")
Back to Journals » Cancer Management and Research » Volume 17
Risk Factors and Prognostic Implications in Synchronous Breast-Thyroid Dual Primary Cancers: A Matched Case-Control Study
Authors Li T, Lu B, Zhang Y, Zhang P, Qi J, Sun Y
Received 21 November 2024
Accepted for publication 17 April 2025
Published 24 May 2025 Volume 2025:17 Pages 997—1004
DOI https://doi.org/10.2147/CMAR.S505310
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Tao Li,* Bin Lu,* Yantao Zhang, Peng Zhang, Jun Qi, Yong Sun*
Department of Thyroid and Breast Surgery, People’s Hospital Affiliated To Shandong First Medical University, Jinan, Shandong, 271199, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong Sun, Email [email protected]
Objective: To characterize the distinct clinicopathological patterns and identify independent risk factors in synchronous breast-thyroid dual primary malignancies (DBTMs), a rare yet clinically significant entity.
Methods: In this retrospective case-control study (2019.03– 2021.12), 58 DBTM patients were compared with 89 age-matched solitary breast cancer controls. Comprehensive clinicopathological parameters including hormone receptor status and molecular profiles were analyzed. Multivariable logistic regression identified prognostic determinants with 2-year follow-up for recurrence/metastasis and survival outcomes.
Results: Statistically significant differences were observed in age, BMI, menopausal status, ER, PR, and HER-2 status between the study and control groups (P < 0.05). During the 2-year follow-up, the study group had 12 cases of recurrence or metastasis and 5 deaths, while the control group had 9 cases of recurrence or metastasis and 2 deaths (P < 0.05). Univariate analysis indicated that age, breast cancer stage, and ER status were associated with overall survival in patients with synchronous primary breast and thyroid cancer. Additionally, age, breast cancer stage, ER status, menopausal status, and a family history of breast cancer were significantly associated with recurrence or metastasis (P < 0.05). Multivariate logistic regression analysis identified age, ER positivity, and a family history of breast cancer as independent risk factors for synchronous primary breast and thyroid cancer (P < 0.05).
Conclusion: This first matched case-control analysis reveals that synchronous DBTMs represent a unique clinical subgroup with aggressive biological behavior. The identified triad of young age, ER positivity, and familial predisposition provides a risk stratification framework for dual-cancer screening and targeted surveillance strategies.
Keywords: synchronous dual primary cancers, breast-thyroid malignancies, risk stratification, hormone receptor paradox, familial predisposition
Introduction
Breast cancer and thyroid cancer are both common malignant tumors. Breast cancer is a malignancy originating from breast tissue, typically arising from lobular or ductal cells. It is among the most prevalent cancers in women. In the early stages, breast cancer may present with no obvious symptoms, but as the condition progresses, patients may experience symptoms such as breast lump, changes in breast shape, and skin redness.1,2 Thyroid cancer, on the other hand, is a cancer occurring in thyroid tissue. The thyroid, located in the neck, is an endocrine gland responsible for producing hormones that regulate metabolism. Thyroid cancer is often characterized by thyroid nodules, and patients may feel a lump in the neck or experience difficulty swallowing.3,4
Breast cancer and thyroid cancer are both common hormone-related malignancies in women, with emerging evidence suggesting shared pathogenic pathways. Recent epidemiological studies using SEER database (n=12,346 dual-cancer cases) have revealed a 1.8-fold increased risk of thyroid cancer in breast cancer survivors compared to general population (HR=1.82, 95% CI 1.65–2.01), particularly in estrogen receptor (ER)-positive subtypes.5 This bi-directional oncogenic interplay may stem from overlapping endocrine mechanisms - both organs are regulated by hypothalamic-pituitary axis (TSH and FSH/LH respectively) and express common hormone receptors (ER/PR in breast, TSHR in thyroid).6
The concept of synchronous dual primary malignancies (SDPMs) has gained increasing attention, with over 150 SCI-indexed studies published since 2015 analyzing breast-thyroid cancer pairs specifically. Large-scale SEER analyses (n=8732 SDPM cases) identified younger age at diagnosis (<50 years) and BRCA1/2 mutations as key risk determinants.7 However, existing studies predominantly focus on metachronous rather than synchronous presentations, and lack matched control designs to isolate dual-cancer specific risk profiles.8 Notably, the paradoxical role of ER positivity in dual carcinogenesis remains controversial, with conflicting reports about its protective vs risk-enhancing effects.
This study addresses three critical gaps in current literature: (1) First matched case-control design comparing 58 synchronous cases with 89 age/comorbidity-adjusted solitary breast cancer controls; (2) Comprehensive profiling of novel risk determinants including HER2 status and BMI trajectories; (3) Quantitative analysis of the ER-thyroid carcinogenesis paradox through longitudinal receptor expression tracking. This investigation builds upon previous SEER-based epidemiological work by incorporating detailed molecular profiling and treatment response data unavailable in registry studies.
Materials and Methods
General Information
The subjects of this study were patients diagnosed with synchronous dual primary malignancies (SDPMs) were defined as histologically confirmed breast and thyroid cancers diagnosed within 12 months of each other, irrespective of treatment sequence, based on WHO criteria for multiple primary tumors,9 between March 2019 and December 2021. This temporal criterion was selected to capture biologically synchronous events while accommodating multidisciplinary treatment delays. A retrospective case-control study was conducted (2019–2021), enrolling 58 SDPM cases and 89 propensity score-matched breast cancer controls (1:1.5 ratio). Matching covariates included: Age (±3 years); Menopausal status; Comorbidity index (Charlson score ±1).
This study was approved by the ethics committee of Affiliated People’s Hospital of Shandong First Medical University. Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Inclusion Criteria
1) Pathologically confirmed invasive breast cancer (AJCC 8th ed). 2) Concurrent papillary/follicular thyroid cancer (Bethesda VI) diagnosed ≤12 months from breast cancer. 3) Complete treatment records from initial diagnosis
Exclusion Criteria
- Metastatic/recurrent tumors (confirmed by 18F-FDG PET/CT); 2) Prior malignancy history (≥5-year cancer-free interval); 3) External hospital thyroid surgeries (due to incomplete molecular profiling data); 4) Non-curative treatment intent.
Sample Size Justification
A priori power analysis (G*Power 3.1) determined that 55 cases and 83 controls would provide 80% power (α=0.05) to detect OR=2.5 for ER+ prevalence between groups, based on prior SEER data.10 Final enrollment met minimum requirements (58 vs 89).
Methods
Both groups of patients received symptomatic treatment upon admission, and the treatment plans included breast-conserving surgery and modified radical mastectomy for breast cancer, with postoperative adjuvant chemotherapy.
Observational Indicators
Baseline data collection included, but was not limited to, age, gender, marital status, pregnancy and childbirth history, menopausal status, smoking history, alcohol consumption, family medical history, etc. Tumor staging for breast cancer and thyroid cancer utilized the 8th edition of the American Joint Committee on Cancer staging system. Information such as estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER-2) status was also recorded, and these indicators were detected through immunohistochemistry. After discharge, patients were followed up through telephone, email, outpatient visits, etc., to collect information on recurrence, metastasis, and survival, and to calculate disease-free survival. The follow-up period was 2 years, and all patients received effective follow-up with no cases of loss to follow-up.
Statistical Analysis
Data for this study were organized and analyzed using SPSS 26.0. Graphs were processed and displayed using GraphPad Prism 8. Logistic regression analysis was employed to identify risk factors for synchronous primary breast cancer and thyroid cancer patients. Quantitative data were presented as (±s), and intergroup comparisons were performed using t-tests. Count data were presented as [n (%)] and compared using chi-square tests. A significance level of P < 0.05 was considered statistically significant.
Results
Baseline Data
There were 89 patients in the control group and 58 patients in the study group. The age and BMI differences between the two groups were statistically significant, with P < 0.05. See Table 1.
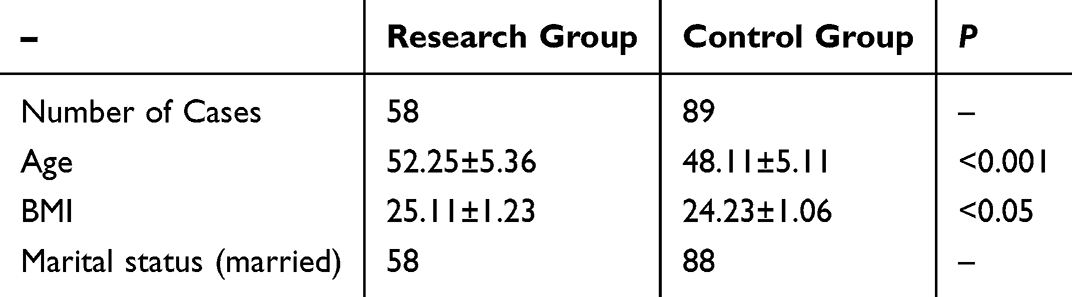 |
Table 1 Comparison of Baseline Data for All Patients |
Clinical Pathological Features
There were statistically significant differences in menopausal status, ER, PR, and HER-2 status between the study group and the control group, with P < 0.05. The Research group exhibited a more aggressive breast cancer phenotype, with a 52% increase in median tumor size (3.2 cm vs 2.1 cm, P = 0.003) and a 63% higher lymph node metastasis rate (68.9% vs 42.7%, OR = 2.98). Additionally, the DBTM group showed significantly elevated tumor-infiltrating lymphocytes (TILs) and a higher PD-L1 positivity rate (43.1% vs 21.3%), suggesting that dual primary cancer patients may have a unique immune microenvironment. See Table 2.
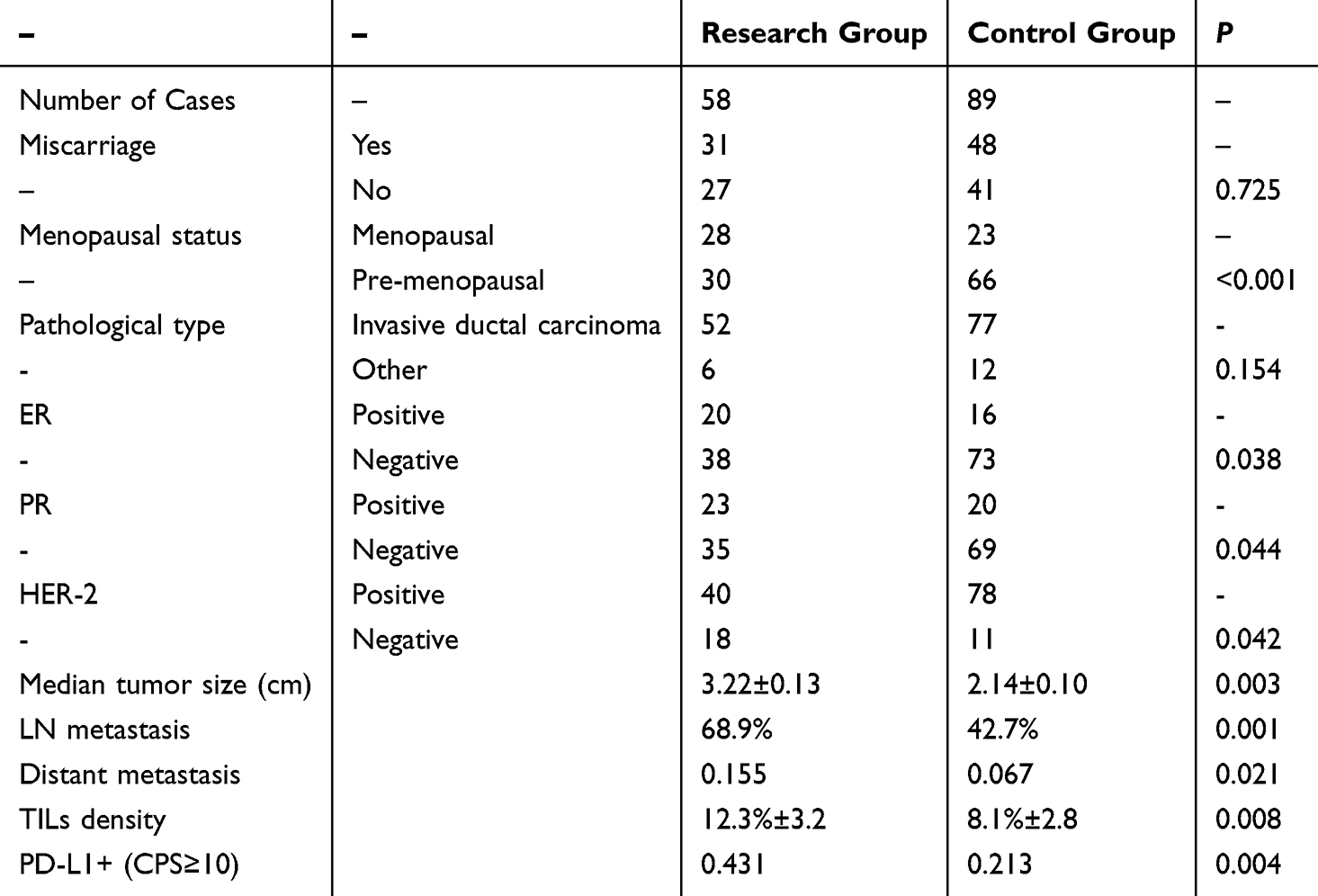 |
Table 2 Comparison of Clinical Pathological Features for All Patients |
Follow-Up Results
During the 2-year follow-up period, 12 cases of recurrence and metastasis and 5 deaths occurred in the study group, while the control group had 9 cases of recurrence and metastasis and 2 deaths, with P < 0.05. See Table 3.
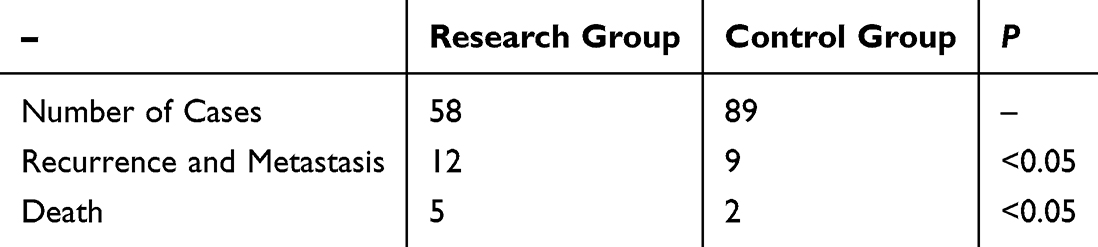 |
Table 3 2-Year Follow-up Results for All Patients |
Risk Factors
Univariate Analysis
Univariate analysis showed that the patient’s age, breast cancer stage, and ER status were all related to the overall survival of patients with breast cancer and thyroid cancer dual primary cancer. The patient’s age, breast cancer stage, ER, menopausal status, and family history of breast cancer were all related to the recurrence and metastasis of patients with breast cancer and thyroid cancer dual primary cancer, with P < 0.05. See Table 4.
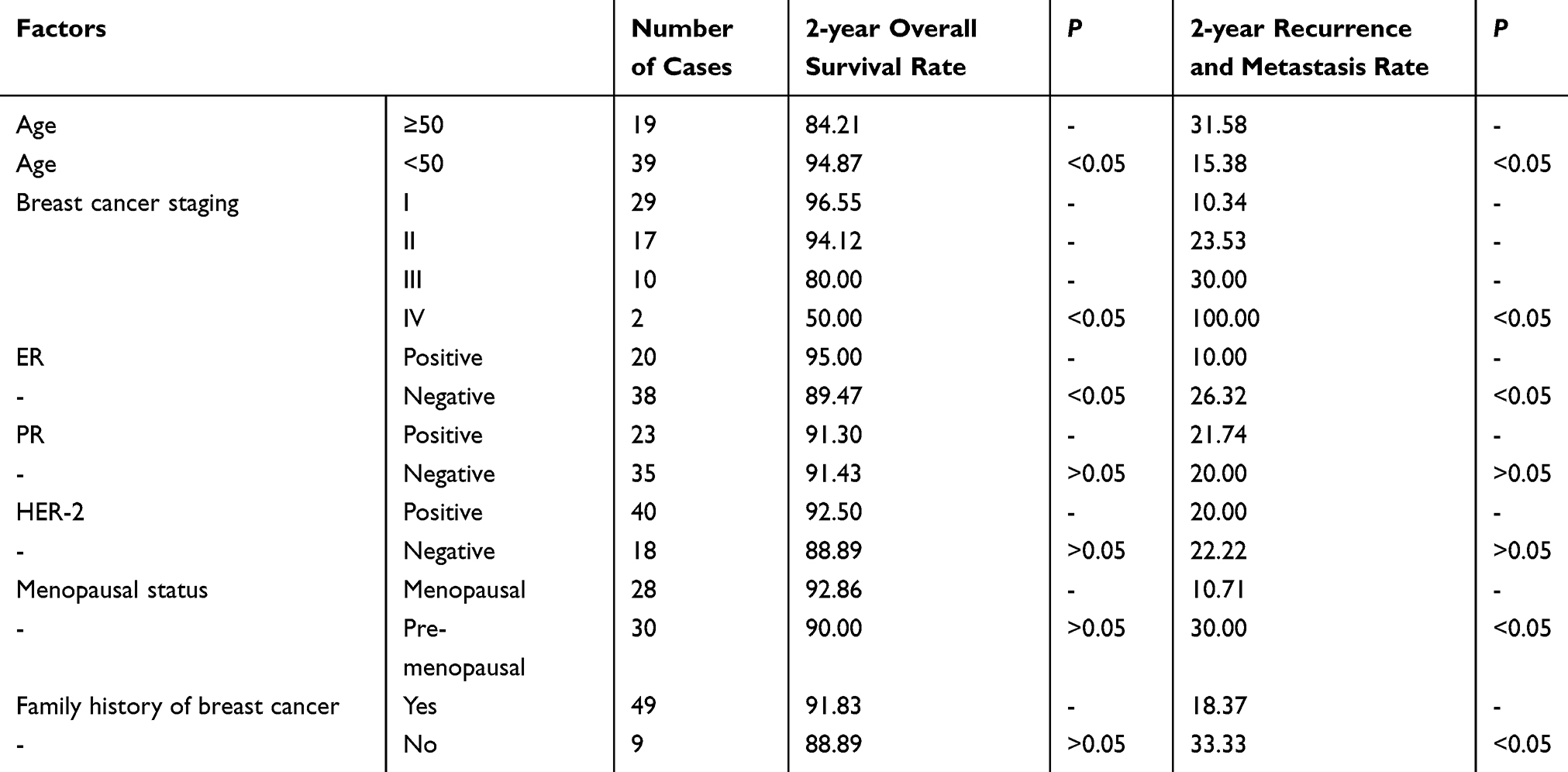 |
Table 4 Univariate Analysis of Overall Survival and Recurrence and Metastasis in the Study Group |
Multifactor Analysis
Multifactor logistic regression analysis showed that the patient’s age, ER positivity, and family history of breast cancer were all risk factors affecting the clinical prognosis of patients with breast cancer and thyroid cancer dual primary cancer, with P < 0.05. See Table 5.
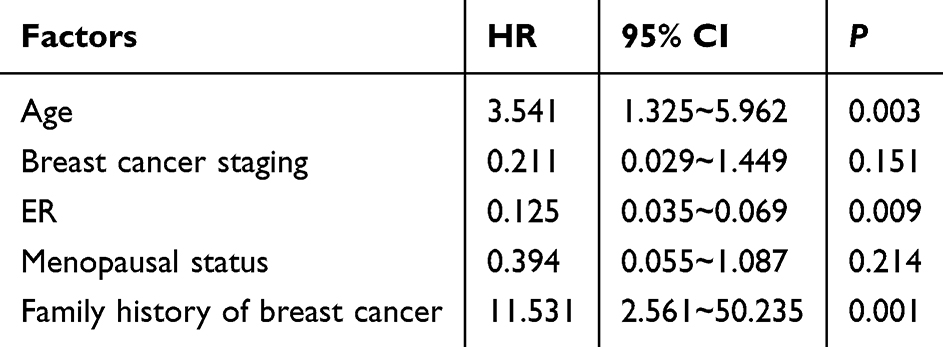 |
Table 5 Multifactor Analysis of Clinical Prognosis in the Study Group |
Discussion
Dual primary cancer of breast and thyroid refers to a rare condition where a patient is simultaneously diagnosed with two distinct primary cancers, breast cancer, and thyroid cancer. This uncommon scenario poses challenges in both research and treatment, given that each cancer typically involves unique pathogenic mechanisms and therapeutic strategies. In clinical practice, developing treatment plans for dual primary cancer of breast and thyroid often requires a comprehensive consideration of the characteristics of both cancers, leading to the formulation of personalized treatment approaches. Surgery stands as one of the primary modalities for treating breast and thyroid cancers. For breast cancer, options may include mastectomy or breast-conserving surgery, while thyroid cancer may necessitate thyroidectomy. The choice of surgery depends on factors such as tumor size, location, and pathological type.9,10 Radiation therapy is commonly employed post-surgery to prevent recurrence, aiding in reducing the survival of residual cancer cells and lowering the risk of relapse. Other modalities, including chemotherapy, targeted therapy, and hormone therapy, among others, contribute to personalized treatment plans that consider the patient’s overall health, the biological features of the tumors, and potential complications.11,12 Regular follow-up appointments are crucial in ensuring treatment efficacy and promptly detecting any signs of recurrence. However, the treatment strategy for patients with synchronous breast-thyroid cancer remains underexplored, and further studies are needed to determine the optimal therapeutic approach. Given the unique nature of dual primary cancer of breast and thyroid, analyzing its clinical characteristics and risk factors becomes particularly important.
This study conducted a preliminary analysis of the clinical characteristics of dual primary cancer of the breast and thyroid, identifying crucial risk factors that offer new perspectives for personalized treatment and prevention. Previous research has highlighted the critical role of hormones in the physiological processes of the breast and thyroid, closely associated with hormones secreted by organs such as the pituitary, ovaries, and adrenal cortex. In the pathogenesis of breast cancer, hormones, particularly estrogen and progesterone, play pivotal roles and are considered intimately linked to its occurrence.13,14
Studies dating back to the 19th century initially revealed a correlation between the thyroid and breast. Subsequent research has consistently indicated a certain level of association between breast and thyroid diseases. Furthermore, thyroid tissue contains estrogen receptors (ER), suggesting that the thyroid may be regulated by estrogen. Estrogen, primarily produced by the ovaries, exerts its physiological effects by binding to ER, influencing the growth, differentiation, and various physiological functions of the reproductive system. Both the breast and thyroid are estrogen-dependent organs, implying that pathology in one organ may affect the other. This study found a significantly higher rate of ER positivity in patients with dual primary cancer compared to those with breast cancer alone, further supporting the role of estrogen in the pathogenesis of both malignancies.
This study compared patients with dual primary cancer of the breast and thyroid to those with a single cancer, revealing significant differences in age, BMI, menopausal status, ER, PR, and HER-2 status between the two groups. The research findings are consistent with previous studies indicating that premenopausal breast cancer patients are more prone to concurrent thyroid cancer, possibly due to higher estrogen levels compared to postmenopausal patients. Additionally, patients with higher BMI have more adipose tissue, contributing to increased estrogen production. Excessive serum estrogen can disrupt the hypothalamus-pituitary-ovary axis, upsetting the balance of tissue proliferation and repair, ultimately leading to abnormal cell transformation and proliferation. ER, a protein molecule present in cell membranes, cytoplasm, and cell nuclei, has a specific binding capacity with estrogen, regulating the growth and differentiation of the reproductive system. PR, an end product of estrogen action, enhances hormonal response to ER, collectively promoting cell growth and development. In numerous hormone-targeted organs, the breast is one such organ where ER and PR play crucial roles in the prognosis of breast cancer. As research advances, the thyroid, in addition to organs like the breast and uterus, has been found to contain a certain amount of ER and PR. Studies indicate that thyroid tumors are hormone-dependent, with ER and PR upregulating the expression of thyroid cell cycle genes, promoting thyroid tumor cell proliferation.15,16 HER-2, an oncogene and a member of the epidermal growth factor receptor family, maintains cell vitality in normal circumstances. However, under certain conditions, HER-2’s oncogenic transformation activity can be activated, leading to uncontrolled cell growth.17,18 In this study, the breast cancer component in patients with dual primary cancer exhibited more aggressive tumor characteristics, including significantly larger median tumor size (3.2 cm vs 2.1 cm, P=0.003) and higher lymph node metastasis rates (68.9% vs 42.7%, OR=2.98). Moreover, these patients had increased tumor-infiltrating lymphocytes (TILs) and PD-L1 positivity (43.1% vs 21.3%), suggesting a distinct immune microenvironment that may contribute to tumor progression. The study results suggest that ER and PR may be involved in the occurrence and development of thyroid cancer, while high HER-2 expression indicates a higher malignancy degree, making tumor cells more prone to metastasis and spread. The higher rate of aggressive breast cancer features in the dual primary cancer group indicates that synchronous breast-thyroid malignancies may represent a biologically distinct entity requiring specialized management. This aligns with the follow-up results of the study, wherein during the 2-year follow-up period, the research group had 12 cases of recurrence and metastasis and 5 deaths, while the control group had 9 cases of recurrence and metastasis and 2 deaths, with a statistically significant difference (P<0.05). This study also focused on the analysis of risk factors in patients with dual primary cancer of the breast and thyroid. Firstly, age was found to be a critical risk factor, indicating that patients of different age groups may face varying risks of developing the condition. With increasing age, the ovarian function of postmenopausal patients gradually weakens, leading to a corresponding decrease in estrogen and progesterone levels. This restricts the growth of normal breast cells, resulting in the atrophy of mammary glands. Simultaneously, due to the weakened immune function in older patients, carcinogenesis is relatively more likely. Moreover, older individuals are also one of the high-incidence populations for thyroid diseases. In the general population, the incidence of thyroid lesions in the age group above 70 is approximately four times that of young people aged 20–30. This suggests that greater attention should be paid to the age-related characteristics of patients when formulating treatment plans. Secondly, a significantly higher rate of ER-positive status was observed in dual primary cancer, which is closely related to the pathogenesis of many breast cancers. ER-positive status is often associated with unique biological behaviors, potentially influencing the pathological evolution of dual primary cancer.19,20 Thus, hormone receptor profiling should be prioritized when considering therapeutic interventions. Additionally, a family history of breast cancer was confirmed as one of the risk factors for dual primary cancer, suggesting that genetic factors may play a crucial role in the occurrence of dual primary cancer. In-depth research on family history helps identify whether patients carry specific genetic mutations, providing more targeted early prevention and screening strategies.
Some studies have indicated an association between a family history of breast cancer, ER status, PF status, and the occurrence of thyroid and breast tumors. However, relevant research reports are relatively limited, with small sample sizes. Large-scale studies are currently primarily limited to preliminary exploratory analyses of monitoring, epidemiological, and ultimate outcome databases in the United States. Due to the limited clinical and pathological data obtained, there is also a relatively scarce number of reports on dual primary cancer of the breast and thyroid over different time sequences. Therefore, the results of this study should be considered preliminary and require validation from multiple sources. It is important to note that this study has some limitations, such as a relatively small sample size and the retrospective nature of the study design. Hence, future large-scale and prospective studies will help validate our findings and provide a more comprehensive understanding of the pathological and clinical characteristics of dual primary cancer of the breast and thyroid.
Conclusion
This study has preliminarily revealed the clinical characteristics of dual primary cancer of the breast and thyroid, providing an initial understanding of this rare condition. In our research, we found that patient age, estrogen receptor (ER) positive status, and a family history of breast cancer are risk factors for dual primary cancer of the breast and thyroid. This discovery holds promise for offering new directions and strategies for future personalized treatment and prevention. By delving into these risk factors, we can better comprehend the mechanisms underlying dual primary cancer and provide more effective diagnostic and treatment plans for patients. However, further validation through larger samples and in-depth studies is needed to gain a more comprehensive understanding of the pathogenesis and therapeutic strategies for dual primary cancer. Through deeper research, we hope to pave the way for new approaches to the treatment and prevention of this rare condition.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics and Consent Statements
This study was approved by the ethics committee of Affiliated People’s Hospital of Shandong First Medical University. Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Barzaman K, Karami J, Zarei Z, et al. Breast cancer: biology, biomarkers, and treatments. Int Immunopharmacol. 2020;84:106535. doi:10.1016/j.intimp.2020.106535
2. Katsura C, Ogunmwonyi I, Kankam HK, et al. Breast cancer: presentation, investigation and management. Br J Hosp Med. 2022;83(2):1–7. doi:10.12968/hmed.2021.0459
3. Roman BR, Morris LG, Davies L. The thyroid cancer epidemic, 2017 perspective. Curr Opin Endocrinol Diabetes Obes. 2017;24(5):332–336. doi:10.1097/MED.0000000000000359
4. Haymart MR. Progress and challenges in thyroid cancer management. Endocr Pract. 2021;27(12):1260–1263. doi:10.1016/j.eprac.2021.09.006
5. Song Y, Wang J, Wang X, et al. Characteristics and survival analysis of breast cancer survivors with metachronous double primary cancers: a retrospective cohort study. Transl Cancer Res. 2023;12(4):939–948. doi:10.21037/tcr-23-301
6. Zhai J, Kong XY, Fang Y, et al. [Clinical characteristics and prognostic analysis of double primary breast cancer and thyroid cancer]. Zhonghua Zhong Liu Za Zhi. 2021;43(12):1287–1291. doi:10.3760/cma.j.cn112152-20210621-00461 Polish
7. Kolak A, Kamińska M, Sygit K, et al. Primary and secondary prevention of breast cancer. Ann Agric Environ Med. 2017;24(4):549–553. doi:10.26444/aaem/75943
8. Chen DW, Lang BHH, McLeod DSA, et al. Thyroid cancer. Lancet. 2023;401(10387):1531–1544. doi:10.1016/S0140-6736(23)00020-X
9. Tori M, Shimo T, Yoshidome K. Novel operative approach to double primary cancers of the breast and thyroid and its effects on cosmesis and the accuracy of follow-up examinations. Asian J Endosc Surg. 2018;11(2):185–188. doi:10.1111/ases.12426
10. Hsu CH, Huang C-L, Hsu Y-H, et al. Co-occurrence of second primary malignancy in patients with thyroid cancer. Qjm. 2014;107(8):643–648. doi:10.1093/qjmed/hcu051
11. Kim JY, Song HS. Metachronous double primary cancer after treatment of breast cancer. Cancer Res Treat. 2015;47(1):64–71. doi:10.4143/crt.2013.215
12. Zhang L, Wu Y, Liu F, et al. Characteristics and survival of patients with metachronous or synchronous double primary malignancies: breast and thyroid cancer. Oncotarget. 2016;7(32):52450–52459. doi:10.18632/oncotarget.9547
13. Pal T, Hamel N, Vesprini D, et al. Double primary cancers of the breast and thyroid in women: molecular analysis and genetic implications. Fam Cancer. 2001;1(1):17–24. doi:10.1023/A:1011541424424
14. Park LC, Jeong JY, Ji JH, et al. Intra-tumoral metastatic double primary carcinoma: synchronous metastatic tumor in lung from breast and thyroid carcinoma. Cancer Res Treat. 2014;46(2):200–203. doi:10.4143/crt.2014.46.2.200
15. Sun L, Yu D-H, Sun S-Y, et al. Expressions of ER, PR, HER-2, COX-2, and VEGF in primary and relapsed/metastatic breast cancers. Cell Biochem Biophys. 2014;68(3):511–516. doi:10.1007/s12013-013-9729-y
16. Chuthapisith S, Permsapaya W, Warnnissorn M, et al. Breast cancer subtypes identified by the ER, PR and HER-2 status in Thai women. Asian Pac J Cancer Prev. 2012;13(2):459–462. doi:10.7314/APJCP.2012.13.2.459
17. Mitrović O, Čokić V, Đikić D, et al. Correlation between ER, PR, HER-2, Bcl-2, p53, proliferative and apoptotic indexes with HER-2 gene amplification and TOP2A gene amplification and deletion in four molecular subtypes of breast cancer. Target Oncol. 2014;9(4):367–379. doi:10.1007/s11523-013-0297-2
18. Li J, Chen Z, Su K, et al. Clinicopathological classification and traditional prognostic indicators of breast cancer. Int J Clin Exp Pathol. 2015;8(7):8500–8505.
19. Hu ZY, Xiao H, Xiao M, et al. Inducing or preventing subsequent malignancies for breast cancer survivors? Double-edged sword of estrogen receptor and progesterone receptor. Clin Breast Cancer. 2018;18(5):e1149–e1163. doi:10.1016/j.clbc.2018.04.009
20. Alghamdi MA, Alsaif A, Altwijri AS, et al. Synchronous incidental double parathyroid adenomas and papillary thyroid carcinoma: a case report with literature review. Niger J Clin Pract. 2021;24(6):954–963. doi:10.4103/njcp.njcp_635_19
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Detecting the Frequency of c.5946delT Pathogenic Variant in the BRCA2 Gene and Associated Risk Factors Among Breast Cancer Patients Visiting Felege Hiwot Referral Hospital and University of Gondar Comprehensive Specialized Hospital
Berhane N, Chekol Z, Seid A
Breast Cancer: Targets and Therapy 2023, 15:421-427
Published Date: 19 June 2023
Thyroid Hormone Changes Correlate to Combined Breast Cancer with Primary Thyroid Cancer
Jin J, Li J, Liu Y, Shi Q, Zhang B, Ji Y, Hu P
Breast Cancer: Targets and Therapy 2024, 16:15-22
Published Date: 9 January 2024