")
Back to Journals » Journal of Pain Research » Volume 18
Research on the Developmental Trajectory of Movement-Evoked Pain and Its Potential Predictors in Patients After Knee Arthroplasty
Authors Ai S , Zhao S , Yan L, Hu H, Niu P , Zhu Y, Zheng M
Received 16 December 2024
Accepted for publication 12 April 2025
Published 21 April 2025 Volume 2025:18 Pages 2127—2136
DOI https://doi.org/10.2147/JPR.S510554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor King Hei Stanley Lam
Shanshan Ai,1,* Sumin Zhao,1,* Lihui Yan,1 Hangying Hu,1 Pengli Niu,2 Yueli Zhu,1,* Meifang Zheng1,*
1Department of Nursing, Integrated Traditional Chinese and Western Medicine of Linping District Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Nursing, The First Hospital of Dalian Medical University, Dalian, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yueli Zhu, Department of Nursing, Integrated Traditional Chinese and Western Medicine of Linping District Hospital, No. 15, Baojian Road, Linping District, Hangzhou, Zhejiang, 311100, People’s Republic of China, Tel +86 189 0681 1351, Email [email protected]
Purpose: This study aimed to investigate the developmental trajectory of movement-evoked pain after knee arthroplasty and analyze the predictors of different developmental trajectory categories.
Patients and Methods: In this study, a total of 178 patients undergoing knee arthroplasty were recruited from the Department of Joint Surgery at a tertiary care hospital in China. Participants completed the General Data Questionnaire, the Social Support Revaluated Scale, and the Pain Catastrophizing Scale on the day before surgery (T1). Movement-evoked pain was assessed using the Pain Numerical Rating Scale at 24 hours (T2), 48 hours (T3), and 72 hours (T4) after knee arthroplasty. The growth mixture model was utilized to identify the developmental trajectories of movement-evoked pain after knee arthroplasty.
Results: Three developmental trajectories of movement-evoked pain after knee arthroplasty were identified: the moderate pain—rise then decline group (47.75%), the moderate pain—continuous decline group (11.80%), and the severe pain—continuous stable group (40.45%). Multivariate logistic regression analysis indicated that social support, pain catastrophization, education, disease duration, and operation time were significant predictors of the types of movement-evoked pain in knee arthroplasty patients (P < 0.05).
Conclusion: This study identifies three potential categories of movement-evoked pain developmental trajectories after knee arthroplasty, with the moderate pain—rising then falling group being the most common. Significant predictors include social support, pain catastrophization, education, disease duration, and operation time.
Keywords: Development Trajectory, Knee Arthroplasty, Movement-evoked Pain, Pain
Introduction
According to a global epidemiological survey, the number of knee arthroplasties in China reached 1 million in 2019, and this trend is increasing annually.1 In the Netherlands, the number of knee arthroplasties is projected to rise by 297% by 2030 compared to 2005 figures.2 In the US, the number of knee arthroplasties is expected to increase by 673% from 2005, reaching approximately 3.48 million. This rising demand places significant pressure on global health resources.3
With advancements in modern medicine, there has been an increasing emphasis on patients’ quality of life and treatment satisfaction. Pain, recognized as the fifth vital sign alongside temperature, pulse, respiration, and blood pressure, is a crucial factor in this context.4 Notably, 44% of knee arthroplasty patients experience pain, with 15% suffering from severe pain postoperatively.5 While early functional exercise is essential for recovery and reducing postoperative complications, it can also lead to movement-evoked pain. This not only hinders the rehabilitation process but can also induce fear and potentially result in chronic pain and emotional disorders.6
Movement-evoked pain is triggered by both active and passive movement of the affected tissues.7 Passive limb movement after knee arthroplasty, initiated early in the postoperative period, has been shown to have better results in the recovery of mobility and function of knee joints.8 Pain occurring within 72 hours after surgery is the most significant predictor of chronic postoperative pain, making effective pain management during this period critical for knee arthroplasty patients.9
Differences in postoperative pain experiences have been noted in cases of bone metastases and uterine diseases at various time points.10,11 These may suggest that similar features may be present after knee arthroplasty. Current research in pain management mainly starts with physiological blockade, using drugs and anesthetic tissues to reduce the release of inflammatory factors and inhibit central sensitisation to alleviate pain. However, the effects of pain are multidimensional, and patients’ pain management needs tend to be diverse.12 A prerequisite for good pain management is the provision of targeted care based on the pain management needs of different patients. movement-evoked pain is an individual-oriented model and assumes differences in the developmental trajectories of individuals within a group. Individuals with the same developmental trajectory are grouped together. Individuals based on shared developmental trajectories are frequently employed to examine the longitudinal progression of postoperative pain.13
Therefore, this study aims to dynamically track and investigate the status of movement-evoked pain within 72 hours post-knee arthroplasty, identify its longitudinal trajectory, and analyze predictive factors across different trajectory categories. These findings may help identify key populations and inform management strategies to mitigate movement-evoked pain after knee arthroplasty.
Materials and Methods
Participants and Procedure
This cross-sectional survey of participants was recruited using convenience sampling from a tertiary care hospital in Dalian, China, between November 2022 and October 2023. The study adhered to the principles of the Declaration of Helsinki and received approval from the Ethics Committee of the First Hospital of Dalian Medical University (PJ-KS-KY-2023-40).
Participants were included based on the following criteria: 1)Patients diagnosed with knee osteoarthritis according to the Diagnostic Guidelines for Osteoarthritis (2021 edition)14 who were admitted for knee arthroplasty; 2) Age ≥ 18 years; 3) Unimpaired consciousness and communication; 4) Informed consent and voluntary participation in the study. Participants with other serious illnesses such as heart disease, cancer, etc, or those wishing to withdraw were excluded, and their relevant data were not included in the study for analysis. Eligible participants were invited to participate by the investigators, who provided detailed information about the study’s purpose, methods, benefits, and potential risks. After receiving complete information, participants signed an informed consent form and completed a questionnaire in the inpatient unit. Socio-demographic, clinical, and therapeutic information was collected from hospital records.
Participants completed pain catastrophizing and social support scales one day prior to knee arthroplasty (T1) and assessed their pain using the Numeric Rating Scale at 24 hours (T2), 48 hours (T3), and 72 hours (T4) postoperatively. The completed questionnaires were reviewed and collected by the researcher to minimize data omission.
All participants received training on using the Numeric Rating Scale during their hospital stay. All surgeries were performed by the same surgical team under general anesthesia. The same analgesic regimen was administered, and functional knee exercises were conducted by the same group of physicians. Data collection was performed face-to-face by the investigator, ensuring that guidelines and questions were addressed uniformly. Participants’ inquiries were responded to promptly, and the completed surveys were verified for completeness. The survey took approximately 25 minutes to complete.
Sample size calculation was conducted based on M. Kendall’s empirical estimation method, requiring at least 5–10 times the number of dependent variables.15 In this study, a sample size of 178 cases was determined by multiplying the number of independent variables by seven, accounting for a 10% non-response rate.
Measures
Sample Characteristics
Socio-demographic and clinical data collected included participants’ age, gender, height, weight, marital status, education, occupation, and disease duration.
Social Support
Social support was evaluated using the Chinese version of the Social Support Revaluated Scale (SSRS).16 This scale comprises three dimensions: objective support, subjective support, and utilization of support, with a total of 10 items. Scores range from 12 to 66, with higher total scores indicating better social support. In this study, the Cronbach’s α coefficient for the SSRS was 0.736.
Pain Catastrophizing
The Chinese version of the Pain Catastrophizing Scale (PCS) was used to assess pain catastrophizing.17 This scale includes three dimensions: rumination, exaggeration, and helplessness, comprising a total of 13 items. Each item is scored from ‘not at all’ (0 points) to “all the time” (4 points), yielding a total score ranging from 0 to 52. Higher scores reflect greater levels of pain catastrophizing. In this study, the Cronbach’s α coefficient for the PCS was 0.899.
Numerical Rating Scale
The NRS is a self-reported tool for patients to rate the intensity of their pain, consisting of 11 points (0–10), where each number represents a different pain level. Higher scores indicate more severe pain.18 In this study, the NRS was utilized to assess the degree of postoperative movement-evoked pain in knee arthroplasty patients.
Analytic Approach
Statistical data analysis was conducted using SPSS 25.0 and Mplus 8.7 software. Initially, descriptive analyses were performed to report sample characteristics, with continuous variables summarized as means and standard deviations, and categorical variables presented as frequencies and percentages. Subsequently, Mplus 8.7 was utilized to establish a latent class model, starting with a single category and incrementally increasing the number of categories to construct a trajectory for the development of movement-evoked pain after knee arthroplasty. The best-fitting model was selected based on model fit indices and clinical significance. Lower Bayesian Information Criterion (BIC), sample size-adjusted BIC (aBIC), and Akaike Information Criterion (AIC) indicate a better model fit. The Lo-Mendell-Rubin (LMR) and the Bootstrapped Likelihood Ratio Test (BLRT) are standard tests for model fit; a P-value < 0.05 suggests that the model with K categories is superior to the model with K-1 categories. Additionally, higher entropy values (closer to 1) indicate greater classification accuracy.
After determining the trajectory categories, statistical analyses were performed using the Chi-square (X²) test and one-way ANOVA. Statistically significant variables were further analyzed through multivariate logistic regression to explore potential predictors of the developmental trajectory of movement-evoked pain after knee arthroplasty. A P-value < 0.05 was considered statistically significant.
Results
Sample Characteristics
In this study, 178 patients with knee arthroplasty were included. The number of patients who completed T1, T2, T3, and T4 after surgery was 187, 183, 183, and 178 respectively. 4 patients were excluded because they did not have surgery, and 5 patients were discharged from the hospital before 72 hours postoperatively, so the total number of change cases of 187 to 178, and the total loss rate was 2.67%. General information is shown in Table 1.
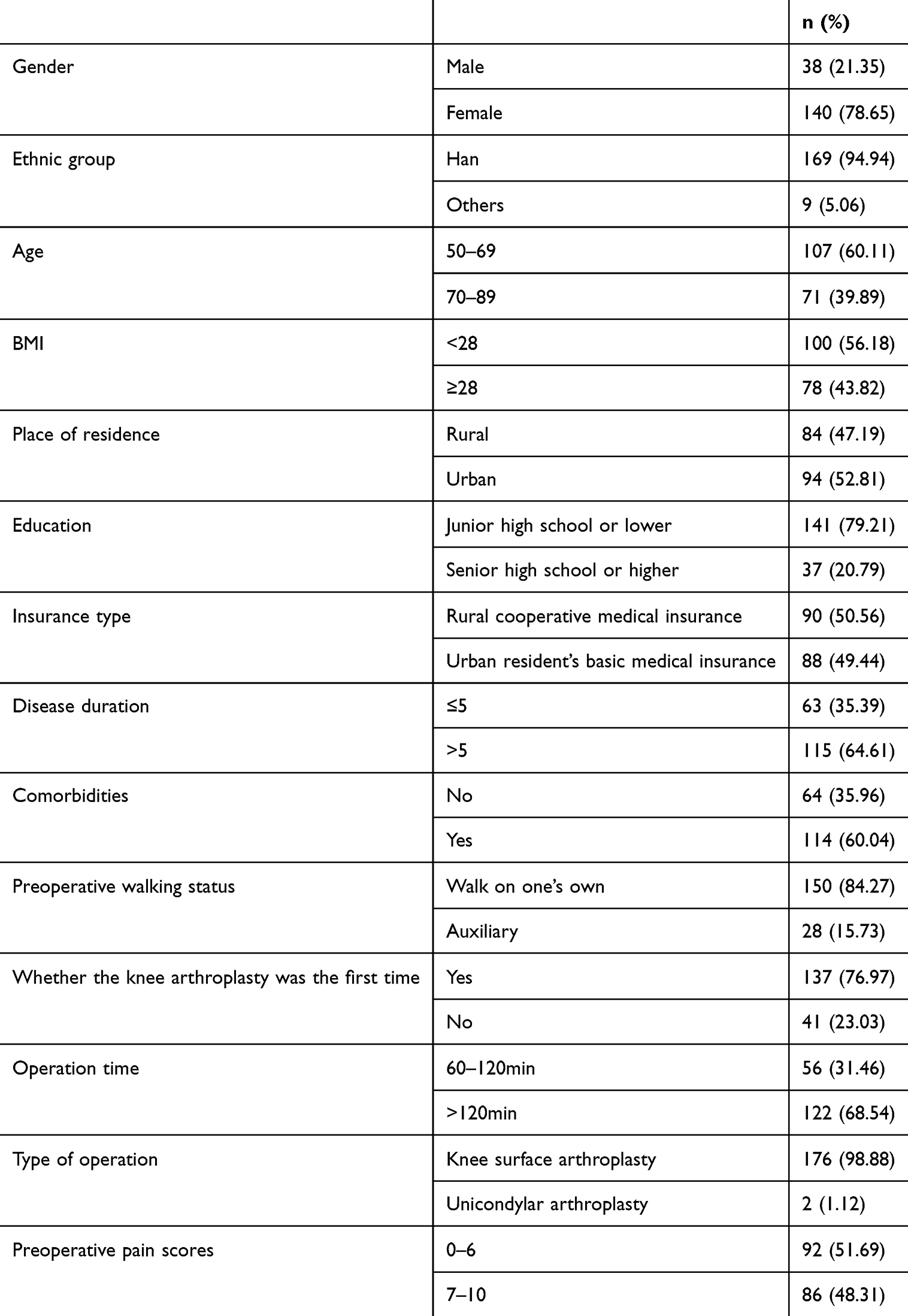 |
Table 1 Baseline Data for Knee Replacement Patients (N=178) |
Identification and Determination of the Trajectory of Movement-Evoked Pain Development After Knee Arthroplasty
The fitting of pain scores during functional joint exercises at T2, T3, and T4 post-knee arthroplasty was analyzed using Growth Mixture Models (GMMs) to establish potential categories for the trajectory of movement-evoked pain development. When the development trajectory of movement-evoked pain was 3 categories, the values of BIC, aBIC, and AIC in the GMM model were lower than the 2 categories, which indicates that the development trajectory of movement-evoked pain in 3 categories was better than the 2 categories. When the development trajectory of movement-evoked pain was 4 categories, the p-value did not reach the significant level (p > 0.05), therefore, the development trajectory of movement-evoked pain in 3 categories was better than the 4 categories. In conclusion. The best model is 3 categories. The model fit indices for each category are presented in Table 2.
 |
Table 2 GMM Fitting Indices for Developmental Trajectory of Postoperative Movement-Evoked Pain (N=178) |
Based on the GMM analysis, three distinct trajectories for the development of movement-evoked pain were identified (Figure 1). The categories were named according to their developmental characteristics. Category 1: This group exhibited moderate pain at 24 hours postoperatively, with pain scores initially rising and then declining over time. It is referred to as the “moderate pain-first-rise-then-fall” group, accounting for 47.75% (n=85) of the sample. Category 2: Patients in this category also reported moderate pain at 24 hours post-surgery, but their pain scores gradually declined in subsequent assessments. This group is termed the “moderate pain-continuously declining” group, comprising 11.80% (n=21) of the participants. Category 3: This group experienced severe pain at 24 hours postoperatively, with pain scores showing fluctuations but overall remaining stable This category is named the “severe pain-continuously stable” group, accounting for 40.45% (n=72) of the total participants.
 |
Figure 1 GMM Development Trajectory of Movement-Evoked Pain Among Patients After Knee Arthroplasty. |
Comparison of Differences in Movement-Evoked Pain After Knee Arthroplasty
Repeated measures ANOVA results showed time point and category interaction terms were statistically significant (F=22.479, P<0.001). Further simple effects analyses showed that intragroup and intergroup differences in postoperative movement-evoked pain at different time points after knee arthroplasty (P<0.001). The results of the simple effects analysis are shown in Table 3.
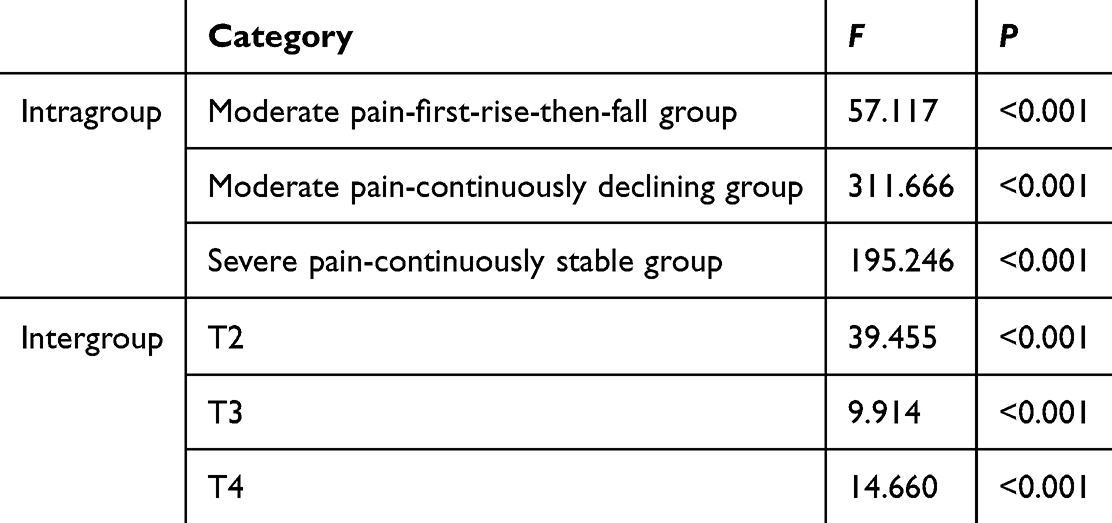 |
Table 3 The Simple Effect Analysis of Movement-Evoked Pain of Each Classes of Patients After Knee Replacement at Each Time Point (N=178) |
Results of a Predictor Analysis of Categories of Trajectory for the Development of Movement-Evoked Pain After Knee Arthroplasty
Results of Univariate Analysis
The results of the X2 test showed statistically significant differences in age, gender, education, disease duration, operation time, and preoperative pain scores for the 3 potential categories of movement-evoked pain after knee arthroplasty (P<0.05). One-way ANOVA results showed statistically significant differences in patients’ social support and pain catastrophizing scores between the three categories(P<0.001). The results of the univariate analysis for the three categories are shown in Table 4.
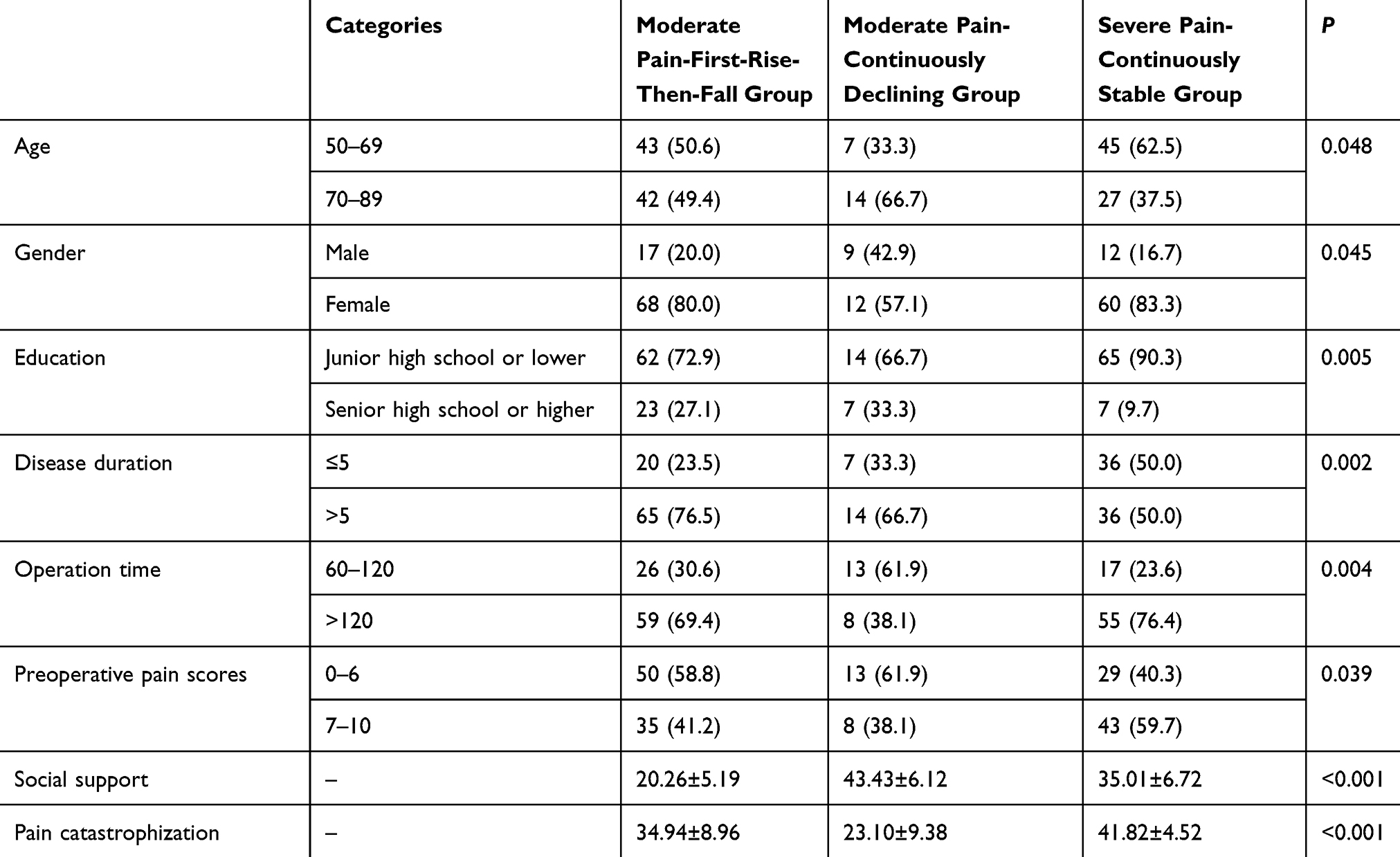 |
Table 4 Univariate Analysis of General Demographics, Social Support, and Pain Catastrophization of Patients in Each Trajectory Category (N=178) |
Results of Multivariate Logistic Regression
Variables that were statistically significant in the univariate analysis (age, gender, education, disease duration, operation time, preoperative pain scores, social support, and pain catastrophizing) were analyzed by multivariate logistic regression. Categorical variables were included after the assignment and continuous variables were included at their original values. Using category 3 as the reference group, results of comparative analyses of Categories 1 and 2 versus Category 3 were obtained. Then using category 2 as the reference group, results of comparative analyses between category 1 and category 2 were obtained. The results showed that social support, pain catastrophization, education, disease duration, and operate time were predictors of potential categories of movement-evoked pain after knee arthroplasty (P < 0.05). Results of multivariate logistic regression analysis were shown in Table 5.
 |
Table 5 Results of Multivariate Logistic Regression Analysis of the Development Trajectory of Movement-Evoked Pain After Knee Arthroplasty (N=178) |
Discussion
Movement-Evoked Pain After Knee Arthroplasty: Identification of Three Distinct Developmental Trajectory Categories
In this study, we identified three potential categories of movement-evoked pain development trajectories after knee arthroplasty using a growth mixture model. The categories were: 1) moderate pain—rising then falling group (47.7%), 2) moderate pain—continuously declining group (11.9%), and 3) severe pain—continuously stable group (40.4%).
Further analysis using repeated measures ANOVA revealed significant differences in movement-evoked pain both within and between groups at different postoperative time points, indicating significant group heterogeneity in movement-evoked pain within the first 72 hours post-surgery.
In our study, the moderate pain—continuously declining group comprised only 11.80% of the total, suggesting that this trajectory is relatively uncommon. Conversely, the moderate pain—rising then falling group, which accounted for 47.75% of patients, emerged as the most prevalent type in clinical practice. This group showed an increasing trend of pain at 48 hours after knee arthroplasty, suggesting that analgesic measures should be strengthened at 48 hours after knee arthroplasty. In the choice of analgesic drugs, analgesia with ketorolac tromethamine is more recommended to reduce postoperative movement-evoked pain.19
The severe pain—continuously stable group, representing 40.45% of participants, consistently experienced severe pain levels after surgery. This indicates that patients in this category are at high risk and warrant increased clinical attention. Healthcare professionals should prioritize the identification of predictors for this population as early as possible and take measures to reduce movement-evoked pain after knee arthroplasty.
In our study, the results show that education and disease duration are predictors of movement-evoked pain after knee arthroplasty. Patients with low education and short disease duration were more likely to enter the severe pain-continuously stable group, the main reason may be the fact that patients with different levels of education have different perceptions of pain, and the patients with low education are more biased towards the perception of pain as an injurious signal and uncontrollable, and they are less able to manage pain effectively.20,21 Patients with higher levels of education are more likely to be successful in pain-related perceptions and taking measures than patients with lower levels of education.22 Therefore, health education on pain-related knowledge should be given in advance to patients with a low level of education to strengthen their knowledge of pain and improve their ability to cope with pain, thus reducing postoperative movement-evoked pain.
The patients with short disease duration are more likely to have movement-evoked pain after knee arthroplasty. The results are similar to the findings of Weiwei Kong.12 The reason for this may be related to the fact that the longer the patient’s disease duration, the longer he suffers from pain, which increases the threshold of pain. As a result, patients with shorter disease duration were more likely to enter the severe pain-continuously stable group compared to patients with longer disease duration.
For patients with short disease duration, we can take measures to reduce postoperative movement-evoked pain, such as fast-acting non-steroidal anti-inflammatory drugs, which can be given in advance to minimize pain caused by functional exercises after knee arthroplasty and to promote patient comfort.
Predictors of Severe Pain in Knee Arthroplasty: Operation Time, Social Support, and Pain Catastrophization
Our study shows that operation time, social support, and pain catastrophization are significant predictors of movement-evoked pain after knee arthroplasty. Patients with longer operation time, lower social support, and higher pain catastrophization levels are more likely to experience severe movement-evoked pain.
Longer operation time are associated with increased movement-evoked pain, aligning with findings from Yiyang Li et al.23 The reason may be that a tourniquet is used in knee arthroplasty in order to reduce intraoperative bleeding, obtain a clearer surgical field of vision, and the purpose of better fit the prosthesis. The prolonged use of a tourniquet during surgery to minimize bleeding can lead to increased swelling and pain at the surgical site.24 In addition, the operation time tends to be directly proportional to the complexity of the surgical procedure; with the longer operation time, the more complex the operation is likely to be.25 Therefore, Longer operation time has a passive influence on postoperative knee mobility and the level of postoperative movement-evoked pain. This underscores the importance of striving to minimize operation times where possible to reduce postoperative pain and enhance recovery.
Social support plays a critical role in pain management. It has been shown to facilitate more effective pain adaptation, and a lack of support can exacerbate pain levels.26 There are various mechanisms that social support influences pain in postoperative movement-evoked pain. Higher social support allows the patient to express the presence of pain, so measures to relieve pain can be given to reduce the level of pain. At the same time, patients with high social support receive more help in decision-making to cope with pain, which is able to increase positive health behaviors and outcomes.27
Pain catastrophization is a notable predictor of high-level movement-evoked pain in knee arthroplasty patients postoperatively. It is similar to the study of Noiseux et al.28 Pain catastrophization, as a negative psychological emotion, is an irrational cognition that individuals are experiencing or expect to experience pain.29 This negative psychological response can lead to overreactions to pain and reduced pain tolerance.30
Transforming patients’ perceptions of pain and adapting to maladaptive feelings can reduce pain catastrophization in patients. Common interventions to reduce the level of pain catastrophization in patients are cognitive behavioral therapy, acceptance therapy, qigong, and yoga exercises.31,32 In addition, social support moderates the effect of pain catastrophizing on postoperative pain in patients with knee arthroplasty.33 Healthcare workers should pay attention to the negative emotional state and social support. Healthcare workers should also give patients correct guidance and interventions. They can promote patients’ positive acceptance and coping with adverse emotions. These measures can enhance patients’ pain tolerance and reduce postoperative movement-evoked pain.
There are some shortcomings in our study. Firstly, in this study, the sample was drawn from a single tertiary care hospital. This may have some bias in the selection of the population. Secondly, this study did not analyze patients who were excluded, which may also have biased the results of the study. Finally, our assessment of movement-evoked pain was limited to the first 72 hours postoperatively, potentially affecting the generalizability of the results. Future research should involve multicenter studies with larger sample sizes and extended follow-up periods to explore pain management strategies in different healthcare settings to more effectively reduce movement-evoked pain after knee arthroplasty.
Conclusion
This study identifies there are three potential categories of movement-evoked pain developmental trajectories after knee arthroplasty. The most common type in the clinic was the moderate pain- rising then falling group. Social support, pain catastrophization, education, disease duration, and operation time were significant predictors of potential categories of movement-evoked pain after knee arthroplasty.
Data Sharing Statement
The data of this study came from the same dataset as the data of the previous article online.33 But the research content and statistical methods are completely different. The article published online explores that social support had a significant moderating effect on the relationship between pain catastrophizing and acute post-surgical pain. This article focuses on tracking the trajectory of movement-evoked pain at 72 hours after knee arthroplasty and analyzes the predictors between different trajectory categories to identify people who are prone to severe movement-evoked pain after knee arthroplasty. Data used for this study can be obtained from the corresponding author upon reasonable request.
Ethics Statement
The study complied with the principles outlined in the Declaration of Helsinki and was also approved by the Ethics Committee of the First Hospital of Dalian Medical University (PJ-KS-KY-2023-40). All participants signed an informed consent form before participating in this study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bian YY, Cheng KY, Chang X. et al. Reports and analysis of amount of Hip and knee arthroplasty in China from 2011 to 2019. Chin J Orthopaedics. 2020;40(21):8.
2. Otten R, van Roermund PM, Picavet HSJ. Trends in the number of knee and Hip arthroplasties: considerably more knee and hip prostheses due to osteoarthritis in 2030. Nederlands Tijdschrift voor Geneeskunde. 2010;154:1534.
3. Kurtz S, Ong K, Lau E, et al. Projections of primary and revision Hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg. 2007;89(4):780–785. doi:10.2106/00004623-200704000-00012
4. Rogers MP, Kuo PC. Pain as the Fifth Vital Sign. Journal of the American College of Surgeons. 2020;231(5):601–602. doi:10.1016/j.jamcollsurg.2020.07.508
5. Yurutkina A, Klaschik S, Kowark P, et al. Pain levels and patient comfort after lower limb arthroplasty comparing i.v. patient-controlled analgesia, continuous peripheral nerve block and neuraxial analgesia: a retrospective cohort analysis of clinical routine data. J Orthopaedic Surg Res. 2022;17(1):381. doi:10.1186/s13018-022-03277-0
6. Lundgren BS. Assessing Movement-Evoked Pain. Am J Nurs. 2023;123(9):9. doi:10.1097/01.NAJ.0000995276.03176.f0
7. Fullwood D, Means S, Merriwether EN, et al. Toward Understanding Movement-evoked Pain (MEP) and its Measurement: a Scoping Review. Clin J Pain. 2021;37(1):61–78. doi:10.1097/AJP.0000000000000891
8. Liao C, Tsauo J, Huang S, et al. Preoperative range of motion and applications of continuous passive motion predict outcomes after knee arthroplasty in patients with arthritis. Knee Surg Sports Traumatol Arthrosc. 2019;27(4):1259–1269. doi:10.1007/s00167-018-5257-z
9. Sayers A, Wylde V, Lenguerrand E, et al. Rest Pain and Movement-Evoked Pain as Unique Constructs in Hip and Knee Replacements. Arthritis Care & Research. 2016;68(2):237–245. doi:10.1002/acr.22656
10. Zhao WJ, Zhang XJ. Trajectory of pain changes after radiofrequency ablation combined with percutaneous vertebroplasty in patients with bone metastases and the factors influencing them.
11. Sang GW. Heterogeneous Trajectories of Persistent Pain After Focused Ultrasound Ablation Surgery for Benign Uterine Diseases Under Enhanced Recovery After Surgery. Chongqing University; 2023.
12. Li H, He YX, Shang JJ. The latent categories of pain care needs in patients after thoracoscopic lung cancer resection. J Nurs Sci. 2024;39(19):35–39.
13. Fang Y, Xiao J. Application progress of growth mixture model in health trajectory research. Chin J Heal Stat. 2020;37(4):637–640.
14. The Joint Surgery Branch of the Chinese Orthopaedic Association, The Subspecialty Group of Osteoarthritis, Chinese Association of Orthopaedic Surgeons, The National Clinical Research Center for Geriatric Disorders (Xiangya Hospital), et al. Chinese guideline for diagnosis and treatment of osteoarthritis (2021 edition). Chin J Orthopaedics. 2021;41(18):1291–1314.
15. Chen F. Multivariate statistical analysis methods for medical treatment. Beijing: China Statistics Press. 2000;128–130.
16. Xiao SY. Theoretical basis and research application of the Social Support Revaluaed Scale. J Clin Psychiatry. 1994;02:98–100.
17. Yap JC, Lau J, Chen PP. Validation of the Chinese Pain Catastrophizing Scale (HK-PCS) in patients with chronic pain. Pain Med. 2008;9(2):186–195. doi:10.1111/j.1526-4637.2007.00307.x
18. Schütze R, Rees C, Smith A, et al. How Can We Best Reduce Pain Catastrophizing in Adults With Chronic Noncancer Pain? A Systematic Review and Meta-Analysis. J Pain. 2018;19(3):233–256. doi:10.1016/j.jpain.2017.09.010
19. Yang QR, Liu X, Wang C, et al. Application Effect and Economic Evaluation of Analgesia Drug After Knee Arthroplasty. Henan Med Res. 2024;33(6):1090–1093.
20. Roth RS, Geisser ME. Educational achievement and chronic pain disability: mediating role of pain-related cognitions. Clin J Pain. 2002;18(5):286–296. doi:10.1097/00002508-200209000-00003
21. Mickle AM, Domenico LH, Tanner JJ. Elucidating factors contributing to disparities in pain-related experiences among adults with or at risk for knee osteoarthritis. Front Pain Res. 2023;4:1058476. doi:10.3389/fpain.2023.1058476
22. Cano A, Mayo A, Ventimiglia M. Coping, pain severity, interference, and disability: the potential mediating and moderating roles of race and education. J Pain. 2006;7(7):459–468. doi:10.1016/j.jpain.2006.01.445
23. Li YY. A Study on the Construction and Validation of Acute Pain Risk Prediction Model After Knee Replacement. Yangtze University; 2013.
24. Kumar N, Yadav C, Singh S, et al. Evaluation of pain in bilateral total knee replacement with and without tourniquet; a prospective randomized control trial. J Clinl Orthopaedics Trauma. 2015;6(2):85–88. doi:10.1016/j.jcot.2015.01.095
25. Yu HY, Ye XH, Li JH. Factors influencing the occurrence of hypotension and protective measures during transurethral electrolysis of the prostate. Zhejiang J Traumatic Surg. 2024;29(9):1639–1641.
26. Matthias MS, Hirsh AT, Ofner S, Daggy J. hips Among Social Support, Patient Activation, and Pain-Related Outcomes. Pain Med. 2022;23(4):676–685. doi:10.1093/pm/pnab306
27. Richmond NL, Meyer ML, Hollowell AG, et al. Social Support and Pain Outcomes After Trauma Exposure Among Older Adults: a Multicenter Longitudinal Study. Clin J Pain. 2018;34(4):366–374. doi:10.1097/AJP.0000000000000545
28. Noiseux NO, Callaghan JJ, Clark CR, et al. Preoperative predictors of pain following total knee arthroplasty. The Journal of Arthroplasty. 2014;29(7):1383–1387. doi:10.1016/j.arth.2014.01.034
29. Sullivan MJL, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain. 2001;17(1):52–64. doi:10.1097/00002508-200103000-00008
30. Hasegawa M, Tone S, Naito Y, et al. Preoperative pain catastrophizing affects pain outcome after total knee arthroplasty. Journal of orthopaedic science: official journal of the. Jpn Orthopaedic Assoc. 2022;27(5):1096–1099. doi:10.1016/j.jos.2021.05.011
31. Luo HY. Li QF.Research hotspots of pain catastrophizing:a visualized analysis based on CiteSpace software. Military Nursing. 2023;40(07):77–81.
32. Pei JH, Chen HX, Gou L, et al. Review of pain catastrophizing in patients underwent total knee arthroplasty.Chin. J Nurs. 2019;54(11):1752–1756.
33. Ai S, Wang Y, Niu P, et al. Pain Catastrophizing and Acute Post-Surgical Pain in Knee Arthroplasty Patients: the Moderating Role of Social Support. J Pain Res. 2024;17:3127–3136. doi:10.2147/JPR.S474652
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.