")
Back to Journals » International Journal of Nanomedicine » Volume 20
Recent Research Progress of Wound Healing Biomaterials Containing Platelet-Rich Plasma
Authors Huang S, Li Q, Li X, Ye H, Zhang L , Zhu X
Received 15 November 2024
Accepted for publication 28 February 2025
Published 31 March 2025 Volume 2025:20 Pages 3961—3976
DOI https://doi.org/10.2147/IJN.S506677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Eng San Thian
Sha Huang,1 Qing Li,2 Xiangyu Li,1 Hailing Ye,1 Luyang Zhang,1 Xiaoyi Zhu3,4
1Department of Plastic Surgery, Shulan (Hangzhou) Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Electrocardiogram, The Second Affiliated Hospital, Zhejiang University School of College, Hangzhou, Zhejiang, People’s Republic of China; 3Department of General Surgery, Shulan (Hangzhou) Hospital, Hangzhou, Zhejiang, People’s Republic of China; 4Department of General Surgery, The Affiliated Hospital of Hangzhou Normal University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Xiaoyi Zhu, Email [email protected]
Abstract: Platelet-Rich Plasma (PRP) is a plasma product obtained by centrifuging autologous blood, containing a high concentration of platelets, white blood cells, and fibrin. PRP is enriched with various growth factors, such as Transforming Growth Factor-beta (TGF-β), Platelet-Derived Growth Factor (PDGF), Epidermal Growth Factor (EGF), Insulin-Like Growth Factor (IGF), and Vascular Endothelial Growth Factor (VEGF), all of which promote tissue growth and repair. Currently, PRP has been widely applied in the clinical field of wound repair and has achieved certain therapeutic effects. Biomaterials, as an important direction in the treatment of wounds, combined with PRP, provide new possibilities to enhance the regenerative repair of wounds by PRP. This article reviews the latest research progress of biomaterials combined with PRP in the treatment of wounds, aiming to provide references for PRP wound treatment, as well as to provide ideas for the development of subsequent medical materials.
Keywords: platelet-rich plasma, prp, wound healing, biomaterials, hydrogel, wound dressing
Graphical Abstract:

Introduction
Trauma is a common issue that is difficult to avoid in production and daily life. Ordinary traumatic wounds can heal through human self-healing capabilities.1 However, when the severity of a traumatic wound exceeds the body’s own healing ability or when the body’s healing ability declines, such as in severe burns,2 pressure sores in malnourished patients,3 and diabetic wounds4 often become difficult to heal and continue to have a serious impact on the patient’s physiology and psychology. The loss of the skin barrier function not only damages the patient’s social functioning but also threatens life if complications such as infection occur. In recent years, the disease spectrum of wound treatment has been constantly changing. With industrial production and the use of electricity and fire becoming more standardized and safer, the number of patients with electric shock injuries and burns has gradually decreased.5,6 However, the incidence of chronic diseases has increased, the number of diabetes patients continues to grow, and there is a trend towards younger patients. The number of patients troubled by diabetic wounds is also increasing, imposing a serious economic burden on society.7 Traditional wound treatment includes methods such as debridement, suturing, and skin grafting, but the treatment time is long, and the treatment effect is not satisfactory. Therefore, for wounds that are difficult to heal, how to cure and shorten the patient’s healing time and reduce the patient’s expenses are urgent issues that need to be resolved in current research.
At present, constructing biomaterials that promote wound healing through tissue engineering is an important and main research field in wound treatment.8–10 Current experimental studies have shown that combining bio-tissue materials with stem cells,11 growth factors,12 and exosomes,13 and other biological preparations can achieve better wound healing effects. Stem cells have limited sources, are difficult to obtain, and have ethical issues. For wound diseases, clinical application is still a long way off and has great limitations. Although there are exosome products on the market, they are difficult to obtain and expensive. If used clinically, they cannot meet the needs of many patients. Growth factors are currently the most widely used and safe wound healing drugs in clinical practice, with reasonable prices and convenient use. However, the types of growth factor products on the market are single, and the clinical use effect is still not satisfactory. Platelet-rich plasma (PRP) can be obtained through autologous blood, the acquisition channel is simple, and there are no ethical issues with other allogeneic biological preparations.14 The clinical preparation method is also simple, which can be prepared through common centrifugal equipment such as hospital centrifuges and has strong clinical feasibility. It is rich in a variety of the body’s own growth factors and has been proven in clinical and scientific research to have great potential in the field of tissue regeneration and repair.
PRP is a plasma product obtained by centrifuging autologous blood, and its platelet concentration is usually 3–7 times higher than that of whole blood.15 A number of studies have reported that PRP has a promoting effect on the repair of bones, skin, and nerves.16–19 Many studies have shown that PRP has great potential in the treatment of diabetic wounds.20,21 In recent years, the application of PRP in wound treatment has achieved preliminary research results. Research on the molecular mechanism of PRP in wound treatment has also made some progress.22 However, at present, from the application of PRP in clinical practice, researchers’ understanding of the mechanism of PRP in wound treatment lacks sufficient depth, which limits the further development of PRP treatment methods. At present, for the treatment of diabetic wounds, hydrogels, artificial dermis, and cell scaffolds are important research directions, which can promote the healing of diabetic wounds.23–25 They can achieve anti-infection, anti-oxidation, anti-inflammatory, and promote tissue regeneration, and other effects on diabetic wounds by directly combining with various materials and drugs.26,27 Research combining PRP and these biomaterials has also made certain progress. Therefore, this review summarizes the current research on the mechanism of PRP in wound treatment and the application of biomaterials, sorting out the connections, which is of great importance for guiding the further reasonable development of biomaterials combined with PRP in the treatment of diabetic wounds.
The Functions of PRP on Wound Healing
The capacity of Platelet-Rich Plasma (PRP) to enhance wound healing is largely attributed to platelets, anucleate blood components that are about 3 μm in diameter and play a pivotal role in hemostasis and thrombus formation at wounds.28 During the wound repair process, platelets become activated and change shape, altering the conformation of the glycoprotein IIb/IIIa complex on the platelet cell membrane and translocating functional proteins such as P-selectin. These substances rapidly bind to the extracellular surface of cells in grafts, flaps, or wounds through transmembrane receptors present on mesenchymal stem cells, osteoblasts, fibroblasts, endothelial cells, and epidermal cells.29 They mediate a variety of cellular functions, including cell migration, differentiation, cell cycle, apoptosis, metabolism, and proliferation.30,31 The molecules released include growth factors (GFs) and cytokines, predominantly located in the α-granules of platelets.32 Key factors in these granules include Transforming Growth Factor (TGF-β1), Platelet-Derived Growth Factor (PDGF), Fibroblast Growth Factor (FGF), Epidermal Growth Factor (EGF), and Vascular Endothelial Growth Factor (VEGF), these factors play very important roles in the healing of wounds and can effectively promote wound healing. Besides these platelet-activated compounds, PRP in plasma also contains significant bioactive factors, such as Hepatocyte Growth Factor (HGF) or Insulin-Like Growth Factor (IGF-1), which originate more from the liver than from platelets,33,34 and are involved in the regulation of cell chemotaxis, cell differentiation, and mitosis.35 These abundant growth factors stimulate mesenchymal and epithelial cells to promote the synthesis of collagen and matrix, facilitating the formation of fibrous connective tissue and scar tissue. In addition to growth factors, structures like micro-vesicles and exosomes are also present in the plasma and play a crucial role in cell communication and signal transduction processes.36
Progress in the Extraction and Application of PRP
Reports on the extraction of PRP emerged in the late 1990s, and over the following decade, numerous different preparation methods were reported, all of which involved centrifugation and platelet activation.14 There is no unified and complete standard for the preparation and use of PRP, and after nearly two decades of development, PRP remains very popular in clinical settings. Traditional PRP preparation methods have certain limitations in terms of collection volume, platelet concentration, and consistency. Nowadays, many innovative preparation methods are continuously emerging and are being improved based on PRP.
PRP can be frozen for storage to achieve a longer shelf life, more efficient inventory management, and more suitable transportation conditions to overcome the limitations in clinical application storage management, which has practical application advantages.37 However, biologically active components in PRP such as platelets, growth factors, and micro-vesicles will inevitably suffer a loss of biological activity during freezing storage and the subsequent thawing process when used. The research results of Su et al (2024) indicate that frozen PRP has stable biological activity and shows significant regulatory capabilities in key wound healing processes, such as macrophage polarization, fibroblast proliferation, and endothelial cell function.38
Rotary Evaporation Plasma Concentration Method
Jon Mercader Ruiz et al (2024), based on previous research and component analysis of PRP, inferred that in addition to platelets and their derived growth factors, other components in the plasma are important and should not be ignored in the therapeutic effects of PRP.39 Therefore, they improved the extraction method of PRP by using a rotary evaporator with a water evaporation method. After obtaining standard PRP (sPRP) through traditional centrifugation, a rotary evaporator is used to remove half the volume of water in the plasma to obtain concentrated PRP (nPRP). The study found no significant difference in protein concentration between blood and sPRP (p<0.0001), but the protein concentration in nPRP almost doubled. Obviously, the method of water evaporation can inevitably increase the concentration of platelets and growth factors. However, the concentration of various ions will also increase accordingly, and the environment of ions that is most suitable for the human body is disrupted. The most direct result is that the pH of nPRP increased to 8.4, and its coagulation time was extended. Therefore, it is necessary to adjust the pH by adding HCl and CaCl2.40 PRP obtained by this method has also been verified in cellular experiments for its stronger ability to promote proliferation.
Lyophilized Platelet-Rich Plasma
Using lyophilization to preserve PRP can achieve a longer storage time. However, PRP must still have sufficient biological activity when used after lyophilization. Nakajima et al (2024) reported a lyophilization method for PRP, and PRP lyophilized by this method still has good anti-inflammatory effects after one year of storage, and the level of biological activity is not affected.41 Lyophilization for preserving PRP greatly extends its storage time, and it does not require stringent storage conditions, facilitating the clinical use and preservation of PRP.
Autologous Platelet and Leukocyte-Rich Fibrin Material
Autologous platelet and leukocyte-rich fibrin material (L-PRF) are also a plasma enrichment product. It only requires a single centrifugation cycle for the blood sample without the need for anticoagulants and activators, making the preparation faster and cheaper, and eliminating potential risks associated with the use of bovine thrombin or other activators.42 Compared with PRP, L-PRF has a higher concentration of leukocytes, which helps immune and antibacterial responses.43 The extracted L-PRF clot is composed of a dense fibrin matrix forming a complex three-dimensional scaffold containing platelets, leukocytes, growth factors, and fibronectin.44 It is reported that one of the advantages of L-PRF over PRP is that its high-density fibrin network is conducive to the slow and gradual release of growth factors.
Autologous Platelet Plasma-Derived Fibrin Scaffold
The autologous platelet plasma-derived protein fibrin scaffold (ABDPS) has been used in wound treatment for many years and is also prepared from autologous blood.45 ABDPS can be locally injected in a liquid state or serve as a matrix for scaffolds. Current research indicates that the main therapeutic components are platelet and plasma-derived growth factors, microvesicles and exosome-like substances, and fibrin.46
The components and mechanisms of action of ABDPS and PRP are similar, but ABDPS is produced from blood through a more complex production process than PRP into an injectable gel or wound dressing application form. For open wounds, wound dressings are the main application form. However, the structure of the wound dressing made from ABDPS is loose, with insufficient strength and support, easy deformation, and poor adhesion and absorption capacity for wounds. Chronic non-healing wounds have variable shapes and depths, and ABDPS as a wound dressing cannot meet the mechanical property requirements of wound healing materials.47 Therefore, the current research direction is to improve the mechanical properties of pure PRP dressings by incorporating PRP into bio-tissue engineering materials while retaining the healing-promoting ability of PRP.48
Clinical Research on Autologous PRP for Wound Healing
Since ancient times, wound healing has been a challenge for humanity. With the changing disease spectrum, chronic non-healing wounds have gradually become a clinical treatment dilemma. Taking diabetic foot as an example, studies have reported that the median healing time for diabetic foot ulcers without surgery is 12 weeks,49 20% of patients cannot heal within a year, and the probability of recurrence within the same year is 40%.50 Existing treatment measures cannot effectively solve the problem of wound healing. Therefore, in the clinic, researchers have been continuously exploring new methods for wound treatment.
In recent clinical studies, there have been many positive reports on the use of PRP for wound treatment. As early as 2019, Tasmania et al concluded that the use of PRP in diabetic foot ulcers can promote wound healing, reduce the volume of ulcers, shorten the time for complete wound healing, reduce the incidence of adverse events, and there is no difference in the probability of wound complications.51 In Grant et al’ 2021 clinical study, it was found that mixing PRP with fat for the treatment of diabetic foot wounds can increase the survival rate of fat grafts and promote early wound vascularization.52
However, at the same time, Ajay et al clinical study involving 60 patients showed that the application of PRP had no significant effect on promoting ulcer healing.53 Napit et al (2024) conducted a clinical controlled study on 130 patients with neuropathic leprosy ulcers, and the results were not sufficient to prove their routine use in the treatment of neuropathic ulcers of leprosy.54 From the current numerous clinical studies and meta-analyses of these clinical studies, PRP treatment for wounds is effective.55 The results obtained by Ajay et al may be related to the extraction method and treatment method of PRP. This indicates that PRP for wound treatment currently lacks a systematic, stable, and promotable treatment plan. Therefore, summarizing the latest research progress of PRP in wound treatment helps to establish an effective plan for the application of PRP.
Although scar formation is the ultimate way of wound healing, excessive scar formation affects aesthetics, and pathological scar formation can also affect patient health. Studies have shown that PRP also has an improvement effect on wound scar formation.56 Zawadzki et al (2024) conducted a clinical study on patients who underwent breast segmentectomy and found that using PRP for postoperative injection at the incision can improve postoperative scars.57 This method only requires one blood drawing and causes minimal harm to the patient. PRP wound injection is clinically feasible for patients who have aesthetic appearance requirements after surgery and for those who have undergone suture after facial trauma. However, injecting through a needle over the wound range also needs to consider whether it will aggravate the damage, so it would be a better research direction if PRP can be used to design non-invasive scar repair materials.
Combination of PRP With Bio-Tissue Engineering Materials for Wound Healing
Bio-tissue engineering materials play an important role in wound treatment, such as artificial dermis,58 acellular allogeneic dermis,59 acellular xenogeneic dermis,60 and various wound dressings.61–64 However, current bio-tissue engineering materials still cannot meet clinical needs. Moreover, materials like acellular allogeneic dermis, although they have good clinical effects, are expensive, and many patients cannot afford the cost of treatment, and the material sources are scarce.65 One characteristic of current bio-tissue engineering materials is the lack of growth-promoting factors. In the clinic, exogenous growth factor drugs are mainly applied to wounds, but there are many shortcomings to this direct application, such as short action time and uneven action.66 The types and effects of growth factors used in the clinic are single, while wound healing is the result of the common growth and regeneration of various cells.67 Many studies have combined growth factors with wound dressing bio-tissue engineering materials and found that it can achieve the effect of drug sustained release, which can better promote wound healing.68,69 However, if this method is applied to actual clinical practice, the evaluation of materials must be according to drug standards to ensure that the production process, storage, and effective performance meet clinical needs. At present, there are no similar products in the clinic. PRP is extracted from autologous sources, has high safety, can be obtained on demand, and all medical institutions have conditions for preparation, which meets the conditions for clinical use. Moreover, PRP has a rich content of growth factors, and if an appropriate method can be found to combine with bio-tissue engineering materials, it will inevitably play a better role. In recent years, studies on the combination of PRP and bio-tissue engineering materials for wound treatment have been continuously reported as shown in Table 1, but it will take many years for their materials to truly enter clinical applications. However, their latest design ideas, principles, and mechanisms are of great reference significance for clinical applications.
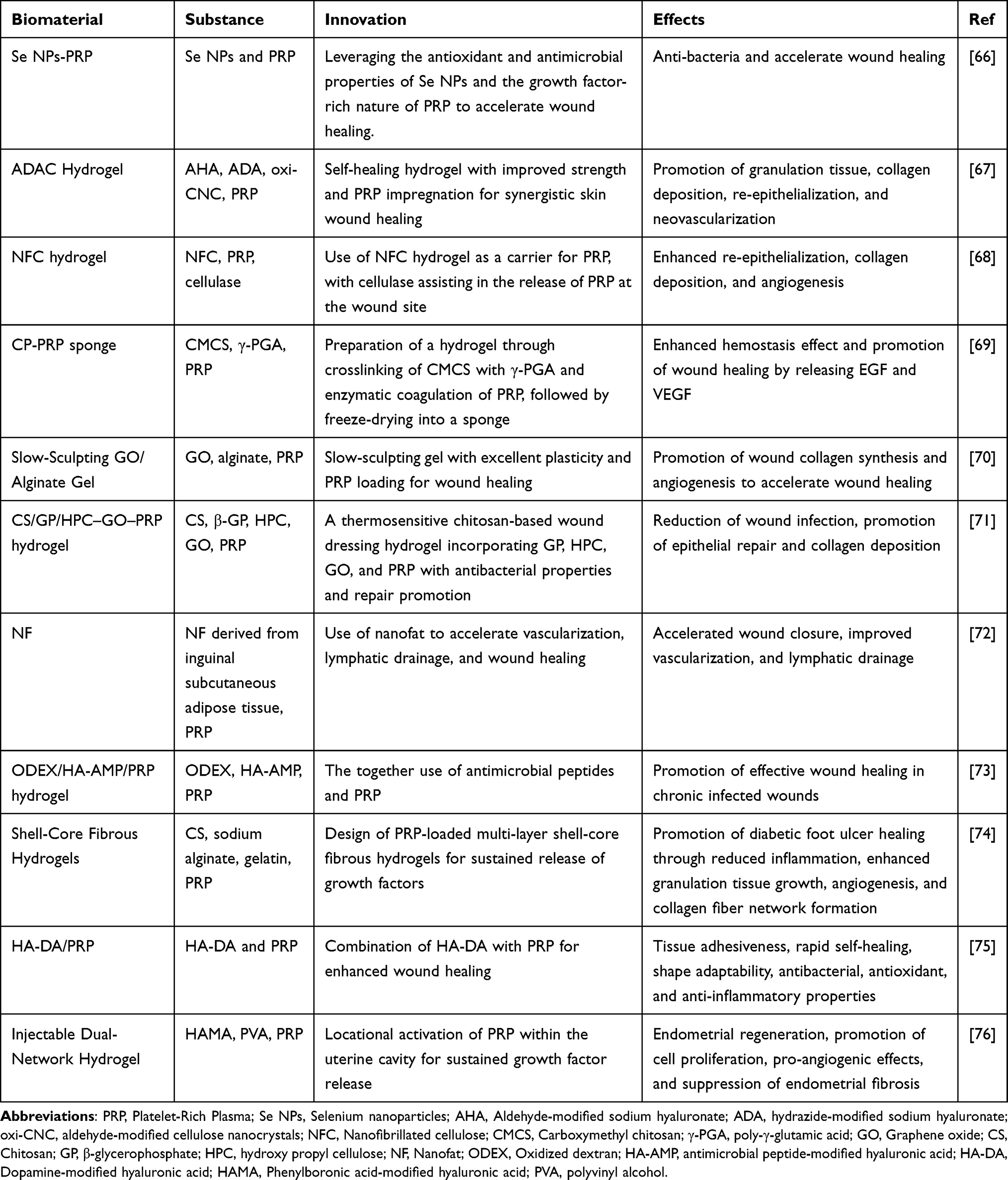 |
Table 1 The Bio-Tissue Engineering Materials Combined With PRP |
Combination of Platelet-Rich Plasma With Selenium Nanoparticles
Selenium nanoparticles (Se NPs) have been proven to be a multifunctional drug with higher bioavailability and lower toxicity.77 Selenium (Se) is an essential trace element in almost all physiological processes of the human body, but it is necessary to control the Se concentration to achieve an effective concentration without exceeding unsafe concentrations.70 Se NPs have all the physiological functions of Se, with low toxicity and high bioactivity. These characteristics make them an ideal choice to solve the safety problem of Se concentration.14 Studies have found that Se NPs have certain antibacterial abilities, and antibacterial research has not found bacterial drug resistance, making Se NPs an ideal candidate for the treatment of infectious and chronic wounds.78 Karas et al combined Se NPs with PRP, hoping that the advantages of both in treating diabetic wounds can be combined while solving the instability of PRP.71 In this study, Se NPs were synthesized by reducing sodium selenite with ascorbic acid in the presence of polyvinylpyrrolidone (PVP) and cetyltrimethylammonium chloride (CTAC), resulting in the formation of orange-colored elemental selenium nanoparticles. The study found that Se NPs have nano-sized particle diameter and a large surface area, have good free radical scavenging ability, can regulate the wound microenvironment, and play a good anti-inflammatory effect. While promoting cell proliferation with PRP, it also regulates inflammatory factors such as interleukin-17A and interleukin-1β. The two regulate wound inflammation in different ways and can play a better role.
Combination of Diverse Hydrogels and Platelet-Rich Plasma
Hydrogel dressings are currently the main research direction for wound treatment and have great application prospects. The effect of combining PRP with hydrogels is naturally an indispensable study. After hydrogels and PRP are mixed to make new wound dressings, the stable release ability of PRP and maintaining the bioactivity of various factors in PRP are important indicators for evaluating the effect of PRP in the material. To improve the effectiveness and stability of PRP, appropriate hydrogel materials should be used to allow bioactive substances to be released through diffusion or material degradation. Plain hydrogels may lack necessary adhesion, injectability, antioxidant properties, and antibacterial properties, and cannot fully meet the treatment requirements of complex diabetic wounds. Li et al (2022) showed that PRP-based hydrogels significantly promote skin wound healing by promoting granulation tissue formation, promoting collagen deposition, and accelerating re-epithelialization and neovascularization (Figure 1).79 Koivunotko et al (2024) combined PRP with nanocellulose hydrogels, the hydrogel slowly degrades and releases PRP during the treatment process, and the two work together to promote wound healing.80 These studies show that PRP has a strong combination ability and application prospects with various hydrogels.
 |
Figure 1 Schematic illustrations of self-healing hyaluronic acid nanocomposite hydrogels with PRP impregnated for skin regeneration. (a and b) Preparation of hyaluronic acid nanocomposite hydrogels with PRP impregnated. (c) Injection of the hyaluronic acid nanocomposite hydrogels with PRP impregnated into a wound area in situ for skin regeneration. Reproduced with permission from Li S, Dong Q, Peng X, et al. Self-healing hyaluronic acid nanocomposite hydrogels with platelet-rich plasma impregnated for skin regeneration. ACS Nano. 2022;16(7):11346–11359. Copyright (2022) American Chemical Society.79 |
Chronic wounds, due to the loss of skin barrier function, and bacterial infection are almost an inevitable issue. How to deal with bacteria on wounds and prevent bacterial infection is an aspect that wound dressing design must consider. Bactericidal through photothermal effect is a popular antibacterial method at present. The photothermal effect kills bacteria by quickly converting light energy into heat energy through near-infrared light irradiation, causing a rapid increase in temperature. PRP, extracted from human plasma, usually needs to be stored under cold conditions to maintain its activity. In hydrogels with photothermal effects, it is unknown whether PRP can still exert its biological activity when the temperature rises rapidly. Many growth factors in PRP are biologically active proteins, and temperature changes are likely to affect them. Liu et al published a study in 2024 that combined PRP with hydrogel dressings with photothermal effects.81 They used chitosan and hydroxypropyl cellulose to form the hydrogel matrix, using graphene oxide as a light-to-heat converter. This hydrogel can quickly raise the temperature by 16 degrees Celsius within 8 minutes under near-infrared light irradiation, with the highest temperature controlled around 43 degrees Celsius. The experimental results in animals also showed that the hydrogel with photothermal effect was better than the hydrogel without photothermal effect. Although the gel contained PRP in the experiment and promoted healing compared to the control group, each experimental group in the experiment contained PRP, so it cannot be concluded that the photothermal effect would affect the activity of PRP, and it is even uncertain whether PRP played a role in the in vitro experiments.
An important issue faced by PRP hydrogels in practical applications is the lack of adhesiveness, leading to the rapid loss of PRP at the wound site and a decrease in its effectiveness.82 Increasing the stability of PRP and its action time at the wound undoubtedly can enhance its therapeutic effect on diabetic wound healing.72 In addition, PRP lacks the ability to regulate oxidative stress, inflammation, and infection at diabetic wounds. Dopamine (DA) happens to supplement this missing capability of PRP. Hydrogels combined with DA not only exhibit wet adhesion to various surfaces but also demonstrate antioxidant and anti-inflammatory properties.83 The two can achieve a variety of healing effects by simply combining them in the same biomaterial.
Duan et al (2024) combined dopamine-modified hyaluronic acid (HA-DA) hydrogels with PRP to construct a series of sticky wound dressings, aiming to achieve the goal of diabetic wound repair through anti-inflammatory, antibacterial, antioxidant, and regenerative promotion as shown in Figure 2.84 To provide injectability to DA-derived hydrogels, they introduced Fe3+ chelating agents into the system. The other advantage of Fe3+ is its potential antibacterial ability based on iron. Through the interaction between catechol groups and PRP proteins, PRP is incorporated and anchored in the HA-DA adhesive network. Therefore, just a few simple ingredients can obtain the urgently needed anti-inflammatory, antioxidant, antibacterial, and regenerative capabilities for wound healing. In Duan et al’s hydrogel, the important photothermal effect characteristic of DA was overlooked. The photothermal effect has been proven to be of great significance for the healing of diabetic wounds. DA has proven to have good near-infrared light conversion ability, and the photothermal conversion ability after combining DA and HA was not verified in this experiment. If it also has photothermal conversion effects, the material’s ability to promote the healing of diabetic wounds will be greatly enhanced.
 |
Figure 2 Scheme of the preparation of HA-DA/PRP adhesives and their applications on diabetic SD rats with infected full-thickness skin defect. The preparation of the designed HA-DA/PRP adhesive required only one step by mixing the solution of HA-DA and the solution of FeCl3 with PRP. PRP is anchored in this network due to the hydrogen bonds between PRP protein and DOPA. By applying HA-DA/PRP adhesive on the wound site, the adhesives serve as a microenvironment regulator for infected diabetic wound healing. Reprinted from Carbohydr Polym. Volume 337. Duan W, Jin X, Zhao Y, et al. Engineering injectable hyaluronic acid-based adhesive hydrogels with anchored PRP to pattern the micro-environment to accelerate diabetic wound healing. 122146, copyright 2024, with permission from Elsevier.84 |
Combination of Wound Sponge Dressing With Platelet-Rich Plasma
Lyophilized sponge dressings have a porous structure and are highly absorbent products that can absorb a large amount of PRP to exert its effects in clinical use. Tang et al (2023) used carboxymethyl chitosan and poly-γ-glutamic acid as the base materials for lyophilized sponges, and added calcium ions and thrombin as PRP and activators as shown in Figure 3.73 PRP was added and then lyophilized to construct lyophilized sponge materials. The platelets in PRP can play a role in wound coagulation and hemostasis, while growth factors can be responsible for promoting wound growth. Although this method of simultaneously lyophilizing PRP and materials to obtain lyophilized sponges is feasible in experimental research, there are obstacles in real clinical applications. As an autologous plasma product, if PRP is extracted and then made into sponge dressings by medical device companies, it increases the production process and is not conducive to clinical application. However, wound sponge dressings can adsorb PRP on their own without the need to incorporate PRP into the material and then lyophilize together. The activators of PRP and the base materials of the dressing can be lyophilized together, and PRP can be added on the spot when used in the clinic, making such materials versatile.
 |
Figure 3 A brief presentation for preparation, microstructure, and mechanism of CP-PRP for hemostasis and wound healing. Reprinted from Int J Biol Macromol. Volume: 247. Tang J, Yi W, Yan J, et al. Highly absorbent bio-sponge based on carboxymethyl chitosan/poly-γ-glutamic acid/platelet-rich plasma for hemostasis and wound healing. 125754. Copyright 2023, with permission from Elsevier.73 |
Combination of Graphene Oxide With Platelet-Rich Plasma
Graphene oxide, as a new type of material, has the advantages of high specific surface area, great thermal stability, special physicochemical properties, good electrical conductivity, and amazing mechanical strength, and can play a synergistic effect with other materials.74 Chen et al incorporated PRP into a graphene oxide-reinforced alginate hydrogel to construct a wound dressing as shown in Figure 4.85 Graphene oxide surfaces contain a variety of oxygen-containing functional groups, have richer surface activity, good hydrophilicity, and biocompatibility, which not only play its role in the hydrogel’s good biocompatibility and moisturizing effect, promoting wound healing, but also have antibacterial properties.75 Although the material showed good results, it is a pity that the study did not further explore whether there were any interactions between the graphene oxide material and PRP.
 |
Figure 4 Preparation and characterization of the GO/Alg/PRP. Preparation route of the GO/Alg/PRP (A). Gross appearance and SEM image of GO/Alg, GO/Alg/PRP at indicated magnification scale, and their porous structure (B and C). Reprinted from Front Bioeng Biotechnol. Volume: 12. Chen N, Li M, Yang J, Wang P, Song G, Wang H. Slow-sculpting graphene oxide/alginate gel loaded with platelet-rich plasma to promote wound healing in rats. 1334087, Creative Commons.85 |
Autologous Fat Components Combined With Platelet-Rich Plasma
Components derived from autologous fat, such as adipose-derived mesenchymal stem cells and Nanofat (NF), have been proven to play an important role in tissue regeneration and repair. NF is an autologous fat derivative obtained through mechanical emulsification and filtration to form a liquid suspension.86 NF is widely used in the fields of regenerative and aesthetic medicine, such as facial rejuvenation, fat filling, scar repair, burn management, and hair loss treatment.87 Like PRP, NF can also be extracted from the patient’s own body. NF contains a high concentration of extracellular matrix, growth factors, adipose tissue-derived stem cells, and microvascular fragments.76 All of these individual components have been proven to promote tissue formation and the development of new blood perfusion microvascular networks.88 Limido et al (2024) mixed NF with PRP for the treatment of full-thickness wounds in mice and found the effect to be better than using NF alone.89 Using PRP on the wound can stabilize NF and significantly accelerate and improve tissue regeneration. Both NF and PRP have been widely used in the clinic, and their combination is therefore rational and feasible in clinical applications. However, the extraction of NF requires the removal of a certain amount of autologous fat tissue from the patient’s fat layer, which is highly traumatic to the patient. For patients suffering from chronic diseases, it is uncertain whether such an operation will cause another chronic non-healing wound, and more clinical studies are needed to determine safety. The mechanical and physical properties of both autologous NF and PRP materials are not ideal, with high fluidity. As a dressing, it is possible to consider improving its mechanical properties for clinical use.
Iseki et al (2024) combined adipose-derived mesenchymal stem cells, photo-curable hydrogels, and PRP to create an injectable cartilage repair hydrogel.90 Hydrogel can provide sufficient mechanical support for the dressing and also support the growth of encapsulated adipose-derived mesenchymal stem cells. The growth factors rich in PRP can also protect mesenchymal stem cells and promote their differentiation.91 The interaction of adipose-derived mesenchymal stem cells, hydrogels, and PRP constitutes a closely connected repair system. The same system is also referential in the repair of diabetic wounds.
Summary and Perspective
PRP Has High Feasibility in the Clinical Treatment of Wounds
The model of extracting PRP from patients and then applying it to diabetic wounds has clinical feasibility. Firstly, the source of PRP is stable PRP can be obtained by centrifuging a harmless amount of blood drawn from the patient, and the existing equipment in the hospital’s laboratory can meet its preparation requirements. The amount obtained is sufficient for small-area wounds commonly seen in clinical practice, such as diabetic foot ulcers. However, for large area burns and other wounds, the source of PRP is still not abundant enough.
PRP is easy to preserve. PRP can be preserved by freezing in common freezers in hospitals.38 Chronic wounds still require a long recovery time even after debridement and skin grafting. During this period, supplementing the wound with growth factors and other substances can promote the growth of granulation tissue, providing a good environment for skin grafting and facilitating the survival of the transplanted skin. PRP can be obtained from the body at one time, preserved by freezing, and used multiple times. Chronic wounds are recurrent and have a high risk of recurrence, and PRP can be preserved by lyophilization for a longer storage time, which can be applied to multiple treatments.
PRP Requires a Standardized Protocol in Wound Treatment to Ensure Effectiveness
At present, there is no standardized guide for the use of PRP in wound treatment, which has led to different hospitals relying more on empirical treatments, resulting in unstable effectiveness. Firstly, there is no unified standard for the source of PRP. There is no standard plan for extracting PRP. The methods of extracting PRP in literature are diverse, and the effectiveness of different methods in the clinic has not been certified. Secondly, there is no screening mechanism for patients suitable for PRP treatment. Most patients with chronic wounds are older and have other underlying diseases. It is uncertain whether the blood extracted from patients can be prepared into qualified PRP. There are no standards for the effectiveness of prepared PRP. The content of key components such as platelets and growth factors in the extracted PRP should meet what standards to be qualified PRP has no standards. Secondly, there are no standards for the use of PRP. The dosage and frequency of PRP use are the basis for its effectiveness. Too little PRP will lead to its ineffectiveness, and too much will cause waste. There are no standards for how to use PRP. The methods used in current research include injection, application within the wound, and combination with wound dressings.
A 2024 review and meta-analysis of 10 randomized controlled trials concluded that PRP treatment for ulcers significantly improved the healing rate and time for diabetic foot patients compared to traditional treatment.92 However, a 2021 clinical study found no improvement in healing rate and time between PRP-containing dressings and regular dressings.53 The main reason for these different conclusions from various studies is the different application methods of PRP. Platelet drugs, food, blood sugar, hypertension, dyslipidemia, and stress levels can all affect the quality and effectiveness of PRP samples.93 Moreover, the method of using PRP also has an important impact on its effectiveness.
Therefore, establishing a complete set of PRP usage standards is of great significance to ensure the effectiveness of its treatment. The first step is to determine the effectiveness of the source of PRP and establish a screening mechanism for patients suitable for PRP treatment. For obtained PRP, screening standards should be established, such as testing platelet content and growth factor content to avoid applying ineffective PRP to patients. Establish reasonable clinical usage standards for PRP to regulate its dosage, frequency, and method of use. The method of using RPR may be the key to its effectiveness. The reason why ordinary PRP dressings are ineffective may be due to incorrect usage methods, which fail to exert their effectiveness. The growth factor substances in PRP are more similar to growth factor drugs used in the clinic. Ordinary gauze dressings do not have enough drug-controlled release capacity and cannot help them exert their effectiveness. There are also a variety of materials used for skin regeneration in the clinic, and a reasonable combination of PRP with these materials can better exert the function of PRP.
Materials Combined With PRP Need to Consider Versatility
PRP, as an autologous transplant material, can only be used on the person from whom it is extracted in clinical use and is directional. Therefore, biomaterials containing PRP must also be usable only by the patient from whom the plasma was extracted. However, current medical device production and PRP extraction are not completed by the same entity. Current experimental research, design, and production are all completed by the same laboratory, and the experimental product contains both PRP and biomaterials. The application of experimental animals as subjects does not consider the unity of PRP extraction and usage. These two situations are different from the actual clinical use. In clinical use, hospitals have the ability to extract and produce PRP but do not have the ability to produce wound dressings. Wound dressings are usually produced by medical device companies. Therefore, the most suitable materials for clinical use should be versatile materials produced by medical device companies that can be used in conjunction with PRP when applied.
PRP Has the Ability to Combine With a Variety of Hydrogel Materials
Hydrogel dressings are an important research area in biomaterials for wound treatment today. They can promote wound healing and also provide a platform for many wound treatment drugs. The combination of drugs that promote wound healing with hydrogels is also an important design strategy for wound dressings today. If the drug is combined with the hydrogel and cannot be released, it will inevitably greatly reduce its effectiveness. Many studies have shown that PRP can be combined with a variety of hydrogel materials, such as methacrylated hyaluronic acid hydrogel,94 dopamine-modified hyaluronic acid hydrogel,84 methacrylate gelatin hydrogel,90 bacterial cellulose hydrogel,95 and alginate hydrogel.96 These studies have also proven that PRP can be combined with hydrogels, which can help PRP act on the wound for a longer time and increase the healing ability of hydrogels.
The Effect of Hydrogels With Photothermal Effect Combined With PRP Needs Further Study
Hydrogels with photothermal effects can quickly convert near-infrared light into heat, achieving the effect of wound sterilization and promoting healing. PRP is extracted from the human body and contains platelets and a variety of growth factors. When the wound temperature rises rapidly and exceeds the normal human body temperature, whether the effective components will denature and whether the effectiveness will decrease is not yet deeply studied. If the rapid increase in temperature causes PRP to become ineffective, then the combination of the two would be detrimental. All current studies have not considered this point. If you want to verify whether PRP is effective under photothermal action, you need to set up control groups with and without PRP under near-infrared light irradiation to observe the effect of PRP after temperature change.
If PRP is still effective after the temperature rises in hydrogels with photothermal effects, then its application range will be greatly expanded. Dopamine is also an excellent photothermal conversion material. There have been studies combining PRP with dopamine-containing hydrogels, but there has been no research on its photothermal effect.
Conclusion
In summary, the application of PRP in wound healing has demonstrated significant potential, particularly in the context of diabetic and chronic wounds. The integration of PRP with various biomaterials, such as hydrogels and sponge dressings, has shown promise in enhancing the regenerative process by leveraging the natural growth factors present in PRP. While the clinical application of PRP has been met with variable success, the development of standardized protocols for PRP extraction, application, and combination with biomaterials is crucial for ensuring consistent therapeutic outcomes. Furthermore, the exploration of PRP’s synergistic effects with novel materials like graphene oxide and selenium nanoparticles holds great potential for advancing wound care. Despite the challenges in optimizing PRP’s stability and activity, especially in innovative dressings with photothermal properties, the future of PRP in wound healing appears bright. As research continues to address the variability in PRP preparation and application methods, the field moves closer to realizing PRP’s full potential in transforming wound care and enhancing patient recovery.
Acknowledgments
This work was supported by Zhejiang Provincial Medical and Healthy Science Foundation of China (No. 2022KY1037).
Declaration
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Devriendt N, de Rooster H. Initial management of traumatic wounds. Vet Clin North Am Small Anim Pract. 2017;47(6):1123–1134. doi:10.1016/j.cvsm.2017.06.001
2. Schiestl C, Meuli M, Trop M, Neuhaus K. Management of Burn Wounds. Eur J Pediatr Surg off J Austrian Assoc Pediatr Surg Al Z Kinderchir. 2013;23(5):341–348. doi:10.1055/s-0033-1356650
3. Munoz N, Posthauer ME, Cereda E, Schols JMGA, Haesler E. The role of nutrition for pressure injury prevention and healing: the 2019 international clinical practice guideline recommendations. Adv Skin Wound Care. 2020;33(3):123–136. doi:10.1097/01.ASW.0000653144.90739.ad
4. Holl J, Kowalewski C, Zimek Z, et al. Chronic diabetic wounds and their treatment with skin substitutes. Cells. 2021;10:3. doi:10.3390/cells10030655
5. Rajkumar J, Chandan N, Lio P, Shi V. The skin barrier and moisturization: function, disruption, and mechanisms of repair. Skin Pharmacol Physiol. 2023;36(4):174–185. doi:10.1159/000534136
6. Proksch E, Brandner JM, Jensen J-M. The skin: an indispensable barrier. Exp Dermatol. 2008;17(12):1063–1072. doi:10.1111/j.1600-0625.2008.00786.x
7. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
8. Frykberg RG, Banks J. Challenges in the Treatment of Chronic Wounds. Adv Wound Care. 2015;4(9):560–582. doi:10.1089/wound.2015.0635
9. Gea S, Putra IB, Lindarto D, et al. Bacterial cellulose impregnated with andaliman (Zanthoxylum Acanthopodium) microencapsulation as diabetic wound dressing. Int J Biol Macromol. 2023;253(Pt 1):126572. doi:10.1016/j.ijbiomac.2023.126572
10. Pasaribu KM, Mahendra IP, Sholeha NA, Masruchin N, Mardawati E, Karina M. Recent Developments of the Agroindustry Byproducts Utilization in Bacterial Cellulose Production and Its Medical Devices Applications. In: Lubis MAR, Lee SH, Mardawati E, et al., editors. Biomass Conversion and Sustainable Biorefinery: Towards Circular Bioeconomy. Singapore: Springer Nature Singapore; 2024:207–228. doi:10.1007/978-981-99-7769-7_10
11. Hassanshahi A, Hassanshahi M, Khabbazi S, et al. Adipose-derived stem cells for wound healing. J Cell Physiol. 2019;234(6):7903–7914. doi:10.1002/jcp.27922
12. Wang Y, Chen L, Ren D-Y, et al. Mussel-inspired collagen-hyaluronic acid composite scaffold with excellent antioxidant properties and sustained release of a growth factor for enhancing diabetic wound healing. Mater Today Bio. 2022;15:100320. doi:10.1016/j.mtbio.2022.100320
13. An Y, Lin S, Tan X, et al. Exosomes from adipose-derived stem cells and application to skin wound healing. Cell Prolif. 2021;54(3):e12993. doi:10.1111/cpr.12993
14. Luo L, Wang Y, Zhang S, et al. Preparation and characterization of selenium-rich polysaccharide from phellinus igniarius and its effects on wound healing. Carbohydr Polym. 2021;264:117982. doi:10.1016/j.carbpol.2021.117982
15. Dohan Ehrenfest DM, Rasmusson L, Albrektsson T. Classification of platelet concentrates: from pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends Biotechnol. 2009;27(3):158–167. doi:10.1016/j.tibtech.2008.11.009
16. Zhou D, Liang Q, Ge X, Xu J. Allogeneic platelet-rich plasma inhibits ferroptosis in promoting wound repair of type 2 diabetic ulcers. Free Radic Biol Med. 2024;215:37–47. doi:10.1016/j.freeradbiomed.2024.02.020
17. Belk JW, Kraeutler MJ, Houck DA, Goodrich JA, Dragoo JL, McCarty EC. Platelet-rich plasma versus hyaluronic acid for knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Am J Sports Med. 2021;49(1):249–260. doi:10.1177/0363546520909397
18. Xuan Z, Yu W, Dou Y, Wang T. Efficacy of platelet-rich plasma for low back pain: a systematic review and meta-analysis. J Neurol Surg Part Cent Eur Neurosurg. 2020;81(6):529–534. doi:10.1055/s-0040-1709170
19. Ulusoy AT, Turedi I, Cimen M, Cehreli ZC. Evaluation of blood clot, platelet-rich plasma, platelet-rich fibrin, and platelet pellet as scaffolds in regenerative endodontic treatment: a prospective randomized trial. J Endod. 2019;45(5):560–566. doi:10.1016/j.joen.2019.02.002
20. de Leon JM, Driver VR, Fylling CP, et al. The clinical relevance of treating chronic wounds with an enhanced near-physiological concentration of platelet-rich plasma gel. Adv Skin Wound Care. 2011;24(8):357–368. doi:10.1097/01.ASW.0000403249.85131.6f
21. Malekpour Alamdari N, Shafiee A, Mirmohseni A, Besharat S. Evaluation of the efficacy of platelet-rich plasma on healing of clean diabetic foot ulcers: a randomized clinical trial in Tehran, Iran. Diabetes Metab Syndr. 2021;15(2):621–626. doi:10.1016/j.dsx.2021.03.005
22. Vladulescu D, Scurtu LG, Simionescu AA, Scurtu F, Popescu MI, Simionescu O. Platelet-rich plasma (PRP) in dermatology: cellular and molecular mechanisms of action. Biomedicines. 2023;12:1. doi:10.3390/biomedicines12010007
23. Wang Y, Zhang Y, Yang Y-P, et al. Versatile dopamine-functionalized hyaluronic acid-recombinant human collagen hydrogel promoting diabetic wound healing via inflammation control and vascularization tissue regeneration. Bioact Mater. 2024;35:330–345. doi:10.1016/j.bioactmat.2024.02.010
24. Dai C, Shih S, Khachemoune A. Skin substitutes for acute and chronic wound healing: an updated review. J Dermatol Treat. 2020;31(6):639–648. doi:10.1080/09546634.2018.1530443
25. Behere I, Ingavle G. In vitro and in vivo advancement of multifunctional electrospun nanofiber scaffolds in wound healing applications: innovative nanofiber designs, stem cell approaches, and future perspectives. J Biomed Mater Res A. 2022;110(2):443–461. doi:10.1002/jbm.a.37290
26. Xu F-W, Lv Y-L, Zhong Y-F, et al. Beneficial effects of green tea EGCG on skin wound healing: a comprehensive review. Mol. 2021;26:20. doi:10.3390/molecules26206123
27. Zhuang Z-M, Wang Y, Feng Z-X, et al. Targeting diverse wounds and scars: recent innovative bio-design of microneedle patch for comprehensive management. Small Weinh Bergstr Ger. 2024;20(18):e2306565. doi:10.1002/smll.202306565
28. Lefrançais E, Ortiz-Muñoz G, Caudrillier A, et al. The lung is a site of platelet biogenesis and a reservoir for haematopoietic progenitors. Nature. 2017;544(7648):105–109. doi:10.1038/nature21706
29. Lubkowska A, Dolegowska B, Banfi G. Growth factor content in PRP and their applicability in medicine. J Biol Regul Homeost Agents. 2012;26(2 Suppl 1):3S–22S.
30. Marx RE. Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg off J Am Assoc Oral Maxillofac Surg. 2004;62(4):489–496. doi:10.1016/j.joms.2003.12.003
31. Sánchez AR, Sheridan PJ, Kupp LI. Is platelet-rich plasma the perfect enhancement factor? A current review. Int J Oral Maxillofac Implants. 2003;18(1):93–103.
32. Sánchez-González DJ, Méndez-Bolaina E, Trejo-Bahena NI. Platelet-rich plasma peptides: key for regeneration. Int J Pept. 2012;2012:532519. doi:10.1155/2012/532519
33. Laron Z. Insulin-like growth factor 1 (IGF-1): a growth hormone. Mol Pathol. 2001;54(5):311–316. doi:10.1136/mp.54.5.311
34. Oliveira AG, Araújo TG, Carvalho BDM, Rocha GZ, Santos A, Saad MJA. The role of hepatocyte growth factor (HGF) in insulin resistance and diabetes. Front Endocrinol. 2018;9:503. doi:10.3389/fendo.2018.00503
35. Garg AK. The use of platelet-rich plasma to enhance the success of bone grafts around dental implants. Dent Implantol Update. 2000;11(3):17–21.
36. Aheget H, Tristán-Manzano M, Mazini L, et al. Exosome: a new player in translational nanomedicine. J Clin Med. 2020;9:8. doi:10.3390/jcm9082380
37. Slichter SJ, Dumont LJ, Cancelas JA, et al. Safety and efficacy of cryopreserved platelets in bleeding patients with thrombocytopenia. Transfusion. 2018;58(9):2129–2138. doi:10.1111/trf.14780
38. Su R, Sun L, Ding Y-F, et al. In vitro studies on the effects of cryopreserved platelet-rich plasma on cells related to wound healing. Platelets. 2024;35(1):2347331. doi:10.1080/09537104.2024.2347331
39. Mercader Ruiz J, Beitia M, Delgado D, et al. Method to obtain a plasma rich in platelet- and plasma-growth factors based on water evaporation. PLoS One. 2024;19(2):e0297001. doi:10.1371/journal.pone.0297001
40. Falvo MR, Gorkun OV, Lord ST. The molecular origins of the mechanical properties of fibrin. Biophys Chem. 2010;152(1–3):15–20. doi:10.1016/j.bpc.2010.08.009
41. Nakajima R, Saita Y, Kobayashi Y, et al. Comparison of bioactive substances in novel-developed freeze-dried platelet-rich plasma (PRP) and activated normal PRP, and investigation of bioactive substance levels after long-term storage. Regener Ther. 2024;27:200–206. doi:10.1016/j.reth.2024.03.021
42. Calciolari E, Dourou M, Akcali A, Donos N. Differences between first- and second-generation autologous platelet concentrates. Periodontol. 2000;2024. doi:10.1111/prd.12550
43. Dohan DM, Choukroun J, Diss A, et al. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part III: leucocyte activation: a new feature for platelet concentrates? Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101(3):e51–55. doi:10.1016/j.tripleo.2005.07.010
44. Kobayashi E, Flückiger L, Fujioka-Kobayashi M, et al. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin Oral Investig. 2016;20(9):2353–2360. doi:10.1007/s00784-016-1719-1
45. Burnouf T, Goubran HA, Chen T-M, Ou K-L, El-Ekiaby M, Radosevic M. Blood-derived biomaterials and platelet growth factors in regenerative medicine. Blood Rev. 2013;27(2):77–89. doi:10.1016/j.blre.2013.02.001
46. Anitua E, Andia I, Ardanza B, Nurden P, Nurden AT. Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb Haemost. 2004;91(1):4–15. doi:10.1160/TH03-07-0440
47. Hsu J-T, Chen Y-W, Ho T-W, et al. Chronic wound assessment and infection detection method. BMC Med Inf Decis Mak. 2019;19(1):99. doi:10.1186/s12911-019-0813-0
48. Qiu M, Chen D, Shen C, Shen J, Zhao H, He Y. Platelet-rich plasma-loaded poly(d,l-lactide)-poly(ethylene glycol)-poly(d,l-lactide) hydrogel dressing promotes full-thickness skin wound healing in a rodent model. Int J Mol Sci. 2016;17:7. doi:10.3390/ijms17071001
49. Morbach S, Furchert H, Gröblinghoff U, et al. Long-term prognosis of diabetic foot patients and their limbs: amputation and death over the course of a decade. Diab Care. 2012;35(10):2021–2027. doi:10.2337/dc12-0200
50. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–2375. doi:10.1056/NEJMra1615439
51. Del Pino-Sedeño T, Trujillo-Martín MM, Andia I, et al. Platelet-rich plasma for the treatment of diabetic foot ulcers: a meta-analysis. Wound Repair Regen. 2019;27(2):170–182. doi:10.1111/wrr.12690
52. Nolan GS, Smith OJ, Heavey S, Jell G, Mosahebi A. Histological analysis of fat grafting with platelet-rich plasma for diabetic foot ulcers-a randomised controlled trial. Int Wound J. 2022;19(2):389–398. doi:10.1111/iwj.13640
53. Gupta A, Channaveera C, Sethi S, Ranga S, Anand V. Efficacy of intralesional platelet-rich plasma in diabetic foot ulcer. J Am Podiatr Med Assoc. 2021;111(3):
54. Napit IB, Shrestha D, Choudhury S, et al. A randomised trial of autologous blood products, leukocyte and platelet-rich fibrin (L-PRF), to promote ulcer healing in leprosy: the table trial. PLoS Negl Trop Dis. 2024;18(5):e0012088. doi:10.1371/journal.pntd.0012088
55. OuYang H, Tang Y, Yang F, et al. Platelet-rich plasma for the treatment of diabetic foot ulcer: a systematic review. Front Endocrinol. 2023;14:1256081. doi:10.3389/fendo.2023.1256081
56. Alser OH, Goutos I. The evidence behind the use of platelet-rich plasma (PRP) in scar management: a literature review. Scars Burns Heal. 2018;4:2059513118808773. doi:10.1177/2059513118808773
57. Zawadzki T, Sitek A, Antoszewski B, Kasielska-Trojan A. Do intraoperative platelet-rich plasma injections influence the final appearance of vertical scars after breast reduction? Spectrophotometric analysis. J Clin Med. 2024;13:3. doi:10.3390/jcm13030691
58. Lv Y, Yang Z, Chen Z, et al. Artificial dermis and autologous platelet-rich plasma for treatment of refractory wounds: a clinical study. Int J Low Extrem Wounds. 2024;23(2):275–282. doi:10.1177/15347346211050710
59. Wei Z, Wang B, Lin T, et al. Acellular allogenic dermis combined with vsd for repair of abdominal wall defect: a case series. Am J Transl Res. 2023;15(3):2233–2240.
60. Miguel MMV, Ferraz LFF, Rossato A, Cintra TMF, Mathias-Santamaria IF, Santamaria MP. Comparison between connective tissue graft and xenogeneic acellular dermal matrix to treat single gingival recession: a data reanalysis of randomized clinical trials. J Esthet Restor Dent Off Publ Am Acad Esthet Dent Al. 2022;34(8):1156–1165. doi:10.1111/jerd.12936
61. Xu C, Akakuru OU, Ma X, Zheng J, Zheng J, Wu A. Nanoparticle-based wound dressing: recent progress in the detection and therapy of bacterial infections. Bioconjug Chem. 2020;31(7):1708–1723. doi:10.1021/acs.bioconjchem.0c00297
62. Zhao J, Qiu P, Wang Y, et al. Chitosan-based hydrogel wound dressing: from mechanism to applications, a review. Int J Biol Macromol. 2023;244:125250. doi:10.1016/j.ijbiomac.2023.125250
63. Chen Y, Wang X, Tao S, et al. Research advances in smart responsive-hydrogel dressings with potential clinical diabetic wound healing properties. Mil Med Res. 2023;10(1):37. doi:10.1186/s40779-023-00473-9
64. Zhang M, Zhao X. Alginate hydrogel dressings for advanced wound management. Int J Biol Macromol. 2020;162:1414–1428. doi:10.1016/j.ijbiomac.2020.07.311
65. Verboket RD, Henrich D, Janko M, et al. Human acellular collagen matrices-clinical opportunities in tissue replacement. Int J Mol Sci. 2024;25:13. doi:10.3390/ijms25137088
66. Shan B-H, Wu F-G. Hydrogel-based growth factor delivery platforms: strategies and recent advances. Adv Mater Deerfield Beach Fla. 2024;36(5):e2210707. doi:10.1002/adma.202210707
67. Singer AJ. Healing mechanisms in cutaneous wounds: tipping the balance. Tissue Eng Part B Rev. 2022;28(5):1151–1167. doi:10.1089/ten.TEB.2021.0114
68. Wu W, Jia S, Xu H, et al. Supramolecular hydrogel microspheres of platelet-derived growth factor mimetic peptide promote recovery from spinal cord injury. ACS Nano. 2023;17(4):3818–3837. doi:10.1021/acsnano.2c12017
69. Ranjan S, Fontana F, Ullah H, Hirvonen J, Santos HA. Microparticles to enhance delivery of drugs and growth factors into wound sites. Ther Deliv. 2016;7(10):711–732. doi:10.4155/tde-2016-0039
70. Fang M, Zhang H, Wang Y, Zhang H, Zhang D, Xu P. Biomimetic selenium nanosystems for infectious wound healing. 再生工程. 2023;4(2):152–160.
71. Karas RA, Alexeree S, Elsayed H, Attia YA. Assessment of wound healing activity in diabetic mice treated with a novel therapeutic combination of selenium nanoparticles and platelets rich plasma. Sci Rep. 2024;14(1):5346. doi:10.1038/s41598-024-54064-2
72. Huang Q, Wu T, Guo Y, et al. Platelet-rich plasma-loaded bioactive chitosan@sodium alginate@gelatin shell-core fibrous hydrogels with enhanced sustained release of growth factors for diabetic foot ulcer healing. Int J Biol Macromol. 2023;234:123722. doi:10.1016/j.ijbiomac.2023.123722
73. Tang J, Yi W, Yan J, et al. Highly absorbent bio-sponge based on carboxymethyl chitosan/poly-γ-glutamic acid/platelet-rich plasma for hemostasis and wound healing. Int J Biol Macromol. 2023;247:125754. doi:10.1016/j.ijbiomac.2023.125754
74. Liu S, Zeng TH, Hofmann M, et al. Antibacterial activity of graphite, graphite oxide, graphene oxide, and reduced graphene oxide: membrane and oxidative stress. ACS Nano. 2011;5(9):6971–6980. doi:10.1021/nn202451x
75. Wu K-H, Wang J-C, Huang J-Y, Huang C-Y, Cheng Y-H, Liu N-T. Preparation and antibacterial effects of Ag/AgCl-doped quaternary ammonium-modified silicate hybrid antibacterial material. Mater Sci Eng C Mater Biol Appl. 2019;98:177–184. doi:10.1016/j.msec.2018.12.142
76. Frueh FS, Später T, Lindenblatt N, et al. Adipose tissue-derived microvascular fragments improve vascularization, lymphangiogenesis, and integration of dermal skin substitutes. J Invest Dermatol. 2017;137(1):217–227. doi:10.1016/j.jid.2016.08.010
77. Adjepong M, Agbenorku P, Brown P, Oduro I. The role of antioxidant micronutrients in the rate of recovery of burn patients: a systematic review. Burns Trauma. 2016;4:18. doi:10.1186/s41038-016-0044-x
78. Wang Z, Zhang P, Ding X, Wang J, Sun D. Co-delivery of ampicillin and β-lactamase inhibitor by selenium nanocomposite to achieve synergistic anti-infective efficiency through overcoming multidrug resistance. Chem Eng J. 2021;414(1):128908. doi:10.1016/j.cej.2021.128908
79. Li S, Dong Q, Peng X, et al. Self-healing hyaluronic acid nanocomposite hydrogels with platelet-rich plasma impregnated for skin regeneration. ACS Nano. 2022;16(7):11346–11359. doi:10.1021/acsnano.2c05069
80. Koivunotko E, Koivuniemi R, Monola J, et al. Cellulase-assisted platelet-rich plasma release from nanofibrillated cellulose hydrogel enhances wound healing. J Control Release off J Control Release Soc. 2024;368:397–412. doi:10.1016/j.jconrel.2024.02.041
81. Liu G, Yang Y, Liu Y, et al. Injectable and thermosensitive hydrogel with platelet-rich plasma for enhanced biotherapy of skin wound healing. Adv Healthc Mater. 2024;13(12):e2303930. doi:10.1002/adhm.202303930
82. Wei S, Xu P, Yao Z, et al. A composite hydrogel with co-delivery of antimicrobial peptides and platelet-rich plasma to enhance healing of infected wounds in diabetes. Acta Biomater. 2021;124:205–218. doi:10.1016/j.actbio.2021.01.046
83. Yan Y, Jiang W, Liu L, et al. Dopamine controls systemic inflammation through inhibition of NLRP3 inflammasome. Cell. 2015;160(1–2):62–73. doi:10.1016/j.cell.2014.11.047
84. Duan W, Jin X, Zhao Y, et al. Engineering injectable hyaluronic acid-based adhesive hydrogels with anchored PRP to pattern the micro-environment to accelerate diabetic wound healing. Carbohydr Polym. 2024;337:122146. doi:10.1016/j.carbpol.2024.122146
85. Chen N, Li M, Yang J, Wang P, Song G, Wang H. Slow-sculpting graphene oxide/alginate gel loaded with platelet-rich plasma to promote wound healing in rats. Front Bioeng Biotechnol. 2024;12:1334087. doi:10.3389/fbioe.2024.1334087
86. Friji MT. Nanofat Grafting: basic research and clinical applications. Plast Reconstr Surg. 2014;134(2):333e–334e. doi:10.1097/PRS.0000000000000333
87. Suh A, Pham A, Cress MJ, et al. Adipose-derived cellular and cell-derived regenerative therapies in dermatology and aesthetic rejuvenation. Ageing Res Rev. 2019;54:100933. doi:10.1016/j.arr.2019.100933
88. Schultz GS, Wysocki A. Interactions between extracellular matrix and growth factors in wound healing. Wound Repair Regen. 2009;17(2):153–162. doi:10.1111/j.1524-475X.2009.00466.x
89. Limido E, Weinzierl A, Ampofo E, Harder Y, Menger MD, Laschke MW. Nanofat accelerates and improves the vascularization, lymphatic drainage and healing of full-thickness murine skin wounds. Int J Mol Sci. 2024;25:2. doi:10.3390/ijms25020851
90. Iseki T, Rothrauff BB, Kihara S, et al. Enhanced osteochondral repair by leukocyte-depleted platelet-rich plasma in combination with adipose-derived mesenchymal stromal cells encapsulated in a three-dimensional photocrosslinked injectable hydrogel in a rabbit model. Stem Cell Res Ther. 2024;15(1):159. doi:10.1186/s13287-024-03750-z
91. Xu Z, Yin W, Zhang Y, et al. Comparative evaluation of leukocyte- and platelet-rich plasma and pure platelet-rich plasma for cartilage regeneration. Sci Rep. 2017;7:43301. doi:10.1038/srep43301
92. Peng Y, Wang J, Liu X, et al. Efficacy of platelet-rich plasma in the treatment of diabetic foot ulcers: a systematic review and meta-analysis. Ann Vasc Surg. 2024;98:365–373. doi:10.1016/j.avsg.2023.05.045
93. Nadarajah S. Does platelet rich plasma (PRP) treatment really work? BMJ. 2024;385:q578. doi:10.1136/bmj.q578
94. Qi J, Li X, Cao Y, et al. Locationally activated PRP via an injectable dual-network hydrogel for endometrial regeneration. Biomaterials. 2024;309:122615. doi:10.1016/j.biomaterials.2024.122615
95. Wang X, Yang X, Xiao X, Li X, Chen C, Sun D. Biomimetic design of platelet-rich plasma controlled release bacterial cellulose/hydroxyapatite composite hydrogel for bone tissue engineering. Int J Biol Macromol. 2024;269(Pt 2):132124. doi:10.1016/j.ijbiomac.2024.132124
96. Xie X, Ao X, Xu R, et al. Injectable, stable, and biodegradable hydrogel with platelet-rich plasma induced by l-serine and sodium alginate for effective treatment of intrauterine adhesions. Int J Biol Macromol. 2024;270(Pt 1):132363. doi:10.1016/j.ijbiomac.2024.132363
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.