")
Back to Journals » Infection and Drug Resistance » Volume 18
Seroprevalence and Clinical Insights of Ocular Herpesvirus Infections: A Cross-Sectional Study Evaluating ELISA as a Diagnostic Tool
Authors Chen S , Peng Q, Wang H, Xie J, Cao H, Xu X
Received 8 March 2025
Accepted for publication 5 June 2025
Published 19 June 2025 Volume 2025:18 Pages 3063—3070
DOI https://doi.org/10.2147/IDR.S527047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Siyuan Chen,1,* Qi Peng,1,* Hailuo Wang,1 Jinglin Xie,1 He Cao,2 Xiaohong Xu1
1Department of Ophthalmology, Air Force Hospital of Eastern Theater Command, Nanjing, Jiangsu, 210002, People’s Republic of China; 2Department of Ophathalmology, Shenzhen People’s Hospital, Southern University of Science and Technology; The second Clinical Medical College, Jinan University, Shenzhen, 518020, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohong Xu, Department of Ophthalmology, Air Force Hospital of Eastern Theatre Command, Nanjing, Jiangsu, 210002, People’s Republic of China, Email [email protected] He Cao, Department of Ophathalmology, Shenzhen People’s Hospital, Southern University of Science and Technology; The second Clinical Medical College, Jinan University, Shenzhen, 518020, People’s Republic of China, Email [email protected]
Aims and Objectives: Ocular infections caused by Herpes simplex virus (HSV) and Varicella-zoster virus (VZV) are major contributors to vision impairment worldwide, necessitating accurate and accessible diagnostic tools. This study aimed to investigate the seroprevalence of HSV and VZV infections in patients with suspected ocular infections and to evaluate associated risk factors.
Methods: We conducted a cross-sectional study using enzyme-linked immunosorbent assay (ELISA) to detect antibodies against HSV and VZV in patients with ocular symptoms. Serological data were stratified into IgG and IgM positivity to differentiate past from active infections. Serological data were stratified into IgG (indicative of past infection) and IgM (suggestive of active infection) positivity to differentiate past from active infections. A total of 200 patients were enrolled, and demographic and clinical data were collected, including age, history of ocular surgery, and immunosuppressive therapy.
Results: The overall seroprevalence for HSV was 14%, and for VZV, it was 9%. Age was a significant risk factor for both infections, with individuals over 50 years (mean age of 48.9 ± 13.8 years) showing increased seropositivity (p < 0.001). The predominant ocular manifestation for HSV was keratitis (69%), while VZV infections were most commonly associated with conjunctivitis (62%). We identified a strong association between ocular surgery and HSV/VZV seropositivity (p < 0.001), and immunosuppressive therapy was significantly linked with VZV seropositivity (p < 0.001).
Conclusion and Recommendations: ELISA-based antibody detection proved effective in identifying both past and active HSV and VZV infections. The findings highlight age, ocular surgery, and immunosuppressive therapy as key risk factors for these infections. Given the diagnostic limitations of ELISA, future studies should incorporate molecular diagnostics for enhanced accuracy. These findings support the use of ELISA for screening high-risk populations, although adjunct molecular testing may improve diagnostic accuracy. Early serological screening in high-risk patients could aid in the timely detection and management of ocular herpesvirus infections.
Keywords: herpes simplex virus, ocular herpesvirus, varicella-zoster virus, ELISA
Introduction
Ocular viral infections caused by HSV and VZV pose a significant global health burden, contributing to severe, sight-threatening complications such as keratitis, anterior uveitis, and retinitis.1 These infections are often mediated by the reactivation of latent viruses residing within the trigeminal or dorsal root ganglia, particularly under conditions of immunosuppression, psychological stress, or aging. HSV and VZV, both belonging to the Herpesviridae family,2 are known for their capacity to establish lifelong latency and recurrent reactivation, underscoring the importance of early and accurate diagnosis to minimize long-term complications and prevent irreversible vision loss.3 Globally, herpetic keratitis is one of the leading causes of infectious corneal blindness, with more than 1.8 million cases reported annually.4 HSV is responsible for a considerable proportion of ocular morbidity, with frequent recurrences complicating its long-term management. It has been estimated that HSV-related keratitis affects approximately 1.5 million people worldwide each year, with 40,000 cases progressing to severe visual impairment.5 VZV, the causative agent of Herpes zoster ophthalmicus (HZO), primarily affects older adults and immunocompromised individuals, leading to serious complications such as postherpetic neuralgia and progressive outer retinal necrosis.6 In China, the burden of ocular HSV and VZV infections is underreported, although hospital-based studies have noted increasing case rates in urban and elderly populations.7 This regional epidemiological gap underscores the importance of localized seroprevalence studies. The increasing incidence of these infections in ageing populations and among immunosuppressed individuals8—including organ transplant recipients and HIV patients—highlights the growing need for effective diagnostic strategies.9 Molecular diagnostic techniques, particularly polymerase chain reaction (PCR), have significantly advanced the ability to detect viral DNA with high sensitivity and specificity.10 Despite the high sensitivity of PCR, ELISA remains a cost-effective and accessible option in resource-limited settings, capable of identifying both past and current infections. ELISA is widely used for detecting virus-specific immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies, aiding in the differentiation between prior exposure and active infection.11 While PCR can confirm the presence of viral DNA in ocular fluids, it may not always be feasible in routine clinical practice, especially in primary healthcare settings where access to advanced molecular laboratories is restricted.12 Despite advancements in antiviral therapies, significant challenges remain in managing ocular herpesvirus infections. In ocular infections, drug delivery barriers and the tendency for recurrence complicate treatment outcomes. Standard antiviral agents such as acyclovir, valacyclovir, and ganciclovir have shown efficacy in reducing viral replication and disease severity, but emerging resistance and incomplete viral clearance necessitate adjunctive therapeutic approaches.13 Corticosteroids, often used in combination with antivirals, are essential in controlling inflammatory manifestations such as HSV-induced anterior uveitis; however, their optimal dosage and duration remain subjects of ongoing debate.14 Given the potential for recurrent and chronic disease courses, long-term prophylaxis with antiviral agents has been suggested for high-risk patients, yet evidence supporting standardized treatment regimens remains inconclusive.15 Epidemiological data on the prevalence of HSV and VZV ocular infections remain limited, particularly in developing regions where diagnostic accessibility is constrained. Seroprevalence studies can provide valuable insights into infection dynamics, aiding in public health planning and resource allocation. However, variations in diagnostic methods, population demographics, and healthcare infrastructure complicate direct comparisons across different geographic regions.16 Therefore, studies utilizing robust serological assays like ELISA are crucial to understanding the true burden of ocular herpesvirus infections and identifying at-risk populations. The present study aims to determine the prevalence of HSV and VZV in patients presenting with ocular infections by leveraging ELISA-based serological testing. By evaluating the sensitivity and specificity of ELISA in detecting virus-specific antibodies, we seek to underscore its clinical utility as a practical and accessible diagnostic tool. Additionally, we aim to analyse the association between viral seropositivity and potential risk factors, providing insights that may guide future diagnostic and therapeutic strategies for ocular herpesvirus infections.
Materials and Methods
All patient data were anonymized and handled in accordance with the Declaration of Helsinki. As patient consent to review medical records was not required by the Institutional Ethics Committee of Shenzhen People’s Hospital, confidentiality and privacy were strictly maintained throughout the study.
Study Design and Population
This cross-sectional study was conducted at the Shenzhen People’s Hospital, between June 2023 and June 2024. The study enrolled 586 patients aged 18–75 years who presented with clinical symptoms of ocular infections, including redness, pain, photophobia, conjunctival congestion, and visual disturbances. Patients with documented immunodeficiency disorders (eg, HIV/AIDS, primary immunodeficiency syndromes), recent antiviral therapy (within the last four weeks), or systemic herpesvirus infections (such as disseminated HSV/VZV infections) were excluded to minimize confounding factors affecting serological responses. The study was approved by the Institutional Ethics Committee of Shenzhen People’s Hospital, Shenzhen, China (Ethics Approval Number: 2024-598-01), and all procedures were conducted following the tenets of the Declaration of Helsinki. Written informed consent was waivered as the retrospective study by ethical committee.
Sample Collection and Processing
Tear fluid and conjunctival swab samples were collected from all participants under aseptic conditions using sterile Dacron swabs. For each patient, the conjunctival swab was taken from the inferior fornix of the affected eye, avoiding corneal contact to prevent epithelial trauma. Tear samples were collected using Schirmer strips placed in the lateral conjunctival sac for 5 minutes. All samples were immediately stored in sterile microcentrifuge tubes and transported on ice to the laboratory. Upon arrival, samples were aliquoted and stored at −20°C until serological testing.
ELISA Testing for HSV and VZV Antibodies
Commercially available enzyme-linked immunosorbent assay (ELISA) kits (HerpeSelect® ELISA, Focus Diagnostics, Cypress, CA, USA) were used to detect IgG and IgM antibodies specific to HSV and VZV in tear and conjunctival swab samples. While ELISA is practical and widely accessible, it cannot confirm active viral replication. Future studies combining ELISA with PCR are recommended for diagnostic confirmation. The assays were performed strictly according to the manufacturer’s protocol. Briefly, 100 µL of patient samples (diluted 1:100) were added to microplate wells pre-coated with viral antigens. The plates were incubated at 37°C for 30 minutes, followed by washing to remove unbound antibodies. A conjugated enzyme-linked secondary antibody was added, and the reaction was developed using a tetramethylbenzidine (TMB) substrate. Optical density (OD) values were measured at 450 nm using a microplate reader (BioTek ELx808, Agilent Technologies, USA). Results were interpreted based on predefined cut-off values provided by the manufacturer:
- IgG/IgM positive: OD ≥ cut-off threshold
- IgG/IgM negative: OD < cut-off threshold
For quality control, positive and negative control sera were included in each assay run to ensure assay reliability.
Statistical Analysis
Statistical analyses were performed using SPSS software (version XX; IBM Corp., Armonk, NY, USA). The prevalence of HSV and VZV infections was calculated as the proportion of patients testing positive for IgG and/or IgM antibodies. Continuous variables (eg, age) were expressed as mean ± standard deviation (SD) and compared between seropositive and seronegative groups using independent t-tests. Categorical variables were analysed using chi-square (χ²) tests to assess associations with HSV/VZV seropositivity. A p-value < 0.05 was considered statistically significant. To assess independent risk factors for HSV and VZV infections, multivariate logistic regression analysis was conducted, adjusting for age, gender, history of prior ocular surgery, and immunosuppressive status. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported for significant predictors.
Results
Demographics Characterisation
The study enrolled a total of 586 patients with a mean age of 48.9 ± 13.8 years, of whom 58% were female (n = 340) and 42% were male (n = 246). The most common clinical presentation was keratitis, observed in 65% of cases, followed by conjunctivitis (25%) and uveitis (10%) (Table 1). A comparison of the mean age between seropositive and seronegative groups revealed a statistically significant association between increasing age and HSV/VZV seropositivity (p < 0.01) (Table 1).
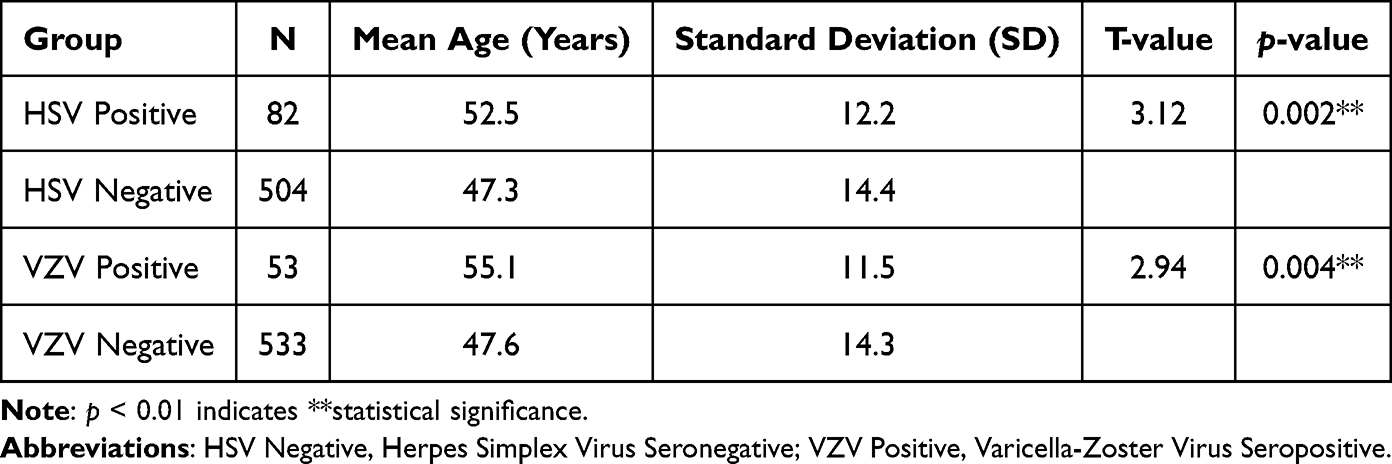 |
Table 1 T Test Results: HSV and VZV Seroprevalence |
Seroprevalence of HSV and VZV
Among the study participants, 82 patients (14%) tested positive for HSV-specific antibodies, whereas 53 patients (9%) tested positive for VZV-specific antibodies. Among HSV-positive cases, 62% (51 patients) had IgG antibodies, indicating prior exposure, while 38% (31 patients) had IgM antibodies, suggestive of recent or active infection. Similarly, among VZV-positive cases, 72% (38 patients) had IgG antibodies, and 28% (15 patients) had IgM antibodies, reflecting ongoing or recent viral activity (Figure 1). These findings suggest a significant burden of HSV and VZV infections in the study population, with a notable proportion presenting with active disease.
 |
Figure 1 Distribution of IgG and IgM Seropositivity in HSV and VZV Cases. |
Clinical Correlations
The majority of HSV-positive cases (69%) were associated with keratitis, followed by uveitis (20%) and conjunctivitis (11%). In contrast, VZV infections were more frequently observed in patients with conjunctivitis (62%), followed by keratitis (28%) and uveitis (10%). Patients with IgM seropositivity for either virus exhibited more severe clinical manifestations, including significant corneal involvement, epithelial damage, and visual impairment. These findings highlight the need for early diagnosis and intervention in cases of acute HSV and VZV infections.
Risk Factor Analysis
A chi-square analysis was conducted to assess the association between HSV/VZV seropositivity and various demographic and clinical risk factors (Table 2). Increasing age was significantly associated with both HSV and VZV infections, with patients older than 50 years being more likely to test positive (p < 0.001). Additionally, a history of ocular surgery was a strong predictor of both HSV and VZV positivity, suggesting that prior surgical interventions may predispose individuals to viral reactivation or increased susceptibility to infection. A significant association was observed between a history of shingles and both HSV (p = 0.001) and VZV (p < 0.001) seropositivity, reinforcing the link between prior herpesvirus infections and subsequent ocular complications. Furthermore, immunosuppressive therapy was strongly correlated with VZV infection (p<0.001), indicating that patients undergoing immunosuppressive treatment are at a higher risk for developing ocular VZV infections. However, the association between immunosuppressive therapy and HSV positivity was not statistically significant (p = 0.12) highlighting the distinct risk profiles for these two viruses. This study identified a significant burden of HSV and VZV infections among patients presenting with ocular symptoms. Age, prior ocular surgery, and a history of shingles were strongly correlated with HSV and VZV seropositivity, suggesting these as key risk factors for ocular herpesvirus infections. Immunosuppressive therapy emerged as a major risk factor for VZV positivity, but its association with HSV was not statistically significant. Additionally, IgM-positive patients presented with more severe ocular manifestations, emphasizing the need for timely clinical intervention. These findings underscore the importance of routine serological screening and targeted management strategies for high-risk individuals.
 |
Table 2 Chi-Square Test – Association Between HSV/VZV Seropositivity and Risk Factors |
Discussion
This study investigated the seroprevalence and risk factors associated with HSV and VZV infections in patients with suspected ocular infections using ELISA-based antibody detection. The overall HSV seroprevalence was 14%, while VZV seroprevalence was 9%, highlighting a substantial burden of ocular herpesvirus infections. These findings align with global epidemiological data, where HSV-related ocular disease remains a leading cause of corneal blindness, particularly in developing nations.17,18 Prior studies in China have reported HSV seroprevalence ranging from 10% to 18% in patients with ocular symptoms, with significant variations based on geographic location, sample type, and diagnostic methodology.19 Similarly, the 9% VZV prevalence observed in our study is consistent with prior reports from China,20 where VZV seroprevalence among ocular infection patients has ranged between 7% and 12%, with a higher burden observed in immunocompromised individuals.21 A notable finding in our study was the predominance of keratitis among HSV-positive patients (69%), followed by uveitis (20%) and conjunctivitis (11%). This may be attributed to differences in referral patterns, diagnostic focus, or geographic HSV strain variability.22 These regional variations could be attributed to differences in diagnostic approaches, patient demographics, and the inclusion criteria of prior studies. In contrast, VZV infections in our cohort were primarily associated with conjunctivitis (62%), whereas studies from other regions have reported a higher prevalence of VZV-associated keratitis and retinitis.23 The high prevalence of conjunctivitis in VZV-positive patients in our study suggests that milder presentations of VZV ocular infections might be more commonly detected when ELISA-based screening is employed, whereas severe cases (eg, necrotizing retinitis) are more frequently diagnosed via PCR-based methods.24
Our findings underscore the importance of age as a major risk factor for HSV and VZV seropositivity, with patients over 50 years significantly more likely to test positive (p < 0.001). These results align with global data, where HSV and VZV seropositivity rates increase with age due to cumulative viral reactivation events.5,25 Similar trends have been observed in Chinese cohorts, where older individuals exhibit a higher frequency of HSV-related keratitis and VZV-induced herpes zoster ophthalmicus.6 The strong association between a history of shingles and VZV seropositivity (p < 0.001) further supports prior evidence that ocular VZV infections often occur in patients with a history of systemic zoster outbreaks, reinforcing the need for early antiviral prophylaxis in high-risk individuals.26 A significant correlation was also observed between ocular surgery and HSV/VZV seropositivity, suggesting that prior surgical interventions may increase susceptibility to viral reactivation (p < 0.001). Previous research in China has highlighted ocular trauma and intraocular procedures as triggers for herpesvirus reactivation, particularly in patients with underlying asymptomatic viral latency.27 This is clinically relevant, as post-surgical HSV/VZV infections can lead to persistent inflammation, corneal scarring, and worsened visual outcomes, emphasizing the importance of preoperative screening and prophylactic antiviral therapy for patients with a known history of herpetic eye disease.
Another key observation in our study was the strong association between immunosuppressive therapy and VZV seropositivity (p< 0.001), while no statistically significant association was found with HSV (p = 0.12). This aligns with prior studies demonstrating that VZV is particularly opportunistic in immunosuppressed individuals, leading to severe ocular manifestations such as progressive outer retinal necrosis (PORN).28 Reports from China similarly indicate that patients undergoing corticosteroid or immunosuppressive therapy for autoimmune diseases exhibit a significantly higher incidence of ocular VZV infections, often requiring intensive antiviral treatment to prevent complications.29 The lack of statistical significance between immunosuppressive therapy and HSV seropositivity in our study suggests that HSV reactivation may be influenced more by local ocular factors than systemic immunosuppression, an area requiring further investigation. Despite its advantages, ELISA-based antibody detection has inherent limitations. While it is a cost-effective and widely accessible tool, it cannot distinguish between active and latent infections. This limitation was addressed in our study by stratifying results into IgG-positive (past infection) and IgM-positive (active infection) cases. However, PCR-based confirmation of viral DNA in ocular samples would have strengthened the diagnostic accuracy. Studies in China and globally have demonstrated that PCR-based detection of HSV and VZV in aqueous humor or tear samples provides superior specificity and sensitivity, particularly in early-stage infections.30 Future studies combining ELISA with PCR-based molecular diagnostics are recommended to confirm active infections and provide a more comprehensive understanding of ocular herpesvirus epidemiology and disease progression. The findings of this study underscore the clinical utility of ELISA in detecting both past and active HSV and VZV infections, especially in resource-limited settings where PCR may not be readily available. Routine ELISA screening among high-risk populations—such as the elderly, postsurgical patients, and immunosuppressed individuals—could facilitate earlier detection and more targeted management. Furthermore, given the high proportion of IgM-positive patients presenting with severe ocular manifestations, our results emphasize the importance of timely intervention to mitigate long-term visual complications.
Conclusion
This study provides valuable epidemiological insights into HSV and VZV ocular infections, demonstrating a high burden of disease and strong associations with age, ocular surgery, and immunosuppressive therapy. The use of ELISA as a diagnostic tool proved effective in detecting both past and active infections, though future studies should incorporate molecular confirmation methods for enhanced diagnostic precision. The results underscore the need for routine serological screening, risk stratification, and optimized treatment strategies for patients at high risk of ocular herpesvirus infections. Prophylactic antiviral therapy may be considered for elderly, immunosuppressed, or postsurgical patients, particularly in regions with high HSV/VZV seroprevalence, to prevent viral reactivation and related complications. Further research focusing on longitudinal patient follow-up, antiviral resistance patterns, and immunological responses could provide deeper insights into disease mechanisms and improved management approaches.
Data Sharing Statement
All data supporting the findings of this study are included in the manuscript. Additional data and materials will be made available upon reasonable request from the authors.
Ethical Approval
The study was approved by the Institutional Ethics Committee of Shenzhen People’s Hospital, Shenzhen, China (Ethics Approval Number: 2024-598-01), and all procedures were conducted following the tenets of the Declaration of Helsinki.
Publication Consent
Written informed consent was waivered as the retrospective study by ethical committee of Shenzhen People’s Hospital, Shenzhen, China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Litt J, Cunningham AL, Arnalich-Montiel F, Parikh R. Herpes zoster ophthalmicus: presentation, complications, treatment, and prevention. Infect Dis Ther. 2024;13(7):1439–1459. doi:10.1007/s40121-024-00990-7
2. Zheng C. The application of a herpes simplex virus Type I vector for transgenic therapy. Microbes Immun. 2025;2(2):16–33. doi:10.36922/mi.7947
3. Tayyar R, Ho D. Herpes simplex virus and varicella zoster virus infections in cancer patients. Viruses. 2023;15(2):439. doi:10.3390/v15020439
4. McCormick I, James C, Welton NJ, et al. Incidence of herpes simplex virus keratitis and other ocular disease: global review and estimates. Ophthalmic Epidemiol. 2022;29(4):353–362. doi:10.1080/09286586.2021.1962919
5. Farooq AV, Shukla D. Herpes simplex epithelial and stromal keratitis: an epidemiologic update. Surv Ophthalmol. 2012;57(5):448. doi:10.1016/j.survophthal.2012.01.005
6. John A, Canaday DH. Herpes zoster in the older adult. Infect Dis Clin N Am. 2017;31(4):811. doi:10.1016/j.idc.2017.07.016
7. Zheng B, Yin D, Geng Y, et al. Herpes zoster incidence and burden in older Chinese: a systematic review and meta-analysis. BMC Public Health. 2025;25:1494. doi:10.1186/s12889-025-22703-6
8. Shen Y, Zhao X, Chen L, et al. A modified HSV-1 oncolytic virus reconciles antiviral and antitumor immunity via promoting IFNβ expression and inhibiting PKR. Int J Biol Macromol. 2024;274:133297. doi:10.1016/j.ijbiomac.2024.133297
9. Engels EA. Epidemiologic perspectives on immunosuppressed populations and the immunosurveillance and immunocontainment of cancer. Am J Transplant. 2019;19(12):3223. doi:10.1111/ajt.15495
10. Yang S, Rothman RE. PCR-based diagnostics for infectious diseases: uses, limitations, and future applications in acute-care settings. Lancet Infect Dis. 2004;4(6):337–348. doi:10.1016/S1473-3099(04)01044-8
11. Alhajj M, Zubair M, Farhana A. Enzyme Linked Immunosorbent Assay. StatPearls [Internet]. StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555922/.
12. Sugita S, Takase H, Nakano S. Role of recent PCR tests for infectious ocular diseases: from laboratory-based studies to the clinic. Int J Mol Sci. 2023;24(9):8146. doi:10.3390/ijms24098146
13. Poole CL, James SH. Antiviral therapies for herpesviruses: current agents and new directions. Clin Ther. 2018;40(8):1282–1298. doi:10.1016/j.clinthera.2018.07.006
14. Pleyer U, Chee SP. Current aspects on the management of viral uveitis in immunocompetent individuals. Clin Ophthalmol. 2015;9:1017. doi:10.2147/OPTH.S60394
15. Vegivinti CTR, Evanson KW, Lyons H, et al. Efficacy of antiviral therapies for COVID-19: a systematic review of randomized controlled trials. BMC Infect Dis. 2022;22:107. doi:10.1186/s12879-022-07068-0
16. Bergeri I, Whelan MG, Ware H, et al. Global SARS-CoV-2 seroprevalence from January 2020 to April 2022: a systematic review and meta-analysis of standardized population-based studies. PLoS Med. 2022;19(11):e1004107. doi:10.1371/journal.pmed.1004107
17. Maple PA, Tanasescu R, Constantinescu CS, et al. Cytomegalovirus, Epstein-Barr virus, herpes simplex virus, and varicella zoster virus infection dynamics in people with multiple sclerosis from Northern Italy. Pathogens. 2024;13(6):499. doi:10.3390/pathogens13060499
18. Rani NA, Moin AT, Patil R, et al. Corrigendum: designing a polyvalent vaccine targeting multiple strains of varicella zoster virus using integrated bioinformatics approaches. Front Microbiol. 2024;15:1498557. doi:10.3389/fmicb.2024.1498557
19. Wang Y, Yan X, Ai W, et al. Disparities in burden of herpes simplex virus type 2 in China: systematic review, meta-analyses, and meta-regressions. Front Immunol. 2024;15:1369086. doi:10.3389/fimmu.2024.1369086
20. Wang L, Sun F, Liu S, et al. Seroprevalence of Varicella Zoster virus in China: an age-stratifed systematic review and meta-analysis. medRxiv. 2019:19009449. doi:10.1101/19009449
21. Xie G, Wei Q, Guo W, et al. An adult co-presented with varicella and herpes zoster caused by varicella zoster virus genotype J, China: a case report. BMC Infect Dis. 2020;20(1):454. doi:10.1186/s12879-020-05192-3
22. Qian Z, Fan H, Tao Y, Li W, Gu W. Herpetic anterior uveitis in a Chinese referral center: clinical manifestations and laboratory test results. Ocul Immunol Inflamm. 2020;28(5):758–763. doi:10.1080/09273948.2019.1619780
23. Yawn BP, Wollan PM, St Sauver JL, Butterfield LC. Herpes Zoster--eye complications: rates and trends. Mayo Clin Proc. 2013;88(6):562–570. doi:10.1016/j.mayocp.2013.03.014
24. Grassmeyer JJ, Bellsmith KN, Bradee AR, Pegany RB, Redd TK. Conjunctival lesions secondary to systemic varicella zoster virus infection. Cornea Open. 2023;2(4):e0022. doi:10.1097/coa.0000000000000022
25. Harbecke R, Oxman MN, Selke S, et al. Prior herpes simplex virus infection and the risk of herpes zoster. J Infect Dis. 2023;229(1):64–72. doi:10.1093/infdis/jiad259
26. Fishman A, Ward J, Pescatore R. For your eyes only, herpes zoster ophthalmicus case study. Rowan-Virtua Research Day. 2019. Available from: https://rdw.rowan.edu/stratford_research_day/2019/may2/16.
27. Itzhaki RF. Corroboration of a major role for herpes simplex virus type 1 in Alzheimer’s disease. Front Aging Neurosci. 2018;10:324. doi:10.3389/fnagi.2018.00324
28. Ahmed S, Lauran M, Ugwoke A, Walton T, Holroyd C, Galloway J. The relationship between Zoster serology, vaccination uptake and infection rates: a single-centre cross-sectional study. Rheumatol Adv Pract. 2024;8(4):rkae127. doi:10.1093/rap/rkae127
29. Chen LK, Arai H, Chen LY, et al. Looking back to move forward: a twenty-year audit of herpes zoster in Asia-Pacific. BMC Infect Dis. 2017;17(1):213. doi:10.1186/s12879-017-2198-y
30. Weidmann M, Meyer-König U, Hufert FT. Rapid detection of herpes simplex virus and varicella-zoster virus infections by real-time PCR. J Clin Microbiol. 2003;41(4):1565–1568. doi:10.1128/JCM.41.4.1565-1568.2003
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.