")
Back to Journals » International Journal of General Medicine » Volume 17
Serum Lipoprotein(a) as Predictive Factor for Early Neurological Deterioration of Acute Ischemic Stroke After Thrombolysis
Authors Wang R, Kong W, Zhang W
Received 25 June 2024
Accepted for publication 22 August 2024
Published 31 August 2024 Volume 2024:17 Pages 3791—3798
DOI https://doi.org/10.2147/IJGM.S475767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Ruiming Wang, Weiguo Kong, Wenhua Zhang
Department of Neurology, Hangzhou Traditional Chinese Medicine Hospital Affiliated to Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
Correspondence: Wenhua Zhang, Department of Neurology, Hangzhou Traditional Chinese Medicine Hospital affiliated to Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China, Tel +86-571-85827888, Fax +86-571-85119481, Email [email protected]
Objective: This study aimed to explore the relationship between serum lipoprotein(a) (LP(a)) levels and early neurological deterioration (END) in patients with acute ischemic stroke (AIS) after thrombolysis.
Methods: In total, 236 patients with AIS after thrombolysis were enrolled in this study. Serum LP(a) levels were measured on admission after thrombolysis. END was defined as an increase of at least two points in the NIHSS score within 48 hours after thrombolysis. Binary logistic regression analysis was used to assess the association between serum LP(a) levels and END.
Results: Overall, patients with END had higher LP(a) than those without END (high LP(a): 38.3% vs 22.2%, intermediate LP(a): 40.3% vs 41.8%, low LP(a): 21.3% vs 36.0%, p< 0.005). In the multivariate analysis, high LP(a) (defined as LP(a) level≥ 300 mg/L) was an independent risk factor for END post-thrombolysis (OR=3.154, 95% CI=1.067– 9.322, p=0.038).
Conclusion: Our findings demonstrated that LP(a) was an independent risk factor for END post-thrombolysis and that LP(a) level≥ 300 mg/L could be associated with END post-thrombolysis in this study population.
Keywords: Lipoprotein(a), early neurological deterioration, acute ischemic stroke, thrombolysis
Introduction
Acute ischemic stroke (AIS) remains a leading cause of disability and mortality globally.1 Although thrombolysis provides an opportunity to recover cerebral blood flow and perfusion,2 the outcomes after thrombolysis are not always positive in all patients. Some AIS patients still suffer from early neurological deterioration (END) even after thrombolysis, which could lead to poor clinical outcomes.3 Besides obvious causes like intracerebral hemorrhage and malignant edema, previous study suggested female sex, hypertension, diabetes, and smoking, were associated with END.4 In clinical practice, treating END may involve strategies such as plasma volume expansion, induced hypertension and enhanced antithrombotic therapy, though none have been definitively validated to date.5 Recent research has shown that the use of argatroban and tirofiban could be helpful in the prevention of END in AIS.5,6 Therefore, it is important to explore the risk factors of END to facilitate early intervention.
The pathophysiological mechanism of END post-thrombolysis remains unclear; some reports suggest that hemodynamic changes due to thrombus extension could be a possible cause.7 Lipoprotein(a) [LP(a)] is associated with the occurrence, recurrence, and prognosis of AIS.8,9 Research has suggested that elevated serum LP(a) level are associated with inflammation, atherosclerosis, and thrombus formation,10 suggesting a possible link between LP(a) and the mechanisms underlying END post-thrombolysis. However, the relationship between LP(a) levels and risk of END post-thrombolysis remains unknown.
By researching this relationship, our study aimed to identify the role of LP(a) as a predictive biomarker for END, offering insights into the pathophysiological mechanisms of END post-thrombolysis, and potential strategies to reduce this risk.
Method
Subjects
This was a single-center observational study. AIS was diagnosed according to criteria set forth by the World Health Organization. Consecutive patients with AIS who were admitted to our hospital with voluntary participation in this study were enrolled between February 2021 to November 2023. The inclusion criteria were as follows: (1) age ≥18 years; (2) thrombolysis treatment (alteplase, 0.9 mg/kg up to a maximum of 90 mg, 10% of the total dosage as a bolus, and the rest for 1 hour); (3) blood samples collected within the first 24 h following the onset of stroke; (4) completed computed tomography (CT) /magnetic resonance imaging (MRI) scans to confirm the diagnosis. The exclusion criteria were as follows: (1) patients without laboratory test data; (2) endovascular interventions; (3) patients with severe chronic diseases or cancer before stroke onset.
Ethics Statement
All subjects provided written informed consent prior to the study, and the protocols were approved by the ethics committee of the Hangzhou Traditional Chinese Medicine Hospital affiliated to Zhejiang Chinese Medical University. All clinical investigations were conducted in accordance with the principles of the Declaration of Helsinki.
Clinical and Laboratory Data Collection
Demographic and clinical data were collected for all enrolled patients, including sex, age, history of smoking, history of drink, hypertension, diabetes mellitus, atrial fibrillation, and previous stroke. Timing data for the thrombolysis procedure were also recorded. Stroke severity was assessed using the National Institutes of Health Stroke Scale (NIHSS), and stroke etiology was determined using the modified Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification. Treatment during hospitalization was followed the guidelines established by the American Heart Association and the American Stroke Association. These data were also registered on the Zhejiang Stroke Medical Quality Control Center Platform, an academic institution that monitors the quality of all reperfusion therapy cases performed at stroke centers in hospitals in Zhejiang Province, China.11
END was defined as an at least 2 points increase in the NIHSS score by at least two points within 48 h post-thrombolysis.6 LP(a) was measured using an immunoturbidimetric method with blood samples drawn after a 12-hour overnight fasting period after thrombolysis at admission.12 According to previous studies,13,14 low LP(a) was defined as LP(a)< 100 mg/L, intermediate LP(a) as 300 mg/L >LP(a)≥100 mg/L, and High LP(a) as LP(a)≥ 300 mg/L.
Statistical Analysis
Statistical analyses were performed using the SPSS software version 22 (IBM Corporation). All analyses were blinded to the participants’ identification information. Measurement data with a normal distribution were described as mean ± standard deviation, measurement data with a non-normal distribution were described as median and interquartile range, and count data were described as the number of cases and percentages. In univariate analysis for comparison between two groups, independent samples t-test was used for measurement variables with normal distribution, non-parametric test was used for measurement data with non-normal distribution, and the chi-square test was used for count data. In the multivariate analysis, binary logistic regression analysis was used with sex, age, and variables with p<0.2 in the univariate analysis in the model. Statistical significance was accepted at the 0.05 level (two-tailed).
Results
A total of 236 patients were included; detailed patient enrollment was shown in Figure 1. No participants died during the follow up. There were no statistical differences between the clinical characteristics of included and excluded subjects.
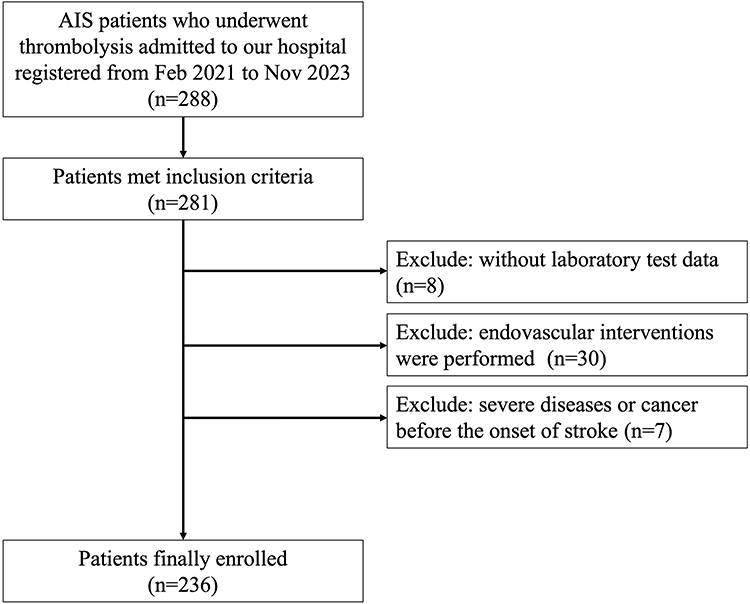 |
Figure 1 The patient flowchart. |
Subject Characteristics
79 (33.5%) patients were female, and the average age was 68.75±14.15 years old. The average level of LP(a) was 277.63±287.96 mg/L.47 (19.9%) patients experienced END. A detailed distribution of LP(a) was shown in Figure 2. 78 (33.1%) were low LP(a) with an average LP(a) level of 52.89±21.87 mg/L, 98 (41.5%) were intermediate LP(a) with an average LP(a) level of 176.87±54.56 mg/L and 60 (25.4%) were high LP(a) with an average LP(a) level of 572.32±301.85 mg/L. Detailed characteristics of the participants according to LP level (a) were presented in Table 1. Except for hypertension (56 (71.8%) vs 76 (77.6%) vs 35 (58.3%), p=0.038), SVO (31 (39.7%) vs 26 (26.5%) vs 12 (20.0%), p=0.032), LDL (2.56±0.87 vs 2.94±0.91 vs 2.91±1.05, p=0.023), and END (10 (12.8%) vs 19 (19.4%) vs 18 (30.0%), p=0.047), there were no statistical differences for other variables between the three groups with different levels of LP(a).
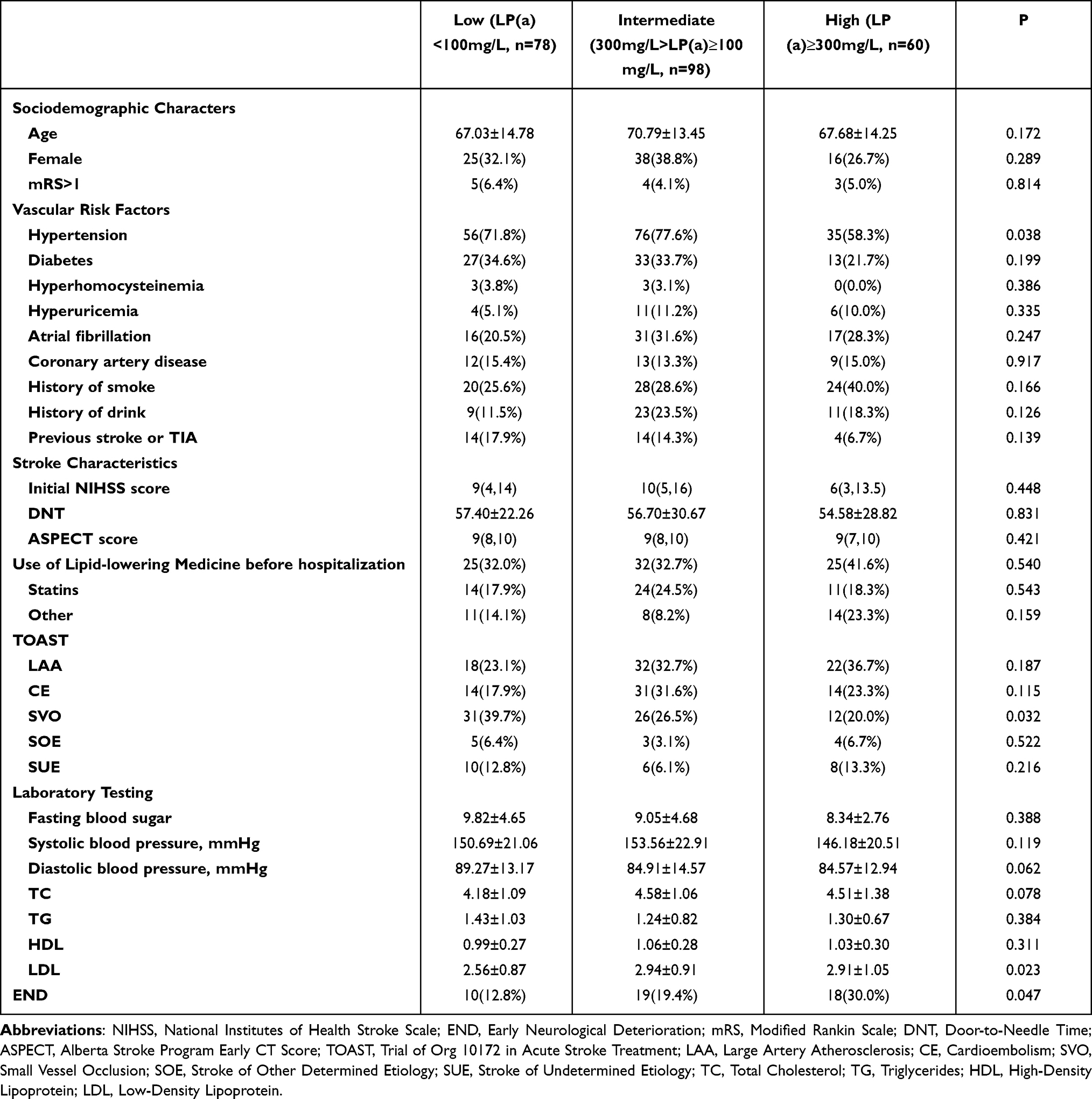 |
Table 1 Characteristics of Participants According to the Level of LP(a) |
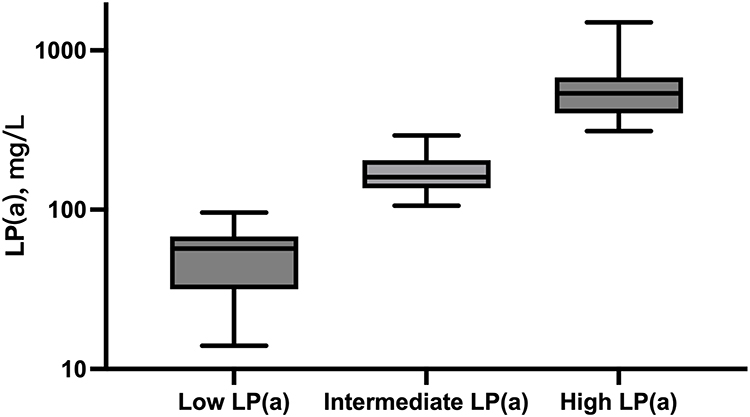 |
Figure 2 Distributions of LP(a). |
Univariate Comparison Between END Group and No END Group
As shown in Table 2, patients with END had more SUE (10 (21.3%) vs 14 (7.4%), p=0.012) and higher LDL (3.18±1.04 vs 2.72±0.91, p=0.005) than those without END. As shown in Figure 3, significant differences in LP(a) levels were observed between the two groups according to the END. There were no other statistically significant differences between the two groups.
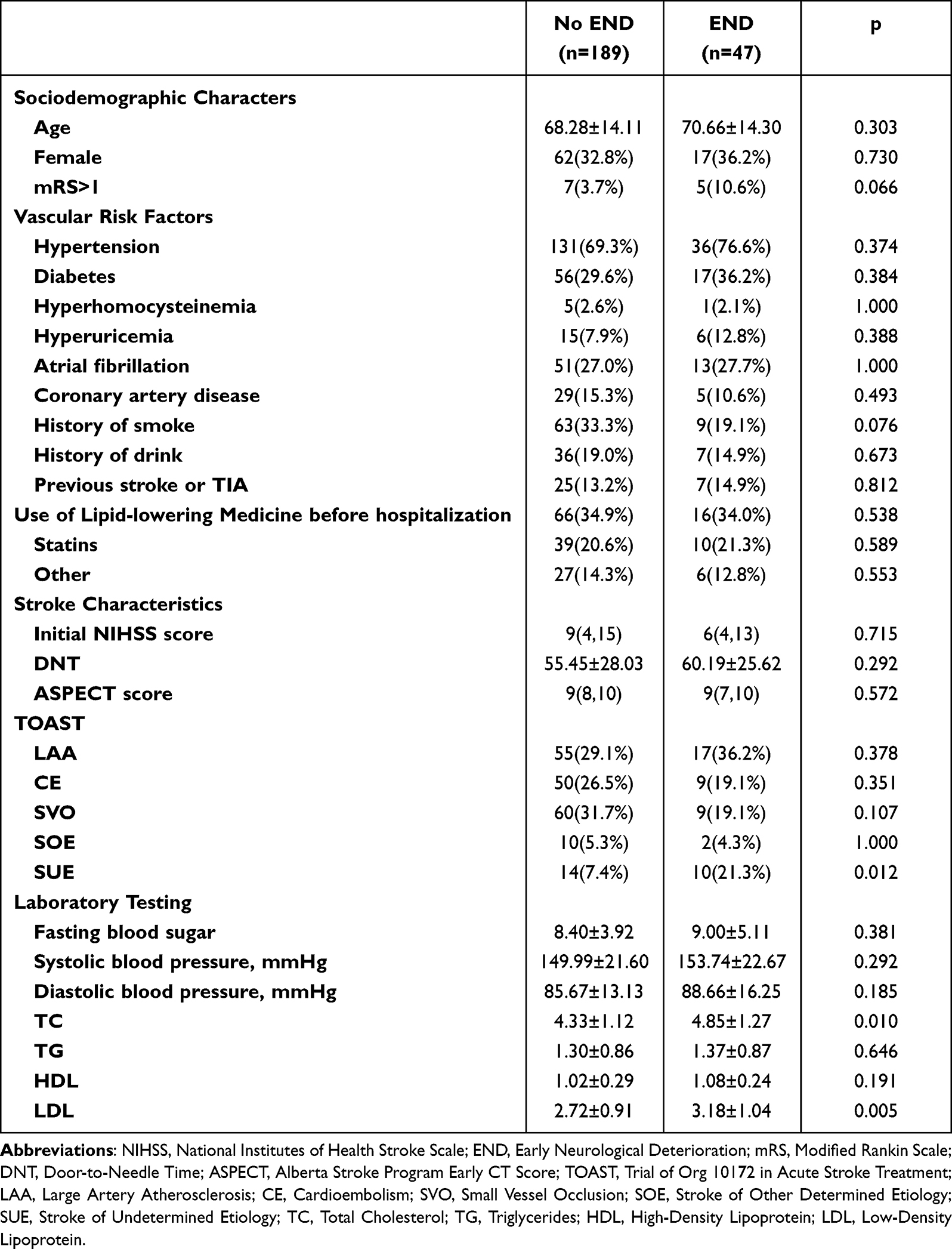 |
Table 2 Characteristics of Participants According to END |
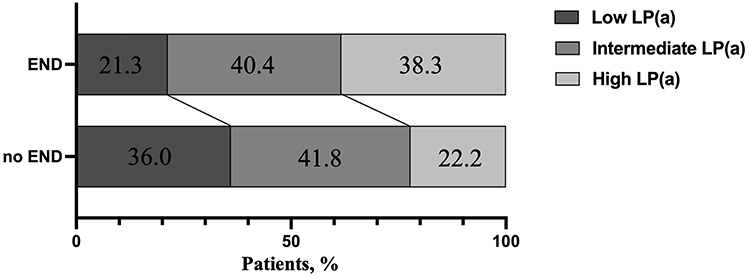 |
Figure 3 Distributions of LP(a) according to END. |
Binary Logistic Regression of Serum Level of LP(a) for END
As Figure 4 shows, after adjusting for age, sex, mRS>1 before onset, history of smoke, SVO, SUE, TC, HDL, LDL, and diastolic blood pressure, High LP(a) (OR=3.154, 95% CI=1.067–9.322, p=0.038) was an independent risk factor for END post-thrombolysis (reference to Low LP(a)).
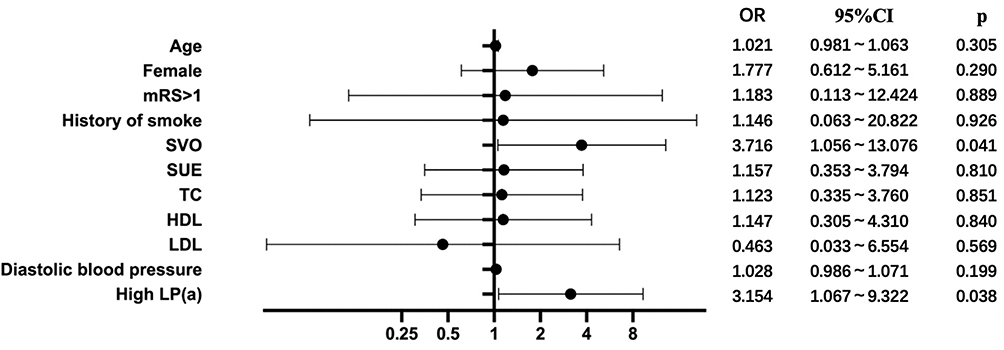 |
Figure 4 Forest plots of binary logistic regression of serum level of LP(a) for END. |
Discussion
The main findings of this study were that the LP(a) level was an independent risk factor for END post-thrombolysis and LP(a) ≥ 300 mg/L was associated with END post-thrombolysis in this study population.
Our findings were consistent with previous study. A previous study demonstrated that serum lipoprotein-associated phospholipase A2 (Lp-PLA2), which binds to lipoproteins in peripheral blood circulation, was associated with END (defined as an increase in the NIHSS score within 10 days after admission) in AIS patients with the TOAST subtype of large arterial atherosclerosis (LAA).15 Our study further confirmed that LP(a) levels were associated with END post-thrombolysis in patients with AIS within 48 h, which could be helpful for early diagnosis and therapy.
The underlying mechanisms of END post-thrombolysis are multifaceted, including reperfusion injury, secondary collateral dysfunction, and extension of thrombus.7 This result is biologically reasonable, considering the roles of LP(a) in ischemic stroke. The apo(a) component of LP(a) shares high homology with plasminogen (PLG) and competes with PLG receptors, thereby interfering with the conversion of PLG to plasmin, blocking fibrin clot dissolution, and promoting thrombus formation.16 What’s more, LP(a) regulates fibrinolysis and promotes thrombus formation by competitively inhibiting tissue plasminogen activator (tPA) via competition with plasminogen activator inhibitor 1 (PAI-1) and PLG.17 Additionally, elevated LP(a) levels can impair platelet function.18 Furthermore, overexpression of the tissue factor pathway inhibitor (TFPI) weakens thrombus formation,19 whereas LP(a) can promote thrombus formation by binding to TFPI through its apo(a) component, leading to TFPI inactivation.20 Therefore, we believe that LP(a) causes END by promoting the progression of arterial thrombus. Moreover, LP(a) promotes inflammation by interacting with inflammatory factors and recruiting inflammatory cells to atherosclerotic plaques, exacerbating atherosclerosis.21,22 Given the critical role of inflammation and atherosclerosis in ischemic stroke, LP(a) may contribute to END by promoting inflammation and atherosclerosis.
Our study carries substantial clinical significance. Our findings suggest that serum LP(a) level is a predictive factor for END post-thrombolysis in AIS. Reducing serum LP(a) to a certain level may prevent END and the poor short-term functional outcomes of thrombolysis. Besides, our study also provides potential targets for therapeutic intervention to improve the outcomes of patients with AIS patients with END. However, this hypothesis should be validated in future studies.
Our study had several limitations. First, this was a single-center prospective study with a small sample size, and further research with larger cohorts and follow-up is required in the future, especially in extremely elderly population since the demographics and risk factors are quite different in this age segment.23 Second, our study did not include laboratory animal experiments to explore the mechanistic pathways underlying the association between apolipoproteins and intracranial pathophysiological changes after thrombosis. Third, no intervention was performed on LP(a) for comparison, which requires further clinical trial. Fourth, due to the exclusion of thrombectomy, some severe cases with large vessel occlusion were not included, which may have led to a bias in the study population. Fifth, our study did not stratify patients based on the cerebral artery territory involved. Since the stroke location could affect prognosis,24 future studies could benefit from considering the topography of cerebral infarcts to see if the predictive value of LP(a) varies by stroke location.
Conclusion
In summary, our study found that serum LP(a) level was an independent factor for END post-thrombolysis, and it could be reasonable to control the LP(a) level below 300 mg/L to avoid END, offering insights into the pathophysiological mechanisms of END post-thrombolysis, and potential strategies to reduce this risk. Future research could explore interventions targeting LP(a) reduction to assess if this decreases the risk of END. Additionally, studying the interaction of LP(a) with other biomarkers of inflammation and thrombosis in diverse populations could provide further insights into the pathophysiology of END.
Data Sharing Statement
The data presented in this manuscript were acquired for this study. Due to privacy issues, it is not available to the community via an open repository. The datasets generated in this study are available from the corresponding author upon reasonable request. Considerations are made based on a review of the reasons for requesting data and procedures to ensure data privacy.
Funding
This work was supported by the Zhejiang Provincial Traditional Chinese Medicine Science and Technology Project (2021ZA102) and The Fifth Batch of National Traditional Chinese Medicine Excellent Clinical Talents Training Project (Announcement from the Personnel and Education Department of the National Administration of Traditional Chinese Medicine. No. 2022-1).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ding Q, Liu S, Yao Y, Liu H, Cai T, Han L. Global, Regional, and National Burden of Ischemic Stroke, 1990-2019. Neurology. 2022;98(3):e279–e290. doi:10.1212/WNL.0000000000013115
2. Phipps MS, Cronin CA. Management of acute ischemic stroke. BMJ. 2020;368(l6983). doi:10.1136/bmj.l6983
3. Simonsen CZ, Schmitz ML, Madsen MH, et al. Early neurological deterioration after thrombolysis: clinical and imaging predictors. Int J Stroke. 2016;11(7):776–782. doi:10.1177/1747493016650454
4. Werring D, Ozkan H, Doubal FN, et al. Early neurological deterioration in acute lacunar ischaemic stroke: systematic review of incidence, mechanisms, and prospects for treatment. Int J Stroke. 2024. doi:10.1177/17474930241273685
5. Zhao W, Li S, Li C, et al. Effects of tirofiban on neurological deterioration in patients with acute ischemic stroke: a randomized clinical trial. JAMA Neurol. 2024;81(6):594. doi:10.1001/jamaneurol.2024.0868
6. Zhang X, Zhong W, Xue R, et al. Argatroban in patients with acute ischemic stroke with early neurological deterioration: a randomized clinical trial. JAMA Neurol. 2024;81(2):118–125. doi:10.1001/jamaneurol.2023.5093
7. Seners P, Hurford R, Tisserand M, et al. Is Unexplained early neurological deterioration after intravenous thrombolysis associated with thrombus extension? Stroke. 2017;48(2):348–352. doi:10.1161/STROKEAHA.116.015414
8. Lange KS, Nave AH, Liman TG, Grittner U, Endres M, Ebinger M. Lipoprotein(a) levels and recurrent vascular events after first ischemic stroke. Stroke. 2017;48(1):36–42. doi:10.1161/STROKEAHA.116.014436
9. Nave AH, Lange KS, Leonards CO, et al. Lipoprotein (a) as a risk factor for ischemic stroke: a meta-analysis. Atherosclerosis. 2015;242(2):496–503. doi:10.1016/j.atherosclerosis.2015.08.021
10. Di Fusco SA, Maggioni AP, Scicchitano P, Zuin M, E D, Colivicchi F. Lipoprotein (a), inflammation, and atherosclerosis. J Clin Med. 2023;12(7):2529. doi:10.3390/jcm12072529
11. Pan X, Pei Y, Zhang M, et al. Association of atrial fibrillation with remote intracerebral hemorrhage after intravenous thrombolysis: results from a multicenter study in China. Neurol Ther. 2024;13(1):127–139. doi:10.1007/s40120-023-00563-9
12. Petersen NH, Schmied AB, Zeller JA, Plendl H, Deuschl G, Zunker P. Lp(a) lipoprotein and plasminogen activity in patients with different etiology of ischemic stroke. Cerebrovasc Dis. 2007;23(2–3):188–193. doi:10.1159/000097640
13. Cinzia F, Daniela P, Elena S, et al. Lipoprotein (a) [Lp(a)]: a possible link between migraine and stroke. Transl Res. 2009;153(1):44–47. doi:10.1016/j.trsl.2008.11.001
14. Murase T, Okubo M, Amemiya-Kudo M, et al. Impact of markedly elevated serum lipoprotein(a) levels (> or = 100 mg/dL) on the risk of coronary heart disease. Metabolism. 2007;56(9):1187–1191. doi:10.1016/j.metabol.2007.04.015
15. Wang Y, Hu S, Ren L, et al. Lp-PLA2 as a risk factor of early neurological deterioration in acute ischemic stroke with TOAST type of large arterial atherosclerosis. Neurol Res. 2019;41(1):1–8. doi:10.1080/01616412.2018.1493850
16. Edelberg JM, Reilly CF, Pizzo SV. The inhibition of tissue type plasminogen activator by plasminogen activator inhibitor-1. The effects of fibrinogen, heparin, vitronectin, and lipoprotein(a). J Biol Chem. 1991;266(12):7488–7493. doi:10.1016/S0021-9258(20)89472-1
17. Ezratty A, Simon DI, Loscalzo J. Lipoprotein(a) binds to human platelets and attenuates plasminogen binding and activation. Biochemistry. 1993;32(17):4628–4633. doi:10.1021/bi00068a021
18. Brammen L, Granegger S, Sinzinger H. The effect of elevated lipoprotein(a) on autologous platelets function: a retrospective analysis. Hell J Nucl Med. 2016;19(3):218–222. doi:10.1967/s002449910403
19. Caplice NM, Panetta C, Peterson TE, et al. Lipoprotein (a) binds and inactivates tissue factor pathway inhibitor: a novel link between lipoproteins and thrombosis[J]. Blood. 2001;98(10):2980–2987. doi:10.1182/blood.v98.10.2980
20. Pan S, Kleppe LS, Witt TA, et al. The effect of vascular smooth muscle cell-targeted expression of tissue factor pathway inhibitor in a murine model of arterial thrombosis[J]. Thromb Haemost. 2004;92(3):495–502. doi:10.1160/TH04-01-0006
21. Sotiriou SN, Orlova VV, Al-Fakhri N, et al. Lipoprotein(a) in atherosclerotic plaques recruits inflammatory cells through interaction with Mac-1 integrin. FASEB J. 2006;20(3):559–561. doi:10.1096/fj.05-4857fje
22. Zheng KH, Tsimikas S, Pawade T, et al. Lipoprotein(a) and oxidized phospholipids promote valve calcification in patients with aortic stenosis[J]. J Am Coll Cardiol. 2019;73(17):2150–2162. doi:10.1016/j.jacc.2019.01.070
23. Arboix A, García-Eroles L, Massons J, Oliveres M, Targa C. Lacunar infarcts in patients aged 85 years and older. Acta Neurol Scand. 2000;101(1):25–29. doi:10.1034/j.1600-0404.2000.00005.x
24. Arboix A, García-Eroles L, Sellarés N, Raga A, Oliveres M, Massons J. Infarction in the territory of the anterior cerebral artery: clinical study of 51 patients. BMC Neurol. 2009;9(1):30. doi:10.1186/1471-2377-9-30
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictors of Early Neurological Deterioration and Functional Outcome in Acute Ischemic Stroke: The Importance of Large Artery Disease, Hyperglycemia and Inflammatory Blood Biomarkers
Sabir Rashid A, Huang-Link Y, Johnsson M, Wetterhäll S, Gauffin H
Neuropsychiatric Disease and Treatment 2022, 18:1993-2002
Published Date: 6 September 2022
Neuroprotection for Nonarteritic Central Retinal Artery Occlusion: Lessons from Acute Ischemic Stroke
Okonkwo ON, Agweye CT, Akanbi T
Clinical Ophthalmology 2023, 17:1531-1543
Published Date: 31 May 2023
Nomogram-Based Prediction of 3-Month Unfavorable Outcome and Early Neurological Deterioration After Endovascular Thrombectomy in Acute Ischemic Stroke
Wu Y, Han J, Cheng Y, Wei M, Liu F, Chen C, Tan Y, Ma W, Yu J, Han J, Luo G, Huo K
Therapeutics and Clinical Risk Management 2025, 21:239-256
Published Date: 27 February 2025