")
Back to Journals » Nature and Science of Sleep » Volume 17
Screening OSA in Chinese Smart Device Consumers: A Real-World Arrhythmia-Related Study
Authors Chen Y , Zhang H, Li J, Xu P, Guo Y, Xie L
Received 6 December 2024
Accepted for publication 23 March 2025
Published 22 April 2025 Volume 2025:17 Pages 663—676
DOI https://doi.org/10.2147/NSS.S509097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yibing Chen,1 Hui Zhang,2 Jing Li,3 Peida Xu,3 Yutao Guo,2 Lixin Xie4,5
1Department of Pulmonary and Critical Care Medicine, The First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China; 2Department of Pulmonary Vessel and Thromboembolic Disease, The Sixth Medical Center of PLA General Hospital, Beijing, 100142, People’s Republic of China; 3HUAWEI Device Co., Ltd., Shenzhen, 518129, People’s Republic of China; 4College of Pulmonary and Critical Care Medicine, The Eighth Medical Center of Chinese PLA General Hospital, Beijing, 100091, People’s Republic of China; 5Chinese Association of Geriatric Research, Beijing, 100853, People’s Republic of China
Correspondence: Lixin Xie, Email [email protected]
Introduction: Early detection of obstructive sleep apnea (OSA) is critical due to its link to cardiovascular diseases. Our previous study validated an algorithm-based photoplethysmography (PPG) smartwatch for OSA risk detection.
Objective: This study aimed to characterize OSA features and assess its association with arrhythmia risk among smart wearable device (SWD) consumers in China in a real-world setting.
Methods: Between December 15, 2019, and January 31, 2022, SWD consumers across China were screened for OSA risk using HUAWEI devices. OSA diagnosis was confirmed via telecare follow-ups, including clinical evaluations and sleep test records. Disease characteristics and arrhythmia risks were analyzed.
Results: In a large cohort of 1,056,494 participants, smart wearable devices (SWDs) effectively identified 19,563 individuals at high risk for OSA, with 1054 confirmed cases. OSA patients demonstrated high prevalence of obesity (46.8%), hypertension (19.8%), and arrhythmia (17.17%). SWDs detected abnormal heart rhythms or suspected arrhythmia in 95.9% of confirmed OSA cases. Age emerged as an independent predictor of arrhythmia risk, while hypertensive OSA patients were older, more obese, and experienced prolonged nocturnal hypoxia (Time length of SpO2< 90%, P=0.020). These findings underscore the utility of SWDs in OSA screening and highlight the significant cardiovascular risks associated with OSA.
Conclusion: PPG-based SWD effectively screened for OSA and identified elevated arrhythmia risks. These findings support their utility for large-scale OSA screening and highlight cardiovascular risks management.
Clinical Trial Registry Name: Mobile Health (mHealth) technology for improved screening, patient involvement and optimizing integrated care in atrial fibrillation.
Registration Number: ChiCTR-OOC-17014138.
Date of Registration: 2017– 12-26.
Date of Last Refreshed On: 2018– 11-18.
Keywords: obstructive sleep apnea, smart wearable device, arrhythmias, hypertension
Introduction
China has the highest prevalence of obstructive sleep apnea (OSA) in the world, yet it remains significantly underdiagnosed. According to a Lancet report, approximately 176 million people in China suffer from OSA, with over 65 million cases classified as moderate or severe.1 However, the clinical diagnosis rate is less than 1%, highlighting a critical gap in detection and management. The severity of OSA, particularly moderate to severe cases, is strongly associated with serious complications, including cardiovascular and cerebrovascular diseases, diabetes, and neuropsychiatric disorders. These complications not only impact patient health but also impose a substantial burden on the nation’s healthcare economy. Traditionally, OSA diagnosis occurs only after complications arise, further delaying intervention. Compounding this issue, sleep medicine is a relatively nascent field in China, and the limited diagnostic and treatment resources are insufficient to meet the growing demand for timely and accurate OSA diagnosis.
Arrhythmia often occurs early as an OSA-associated complication. OSA is an independent risk factor for heart arrhythmia.2,3 The OSA diagnosis and severity are independently associated with incident atrial fibrillation (AF).4 Adjusted by age, sex, body mass index, and indicators of coronary heart disease, individuals with sleep-disordered breathing have four times the odds of AF, three times the odds of non-sustained ventricular tachycardia, and almost twice the odds of complex ventricular ectopy.5 The odds of an arrhythmia after respiratory disturbance are nearly 18 times that of an arrhythmia occurring after normal breathing.6 Compared to non-OSA patients, patients with OSA were associated with higher odds of bradycardia, AF and ventricular premature complexes.4,7–9 In addition, the routine OSA assessment, including the respiratory event index (REI) / apnea-hypopnea index (AHI) / respiratory disturbance index (RDI), may not reflect other important aspects of OSA pathophysiology, such as the degree of low blood oxygen, the distribution of events over the whole sleep, and the degree of sleep fragmentation.2 Therefore, it is necessary to analyze the relationship between OSA and cardiovascular disease burden in combination with other indicators, such as hypoxia. At present, research in China has not produced a sufficiently large population sample dataset to identify a correlation between the two.
The current boom in wearable technology has opened up a new realm for the diagnosis of sleep respiratory diseases.10 Smart wearable devices (SWD) offer the advantage of non-invasive monitoring, with continuous data collection that greatly facilitates personalized health management. The algorithm established based on physiological signals monitored using Photoplethysmography (PPG) technology has already been used as an electronic biomarker for OSA screening. PPG is a non-invasive optical technique. By irradiating the skin with light and measuring the amount of light either transmitted through or reflected back to a photodetector, it can capture fluctuations in blood volume and hemoglobin absorption of light corresponding to the cardiac cycle, and it enables the measurement of physiological parameters such as heart rate and blood oxygen saturation. According to validation research, the accuracy of OSA screening using a wrist-worn reflective PPG device reached 0.84/0.86/0.85 for mild/moderate/severe OSA, respectively.11 Our previous research has demonstrated that smartwatches utilizing PPG technology exhibit considerable potential in OSA screening. Compared to HSAT, the accuracy, sensitivity, and specificity for predicting moderate to severe OSA (AHI≥15) were 87.9%, 89.7%, and 86.0%, respectively. When compared to PSG, the accuracy, sensitivity, and specificity for predicting OSA (AHI≥5) were 81.1%, 76.5%, and 100%, respectively.12 Additionally, PPG-based smart devices have shown excellent performance in AF screening,13,14 effectively screening low-risk general populations with a confirmation rate exceeding 93%. Furthermore, it was found that OSA is a significant risk factor for AF, with high-risk OSA increasing the prevalence of AF by 1.5 times.15 Although the sensors of SWD may be affected by calibration, the environment, or individual differences, it still remains an effective large-scale screening tool in situations with limited medical resources. In this study, we investigated high-risk individuals for OSA among Chinese smart device consumers to understand the diagnosis of OSA, its clinical characteristics, and the relationship between OSA and arrhythmia in a real-world setting.
Methods
We developed wearable smart device-based algorithms to detect OSA and arrhythmias (AF, ectopic, or irregular arrhythmias) (Figure 1).
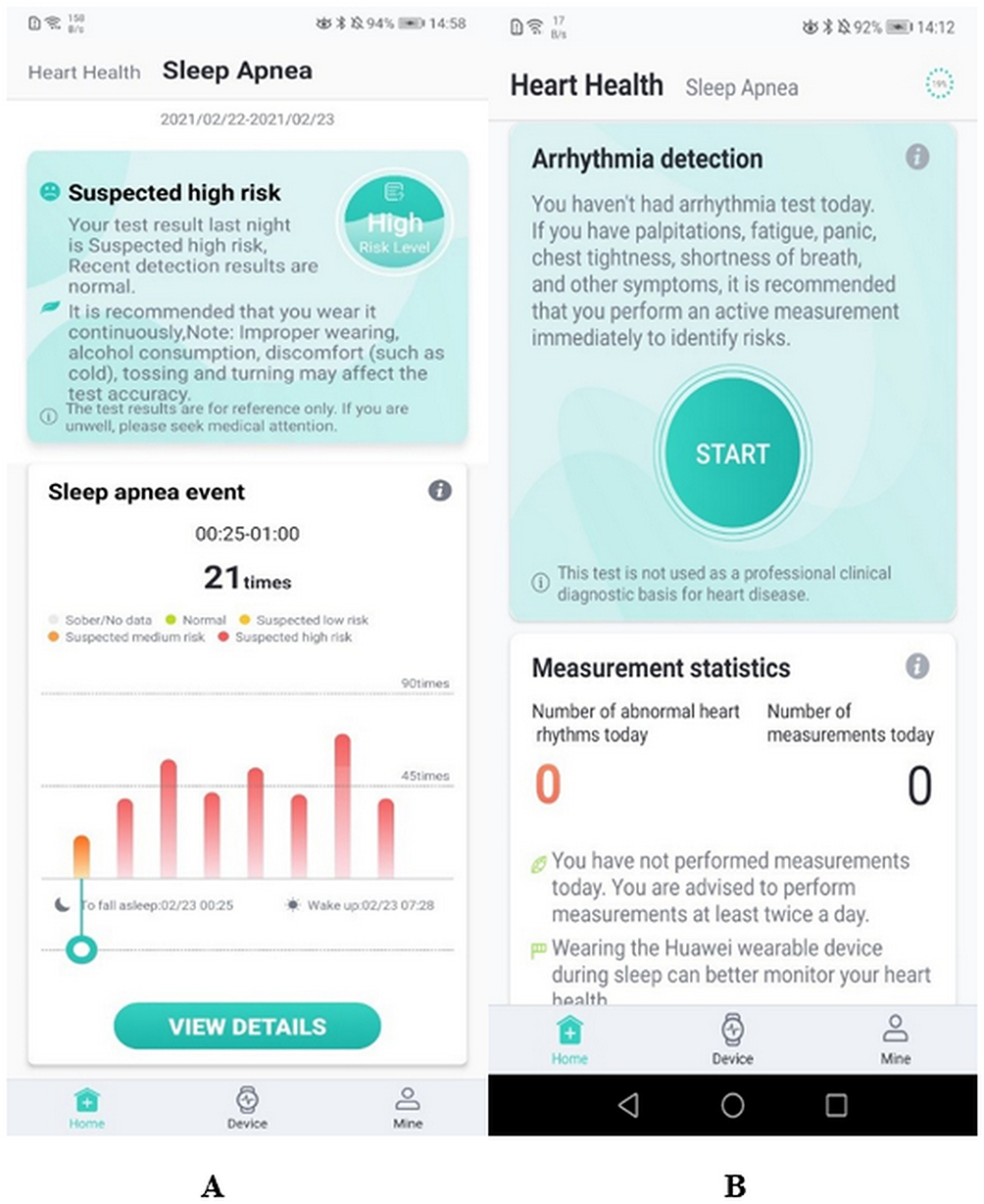 |
Figure 1 Sleep Apnea Study (A) and Heart Health (B) App interface. |
The design and principal findings from the Heart Study were previously reported.15 Inclusion criteria: Generally, smart band or smartwatch (HUAWEI Device Co., Ltd.) wearers aged over 18 can participate in this research freely by downloading a screening app through the App Store from locations across China. After receiving the study design, providing electronic informed consent, and matching compatible smart devices, the participants were entered into the study. Participants retain the autonomy to freely decide whether to continue or discontinue their involvement in our study at any time. Exclusion criteria: Individuals < 18 years old and those who were unable to use smartphones or devices were excluded. Adult subjects entered into this study between Dec 15, 2019, and Jan 31, 2022. All participants were asked to voluntarily complete the questionnaire on OSA and heart health (Supplementals 1 and 2). Subjects who had a compatible wearable PPG sensor could freely decide whether to receive sleep apnea screening plus arrhythmia screening using screening apps. The smart devices in this study were the GT2 series and GT3 series smartwatches and the smart bracelets B6, 4 Pro, 6, 7, as shown in Figure 2. After acquisition, the photoplethysmography data will be anonymized and transferred to a dedicated research platform, accessible exclusively to authorized research personnel. The research platform was reported in a previous study.15
 |
Figure 2 Smartwatches(A) /bracelets(B) adapted to the Heart Health and Sleep Apnea Study (Provided by HUAWEI Device Co., Ltd., owns the final copyright of the figure). |
Ethical Approvement and Clinical Registration
This study was approved by the Central Medical Ethics Committee of Chinese PLA General Hospital (approval number: S2017–105–02) and registered at the Chinese Clinical Trial Registry (ChiCTR) website (ChiCTR-OOC-17014138). Electronic written informed consent was obtained from all participants at enrollment on the research application. Electronic informed consent was signed before enrolling in the research. All user data was anonymized on the research platform for users’ privacy. Participants were completely voluntary without any form of compensation.
OSA Risk Identification with Smartwatches
At least 14-day monitoring was performed using PPG-SWDs. Blood oxygen saturation, heart rate, and sleep duration were monitored to calculate AHI and assess the risk of OSA. The risk levels for OSA were categorized into four groups: normal, low risk, intermediate risk, and high risk. These categories were defined as follows: High risk for sleep apnea was defined as more than 80% of monitoring measures with AHI ≥ 30 during sleep; Intermediate risk for sleep apnea was defined as more than 80% of monitoring measures with 15 < AHI < 30 during sleep; Low risk was defined as more than 80% of monitoring measures with 5 < AHI ≤ 15 during sleep. All other outcomes were classified as normal. Blood oxygen saturation was calculated for individuals with sleep time ≥ 4 h per night or ≥ 7 h per night. Mild hypoxia in OSA is defined as an oxygen saturation decrease to a range between 85% and 89% during sleep, moderate hypoxia as a decrease to a range between 80% and 84% during sleep, and severe hypoxia as a decrease to less than 80% during sleep. In accordance with the YY0784-2010 standard in China,16 we have verified the accuracy of pulse oxygen saturation measurements in smartwatches. Our comparison with arterial blood gas analyses conducted in hospitals (detailing both the sampling method and the analyzer model used) reveals that these smartwatches meet the standard acceptance criteria within the 70% - 100% blood oxygen saturation range. This is evidenced by an Average Root Mean Square Error (ARMS) of less than 4%.
Arrhythmias Identification with Smartwatches
At least 14 days of monitoring using PPG-smart devices was performed per participant. Periodic measurements of PPG were automatically taken every 10 min, and 60s PPG signals were continuously collected. The participants could initiate active measurements at rest, and 45s PPG signals or 30s single ECGs were measured. AF, ectopic, and irregular arrhythmia were identified (Figure 3). The PPG algorithm for AF detection has been reported.12,16 High/low heart rate was defined in terms of beats per minute (BPM)≥100 or BPM≤50 at rest. Irregular rhythm was defined as low or moderate AF risk. Moderate-risk premature beat was defined as 0.5–10% of the ectopic heart rate during the monitored time, and high risk for premature beat was over 10% of the detected ectopic rate during the monitored time.
 |
Figure 3 Interface of the active measurement process (PPG). |
Confirmation of OSA and Arrhythmias by Telemedicine
To ensure adequate statistical power for validating the accuracy of the screening method, a sample size calculation was performed. Based on the preliminary accuracy of 85.9% for the PPG-based screening method for obstructive sleep apnea (OSA), we aimed to detect a 2% change in accuracy (ie, a reduction to 83.9%). Assuming a significance level (α) of 0.05 and a statistical power of 95%, the required sample size was calculated using the standard formula for proportion-based studies. The calculation yielded a sample size of approximately 15,720 participants. Subjects who received a notification of detected AF or high OSA risk could decide whether to be followed up for confirmation of diagnoses of AF or OSA by the mAFA (Mobile Health [mHealth] Technology for Improved Screening, Patient Involvement and Optimizing Integrated Care in Atrial Fibrillation) telecare team for free. After these participants chose “Yes” on the Heart Health Study or Sleep Apnea screening app, the health providers in the mAFA Telecare center contacted them to confirm the diagnosis of arrhythmia or OSA in a hospital setting. Confirmation of OSA diagnosis was made through telephone visits. Patients diagnosed with OSA follow AASM (American Association of Sleep Medicine) guidelines based on PSG (polysomnography), symptoms, and HSAT (home sleep apnea test) completed in hospitals.17 The telephone visit time window lasts two weeks after the first telephone visit, leaving a diagnosis chance for high-OSA-risk consumers. The mAFA telecare team and health providers followed up with the detected subjects with high OSA risk or arrhythmias according to the subjects’ informed consent through telephone. The arrhythmias were further diagnosed with clinical evaluation, 12-lead ECG, or 24-hour Holter monitoring. It is important to note that the heart rhythms measured in this study using PPG technology are derived from heart rate, rather than from an electrocardiogram. Medical history, cardiovascular risk factors, and comorbidities were investigated by questionnaires (Supplementals 1–3) pushed with the research application. The overall flow chart is depicted in Figure 4.
 |
Figure 4 Flow chart of Consumer-led Screening for OSA. Notes: Detected Suspected arrhythmia include: irregular rhythm, suspected atrial fibrillation, high/low heart rate, suspected premature beat etc. |
Statistical Analysis
The primary endpoint was defined as the confirmation or exclusion of OSA diagnosis in high-OSA-risk SWD consumers, as determined during the telephone follow-up. The secondary endpoints include additional questionnaire items administered during the telephone follow-up, specifically the sleep and heart health questionnaires (Supplementals 1–3). Continuous variables were tested for normality with the Kolmogorov–Smirnov test. Data with normal distributions are presented as means ± standard deviations and described. Different group data with normal distributions were compared with the t-test. Logistic regression was conducted to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for confounders. A two-sided P<0.05 was considered statistically significant. Statistical analysis of variables was performed with IBM SPSS Statistics, version 26.0 (IBM, Chicago, IL, USA). To address multiple comparisons, we applied Benjamini-Hochberg FDR (False Discovery Rate) correction for comorbidities analysis and logistic regression p-values. Geographical distribution was depicted by JavaScript, an open framework Vue 2.0. The pie and column charts were created using Microsoft Corporation (2019) Excel software (Version 2311 Build 16.0.17029.20028).
Results
In all, 1,056,494 subjects were enrolled and screened in the study between December 15, 2019, and January 31, 2022, of which 19,563 (1.85%) were identified as having high risk, 41,021 (3.88%) moderate risk, and 126,299 (11.95%) low risk for OSA. Figure 5 illustrates the geographic distribution of 19,563 high-risk OSA participants, showing a higher prevalence of OSA risk in populous and economically developed provinces like Guangdong, Jiangsu, Shandong, and Henan, as identified by SWDs. The patient distribution by age is as follows: 866 patients aged 18 to 29, accounting for 4.43% of the total; 5725 patients aged 30 to 39, representing 29.29%; 7516 patients aged 40 to 49, making up 38.45%; 4145 patients aged 50 to 59, which is 21.21%; 978 patients aged 60 to 69, at 4.98%; 261 patients aged 70 to 79, comprising 1.34%; and finally, 59 patients aged 80 to 96, which accounts for 0.30%. Of these, 17,136 subjects were effectively followed up, and only 1218 (7.1%) subjects went to the hospital for examination, of whom 1079 subjects were further confirmed by HSAT or PSG. The demographic statistics of the 19,563 high-risk patients and 1054 confirmed OSA cases are shown in Table 1.
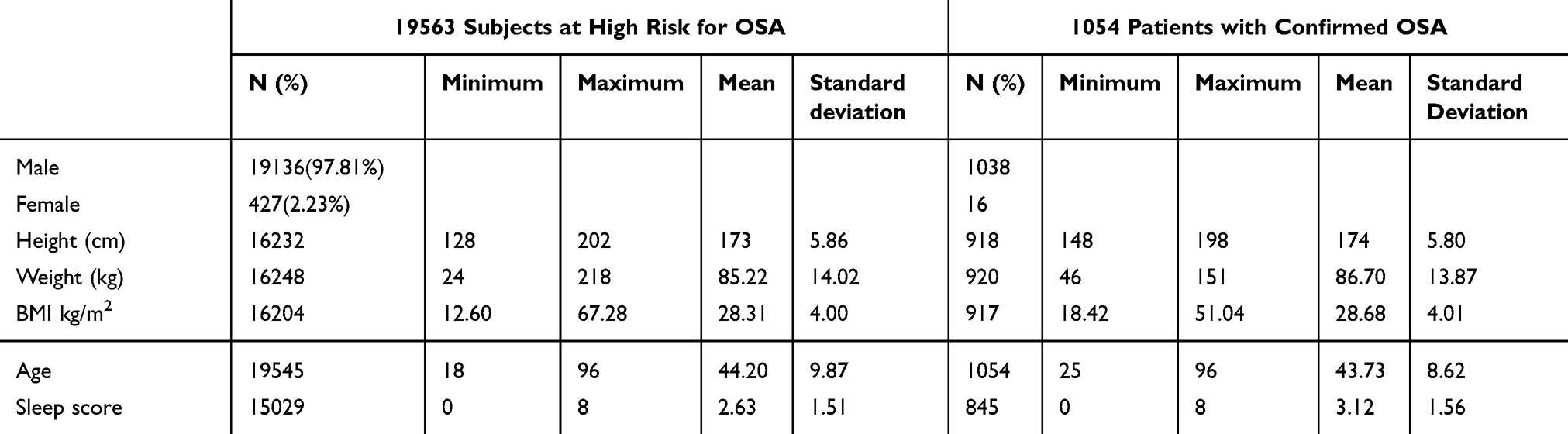 |
Table 1 Demographic Statistics of 19,563 Consumers at High Risk for OSA and 1054 Patients with Confirmed OSA |
 |
Figure 5 Geographic distribution of 19,563 consumers at high risk for OSA. Notes: The orange bubbles represent the number of cases with OSA-high-risk. |
Clinical Profile of Subjects with OSA High-Riskers
The sex, age, height, weight, and medical history of the participants were provided voluntarily. The 16,204 subjects at high risk of OSA and 1054 subjects with OSA diagnosis confirmed by telecare were analyzed. Among the latter group, the most common comorbidity is obesity (46.87%), followed by hypertension (19.83%), arrhythmia (17.17%), rhinitis (14.32%), and pharyngitis (9.30%). Other conditions include tonsil hypertrophy (7.87%), hyperlipidemia (5.40%), diabetes (3.42%), other cardiovascular diseases (3.98%), respiratory diseases (0.38%), and anxiety or depression (0.28%). The OSA severity distribution shows that 69 individuals (6.55%) were mild cases, 181 (17.17%) were moderate cases, 730 (69.26%) were severe cases, and 74 (7.02%) had unknown severity.
Arrhythmia in OSA Patients and OSA High-Riskers
Of the 1054 patients with confirmed OSA, 1011 (95.92%) had an abnormal heart rhythm detected by smart devices (Figure 6), except for “no monitoring” (1.42%) and “normal” (2.66%) individuals. Using the occurrence of arrhythmias in high-risk OSA patients as the dependent variable, and including age, gender, BMI, sleep assessment questionnaire, and hypoxic burden as covariates, logistic regression analysis revealed that, after adjusting for confounding factors, age was the only independent risk factor (Table 2), even after FDR correction (P= 0.000). However, the severity of OSA, sex, and BMI did not show significant differences between the groups with and without arrhythmia as detected by SWD. OSA-high-riskers, the abnormal heart rhythm population also took part in a proportion of 94.45%, except for “no monitoring” (1.73%) and “normal” (3.81%) individuals, as identified by SWD. (Figure 6) The ages of suspected AF consumers (n=370, 53.32±13.67 years) and those with suspected premature beats (n=13,206, 44.15±9.90 years) showed a significant difference (P=0.000).
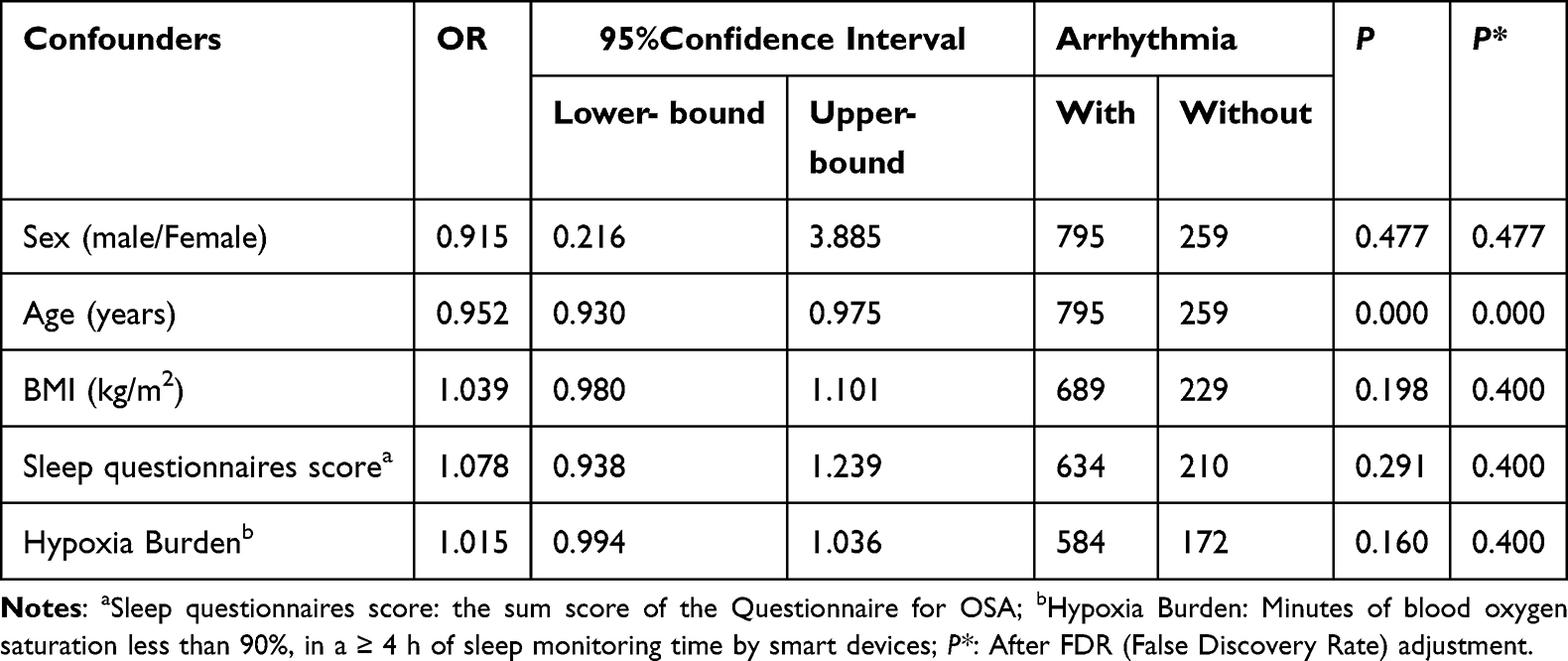 |
Table 2 Logistic Regression for Confounders Factors of Arrhythmia in Confirmed OSA Patients |
 |
Figure 6 Results of cardiac rhythm monitoring by smart devices for 1054 consumers with confirmed OSA and 19,563 high-OSA-risk consumers. |
Furthermore, the analysis of hypoxia’s impact on comorbidities indicated that hypoxia (minutes of blood oxygen saturation below 90%) during both ≥7-hour and ≥4-hour sleep monitoring periods had a statistically significant effect on hypertension (Table 3). However, its effects on obesity, rhinitis, and self-reported arrhythmias were only significant under specific conditions. For instance, hypoxia during ≥4-hour sleep monitoring showed a statistically significant effect on self-reported arrhythmias (P = 0.037, adjusted P = 0.049)(Table 3).
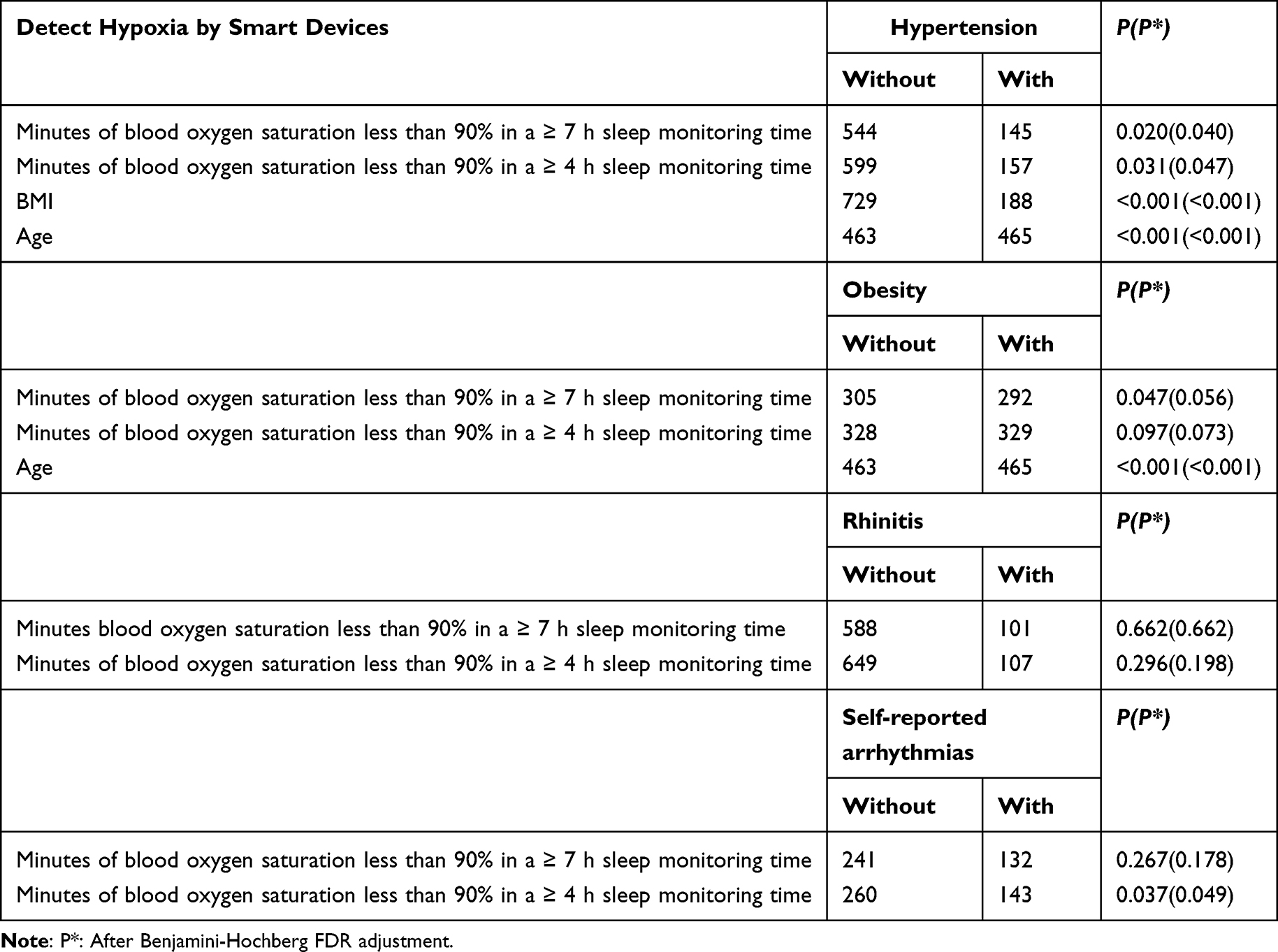 |
Table 3 Impact of Hypoxia on Different Comorbidities |
Discussion
To the best of our knowledge, this was the first study to conduct OSA screening and arrhythmia screening in the real world using wearable smart devices and telemedical follow-ups in China. Our results demonstrated a high level of agreement between high-risk OSA screenings performed by the PPG-based smartwatch and subsequent OSA diagnoses confirmed for the same individuals in hospital settings. In the cohort diagnosed with OSA, a substantial proportion, over two-thirds, were concurrently identified with potentially having suspected arrhythmias using SWD. Additionally, patients with coexisting hypertension demonstrated a notably higher severity of nocturnal hypoxia. These findings support the capability of SWDs in OSA screening and highlight the high prevalence of arrhythmias among OSA patients and high-risk individuals.
Primary Outcome
First, among the 1218 consumers at high risk for OSA who were successfully followed up remotely, the clinical OSA diagnosis rate was 97.7%, illustrating the accuracy of smart devices in screening OSA patients. Among this population, severe OSA was seen in 69.3% of the patients with confirmed OSA. Although, in a previous study, we validated a higher accuracy in screening severe OSA 85.9%,12 the relatively small sample size or confirmation monitoring methods (home sleep apnea or polysomnography tests) in this study may have contributed to this difference. Second, among the 1,056,494 smart device consumers screened nationwide, OSA high-riskers were found in 1.85%, a much lower rate than the prevalence reported in the literature.1 The reason for this may be related to the study population, taking into account the larger proportion with mild and moderate OSA risk detected by the smart device, we did not follow up on all of those with potential OSA risk, which made the 1.85% detection rate way lower than the actual prevalence of OSA. Moreover, most wearable device consumers were relatively young, resulting in a screened population with a high risk for OSA concentrated between 30 and 59 years old. Given that age is a recognized risk factor for OSA,18 an increased prevalence of OSA in older populations is observed, attributable to reduced upper airway muscle tone. At last, our study took more than 2 years to follow up the nearly 20,000 subjects at high risk for OSA screened by smart devices, only to find that merely 1079 (5.5%) patients had been through clinical diagnosis or relevant examinations. This also reflects the lack of public awareness and the low diagnosis rate of OSA in China.
Telephone follow-ups were crucial not only for OSA diagnosis but also for confirming comorbidities. The findings revealed that obesity was the most common comorbidity among OSA patients, followed by hypertension, rhinitis, and arrhythmia. Notably, a higher obesity prevalence was observed in younger OSA patients. Additionally, hypertension was associated with a greater hypoxia burden compared to non-hypertensive patients, aligning with previous studies.19,20 Furthermore, OSA patients with obesity were more likely to have multiple comorbidities, particularly hypertension, rhinitis, diabetes, cardiovascular disease, and hyperlipidemia. However, the presence of rhinitis did not significantly impact the severity of hypoxia or OSA, corroborating findings from other Chinese studies.21 As highlighted in a review,21 in adults, both allergic and nonallergic rhinitis are more likely to exacerbate OSA symptoms rather than increase the risk of OSA. Rhinitis may disrupt sleep architecture, potentially elevating inflammatory mediators and exacerbating rhinitis symptoms.
Due to the reliability of PPG technology for monitoring heart rhythms, it is also used in studies to monitor the heart rhythms of consumers using wearable devices.22,23 A recent study reported a 93.8% accuracy of detection of AF.13 Our study revealed some relationship between arrhythmia and OSA that cannot be ignored. First, we found a high detection rate for detected premature beats of intelligent devices in consumers who are at high risk for OSA and patients with confirmed OSA. Both rates, 72.2% and 67.48%, were significantly higher than the proportion (17.17%) of confirmed arrhythmia reported by patients followed up through telemedicine. This may be related to the fact that a large number of patients were asymptomatic patients with arrhythmias, leading to patients not seeking medical treatment on their own initiative. Few studies on patients with asymptomatic arrhythmias have been reported, but if no intervention is adopted, the potential harm from arrhythmias could be great.24 We analyzed the incidence of arrhythmia in patients with confirmed OSA and identified age as an independent risk factor after adjusting for confounding variables. Further, our results revealed that younger patients were more susceptible to premature beats, whereas older patients were more likely to develop atrial fibrillation (AF). Nevertheless, due to the small sample size, this conclusion needs further research to be confirmed. Second, taking into account the continuous monitoring of wearable devices, these results may reflect the bond between arrhythmia and OSA more accurately. Our previous heart health study24 showed that, compared to the overall AF detection rate of 0.43%, those at high risk for OSA had increased AF prevalence (1.7%). Even after adjusting for age, sex, body mass index, hypertension, diabetes mellitus, cardiovascular diseases, heart failure, and hyperthyroidism, high risk for OSA also increased the risk for AF detection by 1.51-fold.
Although the AF detection rate in our study was much lower than the rate of detected premature beats, the consequences of AF were much more clinically serious. Frequent atrial premature beats and premature atrial contractions (PACs), or short episodes of atrial premature beats may be independent predictors of the development of atrial tachycardia and AF.25,26 However, the impact of completely asymptomatic atrial premature beat PACs is not clear, and there are few relevant studies.27 For this reason, our future research direction is to observe the development of disease in OSA patients with detected premature beats.
Previous studies have elucidated the mechanisms by which OSA can lead to arrhythmia: Intermittent hypoxia triggers autonomic nervous system activation and oxidative stress, causing myocardial cell damage and altered myocardial excitability; recurrent arousals lead to sympathetic activation and coronary vasoconstriction; increased intrathoracic negative pressure may mechanically stretch the myocardium, promoting acute changes in myocardial excitability and structural remodeling.27 CPAP therapy has been shown to immediately reduce heart rate variability in patients with moderate to severe OSA.28 Although these findings are preliminary and necessitate further research, the latest consensus statement from the Asian Pacific Society of Cardiology already advocates for OSA screening in patients with heart failure or arrhythmia.29 The potential progression from early arrhythmia to atrial fibrillation (AF) and premature beats in undiagnosed OSA patients, particularly as they age, warrants additional investigation. In essence, it is crucial to study whether untreated OSA can escalate from initial arrhythmias to final AF in affected individuals.
Limitations
There were many deficiencies in this study. First, the proportion of patients diagnosed by clinicians accounted for a relatively low proportion of consumers at high risk for OSA. The sample was disproportionately male in both consumers at high risk for OSA and the confirmed patients. According to the statistics of our research platform, at present, the proportion of men and women among consumers of smart devices consumers was about 8:2, and this proportion had little difference over time, which also resulted in the low participation of female consumers in our study. In addition, due to the cognitive and operational requirements of smart devices, a few older people (≥60 years old) were enrolled in this study, so the results may not reflect the overall features of this population with a high risk for OSA. Therefore, the results may exhibit significant sex and age bias. While this limits the generalizability of our findings to broader populations, it reflects the current user profile of SWD technology. Second, this study was based on voluntary smart devices consumer participation and telemedicine follow-up, the information obtained was related to the cognitive level of the consumers, and the integrity of medical history data was limited. Thus, the sample size for different analyses was inconsistent. This problem is, in reality, a prevalent limitation inherent in such studies. To address gaps in the medical history of wearable device users, we have collected basic health information through an initial questionnaire. However, by linking data to medical records (with consent), standardizing data collection through digital tools, regular follow-up, incentives for accurate reporting, and cross-checking with medical records can further improve data completeness and accuracy in the future research. Third, due to concern for patients’ privacy, they were not required to upload medical records to the research platform, so the information obtained was only based on the oral statements of patients, resulting in potential deviations in authenticity. Fourth, we only followed up with consumers at high risk for OSA, and normal-, mild-, and moderate-risk consumers were not followed up due to their enormous numbers, which made our sample of limited use for the validation of the false-negative rate of smart device detection. Fifth, the diagnostic rate of OSA patients with arrhythmia was also significantly lower than the proportion of smart device-screened high and medium arrhythmia risk. Concurrently with our primary study, our team conducted a verification of wearable devices’ ability to detect abnormal heart rhythms. Recent research18,30 provides substantial evidence supporting the high accuracy of these devices in identifying abnormal heart rhythms. This rationale underpinned our decision to include heart rhythm detection in our research outcomes for OSA patients and those at high risk.
Future Concerns
The smart wearable device (SWD) utilized in this study shows promising potential for assessing OSA severity and detecting arrhythmias; however, its diagnostic utility for complex comorbidities remains limited due to the inherent constraints of photoplethysmography (PPG) technology. Additionally, the diagnostic accuracy of SWDs varies significantly across devices, highlighting the necessity for rigorous validation of their screening performance.10 Given the well-documented heterogeneity of OSA and its diverse complications,31 future research should prioritize the use of intelligent devices, such as research applications, to differentiate OSA subtypes (eg, excessive sleepiness and insomnia subtypes).32,33 This approach could enable more precise diagnosis, follow-up, and personalized treatment strategies.
To enhance the clinical utility of SWDs, further research and algorithm optimization are critical to improving their ability to identify a wider range of comorbidities and abnormal sleep patterns. While the technology holds significant promise, its current reliance on available physiological signal data restricts its applicability across all clinical scenarios. Future efforts should focus on refining algorithms to expand diagnostic capabilities and broaden their clinical applications.
Beyond diagnostic applications, the long-term convenience of wearable devices offers a unique opportunity to explore their role in remote follow-up management of OSA. For example, their potential in remote monitoring and management following continuous positive airway pressure (CPAP) therapy merits further investigation.34,35 Such advancements could substantially improve patient outcomes and optimize OSA management.
In future studies, we plan to collaborate with healthcare providers and community organizations to recruit a more representative sample, including older individuals, women, and those less familiar with technology, to address the current demographic limitations and enhance the generalizability of our findings.
Conclusion
We employed PPG-based smart wearable devices for extensive OSA screening among Chinese smart wearable consumers, confirming their real-world effectiveness. Our study revealed significant underdiagnosis of OSA in the Chinese population and identified a heightened risk of cardiac arrhythmia in OSA patients and high-risk individuals. These findings underscore the need for comprehensive screening and targeted interventions to manage OSA and its associated cardiovascular comorbidities.
Data Sharing Statement
The data supporting this study’s findings are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Statement
This study was performed according to the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of the Chinese PLA General Hospital (Approval No. S2017-105-02). All participants provided online informed consent in the study application.
Acknowledgment
HUAWEI provided the algorithm model research platform and data for research purposes. Generative AI was not employed in the full process of manuscript preparation.
Author Contributions
Yibing Chen contributed to conceptualization, formal analysis, writing – original draft, project administration, and visualization; Hui Zhang participated in methodology design; Jing Li and Peida Xu (HUAWEI) were responsible for data curation, software programming, and visualization; Yutao Guo and Lixin Xie supervised the study, contributed to funding acquisition and writing – review & editing. All authors have read and approved the final manuscript. All authors contributed to the analysis, drafting, and revising of the article, agreed on the journal for submission, and agreed to be accountable for all aspects of the work.
Funding
This study was financially supported by the China Key Scientific Grant (Grant No. 2021YFC0122500). It mainly supported the remote follow-up information collection of smart device consumers and the paper submission and publishing process.
Disclosure
All authors declare that there are no conflicts of interest to report. The authors affiliated with “HUAWEI Device Co., Ltd.” have no financial or non-financial interests that could be perceived as influencing the work reported in this paper. HUAWEI Device Co., Ltd provided the algorithm and related physiological data for screening and detecting OSA and arrhythmia, all consumer information was anonymous on the research platform.
References
1. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/S2213-2600(19)30198-5
2. Mehra R, Chung MK, Olshansky B, et al. American heart association electrocardiography and arrhythmias committee of the council on clinical cardiology; and stroke council. sleep-disordered breathing and cardiac arrhythmias in adults: mechanistic insights and clinical implications: a scientific statement from the American heart association. Circulation. 2022;CIR0000000000001082.
3. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American heart association. Circulation. 2021;144(3):e56–e67. doi:10.1161/CIR.0000000000000988
4. Cadby G, McArdle N, Briffa T, et al. Severity of OSA is an independent predictor of incident atrial fibrillation hospitalization in a large sleep-clinic cohort. Chest. 2015;148(4):945–952. doi:10.1378/chest.15-0229
5. Mehra R, Benjamin EJ, Shahar E, et al. Sleep heart health study. association of nocturnal arrhythmias with sleep-disordered breathing: the sleep heart health study. Am J Respir Crit Care Med. 2006;173(8):910–916. doi:10.1164/rccm.200509-1442OC
6. Monahan K, Storfer-Isser A, Mehra R, et al. Triggering of nocturnal arrhythmias by sleep-disordered breathing events. J Am Coll Cardiol. 2009;54(19):1797–1804. doi:10.1016/j.jacc.2009.06.038
7. Teo YH, Han R, Leong S, et al. Prevalence, types and treatment of bradycardia in obstructive sleep apnea - A systematic review and meta-analysis. Sleep Med. 2022;89:104–113. doi:10.1016/j.sleep.2021.12.003
8. Gami AS, Hodge DO, Herges RM, et al. Obstructive sleep apnea, obesity, and the risk of incident atrial fibrillation. J Am Coll Cardiol. 2007;49(5):565–571. doi:10.1016/j.jacc.2006.08.060
9. Namtvedt SK, Randby A, Einvik G, et al. Cardiac arrhythmias in obstructive sleep apnea (from the Akershus Sleep Apnea Project). Am j Cardiol. 2011;108(8):1141–1146. doi:10.1016/j.amjcard.2011.06.016
10. Chiang AA, Jerkins E, Holfinger S, et al. OSA diagnosis goes wearable: are the latest devices ready to shine? J Clin Sleep Med. 2024;20(11):1823–1838. doi:10.5664/jcsm.11290
11. Papini GB, Fonseca P, van Gilst MM, Bergmans JWM, Vullings R, Overeem S. Wearable monitoring of sleep-disordered breathing: estimation of the apnea-hypopnea index using wrist-worn reflective photoplethysmography. Sci Rep. 2020;10(1):13512. doi:10.1038/s41598-020-69935-7
12. Chen Y, Wang W, Guo Y, Zhang H, Chen Y, Xie L. A single-center validation of the accuracy of a photoplethysmography-based smartwatch for screening obstructive sleep apnea. Nat Sci Sleep. 2021;13:1533–1544. doi:10.2147/NSS.S323286
13. Perez MV, Mahaffey KW, Hedlin H, et al. Apple Heart Study Investigators. Large-scale assessment of a smartwatch to identify atrial fibrillation. N Engl J Med. 2019;381(20):1909–1917. doi:10.1056/NEJMoa1901183
14. Lubitz SA, Faranesh AZ, Selvaggi C, et al. Detection of atrial fibrillation in a large population using wearable devices: the fitbit heart study. Circulation. 2022;146(19):1415–1424. doi:10.1161/CIRCULATIONAHA.122.060291
15. Guo Y, Wang H, Zhang H, et al. MAFA II investigators. mobile photoplethysmographic technology to detect atrial fibrillation. J Am Coll Cardiol. 2019;74(19):2365–2375. doi:10.1016/j.jacc.2019.08.019
16. Zhang X, Tianbao L, Zhengyu G, et al., Medical electrical equipment - Basic safety and main performance specific requirement of medical pulse oximeter equipment. YY0784-2010, 2010. Standards Press of China.
17. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504. doi:10.5664/jcsm.6506
18. Zhang H, Zhang J, Li HB, et al. Validation of single centre pre-mobile atrial fibrillation apps for continuous monitoring of atrial fibrillation in a real-world setting: pilot cohort study. J Med Internet Res. 2019;21(12):e14909. doi:10.2196/14909
19. Tuomilehto H, Seppä J, Uusitupa M. Obesity and obstructive sleep apnea--clinical significance of weight loss. Sleep Med Rev. 2013;17(5):321–329. doi:10.1016/j.smrv.2012.08.002
20. Natsios G, Pastaka C, Vavougios G, et al. Age, body mass index, and daytime and nocturnal hypoxia as predictors of hypertension in patients with obstructive sleep apnea. J Clin Hypertens. 2016;18(2):146–152. doi:10.1111/jch.12645
21. Zheng M, Wang X, Ge S, et al. Allergic and nonallergic rhinitis are common in obstructive sleep apnea but not associated with disease severity. J Clin Sleep Med. 2017;13(08):959–966. doi:10.5664/jcsm.6694
22. Fuller D, Colwell E, Low J, et al. Reliability and validity of commercially available wearable devices for measuring steps, energy expenditure, and heart rate: systematic review. JMIR mHealth uHealth. 2020;8(9):e18694. doi:10.2196/18694
23. Lubitz SA, Faranesh AZ, Selvaggi C, et al. Detection of Atrial Fibrillation in a Large Population Using Wearable Devices: The Fitbit Heart Study. Circulation. 2022;146(19):1415–1424. Epub 2022 Sep 23. doi:10.1161/CIRCULATIONAHA.122.060291IF
24. Binici Z, Intzilakis T, Nielsen OW, Kober L, Sajadieh A. Excessive supraventricular ectopic activity and increased risk of atrial fibrillation and stroke. Circulation. 2010;121(17):1904–1911. doi:10.1161/CIRCULATIONAHA.109.874982
25. Suzuki S, Sagara K, Otsuka T, et al. Usefulness of frequent supraventricular extrasystoles and a high CHADS2 score to predict first-time appearance of atrial fibrillation. Am J Cardiol. 2013;111(11):1602–1607. doi:10.1016/j.amjcard.2013.01.335
26. Dewland TA, Vittinghoff E, Mandyam MC, et al. Atrial ectopy as a predictor of incident atrial fibrillation: a cohort study. Ann Intern Med. 2013;159(11):721–728. doi:10.7326/0003-4819-159-11-201312030-00004
27. Patel N, Donahue C, Shenoy A, Patel A, El-Sherif N. Obstructive sleep apnea and arrhythmia: a systemic review. Int J Cardiol. 2017;228:967–970. doi:10.1016/j.ijcard.2016.11.137
28. Simantirakis EN, Schiza SI, Marketou ME, et al. Severe bradyarrhythmias in patients with sleep apnoea: the effect of continuous positive airway pressure treatment: a long-term evaluation using an insertable loop recorder. Eur Heart J. 2004;25(12):1070–1076. doi:10.1016/j.ehj.2004.04.017
29. Tan JWC, Leow LC, Wong S, et al. Asian pacific society of cardiology consensus statements on the diagnosis and management of obstructive sleep apnoea in patients with cardiovascular disease. Eur Cardiol. 2022;17:e16. doi:10.15420/ecr.2021.59
30. Fan YY, Li YG, Li J, et al. Diagnostic performance of a smart device with photoplethysmography technology for atrial fibrillation detection: pilot study (Pre-mAFA II Registry). JMIR mHealth uHealth. 2019;7(3):e11437. doi:10.2196/11437
31. Zinchuk A, Yaggi HK. Phenotypic subtypes of OSA: a challenge and opportunity for precision medicine. Chest. 2020;157(2):403–420. doi:10.1016/j.chest.2019.09.002
32. Javaheri S, Javaheri S. Update on persistent excessive daytime sleepiness in OSA. Chest. 2020;158(2):776–786. doi:10.1016/j.chest.2020.02.036
33. Sweetman A, Lack L, McEvoy RD, et al. Bi-directional relationships between co-morbid insomnia and sleep apnea (COMISA). Sleep Med Rev. 2021;60:101519. doi:10.1016/j.smrv.2021.101519
34. Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of adult obstructive sleep apnea with positive airway pressure: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2019;15(2):335–343. doi:10.5664/jcsm.7640
35. Bruyneel M. Telemedicine in the diagnosis and treatment of sleep apnoea. Eur Respir Rev. 2019;28(151):180093. doi:10.1183/16000617.0093-2018
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.