")
Back to Journals » Journal of Pain Research » Volume 18
Repetitive Transcranial Magnetic Stimulation for the Treatment of Complex Regional Pain Syndrome: A Pilot Study
Authors Foglia SD , Drapeau CC, Ramdeo KR, Adams FC, Soppitt DB, Rehsi RS, Shanthanna H , Nelson AJ
Received 6 November 2024
Accepted for publication 24 December 2024
Published 20 January 2025 Volume 2025:18 Pages 367—377
DOI https://doi.org/10.2147/JPR.S496519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Stevie D Foglia,1 Chloe C Drapeau,2 Karishma R Ramdeo,2 Faith C Adams,2 Daniel B Soppitt,2 Ravjot S Rehsi,2 Harsha Shanthanna,1,3 Aimee J Nelson1,2
1School of Biomedical Engineering, McMaster University, Hamilton, ON, Canada; 2Department of Kinesiology, McMaster University, Hamilton, ON, Canada; 3Department of Anesthesia, McMaster University, Hamilton, ON, Canada
Correspondence: Aimee J Nelson, Department of Kinesiology, McMaster University, 1280 Main Street West, Hamilton, ON, L8S 4K1, Canada, Tel +1 905-525-9140 x28053, Fax +1 905-523-6011, Email [email protected]
Purpose: Complex regional pain syndrome (CRPS) is a debilitating chronic pain condition characterized by sensory, motor, and autonomic dysfunction with a world-wide prevalence of 26.2 per 100,000 people per year and is 3 to 4 times more prevalent in females. Repetitive transcranial magnetic stimulation (rTMS) has shown to be beneficial for pain relief in neuropathic pain and initial evidence in CRPS is promising, but studies are limited. The objective of this study was to investigate the feasibility of using rTMS in CRPS patients, to improve pain intensity and quality of life.
Patients and Methods: Six participants (5 lower limb, 1 upper limb, 42 ± 9 yr) took part in an open-label rTMS study comprised of a 9-week intervention and 6-month follow-up. Participants took part in a 4-week induction period (5 days per week) followed by a 5-week tapering period whereby the frequency of rTMS sessions per week was reduced. rTMS was delivered at 10 hz for 2000 pulses at 80% of resting motor threshold over the primary motor cortex. Feasibility was assessed as compliance of attending treatment sessions. Clinical outcomes included pain intensity using the numerical ratings scale, Pain Catastrophizing scale-EN-SF, PROMIS-29 v2.0 profile, and Rainbow Pain Scale.
Results: All participants tolerated the study procedures and 83% of participants completed the 9-week intervention, deeming the protocol feasible. At six months follow-up, data was obtained from 3 individuals. Exploratory analysis revealed a significant reduction in pain intensity (~20%) immediately following the intervention. Categorical improvements in allodynia were observed in four patients immediately following the intervention.
Conclusion: This study demonstrates that rTMS delivered over 9 weeks is feasible and well tolerated in individuals living with CRPS. However, there are challenges in collecting follow-up data for six months and appropriate measures must be taken in randomized controlled trials to ensure follow-up retention.
Keywords: complex regional pain syndrome, repetitive transcranial magnetic stimulation, neuromodulation, chronic pain, feasibility
Introduction
Complex regional pain syndrome (CRPS) is a chronic pain condition that is debilitating and dramatically decreases quality of life. CRPS is characterized by a constellation of sensory, motor, and autonomic dysfunction.1 CRPS differs from other chronic pain conditions; neuropathic or generalized non-specific pain conditions; in that pain is associated with obvious and distinct alterations in sensory processing, sympathetic nervous involvement, and motor dysfunction. CRPS patients commonly present with allodynia whereby non-painful stimuli evoke a painful sensation. The worldwide incidence of CRPS is 26.2 per 100,000 people per year2 and is 3 to 4 times more prevalent in females.2 Options for medical management of CRPS include medications such as opioids, anticonvulsants, antidepressants, and procedures such as sympathetic blockade and invasive spinal cord stimulation.3 However, evidence for these treatments come from medium to low quality randomized controlled trials (RCT).4 At present, CRPS is managed through continued physiotherapy with supportive treatment for pain and mental health.5
Neuroplasticity refers to the ability of the brain and/or spinal cord to change, either through structural reorganization or functional changes in brain activity.6 Neuroplasticity can be induced non-invasively with a form of brain stimulation known as repetitive transcranial magnetic stimulation (rTMS). rTMS applied to the primary motor cortex (M1) reduces symptoms of neuropathic pain in heterogenous groups of patients as shown in sham-controlled studies7 and meta-analyses.8 Our lab demonstrated that rTMS is effective at alleviating electric shock-like pain in an individual with neuropathic pain following spinal cord injury.9 Evidence-based guidelines have supported the use of rTMS as an analgesic tool for chronic pain.10,11 Smaller studies also indicate that rTMS may be effective for pain relief in peripheral neuropathy (PN)12,13 and meta-analysis has demonstrated the benefits of rTMS in pain and quality of life in fibromyalgia.14 For CRPS, data is limited, but initial studies demonstrate that rTMS delivered over M1 is effective at reducing pain by 20–50%.15–19 One study investigating the long-term analgesic effects of 10 sessions of 10 hz rTMS in CRPS found no change in pain at 3 months relative to baseline despite seeing a significant decrease in pain immediately following the intervention.17 To date, one meta-analysis has been performed using rTMS in CRPS.20 The authors conclude that rTMS is a good treatment option for patients with CRPS but acknowledged the lack of and need for a sham controlled RCT in the CRPS literature.20 Importantly, most studies in CRPS used very few stimulation sessions and overall, questions remain regarding the longevity of rTMS induced analgesia in CRPS. Long-term therapeutic effectiveness may be positively reinforced by a gradual tapering of the rTMS treatment over time rather than abruptly stopping after the treatment sessions.7 It is important to test the feasibility of longer rTMS trials aimed at improving the longevity of analgesia in CRPS and patient follow-ups post intervention are needed prior to proceeding to a randomized controlled trial (RCT).
The objective of this pilot study is to investigate the feasibility and tolerability of a 9-week rTMS intervention (including a treatment and tapering phase) in CRPS, to improve pain intensity and quality of life. The intervention used in this study is relatively intense, delivering 25 rTMS sessions in a 9-week period. We hypothesize that 9-weeks of rTMS will produce significant reductions in pain intensity. This work is performed in preparation for a larger RCT, and to establish treatment parameters that are feasible and demonstrate effectiveness.
Materials and Methods
Participants
Six participants (5 lower, 1 upper limb, 42 ± 9 yr) took part in an open-label rTMS pilot study. The presence of CRPS type 1 or type 2 was confirmed by a pain specialist and coauthor (H.S) using the modified Budapest Criteria.21 Pain was defined as neuropathic in nature based on the Douleur Neuropathique en 4 questions (DN4).22 All participants were screened for contraindications to TMS, including the presence of head injury or head surgery, metal implants, history of neurological disease or psychiatric illness, blood relatives with history of seizure, presence of headaches or migraines, and sleep deprivation. All participants maintained their current medications and treatments throughout the duration of the experiment. This study was approved by the Hamilton Integrated Research Ethics Board (#14029) this study complies with the Declaration of Helsinki. Written informed consent was obtained from study participants prior to study commencement for their participation in the study in addition to the publication of this manuscript. This study was registered with clinical trials (NCT05197959) with trial period 01/01/23 to 08/01/24.
Intervention
This was an open-label study involving a 9-week intervention comprised of an induction and tapering period (Figure 1). The induction period consisted of 5 sessions per week of rTMS for 4 weeks (20 sessions total). The tapering period involved 5 sessions of rTMS delivered over 5 weeks (week 1 = 2 sessions, weeks 2 and 3 = 1 session, week 4 = no session, and week 5 = 1 session). There was no session in week 4 to extend the time between sessions. Assessments occurred at baseline (T0), immediately following the induction (T1) and tapering phases (T2), and at one month (F1), three months (F3) and six months (F6) post rTMS. Assessments at T0-T2 were performed at our laboratory at McMaster University while all follow-up assessments were performed virtually.
 |
Figure 1 Experimental timeline. *Indicates the number of experimental sessions per week. N indicates the number of participants that took part in each time period of the study. |
TMS Procedure
rTMS was delivered using a Magstim Rapid 2 stimulator (Magstim, Whitland, UK) over the primary motor cortex. For the individual with CRPS affecting the upper limb, rTMS was delivered over M1 contralateral to the affected upper limb16,23 over the hand representation.8 For participants with lower limb CRPS, rTMS was applied to the vertex (Cz) over the presumed leg representation of the motor cortex.16 Cz was determined using the international 10–20 measurement system. Cortical targets corresponding to the hand and leg representation were digitally registered using Brainsight Neuronavigation software (Rogue Research, Montreal) to ensure accurate delivery of rTMS across sessions. For each session (induction and tapering), rTMS was delivered at 10 hz stimulation frequency for 167 trains for a duration of 1.2s for each train (12 pulses per train) with a 3s inter-train interval for 2004 pulses.9 The intervention took ~11.5 minutes. rTMS was set at an intensity of 80% resting motor threshold (RMT) obtained in the right abductor pollicis brevis (APB) muscle of the dominant hand,23 and this was the case for both lower and upper limb participants. RMT was taken as a measure of baseline cortical excitability24 and was determined using TMS_MTAT_2.0 freeware (http://clinicalresearcher.org/software.htm). The stimulus intensity was set to 37% of the maximum stimulator output (MSO) and twenty TMS pulses were delivered over the APB hotspot to accurately determine the RMT.9 RMT was checked at the beginning of each rTMS session. rTMS was delivered by author S.D.F.
Electromyography Recording
Surface bipolar EMG electrodes were positioned on the skin overlying the right APB muscle. EMG signals were amplified x1000 and filtered from 20 to 2500 Hz (Intronix Model 2024F; Intronix Technologies Corporation, Bolton, Canada). EMG data were acquired using a Cambridge Electronic Device (Power 1401; Cambridge Electronic Design, Cambridge, UK) and visualized using Signal software (Cambridge Electronic Design).
Outcomes
Feasibility
The feasibility of this study will be related to participant compliance of sessions. Compliance of sessions is defined as a minimum of attending 3 sessions per week for 4 weeks (induction) and 5 session over 5-weeks (tapering). We will consider the study feasible if greater than 80% adhere to the intervention (induction and tapering).
Clinical Outcomes
The outcomes of this study followed the Core Outcome Measures for Complex Regional PAin Syndrome Clinical sTudies (COMPACT) recommendations.25 These included self-perceived pain intensity, Patient-Reported Outcomes Measurement Information System 29-Item Profile (PROMIS-29 v2.0), Pain Catastrophizing scale-EN-SF and Rainbow Pain Scale. Pain intensity was rated using the 0–10 Numerical Rating Scale (NRS) and was the primary clinical outcome of this study. PROMIS-29 v2.0 uses the numerical rating (0 to 5) to assess seven health domains including physical function, anxiety, depression, fatigue, sleep disturbances, ability to participate in social roles and activities, and pain interference.26 The Rainbow Pain Scale was used to measure the severity of allodynia type pain using sensory assessments of the affected limb.27 Pain intensity, pain catastrophizing, and PROMIS-29 v2.0 were assessed at T0 to F6. The Rainbow Pain Scale was assessed at T0, T1, and T2 as these sessions were in person, follow-up assessments were completed virtually, and the Rainbow Pain Scale was not performed at the follow-up time points.
Statistical Analysis
Although this study was not powered, analyses were performed on the primary clinical outcome, pain intensity, to investigate the effectiveness of the rTMS intervention. This analysis is to investigate initial potential effectiveness of rTMS before moving to a larger RCT. Normality for pain intensity was assessed using Shapiro–Wilks test. Nonparametric tests were performed on the pain intensity data, specifically a Friedman’s One-Way ANOVA was used to assess changes in pain intensity with a factor of TIME (three levels: T0, T1, T2). SPSS software was used for all statistical analysis (IBM). Due to participant retention during the follow-up period, formal statistical analysis was not applied to the follow-up period data. No formal statistical analysis was applied to Pain Catastrophizing Scale. No analysis was applied to the Rainbow Pain Scale as this outcome is categorical. Similarly, PROMIS-29 v2.0 outcomes are rated in relation to normalized healthy population using T scores to determine the severity of each health domain.21 As such, statistical analysis was not applied on this data.
Results
Participant Characteristics
Participant characteristics are detailed in Table 1. Pain at baseline ranged from 7 to 10 across participants using the numerical rating scale. All participants reported suboptimal (unsatisfactory control) of pain management despite ongoing therapy.
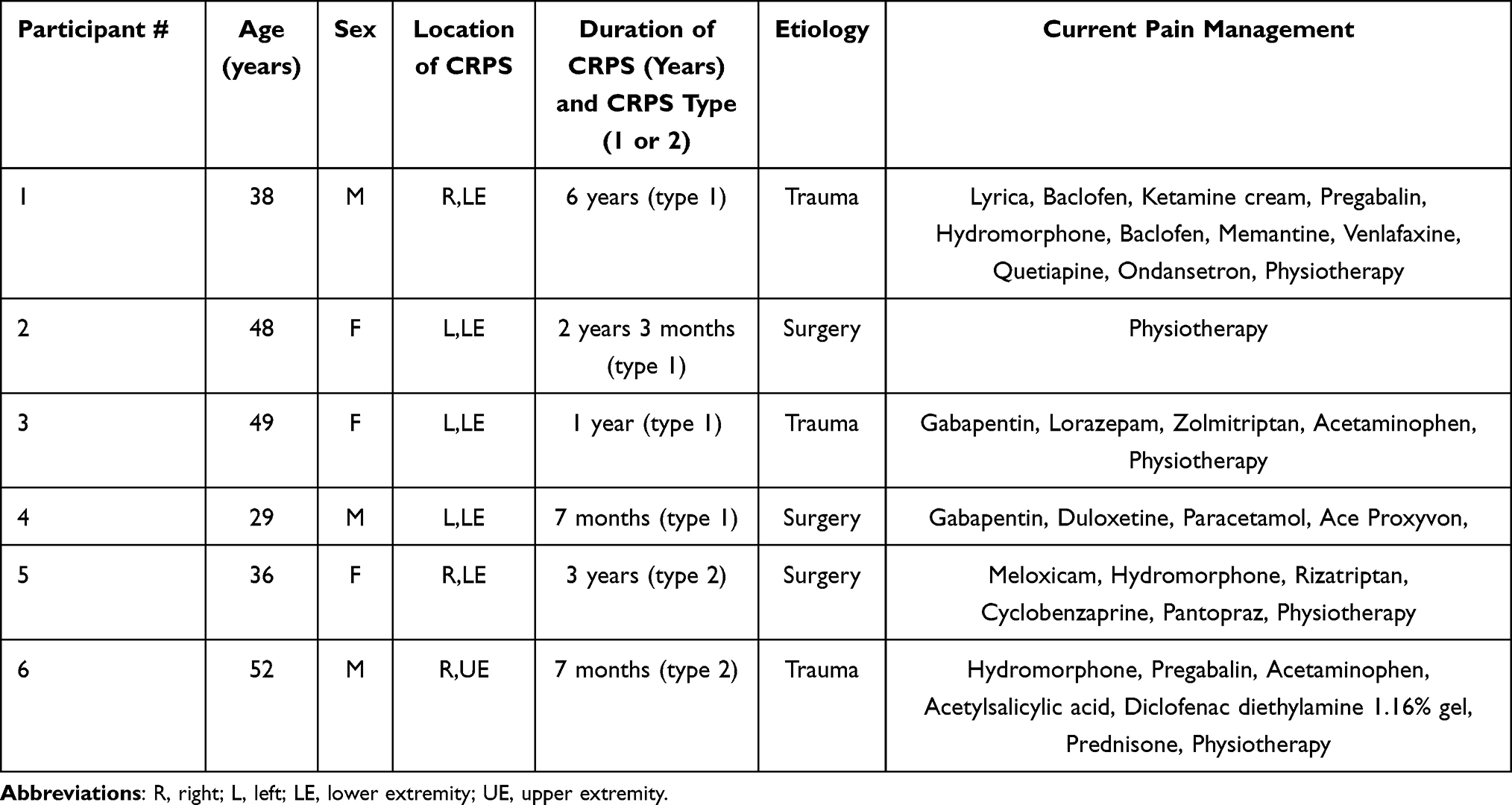 |
Table 1 Participant Characterization |
Feasibility of rTMS Treatment Protocol and Follow-Up
All participants tolerated the study procedures and no adverse events occurred. One participant withdrew from the study following the induction phase due to the opportunity to receive Ketamine infusion at a local hospital. As such, 83% of participants completed the rTMS intervention (induction and tapering). All participants completed 5 sessions per week during the induction period, which was the maximum permitted in this study. At six months follow-up, data was obtained from 3 individuals (Figure 1). Participant feedback indicated the preference to reduce the number of follow-ups which we now propose.
Clinical Outcomes
For pain intensity, ANOVA revealed a significant effect of TIME (X2(2) = 7.54, p = 0.023), such that there was a significant reduction in pain intensity from T0 (8.3 ± 1.2) to T1 (6.8 ± 1.5, p = 0.034). There was no significant reduction in pain at T2 (6.6 ± 1.5, p = 0.059) relative to T0 (Figure 2). Note that one participant left the study before T2 data could be acquired due to an opportunity to receive ketamine infusion. Qualitatively, at six months follow-up, there was no change in NRS relative to baseline, however data from only three participants is available at this time point. For pain catastrophizing, there was a ~16% decrease immediately following the intervention and ~7% decrease at 6 months post intervention (Figure 3).
 |
Figure 2 Pain intensity. Changes in pain intensity across the study. Average pain intensity is illustrated in red. N indicates the number of participants that took part in each time period of the study. |
 |
Figure 3 Pain catastrophizing. Changes in pain catastrophizing across the study. Average pain catastrophizing is illustrated in red. N indicates the number of participants that took part in each time period of the study. |
Changes in PROMIS-29 v2.0 profile are presented in Figure 4. There was a reduction in pain interference from category severe to moderate immediately following the tapering period that persisted at the 1-month follow-up. Sleep disturbance was reduced from category severe to moderate immediately following the induction period that persisted to the end of the tapering period. Physical function was improved from category severe to moderate immediately following the induction period and persisted to 6-month follow-up. There were no changes in depression, anxiety, fatigue, and ability to participate in social roles and activities.
 |
Figure 4 PROMIS-29 v2.0 profile. Outcomes are reported relative to the reference population using T-scores. T-score values are rated as within normal limits, mild, moderate, and severe. N indicates the number of participants that took part in each time period of the study. |
Changes in rainbow pain scale are illustrated in Figure 5. Overall, 4 of the 5 participants with allodynia demonstrated categorical improvement in allodynia of the affected limb. There was no categorical change in P01. There was an abolishment of allodynia type pain in P02 following the tapering period on the dorsal aspect of the foot, as well as at medial plantar, lateral plantar, and saphenous nerve dermatomes immediately following the tapering period. There was a categorical change from serious to significant in P03 on the dorsal side of the foot as well as at the lateral plantar and saphenous nerve dermatomes and change to discrete at the medial plantar dermatome immediately following the tapering period. P04 demonstrated a categorical change from serious to discrete at the plantar side of the foot immediately following the tapering period. There was also a categorical worsening from significant to serious at the lateral plantar, saphenous nerve, tibial nerve, and sural nerve dermatomes immediately following the tapering period. In P05, there was a categorical shift from serious to significant in the lateral plantar, saphenous nerve, and tibial nerve dermatomes immediately following the tapering period. P06 did not present with allodynia, and the rainbow pain scale was not applied to this participant.
 |
Figure 5 Rainbow pain scale of allodynia. Colours represent the severity of allodynia type pain measured on the dorsal and plantar side of the foot. Each area of the foot was divided based on its dermatome, tibial nerve (TN), sural nerve (S), saphenous nerve (SN), medial plantar (MP), lateral plantar (LP), and superficial peroneal (SP). No colour indicates no pain was elicited in that area. Only the affected foot for each participant is illustrated. |
Discussion
This pilot study describes the feasibility, tolerability, and use of rTMS to improve pain and quality of life in 6 individuals with CRPS. The 9-week intervention was deemed to be feasible and tolerable as 83% of individuals successfully completed the intervention. Nine weeks of 10 hz rTMS indicated the potential to reduce pain intensity by ~20%. Pain intensity was significantly reduced following the induction phase (4 weeks of stimulation). We observed a positive categorical shift in allodynia, pain interference, sleep disturbance, and physical function. We discuss these findings and their putative neural mechanisms below.
This study was the first to employ a 9-week rTMS intervention in CRPS which exceeds the 1–10 sessions of rTMS used in most reports in CRPS.17 We note that 5 of 6 participants completed the intervention, indicating that the protocol is tolerated and feasible. Importantly, unique to the protocol is the tapering phase whereby rTMS sessions are reduced in frequency. Previous reports demonstrated the benefit of tapering phases in longevity of analgesia in neuropathic pain.7 Prior to embarking on a larger RCT in CRPS, this study aimed to first determine if this length of protocol is feasible and tolerated within this population. Importantly, the intervention used was relatively intense, delivering 25 rTMS sessions in a 9-week period.
Pain intensity was significantly reduced following the induction phase and reached near significant reduction following the tapering phase. The magnitude of reduction in pain was ~20% similar to the ~22% reduction in pain reported by Delon-Martin.15 Similarly, Gaertner16 report pain relief > 30% at one-week post-stimulation following 10 hz rTMS delivered to motor cortex for one (n=5) or five (n=12) days in individuals with CRPS. Rizzuto,19 in a case report, reported a 30% reduction in pain intensity at one week following 20 sessions of rTMS over 3 weeks. Picarelli17 observed a 51% reduction in pain intensity following 10 sessions of 10 hz rTMS over motor cortex while those experiencing sham indicated a 25% decrease. Importantly, all participants were washed-out of their previous therapies and tried a standard medical and physiotherapy treatment prior to beginning rTMS.17 Collectively, the present and aforementioned studies indicate that 10 hz rTMS reduces pain intensity by 20–50%.
The mechanisms that underpin the reduction in pain following rTMS are not clearly understood. Analgesic effects of rTMS are suggested to be a result of modulation of nociceptive inhibitory circuits from stimulation of M1.28 This stimulation may cause changes in glutamatergic or GABAergic neurotransmitter pathways leading to a suppression of pain sensation.28,29 Patients with CRPS display abnormal processing of pain in brain, spinal cord, and nerves with deficiencies in inhibition of pain. Further, there is evidence of aberrant neuronal circuitry between different segments of the sensory cortex, basal ganglia, prefrontal cortex, and insula.30 Recently, it has been suggested that analgesic effects of rTMS occurs through opioidergic process whereby rTMS delivered to M1 activates the endogenous opioid system.31
One of the most crucial findings of the present study is the categorical improvement in allodynia of the affected limb in four participants. This distinguishes our study from other published studies where such detailed assessment and demonstration were not made. This is important as chronic pain studies look to establish improvements in subgroups of patients or certain characteristics of the clinical problem.32 In a recent case report, we showed that rTMS combined with sensorimotor training abolished allodynia of the hand and reduced it in the forearm from serious to significant in an individual with CRPS type 2 of the upper limb.33 Similarly, in an individual with brachial plexus injury, 10Hz rTMS applied to primary motor cortex abolished allodynia.34
There are several mechanisms that may underpin the reduction in allodynia following rTMS. First, increased activity in the posterior parietal cortex (PPC) has been suggested to underpin allodynia.35 rTMS over M1 may impact activity in PPC via direct and indirect pathways.36 Second, CPRS is associated with central sensitization37 defined as an increased responsiveness of nociceptive neurons in the central nervous system to subthreshold afferent inputs.38 As described above, rTMS may restore inhibitory control at the spinal level and reduce central sensitization.28 Last, CRPS is associated with sympathetic nervous involvement and upregulation of pro-inflammatory cytokines and down regulation of anti-inflammatory cytokines.39 Allodynia may be mediated by inflammation, as animal studies have indicated that antiepileptic calcium channel blockers such as gabapentin and nonsteroidal pro-inflammatory drugs slow the progression or prevent allodynia.40,41 We propose that rTMS may reduce allodynia through modulation of anti-inflammatory cytokines. Previous reports have demonstrated anti-inflammatory effects of rTMS in stroke and depression.42,43
Following rTMS, we observed categorical improvements in pain interference, sleep disturbance, and physical function. Such improvements may result from decreased pain intensity as 4 out of 5 individuals who experienced reductions in pain also experienced improvements in sleep quality. One study in CRPS has demonstrated decreased sleep restlessness when verum rTMS was delivered over the secondary somatosensory cortex, although pain intensity was not assessed.44 Our results differ from Picarelli17 where changes in pain impact questionnaire (PIQ-6) revealed no differences between Sham and Active rTMS.
Considerations
This was an open-label study that did not include a placebo arm, akin to most research in rTMS and CRPS. Individuals living with CRPS experience severe continuous pain and relief is an urgent medical need in these individuals. Therefore, we opted to provide all participants with real stimulation to offer everyone an equal opportunity to a potential therapeutic intervention. Further, our study was designed to assess individuals at 6 months following stimulation; however, only three participants remained in the study at the 6-month mark. Loss at six months follow-up was likely due to our assessment, which was performed virtually, and time managed by the participants themselves. It is likely that future studies should ensure follow-ups are performed in person to maintain commitment to the study.
Conclusion
In conclusion, this open-label pilot study demonstrates that 9-weeks of rTMS delivered over M1 is feasible and has the potential to decrease pain intensity, allodynia, pain interference, sleep disturbance, and improve physical function in individuals with CRPS. These data indicate that rTMS effects may persist up to three months following stimulation. Improvements in study methods and approaches are necessary to ensure follow-ups. Importantly, this study has a small sample size and did not include a sham control. Therefore, evidence from appropriately powered, large scale RCTs are required to establish the benefits of rTMS in CRPS.
Abbreviations
CRPS, complex regional pain; RCT, randomized controlled trials; rTMS, repetitive transcranial magnetic stimulation; syndrome; M1, primary motor cortex; EQUATOR, Enhancing the Quality and Transparency Of Health Research; DN4, Douleur Neuropathique en 4 questions; RMT, resting motor threshold; APB, abductor pollicis brevis; COMPACT, Core Outcome Measures for Complex Regional Pain Syndrome Clinical Studies; PROMIS-29 v2.0, Patient-Reported Outcomes Measurement Information System; NRS, Numerical Rating Scale; PPC, posterior parietal cortex; PIQ-6, pain impact questionnaire; TN, tibial nerve; S, sural nerve; SN, saphenous nerve; MP, medial plantar; LP, lateral plantar; SP, superficial peroneal.
Data Sharing Statement
Deidentified individual participant data will not be shared; however, group data (means) on all outcome measures included in this manuscript will be available upon Email request to the corresponding author Dr. Aimee Nelson. This data will be available for 10 years from the date of publication.
Acknowledgments
The study was supported by the Hamilton Academic Health Sciences Organization AFP Innovation Fund # 20019686.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Hamilton Academic Health Sciences Organization AFP Innovation Fund # 20019686.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gierthmühlen J, Binder A, Baron R. Mechanism-based treatment in complex regional pain syndromes. Nat Rev Neurol. 2014;10(9):518–528. doi:10.1038/nrneurol.2014.140
2. de Mos M, de Bruijn AGJ, Huygen FJPM, Dieleman JP, Stricker BHC, Sturkenboom MCJM. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007;129(1–2):12–20. doi:10.1016/j.pain.2006.09.008
3. Taylor RS, Van Buyten JP, Buchser E. Spinal cord stimulation for complex regional pain syndrome: a systematic review of the clinical and cost-effectiveness literature and assessment of prognostic factors. Eur J Pain. 2006;10(2):91–101. doi:10.1016/j.ejpain.2005.02.004
4. Bruehl S. Complex regional pain syndrome. BMJ. 2015;351:h2730. doi:10.1136/bmj.h2730
5. Goebel A, Barker C, Birklein F, et al. Standards for the diagnosis and management of complex regional pain syndrome: results of a European pain federation task force. Eur J Pain. 2019;23(4):641–651. doi:10.1002/ejp.1362
6. Hallett M. Transcranial magnetic stimulation: a primer. Neuron. 2007;55(2):187–199. doi:10.1016/j.neuron.2007.06.026
7. Attal N, Poindessous-Jazat F, De Chauvigny E, et al. Repetitive transcranial magnetic stimulation for neuropathic pain: a randomized multicentre sham-controlled trial. Brain. 2021;144(11):3328–3339. doi:10.1093/brain/awab208
8. Jiang X, Yan W, Wan R, et al. Effects of repetitive transcranial magnetic stimulation on neuropathic pain: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2022;132:130–141. doi:10.1016/j.neubiorev.2021.11.037
9. Foglia SD, Rehsi RS, Turco CV, Shanthanna H, Nelson AJ. Case report: the feasibility of rTMS with intrathecal baclofen pump for the treatment of unresolved neuropathic pain following spinal cord injury. Front Rehabilitation Sci. 2022;3. doi:10.3389/fresc.2022.893014
10. Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014–2018). Clin Neurophysiol. 2020;131(2):474–528. doi:10.1016/j.clinph.2019.11.002
11. Leung A, Shirvalkar P, Chen R, et al. Transcranial magnetic stimulation for pain, headache, and comorbid depression: INS-NANS expert consensus panel review and recommendation. Neuromodulation. 2020;23(3):267–290. doi:10.1111/ner.13094
12. Abdelkader AA, El Gohary AM, Mourad HS, El Salmawy DA. Repetitive TMS in treatment of resistant diabetic neuropathic pain. Egyptian J Neurol Psychiatr Neurosurg. 2019;55(1):30. doi:10.1186/s41983-019-0075-x
13. Yang S, Kwak SG, Choi GS, Chang MC. Short-term effect of repetitive transcranial magnetic stimulation on diabetic peripheral neuropathic pain. Pain Physician. 2022;25(2):E203–E209.
14. Cheng YC, Chen WY, Su MI, Tu YK, Chiu CC, Huang WL. Efficacy of neuromodulation on the treatment of fibromyalgia: a network meta-analysis. General Hospital Psychiatr. 2024;87:103–123. doi:10.1016/j.genhosppsych.2024.01.007
15. Delon-Martin C, Lefaucheur JP, Hodaj E, et al. Neural correlates of pain-autonomic coupling in patients with complex regional pain syndrome treated by repetitive transcranial magnetic stimulation of the motor cortex. Neuromodulation. 2024;27(1):188–199. doi:10.1016/j.neurom.2023.05.005
16. Gaertner M, Kong JT, Scherrer KH, Foote A, Mackey S, Johnson KA. Advancing transcranial magnetic stimulation methods for complex regional pain syndrome: an open-label study of paired theta burst and high-frequency stimulation. Neuromodulation. 2018;21(4):409–416. doi:10.1111/ner.12760
17. Picarelli H, Teixeira MJ, de Andrade DC, et al. Repetitive transcranial magnetic stimulation is efficacious as an add-on to pharmacological therapy in complex regional pain syndrome (CRPS) type I. J Pain. 2010;11(11):1203–1210. doi:10.1016/j.jpain.2010.02.006
18. Pleger B, Janssen F, Schwenkreis P, Völker B, Maier C, Tegenthoff M. Repetitive transcranial magnetic stimulation of the motor cortex attenuates pain perception in complex regional pain syndrome type I. Neurosci Lett. 2004;356(2):87–90. doi:10.1016/j.neulet.2003.11.037
19. Rizzuto CR, Garland JS, Kim CJ, et al. Utilizing repetitive transcranial magnetic stimulation (rTMS) to relieve pain associated with complex regional pain syndrome (CRPS) type II: a case report. Brain Stimul. 2021;14(5):1406. doi:10.1016/j.brs.2021.07.028
20. Chang MC, Kwak SG, Park D. The effect of rTMS in the management of pain associated with CRPS. Transl Neurosci. 2020;11(1):363–370. doi:10.1515/tnsci-2020-0120
21. Harden RN, Oaklander AL, Burton AW, et al. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 4th edition. Pain Med. 2013;14(2):180–229. doi:10.1111/pme.12033
22. Cruccu G, Truini A. Tools for assessing neuropathic pain. PLoS Med. 2009;6(4):e1000045. doi:10.1371/journal.pmed.1000045
23. Sun X, Long H, Zhao C, et al. Analgesia-enhancing effects of repetitive transcranial magnetic stimulation on neuropathic pain after spinal cord injury: An fNIRS study. Restorat Neurol Neurosci. 2019;37(5):497–507. doi:10.3233/RNN-190934
24. Siebner HR, Rothwell J. Transcranial magnetic stimulation: new insights into representational cortical plasticity. Exp Brain Res. 2003;148(1):1–16. doi:10.1007/s00221-002-1234-2
25. Grieve S, Perez RSGM, Birklein F, et al. Recommendations for a first core outcome measurement set for complex regional pain syndrome clinical sTudies (COMPACT). Pain. 2017;158(6):1083–1090. doi:10.1097/j.pain.0000000000000866
26. Ader DN. Developing the Patient-Reported Outcomes Measurement Information System (PROMIS). Med Care. 2007;45(5):S1. doi:10.1097/01.mlr.0000260537.45076.74
27. Packham TL, Spicher CJ, MacDermid JC, Quintal I, Buckley N. Evaluating a sensitive issue: reliability of a clinical evaluation for allodynia severity. Somatosens Mot Res. 2020;37(1):22–27. doi:10.1080/08990220.2019.1704242
28. Lefaucheur JP, Antal A, Ahdab R, et al. The use of repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) to relieve pain. Brain Stimul. 2008;1(4):337–344. doi:10.1016/j.brs.2008.07.003
29. Ciampi de Andrade D, Mhalla A, Adam F, Texeira MJ, Bouhassira D. Repetitive transcranial magnetic stimulation induced analgesia depends on N-methyl-D-aspartate glutamate receptors. Pain. 2014;155(3):598–605. doi:10.1016/j.pain.2013.12.022
30. Tangella AV. Imaging modalities and their findings in patients with complex regional pain syndrome: a review. Cureus. 2023;15(7):e41747. doi:10.7759/cureus.41747
31. de Andrade DC, Mhalla A, Adam F, Texeira MJ, Bouhassira D. Neuropharmacological basis of rTMS-induced analgesia: the role of endogenous opioids. PAIN. 2011;152(2):320. doi:10.1016/j.pain.2010.10.032
32. Fillingim RB, Loeser JD, Baron R, Edwards RR. Assessment of chronic pain: domains, methods, and mechanisms. J Pain. 2016;17(9 Suppl):T10–20. doi:10.1016/j.jpain.2015.08.010
33. Foglia S, Drapeau C, Rehsi R, Ramdeo K, Shanthanna H, Nelson A. Repetitive transcranial magnetic stimulation with sensorimotor training for the treatment of complex regional pain syndrome type 2 of the upper limb case report. A&A Pract. 2024;18(4):e01768. doi:10.1213/XAA.0000000000001768
34. Bertolucci F, Fanciullacci C, Rossi B, Chisari C. rTMS in the management of allodynia from brachial plexus injuries. Brain Stimul. 2013;6(2):218–219. doi:10.1016/j.brs.2012.03.016
35. Seifert F, Fuchs O, Nickel FT, et al. A functional magnetic resonance imaging navigated repetitive transcranial magnetic stimulation study of the posterior parietal cortex in normal pain and hyperalgesia. Neuroscience. 2010;170(2):670–677. doi:10.1016/j.neuroscience.2010.07.024
36. Koch G, Fernandez Del Olmo M, Cheeran B, et al. Focal stimulation of the posterior parietal cortex increases the excitability of the ipsilateral motor cortex. J Neurosci. 2007;27(25):6815–6822. doi:10.1523/JNEUROSCI.0598-07.2007
37. De Schoenmacker I, Mollo A, Scheuren PS, et al. Central sensitization in CRPS patients with widespread pain: a cross-sectional study. Pain Med. 2023;24(8):974–984. doi:10.1093/pm/pnad040
38. Terminology | International Association for the Study of Pain. International association for the study of pain (IASP). Available from: https://www.iasp-pain.org/resources/terminology/.
39. Schlereth T, Drummond PD, Birklein F. Inflammation in CRPS: role of the sympathetic supply. Auton Neurosci. 2014;182:102–107. doi:10.1016/j.autneu.2013.12.011
40. Salvat E, Yalcin I, Muller A, Barrot M. A comparison of early and late treatments on allodynia and its chronification in experimental neuropathic pain. Mol Pain. 2018;14:1744806917749683. doi:10.1177/1744806917749683
41. He Y, Kim PY. Allodynia. StatPearls. StatPearls Publishing; 2024. Available from: http://www.ncbi.nlm.nih.gov/books/NBK537129/.
42. Zhao X, Li Y, Tian Q, Zhu B, Zhao Z. Repetitive transcranial magnetic stimulation increases serum brain-derived neurotrophic factor and decreases interleukin-1β and tumor necrosis factor-α in elderly patients with refractory depression. J Int Med Res. 2019;47(5):1848–1855. doi:10.1177/0300060518817417
43. Cha B, Kim J, Kim JM, et al. Therapeutic effect of repetitive transcranial magnetic stimulation for post-stroke vascular cognitive impairment: a prospective pilot study. Front Neurol. 2022:13. doi:10.3389/fneur.2022.813597
44. Vanhanen J, Kujala J, Liljeström M, Kalso E, Virkkala J, Harno H. rTMS targeted to the secondary somatosensory cortex influences sleep in CRPS patients, as measured with the OURA ring. Brain Behav. 2023;13(11):e3252. doi:10.1002/brb3.3252
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.