")
Back to Journals » Cancer Management and Research » Volume 16
Safety and Efficacy of Neoadjuvant Chemoimmunotherapy versus Chemotherapy for Non-Small Cell Lung Cancer Undergoing Sleeve Resection
Authors Qiu Y , Yu J, Guo Q, Xu J
Received 8 December 2023
Accepted for publication 8 August 2024
Published 11 September 2024 Volume 2024:16 Pages 1221—1230
DOI https://doi.org/10.2147/CMAR.S453924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bilikere Dwarakanath
Yanjun Qiu, Jinjiang Yu, Quanmin Guo, Jingyan Xu
Department of Cardiothoracic Surgery, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou City, Zhejiang Province, People’s Republic of China
Correspondence: Jingyan Xu, Department of Pharmacy, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, No. 100 Minjiang Boulevard Kecheng District, Quzhou City, Zhejiang Province, 324000, People’s Republic of China, Email [email protected]
Abstract: The prognosis of locally advanced non-small cell lung cancer (NSCLC) remains poor despite the addition of neoadjuvant chemotherapy, as it has been shown to improve 5-year absolute benefit survival by only 5%. Recently, neoadjuvant immunotherapy with immune checkpoint inhibitors (ICIs), combined with chemotherapy has shown promise in the treatment of locally advanced NSCLC. For NSCLC invading the main bronchus, sleeve resection has become the preferred modality to avoid pneumonectomy and reserve more cardiac or pulmonary function and to reduce postoperative morbidity and mortality. However, there has been a paucity of evidence to evaluate the safety and efficacy of neoadjuvant chemoimmunotherapy on bronchial-vascular reconstruction owing to the limited number of patients treated by sleeve lobectomy. Despite promising initial results, key knowledge gaps remain, including the impact on bronchial-vascular reconstruction, biomarkers predictive of ICI response, and the potential for specific perioperative complications associated with neoadjuvant chemoimmunotherapy in the context of sleeve resection. This review summarizes the latest literature evidence on the efficacy and safety of neoadjuvant chemoimmunotherapy approaches to address the unmet needs of sleeve resection of NSCLC treatment, describes the biomarkers predictive of ICI responses, and perioperative outcomes of sleeve resection after neoadjuvant chemoimmunotherapy.
Keywords: NSCLC, neoadjuvant chemotherapy, immune checkpoint inhibitors, sleeve lobectomy
Introduction
Lung cancer is the leading cause of cancer with high morbidity and mortality rates. An estimated 1.2 million diagnosed cases and 1.8 million deaths of lung cancer are reported yearly worldwide.1 In 2022, an estimated 0.87 million new cases and 0.76 million deaths of lung cancer were reported in China.2 Among lung cancer sub-types, non-small cell lung cancer (NSCLC) accounts for over 85% of all cases.3,4 The prognosis for lung cancer remains poor, with the 5-year overall survival (OS) for Stage III lung cancer after diagnosis estimated to be below 20%.3,5,6
The International Association for the Study of Lung Cancer (IASLC) has recently proposed updates to the TNM stage groups in the upcoming ninth edition of the TNM classification for lung cancer. These updates aim to make the classification system more detailed and provide more accurate prognostic information. One of the key changes is the subdivision of the T descriptors, which will offer more precise information on tumor size and extent. Additionally, the N and M descriptors have been refined to better categorize nodal involvement and distant metastasis. This level of detailed staging is crucial because it directly influences treatment decisions and prognostic assessments. For example, being able to distinguish between T2a and T2b tumors can significantly impact the chosen therapeutic approach and the expected outcomes.6
For lung cancer invading the main bronchus, sleeve resection was recommended to avoid pneumonectomy and reserve more cardiac or pulmonary function, with promising perioperative and survival outcomes.7 Historically, the value of neoadjuvant chemotherapy is limited, with an increase of only 5% in 5-year survival compared to surgery alone.8 Hence, neoadjuvant chemoimmunotherapy is gaining prominence as it has been shown to reduce tumour progression and improve surgical prognosis, thereby playing an important role in the treatment of lung cancer.9,10
Immuno-oncology is a field of cancer treatment that uses the body’s immune system to fight cancer.11 Checkpoint inhibitors, such as programmed cell death receptor 1 (PD-1) and programmed cell death ligand 1 (PD-L1) inhibitors, block proteins that prevent the immune system from attacking cancer cells.12 Recently, programmed cell death receptor 1 (PD-1) and programmed cell death ligand 1 (PD-L1) checkpoint inhibitors have shown promise the treatment strategy in many advanced solid tumors, including NSCLC.13,14 Further, neoadjuvant chemoimmunotherapy before resection improves the antitumor response, which could lead to long-term protection.15 However, there has been a paucity of evidence to evaluate the safety and efficacy of neoadjuvant chemoimmunotherapy on bronchial-vascular reconstruction owing to the limited number of patients treated by sleeve resection. It is important to evaluate outcomes with chemoimmunotherapy specifically in sleeve resection patients due to the surgical complexity involved and the uncertainty about its impacts on bronchial-vascular healing and perioperative complications.9 Understanding these outcomes is critical for optimizing treatment strategies and improving surgical prognosis in the patients treated by sleeve resection.
Current evidence gaps include limited data on the safety and efficacy of neoadjuvant chemoimmunotherapy in patients undergoing sleeve resection, particularly regarding its impact on surgical outcomes, bronchial-vascular healing, and long-term survival benefits. In this review, we summarize the efficacy and safety of neoadjuvant chemoimmunotherapy approaches to address the unmet needs of sleeve resection of lung cancer treatment, describe the biomarkers predictive of ICI response, perioperative outcomes of sleeve resection after neoadjuvant chemoimmunotherapy.
Pulmonary Sleeve Resection
Pulmonary sleeve resection is a complex surgical procedure and reconstruction surgery typically performed for patients with locally advanced NSCLC that involves main bronchus or vascular structures.16 Historically, pneumonectomy has frequently been chosen for centrally located tumors involving the main bronchus or main artery. However, recently multiple studies have shown that sleeve resection could be a valid alternative to pneumonectomy, as it enables the removal of a lung tumor without necessitating a pneumonectomy. This procedure requires surgeons to complete airway reconstruction while removing the tumor, which preserves pulmonary function and provides a better postoperative quality of life. Compared to pneumonectomy, sleeve resection has shown to provide lower morbidity and mortality.17,18 Studies have shown that sleeve resection after chemoimmunotherapy to provide better perioperative and survival outcomes.9,19
Efficacy of Neoadjuvant Chemoimmunotherapy in Patients with Sleeve Resection of Lung
Studies have shown that immunotherapy combined with chemotherapy can yield better efficacy than chemotherapy alone as neoadjuvant therapy in patients with sleeve resection of lung.9,15 In a retrospective study, Dai F et al shown the chemoimmunotherapy group had more sleeve resection (36.84% vs 10.26%, p=0.039), pathological complete response (pCR) rate (57.89% vs 5.13%, P<0.001) and major pathologic response (MPR) rate (78.95% vs 10.26%, P<0.001) compared to the chemotherapy group. Further, neoadjuvant chemoimmunotherapy provided significantly better OS (P = 0.014), and longer DFS (P = 0.006) compared to chemotherapy by shrinking tumors.20 In another retrospective study, preoperative radiological evaluation of patients with NSCLC after chemoimmunotherapy revealed that 30.4% patients achieved pCR, 56.5% achieved MPR. Following chemoimmunotherapy, complete resection was accomplished for all patients.9 NADIM Phase II trial evaluated the efficacy of neoadjuvant chemoimmunotherapy (nivolumab plus paclitaxel and carboplatin) in resectable stage IIIA NSCLC, followed by surgical resection. Among the 35 lobectomies (85.3%), 3 of which were sleeve lobectomies (9.4%). After neoadjuvant chemoimmunotherapy, complete resection (R0) was achieved in all patients who underwent surgery after neoadjuvant chemoimmunotherapy. Downstaging was observed in 90.2% and MPR in 82.9% of the patients.15
Additionally, while it is difficult to determine the timing of surgery after neoadjuvant immunotherapy, achieving a suitable timing is important to achieve superior outcomes. While early surgery may lead to surgical complications, delayed surgery may lead to progression of the tumor. A recent consensus statement suggests performing surgery 4 to 6 weeks after the completion of the last dose of immunotherapy. This interval allows for sufficient tumor response while minimizing the risk of immunotherapy-related adverse events and complications during surgery.21
In a study conducted by Hong et al, among the 25 patients with NSCLC involved in the study, 52% of the patients underwent sleeve resection following chemoimmunotherapy. Around 52% patients achieved an MPR with 32% of these patients having a pCR. Around 88% patients showed radiological regression, and three (12%) patients had stable disease.22 Further, in a real-world study, Gao et al assessed 44 patients with NSCLC who underwent robotic-assisted thoracic surgery after three doses of neoadjuvant chemoimmunotherapy. Among them, 4.5% underwent sleeve resection. Of the overall patients, after chemoimmunotherapy, 81.8% patients achieved MPR, and 59.1% achieved pCR.23
In a recent study, Cheng et al demonstrated the efficacy of sleeve lobectomy after neoadjuvant chemoimmunotherapy (vs chemotherapy) in patients with squamous cell lung cancer. Compared with the chemotherapy, a significant advantage with the chemoimmunotherapy was observed as the rate of pCR (42.9% vs 6.1%) and MPR (50.0% vs 15.2%) was high in the chemoimmunotherapy cohort compared to chemotherapy cohort.19 In a retrospective study, Li et al showed that pCR of chemoimmunotherapy was significantly superior to chemotherapy alone (28.2% vs 4.1%, P < 0.001) and no significant differences were noted in postoperative morbidity after sleeve resection.24
First-line treatment with nivolumab plus ipilimumab provided longer overall survival compared to chemotherapy in NSCLC patients, regardless of PD-L1 expression levels. Among patients with a PD-L1 expression level of 1% or more, nivolumab plus ipilimumab resulted in a median overall survival of 17.1 months (95% CI, 15.0 to 20.1) compared to 14.9 months (95% CI, 12.7 to 16.7) with chemotherapy (P = 0.007). The 2-year overall survival rates were 40.0% and 32.8%, respectively. The median duration of response was significantly longer with nivolumab plus ipilimumab at 23.2 months compared to 6.2 months with chemotherapy.25 Another study reported that neoadjuvant nivolumab was associated with minimal side effects, did not delay surgery, and induced a major pathological response in 45% of resected tumors. The tumor mutational burden predicted the pathological response to PD-1 blockade, and treatment induced expansion of mutation-associated, neoantigen-specific T-cell clones in peripheral blood.13 Studies that have reported the results of combination of chemotherapy with immunotherapy are summarized in Table 1.
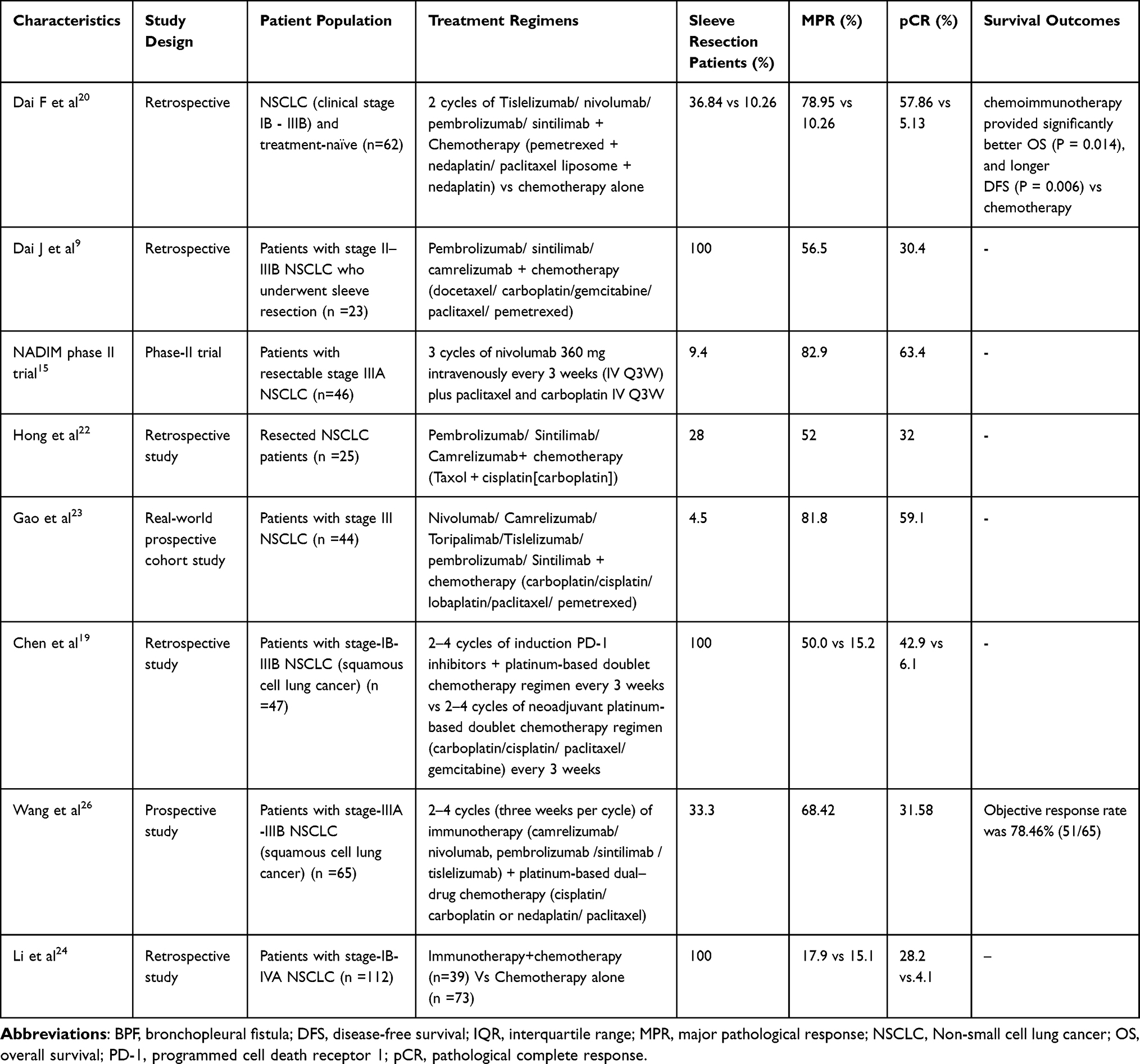 |
Table 1 Summary of Studies of Neoadjuvant Chemoimmunotherapy in Patients with NSCLC |
Safety of Neoadjuvant Chemoimmunotherapy in Patients with Sleeve Resection NSCLC
Studies have shown that chemoimmunotherapy was well tolerated with most adverse events (AEs) being mild to moderate. In a retrospective study by Gao et al, the adverse events observed in patients with NSCLC treated with neoadjuvant chemoimmunotherapy prior to sleeve resection included: grade 3 treatment-related adverse events (18.2% [n=8]), including neutropenia (n = 4), increased aminotransferases (n = 3), anemia (n = 1), and cutaneous capillary endothelial proliferation (n = 1).23 In a study conducted by Dai et al, treatment-related adverse events (TRAE) were observed in 73.9% of patients with NSCLC treated with neoadjuvant chemoimmunotherapy prior to sleeve resection. Observed TRAEs included anemia and neutropenia, with no patients exhibiting serious TRAE.9 In a study conducted by Hong et al after neoadjuvant chemoimmunotherapy (sleeve lobectomy in 52% cases), TRAEs were observed in 52% patients with NSCLC, but none were above grade 3. No death or serious side effects occurred during neoadjuvant therapy.22 In a recent retrospective study, Chen et al, the overall incidence of adverse events in the preoperative setting was comparable between patients who received chemoimmunotherapy vs chemotherapy (42.9% vs 45.5%). The major adverse events reported included myelosuppression (57.1%), skin rash (14.3%), anemia (14.3%), fatigue (4.8%), nausea (4.8%), and serum alanine aminotransferase elevation (4.8%). Furthermore, the majority (66.7%) of the adverse events were of grade 1 or 2.19
In addition to safety and efficacy, evaluating long-term oncological outcomes is crucial for understanding the true benefit of neoadjuvant chemoimmunotherapy in patients undergoing sleeve resection for NSCLC. Current evidence suggests that this approach may lead to improved survival rates and long-term protection against tumor recurrence. For instance, the NADIM phase II trial demonstrated promising results, showing a PFS at 24 months of 77.1% in patients with resectable stage IIIA NSCLC treated with neoadjuvant nivolumab plus chemotherapy.27 Furthermore, Provencio et al reported an OS at 36 months of 81.9% (95% CI, 66.8 to 90.6) in the intention-to-treat population, rising to 91.0% (95% CI, 74.2 to 97.0) in the per-protocol population treated with neoadjuvant chemotherapy plus nivolumab in resectable NSCLC.28 Additionally, a study by Provencio et al indicated that patients achieving a pCR had significantly better long-term survival outcomes compared to those without pCR.29 Despite these encouraging findings, long-term data specifically focusing on sleeve resection patients remain limited. Future studies should aim to provide comprehensive follow-up data, including 5-year survival rates, disease-free survival, and recurrence patterns.
Clinical Factors and Biomarkers Associated with Pathological Response
In a retrospective study conducted by Jiang et al, among the patients with NSCLC (sleeve resection in 22.7% [n=7] of patients) who received neoadjuvant chemoimmunotherapy (n=27)/immunotherapy (n=4), patients with STK11 mutations (were detected in 2 patients [7.7%] through NGS) showed no MPR by final pathological examination.30 In another retrospective study, Dai et al has shown that clinical factors and the immunohistochemistry (IHC) score of other biomarkers involving antitumor immune response were associated with MPR in patients with sleeve resection of NSCLC9 IHC score of the selected biomarkers such as the expression of CD4 (16.5±7.5 vs 22.3±17.3), CD8 (21.6±16.5 vs 30.2±30.5), and CD20 (56.1±36.8 vs 81.5±49.4) were modestly higher in the MPR group, while the expression of PD-1 (14.6±18.7 vs 2.8±2.9), LAG3 (2.0±6.3 vs 0), and TIGIT (6.8±7.9 vs 3.4±3.4) were lower in the MPR group compared to the non-MPR group (p >0.05).9
However, several previous studies have shown that expression of PD-L1 is associated with higher pCR and MPR rates in patients with NSCLC.31,32 Currently, PD-L1 expression levels, tumour mutation burden (TMB) and circulating tumour DNA (ctDNA) among other promising biomarkers are being studied to predict the effect of PD-1/PD-L1 therapies in patients with NSCLC.28,33–35 A previous meta-analysis showed longer overall survival (OS) at ≥1%, ≥5%, ≥10% and ≥50% PD-L1 expression levels in NSCLC on anti-PD-1/PD-L1 monotherapy than chemotherapy.36
Perioperative Outcomes of Sleeve Resection After Neoadjuvant Chemoimmunotherapy
Several studies have demonstrated that sleeve resection after induction of chemoimmunotherapy is safe and feasible. Further, neoadjuvant chemoimmunotherapy was shown to reduce tumor size, cause pathological downstaging, and raise the surgical resection rate of patients with locally advanced NSCLC.9,19,20,22,24 In a retrospective study, Dai et al showed that complete resection was accomplished for all patients who received neoadjuvant chemoimmunotherapy and underwent sleeve resection. Perioperative data were compared between video-assisted thoracoscopic surgery (VATS) (n=8) and thoracotomy (n=15) groups. There were no significant differences in intraoperative blood loss (87.5±51.8 vs 193.9±145.3 mL), operative time (198.8±79.7 vs 225.5±55.0 min), number of lymph nodes examined (16.9±6.6 vs 18.2±6.5), and hospital stay (5.5±2.8 vs 9.2±11.2 days) between the VATS and thoracotomy groups (all P>0.05).9 In a recent retrospective study, Chen et al compared the perioperative data (after sleeve resection) between patients receiving chemoimmunotherapy vs chemotherapy. The chemoimmunotherapy cohort experienced (14.3%) less pulmonary major complications, whereas the chemotherapy cohort experienced more pulmonary and cardiac complications (30.3%) (p = 0.302). Neoadjuvant chemoimmunotherapy did not increase the 30-day risk of postoperative complications.19 In a real-world study, Gao et al demonstrated that R0 resection was achieved in all patients received who neoadjuvant chemoimmunotherapy. Surgical complications occurred in five (11.4%) patients, including air leak (n = 3), chylothorax (n = 2), and surgical site infection (n = 1). There was no re-surgery or postoperative mortality within 90 days.23
In the NADIM phase II study, surgical resection (sleeve resection in 9.4% of patients) following neoadjuvant chemoimmunotherapy showed no operative mortality at either 30 or 90 days in patients with NSCLC. The most common complications observed were prolonged air leak, pneumonia and arrhythmia. R0 resection was achieved in all patients who underwent surgery.15 In a retrospective study, Li et al showed that neoadjuvant chemoimmunotherapy did not increase the incidence of postoperative complications after sleeve lobectomy.24 In a study by Dai F et al, the perioperative outcomes such as operative duration, blood loss, postoperative complications, and hospital stay were comparable between chemoimmunotherapy cohort vs chemotherapy cohort. Furthermore, the authors demonstrated that neoadjuvant chemoimmunotherapy did not increase the risk of delayed surgery.20 Studies that have reported perioperative outcomes in patients with NSCLC after chemotherapy with immunotherapy are summarized in Table 2.
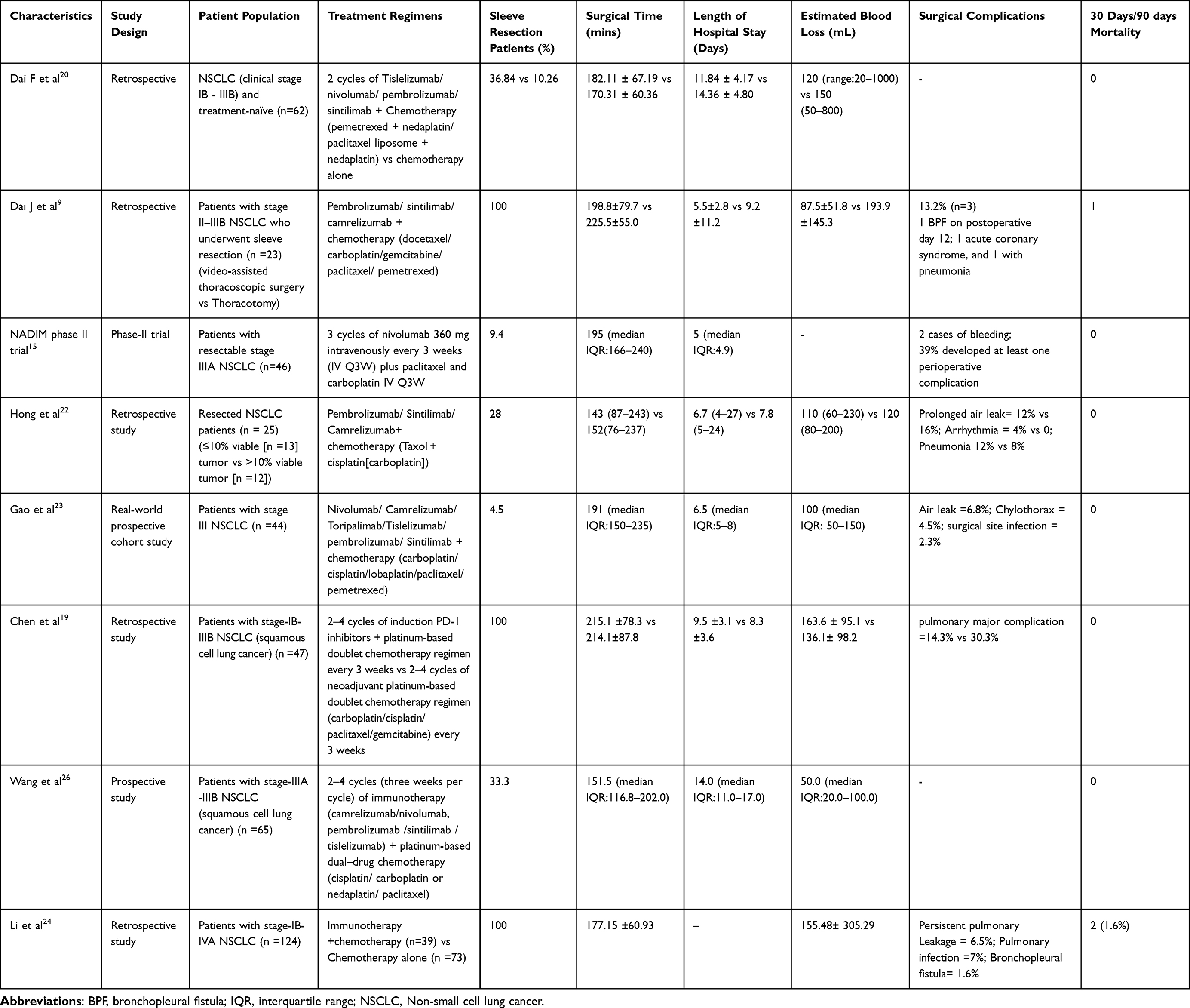 |
Table 2 Perioperative Outcomes in Patients with NSCLC |
It is important to note that studies indicate adhesions are more common following chemoimmunotherapy than after chemotherapy alone. This increased incidence of adhesions, although not significantly affecting the overall complication rate can make surgical dissection more challenging and potentially lengthen the operative time. Addressing these adhesions during surgery requires careful technique and may influence the surgical approach and planning.9,37–40
Despite the promising results observed with neoadjuvant chemoimmunotherapy in patients undergoing sleeve resection, several limitations and knowledge gaps remain. First, most of the existing studies are retrospective and come from a limited number of research groups, which may introduce bias and limit the generalizability of the findings. There is a need for more prospective, multicenter trials to validate these results across diverse populations and clinical settings. Second, the long-term impact of neoadjuvant chemoimmunotherapy on bronchial-vascular healing and postoperative complications in sleeve resection patients is not well understood. Future studies should focus on these specific surgical outcomes to ensure the safety and efficacy of this treatment approach. Third, there is a lack of standardized criteria for assessing pathological responses and perioperative outcomes, making it difficult to compare results across studies. Developing and adopting uniform guidelines would facilitate more consistent and reliable evaluations. Additionally, while some biomarkers have shown promise in predicting responses to chemoimmunotherapy, further research is needed to validate these markers and identify new ones that can help tailor treatments to individual patients. Addressing these limitations and knowledge gaps will be crucial for optimizing the use of neoadjuvant chemoimmunotherapy in sleeve resection patients and improving their clinical outcomes.
Conclusion
Sleeve resection after neoadjuvant chemoimmunotherapy appears to be safe and feasible in patients with NSCLC. Patients receiving neoadjuvant chemoimmunotherapy had higher pCR and MPR rates compared to those receiving chemotherapy alone. These improved response rates are significant as they suggest potential for better long-term survival. Tumor resection rates were higher in patients with neoadjuvant chemoimmunotherapy. Increased pCR and MPR rates are often associated with reduced risk of recurrence and better overall prognosis, indicating that neoadjuvant chemoimmunotherapy may offer substantial survival benefits for patients undergoing sleeve resection. Moreover, higher response rates may enable less invasive surgical approaches. By shrinking tumors more effectively before surgery, neoadjuvant chemoimmunotherapy could facilitate more minimal resections, preserving lung function and reducing perioperative morbidity and mortality. This potential for less invasive surgery can significantly enhance patients’ postoperative quality of life and functional outcomes.
Furthermore, neoadjuvant chemoimmunotherapy did not increase 30- or 90-days mortality rate and risk of postoperative complications. Adverse events with chemoimmunotherapy in patients with NSCLC were tolerable. Overall, neoadjuvant chemoimmunotherapy appears to improve pathological responses in patients with sleeve resection. As very limited studies assessed the efficacy of chemoimmunotherapy in patients with sleeve resection of NSCLC, further large-scale clinical trials or real-world studies are warranted to provide more insights on the clinical safety and efficacy of neoadjuvant chemoimmunotherapy in patients with sleeve resection NSCLC.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chaitanya Thandra K, Barsouk A, Saginala K, Sukumar Aluru J, Barsouk A. Epidemiology of lung cancer. wo. 2021;25(1):45–52. doi:10.5114/wo.2021.103829
2. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chinese Med J. 2022;135(5):584–590. doi:10.1097/CM9.0000000000002108
3. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA a Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
4. Siegel R, DeSantis C, Virgo K, et al. Cancer treatment and survivorship statistics, 2012. Ca a Cancer J Clinicians. 2012;62(4):220–241. doi:10.3322/caac.21149
5. Goldstraw P, Crowley J, Chansky K, et al. The IASLC lung cancer staging project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2(8):706–714. doi:10.1097/JTO.0b013e31812f3c1a
6. Rami-Porta R, Nishimura KK, Giroux DJ, et al. The international association for the study of lung cancer lung cancer staging project: proposals for revision of the TNM stage groups in the forthcoming (ninth) edition of the TNM classification for lung cancer. J Thorac Oncol. 2024;19(7):1007–1027. doi:10.1016/j.jtho.2024.02.011
7. Cusumano G, Marra A, Lococo F, et al. Is sleeve lobectomy comparable in terms of short- and long-term results with pneumonectomy after induction therapy? A multicenter analysis. Ann Thorac Surg. 2014;98(3):975–983. doi:10.1016/j.athoracsur.2014.04.095
8. NSCLC Meta-analysis Collaborative Group.Preoperative chemotherapy for non-small-cell lung cancer: a systematic review and meta-analysis of individual participant data. Lancet. 2014;383(9928):1561–1571. doi:10.1016/S0140-6736(13)62159-5
9. Dai J, Zhu X, Li D, et al. Sleeve resection after neoadjuvant chemoimmunotherapy in the treatment of locally advanced non-small cell lung cancer. Transl Lung Cancer Res. 2022;11(2):188–200. doi:10.21037/tlcr-22-56
10. Koryllos A, Lopez‐Pastorini A, Zalepugas D, et al. Optimal timing of surgery for bronchial sleeve resection after neoadjuvant chemoradiotherapy. J Surg Oncol. 2020;122(2):328–335. doi:10.1002/jso.25945
11. Mukherjee O, Rakshit S, Shanmugam G, Sarkar K. Role of chemotherapeutic drugs in immunomodulation of cancer. Curr Res Immunol. 2023;4:100068. doi:10.1016/j.crimmu.2023.100068
12. Rizzo A, Ricci AD. Biomarkers for breast cancer immunotherapy: PD-L1, TILs, and beyond. Expert Opin Investig Drugs. 2022;31(6):549–555. doi:10.1080/13543784.2022.2008354
13. Forde PM, Chaft JE, Smith KN, et al. Neoadjuvant PD-1 blockade in resectable lung cancer. N Engl J Med. 2018;378(21):1976–1986. doi:10.1056/NEJMoa1716078
14. Gong J, Chehrazi-Raffle A, Reddi S, Salgia R. Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations. J Immunother Cancer. 2018;6(1):8. doi:10.1186/s40425-018-0316-z
15. Román AR, Cruz JL, Macía I, et al. Outcomes of surgical resection after neoadjuvant chemoimmunotherapy in locally advanced stage IIIA non-small-cell lung cancer. Eur J Cardiothorac Surg. 2021;60(1):81–88. doi:10.1093/ejcts/ezab007
16. Zhu XY, Ding C, Xu C, et al. Techniques and outcomes of bronchoplastic and sleeve resection: an 8-year single-center experience. Transl Lung Cancer Res. 2021;10(12):4538–4548. doi:10.21037/tlcr-21-913
17. Ma Z, Dong A, Fan J, Cheng H. Does sleeve lobectomy concomitant with or without pulmonary artery reconstruction (double sleeve) have favorable results for non-small cell lung cancer compared with pneumonectomy? A meta-analysis. Eur J Cardiothorac Surg. 2007;32(1):20–28. doi:10.1016/j.ejcts.2007.03.018
18. Li Z, Chen W, Xia M, et al. Sleeve lobectomy compared with pneumonectomy for operable centrally located non-small cell lung cancer: a meta-analysis. Transl Lung Cancer Res. 2019;8(6):775–786. doi:10.21037/tlcr.2019.10.11
19. Chen T, Ning J, Shen J, et al. Sleeve lobectomy after neoadjuvant chemoimmunotherapy versus chemotherapy for squamous cell lung cancer: a multicenter, retrospective study. JTO Clin Res Rep. 2023;4(4):100472. doi:10.1016/j.jtocrr.2023.100472
20. Dai F, Wu X, Wang X, et al. Neoadjuvant immunotherapy combined with chemotherapy significantly improved patients’ overall survival when compared with neoadjuvant chemotherapy in non-small cell lung cancer: a cohort study. Front Oncol. 2022;12:1022123. doi:10.3389/fonc.2022.1022123
21. Liang W, Cai K, Chen C, et al. Expert consensus on neoadjuvant immunotherapy for non-small cell lung cancer. Transl Lung Cancer Res. 2020;9(6):2696–2715. doi:10.21037/tlcr-2020-63
22. Hong T, Sun T, Zhang M, et al. Surgical perspective in neoadjuvant chemoimmunotherapy for stage
23. Gao Y, Jiang J, Xiao D, et al. Robotic-assisted thoracic surgery following neoadjuvant chemoimmunotherapy in patients with stage III non-small cell lung cancer: a real-world prospective cohort study. Front Oncol. 2022;12:969545. doi:10.3389/fonc.2022.969545
24. Li X, Li Q, Yang F, et al. Neoadjuvant therapy does not increase postoperative morbidity of sleeve lobectomy in locally advanced non–small cell lung cancer. J Thoracic Cardiovasc Surg. 2023;166(4):1234–1244. doi:10.1016/j.jtcvs.2023.03.016
25. Hellmann MD, Paz-Ares L, Bernabe Caro R, et al. Nivolumab plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer. N Engl J Med. 2019;381(21):2020–2031. doi:10.1056/NEJMoa1910231
26. Wang Y, He C, Liu J, et al. The safety and efficacy of preoperative immunotherapy combined with chemotherapy in patients with stage IIIA-IIIB lung squamous cell carcinoma. Thorac Cardiovasc Surg. 2023;71(03):222–230. doi:10.1055/s-0042-1758552
27. Provencio M, Nadal E, Insa A, et al. Neoadjuvant chemotherapy and nivolumab in resectable non-small-cell lung cancer (NADIM): an open-label, multicentre, single-arm, Phase 2 trial. Lancet Oncol. 2020;21(11):1413–1422. doi:10.1016/S1470-2045(20)30453-8
28. Provencio M, Serna-Blasco R, Nadal E, et al. Overall survival and biomarker analysis of neoadjuvant nivolumab plus chemotherapy in operable stage IIIA non–small-cell lung cancer (NADIM phase II trial). JCO. 2022;40(25):2924–2933. doi:10.1200/JCO.21.02660
29. Provencio-Pulla M, Nadal-Alforja E, Cobo M, et al. Neoadjuvant chemo/immunotherapy for the treatment of stages IIIA resectable non-small cell lung cancer (NSCLC): a phase II multicenter exploratory study—NADIM study-SLCG. JCO. 2018;36(15_suppl):8521. doi:10.1200/JCO.2018.36.15_suppl.8521
30. Jiang L, Huang J, Jiang S, et al. The surgical perspective in neoadjuvant immunotherapy for resectable non-small cell lung cancer. Cancer Immunol Immunother. 2021;70(8):2313–2321. doi:10.1007/s00262-021-02847-1
31. Chen Y, Yan B, Xu F, et al. Neoadjuvant chemoimmunotherapy in resectable stage IIIA/IIIB non-small cell lung cancer. Transl Lung Cancer Res. 2021;10(5):2193–2204. doi:10.21037/tlcr-21-329
32. Forde PM, Spicer J, Lu S, et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N Engl J Med. 2022;386(21):1973–1985. doi:10.1056/NEJMoa2202170
33. Zhang F, Guo W, Zhou B, et al. Three-Year Follow-Up of Neoadjuvant Programmed Cell Death Protein-1 Inhibitor (Sintilimab) in NSCLC. J Thorac Oncol. 2022;17(7):909–920. doi:10.1016/j.jtho.2022.04.012
34. Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, Phase 3 trial. Lancet. 2019;393(10183):1819–1830. doi:10.1016/S0140-6736(18)32409-7
35. Samstein RM, Lee CH, Shoushtari AN, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat Genet. 2019;51(2):202–206. doi:10.1038/s41588-018-0312-8
36. Xu Y, Wan B, Chen X, et al. The association of PD-L1 expression with the efficacy of anti-PD-1/PD-L1 immunotherapy and survival of non-small cell lung cancer patients: a meta-analysis of randomized controlled trials. Transl Lung Cancer Res. 2019;8(4):413–428. doi:10.21037/tlcr.2019.08.09
37. Zhang B, Xiao H, Pu X, et al. A real-world comparison between neoadjuvant chemoimmunotherapy and chemotherapy alone for resectable non-small cell lung cancer. Cancer Med. 2023;12(1):274–286. doi:10.1002/cam4.4889
38. Uprety D, Mandrekar SJ, Wigle D, Roden AC, Adjei AA. Neoadjuvant Immunotherapy for NSCLC: current concepts and future approaches. J Thorac Oncol. 2020;15(8):1281–1297. doi:10.1016/j.jtho.2020.05.020
39. Bott MJ, Cools-Lartigue J, Tan KS, et al. Safety and feasibility of lung resection after immunotherapy for metastatic or unresectable tumors. Ann Thorac Surg. 2018;106(1):178–183. doi:10.1016/j.athoracsur.2018.02.030
40. Sepesi B, Zhou N, William WN, et al. Surgical outcomes after neoadjuvant nivolumab or nivolumab with ipilimumab in patients with non-small cell lung cancer. J Thorac Cardiovasc Surg. 2022;164(5):1327–1337. doi:10.1016/j.jtcvs.2022.01.019
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.