")
Back to Journals » International Journal of Nanomedicine » Volume 20
Salivary Extracellular Vesicles in Detection of Head and Neck Cancers: A Systematic Review
Authors Owecki W, Wojtowicz K , Nijakowski K
Received 17 February 2025
Accepted for publication 13 May 2025
Published 26 May 2025 Volume 2025:20 Pages 6757—6775
DOI https://doi.org/10.2147/IJN.S520288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. RDK Misra
Wojciech Owecki,1 Karolina Wojtowicz,2 Kacper Nijakowski3
1Student’s Scientific Group in Department of Conservative Dentistry and Endodontics, Poznan University of Medical Sciences, Poznan, Poland; 2Department of Histology and Embryology, Poznan University of Medical Sciences, Poznan, Poland; 3Department of Conservative Dentistry and Endodontics, Poznan University of Medical Sciences, Poznan, Poland
Correspondence: Kacper Nijakowski, Department of Conservative Dentistry and Endodontics, Poznan University of Medical Sciences, 70 Bukowska Street, Poznan, 60-812, Poland, Email [email protected]
Abstract: Head and neck cancer (HNC) represents approximately 10% of all cancer cases globally, posing a significant public health challenge. Despite advances in therapeutic approaches, the mortality rate associated with HNC continues to rise. A growing body of research highlights the role of extracellular vesicles in cancer progression and pathogenesis, positioning them as promising candidates for novel biomarker discovery. Concurrently, saliva has emerged as a valuable diagnostic fluid due to its non-invasive, accessible, and cost-effective collection methods. This systematic review aims to explore the potential of salivary extracellular vesicles as diagnostic tools for the early detection and monitoring of head and neck cancer. PubMed, Scopus, Web of Science, and Embase were thoroughly searched from database inception to July 16, 2024. Twenty-three eligible studies were included, focusing on original research that described salivary extracellular vesicles as biomarkers in HNC. In oral cancer – predominantly represented by the squamous cell carcinoma subtype – several proteins, including PSB7, AMER3, and LOXL2, as well as a ten-protein panel, demonstrated strong potential as diagnostic biomarkers. Additionally, the analysis of various microRNAs (miR-140, miR-143, miR-145, miR-412-3p, miR-512-3p, miR-1307-5p) and Fourier-transform infrared (FTIR) spectra has shown promising results for oral cancer detection. For oropharyngeal cancer, lactate dehydrogenase B appears to be a promising biomarker. Another potential avenue is the assessment of human papillomavirus (HPV) risk in the development of oropharyngeal cancer. Four studies investigated HNC without specifying the cancer location; however, limited or absent reporting of sensitivity and specificity hampers the reliable evaluation of potential biomarkers. In conclusion, salivary extracellular vesicles hold promise for the detection of HNC, but further research is needed to validate their diagnostic utility.
Keywords: saliva, extracellular vesicles, cancer, biomarkers, diagnosis
Introduction
Head and neck cancer (HNC) constitutes 7.6% of cancer incident cases globally, with the majority classified as head and neck squamous cell carcinoma (HNSCC).1,2 Current treatment strategies for HNC include surgical resection, chemotherapy, immunotherapy, radiation therapy, targeted therapy, or combinations thereof.3 Despite these therapeutic advances, the five-year survival rate ranges from 50% to 85%, depending on tumor location and type.4 Many patients are diagnosed at an advanced stage when prognosis is poor and curative potential is limited.5 This highlights the critical importance of early detection. Effective screening facilitates earlier diagnosis, enabling timely intervention, improving survival rates, and enhancing overall disease management.6,7
The complex nature of HNC, its rapid progression from early to advanced stages, and the anatomical proximity to vital structures underscore the urgent need for reliable, non-invasive biomarkers to aid in early diagnosis, prognosis assessment, and treatment monitoring.8,9 In this context, extracellular vesicles (EVs) have emerged as a promising class of biomarkers with potential applications in cancer screening, prognostication, and real-time disease monitoring.10
EVs are nanoscale, membrane-bound particles secreted by cells into the extracellular environment, playing a critical role in intercellular communication.11–14 This communication is a hallmark of cancer biology, and EVs have been identified as key mediators in this process.15 They transport a variety of biomolecules – including proteins, lipids, RNA, and DNA – which can induce phenotypic changes in recipient cells and modulate the tumor microenvironment. Notably, EVs often carry immunoregulatory molecules that contribute to immune evasion, a hallmark of cancer progression.16 Their selective enrichment with oncogenic cargo enhances their capacity to influence tumor development, recurrence, and therapy resistance.17 EVs have been implicated in multiple stages of cancer progression, including initiation, growth, invasion, and metastasis.18 They also promote angiogenesis, modulate fibroblast activity, alter immune responses, and condition premetastatic niches, all of which are crucial for tumor progression.19 A recent classification system divides EVs into several subtypes: exosomes, microvesicles, supermeres, apoptotic bodies, exomeres, oncosomes, and migrasomes.20
In parallel, saliva has gained increasing attention as a valuable diagnostic fluid due to its rich molecular content and practical advantages.21–23 It contains diverse biomolecules – such as proteins, nucleic acids, inorganic ions, and metabolites – that mirror systemic physiological and pathological conditions.21 Saliva collection is non-invasive, cost-effective, and easy to perform, and the fluid itself is stable and easily accessible.23–26 These features have made it an attractive medium for biomarker discovery across various disease states, including cancers, autoimmune diseases, endocrine disorders, cardiovascular conditions, gastrointestinal diseases, and neurodegenerative disorders.27–32
Given the pivotal role of EVs in cancer pathogenesis and the diagnostic potential of saliva, this systematic review aims to comprehensively evaluate the current evidence on the use of salivary EVs as biomarkers for the detection and monitoring of head and neck cancer. Previous reviews did not present a systematic approach to analyzing the most recent studies from the past five years.33,34 An overview of the concept is schematically illustrated in Figure 1.
 |
Figure 1 Schematic representation of the general design of this systematic review. Included studies described sample collection, isolation of extracellular vesicles, laboratory analysis, and the utility in head and neck cancer detection. Here, in this systematic review, we investigate the potential use of salivary extracellular vesicles in head and neck cancer detection and discuss their utility as cancer biomarkers. |
Materials and Methods
Search Strategy and Data Extraction
Our systematic review was conducted based on the records published to 16th July 2024, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines,35 using the databases PubMed, Scopus, Web of Science and Embase. The search queries included:
- for PubMed: saliva* AND ((extracellular vesicle) OR exosome OR microvesicle OR (apoptotic body OR apoptotic bodies) OR exomere OR migrasome OR oncosome OR supermere) AND (cancer OR carcinoma OR neoplasm OR tumour OR tumor OR oncolog*)
- for Scopus: TITLE-ABS-KEY (saliva* AND (“extracellular vesicle” OR exosome OR microvesicle OR (“apoptotic body” OR “apoptotic bodies”) OR exomere OR migrasome OR oncosome OR supermere) AND (cancer OR carcinoma OR neoplasm OR tumour OR tumor OR oncolog*))
- for Web of Science: TS=(saliva* AND (extracellular vesicle OR exosome OR microvesicle OR apoptotic body OR apoptotic bodies OR exomere OR migrasome OR oncosome OR supermere) AND (cancer OR carcinoma OR neoplasm OR tumour OR tumor OR oncolog*))
- for Embase: saliva* AND (‘extracellular vesicle’ OR exosome OR microvesicle OR ‘apoptotic body’ OR ‘apoptotic bodies’ OR exomere OR migrasome OR oncosome OR supermere) AND (cancer OR carcinoma OR neoplasm OR tumour OR tumor OR oncolog*).
Records were screened by the title, abstract and full text by two independent investigators. Studies included in this review matched all the predefined criteria according to PECOS (“Population”, “Exposure”, “Comparison”, “Outcomes” and “Study design”), as presented in Table 1. Studies regarding cancers other than head and neck were systematically reviewed in another paper.36 A detailed search flowchart is shown in the Section “Results”. The study protocol was registered in International prospective register of systematic reviews PROSPERO (CRD42024573878).
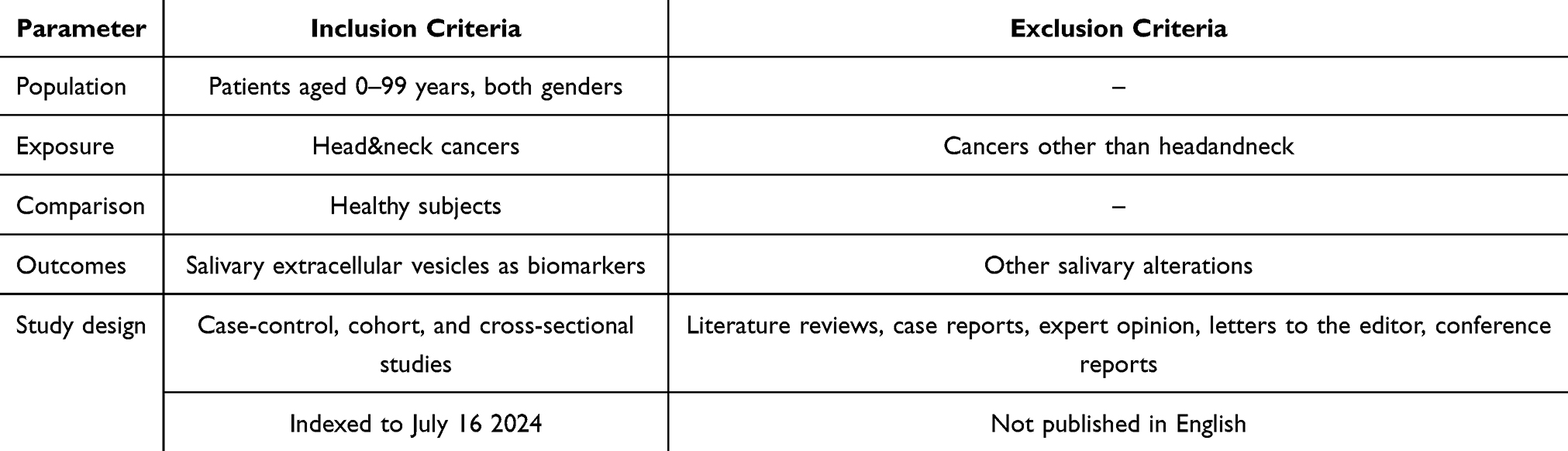 |
Table 1 Inclusion and Exclusion Criteria According to the PECOS |
Quality Assessment of Included Studies
The risk of bias in each individual study was assessed according to the “Study Quality Assessment Tool” issued by the National Heart, Lung, and Blood Institute within the National Institute of Health.37 These questionnaires were answered by two independent investigators, and any disagreements were resolved by discussion between them.
Results
General Information
Following the search criteria presented above, our systematic review included twenty-three studies. The detailed selection strategy for the retrieved records is shown in Figure 2. Table 2 presents data on each eligible study included in this systematic review, including the year of publication, study setting and participants, cancer diagnosis, inclusion and exclusion criteria, TNM staging, and detailed characteristics related to saliva types, sampling methods, centrifugation, storage, and analysis. It also includes potential salivary EV biomarkers for head and neck cancer detection. All studies were published between 2011 and 2024.
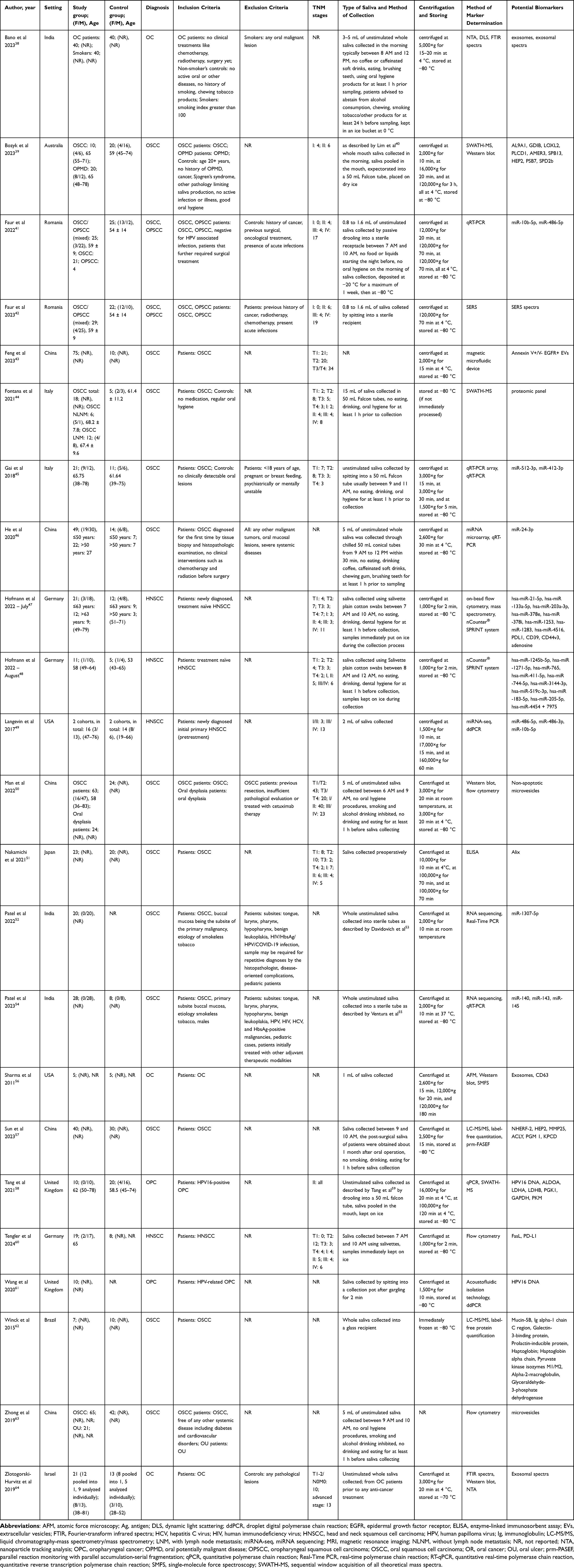 |
Table 2 Characteristics of Included Studies |
 |
Figure 2 PRISMA flow diagram presenting search strategy. |
Participants, Cancer Diagnosis, and TNM Staging
In total, the eligible studies recruited 626 patients diagnosed with head and neck cancers. The included studies investigated oral cancer, oropharyngeal cancer, and head and neck cancer without precise tumor localization. Predominantly, squamous cell carcinomas were analyzed (540 patients, 86.26%). Most cancer patients included in this systematic review were diagnosed with oral cancer (485 patients, 77.48%). Additionally, two studies included a combined total of 54 patients with either oral or oropharyngeal cancer without specific selection.
Data were collected across 11 different countries. The majority of studies were conducted in Asia (nine studies) and Europe (nine studies). TNM staging or tumor stage information was reported in fourteen studies. Advanced cancer stages (III and IV) were slightly more common than early stages (I and II), with 131 (53.69%) and 113 (46.31%) patients, respectively. Conversely, when evaluating tumor stage numerically, lower stages were more prevalent than higher stages (156 and 94 patients, 62.40% and 37.60%, respectively). One study applied a two-level staging classification, in which the advanced stage was predominant.64
Inclusion and Exclusion Criteria
In some studies, the inclusion and exclusion criteria were clearly defined; however, these criteria varied across studies. Several authors excluded participants with systemic diseases such as diabetes, cardiovascular disorders, or infections. The detailed inclusion and exclusion criteria are presented in Table 2.
Saliva Collection, Laboratory Methods
In all included studies, authors collected unstimulated saliva, or stimulation was not reported. When reported, the volume of collected samples ranged from 0.8 mL to 15 mL. In most cases, saliva collection took place in the morning hours (between 6:00 AM and 12:00 noon). Initial centrifugation was typically performed at forces ranging from 1,000×g to 3,000×g, followed by ultracentrifugation. Most samples were stored at −80 °C. A wide range of methods was employed for biomarker identification, with PCR-based techniques being the most common (used in eight studies), followed by mass spectrometry (used in six studies).
Quality Assessment
Figure 3 reports the summarized quality assessment, according to the “Study Quality Assessment Tool” issued by the National Heart, Lung, and Blood Institute within the National Institute of Health.37 The most frequently identified risks of bias were the lack of information on blinding and randomization (reported in all studies), as well as the absence of sample size justification (noted in twenty-one studies). Critical appraisal was conducted by assigning points to each criterion of potential bias (1 point for low risk, 0.5 for unclear risk, and 0 for high risk). Based on the total scores, four studies (17.4%) were classified as having “good” quality (≥80% of the total score), while nineteen studies (82.6%) were considered to have “intermediate” quality (≥60% of the total score).
 |
Figure 3 Quality assessment, including the main potential risk of bias (risk level: green – low, yellow – unspecified, and red – high; quality score: green – good, yellow – intermediate, and red – poor). |
All included studies were classified as level III or IV evidence (case-control studies) according to the five-level scale of the Oxford Centre for Evidence-Based Medicine for diagnostic studies.65
Discussion
Oral Cancer
Oral cancer is considered one of the most prevalent cancers within the head and neck.66 It constitutes a significant public health problem with increasing morbidity among young patients. Poor public awareness hinders early diagnosis, contributing to a high mortality rate.67 Importantly, this cancer is considered preventable since most of the risk factors, including betel nut chewing, alcohol consumption, and tobacco use, can be avoided.68 The term oral cancer generally comprises neoplasms located in the inner lip, hard and soft palate, dorsal surface of the tongue, gums, buccal mucosa, and floor of the mouth.69 Approximately 90% of oral malignancies constitute oral squamous cell carcinoma (OSCC).70 OSCC in its early stage is usually painless, but as the lesions progress, nodularity, ulceration, or tissue attachment may appear, leading to discomfort.71 Oral potentially malignant disorders (OPMDs), which include oral leukoplakia and erythroplakia, oral submucous fibrosis, proliferative verrucous leukoplakia, and oral lichen planus/lichenoid lesions, predispose to the development of OSCC.72,73 The primary method of OSCC treatment is surgical resection assisted with chemo- or radiotherapy, if needed. Other treatment options include immunotherapy, immune checkpoint inhibitors, monoclonal antibodies, photodynamic therapy, or cyclooxygenase-2 inhibitors.74
On the other hand, OSCC diagnosis is established with the help of visual examination, biopsy, toluidine blue or Lugol iodine staining, oral brush biopsy, light-based detection system, cell-free DNA biomarkers, radiological imaging, and saliva-based biomarkers.74,75 Saliva contains various compounds that may serve as potential biomarkers, including DNA and RNA molecules, cytokines, circulating or tissue-derived cells, and EVs.76 Evidence shows that EVs play a pivotal role in oral cancer pathology, regulating tumorigenesis by transferring proteins and microRNAs (miRNAs), modulating the immune system, and contributing to lymphangiogenesis. Moreover, EVs impact natural killer cells, tumor-associated macrophages, and drug resistance during oral cancer treatment.77
In a study by Bozyk et al,39 eight proteins (AL9A1, GDIB, LOXL2, PLCD1, AMER3, SPB13, HEP2, SPD2b) were significantly more abundant in salivary exosomes of OSCC patients compared to controls. These proteins were mostly linked with cancer development, participating in processes like protein homeostasis, cell migration and invasion or Wnt signaling. Further investigation using Western blot confirmed a decreased abundance of LOXL2, AMER3, ALD9A1, and PSB7 in controls compared to both patient groups. A combined panel of PSB7, AMER3, and LOXL2 provided the best results in discriminating between healthy participants and OSCC patients (AUC 0.96, specificity 100%, sensitivity 75%), indicating its potential in the OSCC diagnosis.
Another research focused on miRNAs. MiR‐10b‐5p tended to be downregulated, while miR‐486‐5p upregulated in the oral and oropharyngeal SCC patients group compared to healthy controls; however, without statistical significance. Interestingly, miR‐10b‐5p expression was decreased in stage IV and increased in stage II and III, while miR‐486‐5p was elevated in stage II compared with stage III and IV. Concomitantly, miR-486-5p expression was upregulated in grade 1 (G1) SCC compared to G3 SCC, whereas miR-10b-5p was decreased in G2 and increased in G1 and G3. In non-keratinizing SCC tumors, miR-486-5p was upregulated, and miR-10b-5p was downregulated. None of these observations was statistically significant; the AUC of these miRNAs varied between 0.50 to 0.89 in detecting oral or oropharyngeal cancer (0.72 and 0.59 for combined malignancies), limiting their potential use in cancer diagnosis.41
An interesting method was employed by Faur et al.42 Similarly to the previous study, patients with oropharyngeal SCC and OSCC were grouped together. The authors investigated the surface-enhanced Raman spectra (SERS) of salivary exosomes. The analysis revealed significant differences between the mean intensities of cancer and control groups, especially in the 1740–2540 cm−1 range and other sparse values (350, 700, 960, 1170, 1320, 1500 cm−1, and others). The ROC analysis of salivary exosomes SERS spectra in cancer discrimination exhibited satisfactory values of AUC for the 2000–2200 cm−1 range but worse for a full range of spectra (AUC 0.751 and 0.654, respectively).
Another approach utilized a magnetic microfluidic device to investigate salivary Annexin V− EGFR+ EV and Annexin V+ EGFR+ EV subpopulations. The EGFR (epidermal growth factor receptor) is a cell-surface protein that participates in migration, proliferation, DNA synthesis, and adhesion. Additionally, EGFR overexpression is associated with increased metastatic potential and poor prognosis in oral cancer.78 The level of total EGFR+ EVs was significantly increased in OSCC patients compared to controls. Moreover, the level of Annexin V+ EGFR+ EVs was significantly elevated in patients with stage T3 and T4 OSCC compared to T1 and T2 stages of OSCC. Furthermore, the ratio of Annexin V+ EGFR+ EVs to Annexin V− EGFR+ EVs decreased with the ascending tumor volume. These results indicate that Annexin V+/V− EGFR+ EVs may be considered as potential tools in OSCC detection and disease monitoring.43
Similarly, another study revealed that in non-apoptotic salivary microvesicles with Annexin V−, AXL protein and EGFR were significantly upregulated compared with apoptotic salivary microvesicles with Annexin V.+50 In parallel to EGFR, AXL is involved in several signal transduction cascades and biological processes including cell survival, proliferation, migration, angiogenesis, platelet aggregation and fibrosis.79 The levels of non-apoptotic salivary microvesicles were significantly decreased in healthy individuals and OSCC patients with T1 to T2 stages with respect to OSCC patients with T3 to T4 stages. Notably, comparing a smaller sample of healthy controls and OSCC patients, there was a significantly upregulated ratio of Annexin V−/EGFR+ microvesicles in the latter group. This ratio was also significantly linked with tumor T stage, indicating the potential use of non-apoptotic salivary microvesicles in the detection and prognosis of OSCC.50
A considerable panel of potential OSCC biomarkers was proposed in a proteomic study investigating salivary EVs. Among cancer patients, twelve had lymph node metastasis (LNM), while six did not have (NLNM). The authors found 235 significantly differentially modulated proteins in the comparison of controls and NLNM patients (91 down-represented and 144 up-represented proteins), 157 in the comparison of controls and LNM patients (89 down-represented and 68 up-represented proteins), and 189 in the comparison of NLNM and LNM patients (119 down-represented and 70 up-represented proteins). Proteins found in samples of cancer patients were associated with antimicrobial properties, acute inflammatory response, regulation of blood coagulation, and plasma lipoprotein particle remodeling.44
On the other hand, Gai et al45 investigated salivary EVs miRNAs and revealed eleven significantly deregulated miRNAs in the comparison of OSCC and control groups (upregulated: miR-412-3p, miR-489-3p, miR-512-3p, miR-597-5p, miR-603; downregulated: miR-30e3p, miR-193b-3p, miR-376c-3p, miR-484, miR-720, miR-93-3p). Further analysis of chosen miRNAs confirmed exclusive detection of miR-302b-3p and miR-517b-3p only in the OSCC group and significant upregulation of miR-512-3p and miR-412-3p in patients compared to controls. The latter finding was evaluated with ROC analysis, which exhibited satisfactory results for both miRNAs (AUC 0.847 and 0.871, miR-512-3p and miR-412-3p, respectively). Additionally, investigation of these miRNAs suggested their probable involvement in various pathways activated in OSCC (TGF-β, ErbB signaling, signaling regulating pluripotency of stem cells, proteoglycans- or lysine-associated pathways), which, combined with satisfactory performance, increases their potential in OSCC diagnosis.
A similar approach revealed that in comparison with healthy individuals, 109 exosomal miRNAs were significantly altered in OSCC patients (50 upregulated, 59 downregulated). For further investigation, only miR-24-3p was selected.46 This miRNA is implicated in cancer pathogenesis since it induces cell proliferation and regulates chemosensitivity.80 In OSCC patients, the salivary exosomal miR-24-3p level was significantly higher than in controls. The diagnostic power of this miRNA in distinguishing between OSCC patients and healthy individuals was relatively satisfactory (AUC 0.738), which suggests its potential in OSCC detection.46
Nakamichi et al51 analyzed salivary exosomal Alix (programmed cell death 6-interacting protein) among 23 OSCC patients and 20 healthy donors. The salivary exosomal Alix levels were significantly elevated in patients compared to controls. No OSCC stage-dependent pattern was observed. The performance of salivary exosomal Alix in the detection of OSCC reached fair AUC (0.712) and excellent specificity (100%) but low sensitivity (34.8%). This research shows salivary exosomal Alix as a poor biomarker for early OSCC detection but good for diagnostic confirmation.
Another research investigated OSCC salivary exosomes and revealed three significantly expressed miRNAs, unique for salivary exosomes of OSCC patients. One of them, miR-1307-5p, was significantly upregulated in salivary exosomes and tissue samples of OSCC patients compared to healthy controls. Moreover, the predictive power of this miRNA was determined with ROC analysis, reaching excellent results (AUC 0.99). Interestingly, salivary exosomal miR-1307-5p levels were significantly elevated in chemoresistant patients, patients with high-grade tumors and LNM (compared to patients with complete remission, patients with low-grade tumors and NLNM, respectively). Concomitantly, evidence shows that miR-1307-5p is implicated in cancer pathogenesis by modulating cell apoptosis, proliferation, maintenance of cancer stem cells, and angiogenesis. These findings implicate salivary exosomal miR-1307-5p as a potential biomarker for OSCC diagnosis, prognosis, and monitoring.52
A similar approach was presented by Patel et al;54 seven miRNAs (let-7i, miR-21, miR-30a, miR-140, miR-143, miR-145, miR-423) had significantly differential expression in both salivary exosomes and tissue of OSCC patients with respect to controls. ROC analysis indicated that a combination of salivary exosomal miR-140, miR-143, and miR-145 provides excellent results in detecting OSCC patients (AUC 0.99). Moreover, the authors observed a significant downregulation of salivary exosomal miR-140 and miR-143 in advanced cancer-stage patients. An integrated network analysis revealed that these miRNAs may modulate sixteen potential hub genes, known as driver candidates responsible for the initiation and progression of oral cancer. Collectively, these findings suggest the potential utility of this 3-miRNA panel in OSCC detection, monitoring, and prognosis.
On the other hand, a proteomic study provided potential biomarker candidates for OSCC surgical treatment monitoring. The results revealed 132 upregulated phosphoproteins and 315 upregulated proteins in OSCC patients, respectively, among more than 1000 EV phosphoproteins and 2500 EV proteins. Additionally, ten proteins showed distinctive changes between pre- and post-surgical samples, and a ten-protein panel exhibited excellent results in distinguishing between these samples (ROC analysis AUC 0.90). Among them, six proteins (3 full proteins: NHERF-2, HEP2, MMP25, and 3 phosphoproteins: ACLY, PGM 1, KPCD) were sensitive to surgical status in at least 80%, with HEP2 being the most sensitive.57
Another proteomic study identified eight EV proteins with differential expression levels between OSCC and healthy control groups (Mucin-5B, Ig alpha-1 chain C region, Galectin-3-binding protein, Prolactin-inducible protein, Haptoglobin; Haptoglobin alpha chain, Pyruvate kinase isozymes M1/M2, Alpha-2-macroglobulin, Glyceraldehyde-3-phosphate dehydrogenase). Concomitantly, four and eighteen proteins were detected exclusively in OSCC and control samples, respectively. Interestingly, proteins found in OSCC patients were associated with cellular growth, proliferation and molecular transport, mainly comprising metals. This finding indicates their role in the tumor microenvironment and opens up possibilities for further research.62
Finally, Zhong et al63 presented promising results of salivary microvesicles in OSCC detection and prognosis. The level of salivary microvesicles was significantly elevated in the OSCC group compared to patients with oral ulcer (OU) and controls. Moreover, OSCC LNM patients or patients with higher cancer stages (III and IV) had significantly increased levels of salivary microvesicles with respect to NLNM patients or those with lower cancer stages (I and II), respectively. Furthermore, salivary microvesicle levels significantly correlated with vascular endothelial growth factor C (VEGF‐C) expression in OSCC patients. Importantly, VEGF-C, a pro‐lymphangiogenic growth factor, contributes to cancer development by promoting metastasis. Interestingly, the authors observed equal proportions of apoptotic and non‐apoptotic salivary microvesicles in all groups. Nevertheless, the percentage of apoptotic microvesicles was significantly elevated in OSCC patients with lower pathological grades (I and II) with respect to those with a higher grade (III). Concomitantly, the ratio of apoptotic to non-apoptotic microvesicles significantly and negatively correlated with pathological grade. Additionally, a higher ratio of apoptotic to non-apoptotic microvesicles significantly predicted a better survival rate among OSCC patients.
Three studies investigated oral cancer without a precise specification of the histological type. Bano et al38 analyzed salivary exosomes among three groups: oral cancer patients, healthy smokers, and non-smoking controls. Nanoparticle size was significantly larger in the cancer group compared to the remaining participants when measured by dynamic light scattering, but the differences disappeared in nanoparticle tracking analysis. Interestingly, controls demonstrated a significantly lower proportion of standard-sized exosomes compared to cancer patients. Salivary exosomes exhibited the highest exosomal concentrations in oral cancer patients, while smokers showed elevated particle concentrations compared to non-smoking controls. Concomitantly, a Fourier‑transform infrared (FTIR) spectroscopy investigation revealed that the intensity ratios of I1156/I2922, I1645/I1079, I1645/I2958, I1315/I2922, I1645/I1315 (all in cm−1) were the highest in oral cancer patients (with a significant difference) followed by smokers and controls. Moreover, FTIR peaks at 1156 cm−1 and 1079 cm−1, accredited to the carbohydrate part and the symmetric vibrations of the PO4 group of nucleic acids, presented an analogical pattern, with cancer patients having the highest peak levels. These findings provide insights into the properties of salivary exosomes in distinguishing between oral cancer patients, high-risk smokers, and healthy controls, suggesting their potential role in biomarker development.
Similarly, Sharma et al56 noticed a significantly increased size of exosomes in oral cancer patients compared to non-cancer controls. The authors observed a two to four-fold increase in the density of exosomes in the cancer group with respect to healthy donors. Interestingly, in several oral cancer samples, exosomes were enclosed by multi-vesicular bodies. Additionally, cancer exosomes exhibited a significantly higher density of surface CD63 molecules.
A study by Zlotogorski-Hurvitz et al64 showed considerably larger diameters of salivary exosomes in the oral cancer group compared to controls. Moreover, CD9, CD63, CD81 molecules were more prominent in the cancer samples. FTIR attenuated total reflection spectra revealed that oral cancer samples consistently differed from non-cancer controls at 1072 cm−1 (nucleic acids), 1543 cm−1 (transmembrane proteins), 2854 cm−1, and 2924 cm−1 (membranous lipids). In addition, the intensity ratios of I1033/I1072, I1404/I2924, and I2924/I2854 (all in cm−1) were significantly higher in patients compared to healthy individuals. Two classification models based on the ratios of I1037/2924, I2854/2874 (all in cm−1), spectra absorbance bands in the 900 cm−1–3700 cm−1, and the area under the absorbance spectrum from 950–1500 cm−1, 1720–1760 cm,−1 and 2820–3000 cm−1 provided excellent results (sensitivity 100%, specificity 89%, accuracy 89–100%). These findings suggest a potential use of FTIR spectra in oral cancer detection. In contrast, differences in exosome size, as suggested in this study and in a few studies regarding oral cancer,38,56,64 are opposed by other OSCC studies that describe no significant differences in exosome size.39,52
Oropharyngeal Cancer
Oropharyngeal cancer (OPC) refers to malignancies found in the lateral and posterior pharyngeal walls, the tonsils, the soft palate, and the posterior one-third and base of the tongue. The prevalence of OPC is associated with its risk factors, which include tobacco smoking, HPV, alcohol consumption, and areca nut chewing.81 Oropharyngeal squamous cell carcinoma (OPSCC) occurs in approximately 90% of cases.82 On the other hand, HPV-positive OPC constitutes one-fourth of all cancers related to the head and neck.83 Usually, HPV-positive OPC is associated with younger patients with better prognosis; nevertheless, significant disabilities linked to cancer treatment in advanced stages underscore the need for early detection of this cancer.84 One of the potential biomarkers for OPC detection might be EVs, which are secreted by tumor cells and contain particles present in these cells.85
Two studies regarding OPSCC have already been described above.41,42 Two other papers refer to OPC without stating its squamous type. One of them, comprising HPV-positive OPC patients, revealed that in salivary exosomes, HPV16 E6/7 DNA was detected in 80% of cancer samples and in none of the healthy controls. Moreover, 36 proteins in salivary exosomes were differentially expressed between groups (18 upregulated and 18 downregulated). Interestingly, six main glycolytic enzymes were significantly upregulated in salivary exosomes of OPC patients. These enzymes included Aldolase 19 (ALDOA), Lactate dehydrogenase A/B 20 (LDHA; LDHB), Phosphoglycerate kinase 1 (PGK1), Glyceraldehyde-3-phosphate dehydrogenase (GAPDH), and Pyruvate kinase M1/2 (PKM). The ROC analysis indicated that the best results in discriminating healthy and HPV-OPC patients reached LDHB (AUC 0.93), while the rest of the enzymes exhibited relatively satisfactory performance (AUC 0.785–0.73).58 Interestingly, evidence indicates that LDH might be involved in cancer pathways, since LDH may reflect the level of hypoxia in cancer cells predicting patients’ prognosis.86
Wang et al61 recruited 10 hPV-positive OPC patients to detect HPV16 in various salivary EVs. The majority (92%) of HPV16 signals were located in exosome fraction, approximately twelve times higher than in microvesicles. Using acoustofluidic isolation technology with droplet digital PCR assay, the authors detected HPV16 in 80% of HPV-positive OPC patients, which suggests that this method may evaluate HPV16 risk of developing OPC.
Head and Neck Cancer
Four other studies discussed head and neck cancers without exact specification of one localization of the tumor. In 2022, Hofmann et al47 suggested various possibilities for the potential detection of HNSCC. A significantly higher relative fluorescent intensity was observed for PD-L1, CD39, and CD44v3 in the salivary exosomes of the cancer group compared to controls. Moreover, there was a significantly elevated production of immune suppressive adenosine in salivary exosomes of HNSCC patients. Additionally, the analysis revealed eight miRNAs (hsa-miR-21-5p, hsa-miR-133a-5p, hsa-miR-203a-3p, hsa-miR-378e, hsa-miR-378i, hsa-miR-1253, hsa-miR-1283, hsa-miR-4516) with significantly lower expression ratios in the cancer group, with hsa-miR-133a-5p having the highest significance.
Another study presented an intra-correlation analysis of co-expressed salivary exosomal miRNAs in HNSCC, which revealed the strongest correlation for hsa-miR-765, hsa-miR-1245b-5p, and hsa-miR-1271-5p. Hsa-miR-519c-3p provided the best results as a prognostic indicator of disease-free survival. Interestingly, the comparison of HPV-negative and HPV-positive HNSCC showed that hsa-miR-183-5p, hsa-miR-205-5p, and hsa-miR-4454 + 7975 exhibited significantly increased levels in the latter group. Concomitantly, three miRNAs (hsa-miR-411-5p, hsa-miR-744-5p, hsa-miR-3144-3p) were significantly upregulated in patients with a higher stage of HNSCC compared to those with lower stage, suggesting the diagnostic potential of miRNAs in HNSCC detection and prognosis.48
Both studies mentioned above determined molecular functions of investigated miRNAs in the context of HNSCC development. These functions included cell-to-cell signaling involving RAS/MAPK, NF-κB complex, Smad2/3, and IFN-α pathways, cellular assembly, development, growth, proliferation, organization, maintenance, function, and cellular response to therapeutics, as well as DNA replication.47,48
Similarly, Langevin et al49 analyzed miRNAs in two cohorts of participants. In the initial testing, either salivary exosomal miR-486-5p or miR-486-3p combined with miR-10b-5p enabled discrimination of 80% of HNSCC patients from controls. In the validation stage, miR-10b-5p and miR-486-5p enabled discrimination of patients and controls with a sensitivity of 18% and 45% and specificity of 100% and 89%, respectively. Importantly, miR-486-5p could identify patients with the early stage of HNSCC. Nevertheless, low sensitivity questions the utility of these miRNAs in HNSCC detection.
A recent research showed that salivary exosomal PD-L1, FasL, and TGF-β had elevated levels in the HNSCC group compared to controls. Furthermore, levels of these three molecules were more pronounced in patients with HPV-negative than HPV-positive HNSCC and with advanced than early stages of HNSCC. However, tetraspanin positive analysis reached a significance level only for FasL and PD-L1 (regarding the level between cancer/non-cancer and HPV positive/negative, respectively), indicating these two immunomodulatory proteins as potential candidates for HNSCC diagnosis.60,87 Interestingly, both FasL and PD-L1 are involved in HNSCC pathology, contributing to patients’ prognosis and survival.88,89 Additionally, the average median count of tetraspanin-positive CTLA-4+ particles doubled in the HNSCC group compared to controls, but there was no difference with regard to HPV-related HNSCC.60
Study Limitations
There are some limitations in this paper. The included studies are heterogeneous in terms of the types of salivary EVs investigated, diagnosis of various cancers, and inclusion or exclusion criteria for participants. In most cases, eligible studies investigated diverse potential biomarkers, which hindered comparing their utility. Additionally, only some papers included the results of ROC analysis to assess the diagnostic power of potential salivary biomarkers in HNC detection. The risk of bias was increased due to limited data regarding blinding, randomization and sample size justification. The eligible studies also underscore the absence of standardized methods for EVs isolation or quantification, limiting the reproducibility of utilizing salivary EVs in cancer diagnostics. Indeed, the selection of a particular isolation technique may influence the composition of purified EVs subpopulations, contributing to different results. Furthermore, difficulties encountered in the laboratory processes during EVs isolation and analysis, limited number of participants, diminishing statistical power, as well as heterogeneity among EVs subpopulations are other limitations mentioned in the included studies.
Existing Limitations in Using EVs
Medicine requires non-invasive methods for early cancer detection, based on more appropriate and specific biomarkers. Therefore, the collection of EVs is of great importance. Clinical validation of EVs-based diagnostic tests is essential, as it will pave the way for new diagnostic techniques in medicine. Unfortunately, these techniques still face several limitations.
Firstly, there is a need to develop standardized procedures to ensure a high-quality input material and inter-batch comparability during the sample acquisition process.91 Secondly, the isolation of EVs remains a significant challenge, primarily due to low efficiency. Current isolation procedures include ultracentrifugation, ultrafiltration, size-exclusion chromatography, polyethylene glycol (PEG)-based precipitation, microfluidics-based techniques, and various commercially available EVs isolation kits.90–92 The choice of an appropriate isolation method should always be adjusted to the type of material collected, taking into account its source. In some cases, a combination of different methods is necessary.93
Each method has its advantages and disadvantages. For example, ultrafiltration is relatively expensive and can damage EVs, but the isolation procedure itself is extremely simple.90,94 The size-exclusion chromatography method is more cost-effective and gentler on EVs.92 Density gradient centrifugation facilitates the separation process and yields clean samples, but its long duration and requirement for specialized equipment limit its broader application.94
EVs can be characterized by specific receptors on their membrane. However, the latest research shows that they are often only weakly enriched in membrane receptors, and their specificity may vary depending on the composition of the biofluid from which they are isolated.90 One promising isolation approach involves using magnetic beads for EVs analysis.94 For instance, immunoaffinity capture techniques isolate exosomes by recognition of surface proteins such as CD81, CD63, and CD9. These types of extraction methods are commonly used for isolating EVs from saliva.91
Storage of EVs for future analysis presents another challenge. Their stability is driven by several factors, including temperature. For example, EVs remain stable at 4°C for up to one week. Storage in liquid nitrogen results in long-term preservation of EVs concentration. Additionally, it is also crucial to minimize freeze-thaw cycles during transportation and storage to maintain sample integrity.94
Despite growing knowledge about EVs, their analysis remains challenging. Further research, including clinical studies, is needed to improve laboratory techniques. Fundamental aspects still require clarification - for example, forcing large-scale EVs production from cell lines, transitioning from 2D to 3D cell cultures, developing standardized isolation protocols, ensuring purity and quality control, among others. Moreover, the clinical usefulness of novel biomarkers must be confirmed through comprehensive validation studies.90
Conclusions
Early detection plays a pivotal role in the management of head and neck cancers. This systematic review highlights the potential of salivary extracellular vesicles as promising biomarkers for the diagnosis of these cancers. Notably, several studies reported excellent diagnostic performance in distinguishing cancer patients from healthy individuals. In addition to cancer detection, some EV-based biomarkers have also been proposed for monitoring disease progression and predicting prognosis. However, further research involving larger and more diverse populations is necessary to fully evaluate their clinical utility in head and neck cancer detection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mastronikolis NS, Delides A, Kyrodimos E, et al. Insights into metastatic roadmap of head and neck cancer squamous cell carcinoma based on clinical, histopathological and molecular profiles. Mol Biol Rep. 2024;51(1):597. doi:10.1007/s11033-024-09476-8
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Hu C, Liu M, Li Y, et al. Recent advances and future perspectives of CAR-T cell therapy in head and neck cancer. Front Immunol. 2023;14:1213716. doi:10.3389/fimmu.2023.1213716
4. Eberly HW, Sciscent BY, Lorenz FJ, Rettig EM, Goyal N. Current and emerging diagnostic, prognostic, and predictive biomarkers in head and neck cancer. Biomedicines. 2024;12(2):415. doi:10.3390/biomedicines12020415
5. Hristova VA, Chan DW. Cancer biomarker discovery and translation: proteomics and beyond. Expert Rev Proteomics. 2019;16(2):93–103. doi:10.1080/14789450.2019.1559062
6. Schiffman JD, Fisher PG, Gibbs P. Early detection of cancer: past, present, and future. Am Soc Clin Oncol Educ Book. 2015;(35):57–65. doi:10.14694/EdBook_AM.2015.35.57
7. Mali SB. Molecular screening of head neck cancer. Oral Oncol. 2023;144:106481. doi:10.1016/j.oraloncology.2023.106481
8. Marakala V. Head and neck cancer biomarkers: systematic review and meta-analysis. Clin Chim Acta. 2023;542:117280. doi:10.1016/j.cca.2023.117280
9. Thomaidou AC, Batsaki P, Adamaki M, et al. Promising biomarkers in head and neck cancer: the most clinically important miRNAs. Int J Mol Sci. 2022;23(15):8257. doi:10.3390/ijms23158257
10. Xie C, Ji N, Tang Z, Li J, Chen Q. The role of extracellular vesicles from different origin in the microenvironment of head and neck cancers. Mol Cancer. 2019;18(1):83. doi:10.1186/s12943-019-0985-3
11. Urabe F, Kosaka N, Ito K, Kimura T, Egawa S, Ochiya T. Extracellular vesicles as biomarkers and therapeutic targets for cancer. Am J Physiol Cell Physiol. 2020;318(1):C29–C39. doi:10.1152/ajpcell.00280.2019
12. Abels ER, Breakefield XO. Introduction to extracellular vesicles: biogenesis, RNA cargo selection, content, release, and uptake. Cell Mol Neurobiol. 2016;36(3):301–312. doi:10.1007/s10571-016-0366-z
13. van Niel G, D’Angelo G, Raposo G. Shedding light on the cell biology of extracellular vesicles. Nat Rev Mol Cell Biol. 2018;19(4):213–228. doi:10.1038/nrm.2017.125
14. Gupta D, Zickler AM, El Andaloussi S. Dosing extracellular vesicles. Adv Drug Deliv Rev. 2021;178:113961. doi:10.1016/j.addr.2021.113961
15. Kalluri R, McAndrews KM. The role of extracellular vesicles in cancer. Cell. 2023;186(8):1610–1626. doi:10.1016/j.cell.2023.03.010
16. Wu Q, Zhang H, Sun S, Wang L, Sun S. Extracellular vesicles and immunogenic stress in cancer. Cell Death Dis. 2021;12(10):894. doi:10.1038/s41419-021-04171-z
17. Tai YL, Chu PY, Lee BH, et al. Basics and applications of tumor-derived extracellular vesicles. J Biomed Sci. 2019;26(1):35. doi:10.1186/s12929-019-0533-x
18. Abhange K, Makler A, Wen Y, et al. Small extracellular vesicles in cancer. Bioact Mater. 2021;6(11):3705–3743. doi:10.1016/j.bioactmat.2021.03.015
19. Kogure A, Yoshioka Y, Ochiya T. Extracellular vesicles in cancer metastasis: potential as therapeutic targets and materials. Int J Mol Sci. 2020;21(12):4463. doi:10.3390/ijms21124463
20. Kumar MA, Baba SK, Sadida HQ, et al. Extracellular vesicles as tools and targets in therapy for diseases. Signal Transduct Target Ther. 2024;9(1):27. doi:10.1038/s41392-024-01735-1
21. Zhou Y, Liu Z. Saliva biomarkers in oral disease. Clin Chim Acta. 2023;548:117503. doi:10.1016/j.cca.2023.117503
22. Liu J, Huang D, Cai Y, et al. Saliva diagnostics: emerging techniques and biomarkers for salivaomics in cancer detection. Exp Rev Molecular Diag. 2022;22(12):1077–1097. doi:10.1080/14737159.2022.2167556
23. Kaczor-Urbanowicz KE, Martin Carreras-Presas C, Aro K, Tu M, Garcia-Godoy F, Wong DT. Saliva diagnostics - current views and directions. Exp Biol Med. 2017;242(5):459–472. doi:10.1177/1535370216681550
24. Topkas E, Keith P, Dimeski G, Cooper-White J, Punyadeera C. Evaluation of saliva collection devices for the analysis of proteins. Clin Chim Acta. 2012;413(13–14):1066–1070. doi:10.1016/j.cca.2012.02.020
25. Eftekhari A, Maleki Dizaj S, Sharifi S, et al. Salivary biomarkers in cancer. Adv Clin Chem. 2022;110:171–192. doi:10.1016/bs.acc.2022.06.005
26. Chojnowska S, Baran T, Wilińska I, Sienicka P, Cabaj-Wiater I, Knaś M. Human saliva as a diagnostic material. Adv Med Sci. 2018;63(1):185–191. doi:10.1016/j.advms.2017.11.002
27. Zhang CZ, Cheng XQ, Li JY, et al. Saliva in the diagnosis of diseases. Int J Oral Sci. 2016;8(3):133–137. doi:10.1038/ijos.2016.38
28. Nijakowski K, Owecki W, Jankowski J, Surdacka A. Salivary biomarkers for parkinson’s disease: a systematic review with meta-analysis. Cells. 2024;13(4):340. doi:10.3390/cells13040340
29. Nijakowski K, Owecki W, Jankowski J, Surdacka A. Salivary biomarkers For Alzheimer’s disease: a systematic review with meta-analysis. Int J Mol Sci. 2024;25(2):1168. doi:10.3390/ijms25021168
30. Nijakowski K, Zdrojewski J, Nowak M, Gruszczyński D, Knoll F, Surdacka A. Salivary metabolomics for systemic cancer diagnosis: a systematic review. Metabolites. 2022;13(1):28. doi:10.3390/metabo13010028
31. Nijakowski K, Surdacka A. Salivary biomarkers for diagnosis of inflammatory bowel diseases: a systematic review. Int J Mol Sci. 2020;21(20):7477. doi:10.3390/ijms21207477
32. Nijakowski K, Gruszczyński D, Kopała D, Surdacka A. Salivary metabolomics for oral squamous cell carcinoma diagnosis: a systematic review. Metabolites. 2022;12(4):294. doi:10.3390/metabo12040294
33. Yap T, Pruthi N, Seers C, Belobrov S, McCullough M, Celentano A. Extracellular vesicles in oral squamous cell carcinoma and oral potentially malignant disorders: a systematic review. Int J Mol Sci. 2020;21(4):1197. doi:10.3390/ijms21041197
34. Zhang Y, Liu J, Liu S, et al. Extracellular vesicles in oral squamous cell carcinoma: current progress and future prospect. Front Bioeng Biotechnol. 2023;11:1149662. doi:10.3389/fbioe.2023.1149662
35. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
36. Owecki W, Wojtowicz K, Nijakowski K. Salivary extracellular vesicles in detection of cancers other than head and neck: a systematic review. Cells. 2025;14(6):411. doi:10.3390/cells14060411
37. Study quality assessment tools | NHLBI, NIH. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
38. Bano A, Vats R, Verma D, Yadav P, Kamboj M, Bhardwaj R. Exploring salivary exosomes as early predictors of oral cancer in susceptible tobacco consumers: non-invasive diagnostic and prognostic applications. J Cancer Res Clin Oncol. 2023;149(17):15781–15793. doi:10.1007/s00432-023-05343-4
39. Bozyk N, Tang KD, Zhang X, et al. Salivary exosomes as biomarkers for early diagnosis of oral squamous cell carcinoma. Oral Oncology Reports. 2023:6. doi:10.1016/j.oor.2023.100017
40. Lim Y, Tang KD, Karpe AV, et al. Chemoradiation therapy changes oral microbiome and metabolomic profiles in patients with oral cavity cancer and oropharyngeal cancer. Head Neck. 2021;43(5):1521–1534. doi:10.1002/hed.26619
41. Faur CI, Roman RC, Jurj A, et al. Salivary exosomal MicroRNA-486-5p and MicroRNA-10b-5p in oral and oropharyngeal squamous cell carcinoma. Medicina. 2022;58(10):1478. doi:10.3390/medicina58101478
42. Faur CI, Dinu C, Toma V, et al. A New detection method of oral and oropharyngeal squamous cell carcinoma based on multivariate analysis of surface enhanced raman spectra of salivary exosomes. J Pers Med. 2023;13(5):762. doi:10.3390/jpm13050762
43. Feng J, Xiao BL, Zhang LZ, et al. Simultaneous detection of two extracellular vesicle subpopulations in saliva assisting tumor t staging of oral squamous cell carcinoma. Anal Chem. 2023;95(19):7753–7760. doi:10.1021/acs.analchem.3c00940
44. Fontana S, Mauceri R, Novara ME, Alessandro R, Campisi G. Protein cargo of salivary small extracellular vesicles as potential functional signature of oral squamous cell carcinoma. Int J Mol Sci. 2021;22(20):11160. doi:10.3390/ijms222011160
45. Gai C, Camussi F, Broccoletti R, et al. Salivary extracellular vesicle-associated miRNAs as potential biomarkers in oral squamous cell carcinoma. BMC Cancer. 2018;18(1):439. doi:10.1186/s12885-018-4364-z
46. He L, Ping F, Fan Z, et al. Salivary exosomal miR-24-3p serves as a potential detective biomarker for oral squamous cell carcinoma screening. Biomed Pharmacother. 2020;121:109553. doi:10.1016/j.biopha.2019.109553
47. Hofmann L, Medyany V, Ezić J, et al. Cargo and functional profile of saliva-derived exosomes reveal biomarkers specific for head and neck cancer. Front Med Lausanne. 2022;9:904295. doi:10.3389/fmed.2022.904295
48. Hofmann L, Abou Kors T, Ezić J, et al. Comparison of plasma- and saliva-derived exosomal miRNA profiles reveals diagnostic potential in head and neck cancer. Front Cell Dev Biol. 2022;10:971596. doi:10.3389/fcell.2022.971596
49. Langevin S, Kuhnell D, Parry T, et al. Comprehensive microRNA-sequencing of exosomes derived from head and neck carcinoma cells in vitro reveals common secretion profiles and potential utility as salivary biomarkers. Oncotarget. 2017;8(47):82459–82474. doi:10.18632/oncotarget.19614
50. Man QW, Li RF, Bu LL, Zhao Y, Liu B. Salivary non-apoptotic tumoral microvesicles: a potential progressive marker in oral cancer patients. J Cell Mol Med. 2022;26(24):5955–5965. doi:10.1111/jcmm.17461
51. Nakamichi E, Sakakura H, Mii S, et al. Detection of serum/salivary exosomal Alix in patients with oral squamous cell carcinoma. Oral Dis. 2021;27(3):439–447. doi:10.1111/odi.13565
52. Patel A, Patel S, Patel P, Mandlik D, Patel K, Tanavde V. Salivary exosomal miRNA-1307-5p predicts disease aggressiveness and poor prognosis in oral squamous cell carcinoma patients. Int J Mol Sci. 2022;23(18):10639. doi:10.3390/ijms231810639
53. Davidovich E, Aframian DJ, Shapira J, Peretz B. A comparison of the sialochemistry, oral pH, and oral health status of Down syndrome children to healthy children. Int J Paediatr Dent. 2010;20(4):235–241. doi:10.1111/j.1365-263X.2010.01045.x
54. Patel A, Patel P, Mandlik D, et al. A novel 3-miRNA network regulates tumour progression in oral squamous cell carcinoma. Biomark Res. 2023;11(1):64. doi:10.1186/s40364-023-00505-5
55. Ventura TMO, Ribeiro NR, Taira EA, et al. Radiotherapy changes the salivary proteome in head and neck cancer patients: evaluation before, during, and after treatment. Clin Oral Investig. 2022;26(1):225–258. doi:10.1007/s00784-021-03995-5
56. Sharma S, Gillespie BM, Palanisamy V, Gimzewski JK. Quantitative nanostructural and single-molecule force spectroscopy biomolecular analysis of human-saliva-derived exosomes. Langmuir. 2011;27(23):14394–14400. doi:10.1021/la2038763
57. Sun J, Wang X, Ding Y, et al. Proteomic and phosphoproteomic landscape of salivary extracellular vesicles to assess OSCC therapeutical outcomes. Proteomics. 2023;23(5):e2200319. doi:10.1002/pmic.202200319
58. Tang KD, Wan Y, Zhang X, et al. Proteomic alterations in salivary exosomes derived from human papillomavirus-driven oropharyngeal cancer. Mol Diagn Ther. 2021;25(4):505–515. doi:10.1007/s40291-021-00538-2
59. Tang KD, Menezes L, Baeten K, et al. Oral HPV16 prevalence in oral potentially malignant disorders and oral cavity cancers. Biomolecules. 2020;10(2):223. doi:10.3390/biom10020223
60. Tengler L, Tiedtke M, Schütz J, et al. Optimization of extracellular vesicles preparation from saliva of head and neck cancer patients. Sci Rep. 2024;14(1):946. doi:10.1038/s41598-023-50610-6
61. Wang Z, Li F, Rufo J, et al. Acoustofluidic salivary exosome isolation: a liquid biopsy compatible approach for human papillomavirus-associated oropharyngeal cancer detection. J Mol Diagn. 2020;22(1):50–59. doi:10.1016/j.jmoldx.2019.08.004
62. Winck FV, Prado Ribeiro AC, Ramos Domingues R, et al. Insights into immune responses in oral cancer through proteomic analysis of saliva and salivary extracellular vesicles. Sci Rep. 2015;5(1):16305. doi:10.1038/srep16305
63. Zhong WQ, Ren JG, Xiong XP, et al. Increased salivary microvesicles are associated with the prognosis of patients with oral squamous cell carcinoma. J Cell Mol Med. 2019;23(6):4054–4062. doi:10.1111/jcmm.14291
64. Zlotogorski-Hurvitz A, Dekel BZ, Malonek D, Yahalom R, Vered M. FTIR-based spectrum of salivary exosomes coupled with computational-aided discriminating analysis in the diagnosis of oral cancer. J Cancer Res Clin Oncol. 2019;145(3):685–694. doi:10.1007/s00432-018-02827-6
65. OCEBM Levels of Evidence. Available from: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence.
66. Liu C, Wang M, Zhang H, et al. Tumor microenvironment and immunotherapy of oral cancer. Eur J Med Res. 2022;27(1):198. doi:10.1186/s40001-022-00835-4
67. Warnakulasuriya S, Kerr AR. Oral Cancer Screening: past, Present, and Future. J Dent Res. 2021;100(12):1313–1320. doi:10.1177/00220345211014795
68. Abati S, Bramati C, Bondi S, Lissoni A, Trimarchi M. Oral cancer and precancer: a narrative review on the relevance of early diagnosis. Int J Environ Res Public Health. 2020;17(24):9160. doi:10.3390/ijerph17249160
69. Sarode G, Maniyar N, Sarode SC, Jafer M, Patil S, Awan KH. Epidemiologic aspects of oral cancer. Dis Mon. 2020;66(12):100988. doi:10.1016/j.disamonth.2020.100988
70. Badwelan M, Muaddi H, Ahmed A, Lee KT, Tran SD. Oral squamous cell carcinoma and concomitant primary tumors, what do we know? A review of the literature. Curr Oncol. 2023;30(4):3721–3734. doi:10.3390/curroncol30040283
71. Tan Y, Wang Z, Xu M, et al. Oral squamous cell carcinomas: state of the field and emerging directions. Int J Oral Sci. 2023;15(1):44. doi:10.1038/s41368-023-00249-w
72. Kerr AR, Lodi G. Management of oral potentially malignant disorders. Oral Dis. 2021;27(8):2008–2025. doi:10.1111/odi.13980
73. Mello FW, Miguel AFP, Dutra KL, et al. Prevalence of oral potentially malignant disorders: a systematic review and meta-analysis. J Oral Pathol Med. 2018;47(7):633–640. doi:10.1111/jop.12726
74. Chamoli A, Gosavi AS, Shirwadkar UP, et al. Overview of oral cavity squamous cell carcinoma: risk factors, mechanisms, and diagnostics. Oral Oncol. 2021;121:105451. doi:10.1016/j.oraloncology.2021.105451
75. Jagadeesan D, Sathasivam KV, Fuloria NK, et al. Comprehensive insights into oral squamous cell carcinoma: diagnosis, pathogenesis, and therapeutic advances. Pathol Res Pract. 2024;261:155489. doi:10.1016/j.prp.2024.155489
76. Cristaldi M, Mauceri R, Di Fede O, Giuliana G, Campisi G, Panzarella V. Salivary biomarkers for oral squamous cell carcinoma diagnosis and follow-up: current status and perspectives. Front Physiol. 2019;10:1476. doi:10.3389/fphys.2019.01476
77. Leung LL, Riaz MK, Qu X, Chan J, Meehan K. Profiling of extracellular vesicles in oral cancer, from transcriptomics to proteomics. Semi Cancer Biol. 2021;74:3–23. doi:10.1016/j.semcancer.2021.01.002
78. Ribeiro FAP, Noguti J, Oshima CTF, Ribeiro DA. Effective targeting of the epidermal growth factor receptor (EGFR) for treating oral cancer: a promising approach. Anticancer Res. 2014;34(4):1547–1552.
79. Tang Y, Zang H, Wen Q, Fan S. AXL in cancer: a modulator of drug resistance and therapeutic target. J Exp Clin Cancer Res. 2023;42(1):148. doi:10.1186/s13046-023-02726-w
80. Sun X, Xiao D, Xu T, Yuan Y. miRNA-24-3p promotes cell proliferation and regulates chemosensitivity in head and neck squamous cell carcinoma by targeting CHD5. Future Oncol. 2016;12(23):2701–2712. doi:10.2217/fon-2016-0179
81. Nikkilä R, Tolonen S, Salo T, Carpén T, Pukkala E, Mäkitie A. Occupational etiology of oropharyngeal cancer: a literature review. Int J Environ Res Public Health. 2023;20(21):7020. doi:10.3390/ijerph20217020
82. Psyrri A, Prezas L, Burtness B. Oropharyngeal cancer. Clin Adv Hematol Oncol. 2008;6(8):604–612.
83. Tanaka TI, Alawi F. Human papillomavirus and oropharyngeal cancer. Dent Clin North Am. 2018;62(1):111–120. doi:10.1016/j.cden.2017.08.008
84. You EL, Henry M, Zeitouni AG. Human papillomavirus-associated oropharyngeal cancer: review of current evidence and management. Curr Oncol. 2019;26(2):119–123. doi:10.3747/co.26.4819
85. Mayne GC, Woods CM, Dharmawardana N, et al. Cross validated serum small extracellular vesicle microRNAs for the detection of oropharyngeal squamous cell carcinoma. J Transl Med. 2020;18(1):280. doi:10.1186/s12967-020-02446-1
86. Uehara T, Doi H, Ishikawa K, et al. Serum lactate dehydrogenase is a predictive biomarker in patients with oropharyngeal cancer undergoing radiotherapy: retrospective study on predictive factors. Head Neck. 2021;43(10):3132–3141. doi:10.1002/hed.26814
87. Zdrojewski J, Nowak M, Nijakowski K, et al. Potential immunohistochemical biomarkers for grading oral dysplasia: a literature review. Biomedicines. 2024;12(3):577. doi:10.3390/biomedicines12030577
88. Costa EFD, Lima TRP, Lopes-Aguiar L, et al. FAS and FASL variations in outcomes of tobacco- and alcohol-related head and neck squamous cell carcinoma patients. Tumour Biol. 2020;42(7):1010428320938494. doi:10.1177/1010428320938494
89. Paderno A, Petrelli F, Lorini L, Capriotti V, Gurizzan C, Bossi P. The predictive role of PD-L1 in head and neck cancer: a systematic review and meta-analysis. Oral Oncol. 2024;153:106799. doi:10.1016/j.oraloncology.2024.106799
90. Solovicová V, Ďatková A, Bertók T, et al. Advances in magnetic affinity-based isolation/detection of exosomes for robust diagnostics. Microchim Acta. 2025;192(4):206. doi:10.1007/s00604-025-07048-6
91. Leung LL, Qu X, Chen B, JYk C. Extracellular vesicles in liquid biopsies: there is hope for oral squamous cell carcinoma. Extracell Vesicles Circ Nucleic Acids. 2024. doi:10.20517/evcna.2024.29
92. Yin H, Zhang M, Zhang Y, Zhang X, Zhang X, Zhang B. Liquid biopsies in cancer. Mol Biomed. 2025;6(1):18. doi:10.1186/s43556-025-00257-8
93. Liu ZX, Chen G, Yu ZL. Advances in subpopulation separation and detection of extracellular vesicles: for liquid biopsy and downstream research. Theranostics. 2025;15(3):1135–1155. doi:10.7150/thno.106459
94. Li Z, Yan J, Li X, et al. Advancements in extracellular vesicles biomanufacturing: a comprehensive overview of large-scale production and clinical research. Front Bioeng Biotechnol. 2025;13:1487627. doi:10.3389/fbioe.2025.1487627
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nanotechnology: A Promising Approach for Cancer Diagnosis, Therapeutics and Theragnosis
Dessale M, Mengistu G, Mengist HM
International Journal of Nanomedicine 2022, 17:3735-3749
Published Date: 26 August 2022
Manuscript Title: A 4-miRNAs Serum Panel for Obstructive Sleep Apnea Syndrome Screening
Mo J, Zeng C, Li W, Song W, Xu P
Nature and Science of Sleep 2022, 14:2055-2064
Published Date: 9 November 2022
Ability of Blood Cell Parameters to Predict Clinical Outcomes of Nivolumab Monotherapy in Advanced Esophageal Squamous Cell Carcinoma
Hamai Y, Emi M, Ibuki Y, Kurokawa T, Yoshikawa T, Ohsawa M, Hirohata R, Kitasaki N, Okada M
OncoTargets and Therapy 2023, 16:263-273
Published Date: 10 April 2023
Globoid Cell Leukodystrophy (Krabbe Disease): An Update
Maghazachi AA
ImmunoTargets and Therapy 2023, 12:105-111
Published Date: 31 October 2023
Extracellular Vesicles in Idiopathic Pulmonary Fibrosis: Pathogenesis, Biomarkers and Innovative Therapeutic Strategies

Yang Y, Lv M, Xu Q, Wang X, Fang Z
International Journal of Nanomedicine 2024, 19:12593-12614
Published Date: 25 November 2024