")
Back to Journals » Nature and Science of Sleep » Volume 17
Relationship Between Obstructive Sleep Apnea and Enuresis in Children: Current Perspectives and Beyond
Authors Wang Z , Zhang P, Shi R, Yang S, Liu K, Zhou Z , Li Q
Received 12 August 2024
Accepted for publication 17 January 2025
Published 3 February 2025 Volume 2025:17 Pages 211—222
DOI https://doi.org/10.2147/NSS.S489710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Valentina Alfonsi
Zhan Wang,1,* Pengpeng Zhang,2,* Run Shi,3,* Shuai Yang,1 Kui Liu,4 Zhaokai Zhou,1 Qi Li5
1Pediatric Urodynamic Center, Department of Urology, The First Affiliated Hospital of Zhengzhou University, Henan Joint International Pediatric Urodynamic Laboratory, Zhengzhou, 450052, People’s Republic of China; 2Department of Lung Cancer, Tianjin Lung Cancer Center, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin’s Clinical Research Center for Cancer, Tianjin Medical University Cancer Institute and Hospital, Tianjin, People’s Republic of China; 3Department of Oncology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 4Department of Pediatric Surgery, The First Affiliated Hospital of Henan University of Science and Technology, Luoyang, 471000, People’s Republic of China; 5Department of Pediatric Surgery, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450052, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhaokai Zhou, Pediatric Urodynamic Center, Department of Urology, The First Affiliated Hospital of Zhengzhou University, Henan Joint International Pediatric Urodynamic Laboratory, Zhengzhou, 450052, People’s Republic of China, Email [email protected] Qi Li, Department of Pediatric Surgery, the First Affiliated Hospital of Zhengzhou University, Zhengzhou, 450052, People’s Republic of China, Email [email protected]
Background: Nocturnal enuresis (NE) and obstructive sleep apnea (OSA) are common diseases in children, which often cause various social and psychological problems. The coexistence of both seriously affects the physical and mental health of children. However, whether OSA can directly lead to NE and the specific pathogenesis is still unclear. Moreover, the benefits of surgical and non-surgical treatments for OSA on NE symptoms remain controversial. This review summarizes the relationship between NE and OSA and how to treat them, aiming to provide a reference for the clinical treatment of OSA and NE in children.
Methods: All pertinent original publications to this point from PubMed database have been collected, including investigations on the connection between OSA and NE as well as studies on the mechanism and therapeutic strategy of NE in children with OSA.
Results: There is a bidirectional relationship between OSA and NE in children. NE increases with the incidence of OSA, and children with NE often have sleep-disordered respiratory disease. Children with OSA may be susceptible to NE due to aberrant humoral factors secretion, sleep-wake disorder, bladder dysfunction, obesity, and psychosomatic factors. It has been suggested that adenotonsillectomy (AT) may be the best treatment option for children suffering from OSA with NE. The benefits of positive airway pressure (PAP) therapy in children with NE remain to be further studied.
Conclusion: NE and OSA comorbidity seriously affect the physical and mental health of children. AT can benefit children with OSA and NE. A comprehensive multidisciplinary evaluation of children with NE and OSA is needed, and the mechanism and treatment of NE in children with OSA need to be further explored.
Keywords: obstructive sleep apnea, nocturnal enuresis, children, atrial natriuretic peptide, sleep-wake disorder, adenotonsillectomy
Introduction
Nocturnal enuresis (NE) and obstructive sleep apnea (OSA) are both common diseases in children.1 Intermittent incontinence that occurs during the waking state is called daytime urinary incontinence.1 In contrast, NE, commonly known as bed-wetting, is a special type of urinary incontinence that occurs during sleep.1,3 According to the International Children’s Continence Society (ICCS) criteria, NE refers to the occurrence of involuntary urine leakage symptoms in children aged >5 years during nighttime sleep with a frequency >1 time/month and a duration >3 months after excluding organic causes.3 ICCS classifies NE into two types: primary and secondary NE or NE into monosymptomatic and non-monosymptomatic NE based on the absence or presence of other lower urinary tract symptoms.3 According to the latest epidemiologic studies, between 6% and 16% of children above the age of five have NE.5–8 A cross-sectional study from Korea showed that the prevalence of NE did not significantly decrease with age, with a prevalence of NE of up to 2.6% aged 16–40 years.8 The etiology of NE is complicated, and the pathogenesis is not completely known. It is generally believed to be the result of the interaction among sleep-awakening disorder, nocturnal polyuria, bladder and urethra dysfunction, neurotransmitter and receptor abnormalities in the central nervous system, and genetic factors.10–13 Mental and behavioral abnormalities are often one of the adverse events caused by NE.13 The development of voiding control function in children depends on the increase of bladder capacity, autonomous control of the urethral sphincter, and voiding reflex.1,3 Any problem of them can lead to NE.
OSA in children refers to repeated airway partial or complete collapse and obstruction and disturbed sleep ventilation and sleep structure, leading to sleep hypoxia, hypercapnia, sympathetic excitation, activated oxidative stress, and inflammatory damage response.15–17 The clinical manifestations of OSA include snoring, breath holding, laborious breathing, mouth breathing, and awakening difficulties during sleep, which can also result in growth retardation, non-specific behavioral disorders, cognitive dysfunction, and decreased intelligence and learning.14 Polysomnography is currently the gold standard for the diagnosis of OSA in children. Apnoea–hypopnoea index (AHI) is the most commonly reported polysomnographic parameter describing OSA severity in the literatures. If the AHI detected by PSG during sleep monitoring is more than five events per hour, OSA can be diagnosed.14 The prevalence of OSA in children is 1% to 4%.15 OSA in children is commonly caused by compliance changes brought on by increased upper airway resistances, such as allergies sinusitis, laryngeal cartilaginous softness, obesity-related airway stenosis, craniofacial deformity, and similar conditions. The most frequent reason is tonsil and/or adenoid hypertrophy.16
The peak age of children with NE and OSA is 5–7 years old, and they often cause various psychosocial problems, which have serious negative effects on the life quality of children and their families.14,17 At present, the influence of OSA on NE has been widely concerned by scholars. Many studies have suggested that cardiopulmonary and renal reflex-induced neuroendocrine disorder may play an important role in the mechanism of NE in children with OSA, but its specific pathogenesis is still unclear.9,10 Moreover, the benefits of the surgical and non-surgical treatments of OSA in children with NE remain controversial. In this review, we summarized the pathogenesis and benefits of treatment of NE caused by OSA, which aimed to provide a reference for the clinical treatment of NE in children with OSA.
Methods
This study conducted an extensive search for papers published from 1981 to 2024 using the PubMed database. We use the search terms: “((Nocturnal enuresis) AND (Obstructive sleep apnea)) AND (Children)”. In order to maintain a focus on formal and significant scholarly contributions, only articles and reviews were included. Each included literature was independently reviewed and examined by at least three authors for relevance and quality to the study topic.
Results
The Association Between OSA and NE and the Severity of the Comorbidity
There is a bidirectional relationship between OSA and NE in children. The incidence of NE increases along with OSA and children with NE often have respiratory disorder disease.1,15 Both diseases have an underlying sleep disorder characterized by sleep fragmentation and altered wake response. Abnormal facial pattern (dolicofacial) and head posture were observed in children with NE, features closely linked to OSA.18 Using bladder manometry, researchers monitored the bladder pressure of patients throughout the night and found that arousal disorder-related symptoms such as detrusor hyperactivity, bladder instability, and increased nocturnal urination were all linked to NE.19 Subclinical symptoms of disturbed breathing, respiratory arousals, and hypopneas are often observed in children with therapy-resistant NE who have no prior history of snoring or sleep apnea.20 In the recent study, 68.5% of the children with primary NE had OSA, with two-thirds having moderate-to-severe OSA (AHI ≥ 5 episodes/h).21 Children with primary NE were at risk for the development of OSA in children with primary NE were associated with nasal obstruction due to nasal blockage, the adenoid/adult facial phenotype, and an arched palate. Without regard to gender, patients with refractory NE had a noticeably greater frequency of OSA.22 Moreover, it has been reported that children with OSA constituted about 27% of the pediatric population, and 8–47% of children with OSA had symptoms of NE, which suggests that it had an important clinical significance to ask and evaluate bedwetting for children with OSA.23,24 OSA is frequent in children with monosymptomatic NE. The study by Ferrara et al found that the prevalence of sleep disorders in children with NE was high: 7% of children had sleep apnea, 41.2% had bruxism, 57.8% had snoring, 47.3% had sleep talking, and 15.7% had restless sleep.25 Sleep questionnaires showed that the NE children had more sleep problems than the control group, especially breathing disorders, and daytime sleepiness.26 A recent prospective study included 140 NE patients, 87 patients (aged 9.5 ± 2.6 years) underwent polysomnography, 6 of them were diagnosed with severe apnea, and 40.7% with mild/moderate apnea.27 Soylu et al reported that 80% of patients with primary NE and 36% of secondary NE patients had OSA, while the frequency of primary and secondary NE for OSA children was 24% and 6%, respectively.23 All these suggest that children with OSA and NE are a large group and need more scholars’ attention. The presence of frequent partial or complete OSA can interfere with normal sleep and breathing during sleep, resulting in OSA causing a range of symptoms.14 A cross-sectional observational study of children aged 6–12 years showed that 22.3% of elementary school children had NE, and OSA was a common problem in children with NE.28 For school-age children, males, obesity, an early bedtime, loud snoring, dyspnea, and night-time open-mouth breathing were all considered possible independent risk factors for NE.28 Moreover, A multitude of studies had also shown that the prevalence of NE in OSA children was about 33–50%, while 54% of children with NE showed some degree of sleep-disordered breathing, which further indicated a significant bidirectional relationship between OSA and NE.29,30 Interestingly, the arousal index of NE children with OSA was higher than those without OSA.31 However, the study by Banhara et al found that no significant correlation was observed between OSA symptoms and NE, while the Pierre Robin sequence, a congenital craniofacial malformation, served as a greater risk for NE.32
Health-related quality of life (HRQoL) is described as an individual’s comprehensive perception of disease, life condition, and adaptability. It is composed of multidimensional aspects such as physiological, psychological, emotional, social, and spiritual functions, which can evaluate the patient’s subjective feelings about medical conditions.33 Snoring raises the risk of behavioral and psychological issues, as well as decreased HRQoL, in children with monosymptomatic NE. Besides, HRQoL has been negatively impacted by both NE and OSA, ranging in severity from snoring to OSA.34 It has been demonstrated that children with chronic diseases such as NE and OSA had lower HRQoL, which can seriously affect the physical function, emotional state, social function, responsibilities, and health awareness of children and their families.35,36 Children with NE often have tension, an inferiority complex, excessive anxiety, and extreme pain and guilt after bed-wetting.35 Children with OSA are also often suffering from the burden of a series of clinical manifestations such as short stature, withdrawal, and low spirit.36 The HRQoL of OSA children, both with and without NE, was found to be identical, indicating that the primary cause causing the HRQoL impairment was OSA rather than NE.16 However, some studies have found that children with both NE and OSA have a more pronounced impairment in HRQoL compared to children with either NE or OSA alone, suggesting that comorbid NE and OSA have a negative additive effect on HRQoL.33
Possible Pathogenesis of NE in Children With OSA
Abnormal Secretion of Humoral Factors
Studies have demonstrated that children with OSA have elevated atrial natriuretic peptide (ANP), decreased antidiuretic hormone (ADH), and more nocturnal urine volume.1,37,38 The possible mechanism of NE caused by abnormal humoral factors secretion is as follows (Figure 1A). First, due to the repeated OSA in children with OSA during sleep, the partial pressure of blood oxygen gradually decreases and the partial pressure of carbon dioxide gradually increases, forming a hypoxic environment and hypercapnia, which causes pulmonary arterial hypertension and pulmonary vasoconstriction, increasing the cardiac preload and atrial volume.38 Moreover, the negative pressure in the chest increases when the patients try to improve the hypoxia environment, further aggravating the cardiac preload and increasing the atrial volume.39 However, increased cardiac preload and atrial volume is a pull stimulation on the atrial wall, which can stimulate the release of ANP from atrial myocytes.39 ANP has the function of promoting the kidney to expel sodium and water and inhibiting ADH and the renin-angiotensin-aldosterone system.40 Increased secretion of ANP can lead to NE. Usually, the ADH level has a rhythm of decreasing day and increasing at night, which causes increased urine reabsorption and reduced urine production during sleep.41 However, the nocturnal ADH level was lower in children with OSA, producing large amounts of hypotonic urine, which might be that the developing brain of children and normal hormone secretion was affected and the stable circadian rhythm was changed due to the low oxygen environment.42 In addition, most children with OSA recovered the normal ANP and ADH levels after adenotonsillectomy (AT), which might be one of the reasons for the improvement of NE symptoms.43
 |
Figure 1 Reflex mechanisms of OSA induced NE. (A) Abnormal secretion of humoral factors. (B) Sleep-wake disorder. (C) Bladder dysfunction. |
The autonomic nervous system-related neurotransmitters, brain natriuretic peptide (BNP), and endothelin system may also be involved in NE. Studies have shown that decreased sympathetic nerve activity and catecholamines after AT were also associated with the improvement of NE.44 Angeli et al found that children with NE had increased rapid-eye-movement sleep duration, indicating sympathetic overactivity, while patients with overactive bladder had non-rapid-eye-movement sleep-related symptoms of NE, which was possibly related to parasympathetic nerve stimulation. Both sympathetic and parasympathetic overactivities were associated with sleep disorders in children with NE.45 Other studies had shown that the BNP was increased in children with OSA and NE, and the degree of increase was related to the severity of OSA.43 BNP is also secreted by cardiomyocytes, which can encourage sodium excretion, prevent the renin-angiotensin-aldosterone pathway, and reduce the release of ADH, thereby promoting urination.46 However, a longitudinal prospective intervention study in children aged 5 to 14 years showed that a total of 85.8% of children had partial or complete improvement in NE after airway obstruction surgery and 42.8% showed complete remission with elevated BNP but no increase in the ADH. Thus, the improvement in NE was not explained by synergistic changes in BNP and ADH.41 Furthermore, the endothelial system was also a potential physiological pathway in NE.47 The endothelial pathway has been pointed out to play a critical role in natriuretic, diuretic, and the central regulation of the synthesis of ADH and other hypothalamic hormones, which may indirectly act by affecting ADH and renin-angiotensin-aldosterone system.48,49
Sleep-Wake Disorder
One of the main contributing factors to the pathophysiology of NE in children with OSA is the disruption of the waking mechanism during sleep. The brains of children are not fully developed. Lack of development in the regulation of the hypothalamic sleep-wake centers causes sleep awakening disorder, leading to NE (Figure 1B).Compared to NE children without OSA, the NE children with OSA were more difficult to wake up in the morning by the evaluation of nocturnal polysomnosis monitoring, which indicated that the sleep structure of children with OSA was partly related to the occurrence of NE.50 NE occurred in children with OSA because they were unable to wake up in time by the regular awakening mechanism, despite the stimulation of bladder filling and detrusor contraction causing a need for micturition.3 Kovacevic et al found that most children could not be awakened before AT but could wake up and urinate after surgery.43 This phenomenon might be because OSA was relieved after AT in children with OSA and normal sleep was not disturbed, allowing normal self-arousal mechanisms to take effect.
Disturbed sleep architecture in children with OSA was manifested by recurrent cortical awakening during sleep.9,50 Nocturnal polysomnography showed that children with OSA had frequent cortical awakenings associated with light sleep, but less actual awakenings.50 The occurrence of NE was also associated with frequent cortical arousal.9 Furthermore, a number of current studies have suggested that deep sleep has been linked to frequent arousal in experimental settings and contributes to NE.52–54 Compared to their healthy peers, NE children with OSA were reported to be more likely to experience repeated arousal.51 Therefore, it was speculated that the mechanism of sleep-wake disorder promoting NE could be summarized. Children with OSA developed a hypoxic environment due to OSA. A hypoxic environment is an arousal stimulus to the brain, which can lead to sleep structure disturbance and repeated cortical arousal, resulting in increased true arousal threshold and decreased sensitivity to bladder filling and detrusor contraction stimulation. The inability to respond to bladder filling or wake up in time led to NE.52 Snoring in children with OSA could increase sleep pressure, further raising the awakening threshold.53
Bladder Dysfunction
The detrusor, urethral sphincter, and conscious control work together to produce urination, a complicated positive feedback reflex. Children suffering from OSA may have recurrent periods of intermittent hypoxia, resulting in elevated urinary nerve signaling, detrusor overactivity, internal sphincter contraction, and increased excitability of the bladder receptors, which is one of the reasons for NE (Figure 1C). Studies have found that the pathophysiology of NE was associated with elevated intra-abdominal pressure and bladder pressure resulting from breathing efforts against an obstructed airway.54 An important cause of NE in children with OSA was bladder dysfunction, including reduced functional bladder capacity, nocturnal detrusor overactivity, and urethral instability. The detrusor overactivity of NE children will be further aggravated by the deterioration of OSA.21 By urodynamics examination, 30% of OSA kids experienced bladder instability according to Watanabe et al.55 This might be due to the suppression of the pontine micturition center caused by the hypoxic environment in OSA children during night sleep, resulting in detrusor overactivity, incomplete bladder relaxation, and decreased bladder volume during urinary storage. A smaller bladder capacity could initiate urination. In addition, the low oxygen environment can also affect the urination reflex arc, causing the bladder to go out of control and leading to NE. However, other studies have shown that children with OSA and NE had longer detrusor contraction time and higher bladder pressure compared to children without NE or OSA, while there were no differences in bladder volume, neuromuscular characteristics, and urethral sphincter function.56 This might be due to the need for vigorous breathing in OSA patients, resulting in a significant increase in abdominal and bladder pressure and promoting urination.
Obesity and Psychophysiological Factors
Obesity or overweight is not only a risk factor for OSA but also NE. The association between NE and OSA was more pronounced in children with obesity, and higher AHI was seen among them.21,57 On the one hand, this association might be attributed to the fact that obesity could increase upper airway collapse through mechanical effects.57 On the other hand, children with obesity have poor mental health and social function, dissatisfaction with their weight, and impaired self-esteem, producing depression, which would cause children with obesity to stay up late, and then affect the release of ADH and promote NE. NE would further increase the psychological burden on children, forming a vicious circle of NE, psychology, and obesity.33,57 Moreover, Demirbas et al found that screen time exposure might be a contributing factor to sleep disorder in children with NE, and controlling screen time in childhood within the normal range was thought to contribute to the treatment of NE.58 This approach was beneficial and easy to apply, with a positive impact on response to treatment and relapse. However, as required by evidence-based medicine regulations, further randomized controlled studies and meta-analyses were needed to support these results.
In addition, other studies have shown that one possible link between OSA and NE could be inflammation and that obesity played an important role in the inflammatory response.3 More fat cells are found in visceral fat than in subcutaneous fat, which encourages macrophages to secrete more proinflammatory cytokines and triggers an inflammatory response.59 There was a strong positive correlation between proinflammatory cytokines level and body mass index in adults, particularly in the region of visceral obesity.59 Likewise, it was reported that the inflammatory response was assessed using C-reactive protein levels and the positive correlation between C-reactive protein levels and visceral fat regions in adolescents showed that visceral obesity is the important cause of the systemic inflammatory response.60 It has been demonstrated that the severity of OSA was correlated with visceral adiposity in adolescents.61 According to the aforementioned findings, inflammatory cytokines might be involved in the mediation of OSA and NE in children with obesity. Besides, allergy reactions triggered by inflammatory cytokines in allergic illnesses might result in NE. Studies have found that OSA children with allergy had a much higher chance of developing NE (P < 0.001), indicating that there might be a combination of both conditions in the pathophysiology of NE.62 While we can hypothesize that inflammatory cytokines may be involved in this relationship, more research is needed to determine the precise mechanism.
Genetics, Gender, and Others
It had been reported that OSA patients had familial clustering, and genetic factors might be related to the pathogenesis of OSA, or it might be that the risk factors associated with OSA were related to heredity. So far, no genetic diagnostic marker genes for OSA have been confirmed.63 Genetic factors played a decisive role in many NE patients. Pedigree analysis and the twin method all showed that NE had a high heritability. It was generally believed that NE followed the pattern of autosomal dominant inheritance. Whether NE and OSA share common genes remains to be further investigated. Nevertheless, behavior and maturational delay remain the most significant cause of NE.64
The study found that the severity of OSA was positively correlated with the prevalence of NE. However, OSA girls were more likely to eventually cease NE than boys. Some scholars speculated that it might be due to the different sensitivity of the kidney to different sex hormones.37,65
The state of renal hyperfiltration at night might also be one of the causes of NE. It has been demonstrated that the diastolic blood pressure and excretion of urinary sodium increase in tandem with the severity of OSA. Pressure-induced natriuresis is caused by recurrent increases in systemic blood pressure following nocturnal obstructive episodes.66 Effective OSA treatment can control natriuresis and polyuria.67 Glomerular filtration fraction was significantly increased in OSA patients, and the extent of its increase was related to the degree of hypoxia. The more severe night-time hypoxia, the more likely patients were to show a renal hyperfiltration state, which further increased nocturnal urine volume. It might be related to the damage of the hypoxia environment to renal tissue structure, resulting in decreased concentration or dilution functions of the kidney.68,69
Improvement of NE by OSA Treatment
Surgical Intervention
For children with OSA, AT is a simple and effective method that may alleviate NE in this population. It is possible that the occurrence of night apnea is reduced by removing the tonsils and adenoids, which reduces the release of ANP and ADH and leads to a normal arousal threshold in turn, thereby effectively alleviating NE.71–73 In 1977, Simmons et al first reported two cases of NE in OSA children, but NE was cured after the elimination of OSA by surgery (adenoidal tonsillectomy, tracheotomy).70 Interestingly, a child suffering from primary NE with chronic recurrent otitis media with effusion, adenoid hypertrophy, and severe snoring still wet the bed after various treatments, including limiting fluid intake before bedtime and waking the child to urinate at night. However, the phenomenon disappeared immediately without any discomfort after AT.56 At present, the cure rate of children with NE and OSA after nasopharyngeal surgery is 62–90%.23 Similarly, Kaya et al found that 52% of the children with NE had complete resolution for NE. Also, the rest of these children had a significant decrease in NE, and daytime bedwetting occurrence decreased significantly after AT.71 Ahmadi et al came to a similar conclusion that 51 (60.7%) of the children had fully recovered from NE, and 22 (26.2%) had exhibited some improvement following AT.72 Some researchers constructed that NE was resolved in more than half of the OSA children after AT.43,74–76
Nevertheless, considering that spontaneous regression typified the natural history of NE, Snow et al investigated whether AT had additional benefits for children with non-severe OSA.37 According to whether to perform AT, 393 children with non-severe OSA were divided into the observation group (201 patients) and the AT group (192 patients). The results showed that the regression rate of NE was around two times higher comparing the AT group to the observation group. AT had a good clinical efficacy, which suggested that children with non-severe OSA could consider using AT to treat chronic and cumbersome NE problems, especially when parents consulted about the benefits and risks of surgical intervention in children with NE and non-severe OSA. Martenstyn et al reported that the OSA children who received AT were less likely to develop NE compared with those without AT.50 The children with NE and severe OSA monitored by nocturnal polysomnosis were more likely to have an improvement in bedwetting after the surgery. This phenomenon may be attributed to the relatively mild OSA as a co-morbid disease of NE, while severe OSA is the pathogenic cause of NE. This speculation needs to be further investigated. Although it had been noted that NE improved following AT,62 a different study discovered that not all children with OSA and NE had dryness.76 Kalorin et al pointed out that urine incontinence neither before nor after tonsillectomy was correlated with tonsillar hypertrophy.77 Similarly, Facundo et al also found that surgical management of airway obstruction had no influence on the resolution of NE for individuals with OSA.78 They found no statistically significant differences in age, race, gender, body mass index, NE types, or AHI between patients treated with AT and those who abandoned the treatment. Many studies have shown that children’s age, obesity index, comorbidities such as allergic rhinitis and structural airway abnormalities may all affect the outcome of surgical treatment of OSA the improvement of NE.77–80 In addition, the criteria for describing OSA was unclear in some prospective studies evaluating the relationship between OSA and primary monosymptomatic NE, which might influence the results.80,81 The role of OSA treatment in the improvement of NE children has been mentioned above. Herein, we dissect relevant representative outcomes in the current data (Table 1).
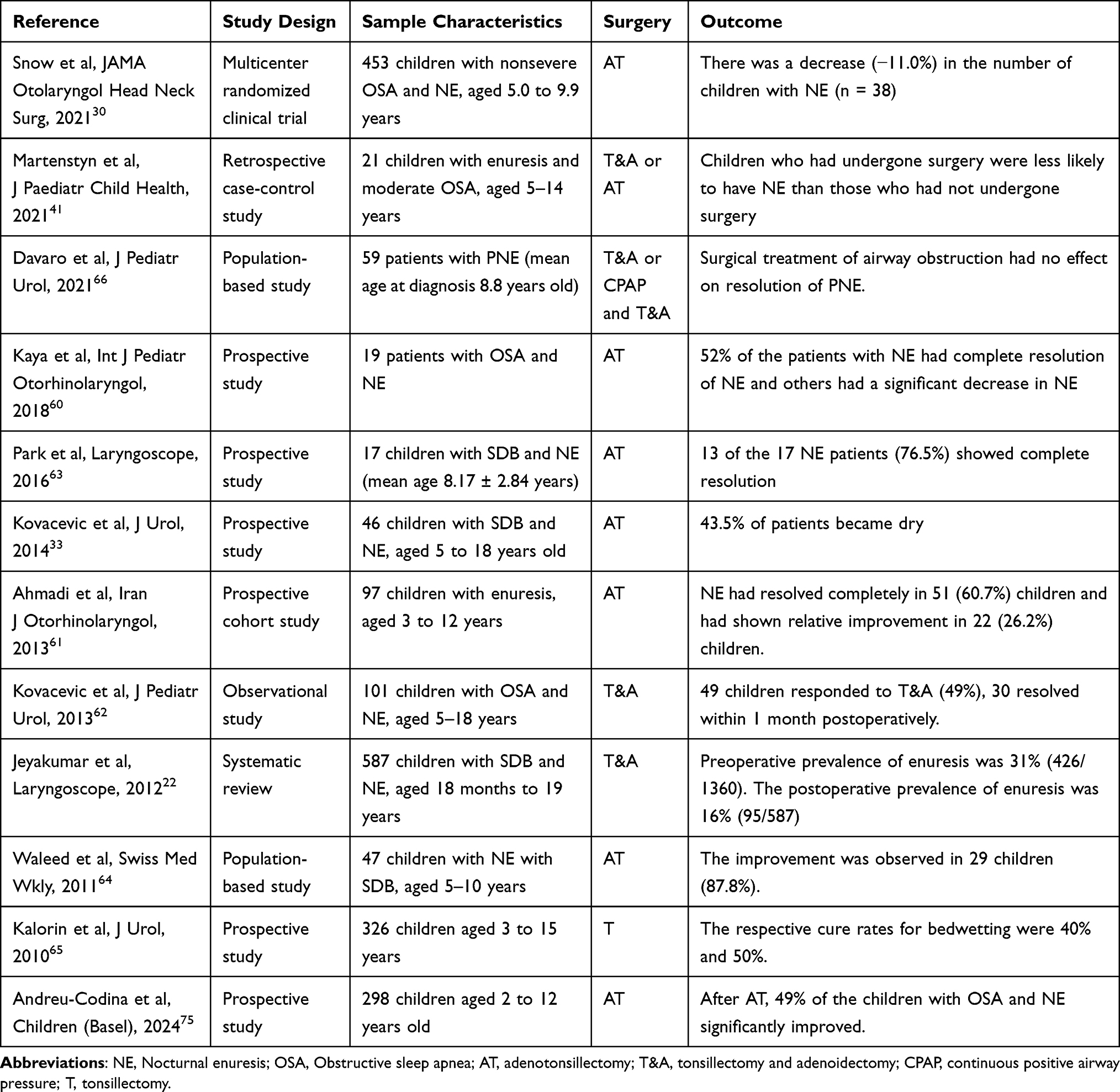 |
Table 1 Outcome of the Treatment for Obstructive Sleep Apnea in Children With Enuresis Nocturna |
Non-Surgical Treatment
In addition to surgical intervention, some non-surgical treatments, such as positive airway pressure (PAP) therapy, have been found to be effective in improving NE symptoms in patients with OSA. PAP can improve sleep quality, reduce nocturnal awakenings, and enhance oxygenation levels through sustained airway positive pressure, which may indirectly contribute to the alleviation of NE.82 Although there are fewer relevant researches, some studies have shown that the frequency of nocturnal urination, the nocturnal urine volume, and the nocturia excretion of Na(+) in patients with OSA were significantly reduced after treatment with transnasal continuous PAP.84–87 Furthermore, a meta-analysis suggests that continuous PAP may be an effective treatment for reducing NE associated with OSA and improving the quality of life for such patients.87 However, researches on the effects of PAP on NE in children are still limited and further exploration and evaluation is urgently needed. Research advances in this field will help deepen our understanding of NE treatment and provide more comprehensive therapeutic strategies.
Strengths and Limitations
We retrospectively summarize the research literature on children NE combined with OSA over the past four decades, and systematically analyze the bidirectional relationship between NE and OSA, the possible mechanisms by which OSA promotes NE, and the effects of surgical and non-surgical interventions of OSA on NE symptoms. This broadens our understanding of the etiology of NE in children with comorbid OSA and provides new treatment ideas and intervention strategies for the clinicians. In addition, this study also emphasized the complex interaction between children NE and OSA, suggesting that future studies should focus on the in-depth exploration of the relationship between the two, as well as more effective treatments, especially in terms of behavioral interventions and non-surgical treatments for further evaluation. However, there are several restrictions on this review. First of all, this review exclusively covered English literature, and the significant works in other languages were left out of the analysis. Next, this study only used the PubMed database as a data source. Relying on a single data source may result in a less comprehensive understanding of a particular domain, limiting the depth and breadth of the analysis. Therefore, future research could consider integrating other databases and data types to provide a more comprehensive analysis and to remedy the shortcomings of the current study.
Conclusions
The co-incidence of NE and OSA seriously affects the physical and mental health of children. The possible mechanisms of NE in children with OSA are that abnormal humoral factors (including ANP, ADH, BNP, catecholamines, renin-angiotensin-aldosterone system, inflammatory factors, etc) and dysfunction of kidney self-regulation lead to more nighttime urine volume in children. Abnormal regulation of the central nervous system and urination reflex promote overactivity of the bladder and aggravate instability of the bladder at night. The elevated arousal threshold due to sleep-wake disorder makes children with OSA unable to wake up without responding to bladder-filling signals or detrusor contraction stimulation. Obesity, psycho-psychological factors, genetics, gender, and family factors further promote the formation of NE, which ultimately leads to bedwetting in children with OSA. The exact mechanism of NE is not yet conclusive, but ANP levels and sleep-wake disorders may play a crucial role, and AT and PAP can benefit children with OSA and NE co-morbidity. In conclusion, a comprehensive multidisciplinary evaluation of children with NE and OSA is needed, and further studies are needed on the pathogenesis, prevention, and treatment of NE in children with OSA.
Abbreviations
NE, Nocturnal enuresis; OSA, Obstructive sleep apnea; AT, Adenotonsillectomy; ANP, Atrial natriuretic peptide; ICCS, International Children’s Continence Society; AHI, Apnoea–hypopnoea index; HRQoL, Health-related quality of life; ADH, Antidiuretic hormone; BNP, Brain natriuretic peptide; PAP, Positive airway pressure.
Consent for Publication
All authors have seen and approved the manuscript and consent publication.
Author Contributions
All authors made a significant contribution to this work, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Postdoctoral Fellowship Program of CPSF under Grant Number GZC20241552, Joint Co-construction Project of Henan Medical Science and Technology Research Program (LHGJ20240277).
Disclosure
The authors declare that they have no competing interests.
References
1. Karamaria S, Ranguelov N, Hansen P. et al. Impact of New vs. Old International Children’s Continence Society Standardization on the Classification of Treatment Naïve Enuresis Children at Screening: the Value of Voiding Diaries and Questionnaires. Front Pediatr. 2022;10:862248. doi:10.3389/fped.2022.862248
2. Chang SJ, Van Laecke E, Bauer SB, et al. Treatment of daytime urinary incontinence: a standardization document from the International Children’s Continence Society. Neurourol Urodyn. 2017;36(1):43–50. doi:10.1002/nau.22911
3. Nevéus T, Fonseca E, Franco I, et al. Management and treatment of nocturnal enuresis-an updated standardization document from the International Children’s Continence Society. J Pediatr Urol. 2020;16(1):10–19. doi:10.1016/j.jpurol.2019.12.020
4. Pandey S, Oza H, Shah H, et al. Rate and risk factors of nocturnal enuresis in school going children. Ind Psychiatry J. 2019;28(2):306–311. doi:10.4103/ipj.ipj_15_18
5. Wang XZ, Wen YB, Shang XP, et al. The influence of delay elimination communication on the prevalence of primary nocturnal enuresis-a survey from Mainland China. Neurourol Urodyn. 2019;38(5):1423–1429. doi:10.1002/nau.24002
6. Sarici H, Telli O, Ozgur BC, et al. Prevalence of nocturnal enuresis and its influence on quality of life in school-aged children. J Pediatr Urol. 2016;12(3):159.e1–6. doi:10.1016/j.jpurol.2015.11.011
7. Fockema MW, Candy GP, Kruger D, et al. Enuresis in South African children: prevalence, associated factors and parental perception of treatment. BJU Int. 2012;110(11 Pt C):E1114–20. doi:10.1111/j.1464-410X.2012.11416.x
8. Baek M, Park K, Lee H-E, et al. A nationwide epidemiological study of nocturnal enuresis in Korean adolescents and adults: population based cross sectional study. J Korean Med Sci. 2013;28(7):1065–1070. doi:10.3346/jkms.2013.28.7.1065
9. Su MS, Xu L, Pan W-F, et al. Current perspectives on the correlation of nocturnal enuresis with obstructive sleep apnea in children. World J Pediatr. 2019;15(2):109–116. doi:10.1007/s12519-018-0199-6
10. Dang J, Tang Z. Pathogenesis and brain functional imaging in nocturnal enuresis: a review. Exp Biol Med (Maywood). 2021;246(13):1483–1490. doi:10.1177/1535370221997363
11. von Gontard A, Hussong J, Yang SS, et al. Neurodevelopmental disorders and incontinence in children and adolescents: attention-deficit/hyperactivity disorder, autism spectrum disorder, and intellectual disability-A consensus document of the International Children’s Continence Society. Neurourol Urodyn. 2022;41(1):102–114. doi:10.1002/nau.24798
12. Zhong S, Zhang L, Wang M, et al. Abnormal resting-state functional connectivity of hippocampal subregions in children with primary nocturnal enuresis. Front Psychiatry. 2022;13:966362. doi:10.3389/fpsyt.2022.966362
13. Sinha R, Raut S. Management of nocturnal enuresis - myths and facts. World J Nephrol. 2016;5(4):328–338. doi:10.5527/wjn.v5.i4.328
14. Kaditis AG, Alonso Alvarez ML, Boudewyns A, et al. Obstructive sleep disordered breathing in 2- to 18-year-old children: diagnosis and management. Eur Respir J. 2016;47(1):69–94. doi:10.1183/13993003.00385-2015
15. Choong WY, Teh KW, Lau MN, et al. A multicenter study on the prevalence of adults and children seeking orthodontic treatment at high risk of obstructive sleep apnea. Cranio. 2023;41(4):340–347. doi:10.1080/08869634.2022.2043023
16. Brouilette R, Hanson D, David R, et al. A diagnostic approach to suspected obstructive sleep apnea in children. J Pediatr. 1984;105(1):10–14. doi:10.1016/S0022-3476(84)80348-0
17. Sirimongkolchaiyakul O, Sutheparank C, Amornchaicharoensuk Y. The Prevalence of Nocturnal Enuresis in Bangkok, Thailand: a Descriptive and Questionnaire Survey of 5 to 15 Year-Old School Students. Glob Pediatr Health. 2023;10:2333794x231189675. doi:10.1177/2333794X231189675
18. Carotenuto M, Esposito M, Pascotto A. Facial patterns and primary nocturnal enuresis in children. Sleep Breath. 2011;15(2):221–227. doi:10.1007/s11325-010-0388-6
19. Vijaya G, Digesu GA, Derpapas A, et al. Changes in detrusor muscle oxygenation during detrusor overactivity contractions. Eur J Obstet Gynecol Reprod Biol. 2012;163(1):104–107. doi:10.1016/j.ejogrb.2012.03.030
20. Nevéus T, et al. Respiration during sleep in children with therapy-resistant enuresis. Acta Paediatr. 2014;103(3):300–304. doi:10.1111/apa.12515
21. Shafiek H, Evangelisti M, Abd-elwahab NH, et al. Obstructive Sleep Apnea in School-Aged Children Presented with Nocturnal Enuresis. Lung. 2020;198(1):187–194. doi:10.1007/s00408-019-00304-6
22. El-Mitwalli A, Bediwy AS, Zaher AA, et al. Sleep apnea in children with refractory monosymptomatic nocturnal enuresis. Nat Sci Sleep. 2014;6:37–42. doi:10.2147/NSS.S59317
23. Soylu Özler G, Özler S. Coexistence of Upper Airway Obstruction and Primary and Secondary Enuresis Nocturna in Children and the Effect of Surgical Treatment for the Resolution of Enuresis Nocturna. Adv Med. 2014;2014:656431. doi:10.1155/2014/656431
24. Wang RC, Elkins TP, Keech D, et al. Accuracy of clinical evaluation in pediatric obstructive sleep apnea. Otolaryngol Head Neck Surg. 1998;118(1):69–73. doi:10.1016/S0194-5998(98)70377-8
25. Ferrara P, Cammisa I, Zona M, et al. Do Sleep Disorders Influence the Prognosis and the Response to the Therapy in Enuretic Children? Urology Research and Practice. 2023;49(1):59–62. doi:10.5152/tud.2023.21356
26. Fernandes AER, Roveda JRC, Fernandes CR, et al. Relationship between nocturnal enuresis and sleep in children and adolescents. Pediatr Nephrol. 2023;38(5):1427–1438. doi:10.1007/s00467-022-05818-5
27. Nascimento Fagundes S, Azevedo Soster L, Lebl AS, et al. Impact of a multidisciplinary evaluation in pediatric patients with nocturnal monosymptomatic enuresis. Pediatr Nephrol. 2016;31(8):1295–1303. doi:10.1007/s00467-016-3316-6
28. Alshehri AA, Zaki MSH, Nour SO, et al. Sleep-Disordered Breathing and Its Association with Nocturnal Enuresis at the Primary Schools in Saudi Arabia: a Cross-Sectional Study. Children. 2023;10(6):1074 doi:10.3390/children10061074.
29. Jeyakumar A, Rahman SI, Armbrecht ES, et al. The association between sleep-disordered breathing and enuresis in children. Laryngoscope. 2012;122(8):1873–1877. doi:10.1002/lary.23323
30. Bascom A, Penney T, Metcalfe M, et al. High risk of sleep disordered breathing in the enuresis population. J Urol. 2011;186(4 Suppl):1710–1713. doi:10.1016/j.juro.2011.04.017
31. Sakellaropoulou AV, Hatzistilianou MN, Emporiadou MN, et al. Association between primary nocturnal enuresis and habitual snoring in children with obstructive sleep apnoea-hypopnoea syndrome. Arch Med Sci. 2012;3(3):521–527. doi:10.5114/aoms.2012.28809
32. Banhara FL, Trindade IEK, Trindade-Suedam IK, et al. Respiratory sleep disorders, nasal obstruction and enuresis in children with non-syndromic Pierre Robin sequence. Braz J Otorhinolaryngol. 2022;88(Suppl 1):S133–s141. doi:10.1016/j.bjorl.2021.05.002
33. Wolfe-Christensen C, Kovacevic LG, Abdulhamid I, et al. Comorbid monosymptomatic nocturnal enuresis and snoring exhibit an additive effect on impairments in health-related quality of life. J Pediatr Urol. 2019;15(6):643.e1–643.e5. doi:10.1016/j.jpurol.2019.08.014
34. Wolfe-Christensen C, Kovacevic LG, Mirkovic J, et al. Lower health related quality of life and psychosocial difficulties in children with monosymptomatic nocturnal enuresis--is snoring a marker of severity? J Urol. 2013;190(4 Suppl):1501–1504. doi:10.1016/j.juro.2013.01.060
35. Eray Ş, Tekcan D, Baran Y. More anxious or more shy? Examining the social anxiety levels of adolescents with primary enuresis nocturna: a controlled study. J Pediatr Urol. 2019;15(4):343.e1–343.e5. doi:10.1016/j.jpurol.2019.04.002
36. Garbarino S, Bardwell WA, Guglielmi O, et al. Association of Anxiety and Depression in Obstructive Sleep Apnea Patients: a Systematic Review and Meta-Analysis. Behav Sleep Med. 2020;18(1):35–57. doi:10.1080/15402002.2018.1545649
37. Snow A, Vazifedan T, Baldassari CM. Evaluation of Nocturnal Enuresis After Adenotonsillectomy in Children With Obstructive Sleep Apnea: a Secondary Analysis of a Randomized Clinical Trial. JAMA Otolaryngol Head Neck Surg. 2021;147(10):887–892. doi:10.1001/jamaoto.2021.2303
38. Balaban M, Aktas A, Sevinc C, et al. The relationship of enuresis nocturna and adenoid hypertrophy. Arch Ital Urol Androl. 2016;88(2):111–114. doi:10.4081/aiua.2016.2.111
39. Wada H, Kimura M, Tajima T, et al. Nocturnal enuresis and sleep disordered breathing in primary school children: potential implications. Pediatr Pulmonol. 2018;53(11):1541–1548. doi:10.1002/ppul.24156
40. Rittig S, Knudsen UB, Nørgaard JP, et al. Diurnal variation of plasma atrial natriuretic peptide in normals and patients with enuresis nocturna. Scand J Clin Lab Invest. 1991;51(2):209–217. doi:10.1080/00365519109091109
41. Ribeiro A, Bastos Netto JM, Figueiredo AAD, et al. Enuresis and upper airway obstruction: BNP and ADH hormones behavior before and after airway surgery. Int Braz J Urol. 2022;48(6):937–943. doi:10.1590/s1677-5538.ibju.2022.0313
42. Zhang A, Li S, Zhang Y, et al. Nocturnal enuresis in obese children: a nation-wide epidemiological study from China. Sci Rep. 2019;9(1):8414. doi:10.1038/s41598-019-44532-5
43. Kovacevic L, Wolfe-Christensen C, Lu H, et al. Why does adenotonsillectomy not correct enuresis in all children with sleep disordered breathing? J Urol. 2014;191(5 Suppl):1592–1596. doi:10.1016/j.juro.2013.10.032
44. Ding H, Wang M, Hu K, et al. Adenotonsillectomy can decrease enuresis and sympathetic nervous activity in children with obstructive sleep apnea syndrome. J Pediatr Urol. 2017;13(1):41.e1–41.e8. doi:10.1016/j.jpurol.2016.10.009
45. Angeli M, Bitsori M, Rouva G, et al. The role of the autonomic nervous system in nocturnal enuresis. J Pediatr Urol. 2023;19(1):6–18. doi:10.1016/j.jpurol.2022.10.015
46. Sun C, Xu Y, Luo C, et al. Relationship between enuresis and obstructive sleep apnea-hypopnea syndrome in children. J Int Med Res. 2020;48(12):300060520977407. doi:10.1177/0300060520977407
47. Breinbjerg A, Jørgensen CS, Borg B, et al. The genetics of incontinence: a scoping review. Clin Genet. 2023;104(1):22–62. doi:10.1111/cge.14331
48. Boesen EI. Endothelin receptors, renal effects and blood pressure. Curr Opin Pharmacol. 2015;21:25–34. doi:10.1016/j.coph.2014.12.007
49. Rossi NF. Regulation of vasopressin secretion by ETA and ETB receptors in compartmentalized rat hypothalamo-neurohypophysial explants. Am J Physiol Endocrinol Metab. 2004;286(4):E535–41. doi:10.1152/ajpendo.00344.2003
50. Martenstyn JA, Machaalani R, Caldwell P, et al. Relationship between sleep respiration, architecture and childhood enuresis: correlates between polysomnography and questionnaire. J Paediatr Child Health. 2021;57(12):1923–1928. doi:10.1111/jpc.15613
51. Wolfish NM, Pivik RT, Busby KA. Elevated sleep arousal thresholds in enuretic boys: clinical implications. Acta Paediatr. 1997;86(4):381–384. doi:10.1111/j.1651-2227.1997.tb09027.x
52. Liguori C, Placidi F, Palmieri MG, et al. Continuous Positive Airway Pressure Treatment May Improve Optic Nerve Function in Obstructive Sleep Apnea: an Electrophysiological Study. J Clin Sleep Med. 2018;14(6):953–958. doi:10.5664/jcsm.7158
53. Morrison C, Mussad A, Cunnington P, et al. Diagnosis and perioperative management in pediatric sleep-disordered breathing. Paediatr Anaesth. 2019;29(3):291–292. doi:10.1111/pan.13584
54. Arai H, Furuta H, Kosaka K, et al. Polysomnographic and urodynamic changes in a case of obstructive sleep apnea syndrome with enuresis. Psychiatry Clin Neurosci. 1999;53(2):319–320. doi:10.1046/j.1440-1819.1999.00550.x
55. Watanabe H, Kawauchi A, Kitamori T, et al. Treatment System for Nocturnal Enuresis according to an Original Classification System. Eur Urol. 1994;25(1):43–50. doi:10.1159/000475246
56. Jönson Ring I, Markström A, Bazargani F, et al. Sleep disordered breathing in enuretic children and controls. J Pediatr Urol. 2017;13(6):620.e1–620.e6. doi:10.1016/j.jpurol.2017.05.012
57. Ferrara P, Fabrizio GC, Franco D, et al. Association among nocturnal enuresis, body weight and obstructive sleep apnea in children of south Italy: an observational study. Minerva Pediatr. 2019;71(6):511–514. doi:10.23736/S0026-4946.16.04497-2
58. Demirbas A, Gercek HG. The effect of screen time on the presentation and treatment of primary monosymptomatic nocturnal enuresis. BMC Urol. 2023;23(1):22. doi:10.1186/s12894-023-01184-y
59. Ma Y, Shen Y, Liu X. Association between enuresis and obesity in children with primary monosymptomatic nocturnal enuresis. Int Braz J Urol. 2019;45(4):790–797. doi:10.1590/s1677-5538.ibju.2018.0603
60. Gozal D. C-reactive protein and obstructive sleep apnea syndrome in children. Front Biosci. 2012;E4(7):2410–2422. doi:10.2741/e553
61. Gaines J, Vgontzas AN, Fernandez-Mendoza J, et al. Increased inflammation from childhood to adolescence predicts sleep apnea in boys: a preliminary study. Brain Behav Immun. 2017;64:259–265. doi:10.1016/j.bbi.2017.04.011
62. Tsai JD, Chen H-J, Ku M-S, et al. Association between allergic disease, sleep-disordered breathing, and childhood nocturnal enuresis: a population-based case-control study. Pediatr Nephrol. 2017;32(12):2293–2301. doi:10.1007/s00467-017-3750-0
63. Wang H, Goodman MO, Sofer T, et al. Cutting the fat: advances and challenges in sleep apnoea genetics. Eur Respir J. 2021;57(5):2004644. doi:10.1183/13993003.04644-2020
64. Graham KM, Levy JB. Enuresis. Pediatr Rev. 2009;30(5):165–72;quiz173. doi:10.1542/pir.30.5.165
65. Singh M, Hanis CL, Redline S, et al. Sleep apnea and galectin-3: possible sex-specific relationship. Sleep and Breathing. 2019;23(4):1107–1114. doi:10.1007/s11325-019-01788-5
66. O’Driscoll DM, Foster AM, Davey MJ, et al. Can actigraphy measure sleep fragmentation in children? Arch Dis Child. 2010;95(12):1031–1033. doi:10.1136/adc.2009.166561
67. Umlauf MG, Chasens ER. Bedwetting--not always what it seems: a sign of sleep-disordered breathing in children. J Spec Pediatr Nurs. 2003;8(1):22–30. doi:10.1111/j.1744-6155.2003.tb00180.x
68. Tsampalieros A, Blinder H, Hoey L, et al. Obstructive sleep apnea and hypertension in pediatric chronic kidney disease. Pediatr Nephrol. 2019;34(11):2361–2370. doi:10.1007/s00467-019-04295-7
69. Kumar S, Goyal A, Atlani M, et al. Obstructive sleep apnea and ambulatory blood pressure abnormalities in children with chronic kidney disease. Blood Press Monit. 2023;28(3):129–133. doi:10.1097/MBP.0000000000000642
70. Simmons FB, Guilleminault C, Dement WC, et al. Surgical management of airway obstructions during sleep. Laryngoscope. 1977;87(3):326–338. doi:10.1288/00005537-197703000-00005
71. Kaya KS, Türk B, Erol ZN, et al. Pre- and post-operative evaluation of the frequency of nocturnal enuresis and Modified Pediatric Epworth Scale in pediatric obstructive sleep apnea patients. Int J Pediatr Otorhinolaryngol. 2018;105:36–39. doi:10.1016/j.ijporl.2017.11.033
72. Ahmadi MS, Amirhassani S, Poorolajal J. The effect of adenotonsillectomy on pediatric nocturnal enuresis: a prospective cohort study. Iran J Otorhinolaryngol. 2013;25(70):37–40.
73. Kovacevic L, Jurewicz M, Dabaja A, et al. Enuretic children with obstructive sleep apnea syndrome: should they see otolaryngology first? J Pediatr Urol. 2013;9(2):145–150. doi:10.1016/j.jpurol.2011.12.013
74. Park S, Lee JM, Sim CS, et al. Impact of adenotonsillectomy on nocturnal enuresis in children with sleep-disordered breathing: a prospective study. Laryngoscope. 2016;126(5):1241–1245. doi:10.1002/lary.25934
75. Andreu-Codina M, Nikolic-Jovanovic D, Esteller E, et al. The Relationship between Nocturnal Enuresis and Obstructive Sleep Apnea in Children. Children (Basel). 2024;11(9). doi:10.3390/children11091148.
76. Waleed FE, Samia AF, Samar MF. Impact of sleep-disordered breathing and its treatment on children with primary nocturnal enuresis. Swiss Med Wkly. 2011;141:w13216. doi:10.4414/smw.2011.13216
77. Kalorin CM, Mouzakes J, Gavin JP, et al. Tonsillectomy does not improve bedwetting: results of a prospective controlled trial. J Urol. 2010;184(6):2527–2531. doi:10.1016/j.juro.2010.08.040
78. Davaro F, Kaba A, Osei H, et al. Treatment of obstructive sleep apnea does not treat primary nocturnal enuresis. J Pediatr Urol. 2021;17(2):182.e1–182.e6. doi:10.1016/j.jpurol.2020.12.022
79. Ersu R, Chen ML, Ehsan Z, et al. Persistent obstructive sleep apnoea in children: treatment options and management considerations. Lancet Respir Med. 2023;11(3):283–296. doi:10.1016/S2213-2600(22)00262-4
80. Abdollohi-Fakhim S, Talebi A, Naghavi-Behzad M, et al. Effects of adenotonsillar hypertrophy corrective surgery on nocturnal enuresis of children. Niger Med J. 2016;57(1):69–73. doi:10.4103/0300-1652.180558
81. Kovacevic L, Lu H, Wolfe-Christensen C, et al. Adenotonsillectomy Normalizes Hormones and Urinary Electrolytes in Children With Nocturnal Enuresis and Sleep-Disordered Breathing. Urology. 2015;86(1):158–161. doi:10.1016/j.urology.2015.04.011
82. Wall E, Crew AD, Varkonyi PI. Continuous positive airway pressure breathing (CPAP). Apparatus for use in neonates or adults. Anaesthesia. 1975;30(1):67–72. doi:10.1111/j.1365-2044.1975.tb00798.x
83. Krieger J, Petiau C, Sforza E, et al. Nocturnal pollakiuria is a symptom of obstructive sleep apnea. Urol Int. 1993;50(2):93–97. doi:10.1159/000282460
84. Liu S, Liu L. [Effect of treatment with continuous positive airway pressure on nocturnal polyuria in patients with obstructive sleep apnea syndrome]. Zhonghua Jie He He Hu Xi Za Zhi. 2001;24(3):158–160. Danish
85. Miyauchi Y, Okazoe H, Okujyo M, et al. Effect of the continuous positive airway pressure on the nocturnal urine volume or night-time frequency in patients with obstructive sleep apnea syndrome. Urology. 2015;85(2):333–336. doi:10.1016/j.urology.2014.11.002
86. Miyazato M, Tohyama K, Touyama M, et al. Effect of continuous positive airway pressure on nocturnal urine production in patients with obstructive sleep apnea syndrome. Neurourol Urodyn. 2017;36(2):376–379. doi:10.1002/nau.22936
87. Wang T, Huang W, Zong H, et al. The Efficacy of Continuous Positive Airway Pressure Therapy on Nocturia in Patients With Obstructive Sleep Apnea: a Systematic Review and Meta-Analysis. Int Neurourol J. 2015;19(3):178–184. doi:10.5213/inj.2015.19.3.178
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.