s40257-021-00665-w
11. Mazzetti A, Moro L, Gerloni M, Cartwright M. Pharmacokinetic profile, safety, and tolerability of clascoterone (cortexolone 17-alpha propionate, CB-03-01) topical cream, 1% in subjects with acne vulgaris: an open-label phase 2a study. J Drugs Dermatol. 2019;18(6):563.
12. Cunningham KN, Moody K, Alorainy M, Rosmarin D. Use of topical clascoterone for the treatment of hidradenitis suppurativa. JAAD Case Rep. 2023;36:38–39. doi:10.1016/j.jdcr.2023.04.002
13. Der Sarkissian SA, Sun HY, Sebaratnam DF. Cortexolone 17alpha-propionate for hidradenitis suppurativa. Dermatol Ther. 2020;33(6):e14142. doi:10.1111/dth.14142
14. Hargis A, Yaghi M, Maskan Bermudez N, Lev-Tov H. Clascoterone in the treatment of mild hidradenitis suppurativa. J Am Acad Dermatol. 2024;90(1):142–144. doi:10.1016/j.jaad.2023.08.064
15. Sun HY, Sebaratnam DF. Clascoterone as a novel treatment for androgenetic alopecia. Clin Exp Dermatol. 2020;45(7):913–914. doi:10.1111/ced.14292
16. Cartwright M, Mazzetti A, Moro L, et al. A summary of in vitro, Phase I, and Phase II studies evaluating the mechanism of action, safety, and efficacy of clascoterone (cortexolone 17a propionate, CB-03-01) in androgenetic alopecia. J Am Acad Dermatol. 2019;81(4):AB13. doi:10.1016/j.jaad.2019.06.087
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Open-Label Extension Study Comparing Latanoprost 0.005% Without vs With Benzalkonium Chloride in Open-Angle Glaucoma or Ocular Hypertension
Shen Lee B, Malhotra R, Sall K, Mitchell B, Peace J
Clinical Ophthalmology 2022, 16:2285-2293
Published Date: 19 July 2022
The Efficacy and Safety of Anlotinib in Extensive-Stage Small Cell Lung Cancer: A Multicenter Real-World Study
Zheng HR, Jiang AM, Gao H, Liu N, Zheng XQ, Fu X, Zhang R, Ruan ZP, Tian T, Liang X, Yao Y
Cancer Management and Research 2022, 14:2273-2287
Published Date: 2 August 2022
Relative Safety and Efficacy of Two Doses of Tandospirone Citrate for Generalized Anxiety Disorder: A Multicenter Randomized Controlled Trial
Li Q, Zhang H, Lin G, Shi S, Zhang Y, Ji J, Yang L, Yao J, Wu W
Neuropsychiatric Disease and Treatment 2022, 18:1653-1664
Published Date: 8 August 2022
Biosimilars: Science, Implications, and Potential Outlooks in the Middle East and Africa
Batran RA, Elmoshneb M, Hussein AS, Hussien OM, Adel F, Elgarhy R, Morsi MI
Biologics: Targets and Therapy 2022, 16:161-171
Published Date: 6 October 2022
Clinical Evaluation of Risankizumab in the Treatment of Adults with Moderately to Severely Active Crohn’s Disease: Patient Selection and Reported Outcomes
Horst S, Cross RK
Drug Design, Development and Therapy 2023, 17:273-282
Published Date: 31 January 2023