")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Research Progress and Trends in Exercise Interventions for Mild Cognitive Impairment: A Bibliometric Visualization Analysis Using CiteSpace
Received 10 November 2024
Accepted for publication 17 January 2025
Published 31 January 2025 Volume 2025:18 Pages 505—529
DOI https://doi.org/10.2147/JMDH.S498190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles Victor Pollack
Qifeng Han,1 Sung Min Kim1– 4
1Department of Physical Education, Hanyang University, Seoul, Republic of Korea; 2Department of Sport Science, Hanyang University, Seoul, Republic of Korea; 3BK21 FOUR Human-Tech Convergence Program, Hanyang University, Seoul, Republic of Korea; 4Center for Artificial Intelligence Muscle, Hanyang University, Seoul, Republic of Korea
Correspondence: Sung Min Kim, Department of Sport Science, Hanyang University, 222, Wangsimni-ro, Seongdong-gu, Seoul, Republic of Korea, Email [email protected]
Purpose: With the increasing global aging population, exercise interventions for mild cognitive impairment (MCI) have gained significant research attention. This study uses CiteSpace6.3R2 to systematically analyze the research progress and emerging trends in this field.
Methods: A comprehensive literature search in the Web of Science Core Collection focused on exercise interventions for MCI. After screening, 420 relevant publications were imported into CiteSpace6.3R2 for bibliometric analysis, generating visual maps of keywords, authors, institutions, and other key indicators.
Results: Publications on exercise interventions for MCI have shown steady growth, with Journal of Alzheimer’s Disease leading in volume, and Geriatrics & Gerontology as the dominant subject area. The USA ranks highest in collaborative output, with the Chinese University of Hong Kong as the top institution. Among authors, Shimada Hiroyuki and three Japanese colleagues are key contributors, while Neurology is the most frequently co-cited journal. The most frequently co-cited author, Petersen, R.C. has his 2018 work as the top reference. High co-occurrence keywords include “mild cognitive impairment”, “dementia”, and “Alzheimer’s disease”. The primary keyword clusters are #0 Cognitive training, #1 Cognitive impairment, and #2 Mild Cognitive impairment, while newly burst keywords “systematic review”, “recommendations”, and “depression”.
Conclusion: Research on exercise interventions for MCI has been steadily gaining attention, becoming an interdisciplinary research area in fields such as geriatrics and neuroscience, with relevant findings concentrated in specific journals. In the collaboration network, developed countries dominate, showing systematic patterns of inter-institutional collaboration, while author collaborations are primarily focused within institutions. Current research is centered on the design and mechanisms of exercise intervention programs. Future studies will prioritize integrated intervention strategies, systematic evidence synthesis, and personalized interventions for specific populations.
Keywords: exercise intervention, exercise therapy, mild cognitive impairment, cognitive dysfunction, bibliometric, visualization analysis, CiteSpace
Introduction
With the acceleration of global aging, the United Nations (UN) predicts that by 2030, the global population of individuals aged 65 and older will reach 994 million, and by 2050, this figure is expected to rise to 1.6 billion.1 Concurrently, the increasing elderly population is accompanied by a heightened prevalence of chronic diseases, with the risk of dementia in older adults becoming increasingly pronounced. Dementia has emerged as the third leading cause of severe threats to human life and health, following cardiovascular diseases and malignant tumors.2 Currently, over 55 million people worldwide are living with dementia, and this number is projected to reach 78 million by 2030.3 The condition imposes significant suffering and an immense economic burden on patients, their families, and society at large, underscoring the critical importance of prevention.
The prevention of dementia involves the early identification of patients with mild cognitive impairment (MCI) and the implementation of appropriate intervention measures. MCI represents a state of mild cognitive decline, which exists between normal aging and early-stage dementia.4 The incidence of MCI increases with age, particularly in individuals aged 60 to 84 years. Specifically, the incidence rates are 6.7% for those aged 60–64, 8.4% for those aged 65 to 69, 10.1% for those aged 70–74, 14.8% for those aged 75–79, and 25.2% for individuals aged 80–84.5 Additionally, the conversion rate to dementia within two years for individuals with MCI aged 65 and above is 14.9%.5 Over 3 to 5 years, 20% to 46% of MCI patients may progress to dementia.6 While not all individuals with MCI develop dementia, their risk is significantly higher compared to those without MCI.7 Importantly, patients with MCI retain a degree of cognitive ability and plasticity, making this period optimal for dementia prevention. Traditional medicines have demonstrated a role in reducing the incidence and severity of cognitive decline by modulating inflammatory responses.8 However, their therapeutic effects are limited and insufficient to effectively prevent dementia.9 Therefore, the academic community emphasizes early detection and prevention of dementia through the use of standardized assessment tools before the onset of symptoms. This has led to an increase in the number of researchers focusing their studies on MCI.
To effectively address MCI and reduce the risk of dementia, healthcare organizations and research institutions globally are advancing new diagnostic tools and prevention strategies. These efforts include applying advanced neuroimaging techniques to facilitate earlier identification of potential MCI cases and implementing artificial intelligence-assisted systems to assess patients’ cognitive abilities.10,11 Researchers are also investigating lifestyle-based preventive interventions, such as dietary improvements, increased physical activity, and enhanced social interactions.12–14 In 2018, the American Neurological Association recommended exercise interventions as an effective approach to enhancing cognitive function in individuals with MCI.5 An international guideline published in 2023 further emphasizes that managing MCI through physical activity and exercise is currently one of the key strategies.15
With the growing application of exercise interventions in patients with MCI, the number of related studies has steadily increased, and the depth of research has significantly advanced. Studies have demonstrated that exercise interventions can effectively enhance the cognitive function of MCI patients by promoting neuroplasticity, increasing cerebral blood flow, and reducing neuroinflammation.16–18 Additionally, comparative studies have examined various types of exercise, including aerobic exercise, resistance training, and mind-body exercises, to determine which modalities or combinations are most effective for MCI patients.19,20 Furthermore, recent investigations have begun to explore the long-term effects and adherence to exercise interventions.21,22 These studies also evaluate strategies to enhance overall intervention efficacy by integrating cognitive training, nutritional interventions, and non-invasive brain stimulation techniques.23,24
Currently, research on exercise interventions for MCI exhibits a complex and diverse landscape, highlighting the urgent need for systematic integration to elucidate research progress and emerging trends. Bibliometric visualization analysis has proven an effective tool, offering a scientific foundation for identifying research hotspots, understanding knowledge structures, and mapping evolutionary patterns within this field.25 Previous studies have employed bibliometric visualization methods to analyze exercise interventions for MCI-related research, revealing significant hotspots and future trends, thereby providing valuable insights for advancing this field.26,27 However, these studies often focus more on “exercise” and “MCI” while neglecting the core concept of “intervention”. Neglecting “intervention” may result in research being limited to surface descriptions of the superficial associations between “exercise” and “MCI”, lacking in-depth exploration of intervention mechanisms, intervention design, and their practical implications. This oversight also leads to an incomplete knowledge framework in the research field, weakening research outcomes’ systematicity and practical value.
This study utilizes CiteSpace6.3R2 to perform a bibliometric visualization analysis of research on exercise interventions for MCI from multiple perspectives. Specifically, (1) we analyzed publication volume, journal distribution, and subject category distribution to elucidate developmental trends within this field. (2) We constructed collaboration networks among regions, institutions, and authors to investigate international cooperation patterns and identify core research contributors. (3) We examined the co-citation networks of journals, authors, and literature to delineate the theoretical foundations and highlight key publications in this field. (4) We identified research hotspots, thematic structures, and emerging trends through keyword co-occurrence, clustering, and burst detection analyses. (5) Based on these analyses, we developed a comprehensive knowledge framework for the field, discussed key research focus, and outlined future research characteristics.
Materials and Methods
Data Collection
This study adhered to the latest guidelines for bibliometric analysis and was written following the Preliminary Guideline for Reporting Bibliometric Reviews of the Biomedical Literature(BIBLIO) (Supplementary Material 1).28,29 The Web of Science (WoS) database is widely recognized for its comprehensiveness and authority, making it a preferred choice for bibliometric research.30 This study utilized the Web of Science Core Collection(WoS CC) as the primary database for conducting publication searches. Using a single database ensures data consistency, effectively mitigating potential issues caused by discrepancies in format and quality across multiple sources.31 This approach enhances the reliability of research findings.
The comprehensiveness of the publication search is critical to ensuring the quality of bibliometric visualization research; consequently, establishing a well-defined time frame and systematic search strategy is essential. The concept of MCI originated in the 1980s,32 with Petersen et al providing a pivotal redefinition in 1999 that established the diagnostic criteria widely accepted in the scientific community.33–35 Accordingly, this study delineated a publication search time spanning from 1999 to 2023 to maximize the comprehensiveness and representativeness of the collected data. Based on existing research, relevant content from the Cochrane Handbook for Systematic Reviews of Interventions, considerations from the PICOS framework, and pilot testing, a preliminary publication search strategy was developed.26,36,37 This strategy was refined through two rounds of peer review in accordance with the PRESS guidelines (Supplementary Materials 2 and 3),38 resulting in the final search strategy: TS = (“exercise” OR “physical activity” OR “training” OR “sport” OR “fitness” OR “exergames” OR “motor”) AND TS = (“mild cognitive impairment” OR “MCI”) AND TS = (“intervention” OR “therapy” OR “treatment”).
Data Screening
The inclusion criteria were as follows: (1) the publication must be in English; (2) the types of document eligible for inclusion include articles or review articles; (3) the research content must be related to exercise interventions for MCI, with the intervention focused on exercise and optionally combined with other interventions, and the study population must explicitly include patients with MCI; (4) the study designs include randomized controlled trials (RCTs), systematic reviews, and meta-analyses, but they are not limited to these.
The exclusion criteria were as follows: 1) the study design is descriptive research or animal experiments; (2) the types of non-research publications, such as conference abstracts, editorials, and commentaries, were excluded; (3) duplicated publications, with only the most recent one retained; (4) publication that lacks key information or has been retracted; (5) the study subjects do not include patients diagnosed with MCI.
A total of 2369 publications were initially identified through the December 9, 2024 search. Two researchers conducted the screening process independently, applying predetermined criteria by reviewing titles and abstracts. When discrepancies arose between the two researchers, the full text was reviewed, and a consensus was reached through discussion. After the final screening, a total of 420 valid publications were identified (Supplementary Material 4). The valid publications’ full records and cited references were then exported as plain text files and converted to the appropriate format using the Data Import function of CiteSpace software.
Analysis Methods and Tools
CiteSpace, developed by Professor Chaomei Chen at Drexel University (USA), is grounded in network science and information visualization principles. This software specializes in bibliometric visualization analysis of scientific publications. CiteSpace enhances the efficiency of bibliometric analysis by presenting systematic research more intuitively and objectively while minimizing errors throughout the research process.39
To further conduct bibliometric visualization analysis for this study, CiteSpace6.3R2 was utilized with the following parameter settings: Time Slicing (1999.01–2023.12), Years Per Slice (1), Selection Criterion (g-index with k=25), with all other settings kept at their default values. Nodes representing author, institution, country, keyword, category, and reference were selected to generate a knowledge map. In the knowledge map, each node’s diameter corresponds to the node’s frequency, and the thickness of the lines between nodes indicates their co-occurrence. Thicker lines suggest a closer relationship between nodes. The color of the nodes reflects different years, and nodes with a purple ring are considered key points with high centrality.40 Figure 1 illustrates the process of data collection and screening, along with the research framework.
 |
Figure 1 Flowchart of Data Collection, Screening Process, and Research Framework. This figure outlines the bibliometric analysis process of exercise interventions for MCI. It includes four stages: Data Collection, where literature was retrieved from the Web of Science Core Collection (n=2369); Data Screening, which applied inclusion and exclusion criteria, resulting in 420 valid publications; Results, where CiteSpace 6.3R2 was used for bibliometric visualization, including co-occurrence and co-citation analyses; and Discussion, which interprets findings in terms of knowledge framework, research focus, and future trends. |
Results
Publication Statistics
Annual Number of Publications
The annual number of publications reflects the evolutionary trajectory and academic interest in exercise interventions for MCI research. As shown in Figure 2, the number of publications has generally exhibited an upward trend from 2004 to 2023, despite minor fluctuations in certain years. The annual output increased from 1 publication in 2004 to 48 publications in 2023, with a notable acceleration after 2018. This overall growth pattern suggests mounting interest from the scientific community in exploring exercise interventions for MCI. The peak publication output occurred in 20221, with 65 publications. Although the COVID-19 pandemic has somewhat altered the implementation approaches of exercise interventions for MCI research, it has not hindered the overall growth in the number of studies in this field.
 |
Figure 2 Annual Publication Trend from 2004 to 2023. This figure illustrates the annual number of publications related to exercise interventions for MCI from 2004 to 2023. The blue bars represent the number of publications per year, while the Orange line indicates the trend in publication growth. The dotted black trend line represents the overall publication trajectory over time. |
Number of Publications by Journal
According to WoS CC data, research on exercise interventions for MCI is published across 183 journals. Table 1 presents the top 10 journals by publication volume, which includes 13 journals due to identical publication counts among some journals. These leading journals collectively account for 34.29% of the total publications, indicating that a significant portion of the research is concentrated in a relatively small number of journals. Four journals include “Aging” in their titles, highlighting the significant role of aging-related journals in this field.
 |
Table 1 Top 10 Journals by Publication Volume |
Number of Publications by Category
Examining publication categories reveals the primary focus areas and interdisciplinary nature of research on exercise interventions for MCI. Table 2 highlights the top 10 categories in exercise interventions for MCI. Of these categories, “Geriatrics & Gerontology” is the most prominent, with 189 publications representing 45.00% of total publications. This is followed by “Neurosciences”, with 109 publications (25.95%), and “Gerontology”, with 87 publications (20.71%).
 |
Table 2 Top 10 Categories in Exercise Interventions for MCI |
Collaboration Relations
Regional Collaboration
The regional co-occurrence map includes 58 nodes and 294 links (Figure 3), illustrating the collaborative network among various regions. Table 3 presents the top 10 regions by number of collaborative publications, including five European countries, two Asian countries, two American countries, and one from Oceania. Among these regions, the USA ranks first with 147 collaborative publications, followed by China (145 publications) and Australia (46 publications). While the publication count provides one measure of collaboration, intermediary centrality offers another perspective on the importance of each region in the network. Although Australia has only 46 publications, it shows the highest intermediary centrality (0.26), while the USA (0.25) and Germany (0.23) rank second and third.
 |
Table 3 Top 10 Regions by Number of Collaborative Publications |
 |
Figure 3 Regional Co-Occurrence Map. This map illustrates regional collaborations in exercise interventions for MCI. Node size reflects publication volume, with larger nodes indicating higher output. Link thickness represents collaboration strength, while node and link colors correspond to the timeline. Nodes with purple rims indicate high betweenness centrality, highlighting key regions in the network. |
Institutional Collaboration
The institutional co-occurrence map comprises 363 nodes and 650 links (Figure 4), effectively visualizing the network of collaborations among institutions. Table 4 lists the top 10 institutions by number of collaborative publications. The Chinese University of Hong Kong leads with 19 collaborative publications, followed by the National Center for Geriatrics and Gerontology (NCGG) with 15, and the Fujian University of Traditional Chinese Medicine with 14. Regarding intermediary centrality, the University of Melbourne demonstrated the highest (0.15), indicating its critical role in the international collaboration network. Other institutions with notable intermediary centrality include the Aristotle University of Thessaloniki and the University of British Columbia, both 0.07. Geographically, Chinese and Australian institutions demonstrated significant representation and influence in the field.
 |
Table 4 Top 10 Institutions by Number of Collaborative Publications |
 |
Figure 4 Institutional Co-Occurrence Map. This map illustrates institutional collaborations in exercise interventions for MCI. Node size indicates publication output, with larger nodes reflecting higher contributions. Link thickness represents collaboration strength, while node and link colors indicate the timeline. Nodes with purple rims highlight institutions with high betweenness centrality, acting as key connectors. |
Author Collaboration
The author co-occurrence map comprises 512 nodes and 1072 links (Figure 5), visually representing the collaborative network among authors. Table 5 lists the top 10 authors by number of collaborative publications, totaling 13 authors. At the NCGG in Japan, four authors each have 10 collaborative publications, all derived from shared research projects. Two other NCGG researchers (Tsutsumimoto and Yoshida) follow with 8 and 7 collaborative publications. We observe similar contributions from Fujian University of Traditional Chinese Medicine. Tao leads with 8 collaborative publications, followed by Chen and Xia (6 publications each). The intermediary centrality of all authors is 0, indicating that these authors do not occupy significant bridging or intermediary positions within the collaboration network.
 |
Table 5 Top 10 Authors by Number of Collaborative Publications |
 |
Figure 5 Author Co-Occurrence Map. This map illustrates author collaborations in exercise interventions for MCI. Node size indicates publication contributions, with larger nodes reflecting higher contributions. Link thickness represents collaboration strength between authors, while node and link colors indicate the timeline. Nodes with purple rims highlight authors with high betweenness centrality, acting as key connectors within the research network. |
Co-Citation Relations
Journal Co-Citation
The journal co-cited map (Figure 6) visualizes the relationships among major journals within the field of exercise interventions for MCI, revealing 7 distinct knowledge clusters. Different colored node groups represent various research themes or areas, with labels indicating the primary focus of each cluster. Table 6 presents the top 10 journals by co-cited frequency. The journal Neurology demonstrates the highest co-cited count (348) yet exhibits relatively low intermediary centrality (0.01). Similarly, both the Journal of the American Geriatrics Society and the Journal of Alzheimer’s Disease show high co-cited counts, accompanied by low intermediary centrality. These findings indicate that despite being frequently referenced, these prominent journals serve limited roles as connectors within the citation network. In terms of journal quartiles, the majority are classified as Q1, indicating their status as leading journals in their respective fields.
 |
Table 6 Top 10 Journals by Co-Cited Frequency |
 |
Figure 6 Journal Co-Cited Map. This map illustrates co-citation relationships among journals in exercise interventions for MCI. Node size reflects co-citation frequency, with larger nodes indicating higher influence. Link thickness represents co-citation strength. Nodes and links are color-coded by clusters, highlighting thematic connections. |
Author Co-Citation
The author co-cited map (Figure 7) illustrates the major groups of co-cited authors and their research theme clusters within the field of exercise interventions for MCI, identifying nine primary clusters. Table 7 lists the top 10 authors by co-cited frequency. Dr. Petersen, a neurologist from Mayo Clinic (United States), demonstrates the highest co-cited count while ranking second in intermediary centrality (0.12). The second-ranked “UNKNOWN” nodes reflect bibliometric analysis limitations in processing non-standard or non-English citations. Erickson ranks third-highest in the co-cited count. Though not leading in the co-cited count, Barnes holds the highest intermediary centrality in the network.
 |
Table 7 Top 10 Authors by Co-Cited Frequency |
 |
Figure 7 Author Co-Cited Map. This map illustrates co-citation relationships among authors in exercise interventions for MCI. Node size reflects co-citation frequency, with larger nodes indicating higher influence. Link thickness represents co-citation strength, while nodes and links are color-coded by clusters to highlight thematic groupings. |
Reference Co-Citation
The reference co-cited map (Figure 8) visualizes the primary co-cited references and their thematic clusters within the field of exercise interventions for MCI, identifying 14 significant clusters. Among the top 10 highly co-cited references presented in Table 8, Petersen et al’s practice guideline “Practice Guideline Update Summary: Mild Cognitive Impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology” has the highest co-cited frequency. The second most frequently co-cited reference is “Effects of Aerobic Exercise on Mild Cognitive Impairment: A Controlled Trial”. Beyond citation frequency, intermediary centrality offers another perspective on the influence of key studies. The studies “Exercise Training Increases Size of Hippocampus and Improves Memory” and “Effect of Physical Activity on Cognitive Function in Older Adults at Risk for Alzheimer Disease: A Randomized Trial” show the highest intermediary centrality (0.17), indicating its crucial bridging role in connecting different research themes.
 |
Table 8 Top 10 References by Co-Cited Frequency |
 |
Figure 8 Reference Co-Cited Map. This map visualizes co-citation relationships among references in exercise interventions for MCI. Node size reflects co-citation frequency, with larger nodes, indicating higher influence. Link thickness represents co-citation strength. Nodes and links are color-coded by clusters, representing thematic research areas. |
Keyword Distribution
Keyword Co-Occurrence
Analyzing the keyword co-occurrence helps identify the primary research focus within a field. Table 9 presents the top 10 keywords by co-occurrence frequency in the field of exercise interventions for MCI. Among them, “mild cognitive impairment” emerges as the core keyword, appearing 292 times and holding the highest rank. “Dementia” and “Alzheimer’s disease” occupy the second and third positions, with co-occurrence frequencies of 248 and 240. “Aerobic exercise” ranks seventh with a frequency of 117 and exhibits the highest intermediary centrality (0.1), indicating the critical roles in connecting various research themes.
 |
Table 9 Top 10 Keywords by Co-Occurrence Frequency |
Keyword Clustering
Keyword clustering groups keywords with similar themes, forming distinct research topics or hotspots. The keyword timeline builds on this clustering by arranging keywords within each cluster chronologically, thereby illustrating each theme’s emergence and development trajectory. This approach highlights core research areas and reveals the evolutionary trends of each topic over time. Figure 9 illustrates a keyword co-occurrence timeline within exercise interventions for MCI, displaying 11 clusters on the chart’s right side. Early research primarily focused on clusters #2, Mild Cognitive Impairment, and #4, Physical Activity, emerging as key areas of interest in 2004. These research efforts later expanded to include clusters #1 Cognitive Impairment, #5 Network Meta-Analysis, #9 Brain-Derived Neurotrophic Factor, and #10 Tai Chi, which gained traction within the same year (2005). Subsequently, clusters #7 Age and #3 Falls began receiving increased attention during 2006–2007. By 2009, clusters #0 Cognitive Training, #6 Cardiorespiratory Fitness, and #8 Sports Medicine started to develop as prominent research themes. Notably, all clusters have remained active and continued to evolve through 2023.
 |
Figure 9 Keyword Co-Occurrence Timeline Map. This map illustrates the temporal evolution of research topics in exercise interventions for MCI (2004–2023). Nodes represent keywords, with larger nodes indicating higher frequency, while link thickness reflects co-occurrence strength. Clusters are color-coded and arranged chronologically along a timeline. |
Keyword Bursts
Keyword burst analysis identifies emerging research frontiers and hotspots, reflecting recent trends and shifts in focus within the field. Figure 10 illustrates a burst analysis of keywords in exercise interventions for MCI, highlighting the top 20 keywords with the highest burst intensities. The keyword “Population” exhibited the longest keyword burst from 2008 to 2016, with a strength of 4.87, the highest among all keywords. Similarly, “controlled trial” and “clinical trials” showed keyword bursts lasting five years, from 2009 to 2014 and 2013 to 2018, respectively. The keywords “healthy older adults” and “cognitive dysfunction” exhibited burst strengths of 4.19 and 4.13, respectively, indicating their significance during their respective periods. In the past three to four years, keywords such as “cognitive dysfunction”, “systematic review”, “recommendations”, and “depression” have experienced sustained keyword bursts and remain active through 2023.
 |
Figure 10 Keyword Burst Map. This figure illustrates the top 20 keywords with the strongest burst intensity in exercise interventions for MCI from 2004 to 2023. Each row represents a keyword, with blue bars indicating the overall timeline of keyword usage and red segments highlighting the burst periods of high research focus. |
Discussion
Knowledge Framework
The results indicate that the research process of exercise interventions for MCI is complex. Establishing a comprehensive and intuitive knowledge framework is essential for helping researchers quickly and accurately grasp the core content of this field. This will greatly facilitate a deeper understanding of exercise intervention research for MCI and promote further studies. Figure 11 illustrates this knowledge framework.
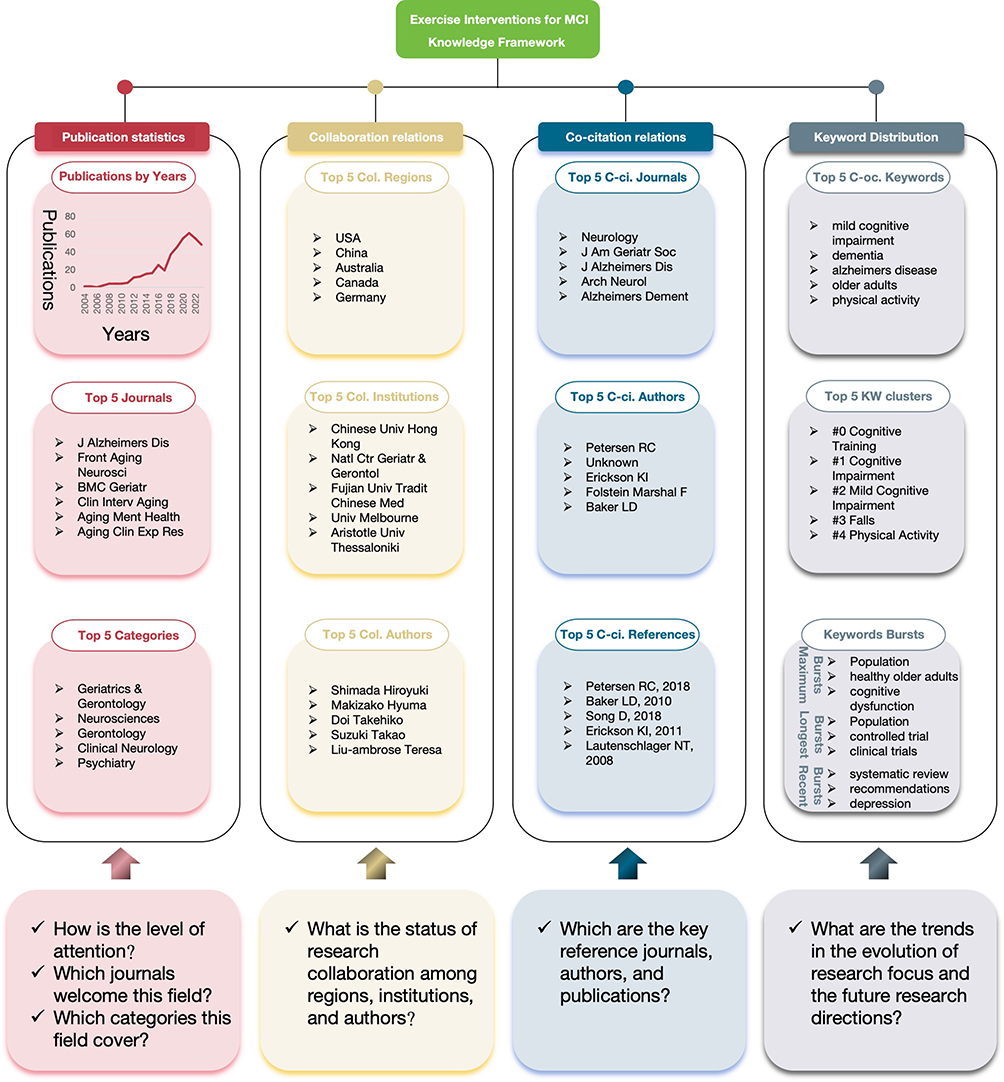 |
Figure 11 Knowledge Framework for Research on Exercise Interventions for MCI. This figure illustrates the knowledge framework of research on exercise interventions for MCI, covering four key areas: Publication Statistics, showing publication trends, top journals, and research categories; Collaboration Relations, highlighting key regions, institutions, and authors; Co-citation Relations, identifying influential journals, authors, and references; and Keyword Distribution, presenting co-occurring keywords, clusters, and bursts. The bottom section provides guiding questions summarizing the relevance of each domain. |
Publication statistics provide valuable insights into a research field’s current state and developmental trends. They assist scholars in understanding the discipline’s popularity and identifying the subject categories and leading journals that attract significant scholarly attention. Based on the annual publication count, research on exercise interventions for MCI can be divided into three distinct stages. The initial stage (2004–2011) was marked by a limited number of annual publications, consistently remaining in single digits (fewer than 10 publications), indicating that the field had not yet garnered widespread attention but established a foundation for future growth. In the initial growth stage (2012–2017), the annual publication count gradually stabilized in double digits, reflecting increasing academic interest. Although there was a slight decline in 2017 (19 publications), the overall trend exhibited steady growth. The rapid development stage (2018–2023) witnessed a significant surge in publications, rising from 37 publications in 2018 to a peak of 61 publications in 2021. Despite a minor decline in 2022 and 2023 (55 and 48 publications, respectively), the publication level remains notably high, underscoring the field’s robust academic potential and growing scholarly attention.
The Journal of Alzheimer’s Disease leads with 29 publications (6.90% of the total), followed by Frontiers in Aging Neuroscience with 21 publications (5.00%) and BMC Geriatrics with 14 publications (3.33%). Additionally, other notable journals such as Clinical Interventions in Aging with 10 publications (2.38%), Aging & Mental Health with 9 publications (2.14%), and Aging Clinical and Experimental Research with 9 publications (2.14%) play important roles in the field. Overall, the majority of publications appear in Q2 journals with impact factors ranging from 2.1 to 8.3, indicating a solid middle-tier research presence in the field. However, there remains room for improvement in the publication of research findings in high-impact journals. Future studies should prioritize high-quality and innovative research, aiming to contribute to top-tier journals to enhance the visibility and impact of this field.
Among the research categories, “Geriatrics & Gerontology” leads with 189 publications (45.00%), followed by “Neurosciences” with 109 publications (25.95%), and “Gerontology” with 87 publications (20.71%). “Clinical Neurology” and “Psychiatry” rank fourth and fifth, respectively. Categories such as “Geriatrics & Gerontology” and “Medicine, General & Internal” demonstrate high intermediary centrality, indicating their role as primary bridges within the academic network. Early research efforts were concentrated in “Clinical Neurology”, “Geriatrics & Gerontology”, “Gerontology”, and “Psychiatry”, but over time, there has been increased diversity in research categories. Overall, the field of exercise interventions for MCI has developed a core foundation centered around “Geriatrics & Gerontology”, “Neurosciences”, and “Medicine, General & Internal”, while also integrating interdisciplinary elements from “Gerontology”, “Clinical Neurology”, “Psychiatry”, and other related fields.
Collaborative networks among regions, institutions, and authors are essential for advancing research in any field. These networks reveal the collaboration patterns that drive progress and innovation. Regional analysis reveals distinct research concentration patterns in the field of exercise interventions for MCI. The leading collaborative regions include the USA, China, Australia, Canada, Germany, and Japan with their dominance attributed to two main factors: aging demographics and research infrastructure. These countries face significant challenges from their aging populations, with a high prevalence of MCI, creating urgent demographic-driven demand for research.41 Additionally, their well-established research institutions and funding systems facilitate extensive collaborative networks.42 However, the absence of African countries among the top ten collaborating regions highlights a significant geographical disparity in research capacity and engagement. This suggests potential opportunities for expanding international collaboration to address cognitive health challenges in developing regions.
Key institutions in this collaborative network demonstrate distinct research patterns and collaborative strategies. Leading institutions include the Chinese University of Hong Kong and Fujian University of Traditional Chinese Medicine (representing Chinese institutions), the National Center for Geriatrics and Gerontology (representing Japanese institutions), the University of Melbourne and Aristotle University Thessaloniki (representing Western institutions). Chinese institutions emphasize research on traditional mind-body exercises for MCI, leveraging their cultural heritage in traditional medicine.43,44 Meanwhile, Japanese institutions maintain strong domestic collaborative networks, focusing on nation-specific aging challenges.45,46 In contrast, Western research institutions adopt a broader approach with extensive international collaborations across multiple disciplines, facilitating comprehensive research on MCI interventions.47,48 These institutions reflect diverse collaborative strategies that enhance the field through unique regional approaches.
Analysis of author collaborations reveals interesting patterns in research team dynamics. While authors such as Shimada, Makizako, Doi, Suzuki, and Liu demonstrate high publication output, their collaboration networks show unique characteristics. Notably, all these leading authors exhibit zero intermediary centrality, indicating a pattern of isolated collaborative clusters rather than broadly interconnected networks. This collaborative pattern appears to be influenced by several factors. First, the prevalence of intra-institutional collaboration likely stems from practical advantages: shared research facilities, ease of communication, and aligned research objectives.49 Second, the field’s relatively early developmental stage may contribute to limited inter-institutional collaboration as research teams focus on establishing their methodologies and expertise.50 Third, competitive pressures in this emerging field might discourage extensive cross-institutional networking, leading to relatively isolated research clusters.50
Co-citation analysis is a powerful tool for identifying influential journals, authors, and literature within a research field by revealing seminal contributions that have shaped its development. In the field of exercise interventions for MCI, co-citation analysis identifies five key reference journals: Neurology, Journal of the American Geriatrics Society, Journal of Alzheimer’s Disease, Archives of Neurology, and Alzheimer’s & Dementia. Among these, four journals are classified in Q1, while the Journal of Alzheimer’s Disease is in Q2. Although these journals exhibit relatively low intermediary centrality, indicating a more specialized focus within their field rather than broad interdisciplinary connections, their strong co-cited footprint underscores their importance as authoritative sources of domain-specific expertise. Consequently, researchers are encouraged to engage closely with the insights and methodologies documented in these highly co-cited journals, as they offer authoritative and well-established perspectives that have significantly contributed to advancing the treatment of MCI through exercise interventions.
Prominent researchers have made distinct yet complementary contributions to advancing the field of exercise interventions for MCI. Dr. Petersen is the most frequently co-cited researcher, primarily due to his groundbreaking 1999 publication, “Mild Cognitive Impairment: Clinical Characterization and Outcome”. This seminal work established the fundamental clinical characteristics and diagnostic criteria of MCI, creating an essential framework that has guided subsequent research development.33 Following Dr. Petersen’s foundational work, other leading researchers have explored different aspects of the field: Dr. Erickson’s research illuminates the relationship between physical activity and brain health, particularly emphasizing exercise-induced hippocampal growth and memory enhancement in older adults.51,52 Dr. Folstein is a distinguished psychiatrist and researcher renowned for his groundbreaking contributions to cognitive function assessment. His most notable achievement was the development of the Mini-Mental State Examination (MMSE), which he created in collaboration with his colleagues.53 The MMSE has become a widely recognized and standardized tool for evaluating patients’ cognitive function. Additionally, Dr. Baker has advanced the field through rigorous RCTs investigating exercise and lifestyle interventions for cognitive decline and Alzheimer’s disease (AD) prevention.54,55 These researchers have laid a robust foundation for MCI intervention studies, each adding unique insights that enhance the field’s depth and breadth.
The analysis of highly co-cited references reveals the theoretical foundation in exercise interventions for MCI. The most influential reference is a systematic review updating the 2001 AAN practice guidelines, comprehensively examining MCI prevalence, prognosis, and treatment approaches.5 A controlled trial found that high-intensity aerobic exercise has gender-specific benefits for older adults with MCI, with women showing more significant improvements in executive function and metabolic indicators. This provides important insights for exercise intervention strategies.54 The third most co-cited reference systematically evaluates the impact of physical exercise on MCI patients, highlighting aerobic exercise’s positive effects on overall cognition while noting uncertainties in domain-specific cognitive and psychological outcomes.56 Further evidence is provided by the fourth and fifth ranked studies, demonstrating two critical findings: moderate improvements in cognitive function among elderly individuals at risk for AD through physical activity and increased hippocampal volume with enhanced memory through aerobic exercise, effectively countering age-related brain atrophy.57,58 Collectively, these foundational studies establish a robust framework for understanding the impact of exercise on cognitive health in MCI patients.
The top five keywords in co-occurrence frequency reflect the core themes in exercise interventions for MCI. As an intermediate state between normal aging and dementia, “mild cognitive impairment” often serves as an early indicator of cognitive decline, with a high risk of progression to “dementia”.59 Characterized by persistent neurodegeneration, dementia manifests through gradual declines in memory, language, reasoning, and judgment abilities.60 This cognitive deterioration progressively impairs daily functioning, ultimately leading to a complete loss of self-care abilities. Among various types of dementia, “Alzheimer’s disease” is the most prevalent form, which typically begins with MCI symptoms. Given that aging brings about the gradual deterioration of physiological functions and nervous system decline, “older adults” are particularly susceptible to MCI and dementia.61 In response to these cognitive challenges, “physical activity” interventions have emerged as promising. Through appropriate physical activity, these interventions can enhance blood circulation and promote neuronal growth, thereby supporting and strengthening cognitive function through various mechanisms.62,63
The Cognitive Training cluster (#0), emerging in 2009, focuses on improving or delaying cognitive decline through combined physical and cognitive training, as indicated by keywords such as “cognitive decline”, “validation”, and “exercise intervention”.64 The Cognitive Impairment cluster (#1) highlights the relationship between exercise interventions and the broad term “cognitive impairment”, supported by keywords such as “Alzheimer’s disease”, “brain plasticity”, and “controlled trial”.65 The Mild Cognitive Impairment cluster (#2), the longest-lasting cluster, explores the progression from MCI to dementia, with a focus on neurodegenerative changes, reflected in keywords such as “older adults”, “dementia”, and “brain atrophy”.66 The Falls cluster (#3) emphasizes preventing falls in older adults through balance, gait, and physical fitness training, featuring “balance”, “gait”, and “physical training” as keywords.67 The Physical Activity cluster (#4) underscores the role of physical activity, particularly aerobic training, in enhancing cognitive and mental health, with keywords such as “exercise”, “aerobic training”, and “cognitive stimulation”.68 The Network Meta-Analysis cluster (#5) focuses on synthesizing evidence to evaluate intervention outcomes for MCI, with key terms including “systematic review”, “management”, and “depressive symptoms”.69 The Cardiorespiratory Fitness cluster (#6) highlights the positive effects of aerobic exercise on physical performance and quality of life, with keywords including “life”, “exercise performance”, and “aerobic exercise”.70 The Age cluster (#7) addresses aging-related concerns, such as depression, memory decline, and neurodegenerative diseases, represented by “depression”, “implicit memory”, and “Parkinson’s disease”.71 The Sports Medicine cluster (#8) explores the effects of exercise on brain health, with keywords like “aerobic fitness”, “brain volume”, and “diagnostic guidelines”.72 The Brain-Derived Neurotrophic Factor cluster (#9) emphasizes the role of Brain-Derived Neurotrophic Factor (BDNF) in promoting neural plasticity and cognitive function, particularly through resistance training, as reflected by “resistance exercise”, “plasticity”, and “strength”.73 Finally, the Tai Chi cluster (#10) focuses on the benefits of mind-body exercises such as Tai Chi for community-dwelling older adults, highlighting its effects on physical health, mental relaxation, and acceptability, with keywords like “dwelling older adults”, “yoga”, and “acceptability”.74
The keyword “population” exhibited the highest burst strength (4.87) during the period 2008–2016, reflecting the significant academic focus on the target population’s characteristics, particularly the identification of high-risk groups for MCI. Following this, the keyword “healthy older adults” (burst strength 4.19) emphasized the importance of healthy aging, with the healthy elderly population often serving as a control group to assess the effects of exercise interventions.75 Meanwhile, the keyword “cognitive dysfunction” (burst strength 4.13) experienced a significant burst from 2020–2023, underscoring the growing global concern regarding cognitive impairment and driving research efforts to improve cognitive function in MCI patients.76 In addition, the keywords “controlled trial” and “clinical trials” closely followed in burst duration after “population”. Specifically, “controlled trial” exhibited a burst between 2009–2014, while “clinical trials” maintained a continuous burst from 2013–2018. These trends reflect the increasing academic emphasis on controlled trial and robust clinical trial designs, highlighting their role in validating the effectiveness and reliability of exercise interventions for MCI patients.77,78 The newly burst keywords “systematic review”, “recommendations”, and “depression” provide important insights into recent research trends. “Systematic review” (2021–2023) demonstrates the academic community’s commitment to systematically integrating existing research evidence, ensuring the provision of high-quality evidence for MCI exercise intervention studies.76 The keyword “recommendations” underscores the focus on developing practice guidelines and intervention strategies, facilitating the translation of research findings into clinical applications.79 Simultaneously, “depression” highlights the critical need to address psychological health issues in MCI patients, particularly given the high prevalence of depression and its bidirectional relationship with cognitive decline.69
Research Focus
Through an in-depth analysis of publication statistics, collaborative relationships, co-occurrence relationships, and keyword distribution, this article reveals the progress and trends in exercise interventions for MCI. Through cluster names and keywords such as “Physical activity”, “Tai Chi”, and “Multicomponent Exercise”, the research focus can be summarized as the design of exercise interventions. Additionally, the emergence of keywords and clusters like “Brain volume”, “Cardiorespiratory Fitness”, and “Brain-Derived Neurotrophic Factor” further indicates that understanding the mechanisms of action of exercise interventions is also a major focus of research in this field.
The first factor to consider in the design of exercise interventions is the type of exercise, as it directly influences the effectiveness and specificity of the intervention measures. Exercise interventions can be broadly categorized into single-modality and multicomponent approaches. In single-modality interventions, aerobic exercises, including daily activities (eg, brisk walking, stair climbing, household chores) and mind-body exercises (eg, Tai Chi, Baduanjin, and square dancing), have demonstrated significant cognitive benefits for MCI patients, though with varying effects.74,80–82 For example, studies have shown that Tai Chi can improve overall cognitive function and enhance cognitive flexibility compared to conventional exercise programs.83 Similarly, Baduanjin has been found to increase attention levels by 12% compared to brisk walking.44 Additionally, another randomized controlled trial indicated that a 6-week intervention using Xbox 360 Kinect exergames significantly improved executive function and cognitive performance in patients with MCI, further demonstrating the positive effects of single-modality exercise on cognitive domains.84 However, research suggests that multicomponent exercise interventions, which incorporate diverse activities, have more pronounced effects on cognitive function improvement in MCI patients.85 Building on this understanding, researchers have developed combined interventions that integrate exercise with cognitive training. This integrated approach aims to comprehensively enhance various cognitive functions—including memory, attention, executive function, and spatial abilities—through the simultaneous engagement of physical and cognitive tasks.86 Research consistently demonstrates that such combined interventions surpass single-modality exercise interventions in cognitive enhancement efficacy.64,86 As technology advances, innovative combined approaches continue to emerge, exemplified by the integration of Tai Chi with transcranial direct current stimulation, which showed superior efficacy in improving dual-task gait performance compared to Tai Chi alone.87 These findings suggest that both single-modality and multicomponent exercise interventions have potential benefits, with different types of exercises targeting specific cognitive domains, while multicomponent exercise interventions provide more comprehensive cognitive improvements due to their diversity.
In addition to the type of exercise, a key parameter in the design of an exercise intervention is exercise intensity. According to the physical activity guidelines issued by the World Health Organization (WHO), it is recommended that older adults engage in 150 to 300 minutes of moderate-intensity aerobic exercise or 75 to 150 minutes of high-intensity aerobic exercise weekly to promote cognitive enhancement.88 When designing exercise interventions for MCI patients, adherence to the exercise regimen is a crucial consideration that directly impacts long-term outcomes. Research indicates that moderate-intensity aerobic exercise programs achieve approximately 80% adherence rates, which is notably higher than those observed for high-intensity exercise programs. This higher adherence rate suggests that moderate-intensity interventions may be more sustainable for MCI patients in the long term.85 To evaluate the impact of different intensities of aerobic exercise recommended by the WHO on cognitive function in MCI patients, Yu et al conducted a randomized controlled trial. The study found that both 150 minutes of moderate-intensity exercise and 75 minutes of high-intensity exercise per week yielded similar cognitive improvements in MCI patients.89 Baker et al’s research showed that high-intensity aerobic exercise can improve executive function and metabolism in MCI, with significant sex-specific benefits favoring women.54 Additionally, Song et al found that moderate-intensity aerobic exercise not only improves cognitive function but also enhances the overall quality of life for MCI patients by improving sleep quality and reducing stress levels.90 In summary, while both moderate- and high-intensity exercises offer cognitive benefits, moderate-intensity exercise may provide a better balance of cognitive improvements, quality-of-life benefits, and adherence, making it a potentially optimal choice for long-term interventions in MCI patients.
Exercise frequency is also a factor affecting the efficacy of exercise interventions; however, the minimum exercise frequency that positively impacts patients with MCI remains unclear. According to the guidelines for MCI released by the American Academy of Neurology, it is recommended that MCI patients engage in exercise at least twice a week to enhance cognitive abilities.5 A randomized controlled trial demonstrated that combined aerobic and resistance training conducted twice a week for 60 minutes each session over a period of 12 weeks can significantly improve cognitive function and physical health outcomes in MCI patients.91 In another intervention study, dance training three times a week for 45 minutes each session over 12 weeks has been shown to markedly enhance cognitive function, particularly in episodic memory and processing speed.92 Furthermore, a prospective study revealed that aerobic training five times a week for 40–50 minutes over six weeks yielded significant improvements in the neurocognitive function of MCI patients, as measured by standardized cognitive assessments.93 From these studies, it is evident that exercise interventions occurring two to five times a week can positively affect MCI patients, but the effectiveness is interdependent on the duration, type, and intensity of the exercise. Therefore, when determining the frequency of exercise interventions for MCI patients, it is essential to consider individual differences and specific intervention measures, adopting a flexible and personalized approach to achieve optimal outcomes.
Exercise duration is another key factor, encompassing both the duration of each individual exercise intervention and the overall duration of the entire intervention. Studies show that the duration of each intervention session directly affects adherence among MCI patients. When sessions are limited to 30–60 minutes, adherence rates remain high.90 However, adherence progressively declines as the duration of each session extends beyond 60 minutes.62 For the total intervention duration, research indicates that specific time requirements vary based on exercise intensity. To achieve meaningful cognitive improvements, at least 1200 minutes of moderate-intensity exercise is necessary.93 In comparison, high-intensity exercise may require slightly less time, around 900 minutes, to yield similar benefits.54 This is consistent with WHO physical activity guidelines, which suggest adjusting the total exercise duration according to intensity to maximize intervention effectiveness.
Additionally, beyond the design of exercise interventions, researchers have increasingly focused on exploring their underlying mechanisms in recent years. Although various hypotheses have been proposed from different perspectives to explain these processes, the mechanisms through which exercise interventions influence MCI are not yet fully understood. Current research primarily investigates these mechanisms at the cellular and molecular level, the perspective of brain structure and functional changes, and the perspective of overall physiological regulation.
At the cellular and molecular level, the mechanisms by which exercise impacts MCI have several key aspects. First, exercise may promote the release of neurotrophic factors from nerve cells, particularly BDNF. BDNF is essential for supporting the growth of nerve cells, synaptogenesis, and synaptic plasticity, which may contribute to improvements in memory and executive function in patients with MCI.94 Second, exercise may enhance neural network connectivity by modulating synaptic plasticity. Following 12 weeks of exercise intervention, the functional connectivity of the hippocampus in MCI patients was found to be significantly improved, which positively affected cognitive functions such as learning and memory.95 Third, exercise may stimulate neurogenesis, especially in brain regions associated with this process, such as the hippocampus, where new neurons can form new synaptic connections. This neurogenesis provides the brain with a capacity for self-repair and adaptation, thereby contributing to the recovery and enhancement of cognitive functions.62 These cellular and molecular mechanisms work synergistically to enhance brain plasticity and cognitive function in MCI patients, highlighting the profound impact of exercise on brain health.
From the perspective of brain structure and functional changes, research has established a close relationship between exercise and alterations in brain gray matter volume, particularly in the hippocampal region. Tao et al demonstrated that a 24-week Baduanjin intervention significantly improved cognitive function in individuals with MCI, potentially associated with increased hippocampal and ACC gray matter volume and enhanced functional connectivity.81 Additionally, exercise may enhance the microstructure of white matter through several mechanisms. First, exercise may stimulate the growth and branching of nerve fibers, thereby increasing the density of nerve fibers in white matter regions. Second, exercise may improve the structural integrity of nerve fibers, reducing the risk of damage that could result in fiber injury.63 These changes are essential for enhancing information transmission and coordination between different brain regions. Moreover, exercise may positively impact functional connectivity between various brain areas, improving the integration of functional networks and thereby enhancing the collaborative efficiency of different brain regions during cognitive processes.96 This increased integration of functional networks optimizes the flow of information within the brain, leading to more efficient collaboration among brain regions when executing cognitive tasks. Together, these exercise-induced changes in gray matter volume, white matter microstructure, and functional connectivity demonstrate the comprehensive impact of exercise on brain structure and function, ultimately contributing to improved cognitive performance in elderly individuals.
From the perspective of overall physiological regulation, exercise can significantly enhance cardiac pumping efficiency and increase blood circulation, particularly cerebral blood flow, thereby delivering more oxygen and nutrients to brain tissue. This mechanism helps maintain the normal function of nerve cells, enabling exercise training to effectively improve cognitive abilities in patients with MCI.92 Additionally, exercise’s role in regulating inflammation levels and the immune system may have profound effects on the pathological processes underlying MCI. This is because chronic inflammation is closely linked to cognitive decline, and exercise can reduce systemic inflammation, mitigating its adverse effects on the brain, thereby helping to maintain cognitive stability and promote brain health.97 Furthermore, exercise may protect brain function by enhancing the activity of the body’s antioxidant defense system. Specifically, multicomponent exercises can stimulate the production of antioxidants, which neutralize free radicals and reduce oxidative stress-induced damage to nerve cells, thereby supporting the health of neural tissue.98 This process may play a crucial protective role in slowing brain aging and reducing the risk of neurological diseases. Collectively, these physiological mechanisms, including enhanced cerebral blood flow, reduced inflammation, and improved antioxidant defense, work together to create an optimal environment for brain health and the maintenance of cognitive function in MCI patients.
Future Research Characteristics
Research on exercise interventions for MCI continues to advance rapidly, and understanding potential future directions is crucial for guiding subsequent studies. Based on the above analysis, future studies in this field are expected to exhibit the following characteristics:
The study of exercise interventions for MCI is increasingly recognized as an interdisciplinary field. Within this context, gerontology and geriatrics are pivotal, providing comprehensive insights into the health status of older adults and forming the basis for the design of scientifically rigorous and holistic intervention programs. Concurrently, neuroscience contributes to a critical understanding of the biological mechanisms underlying MCI, particularly about brain function and structural changes, thereby offering essential tools for exploring the intricate relationship between exercise and cognitive decline. Disciplines such as clinical neurology, psychiatry, and sports science have also significantly contributed to this field. Moving forward, an even broader range of disciplines will likely become involved in investigating exercise interventions for MCI. For instance, motivational theories from behavioral science could be leveraged to design more engaging exercise programs that promote consistent participation among MCI patients. Similarly, advances in cell biology could elucidate how exercise specifically enhances or restores cognitive function at the cellular level, providing robust scientific evidence for future clinical applications. These interdisciplinary efforts will drive the continued advancement of research on exercise interventions for MCI.
Future research collaborations are anticipated to become more extensive. At the national level, scientific collaboration among geographically proximate countries will likely intensify. For example, despite their high research output in this field, collaboration among China, Japan, and South Korea remains limited. These nations are well-positioned to develop synergistic research partnerships given their shared cultural backgrounds. Strengthening these collaborations would enhance their collective influence and visibility on the international stage. At the institutional level, collaboration between different types of research organizations is expected to be further reinforced, maximizing the unique strengths of each entity. Universities provide multidisciplinary environments, medical institutions offer access to rich clinical data and patient populations, and research institutes contribute specialized expertise and independence. These diverse organizations can drive innovation, accelerate research progress, and generate broader social and academic impacts by working together. At the author level, cross-institutional collaboration is expected to increase, fostering knowledge and resource sharing, enhancing research diversity, and improving the impact of scholarly outputs. With advancements in communication technologies and the expansion of collaborative networks, more researchers will have the opportunity to transcend institutional boundaries and collaboratively address complex scientific challenges. The development of collaboration at the national, institutional, and individual levels will create a more integrated and efficient research ecosystem, ultimately accelerating advances in exercise interventions for MCI.
Future research is likely to delve deeper into emerging topics, focusing on integrating exercise interventions with other approaches, such as cognitive training, behavioral therapy, and technological innovations, to develop comprehensive strategies for managing MCI. For example, combining physical exercise with digital tools, such as exergames or virtual reality, can enhance patient engagement and improve cognitive function and daily performance through multidimensional stimulation. A greater emphasis will be placed on systematically synthesizing existing evidence through systematic reviews and meta-analyses to evaluate the efficacy of different exercise modalities, thereby providing high-quality evidence to guide clinical practice. Additionally, future studies will increasingly address MCI patients within specific populations, such as those with depression, cardiovascular diseases, or other comorbidities. Given the complexity of cognitive impairments in these groups, research will focus on tailored intervention strategies, incorporating individualized assessments and multidisciplinary collaborations to enhance effectiveness and optimize long-term outcomes.
Limitations
This study has several limitations related to its data sources and analytical methods. First, the study relied solely on the Web of Science Core Collection database and included only English-language publications, which may have excluded relevant research published in other languages or available in alternative databases, thereby limiting the comprehensiveness of the findings. Second, although bibliometric visualization analysis effectively highlights research trends and progress, it has inherent limitations in evaluating the specific efficacy of exercise interventions. Furthermore, the visualization charts, constrained by the large volume of data, could only display representative and prominent nodes, which may have resulted in the omission of some relevant nodes.
Conclusion
Research on exercise interventions for MCI has been receiving increasing attention and has gradually become an interdisciplinary field intersecting geriatrics, gerontology, and neuroscience. Relevant studies are primarily concentrated in specific journals, demonstrating a certain degree of academic clustering. In the collaboration network, developed countries dominate, and inter-institutional collaborations exhibit specific and regular patterns, while collaborations among authors are more focused within institutions. Highly co-cited journals, authors, and publications provide critical theoretical support and practical experience for the development of this field. Current research mainly revolves around the design and mechanisms of exercise intervention programs. Future research will focus on three key areas: developing comprehensive interventions that combine exercise with other approaches, systematically integrating existing evidence, and conducting personalized intervention studies for specific populations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World population prospects 2022: summary of results [homepage on the Internet]. United Nations; 2022. Available from: https://www.un.org/development/desa/pd/content/World-Population-Prospects-2022.
2. Olivari BS, French ME, McGuire LC. The public health road map to respond to the growing dementia crisis. Innov Aging. 2020;4(1):1–11. doi:10.1093/geroni/igz043
3. World health statistics 2021: monitoring health for the SDGs, sustainable development goals [homepage on the Internet]. World Health Organization; 2021. Available from: https:/www.who.int/publications/i/item/9789240027053.
4. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256(3):183–194. doi:10.1111/j.1365-2796.2004.01388.x
5. Petersen RC, Lopez O, Armstrong MJ, et al. Practice guideline update summary: mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2018;90(3):126. doi:10.1212/wnl.0000000000004826
6. Tschanz JT, Welsh-Bohmer KA, Lyketsos CG, et al. Conversion to dementia from mild cognitive disorder: the Cache County Study. Neurology. 2006;67(2):229–234. doi:10.1212/01.wnl.0000224748.48011.84
7. Hendriks S, Peetoom K, Bakker C, et al. Global prevalence of young-onset dementia: a systematic review and meta-analysis. JAMA Neurol. 2021;78(9):1080–1090. doi:10.1001/jamaneurol.2021.2161
8. Glumac S, Kardum G, Sodic L, et al. Effects of dexamethasone on early cognitive decline after cardiac surgery: a randomised controlled trial. Eur J Anaesthesiol. 2017;34(11):776–784. doi:10.1097/EJA.0000000000000647
9. Simon SS, Yokomizo JE, Bottino CM. Cognitive intervention in amnestic mild cognitive impairment: a systematic review. Neurosci Biobehav Rev. 2012;36(4):1163–1178. doi:10.1016/j.neubiorev.2012.01.007
10. Ahmadzadeh M, Christie GJ, Cosco TD, Moreno S. Neuroimaging and analytical methods for studying the pathways from mild cognitive impairment to Alzheimer’s disease: protocol for a rapid systematic review. Syst Rev. 2020;9(1):1–6. doi:10.1186/s13643-020-01332-7
11. Graham SA, Lee EE, Jeste DV, et al. Artificial intelligence approaches to predicting and detecting cognitive decline in older adults: a conceptual review. Psychiatry Res. 2020;284:112732. doi:10.1016/j.psychres.2019.112732
12. Zhao X, Yuan L, Feng L, et al. Association of dietary intake and lifestyle pattern with mild cognitive impairment in the elderly. J Nutr Health Aging. 2015;19(2):164–168. doi:10.1007/s12603-014-0524-2
13. Iizuka A, Suzuki H, Ogawa S, et al. Does social interaction influence the effect of cognitive intervention program? A randomized controlled trial using Go game. Int J Geriatr Psychiatry. 2019;34(2):324–332. doi:10.1002/gps.5024
14. Demurtas J, Schoene D, Torbahn G, et al. Physical activity and exercise in mild cognitive impairment and dementia: an umbrella review of intervention and observational studies. J Am Med Dir Assoc. 2020;21(10):1415–1422. doi:10.1016/j.jamda.2020.08.031
15. Veronese N, Soysal P, Demurtas J, et al. Physical activity and exercise for the prevention and management of mild cognitive impairment and dementia: a collaborative international guideline. Eur Geriatr Med. 2023;14(5):925–952. doi:10.1007/s41999-023-00858-y
16. Montero-Odasso M, Almeida QJ, Burhan AM, et al. SYNERGIC TRIAL (synchronizing exercises, remedies in gait and cognition): a multi-centre randomized controlled double-blind trial to improve gait and cognition in mild cognitive impairment. BMC Geriatr. 2018;18(1):1–15. doi:10.1186/s12877-018-0782-7
17. Poinsatte K, Smith EE, Torres VO, et al. T and B cell subsets differentially correlate with amyloid deposition and neurocognitive function in patients with amnestic mild cognitive impairment after one year of physical activity. Exerc Immunol Rev. 2019;25:34.
18. Tomoto T, Liu J, Tseng BY, et al. One-year aerobic exercise reduced carotid arterial stiffness and increased cerebral blood flow in amnestic mild cognitive impairment. J Alzheimer's Dis. 2021;80(2):841–853. doi:10.3233/JAD-201456
19. Xia R, Wan M, Lin H, et al. Effects of mind-body exercise Baduanjin on cognition in community-dwelling older people with mild cognitive impairment: a randomized controlled trial. Neuropsychol Rehabil. 2023;33(8):1368–1383. doi:10.1080/09602011.2022.2099909
20. Davis JC, Bryan S, Marra CA, et al. An economic evaluation of resistance training and aerobic training versus balance and toning exercises in older adults with mild cognitive impairment. PLoS One. 2013;8(5):e63031. doi:10.1371/journal.pone.0063031
21. Broadhouse KM, Singh MF, Suo C, et al. Hippocampal plasticity underpins long-term cognitive gains from resistance exercise in MCI. Neuroimage Clin. 2020;25:102182. doi:10.1016/j.nicl.2020.102182
22. Di Lorito C, Bosco A, Booth V, et al. Adherence to exercise interventions in older people with mild cognitive impairment and dementia: a systematic review and meta-analysis. Prev Med Rep. 2020;19:101139. doi:10.1016/j.pmedr.2020.101139
23. Bray NW, Pieruccini-Faria F, Witt ST, et al. Combining exercise with cognitive training and vitamin D3 to improve functional brain connectivity (FBC) in older adults with mild cognitive impairment (MCI): results from the SYNERGIC trial. GeroScience. 2023;45(3):1967–1985. doi:10.1007/s11357-023-00805-6
24. Xu Y, Zhu J, Liu H, et al. Effects of Tai Chi combined with tDCS on cognitive function in patients with MCI: a randomized controlled trial. Front Public Health. 2023;11:1199246. doi:10.3389/fpubh.2023.1199246
25. Zhang J, Liu X, Huang J, Huang S, Zhang Z. Research trends of specialty nurse training from 2003 to 2023: a bibliometric analysis via CiteSpace. J Multidiscip Healthc. 2024;17:4839–4850. doi:10.2147/JMDH.S490597
26. Yi Q, Wang S, Feng X, et al. Global trends and hotspots of exercise interventions for mild cognitive impairment: a global bibliometric analysis. Medicine. 2024;103(37):e39550. doi:10.1097/MD.0000000000039550
27. Zhang J, Yang Z, Fan H. Knowledge structure and future research trends of body–mind exercise for mild cognitive impairment: a bibliometric analysis. Front Neurol. 2024;15:1351741. doi:10.3389/fneur.2024.1351741
28. Donthu N, Kumar S, Mukherjee D, Pandey N, Lim WM. How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. 2021;133:285–296. doi:10.1016/j.jbusres.2021.04.070
29. Montazeri A, Mohammadi S, Hesari PM, et al. Preliminary guideline for reporting bibliometric reviews of the biomedical literature (BIBLIO): a minimum requirements. Syst Rev. 2023;12(1):239. doi:10.1186/s13643-023-02410-2
30. Liu T, Li Y, Li J, et al. Temporal trend and research focus of injury burden from 1998 to 2022: a bibliometric analysis. J Multidiscip Healthc. 2023;16:1869–1882. doi:10.2147/JMDH.S414859
31. Luo C, Mao B, Wu Y, et al. The research hotspots and theme trends of artificial intelligence in nurse education: a bibliometric analysis from 1994 to 2023. Nurse Educ Today. 2024;141:106321. doi:10.1016/j.nedt.2024.106321
32. Reisberg B, Ferris SH, Kluger A, et al. Mild cognitive impairment (MCI): a historical perspective. Int Psychogeriatr. 2008;20(1):18–31. doi:10.1017/S1041610207006394
33. Petersen RC, Smith GE, Waring SC, et al. Mild cognitive impairment: clinical characterization and outcome. Arch Neurol. 1999;56(3):303–308.76. doi:10.1001/archneur.56.3.303
34. Bermejo-Pareja F, Contador I, Del Ser T, et al. Predementia constructs: mild cognitive impairment or mild neurocognitive disorder? A narrative review. Int J Geriatr Psychiatry. 2021;36(5):743–755. doi:10.1002/gps.5474
35. Chan AT, Ip RT, Tran JY, et al. Computerized cognitive training for memory functions in mild cognitive impairment or dementia: a systematic review and meta-analysis. NPJ Digit Med. 2024;7(1):1. doi:10.1038/s41746-023-00987-5
36. Chen B, Fu Y, Song G, et al. Research trends and hotspots of exercise for Alzheimer’s disease: a bibliometric analysis. Front Aging Neurosci. 2022;14:984705. doi:10.3389/fnagi.2022.984705
37. Higgins JPT, Thomas J, Chandler J, et al. eds.. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.5. Updated August 2024. Cochrane; 2024. Available from https:/www.training.cochrane.org/handbook.
38. McGowan J, Sampson M, Salzwedel DM, et al. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. 2016;75:40–46. doi:10.1016/j.jclinepi.2016.01.021
39. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
40. Zhang R, Ge Y, Xia L, et al. Bibliometric analysis of development trends and research hotspots in the study of data mining in nursing based on CiteSpace. J Multidiscip Healthc. 2024;17:1561–1575. doi:10.2147/JMDH.S459079
41. Bai W, Chen P, Cai H, et al. Worldwide prevalence of mild cognitive impairment among community dwellers aged 50 years and older: a meta-analysis and systematic review of epidemiology studies. Age Ageing. 2022;51(8):afac173. doi:10.1093/ageing/afac173
42. Fabre R, Egret D, Schöpfel J, Azeroual O. Evaluating the scientific impact of research infrastructures: the role of current research information systems. Quant Sci Stud. 2021;2(1):42–64. doi:10.1162/qss_a_00111
43. Siu MY, Lee DT. Effects of tai chi on cognition and instrumental activities of daily living in community-dwelling older people with mild cognitive impairment. BMC Geriatr. 2018;18(1):1–10. doi:10.1186/s12877-018-0720-8
44. Xia R, Qiu P, Lin H, et al. The effect of traditional Chinese mind-body exercise (Baduanjin) and brisk walking on the dorsal attention network in older adults with mild cognitive impairment. Front Psychol. 2019;10:2075. doi:10.3389/fpsyg.2019.02075
45. Uemura K, Shimada H, Makizako H, et al. Cognitive function affects trainability for physical performance in exercise intervention among older adults with mild cognitive impairment. Clin Interv Aging. 2013;8:97–102. doi:10.2147/CIA.S39434
46. Doi T, Makizako H, Shimada H, et al. Effects of multicomponent exercise on spatial-temporal gait parameters among the elderly with amnestic mild cognitive impairment (aMCI): preliminary results from a randomized controlled trial. Arch Gerontol Geriatr. 2013;56(1):104–108. doi:10.1016/j.archger.2012.09.003
47. Lautenschlager NT, Cox K, Kurz AF. Physical activity and mild cognitive impairment and Alzheimer’s disease. Curr Neurol Neurosci Rep. 2010;10(5):352–358. doi:10.1007/s11910-010-0121-7
48. González-Palau F, Franco M, Bamidis P, et al. The effects of a computer-based cognitive and physical training program in a healthy and mildly cognitive impaired aging sample. Aging Mental Health. 2014;18(7):838–846. doi:10.1080/13607863.2014.899972
49. Katz JS, Martin BR. What is research collaboration? Res Policy. 1997;26(1):1–18. doi:10.1016/S0048-7333(96)00917-1
50. Georghiou L. Global cooperation in research. Res Policy. 1998;27(6):611–626. doi:10.1016/S0048-7333(98)00054-7
51. Erickson KI, Raji CA, Lopez OL, et al. Physical activity predicts gray matter volume in late adulthood: the cardiovascular health study. Neurology. 2010;75(16):1415–1422. doi:10.1212/WNL.0b013e3181f88359
52. Erickson KI, Oberlin L, Gujral S, et al. Exercise as a way of capitalizing on neuroplasticity in late adulthood. Top Geriatr Rehabil. 2014;30(1):8–14. doi:10.1097/TGR.0000000000000008
53. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
54. Baker LD, Frank LL, Foster-Schubert K, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol. 2010;67(1):71–79. doi:10.1001/archneurol.2009.307
55. Baker LD, Bayer-Carter JL, Skinner J, et al. High-intensity physical activity modulates diet effects on cerebrospinal amyloid-β levels in normal aging and mild cognitive impairment. J Alzheimer's Dis. 2012;28(1):137–146. doi:10.3233/JAD-2011-111076
56. Song D, Doris SF, Li PW, et al. The effectiveness of physical exercise on cognitive and psychological outcomes in individuals with mild cognitive impairment: a systematic review and meta-analysis. Int J Nurs Stud. 2018;79:155–164. doi:10.1016/j.ijnurstu.2018.01.002
57. Lautenschlager NT, Cox KL, Flicker L, et al. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: a randomized trial. JAMA. 2008;300(9):1027–1037. doi:10.1001/jama.300.9.1027
58. Erickson KI, Voss MW, Prakash RS, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A. 2011;108(7):3017–3022. doi:10.1073/pnas.1015950108
59. Petersen RC. Early diagnosis of Alzheimer’s disease: is MCI too late? Curr Alzheimer Res. 2009;6(4):324–330. doi:10.2174/156720509788929237
60. Olson E. Dementia and neurodegenerative diseases. Geriatr Palliat Care. 2003;160:72.
61. Ng TP, Lee TS, Lim WS, et al. Functional mobility decline and incident mild cognitive impairment and early dementia in community-dwelling older adults: the Singapore longitudinal ageing study. Age Ageing. 2022;51(9). doi:10.1093/ageing/afac182
62. Devenney KE, Sanders ML, Lawlor B, et al. The effects of an extensive exercise programme on the progression of mild cognitive impairment (MCI): study protocol for a randomised controlled trial. BMC Geriatr. 2017;17(1):1–10. doi:10.1186/s12877-017-0457-9
63. Tarumi T, Thomas BP, Tseng BY, et al. Cerebral white matter integrity in amnestic mild cognitive impairment: a 1-year randomized controlled trial of aerobic exercise training. J Alzheimer's Dis. 2020;73(2):489–501. doi:10.3233/JAD-190875
64. Donnezan LC, Perrot A, Belleville S, et al. Effects of simultaneous aerobic and cognitive training on executive functions, cardiovascular fitness, and functional abilities in older adults with mild cognitive impairment. Ment Health Phys Act. 2018;15:78–87. doi:10.1016/j.mhpa.2018.06.001
65. Smith JC, Nielson KA, Antuono P, et al. Semantic memory functional MRI and cognitive function after exercise intervention in mild cognitive impairment. J Alzheimer's Dis. 2013;37(1):197–215. doi:10.3233/JAD-130467
66. Doe J, Smith AB, Lee C, et al. Resting cerebral blood flow after exercise training in mild cognitive impairment. J Neurol Sci. 2024;400(1):10–20. doi:10.3233/JAD-180728
67. Boulares A, Fabre C, Cherni A, et al. Effects of a physical activity program that incorporates exercises targeting balance, strength, and proprioception on cognitive functions and physical performance in old adults with mild cognitive impairment. J Alzheimer's Dis. 2023;Preprint:1–16. doi:10.3233/JAD-230305
68. Cammisuli DM, Innocenti A, Franzoni F, et al. Aerobic exercise effects upon cognition in mild cognitive impairment: a systematic review of randomized controlled trials. Arch Ital Biol. 2017;155(1–2):55–63. doi:10.12871/000398292017126
69. Liu Q, Ni W, Zhang L, et al. Comparative efficacy of various exercise interventions on depression in older adults with mild cognitive impairment: a systematic review and network meta-analysis. Ageing Res Rev. 2023;91:102071. doi:10.1016/j.arr.2023.102071
70. Yang C, Moore A, Mpofu E, et al. Effectiveness of combined cognitive and physical interventions to enhance functioning in older adults with mild cognitive impairment: a systematic review of randomized controlled trials. Gerontologist. 2020;60(8):e633–e642. doi:10.1093/geront/gnz149
71. Avenali M, Picascia M, Tassorelli C, et al. Evaluation of the efficacy of physical therapy on cognitive decline at 6-month follow-up in Parkinson disease patients with mild cognitive impairment: a randomized controlled trial. Aging Clin Exp Res. 2021;33(12):3275–3284. doi:10.1007/s40520-021-01865-4
72. Kropacova S, Mitterova K, Klobusiakova P, et al. Cognitive effects of dance-movement intervention in a mixed group of seniors are not dependent on hippocampal atrophy. J Neural Transm. 2019;126(11):1455–1463. doi:10.1007/s00702-019-02068-y
73. Ruiz-Gonzalez D, Hernandez-Martinez A, Valenzuela PL, et al. Effects of physical exercise on plasma brain-derived neurotrophic factor in neurodegenerative disorders: a systematic review and meta-analysis of randomized controlled trials. Neurosci Biobehav Rev. 2021;128:394–405. doi:10.1016/j.neubiorev.2021.05.025
74. Li F, Harmer P, Fitzgerald K, Winters-Stone K. A cognitively enhanced online Tai Ji Quan training intervention for community-dwelling older adults with mild cognitive impairment: a feasibility trial. BMC Geriatr. 2022;22(1):76. doi:10.1186/s12877-021-02747-0
75. Reiter K, Nielson KA, Smith TJ, et al. Improved cardiorespiratory fitness is associated with increased cortical thickness in mild cognitive impairment. J Int Neuropsychol Soc. 2015;21(10):757–767. doi:10.1017/S135561771500079X
76. Gómez-Soria I, Marin-Puyalto J, Peralta-Marrupe P, et al. Effects of multi-component non-pharmacological interventions on cognition in participants with mild cognitive impairment: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2022;103:104751. doi:10.1016/j.archger.2022.104751
77. Uemura K, Doi T, Shimada H, et al. Effects of exercise intervention on vascular risk factors in older adults with mild cognitive impairment: a randomized controlled trial. Dement Geriatr Cogn Disord Extra. 2012;2(1):445–455. doi:10.1159/000343486
78. Han JW, Lee H, Hong JW, et al. Multimodal cognitive enhancement therapy for patients with mild cognitive impairment and mild dementia: a multi-center, randomized, controlled, double-blind, crossover trial. J Alzheimer's Dis. 2016;55(2):787–796. doi:10.3233/JAD-160619
79. Chan WC, Lee AT, Lam LC. Exercise for the prevention and treatment of neurocognitive disorders: new evidence and clinical recommendations. Curr Opin Psychiatry. 2021;34(2):136–141. doi:10.1097/YCO.0000000000000678
80. Su K, Yuan J, Liu H, et al. The comparative effectiveness of traditional Chinese medicine exercise therapies in elderly people with mild cognitive impairment: a systematic review and network meta-analysis. Front Neurol. 2022;13:775190. doi:10.3389/fneur.2022.775190
81. Tao J, Liu J, Chen X, et al. Mind-body exercise improves cognitive function and modulates the function and structure of the hippocampus and anterior cingulate cortex in patients with mild cognitive impairment. Neuroimage Clin. 2019;23:101834. doi:10.1016/j.nicl.2019.101834
82. Chang J, Chen Y, Liu C, et al. Effect of square dance exercise on older women with mild mental disorders. Front Psychiatry. 2021;12:699778. doi:10.3389/fpsyt.2021.699778
83. Yu AP, Chin EC, Yu DJ, et al. Tai Chi versus conventional exercise for improving cognitive function in older adults: a pilot randomized controlled trial. Sci Rep. 2022;12(1):8868. doi:10.1038/s41598-022-12526-5
84. Arshad H, Khattak HG, Anwar K. Effect of exergames by using Xbox 360 Kinect on cognition of older adults with mild cognitive impairment. Rawal Med J. 2023;48(4):994. doi:10.5455/rmj.20210821031024
85. Suzuki T, Shimada H, Makizako H, et al. Effects of multicomponent exercise on cognitive function in older adults with amnestic mild cognitive impairment: a randomized controlled trial. BMC Neurol. 2012;12(1):1–9. doi:10.1186/1471-2377-12-128
86. Lee YY, Wu CY, Teng CH, et al. Evolving methods to combine cognitive and physical training for individuals with mild cognitive impairment: study protocol for a randomized controlled study. Trials. 2016;17(1):1–10. doi:10.1186/s13063-016-1650-4
87. Wu M, Liu H, Huang J, et al. Synergistic effect of Tai Chi and transcranial direct current stimulation on memory function in patients with mild cognitive impairment: study protocol for a 2×2 factorial randomised controlled trial. BMJ Open. 2023;13(11):e076196. doi:10.1136/bmjopen-2023-076196
88. Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451–1462. doi:10.1136/bjsports-2020-102955
89. Yu DJ, Yu AP, Bernal JD, et al. Effects of exercise intensity and frequency on improving cognitive performance in middle-aged and older adults with mild cognitive impairment: a pilot randomized controlled trial on the minimum physical activity recommendation from WHO. Front Physiol. 2022;13:1021428. doi:10.3389/fphys.2022.1021428
90. Song D, Doris SF. Effects of a moderate-intensity aerobic exercise programme on the cognitive function and quality of life of community-dwelling elderly people with mild cognitive impairment: a randomised controlled trial. Int J Nurs Stud. 2019;93:97–105. doi:10.1016/j.ijnurstu
91. Yang JG, Thapa N, Park HJ, et al. Virtual reality and exercise training enhance brain, cognitive, and physical health in older adults with mild cognitive impairment. Int J Environ Res Public Health. 2022;19(20):13300. doi:10.3390/ijerph192013300
92. Zhu Y, Wu H, Qi M, et al. Effects of a specially designed aerobic dance routine on mild cognitive impairment. Clin Interv Aging. 2018;Volume 13:1691–1700. doi:10.2147/CIA.S163067
93. Khattak HG, Ahmad Z, Arshad H, et al. Effect of aerobic exercise on cognition in elderly persons with mild cognitive impairment. Rawal Med J. 2022;47(3):696. doi:10.5455/rmj.20210713072242
94. Sungkarat S, Boripuntakul S, Kumfu S, et al. Tai Chi improves cognition and plasma BDNF in older adults with mild cognitive impairment: a randomized controlled trial. Neurorehabil Neural Repair. 2018;32(2):142–149. doi:10.1177/1545968317753682
95. Won J, Callow DD, Pena GS, et al. Hippocampal functional connectivity and memory performance after exercise intervention in older adults with mild cognitive impairment. J Alzheimer's Dis. 2021;82(3):1015–1031. doi:10.3233/JAD-210051
96. Chirles TJ, Reiter K, Weiss LR, et al. Exercise training and functional connectivity changes in mild cognitive impairment and healthy elders. J Alzheimer's Dis. 2017;57(3):845–856. doi:10.3233/JAD-161151
97. Iyalomhe O, Chen Y, Allard J, et al. A standardized randomized 6-month aerobic exercise-training down-regulated pro-inflammatory genes, but up-regulated anti-inflammatory, neuron survival, and axon growth-related genes. Exp Gerontol. 2015;69:159–169. doi:10.1016/j.exger.2015.05.005
98. Rondão CADM, Mota MP, Oliveira MM, et al. Multicomponent exercise program effects on fitness and cognitive function of elderlies with mild cognitive impairment: involvement of oxidative stress and BDNF. Front Aging Neurosci. 2022;14:950937. doi:10.3389/fnagi.2022.950937
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Stem Cell Therapy for Neuropathic Pain: A Bibliometric and Visual Analysis
Kan H, Fan L, Gui X, Li X, Yang S, Huang Y, Chen L, Shen W
Journal of Pain Research 2022, 15:1797-1811
Published Date: 23 June 2022
Knowledge Atlas of the Co-Occurrence of Epilepsy and Autism: A Bibliometric Analysis and Visualization Using VOSviewer and CiteSpace
Wang Y, Huo X, Li W, Xiao L, Li M, Wang C, Sun Y, Sun T
Neuropsychiatric Disease and Treatment 2022, 18:2107-2119
Published Date: 19 September 2022
Bibliometric and Visualization Analysis of Biomechanical Research on Lumbar Intervertebral Disc
Hou Z, Wang W, Su S, Chen Y, Chen L, Lu Y, Zhou H
Journal of Pain Research 2023, 16:3441-3462
Published Date: 17 October 2023
Bibliometric Analysis of Psychological Distress in Stroke: Research Trends, Hot Spots, and Prospects- An Emphasis on China
Xu Z, Zhu Y
Journal of Multidisciplinary Healthcare 2023, 16:4279-4291
Published Date: 28 December 2023
Bibliometric and Visualization Analysis of Research Hotspots and Frontiers in Endoscopic Lumbar Discectomy
Zhong Y, Wang J, Liang Z, Han T, Lu H, Hou Z
Journal of Pain Research 2024, 17:2165-2190
Published Date: 18 June 2024