")
Back to Journals » Infection and Drug Resistance » Volume 18
Risk Factor Analysis and Molecular Epidemiological Investigation of Carbapenem-Resistant Enterobacteriaceae (CRE) Infection in Patients with Acute Pancreatitis
Authors Yang F , Liu F, Zhao X, Chen Q
Received 24 October 2024
Accepted for publication 9 January 2025
Published 16 January 2025 Volume 2025:18 Pages 297—306
DOI https://doi.org/10.2147/IDR.S498829
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Fangfang Yang,1 Fang Liu,2 Xiaoji Zhao,1 Qian Chen2
1Department of Clinical Laboratory, The Third Hospital of Mianyang, Sichuan Mental Health Center, Mianyang, People’s Republic of China; 2Department of Clinical Laboratory, Chongqing Red Cross Hospital (Jiangbei District People’s Hospital), Chongqing, People’s Republic of China
Correspondence: Qian Chen, Chongqing Red Cross Hospital (Jiangbei District People’s Hospital), Chongqing, 400000, People’s Republic of China, Email [email protected]
Objective: Patients with acute pancreatitis (AP) complicated by carbapenem-resistant Enterobacteriaceae (CRE) infection often have a higher mortality rate. However, little investigation on the risk factor analysis has been published for the AP complicated by CRE. Therefore, this study conducted a retrospective analysis of the clinical characteristics, risk factors, and molecular epidemiological features associated with CRE infection in patients with AP.
Methods: A total of 240 patients with AP were admitted to our hospital from 2011 to 2021 as the research objects, and were divided into a CRE group of 60 cases and a non-CRE group of 180 cases based on whether they were co-infected with CRE or not. Furthermore, both univariate analysis and multivariate analysis were used to analyze the risk factors of AP co-infection with CRE. In the CRE group, polymerase chain reaction (PCR) and agarose gel electrophoresis (AGE) were used to detect the expression of five common carbapenemase genes including blaKPC, blaIMP, blaVIM, blaNDM, and blaOXA-48.
Results: The pathogenic bacteria in the CRE group are composed of Klebsiella pneumonia at 35.00%, Escherichia coli at 33.33%, Enterobacter cloacae at 25.00%, and Citrobacter freundii at 6.67%. Multivariate analysis showed that APACHE-II scores (OR=1.22), history of abdominal surgery (OR=81.82), and ERCP (OR=3.66) were independent risk factors for AP co-infection with CRE (P< 0.05). About half (18/40) of the CRE carried carbapenemase genes. blaKPC was the major carbapenemase gene.
Conclusion: There are many risk factors for AP co-infection with CRE, which can occur in patients with high APACHE-II scores, experienced ERCP, and a history of abdominal surgery.
Keywords: acute pancreatitis, carbapenem-resistant Enterobacteriaceae (CRE), infection, risk factors
Introduction
Acute pancreatitis (AP) is the activation of pancreatic enzymes caused by various reasons and may lead to local damage, systemic inflammatory response syndrome, and organ failure. It is one of the common gastrointestinal diseases and is potentially lethal.1 In the United States, the AP is the main cause of hospitalization for gastrointestinal diseases, for which approximately 275,000 patients are hospitalized by AP each year and the total treatment cost reaches approximately US$2.6 billion.2
Biliary diseases, hypertriglyceridemia, and alcoholism are the most common causes of AP.3 However, other causes including trauma, surgery, pregnancy, infection, drugs, inherited metabolic diseases and autoimmune diseases can also lead to AP, among which infection is closely related to the mortality of patients.4 AP is often accompanied by two major clinical courses, the first one is systemic inflammatory response syndrome (SIRS) and the other one is compensatory anti-inflammatory response syndrome (CARS).5 The former course usually occurs early and lasts for 1 or 2 weeks. The latter ranges from a few weeks to a few months and is characterized by the presence of local complications and related infectious complications that often occur in the later stage of the disease and usually last for a rather long time.6 Research indicates that 80% of deaths occur in the terminal stage, as a result of infection.
The early stages of AP are sterile, but as the disease progresses, bacterial overgrowth and translocation can occur due to inflammatory reactions, intestinal barrier dysfunction, and frequent use of prophylactic antibiotics, making patients susceptible to multidrug-resistant Gram-negative bacterial (MDR-GNB) infections.7,8 Among them, carbapenem-resistant Enterobacteriaceae (CRE) have attracted attention due to their high resistance rate to most antibiotics. Recently, the infection rate of CRE has increased in patients with AP concurrent infection.9 The high mortality caused by the AP complicated by the CRE and the shortage of effective anti-infective treatment have brought great challenges to the clinic.
Carbapenemase production is the main resistance mechanism of CRE.10 Globally, the most important carbapenemases in CRE are divided into three categories: (1) class A serine enzymes, such as KPC-type enzymes; (2) class B metalloenzymes, such as NDM, VIM, and IMP; (3) d-serine enzymes, such as OXA-48-type enzymes.11 Some observational studies have shown that the mortality of patients with bacteremia caused by carbapenem-resistant Enterobacteriaceae is as high as 40% to 60.12,13 However, little investigation on the risk factor analysis has been published for the AP complicated by the CRE. Therefore, this study conducted a retrospective analysis of the clinical characteristics and risk factors associated with CRE infection in patients with AP and also examined the molecular epidemiological features to provide references for clinical prevention and control of AP.
Materials and Methods
Study Design and Population
The study was conducted at a general hospital in southwest China, where 240 non-repetitive patients with AP co-infection were collected from April 2011 to December 2021 through the hospital’s electronic case system and clinical microbiology database. Based on the presence or absence of CRE co-infection, the patients were divided into the CRE group (n=60) and the non-CRE group (n=180). It is important to note that if multiple detections of CRE occurred in the same hospitalized patient, only the first infective case was considered.
The criteria for AP include the following requirements: (1) the patients must meet the 2012 revision of the Atlanta classification;14 (2) the hospitalized days of patients are more than 2. The exclusion criteria are as follows: (1) age < 18 years old; (2) the clinical data is incomplete. The detailed experimental process is shown in the flow chart (Figure 1).
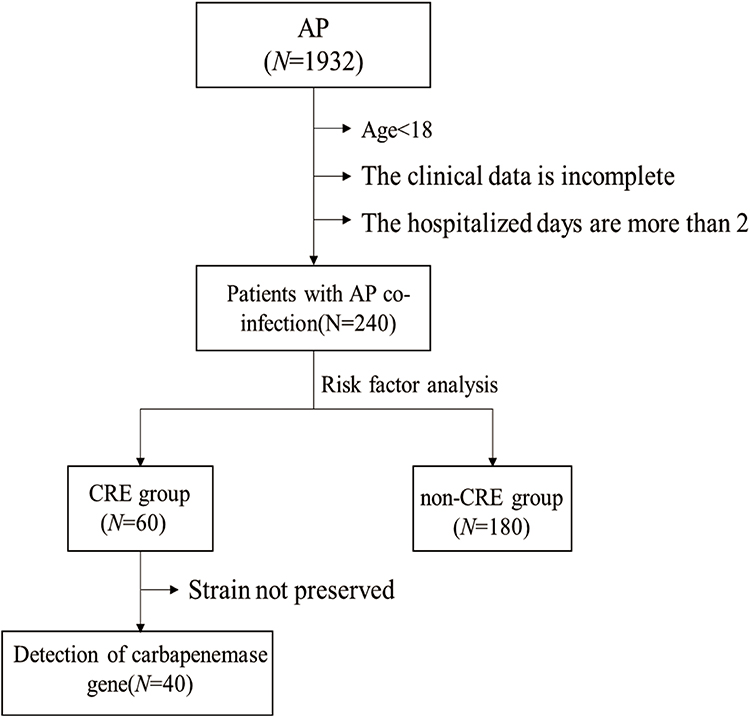 |
Figure 1 The flowchart of study design. Abbreviations: AP, acute pancreatitis; CRE, carbapenem-resistant Enterobacteriaceae. |
Clinical Data Statistics and Analysis
A retrospective comparative analysis was conducted using various parameters as potential risk factors: (1) General hospitalization data including age, sex, transfer status, and etiology; (2) prognosis indicators containing death rate, shock, total hospitalization days, and ICU admission.; (3) Underlying diseases; (4) Infections during hospitalization; (5) Invasive procedures; (6) Antibacterial drug usage before detection of CRE.
Antibiotic Susceptibility Test
According to the Clinical and Laboratory Standards Institute (CLSI) guideline M45,15 antimicrobial susceptibility testing was conducted using microdilution and disk diffusion methods.
The criteria for CRE were as follows: any isolated Enterobacteriaceae resistant to meropenem (disc diffusion diameter ≤19 mm, ertapenem ≤19 mm), ertapenem (minimum inhibitory concentration (MIC) ≥2 μg/mL) or imipenem (MIC≥4 μg/mL).
Detection of Carbapenemase Gene
Common carbapenemase genes, including Ambler’s class A (KPC enzymes), class B metallo-beta-lactamase (NDM, VIM, and IMP enzymes), and class D oxacillinase (OXA-48-like enzymes), were detected in 40 strains of the CRE group. DNA templates were extracted by metal baths. The primer sequences specifically employed for detecting carbapenemase-producing isolates are presented in Table 1. Each reaction mix (20 μL) contained 10 uL PCR master mix (SYBR Premix Ex Taq II; Takara Bio Inc), 1 μL of each forward and reverse primer (100μM), 6 μL of molecular grade nuclease-free water, and 2 μL of DNA template. Amplification was done at 95 °C for 3 minutes as the initial step for predenaturation, followed by denaturation at 92 °C for 20 seconds, annealing at 68 °C for 20 seconds (1.5 °C decrease and 6 seconds increase per cycle) and extension at 72°C for 30 seconds were repeated for 8 cycles. Then 25 cycles of denaturation at 92 ° C for 20 seconds, annealing at 55 °C for 20 seconds, and extension at 72 °C for 30 seconds were repeated. The final elongation was at 72 °C for 5 minutes. All PCR amplicons were analyzed by horizontal gel-electrophoresis in a 1% (weight/volume) (Bio-BAD subcell G1, USA) Tris/Acetate/EDTA 50 x concentrate buffer. The agarose was stained with 4 uL of Gel-red (Bio-Rad, USA). About 5 μL of amplicons were put into the wells and run in a 1 x Tris-acetate EDTA (TAE) at 150 volts for 30 minutes. DL2000 (Takara, AJG1332A) was used as a marker. The amplicons were visualized with the BIO-RAD GelDoo XR (Bio-Rad, USA).
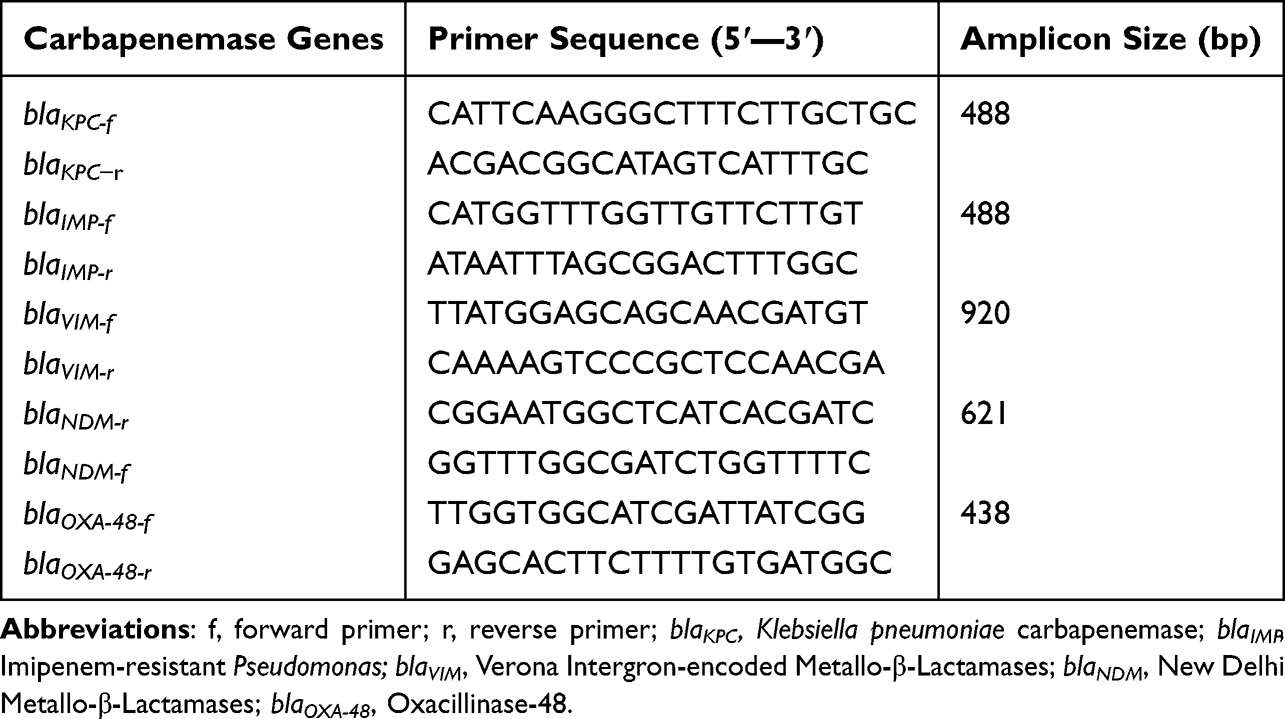 |
Table 1 Primer Sequences Used in This Article |
Statistical Analysis
SPSS 24.0 (IBM SPSS software, Armonk, NY, USA) was used to analyze the results. Categorical variables were shown as frequencies and proportions. For continuous variables, normally distributed data were reported by mean and standard deviation. The difference between the two groups was tested by Student’s t-test. Skewed variables were represented by median and interquartile ranges. Mann–Whitney U-test was used to compare the differences between the two groups. In univariate analyses, categorical variables were analyzed using either the Chi-square or Fisher’s exact test. The Logistic regression method was used to determine the relationship between the potential risk factors and the pancreatitis co-infection with CRE. P-value <0.05 was considered significant.
Results
Sample Source and Species Distribution of CRE Infection in AP
In the CRE group, the isolates were obtained from sputum (10%), gastric juice (1.67%), urine (5%), abdominal drainage fluid (36.67%), wound secretion (10%), bile (21.67%), and blood (15%) (Table 2). The distribution of pathogens in the CRE group is listed in Table 3. It can be seen that the bacteria of AP co-infected with CRE included Klebsiella pneumoniae at 35.00%, Escherichia coli at 33.33%, Enterobacter cloacae at 25.00%, and Citrobacter freundii at 6.67% (Table 3).
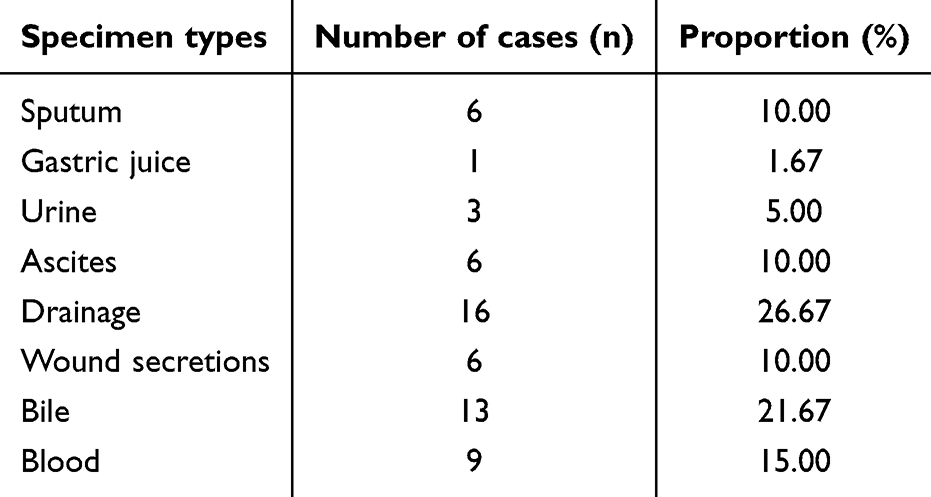 |
Table 2 The Specimen Types of Pathogens in the CRE Group |
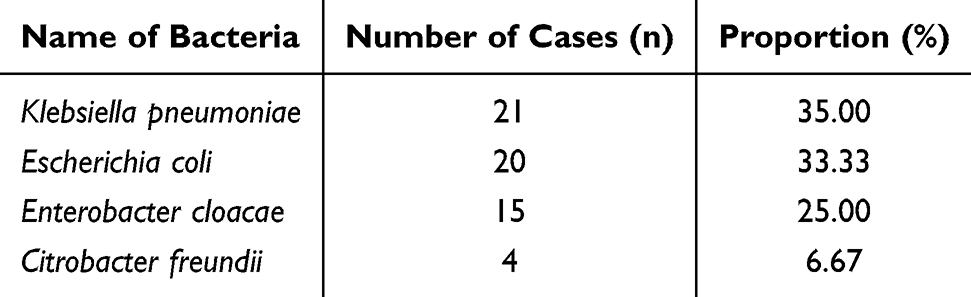 |
Table 3 The Distribution of Pathogens in the CRE Group |
Univariate Analysis of AP Complicated with CRE Infection
The results of the related risk factors analysis are listed in Table 4. It is shown that AP co-infection with CRE is related to the age, total number of hospitalized days, hospitalized days before the detection of CRE, ICU duration, days of fasting, score of APACHE II, history of abdominal surgery within 6 months, basic hyperlipidemia, diabetes, kidney disease, combined infections of abdominal, lung and urinary tract, catheterization and days of enteral nutrition, puncture, ERCP, drainage tube, gastric tube, urinary catheter, intravenous, hemofiltration, other invasive operations and the usage of antibacterial drugs before testing. The differences are statistically significant (P<0.05).
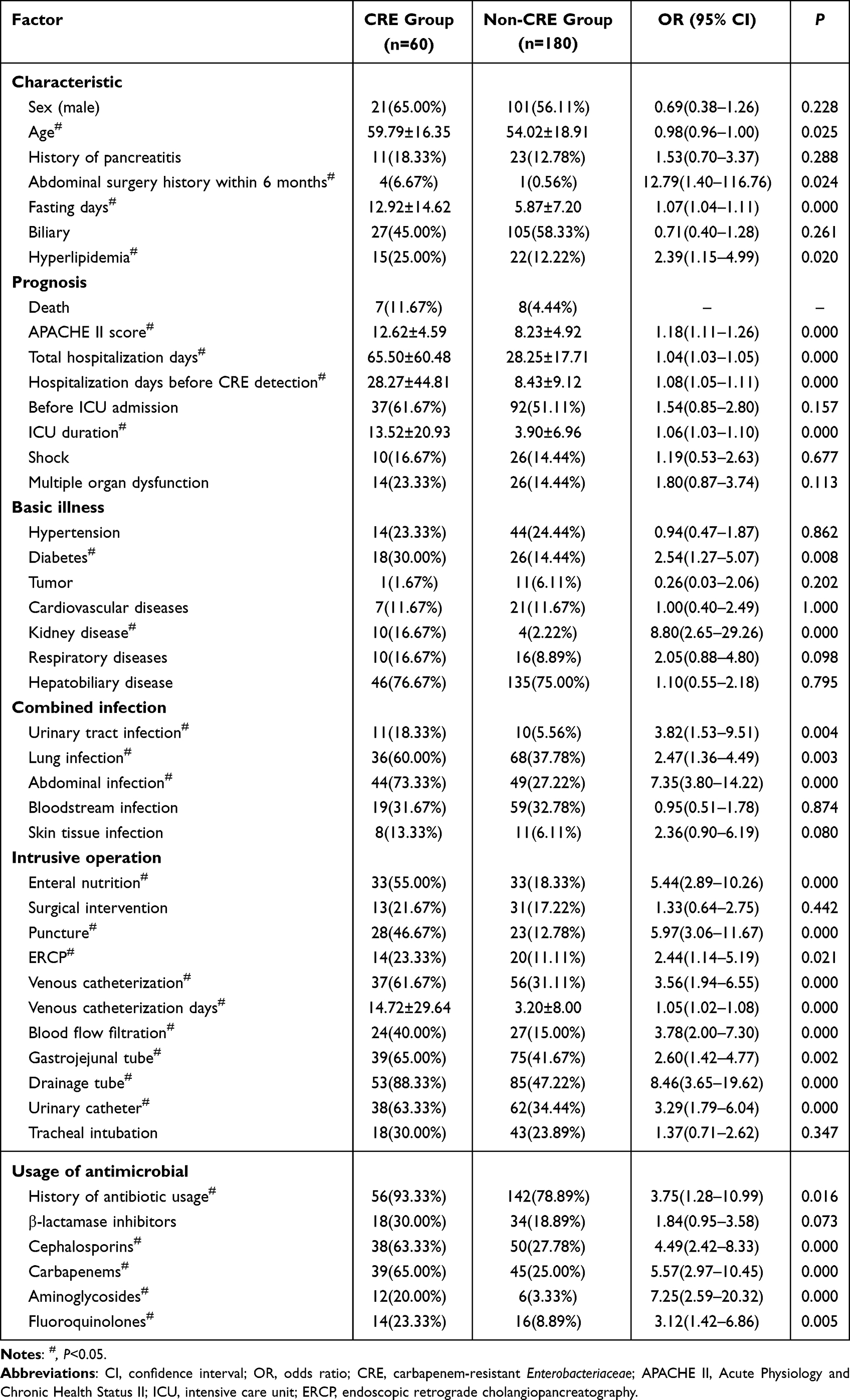 |
Table 4 Univariate Analysis of AP Complicated with CRE Infection |
Multivariate Analysis of AP Complicated with CRE Infection
The results of multivariate analysis for the CRE infections in the AP are listed in Table 5. It is shown that the APACHE II score at admission, history of abdominal surgery within 6 months, and ERCP were independent risk factors of AP co-infection with CRE (P<0.05).
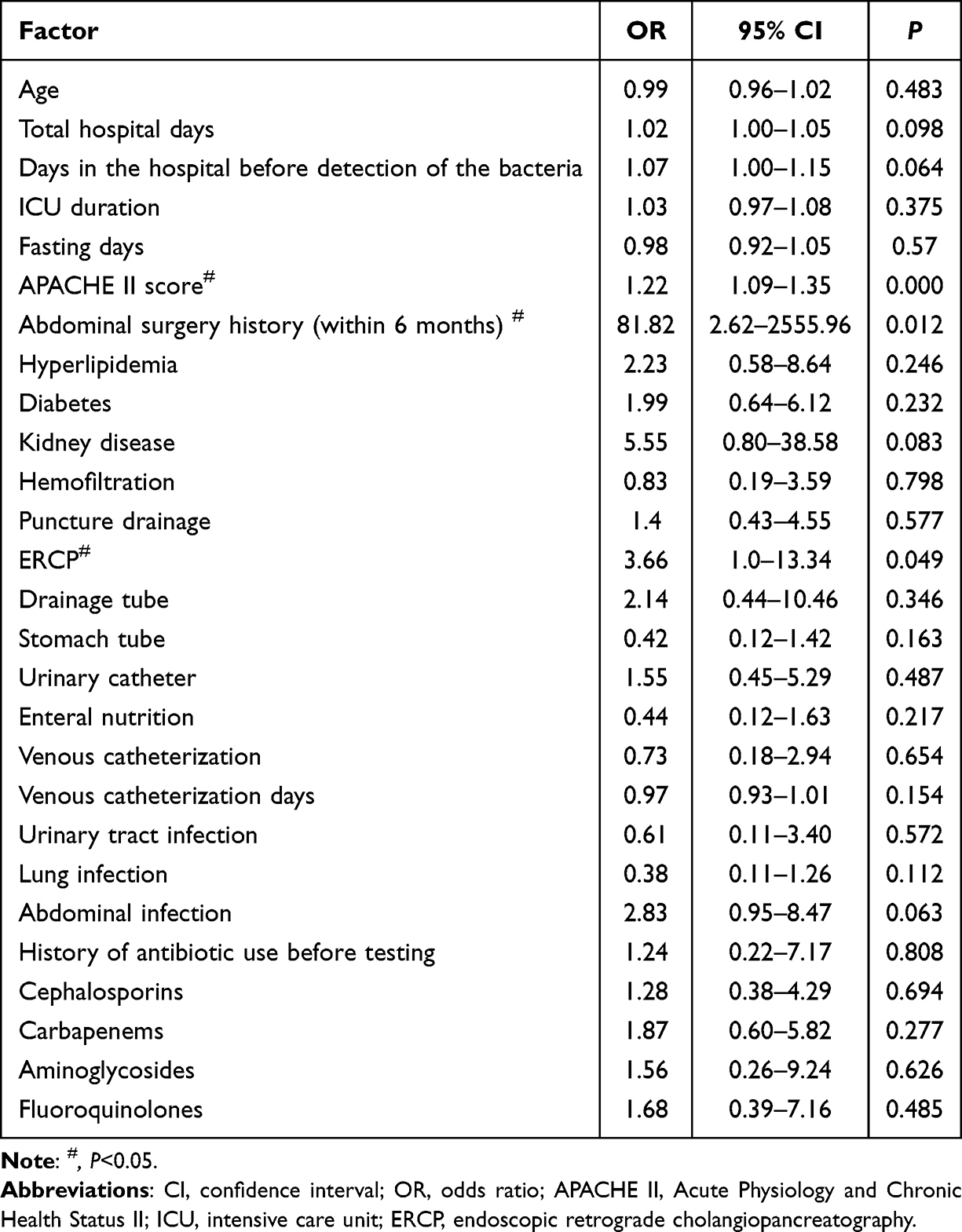 |
Table 5 Multivariate Analysis of AP Complicated with CRE Infection |
Detection of Carbapenemase Gene
The results indicated that 18 (45%) of the 40 strains expressed carbapenemase genes, of which 7 expressed blaKPC, and all were strains of Klebsiella pneumoniae (kpn). 7 strains expressed blaNDM, including 1 strain of kpn, 5 strains of Escherichia coli (eco), 1 in Citrobacter freundii (cfr). A total of 4 strains of kpn expressed both blaKPC and blaNDM genes simultaneously. No strains expressed the blaIMP, blaVIM, or blaOXA−48 genes. Refer to Figure 2 and Table 6 for further details.
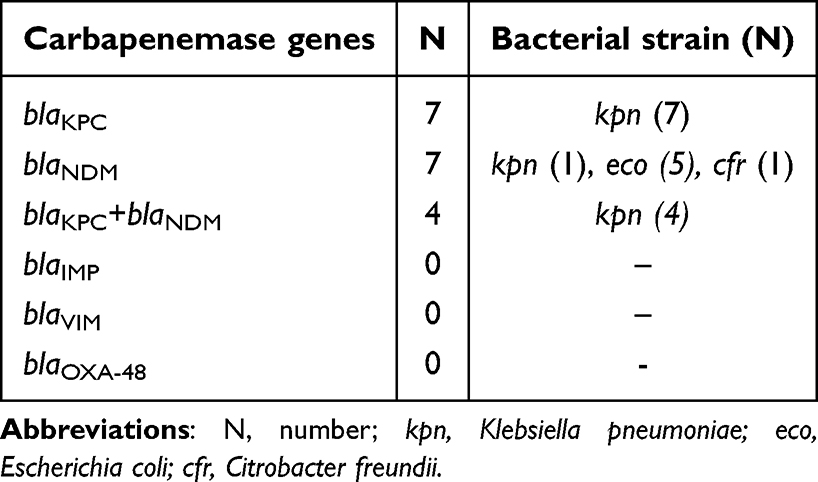 |
Table 6 Amplification Result of Carbapenemase Gene |
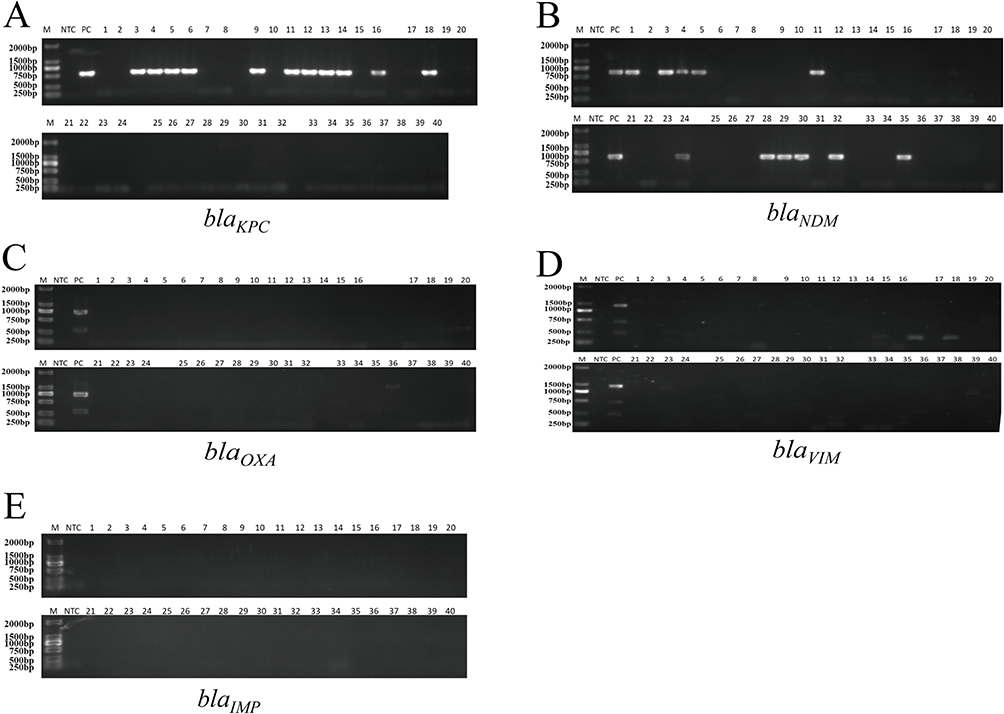 |
Figure 2 Detection of carbapenemase gene, including blaKPC (A), blaNDM (B), blaIMP (C), blaVIM (D), blaOXA-48 (E). Add 5μL of DNA marker into the prepared gel tank to the first well, add a no-template control to the second well, add positive sample controls (blaKPC, blaNDM, blaVIM, blaOXA-48 have positive controls, blaIMP has no positive control strain) to the third well, and start adding samples from the fourth well. After adding samples to each row (8 samples), leave one well empty and then add a second row (8 samples). Abbreviations: M, maker; NTC, no template control; PC, positive sample control. |
Discussion
With a diverse range of clinical manifestations, AP is mild and transient but can rapidly progress to a severe and fatal condition. However, the majority of AP-related deaths are attributed to infection complications.16 It has been reported that 40% to 70% of severe AP patients develop bacterial infections during the natural course of the disease, with infection being the most significant risk factor for mortality in these cases.17 Moreover, CRE infection is a thorny problem in the treatment of AP. However, limited research has been published on this topic in recent years.
The co-infection of pathogenic bacteria in AP primarily consists of Gram-negative bacteria, particularly Enterobacteriaceae species which can cause respiratory tract infections, urinary tract infections, abdominal cavity infections, and surgical site infections. With the widespread use of broad-spectrum antibiotics, there has been an increase in multi-drug resistant Enterobacteriaceae strains as well.18 In recent years, due to the emergence and spread of carbapenemase genes within these strains, there has been a sharp rise in CRE rates leading to considerable difficulties in clinical anti-infection treatments.
In the study, most of the bacteria detected in patients with AP complicated with CRE was Klebsiella pneumoniae (35.00%), followed by Escherichia coli (33.33%), consistent with the prevalence of CRE in China.19,20 As the 2021 CHINET shows, from 2005 to 2021, the resistance rates of Klebsiella pneumoniae to Meropenem and Imipenem increased from 2.9% and 3.0% to 24.4% and 25.3%, respectively.21 This phenomenon may be related to the fact that Klebsiella pneumoniae is more prone to produce extended-spectrum β-Lactamase (ESBLS), AmpC enzyme, and carbapenemase. The primary resistance mechanisms of CRE include: (1) production of carbapenemase; (2) reduced intracellular antibiotic levels, which are attributed to decreased absorption due to changes in membrane porins and increased excretion resulting from overexpression of efflux pumps. This is often accompanied by overexpression of ESBLs and/or AmpC beta-lactamases.22 In our study, different types of carbapenem-resistant genes were detected in 45% of the isolates. The remaining 55%, although identified as CRE in drug susceptibility testing, had a loss of carbapenem-resistance gene expression, possibly related to the production of other β-lactamases, loss of porins, and overexpression of efflux pumps.
In the univariate analysis, we found that AP combined with CRE infection was related to age, total hospitalization days, hospitalization days before CRE detection, ICU duration, fasting days, hyperlipidemia, diabetes, kidney disease, combined with abdominal cavity, lung, urinary tract infection, enteral nutrition, puncture, drainage tube, gastric tube, catheter, venous catheterization and days, hemofiltration and the use of antibiotics before detection (P<0.05). However, the multivariate analysis of this study showed that there was no significant difference in the above covariates, which may be related to the individual differences of patients.
The results of multivariate analysis showed that there were three independent risk factors for AP combined with CRE infection: (1) APACHE II score: The APACHE II scoring system is widely used in intensive care units (ICU).23 The higher the score of the patients on admission, the more severe the clinical symptoms of the patients, and there may have been multiple organ dysfunction failure, which will further aggravate pancreatic necrosis, gastrointestinal mucosal damage, and bacterial translocation, increase the risk of infection, and be more prone to CRE infection. (2) Abdominal surgery history: Due to the large area of the abdominal cavity and the complex physiological functions, it is easy to cause some physiological functions of the patients to be destroyed during the operation. Therefore, infection is a common complication of abdominal surgery, including incision infection, and pulmonary infection. The incidence of postoperative infection is 1%−5%.24 In addition, the decreased immunity of severely injured patients also increases the chance of CRE infection. (3) Endoscopic retrograde cholangiopancreatography (ERCP): ERCP has the advantages of reduced trauma, fewer complications, faster postoperative recovery, and shorter hospital stays. It has been widely used in the diagnosis and treatment of benign and malignant pancreaticobiliary diseases.25 However, ERCP is an invasive surgery and may cause some related adverse events. It has been reported that the incidence of infection after ERCP was 3.58% to 13.51%, and the incidence of bacteremia was 3.56%.26
The emergence of carbapenemase (CHBLs) has always been the main mechanism of CRE resistance. We detected the genes of five common CHBLs with a detection rate of 45%, mainly blaKPC and blaNDM genes, which is consistent with previous reports.27 The other strains did not detect the common five drug resistance genes, which may be due to other drug resistance mechanisms, such as the lack of membrane porin, the abnormal expression of efflux pump, or the production of drug resistance genes not detected in this study, which needs further study.28
There are still some limitations in our research. Firstly, this is a 10-year retrospective study conducted in a single center. There may be limitations due to geographic limitations, insufficient sample size, and unobserved confounding factors. Additionally, due to the extended period, the bacterial strain was not fully preserved. Although there were 60 subjects in the CRE group, we ultimately conducted resistance gene testing on only 40 of them. Secondly, in the case of patients who had been treated in other hospitals, the data were not comprehensive enough, and the laboratory data and antibiotic use in other hospitals were not analyzed. Additionally, due to the long period of the case collation, some current laboratory projects have not been carried out at the beginning, so some potential risk factors cannot be confirmed. These will require further investigation in subsequent studies by increasing sample size and employing a prospective cohort study design to delve deeper into the findings.
Conclusions
In conclusion, to reduce the incidence of CRE infection in AP, we should evaluate critically ill patients, strengthen clinical management, isolate and protect patients with a history of abdominal surgery in the past six months, and strictly standardize the indications and aseptic techniques of ERCP. In the future, we will continue to conduct further research on the resistance mechanism of strains without carbapenem-resistant genes.
Data Sharing Statement
Data and materials associated with this work are available by request from the corresponding author.
Ethical Approval
As the study was performed with retrospective resources and will not have any impact on the diagnosis and treatment of patients, the ethics committee of the Third Hospital of Mianyang has approved the exemption of informed consent. This study was approved through the local ethics committee of the Third Hospital of Mianyang (approval number: 2024-48). This study complies with the Declaration of Helsinki.
Acknowledgments
We sincerely thank Dr. Niu Siqiang for his help on the paper.
Funding
This study was supported by the joint medical (including traditional Chinese medicine) research project by Health Commission and Science and Technology Bureau of Jiangbei District, Chongqing (202321).
Disclosure
The authors declare that they have no competing interests.
References
1. Zerem E, Kurtcehajic A, Kunosić S, et al. Current trends in acute pancreatitis: diagnostic and therapeutic challenges. World J Gastroenterol. 2023;29(18):2747–2763.
2. Peery AF, Crockett SD, Murphy CC, et al. Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States: update 2021. Gastroenterology. 2022;162(2):621–644. doi:10.1053/j.gastro.2021.10.017
3. Lee PJ, Papachristou GI. New insights into acute pancreatitis. Nat Rev Gastroenterol Hepatol. 2019;16(8):479–496.
4. Wu D, Jia Y, Cai W, et al. Impact of multiple drug-resistant Gram-negative bacterial bacteraemia on infected pancreatic necrosis patients. Front Cell Infect Microbiol. 2022;12(1044188). doi:10.3389/fcimb.2022.1044188.
5. Qiu M, Zhou X, Zippi M, et al. Comprehensive review on the pathogenesis of hypertriglyceridaemia-associated acute pancreatitis. Annals Med. 2023;55(2):2265939. doi:10.1080/07853890.2023.2265939
6. Ding L, Yang Y, Li H, et al. Circulating Lymphocyte Subsets Induce Secondary Infection in Acute Pancreatitis. Front Cell Infect Microbiol. 2020;10(128). doi:10.3389/fcimb.2020.00128.
7. Yang N, Ke L, Tong Z, et al. The effect of thymosin α1 for prevention of infection in patients with severe acute pancreatitis. Expert Opin Biol Ther. 2018;18(sup1):53–60. doi:10.1080/14712598.2018.1481207
8. Párniczky A, Lantos T, Tóth EM, et al. Antibiotic therapy in acute pancreatitis: from global overuse to evidence based recommendations. Pancreatology. 2019;19(4):488–499. doi:10.1016/j.pan.2019.04.003
9. Lin H, Wang P, Lu Y, et al. Clinical and Genomic Characteristics of Carbapenem-Resistant Klebsiella pneumoniae Isolates from Acute Pancreatitis with Infection in China. Clin Lab. 2023;69(7). doi:10.7754/Clin.Lab.2022.221017.
10. Ma J, Song X, Li M, et al. Global spread of carbapenem-resistant Enterobacteriaceae: epidemiological features, resistance mechanisms, detection and therapy. Microbiol Res. 2023;266(127249):127249. doi:10.1016/j.micres.2022.127249
11. Nordmann P, Dortet L, Poirel L. Carbapenem resistance in Enterobacteriaceae: here is the storm! Trends Mol Med. 2012;18(5):263–272. doi:10.1016/j.molmed.2012.03.003
12. Daikos GL, Tsaousi S, Tzouvelekis LS, et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections: lowering mortality by antibiotic combination schemes and the role of carbapenems. Antimicrob Agents Chemother. 2014;58(4):2322–2328. doi:10.1128/AAC.02166-13
13. Wu D, Xiao J, Ding J, et al. Predictors of Mortality and Drug Resistance Among Carbapenem-Resistant Enterobacteriaceae-Infected Pancreatic Necrosis Patients. Infect Dis Ther. 2021;10(3):1665–1676. doi:10.1007/s40121-021-00489-5
14. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
15. Institute CALS. Methods for antimicrobial dilution and disk susceptibility testing of infrequently isolated or fastidious bacteria [M]. CLSI Guideline M45. 2015;2015:1.
16. Wu D, Lu W, Huang Y, et al. The impact of multi-drug resistant Pseudomonas aeruginosa infections on acute pancreatitis patients. BMC Infect Dis. 2023;23(1):340. doi:10.1186/s12879-023-08230-y
17. Lv C, Zhang ZX, Ke L. Early prediction and prevention of infected pancreatic necrosis. World J Gastroenterol. 2024;30(9):1005–1010. doi:10.3748/wjg.v30.i9.1005
18. Lu JD, Cao F, Ding YX, et al. Timing, distribution, and microbiology of infectious complications after necrotizing pancreatitis. World J Gastroenterol. 2019;25(34):5162–5173. doi:10.3748/wjg.v25.i34.5162
19. Yu H, Qu F, Shan B, et al. Detection of the mcr-1 Colistin Resistance Gene in Carbapenem-Resistant Enterobacteriaceae from Different Hospitals in China. Antimicrob Agents Chemother. 2016;60(8):5033–5035. doi:10.1128/AAC.00440-16
20. Zhang R, W CE, Zhou H, et al. Prevalence and genetic characteristics of carbapenem-resistant Enterobacteriaceae strains in China. Lancet Infect Dis. 2017;17(3):256–257. doi:10.1016/S1473-3099(17)30072-5
21. CHINET.Available from: https://www.chinets.com/Document/Index.
22. Codjoe FS, Donkor ES. Carbapenem Resistance: a Review. Med Sci. 2017;6(1):1. doi:10.3390/medsci6010001
23. Al-Hadeedi S, Fan ST, Leaper D. APACHE-II score for assessment and monitoring of acute pancreatitis. Lancet. 1989;2(8665):738. doi:10.1016/S0140-6736(89)90795-2
24. Liu Z, Dumville JC, Norman G, et al. Intraoperative interventions for preventing surgical site infection: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2018;2(2):Cd012653. doi:10.1002/14651858.CD012653.pub2
25. Mayumi T, Okamoto K, Takada T, et al. Tokyo Guidelines 2018: management bundles for acute cholangitis and cholecystitis. J Hepato-Biliary-Pancreatic Sci. 2018;25(1):96–100. doi:10.1002/jhbp.519
26. Du M, Suo J, Liu B, et al. Post-ERCP infection and its epidemiological and clinical characteristics in a large Chinese tertiary hospital: a 4-year surveillance study. Antimicrob Resist Infect Control. 2017;6(131). doi:10.1186/s13756-017-0290-0.
27. Muscarella LF. Risk of transmission of carbapenem-resistant Enterobacteriaceae and related “superbugs” during gastrointestinal endoscopy. World J Gastrointestinal Endoscopy. 2014;6(10):457–474. doi:10.4253/wjge.v6.i10.457
28. Sader HS, Carvalhaes CG, Arends SJR, et al. Aztreonam/avibactam activity against clinical isolates of Enterobacterales collected in Europe, Asia and Latin America in 2019. J Antimicrob Chemother. 2021;76(3):659–666. doi:10.1093/jac/dkaa504
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.