")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Risk Factors of Prolonged Mechanical Ventilation in Post Coronary Artery Bypass Graft Patients: A Scoping Review
Authors Kumalasari RI , Kosasih CE, Priambodo AP
Received 23 June 2024
Accepted for publication 5 February 2025
Published 17 February 2025 Volume 2025:18 Pages 903—915
DOI https://doi.org/10.2147/JMDH.S483973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Regina Indah Kumalasari,1 Cecep Eli Kosasih,2 Ayu Prawesti Priambodo2
1Master Study Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Cecep Eli Kosasih, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Fax +62 02287793411, Email [email protected]
Abstract: Prolonged mechanical ventilation (PMV) following CABG surgery is associated with increased patient morbidity and mortality. A consensus has yet to be reached regarding the time limit for PMV. Various studies have identified factors that influence PMV in patients following CABG surgery, but a review has yet to synthesize the results systematically. This review aimed to identify the definition and factors associated with PMV in patients following isolated CABG surgery. This scoping review used the framework developed by Arksey and O’Malley (2005). Primary sources of information were searched through 5 databases: PubMed, Scopus, Oxford Academy, Sage, and CINAHL and two search engines: Science Direct and Google Scholar, accessed on October 25, 2023. Eight articles with a total of 12,178 participants were included in this review. The PMV time limits used in the studies varied from > 12 hours to > 48 hours. The factors affecting PMV were grouped into preoperative, intraoperative and postoperative, with factors that have a high influence, including NYHA class, acute kidney injury and mediastinitis. Differences in the number of factors examined, criteria, characteristics, and time limits of the PMV used to make the study’s results vary. Establishing guidelines regarding PMV time limits is essential according to current conditions.
Keywords: coronary artery bypass graft, factors, prolonged mechanical ventilation
Introduction
Prolonged Mechanical Ventilation (PMV) is one of the complications after cardiac surgery.1 PMV can be caused by respiratory distress, severe underlying conditions, decreased cardiac function, or infection.2,3 The incidence of prolonged mechanical ventilation in post-CABG patients globally varies depending on various factors and the definition of PMV, ranging from 2.18% to 48.11%.4,5 Until now, there has not been a consensus regarding the time defined as PMV.
PMV can adversely affect patient outcomes following CABG surgery.4 PMV increases mortality and prolongs Length of Stay (LOS) in the ICU and hospital.4,6,7 There is an effective risk score to predict the prognosis of patients with coronary artery disease and help and guide the intensivists for the close follow-up of the patients using the Intermountain Risk Score (IMRS).8,9 A study by Cinar et al (2023) found that IMRS was significantly higher in STEMI patients who did not survive than those who survived.9 According to Cislaghi et al (2009), PMV increases the risk of LOS up to six times higher.10 PMV also increases the risk of delirium and hemofiltration following cardiac surgery.5 Furthermore, the high incidence of ventilator-associated pneumonia can affect patient prognosis.11 Previous research conducted in Iran stated that the dominant predictor for PMV in postoperative cardiac surgery patients was the 24-hour postoperative creatinine value.12 While research conducted in China stated that delirium after CABG surgery was the dominant factor for PMV.13
Various studies have been conducted to find factors affecting PMV in patients following CABG surgery, but studies have yet to be systematically reviewed to explore PMV and its influencing factors. A previous study reported that discontinuing mechanical ventilation, extubation, and prevention of PMV is clinically essential for patients.14 Early extubation following cardiac surgery has beneficial clinical effects, including improved patient comfort, increased patient mobility, decreased respiratory complications and decreased cost of care.15 Therefore, it is essential to explore the factors influencing PMV to help healthcare workers systematically anticipate and effectively manage complications due to PMV.16 Close monitoring and prompt intervention in patients with identified risk factors can contribute to improved postoperative outcomes and reduced healthcare costs.17,18
Based on our literature search, no studies have been systematically reviewed to explore synthesizing PMV and its influencing factors starting from the preoperative, intraoperative and postoperative stages. Based on these considerations, it is necessary to examine the factors that influence PMV in postoperative CABG patients through a scoping review so that it can provide input to anticipate and manage the occurrence of PMV in this population.
Materials and Methods
Design
This review used a scoping review design. Scoping reviews have a more comprehensive conceptual framework to explain relevant research findings. The scoping review framework consists of several stages, including articulating the research question, identifying relevant studies, selecting studies, mapping data, compiling literature search results, summarizing, and reporting.19 This research protocol was not published or registered.
Eligibility Criteria
The articles in this review were selected by three reviewers based on the PRISMA Extension for Scoping Reviews (PRISMA-ScR) (see Figure 1).20 This research article’s questions and eligibility criteria used the PCC (Population, Concept, and Context) approach.21 The research questions in this review are: What is the definition of Prolonged Mechanical Ventilation in postoperative CABG patients? What are the significant factors influencing Prolonged Mechanical Ventilation in postoperative CABG patients?
 |
Figure 1 PRISMA Flow Diagram. Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.20 |
P (Population): Adults and patients post Coronary Artery Bypass Graft surgery.
C (Concept): Prolonged Mechanical Ventilation
C (Context): Risk Factors
The inclusion criteria in this review were full-text articles in English, published from 2013–2023, with case-control, cross-sectional, longitudinal, and cohort study designs that addressed factors affecting PMV in post-CABG patients. Furthermore, this review excluded non-English language studies, qualitative studies, inaccessible full-text publications, and secondary studies.
Data Collection and Analysis
Search Strategy
The literature search was conducted systematically using five databases (PubMed, Scopus, Oxford Academy, Sage, and CINAHL) and two search engines (Science Direct and Google Scholar). It was Accessed on October 25, 2023. The keywords used were
Coronary Artery Bypass Graft OR Coronary Artery Bypass Surgery OR Prolonged Mechanical Ventilation OR Prolonged Mechanical Ventilation OR Factors OR Risk Factor OR Predictor.
Study Selection and Quality Appraisal
Three authors independently selected relevant studies that met the eligibility criteria. The authors used Mendeley Reference Manager to check for duplicates during the initial article selection process. The authors then checked the titles and abstracts. They read the entire paper according to the relevance of the selected research topic and based on the inclusion and exclusion criteria set by the authors. In the final stage of study selection, the authors evaluated each paper that met the inclusion criteria using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case-Control and Cohort Studies.22
Ratings consist of ``Yes”, ``No”, ``Unclear”, and ``Not Applicable”, with each ``Yes” answer worth one and the other answers worth 0. The sum of these ratings determines how suitable the item is for inclusion in this review. This allows researchers to determine the reliability and relevance of their findings for inclusion in further discussion. After the JBI assessment, we excluded all studies with a JBI score below 70, with final approval from the first, second, and third authors, so that the final decision resulted in a unanimous opinion on the appropriateness of the studies to be analyzed in depth in this scoping review.
Data Extraction and Analysis
At the data extraction and analysis stage, this review used extraction tables to describe all research findings related to the research topic. The extraction table contains information related to study characteristics, including author, study design, country, type of surgery, PMV, sample (number of patients and number of PMV patients), study findings (category of factors and PMV factors), and JBI final results. All studies analyzed were primary studies with case-control, cross-sectional and cohort designs. Data analysis was conducted thematically and qualitatively with an exploratory, descriptive approach. The data analysis process began with identifying and presenting the data obtained in tabular form based on the articles reviewed. After the data were obtained, the authors analyzed and discussed the results of each study with a focus on the factors that influence the PMV of patients after CABG surgery. The author categorized these factors into three categories based on the research findings, namely preoperative factors, intraoperative factors and postoperative factors.
Results
Study Selection
The study selection results in the initial stage of this review resulted in 859 articles. The authors then selected articles based on title, abstract, and predetermined inclusion criteria, leaving 41 studies, which were further analyzed based on full-text analysis of the articles. A total of 25 articles were excluded because they were not in English and did not discuss CABG and PMV. Sixteen studies were evaluated using the JBI tool, and one article was excluded due to ineligibility. Seven articles were excluded because the population did not fit the criteria, ie the articles included combined CABG surgery with other heart surgeries such as valve, heart tumour removal, and congenital correction. As a result, eight studies were eligible and included in the final analysis. Figure 1 shows the study selection process, which resulted in eight studies. These studies were analyzed in this scoping review using the PRISMA flowchart.
Study Characteristics
Most studies analyzed in this review were retrospective cohort studies (n=7) and one case-control study. Most studies (n=7) were conducted in developed countries (see Table 1). The total number of participant data was 12,178. The total number of participants who experienced Prolonged Mechanical Ventilation (PMV) was 2,431 participants (19.96%). The prevalence of PMV ranges from 2.18% to 48.11%.4,5 The results of the JBI analysis showed that most studies analyzed by the cohort method were of good quality (>70%). Most of the studies needed improvement in not including follow-up time, the reasons for defaulting not being explained, and the lack of strategies to overcome incomplete follow-up.
Definition of PMV
The time limit defined as PMV differed in each study: >12 hours, >24 hours and >48 hours. Most articles stated that PMV used mechanical ventilation for more than 24 hours (5 articles) (see Table 1). Most articles used 24 hours based on the threshold the Society of Thoracic Surgeons used to define PMV, which is the total time of mechanical ventilation after CABG surgery > 24 hours.13,23,24
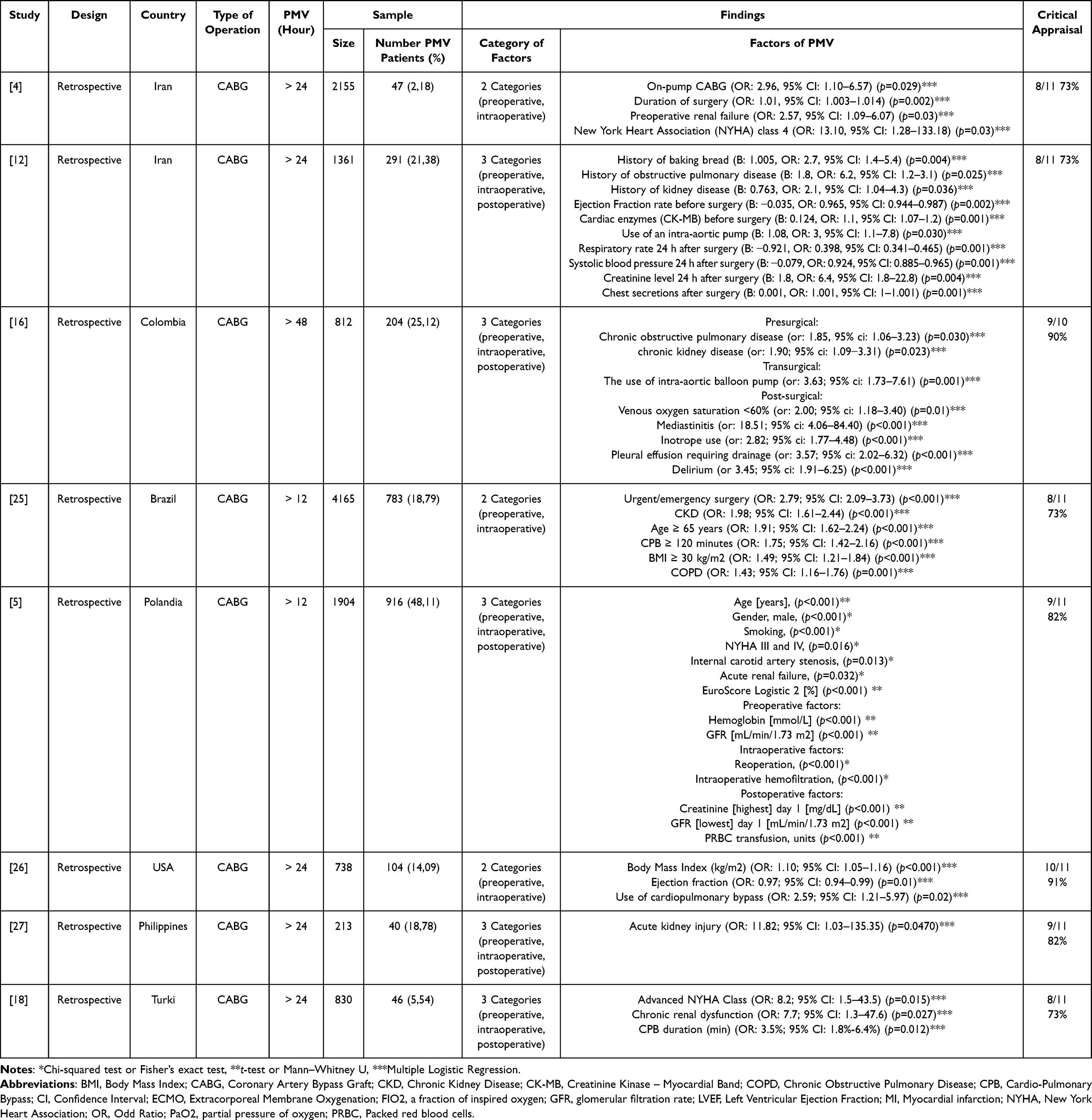 |
Table 1 Characteristics of Study |
Factors Affecting PMV
This review identified factors that significantly affect PMV in CABG patients. The analysis results in this review showed that the factors affecting PMV had heterogeneous results. Based on the analysis, demographic characteristics, clinical conditions before surgery, laboratory test results before surgery, comorbidities, surgical findings, use of intra-operative devices, complications, and clinical findings after surgery have a significant association with PMV in postoperative CABG patients. In order to simplify, we categorized these factors into three categories: preoperative, intraoperative and postoperative factors (see Table 1).
In this review, the factors related to PMV included in the category of preoperative factors were demographic characteristics (age and gender), preoperative clinical conditions (BMI, NYHA class, ejection fraction, emergency surgery, and EuroScore Logistic 2), comorbidities (renal dysfunction, COPD, and internal carotid artery stenosis), history of smoking, and laboratory test results (haemoglobin and CK-MB). Intraoperative factors include surgical findings (long duration of surgery and reoperation) and use of intraoperative devices (IABP, use of CPB machine, and intraoperative hemofiltration). Postoperative factors that significantly influenced PMV were complications (pleural effusion requiring drainage, acute kidney injury, delirium, and mediastinitis) and clinical findings after surgery (chest secretions after surgery, 24-hour systolic blood pressure, 24-hour respiratory frequency, PRBC transfusion, venous oxygen saturation < 60%, and inotropic use). The most dominant significant and included factors from the studies the authors analyzed were using a CPB machine or CPB time (n=4) and renal dysfunction (n=6).
We categorize the factors affecting PMV into three levels based on OR values: low (OR value < 4), medium (OR value ≥ 4 to 8), and high (OR value > 8). Factors at the high level have the most substantial influence, based on the high OR value. On the other hand, factors with OR values below four were categorized as low. Most of the factors are at a low risk of influencing PMV. Factors included in the moderate level were renal dysfunction and COPD. Factors that strongly influence include NYHA class, mediastinitis and acute kidney injury after surgery.
Discussion
The review found various factors affecting PMV, which authors grouped into three categories: preoperative, intraoperative, and postoperative (see Table 2). Preoperative factors that most influence PMV are clinical conditions such as NYHA class III and IV.4,18,23 High NYHA class indicates the patient’s inability to tolerate early weaning due to poor cardiovascular reserve.4 Patients with left ventricular dysfunction and low ejection fraction also take more time to achieve hemodynamic stability due to decreased end-diastolic volume and cardiac output, which leads to decreased cardiac preload and afterload. Therefore, patients may need a more extended period of mechanical ventilation to reach weaning criteria.12 The prognostic role of cardiac reserve and the predictive value of parameters such as SYNTAX and EuroSCORE II scores are valuable for early detection of possible postoperative complications.28–30 PMV patients have parameters similar to those with high SYNTAX and EuroSCORE II scores.28,29 The combination of EuroSCORE II and SYNTAX scores is also helpful in predicting early major complications after CABG surgery.31 High Euroscore scores are predictors of PMV, while low Euroscore 2 scores indicate faster extubation in cardiac surgery patients.5,32
 |
Table 2 Factors Affecting PMV Following CABG Surgery |
Preoperative clinical conditions such as emergency surgery status and the presence of internal carotid artery stenosis may indicate poor patient condition even before surgery, which in turn can increase the risk of postoperative complications such as PMV.5,25 Internal carotid artery stenosis in CAD patients can cause decreased cerebral perfusion and cognitive impairment such as delirium which makes it difficult for patients to wean ventilators. The risk of PMV after CABG surgery increases in patients with internal carotid artery stenosis, plus other risk factors such as advanced age, renal dysfunction, PPOK, CHF, and myocardial infarction.33–35 Laboratory examinations such as cardiac enzyme CK-MB and haemoglobin before surgery can also provide helpful information to predict PMV.5,12 Elevated CK-MB levels may indicate myocardial damage.36 In contrast, preoperative low haemoglobin may reduce the body’s ability to transport oxygen and increase stress on the cardiovascular system.37 Both can potentially lead to complications such as respiratory failure requiring prolonged use of mechanical ventilation.38 Other preoperative factors that have a significant influence on PMV are comorbidities such as renal dysfunction and COPD.12,18 Renal dysfunction can lead to fluid and electrolyte imbalances, which can develop respiratory complications and prolonged need for mechanical ventilation.39 The majority of COPD patients undergoing CABG are reported to require long-term mechanical ventilation or more than 48 hours due to significantly reduced vital capacity, total lung capacity, and functional residual capacity, which also results in proportionally increased mortality.40 Smoker status also has a significant impact on the post-CABG functional capacity decline, with active smokers more prone to prolonged ventilator use and atelectasis.41 Smoking is one of the preoperative risk factors that may increase postoperative complications.5,41
Demographic characteristics such as age, gender, and high body mass index also influence PMV.5,25,26 Older patients have an increased risk of low cardiac output syndrome (LCOS), which contributes to the occurrence of PMV after CABG surgery.42 In addition, older age is associated with a higher probability of comorbidities such as diabetes, which can further complicate recovery and increase the risk of postoperative complications that require prolonged use of mechanical ventilation.43 Women are reportedly more at risk of PMV than men.1,44 The reason for the high incidence of prolonged mechanical ventilation among women is that women more often show symptoms of coronary heart disease at an advanced age (because it is associated with decreased levels of the hormone estrogen, which is said to inhibit atherosclerosis), so comorbid conditions are more often found.45 A high body mass index may also increase the complexity of the surgical procedure and hinder postoperative pulmonary rehabilitation.46
Based on our review, events during surgery can also predict the occurrence of PMV after CABG surgery. Intraoperative factors that influence the occurrence of PMV include the initiation of the use of assistive devices during surgery, such as IABP and CPB machines.4,12,16,18,25,26 This may be due to the worsening of the patient’s condition during surgery, which requires invasive device support to stabilize their hemodynamics. However, the use of devices such as CPB machines can also trigger the release of inflammatory mediators due to the extracorporeal processing of blood, which ultimately contributes to pulmonary oedema so that respiratory failure and PMV can occur.47 The use of CPB machines is the most dominant intraoperative factor in PMV. Longer CPB machine use increases the risk of PMV, whereas an increase of 1 minute above 82.5 minutes is associated with a 3.5% increased risk of PMV.18 Intraoperative use of IABP has also been reported to increase the duration of mechanical ventilation three times longer.12 This may be related to the unstable hemodynamics of patients with IABP, resulting in difficulty weaning patients from mechanical ventilation.48
Other intraoperative factors that affect PMV are the duration of surgery and reoperation. The long duration of CABG surgery is due to various factors, including the complexity of the surgical procedure, successful weaning of the heart from the cardiopulmonary bypass machine, and the surgeon’s skill.49 Research conducted by Totonchi et al (2014) reported that operating time> 4 hours affects the occurrence of PMV (p<0,001).1 Reoperation also increases the risk of prolonged use of mechanical ventilation related to anatomical and physiological changes, such as the presence of scar tissue from previous surgery, which has the potential to cause longer operating times and increased trauma to surrounding tissues.50 In addition, reoperation is often caused by complications such as bleeding or infection, which can further increase the inflammatory response, exacerbating postoperative complications such as respiratory distress and requiring prolonged ventilatory support.51,52
Clinical findings and postoperative complications of CABG were significant predictors of PMV. Postoperative acute kidney injury (AKI) increases the risk of PMV by 11 times.27 with serum creatinine levels as a marker of diagnosis and prognosis.53 Postoperative AKI characterized by elevated serum creatinine levels may be due to intraoperative hypotension and cardiac complications resulting in renal hypoperfusion and may also be a systemic inflammatory response and multiorgan dysfunction. AKI can lead to respiratory insufficiency and the need for prolonged ventilatory support.53,54 The next most significant postoperative complication affecting PMV is mediastinitis. Patients with mediastinitis had an 18.51- times higher risk of PMV.16 Gram-negative bacterial infections cause the majority of mediastinitis. However, in rare cases, it can also be caused by fungal infections such as Aspergillus, which can contribute to the complexity of treatment and potentially prolong the need for mechanical ventilation.55,56 Delirium after CABG surgery may also increase the risk of PMV by 3-fold.16 Delirium may result from increased inflammatory mediators, subclinical cerebral infarction, neurotransmitter changes, generalized hypoperfusion, and perioperative cellular hypoxia, which may be exacerbated by prolonged bypass time.57 Pleural effusion requiring drainage increases the risk of PMV by 3.57 times.58 Pleural effusion can increase intrathoracic pressure, decrease cardiac output, shock volume, and mean arterial pressure, resulting in respiratory distress requiring prolonged mechanical ventilation.59
Postoperative clinical findings such as bleeding requiring transfusion increased the risk of PMV by 23- times.44 Bleeding after cardiac surgery can have severe consequences such as pericardial tamponade, infection, and organ dysfunction, making it difficult to wean patients from mechanical ventilation.60 Anemia due to bleeding reduces oxygen delivery to body tissues, so patients experience hypoxic anaemia.49 Furthermore, when postoperative bleeding occurs, the patient will require transfusions, which could potentially result in transfusion-related lung injury or circulatory overload due to massive transfusions to manage the bleeding.7
Another clinical parameter is the number of breaths in 24 hours, a protective factor. By increasing each unit of RR, PMV decreases by 0.921 hours.12 In addition, the amount of chest secretions in the first hour and second hour after surgery also affects PMV, which is attributed to the establishment of proper chest drainage with the removal of secretions, preventing pressure on the heart and lungs.12 The use of inotropic (including epinephrine, dobutamine or dopamine) as a post-surgical variable was shown to be a strong predictor for PMV after CABG.1,16 Postoperative systolic blood pressure is associated with the duration of mechanical ventilation.12 This could be because blood pressure is directly related to the amount of ventilation; it is understood that if blood pressure decreases or increases, the volume of blood exchanged with air in the lungs changes, which will result in a direct effect on the ventilation rate.12
Several laboratory results after CABG surgery may also be predictors of PMV. Studies have consistently shown that low levels of venous oxygen saturation, specifically central venous oxygen saturation (ScvO2) below 60%, are associated with unfavourable outcomes following cardiac surgery.16,61 A low level of venous saturation reflects an imbalance between oxygen supply and demand, which can lead to inadequate tissue oxygenation and hemodynamic instability that ultimately causes the patient to require prolonged use of mechanical ventilation.62
Identifying risk factors is essential to optimize patient care and improve recovery after CABG surgery. Nurses are critical in assessing and managing risk factors to prevent PMV and related complications. By recognizing these factors early, nurses can implement targeted interventions such as respiratory care, mobilization, and early ambulation to reduce the risk of PMV. In addition, close monitoring and prompt intervention in patients with identified risk factors can contribute to improved postoperative outcomes and reduced healthcare costs.
Strengths and Limitations
The limitation of this scoping review is that it is difficult for the authors to group the factors and classify the level of factors into three categories. Because the articles the authors analyzed were quite heterogeneous, the results obtained in each article varied depending on the characteristics and variables used. In addition, the PMV time threshold used in these studies is not uniform, which may affect the findings in this article, so it becomes our limitation. Research on factors affecting PMV measured using the same time threshold can be conducted to obtain more specific and accurate results.
Despite some limitations, this review is a complete and up-to-date review that discusses PMV in CABG patients, categorizing factors into three stages: preoperative, intraoperative, and postoperative. In addition, this review used articles assessed using the JBI tool so that the articles analyzed in this review were of good quality. This review may provide a deeper understanding of the factors influencing PMV in CABG patients. Thus, it may help healthcare professionals allocate postoperative medical resources immediately after CABG surgery so that PMV can be prevented and managed correctly.
Conclusion
Based on the analysis of eight articles, various risk factors affecting the occurrence of PMV can be categorized into preoperative, intraoperative and postoperative factors. Factors that strongly influence PMV are NYHA class, mediastinitis and postoperative acute kidney injury. Among all the factors affecting PMV, the advanced NYHA class (3 and 4) was the most dominant factor from the articles studied. This makes incorporating NYHA class assessment before CABG surgery into CABG preoperative guidelines or checklists necessary. Evidence suggests that NYHA class evaluation can provide valuable insight into the functional status of patients and assist in PMV risk stratification after CABG surgery. In addition, results vary between studies, which may be due to differences in the number of factors examined, criteria, characteristics, and PMV cutoffs used. Therefore, it is essential to establish guidelines regarding the PMV time limit according to current conditions. Its use still takes into account patient characteristics and guidelines at each institution.
Acknowledgments
All authors thank Universitas Padjadjaran for facilitating the database and supporting funding for this review.
Disclosure
The authors report no conflicts of interest in this research.
References
1. Totonchi Z, Baazm F, Chitsazan M, Seifi S, Chitsazan M. Predictors of prolonged mechanical ventilation after open heart surgery. J Cardiovasc Thorac Res. 2014;6(4):211–216. doi:10.15171/jcvtr.2014.014
2. Sanson G, Sartori M, Dreas L, Ciraolo R, Fabiani A. Predictors of extubation failure after open-chest cardiac surgery based on routinely collected data. The importance of a shared interprofessional clinical assessment. Eur J Cardiovasc Nurs. 2018;17(8):751–759. doi:10.1177/1474515118782103
3. Stone IRJ, Schwartz L, Schwartz L. Risk stratification for prolonged mechanical ventilation after cardiac surgery in children. J Cardiothorac Vasc Anesth. 2020;34(4):949–950. doi:10.1053/j.jvca.2019.12.017
4. Amini S, Morovatdar N, Karrari SP, et al. the risk factors of prolonged mechanical ventilation after isolated coronary artery bypass graft surgery. Evid Based Care J. 2023;31(1):7–14.
5. Kotfis K, Szylińska A, Listewnik M, et al. Balancing intubation time with postoperative risk in cardiac surgery patients – a retrospective cohort analysis. Ther Clin Risk Manag. 2018;14:2203–2212. doi:10.2147/TCRM.S182333
6. Bartz RR, Ferreira RG, Schroder JN, et al. Prolonged pulmonary support after cardiac surgery: incidence, risk factors and outcomes: a retrospective cohort study. J Crit Care. 2015;30(5):940–944. doi:10.1016/j.jcrc.2015.04.125
7. Zochios V, Chandan JS, Schultz MJ, et al. The effects of escalation of respiratory support and prolonged invasive ventilation on outcomes of cardiac surgical patients: a retrospective cohort study. J Cardiothorac Vasc Anesth. 2020;34(5):1226–1234. doi:10.1053/j.jvca.2019.10.052
8. Ilker H M, Faysal S, Çağdaş Y A, Murat S, Ç T. Prognostic value of intermountain risk score for short- and long-term mortality in patients with cardiogenic shock. Coron Artery Dis. 2023;34(2):154–159. doi:10.1097/MCA.0000000000001219
9. Çınar T, Şaylık F, Akbulut T, et al. Evaluation of intermountain risk score for short- and long-term mortality in ST Elevation myocardial infarction patients. Angiology. 2023;74(4):357–364. doi:10.1177/00033197221105753
10. Cislaghi F, Condemi AM, Corona A. Predictors of prolonged mechanical ventilation in a cohort of 5123 cardiac surgical patients. Eur J Anaesthesiol. 2009;26(5):396–403. doi:10.1097/EJA.0b013e3283232c69
11. Zhang ZY, Cui R, An B, An B. A study of mechanical ventilation in the ICU after cardiac surgery: a bibliometric analysis. J Thorac Dis. 2022;14(4):1212–1224. doi:10.21037/jtd-22-233
12. Rahimi S, Abdi A, Salari N, Shohaimi S, Naghibeiranvand M. Factors associated with long-term mechanical ventilation in patients undergoing cardiovascular surgery. BMC Cardiovasc Disord. 2023;23(1):1–9. doi:10.1186/s12872-023-03315-7
13. Meng Y, Gu H, Qian X, et al. Establishment of a nomogram for predicting prolonged mechanical ventilation in cardiovascular surgery patients. Eur J Cardiovasc Nurs. 2023;22(6):594–601. doi:10.1093/eurjcn/zvac076
14. Fonseca L, Vieira FN, Azzolin KDO. Factors associated to the length of time on mechanical ventilation in the postoperative period of cardiac surgery. Rev Gaúcha Enferm. 2014;35(2):67–72. doi:10.1590/1983-1447.2014.02.44697
15. Firoozabadi MD, Ebadi A, Sheikhi MA. Extubation time and postoperative blood pressure in CABG patient. Bali Med J. 2017;6(1):186. doi:10.15562/bmj.v6i1.475
16. Daza-Arana JE, Lozada-Ramos H, Ávila-Hernández DF, Ordoñez-Mora LT, Sánchez DP. Prolonged mechanical ventilation following coronary artery bypass graft in Santiago de Cali, Colombia. Vasc Health Risk Manag. 2022;18:767–781. doi:10.2147/VHRM.S367108
17. Flegler S, Paro FM. Factors associated with intubation time and ICU stay after CABG. Brazilian J Cardiovasc Surg. 2015;30(6):631–635.
18. Gumus F, Polat A, Yektas A, et al. Prolonged mechanical ventilation after CABG: risk factor analysis. J Cardiothorac Vasc Anesth. 2015;29(1):52–58. doi:10.1053/j.jvca.2014.09.002
19. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol Theory Pract. 2005;8(1):19–32. doi:10.1080/1364557032000119616
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372.
21. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
22. Joanna Briggs Institute (JBI). JBI’s critical appraisal tools [Internet]. Joanna Briggs Institute. 2022. Available from: //jbi.global/critical-appraisal-tools..
23. Michaud L, Dureau P, Kerleroux B, et al. Development and validation of a predictive score for prolonged mechanical ventilation after cardiac surgery. J Cardiothorac Vasc Anesth. 2022;36(3):825–832. doi:10.1053/j.jvca.2021.07.016
24. Sharma V, Rao V, Manlhiot C, Boruvka A, Fremes S, Wąsowicz M. A derived and validated score to predict prolonged mechanical ventilation in patients undergoing cardiac surgery. J Thorac Cardiovasc Surg. 2017;153(1):108–115. doi:10.1016/j.jtcvs.2016.08.020
25. Dallazen-Sartori F, Albuquerque LC, Magedanz EH, et al. Risk score for prolonged mechanical ventilation in coronary artery bypass grafting. Int J Cardiovasc Sci. 2021;34(3):264–271.
26. Wise ES, Stonko DP, Glaser ZA, et al. Prediction of prolonged ventilation after coronary artery bypass grafting: data from an artificial neural network. Heart Surg Forum. 2017;20(1):E7–14. doi:10.1532/hsf.1566
27. Acosta JJS, Orcasitas JF. Predictors of prolonged mechanical ventilation after CABG among Filipino adults with CAD. SPMC J Heal Care Serv. 2016;2(1):29–39.
28. Hayıroğlu Mİ, Keskin M, Uzun AO, et al. Predictors of in-hospital mortality in patients with st-segment elevation myocardial infarction complicated with cardiogenic shock. Heart Lung Circ. 2019;28(2):237–244. doi:10.1016/j.hlc.2017.10.023
29. Hayıroğlu Mİ, Keskin M, Uzun AO, et al. Predictive value of SYNTAX score II for clinical outcomes in cardiogenic shock underwent primary percutaneous coronary intervention; a pilot study. Int J Cardiovasc Imaging. 2018;34(3):329–336. doi:10.1007/s10554-017-1241-9
30. Hayıroğlu Mİ, Çanga Y, Yıldırımtürk Ö, et al. Clinical characteristics and outcomes of acute coronary syndrome patients with intra-aortic balloon pump inserted in intensive cardiac care unit of a tertiary clinic. Turk Kardiyol Dern Ars. 2018;46(1):10–17. doi:10.5543/tkda.2017.11126
31. Fukui T, Uchimuro T, Takanashi S. EuroSCORE II with SYNTAX score to assess risks of coronary artery bypass grafting outcomes. Eur J Cardiothorac Surg. 2015;47(1):66–71. doi:10.1093/ejcts/ezu045
32. Bauer A, Korten I, Juchem G, Kiesewetter I, Kilger E, Heyn J. EuroScore and IL-6 predict the course in ICU after cardiac surgery. Eur J Med Res. 2021;26(1). doi:10.1186/s40001-021-00501-1
33. Lal BK, Dux MC, Sikdar S, et al. Asymptomatic carotid stenosis is associated with cognitive impairment. J Vasc Surg. 2017;66(4):1083–1092. doi:10.1016/j.jvs.2017.04.038
34. Tariq K, Khushk SA, Tareen I, et al. Elevated glycosylated hemoglobin is harbinger of adverse short-term outcomes following coronary artery bypass grafting. Pakistan Hear J. 2021;54(1):79–84. doi:10.47144/phj.v54i1.2069
35. Fitch ZW, Debesa O, Ohkuma R, et al. A protocol-driven approach to early extubation after heart surgery. J Thorac Cardiovasc Surg. 2014;147(4):1344–1350. doi:10.1016/j.jtcvs.2013.10.032
36. Rashid S, Malik A, Khurshid R, Faryal U, Qazi S. The diagnostic value of biochemical cardiac markers in acute myocardial infarction. IntechOpen. 2016;13.
37. Warner MA, Hanson AC, Schulte PJ, et al. Preoperative anemia and postoperative outcomes in cardiac surgery: a mediation analysis evaluating intraoperative transfusion exposures. Anesth Analg. 2024;138(4):728–737. doi:10.1213/ANE.0000000000006765
38. Mahmood E, Knio ZO, Mahmood F, et al. Preoperative asymptomatic leukocytosis and postoperative outcome in cardiac surgery patients. PLoS One. 2017;12(9):e0182118. doi:10.1371/journal.pone.0182118
39. Fan PY, Chen CY, Lee CC, et al. Impact of renal dysfunction on surgical outcomes in patients with aortic dissection. Med. 2019;98(20):e15453.
40. Ovalı C, Şahin A. Chronic obstructive pulmonary disease and off-pump coronary surgery. Ann Thorac Cardiovasc Surg. 2018;24(4):193–199. doi:10.5761/atcs.oa.17-00231
41. Alsubaiei ME, Althukair W, Almutairi H. Functional capacity in smoking patients after coronary artery bypass grafting surgery: a quasi-experimental study. J Med Life. 2023;16(12):1760. doi:10.25122/jml-2023-0282
42. Ding WJ, Ji Q, Shi YQ, Ma RH. Predictors of low cardiac output syndrome after isolated coronary artery bypass grafting. Int Heart J. 2015;56(2):144–149. doi:10.1536/ihj.14-231
43. Kotfis K, Szylińska A, Listewnik M, Brykczyński M, Ely EW, Rotter I. Diabetes and elevated preoperative HbA1c level as risk factors for postoperative delirium after cardiac surgery: an observational cohort study. Neuropsychiatr Dis Treat. 2019;15:511–521. doi:10.2147/NDT.S196973
44. Aksoy R, Karakoc AZ, Cevirme D, et al. Predictive factors of prolonged ventilation following cardiac surgery with cardiopulmonary bypass. Brazilian J Cardiovasc Surg. 2021;36(6):780–787. doi:10.21470/1678-9741-2020-0164
45. Blasberg JD, Schwartz GS, Balaram SK. The role of gender in coronary surgery. Eur J Cardiothorac Surg. 2011;40(3):715–721.
46. Saleh HZ, Shaw M, Al-Rawic O, et al. Outcomes and predictors of prolonged ventilation in patients undergoing elective coronary surgery. Interact Cardiovasc Thorac Surg. 2012;15(1):51–56. doi:10.1093/icvts/ivs076
47. Huffmyer JL, Groves DS. Pulmonary complications of cardiopulmonary bypass. Best Pract Res Clin Anaesthesiol. 2015;29(2):163–175. doi:10.1016/j.bpa.2015.04.002
48. Keranovic S, Salihovic E, Zrnanovic D, Prelic M, Piric A, Kikanovic T. Inotropic and mechanical support of critically Ill patient after cardiac surgery. Med Arch. 2020;74(3):236–239. doi:10.5455/medarh.2020.74.236-239
49. Sudjud RW, Kadarsah RK, Hintono EDC. Angka kejadian ventilasi mekanis berkepanjangan pada pasien pasca bedah pintas arteri koroner di RSUP Dr. Hasan Sadikin Bandung Tahun 2014–2016. J Anestesi Perioper. 2020;8(1):47–55. doi:10.15851/jap.v8n1.2015
50. Faritous ZS, Aghdaie N, Yazdanian F, Azarfarin R, Dabbagh A. Perioperative risk factors for prolonged mechanical ventilation and tracheostomy in women undergoing coronary artery bypass graft with cardiopulmonary bypass. Saudi J Anaesth. 2011;5:167–9.
51. Stojkovic B, Jovanovic T, Vukovic P, et al. Blood loss and intraoperative salvage procedure in patients underwent coronary artery bypass reoperative surgery. J Clin Exp Cardiolog. 2013;04(04).
52. Kristensen KL, Rauer LJ, Mortensen PE, Kjeldsen BJ. Reoperation for bleeding in cardiac surgery. Interact Cardiovasc Thorac Surg. 2012;14(6):709–713. doi:10.1093/icvts/ivs050
53. Palomba H, De Castro I, Neto ALC, Lage S, Yu L. Acute kidney injury prediction following elective cardiac surgery: AKICS Score. Kidney Int. 2007;72(5):624–631. doi:10.1038/sj.ki.5002419
54. Rosner MH, Okusa MD. Acute kidney injury associated with cardiac surgery. Clin J Am Soc Nephrol. 2006;1(1):19–32. doi:10.2215/CJN.00240605
55. Charbonneau H, Maillet JM, Faron M, et al. Mediastinitis due to Gram-negative bacteria is associated with increased mortality. Clin Microbiol Infect. 2014;20(3). doi:10.1111/1469-0691.12369
56. Monteiro OMC, Higa Júnior MG, Palhares MA, de O NM, de SC MM, Chang MR. A rare case of aspergillus mediastinitis after coronary artery bypass surgery: a case report and literature review. Am J Case Rep. 2021;22(1). doi:10.12659/AJCR.933193
57. Patel AK, V. BK, Clarke EC, et al. Delirium in children after cardiac bypass surgery. Pediatr Crit Care Med. 2017;18(2):165–171. doi:10.1097/PCC.0000000000001032
58. Williams BJ, Bannon P. Predictors of pleural effusion after coronary artery bypass surgery. Heart Lung Circ. 2021;30:S54–5.
59. Khaja M, Santana Y, Guerra MAR, et al. Isolated left atrial cardiac tamponade caused by pleural effusion. Cureus. 2020;12(11). doi:10.7759/cureus.11578
60. Xuejie L, Wang R, Sun D, et al. Risk factors for hypocoagulability after cardiac surgery: a retrospective study. Clin Appl Thromb. 2023;29.
61. Lanning KM, Erkinaro TM, Ohtonen PP, et al. Accuracy, precision, and trending ability of perioperative central venous oxygen saturation compared to mixed venous oxygen saturation in unselected cardiac surgical patients. J Cardiothorac Vasc Anesth. 2022;36(7):1995–2001. doi:10.1053/j.jvca.2021.08.103
62. Ranucci M, Isgrò G, Carlucci C, De La Torre T, Enginoli S, Frigiola A. Central venous oxygen saturation and blood lactate levels during cardiopulmonary bypass are associated with outcome after pediatric cardiac surgery. Crit Care. 2010;14(4):1–10. doi:10.1186/cc9217
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.