")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Significant Predictors of Azithromycin in Population Pharmacokinetic Analysis: A Systematic Review
Authors Zhang R, Fang Y, Wang Y, Fan J, Yin W, Fan W, Yu Y, Lin B
Received 26 January 2025
Accepted for publication 21 June 2025
Published 4 July 2025 Volume 2025:19 Pages 5709—5725
DOI https://doi.org/10.2147/DDDT.S519597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Runcong Zhang,1,2,* Yuebin Fang,3,* Yinhui Wang,1,2 Jing Fan,1,2 Weiming Yin,1,2 Weibin Fan,1,2 Yuetian Yu,2,4,5 Bin Lin1,2,4
1Department of Pharmacy, Changxing People’s Hospital, Changxing, Zhejiang, People’s Republic of China; 2Key Laboratory of Intelligent Pharmacy and Individualized Therapy of Huzhou, Changxing, Zhejiang, People’s Republic of China; 3Department of General Practice, Changxing People’s Hospital, Changxing, Zhejiang, People’s Republic of China; 4Key Laboratory of Multiple Organ Failure (Zhejiang University), Ministry of Education, Hangzhou, Zhejiang, People’s Republic of China; 5Department of Critical Care Medicine, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Lin, Department of Pharmacy, Changxing People’s Hospital, Changxing, Zhejiang, 313100, People’s Republic of China, Tel/Fax +86-572-6267652, Email [email protected] Yuetian Yu, Department of Critical Care Medicine, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200127, People’s Republic of China, Tel/Fax +86-13818227011, Email [email protected]
Abstract: Azithromycin is widely used to treat infections caused by susceptible bacteria and is the first-line treatment for mycoplasma pneumonia in pediatric patients. However, in clinical practice, large between-patient variability has been observed. Several population pharmacokinetic studies have been conducted to identify covariates and guide individualized therapy. This study evaluated published population pharmacokinetic studies and explored the significant covariates. The PubMed, Embase, and Web of science databases were systematically searched from their inception to 30 May 2024. Information on study design, characteristics, and final model parameters was extracted and compared. Time–concentration curves and forest plots were used to examine pharmacokinetic characteristics and identify covariates, respectively. Fifteen population pharmacokinetic studies were included in the review: three involved preterm neonates, two involved children, two involved pregnant/non-pregnant women, and eight involved adults. The median apparent clearance value was higher for adults (1.66 L/h/kg) than for children (1.28 L/h/kg) and preterm neonates (0.187 L/h/kg). For all populations, body weight significantly influenced the apparent clearance and distribution volume. In children, age and liver function influenced azithromycin clearance; whereas for women, clearance was reduced by 38% in case of pregnancy, non-African descent, and oral contraceptive use. Azithromycin was shown to distribute across plasma, tissues, and cells, with notable concentration differences. The azithromycin dose regimen is determined based on body weight. However, for children and women, additional predictors should be considered for individualized therapy. Further azithromycin population studies of the dose–exposure–response relationship are needed to achieve accurate dose adjustments.
Keywords: azithromycin, population pharmacokinetics, nonlinear mixed effect model, individualized drug therapy
Introduction
Azithromycin (AZM), a second-generation macrolide antibiotic, is an erythromycin synthetic intermediate derivative with a 15-membered lactone ring azalide parent structure. It was developed by Pfizer and then approved by the Food and Drug Administration (FDA) for marketing in 1991.1 As a broad-spectrum antimicrobial, AZM is extensively used worldwide for the treatment of acute bacterial exacerbations of chronic bronchitis, community-acquired pneumonia, acute otitis media, acute bacterial sinusitis, and uncomplicated skin and skin structure infections.2,3 Recent clinical studies have demonstrated its beneficial effects in chronic obstructive pulmonary disease,4–6 non-cystic fibrosis bronchiectasis,7,8 and malaria.9–11 According to the latest World Health Organization (WHO) data, azithromycin ranks among the most frequently prescribed antibiotics globally.12 Between 2020 and 2022, outpatient prescriptions for azithromycin in the United States increased annually, reaching 34.9 million prescriptions in 2022.13
Similar to other macrolide antibiotics, AZM inhibits bacterial protein synthesis by binding to and interfering with the assembly of the 50S large ribosomal subunit and growth of the nascent polypeptide chain.14–16 It also shows moderate activity against the malaria parasite Plasmodium spp., with delayed killing achieved via the apicoplast.17 Other activities of AZM include anti-inflammatory and immunomodulatory effects exerted through multiple pathways and mechanisms.1
In adults, the oral administration of 500 mg AZM results in low bioavailability (17–37%), with peak plasma concentrations (0.2–0.4 mg/L) reached within 2–4 h.18,19 Higher peak concentrations (1.14 ± 0.14 mg/L) are obtained after intravenous administration. Plasma protein binding decreases from 51% to 7% when plasma AZM concentrations increase from 0.02 mg/L to 2 mg/L, with a volume of distribution (Vd) of the drug of approximately 30 L/kg.2,20 The rapid blood-to-tissue distribution of AZM results in concentrations in plasma that are significantly lower than those in blood, and in high concentrations in target tissues. The plasma half-life of AZM is approximately 70 h for oral and 50 h for intravenous formulations.1,21 This pharmacokinetic characteristic of AZM accounts for the rapid achievement of the desired drug exposure with less frequent administration. On the other hand, the longer half-life of AZM means that patients receiving treatment have a longer duration of subinhibitory concentrations and are more susceptible to developing resistance once the administered dose fails to kill the target pathogen in its entirety.22 AZM is mainly eliminated unchanged in the feces via biliary excretion, with only about 6% (oral dose) to 11% (24 h after the first intravenous dose) recovered unchanged in the urine.1,2,20
The pharmacokinetics (PK) of AZM vary considerably among different populations. Previous studies have shown overexposure in preterm infants (~ 3.2-fold) compared with older children (aged 0.5–2 years)23,24 but inadequate exposure in pregnant women.25 Overexposure increases the risk of adverse reactions and interactions whereas inadequate exposure increases the risk of drug resistance, such that drug concentrations should be carefully determined.26 It is therefore critical to identify the factors that influence interindividual PK variability and to adjust the dose accordingly.
Population pharmacokinetics (PPK) describe the typical PK of the target population and identify factors that contribute to the variability. In recent years, PPK has been increasingly integrated into clinical practice. Compared to post-treatment interventions with empirical therapy and therapeutic drug monitoring, Bayesian forecasting and Monte Carlo simulation based on PPK have enabled dose individualization and dose adjustment, both at the beginning of and during treatment.27,28
At present, several PPK studies of AZM have been conducted in different populations to identify covariates that significantly affect the drug’s PK; however, there is still no systematic review summarizing and analyzing PPK model data for AZM. In the following, we provide a review of published PPK studies and identify the significant covariates affecting AZM PK. Our analysis can serve as the basis for the rational use of AZM and highlights the knowledge gaps needing further research.
Methods
Search Strategy
The PubMed, Web of Science, and Embase databases were searched systematically for PPK studies of AZM, from their inception to 30 May 2024, according to the principles of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.29 The following search terms were employed: “Azythromycin”, “Sumamed”, “Toraseptol”, “Vinzam”, “CP-62993”, “CP 62993”, “CP62993”, “Zithromax”, “Azitrocin”, “Azadose”, “Ultreon”, “Zitromax”, “Azithromycin Dihydrate”, “Dihydrate, Azithromycin”, “Azithromycin Monohydrate”, “Monohydrate Azithromycin”, “Goxal”, or “Zentavion” and “population pharmacokinetic*” “pharmacokinetic model*” “nonlinear mixed effect model”, “NONMEM”, “WINNONMIX”, “P-PHARM”, “MWPHARM”, “nlmixed”, “NLME”, and “MONOLIX.” The search strategy is described in Table S1.
All studies identified from databases and other sources were screened to assess their eligibility. A study was considered eligible if it met the following criteria: the study population was human; AZM was the study drug, regardless of its formulation; and a non-linear mixed-effect modeling approach was adopted. A study was excluded if it met the following criteria: review article or use of modeling data from the literature; published in a language other than English; and insufficient information on modeling to allow model reproduction. Two independent authors screened the titles and abstracts, as well as the full text, of each article to determine their eligibility. Discrepancies were resolved by a third senior investigator.
Data Extraction
The following information was extracted from all included articles using a standardized data collection method: study design, including type of study, number of patients and observations, sampling design, dose regimens, research period, and the country where the study was conducted; characteristics of the study population, including sex, weight, age, and race; bioanalytical methods, including type of instrument, lower limit of quantification (LLQ), and methods for determining concentrations below the LLQ; and information on the PPK model, including the data analysis software and algorithm, the structural model, parameter estimates, covariates, between-subject variability (BSV), residual unexplained variability (RUV), model evaluation, and model applications.
Study Quality
To assess the quality of the included studies scientifically and systematically, detailed criteria were developed based on the clinical PK and population PK-pharmacodynamics (PD) guidelines for writing and evaluating,30,31 as shown in Table S2. There were five main evaluation criteria (title/abstract, background, methods, results, and discussion/conclusion), with a total of 35 items. An included study that conformed with the content of an item was assigned 1 point (otherwise 0 points). Compliance was used to evaluate the quality of each identified PPK study. The compliance rate was calculated using Eq. (1):

Study Comparisons
Data on the characteristics of each study, including design, population characteristics, and PPK model information, were put into standard tabular format for analysis and comparison. Based on the information from the PPK models of the included studies, Monte Carlo simulations were used to draft time–concentration curves, with visual predictive distribution (VPD) plots used to explore differences in PK profiles among the different study populations.32,33 Based on the assumption that the predictive distribution of the simulated PK profiles of AZM sufficiently represented the features of each model and its original data,32 simulated concentration–time curves were compared with the corresponding literature concentration distributions to assess the accuracy of the results.
The concentration–time profiles of preterm neonates (0.85 kg, postmenstrual age 26 weeks), children (20 kg, 6 years), pregnant women (60 kg, 27 years), non-pregnant women (55 kg, 27 years), and adults (70 kg, 40 years) were plotted according to the established PPK model and the cohorts in each study. Preterm neonates and children received 10 mg AZM/kg; pregnant/non-pregnant women and other adults received 500 mg. Except for the group of pregnant and non-pregnant women, a steady-state drug concentration was assumed for all patients, and all were modeled as male. Monte Carlo simulations were conducted using NONMEM (version 7.5; ICON Development Solutions, Ellicott City, MD, USA). R software (version 4.3.3; www.r-project.org) was employed for visualization.
Clearance (CL) is one of the most important PK parameters in patients treated with antibacterial drugs, as it significantly influences drug exposure and individualized dosing. Therefore, the effects of the covariates on the CL in each study were summarized and are presented as forest plots, generated using the “forestplot” add-on package in R (version 3.1.3; https://gforge.se/packages/).
In studies with similar population characteristics, common continuous covariates were adjusted to the same range for the purpose of comparison (eg, weight). For continuous covariates appearing in only one study, the reported range was used. For binary covariates such as pregnancy, values of 0 and 1 were used. The reference values of CL were normalized to the median covariate values in each study. The effect of the identified covariates on CL in each study was expressed as the percentage of the range of the calculated CL divided by the reference value.33 CL was considered clinically significant if < 80% or > 125%.34
Results
Study Identification
From the 434 studies initially identified in PubMed (319), Embase (6), and the Web of Science (109), 20 were eligible for full-text screening; the others were duplicates or unrelated to PPK. Four studies were then excluded because they used data from other reference models, and another was excluded due to missing PPK parameters. Thus, 15 studies were finally included in this systematic review. The PRISMA flow diagram illustrates the screening and organization of the studies (Figure 1).
 |
Figure 1 PRISMA flow diagram used to identify azithromycin (AZM) population pharmacokinetics studies. Notes: PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). Creative Commons.35 |
Study Quality
Except for three articles with compliance rates below 70%, all of the studies had rates above 70%, with a median of 77.1% (range: 65.7–88.6%). The low coincidence rate of several studies was due to the lack of relevant items, such as items on PK data, methods for handling missing data, and methods used for base model evaluation. The quality analysis of the included studies of AZM PPK is shown in Table S3.
Study Comparisons
General Characteristics
Of the 15 included studies, 8 were conducted in adult populations. Six of those studies were performed in healthy patients, and three studies only enrolled males.36–42 Two studies explored the PK profiles of AZM in pregnant/non-pregnant women.25,43 The other five studies were conducted in preterm neonates born at approximately 26 weeks23,44,45 and in children 1–12 years of age.46,47 A sparse sampling strategy was employed in three studies,37,41,43,46 and intensive sampling in nine.23,25,36,38,39,42,44,45,48 Only Zheng et al40 employed a combination of sparse- and intensive sampling. In one study, the sampling strategy was not reported.47 With the exception of the study of Wu et al,41 in which AZM was administered as eyedrops and the samples consisted of tears, in all studies blood samples were collected after oral or intravenous drug administration. The characteristics of the included studies are detailed in Table 1.
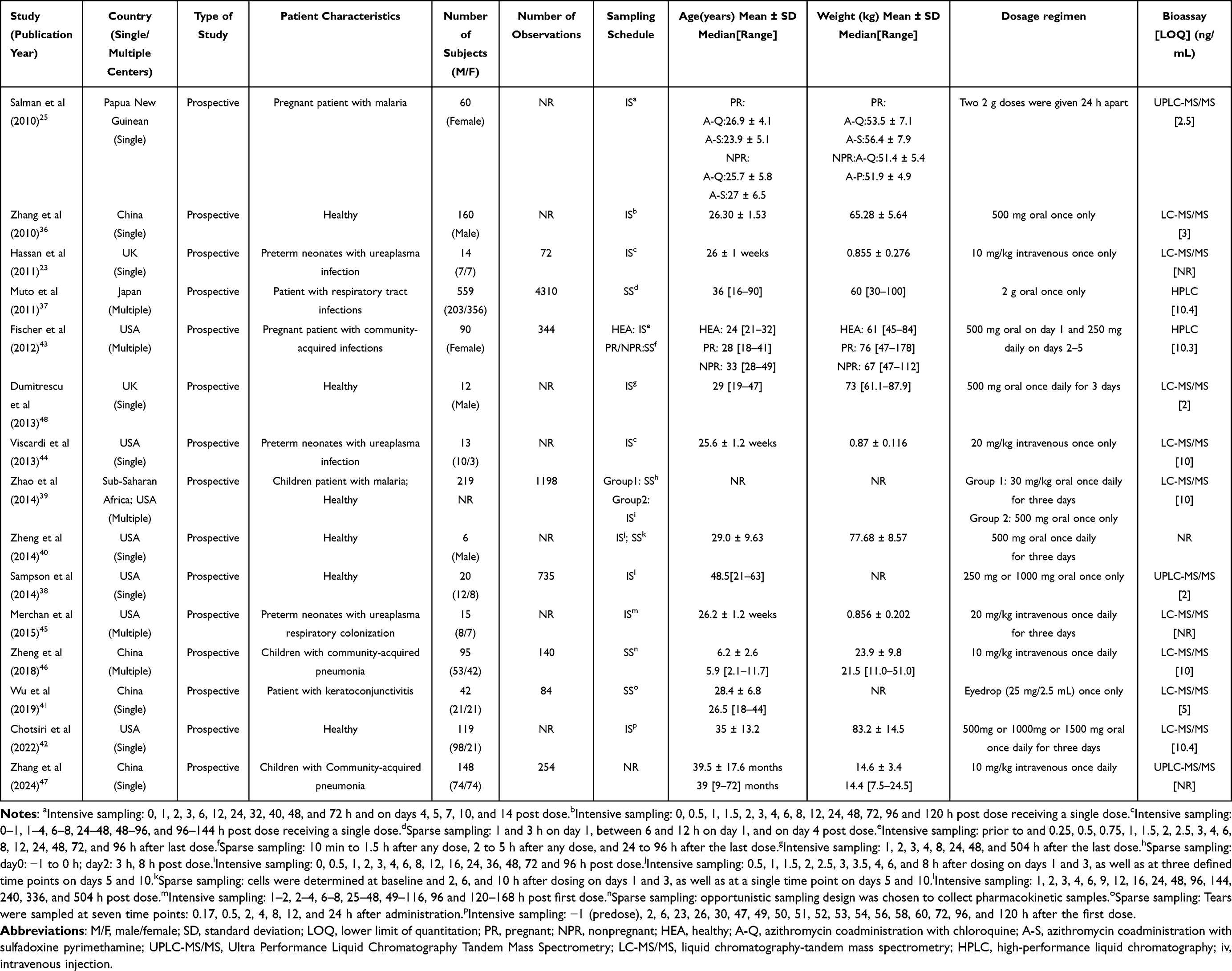 |
Table 1 Characteristics of Included Studies |
Population Pharmacokinetic Studies
Seventeen PPK models were developed in the 15 studies, as Salman et al25 and Fischer et al43 developed separate PPK models for pregnant and non-pregnant women. NONMEM and first-order conditional estimation with interaction (FOCE-I) were the most commonly used software and algorithm, respectively.49 A two-compartment or three-compartment model with first-order absorption and elimination kinetics was used to describe the AZM PPK profiles in 13 of the 15 studies (86.7%); in the others, one-compartment47 and four-compartment38 models were used. The modeling strategies and final parameters of the included studies are presented in Table 2.
 |
Table 2 Modeling Strategies and Final Parameters of Included Studies |
In the VPD plots, virtual patients were categorized into two groups (plasma and non-plasma concentration groups) according to the compartment concentration and corresponding dosing regimen. The plasma concentration group was divided into five subgroups based on age, body weight, and dosing regimen; the non-plasma concentration group included whole-blood, polymorphonuclear cells (PMNs), peripheral blood mononuclear cells (PBMCs), muscle interstitial space fluid (ISF) and subcutis ISF, as shown in Figures 2 and 3. Virtual patients included preterm infants, children, pregnant women, and adults, and the dosing regimen was divided into two modalities. Details on the groups of virtual patients are provided in Table 3. With the exceptions of the pregnancy and non-pregnancy groups, all patients receiving AZM monotherapy were defined as males, and the drug was assumed to have reached a steady-state concentration.
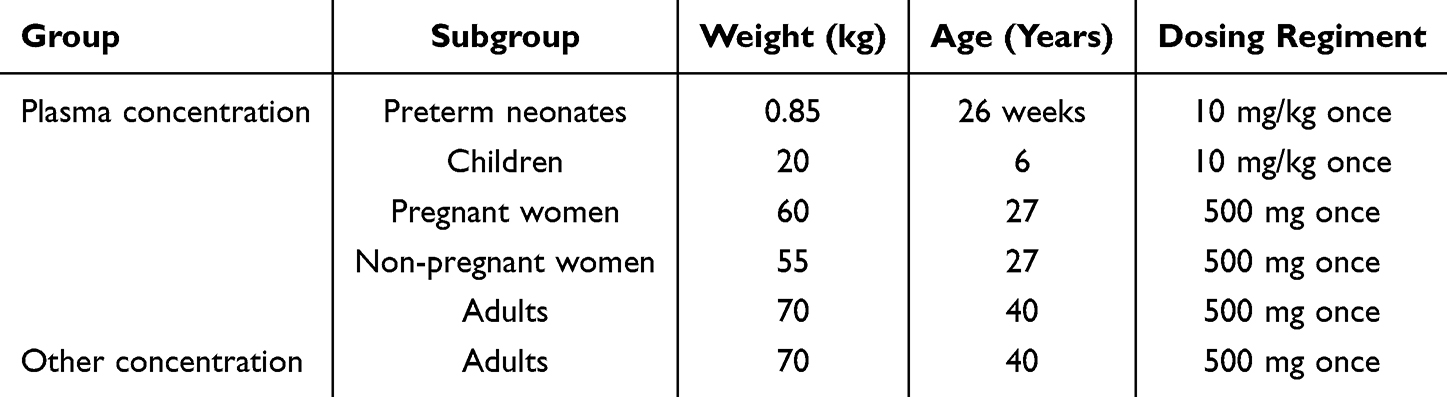 |
Table 3 Charcateristics of Virtual Patients and Dosing Regimens |
 |
Figure 2 Concentration–time profiles of AZM in (A) preterm neonates, (B) children, (C) pregnant women, (D) non-pregnant women, and (E) adults in the retrieved studies. The solid line represents the median of the simulated concentration–time profiles, and the light shadows are the 10th–90th percentiles of those profiles. All patients were assumed to be male except for those in the pregnancy/non-pregnancy group. Preterm neonates and children received AZM intravenous monotherapy at a dose of 10 mg/kg while pregnant/non-pregnant women and other adults received oral AZM monotherapy at a dose of 500 mg. |
 |
Figure 3 Non-plasma concentration–time profiles of AZM in adults according to the retrieved studies. The solid line represents the median of the simulated concentration–time profile, and the light shadows are the 10th–90th percentiles of those profiles. All patients were assumed to be male and received AZM monotherapy at a dose of 500 mg. Abbreviations: PMNs, polymorphonuclear cells; PBMCs, peripheral blood mononuclear cells; ISF, interstitial space fluid. |
AZM plasma exposure varied widely among the different age groups, with peak concentrations of approximately 5 mg/L in preterm neonates and 2 mg/L in children. Similar concentration–time profiles were achieved in the pregnancy/non-pregnancy groups and adult group of each study when the administered dose was the same. The concentration of AZM in non-plasma compartments differed substantially across different tissues and cells, whereas in whole blood it was similar to that in plasma. Non-plasma concentration–time profiles indicated that the AZM concentrations in PMNs and PBMCs were thousands of times higher than those in plasma, while the concentrations in muscle ISF and subcutis ISF were substantially lower than in plasma. In the included studies, when AZM was administered at therapeutic doses, its CL varied significantly across different populations. The CL/kg estimated in the three studies of preterm neonates was 0.187, 0.217, and 0.156 (L/h/kg), respectively; in the two studies in children, it was 1.27 and 1.29 (L/h/kg), respectively, with higher values estimated in pregnant/non-pregnant woman and in adults (median of 1.66 L/h/kg).
All of the studies, except those of Dumitrescu et al48 and Chotsiri et al,42 identified potential covariates with respect to the between-subject variability (BSV) of AZM PK by forward inclusion and backward elimination. However, three studies38,40,41 failed to identify significant covariates. The covariates of CL and Vd that were investigated and retained in the final model are summarized in online Table S4. The covariates identified for CL included weight, age, pregnancy, lean body weight, alanine aminotransferase (ALT), and co-administered medication. The effect of each covariate on CL is presented in the forest plot (Figure 4).
 |
Figure 4 Effects of covariates for the apparent clearance (CL) of AZM. The horizontal bars represent the effect of covariates on the CL according to each study. The typical CL in each study was considered to be 1. The x-axis refers to the effect of each identified covariate on CL, expressed as the ratio of the value of CL in the range of each covariate and the typical value of CL. The shaded area ranges from 0.8 to 1.25. N, no; Y, yes. |
The 10 studies identifying significant covariates found a significant effect of body weight on AZM CL; in 8 studies (80%), the range of CL variation was > 20%. In the two studies that examined the effect of age on CL,37,47 the impact was more clinically significant in children (range: 0.57–1.30) than in adults (range: 0.91–1.16). Zheng et al46 reported that an ALT > 40 in the pediatric population reduced the CL of AZM by 24%. Fischer et al43 showed that pregnancy, non-African heritage, and oral contraceptive use reduced the CL of AZM by up to 38%. The most frequently reported covariates that influenced AZM Vd were age and body weight.
All studies used exponential models to describe BSV. The median (range) BSV was as follows: CL, 31.15% (6.19–122.00%) (n = 14); Vd, 84.90% (0.01–189.00%) (n = 13); and Ka, 59.40% (41.00–110.00%) (n = 5). The residual unexplained variability (RUV) described by the proportional models typically ranged from 1.94% to 74.00%, with substantial differences between the various compartment models.
The internal evaluation methods for the models in the examined studies primarily included goodness-of-fit (GOF) plots, visual predictive checks, normalized prediction distribution error (NPDE), quantile–quantile (Q–Q) plots, and bootstrap. Each study employed at least one of these methods to assess the accuracy and robustness of the final model. Additionally, two studies demonstrated strong predictive performance of the final model through external validation using independent datasets.
Five studies23,41,44,46,47 performed model-based simulations in adults, but another study41 did not give the corresponding simulated dose. In the studies of preterm neonates by Hassan et al23 and Viscardi et al,44 a dosage regimen of 20 mg AZM/kg/d × 3 days was found to be sufficient to maintain AZM plasma levels above the minimum inhibitory concentration required to inhibit the growth of 50% bacteria (MIC50) (1 mg/L). For children, Zheng et al46 recommended dose adjustments based on liver function as follows: for ALT ≤ 40, a loading dose of 15 mg/kg/d and a maintenance dose of 10 mg/kg/d; and for ALT > 40, a 15% reduction in the AZM dose. Zhang et al47 recommended dose adjustments according to age and body weight.
Discussion
AZM, a second-generation macrolide antimicrobial drug, is used in the treatment of infections and is the first-line drug for mycoplasma pneumonia in pediatric patients. The dose–exposure–response relationship of AZM has been intensively investigated with the aim of achieving individualized therapy. However, although several PPK studies have been published, the sources of PK variability were unclear. This review is the first to summarize currently available PPK studies of the covariates that significantly influence AZM exposure.
We performed a systematic initial screening of literature across three major medical databases in accordance with predefined search strategies. The preliminary results underwent secondary screening based on inclusion/exclusion criteria, and the remaining studies were included after quality assessment (Table S3, Compliance ≥60%). The screening and quality assessment processes ensured the validity and rigor of the included literature, establishing a solid foundation for the subsequent review analysis. Furthermore, this methodology enhances the quality of evidence and strengthens the reliability of the findings.
All studies conducted in adult patients treated with oral AZM showed similar concentration–time profiles for patients with the same demographic characteristics. The large differences in PK between children and adults could be attributed to the fact that adults are administered AZM orally, whereas in children it is administered intravenously, which results in higher exposure.2,24 Preterm neonates were more highly exposed than children injected with the same dose of AZM. As AZM is mostly eliminated by the biliary route, bile secretion in adults is approximately 600 mL/day, whereas no real data are available for children and preterm infants, but it is clear that they are significantly lower than adult levels.50 Preterm neonates producing less bile than term infants due to the weaker development of the gallbladder in preterm neonates than term infants.23,51 This may be one of the reasons for the above pharmacokinetic differences. In addition, a sequential increase in Vd/kg in preterm infants, children, and adults can lead to this phenomenon.
Body weight was the most significant covariate affecting the PK of AZM in patients. In 10 studies,23,25,36,37,39,43–47 total CL increased with increasing body weight, with 9 of those studies indicating a considerable change (> 20%). Therefore, the AZM dose should be adjusted according to body weight in both lean and obese patients to ensure efficacy and safety.
Muto et al37 and Zhang et al47 included age as a significant covariate affecting the CL of AZM. In Muto et al’s study, the impact of age on CL was between 0.8 and 1.25 (Figure 4) and thus of no clinical significance. The contrasting findings of Zhang et al’s study may be related to its inclusion only of children 1–6 years of age. In this age range, as the gallbladder grows and develops in children, there is a subsequent increase in bile production, which leads to changes in the CL of AZM.52–54 Zheng et al46 identified ALT as a significant covariate affecting AZM PK in children, such that impaired liver function could reduce the biliary secretion of AZM into bile, thereby increasing the plasma concentration. Existing studies fail to adequately address both adolescent (10–19 years) and elderly patients (≥65 years) populations, creating an evidence gap that demands targeted research to quantify age-dependent effects.
Fischer et al43 reported racial variability in the effect of pregnancy on AZM PK. In Asian, Caucasian, Hispanic, and Pacific Islander women, AZM CL/F and CLD-P2/F were 38.05% and 65.00% lower, respectively, than in women who were not pregnant and not using oral contraceptives.43 This may reflect the significant increase in estrogen levels during pregnancy, which increases AZM bioavailability and decreases hepatobiliary excretion.55–57 In African-American populations, Fischer et al43 and Salman et al25 showed no effect of pregnancy on AZM CL. The only significant relationship identified by Salman et al in their PPK analysis was between pregnancy and Vc/F,25 with the latter being 86% higher, attributable to the increase in plasma volume during pregnancy.58 Thus, in clinical practice, the effects of race and pregnancy need to be considered in determining the dose of AZM.
The coadministration of oral contraceptives in nonpregnant women also influenced the AZM CL/F, producing a decrease comparable to that occurring during pregnancy in women of non-African American ancestry.43 This phenomenon has been described for other drugs59,60 and is most likely related to the fact that the main ingredient in contraceptives is estrogen. Other studies have shown that the co-administration of AZM with chloroquine has no significant effect on its PK.
Three studies38,40,48 reported differences in AZM concentrations across different compartments. Concentration in PMNs and PBMCs were 1,000 times higher than in plasma, whereas those in subcutis ISF and muscle ISF were only a few tenths of the plasma concentration. After multiple doses, AZM accumulates in acidic cell compartments (PMNs and PBMCs), with its subsequent slow release being responsible for its long terminal half-life61 but also contributing to increased drug resistance. Due to the long half-life of AZM, if the pathogen is not eradicated and cleared within a short period, it remains exposed to sub-therapeutic concentrations for an extended duration, which significantly increases the risk of resistance development. Zheng et al40 recommended that oral AZM for the prevention and treatment of skin and skin structure infections should be prescribed with caution. In the treatment of other infections, timely dose adjustments are necessary to rapidly eradicate the pathogen, or AZM should be combined with other antimicrobial agents.
This review included one population PK/PD study.37 A previous study suggested that a clinical exposure–efficacy relationship of AZM could be characterized using the area under the curve AUC/MIC as a population PK/PD index.62 In the population PK/PD study, the percentage of bacteriological and clinical success was much higher in patients with an AUC/MIC > 5 than in those with an AUC/MIC ≤ 5, and a negative association was determined between the AZM AUC and the incidence of diarrhea.37 Additional prospective population PK/PD studies are needed to develop a comprehensive perspective on the dose–exposure–response relationship. Due to the widespread use of AZM in pediatric populations, PK/PD studies using AUC/MIC as a pharmacodynamic index are more urgent. In addition, the concentration of AZM should not be limited to blood the concentration, but should also include the concentration in target tissues, and such studies can effectively promote the individualization of AZM treatment in pediatric populations.
Limitations
Our systematic review had the following limitations: (1) The inclusion of only English language literature may have missed some of the high quality non-English language literature and would have resulted in some statistical differences in terms of geography and ethnicity; (2) the population PK/PD model was not examined in, it was only briefly considered in the Results and Discussion sections; (3) comparing pharmacokinetic models using standardized virtual populations with identical covariates across age groups may obscure inherent population characteristics in each original model.
Conclusions
Our review of published PPK studies of AZM showed that the PK of AZM differs between adult and pediatric patients, with a lower CL in preterm neonates and children. Our results support the dosing of AZM according to body weight, but the effects of age and liver function in children, as well as pregnancy, race, and contraceptive effects in women, should also be considered. AZM dose–exposure–response determination through additional studies will facilitate individualized therapy and reduce drug resistance.
Acknowledgments
We sincerely thank the editors and all reviewers for their hard work.The English in this document has been checked by at least two professional editors, both native speakers of English. For a certificate, please see: http://www.textcheck.com/certificate/2VK2oN
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Runcong Zhang and Yuebin Fang are co-first authors.
Funding
This research was supported by the Joint Funds of the Hospital Pharmacy Special Research Funding Project of the Zhejiang Pharmaceutical Association under Grant No.2022ZYY42.
Disclosure
The authors declare no conflict of interest.
References
1. Parnham MJ, Erakovic Haber V, Giamarellos-Bourboulis EJ, Perletti G, Verleden GM, Vos R. Azithromycin: mechanisms of action and their relevance for clinical applications. Pharmacol Ther. 2014;143(2):225–245. doi:10.1016/j.pharmthera.2014.03.003
2. ZITHROMAX®. (Azithromycin) Tablets [Prescribing Information]. Groton: Pfizer, Inc; 2021.
3. Abdallah YB, Belfeki N, Klopfenstein T, Zayet S. Pulmonary cavitary disease due to Mycobacterium xenopi. Infectious Med. 2022;1(1):63–66. doi:10.1016/j.imj.2021.11.001
4. Aaron SD. Management and prevention of exacerbations of COPD. BMJ. 49:3g5237. doi:10.1136/bmj.g5237
5. Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med. 2011;365(8):689–698. doi:10.1056/NEJMoa1104623
6. Donath E, Chaudhry A, Hernandez-Aya LF, Lit L. A meta-analysis on the prophylactic use of macrolide antibiotics for the prevention of disease exacerbations in patients with chronic obstructive pulmonary disease. Respir Med. 2013;107(9):1385–1392. doi:10.1016/j.rmed.2013.05.004
7. Henkle E, Aksamit TR, Barker AF, et al. Pharmacotherapy for non-cystic fibrosis bronchiectasis: results from an NTM info & research patient survey and the bronchiectasis and NTM research registry. Chest. 2017;152(6):1120–1127. doi:10.1016/j.chest.2017.04.167
8. Wong C, Jayaram L, Karalus N, et al. Azithromycin for prevention of exacerbations in non-cystic fibrosis bronchiectasis (EMBRACE): a randomised, double-blind, placebo-controlled trial. Lancet. 9842;380. doi:10.1016/s0140-6736(12)60953-2
9. Arzika AM, Maliki R, Boubacar N, et al. Biannual mass azithromycin distributions and malaria parasitemia in pre-school children in Niger: a cluster-randomized, placebo-controlled trial. PLoS Med. 2019;16(6):e1002835. doi:10.1371/journal.pmed.1002835
10. Arzika AM, Maliki R, Goodhew EB, et al. Effect of biannual azithromycin distribution on antibody responses to malaria, bacterial, and protozoan pathogens in Niger. Nat Commun. 2022;13(1):976. doi:10.1038/s41467-022-28565-5
11. Chandramohan D, Dicko A, Zongo I, et al. Effect of adding azithromycin to seasonal malaria chemoprevention. N Engl J Med. 2019;380(23):2197–2206. doi:10.1056/NEJMoa1811400
12. WHO Database [homepage on the Internet]. Global Antimicrobial Resistance and Use Surveillance System (GLASS) report antibiotic use data for 2022; 2025. Available from: https://www.who.int/pubLications/i/item/9789240062702.
13. Centers for Disease Control and Prevention Database [homepage on the Internet]. Outpatient antibiotic prescriptions — United States, 2022; 2025. Available from: https://archive.cdc.gov/#/details?url=https://www.cdc.gov/antibiotic-use/data/report-2022.html.
14. Champney WS, Burdine R. Azithromycin and clarithromycin inhibition of 50S ribosomal subunit formation in Staphylococcus aureus cells. Curr Microbiol. 1998;36(2):119–123. doi:10.1007/s002849900290
15. Champney WS, Tober CL, Burdine R. A comparison of the inhibition of translation and 50S ribosomal subunit formation in Staphylococcus aureus cells by nine different macrolide antibiotics. Curr Microbiol. 1998;37(6):412–417. doi:10.1007/s002849900402
16. Hansen JL, Ippolito JA, Ban N, Nissen P, Moore PB, Steitz TA. The structures of four macrolide antibiotics bound to the large ribosomal subunit. Mol Cell. 2002;10(1):117–128. doi:10.1016/s1097-2765(02)00570-1
17. Dahl EL, Rosenthal PJ. Multiple antibiotics exert delayed effects against the Plasmodium falciparum apicoplast. Antimicrob Agents Chemother. 2007;51(10):3485–3490. doi:10.1128/aac.00527-07
18. Luke DR, Foulds G. Disposition of oral azithromycin in humans. Clin Pharmacol Ther. 1997;61(6):641–648. doi:10.1016/s0009-9236(97)90098-9
19. Coates P, Daniel R, Houston AC, Antrobus JH, Taylor T. An open study to compare the pharmacokinetics, safety and tolerability of a multiple-dose regimen of azithromycin in young and elderly volunteers. Eur J Clin Microbiol Infect Dis. 1991;10(10):850–852. doi:10.1007/bf01975839
20. Singlas E. [Clinical pharmacokinetics of azithromycin. Pathol Biol. 1995;43(6):505–511. PMID: 8539072.
21. Lode H, Borner K, Koeppe P, Schaberg T. Azithromycin--review of key chemical, pharmacokinetic and microbiological features. J Antimicrob Chemother. 1996;37:1–8. doi:10.1093/jac/37.suppl_c.1
22. Kong FYS, Horner P, Unemo M, Hocking JS. Pharmacokinetic considerations regarding the treatment of bacterial sexually transmitted infections with azithromycin: a review. J Antimicrob Chemother. 2019;74(5):1157–1166. doi:10.1093/jac/dky548
23. Hassan HE, Othman AA, Eddington ND, et al. Pharmacokinetics, safety, and biologic effects of azithromycin in extremely preterm infants at risk for ureaplasma colonization and bronchopulmonary dysplasia. J Clin Pharmacol. 2011;51(9):1264–1275. doi:10.1177/0091270010382021
24. Jacobs RF, Maples HD, Aranda JV, et al. Pharmacokinetics of intravenously administered azithromycin in pediatric patients. Pediatr Infect Dis J. 2005;24(1):34–39. doi:10.1097/01.inf.0000148927.48680.fc
25. Salman S, Rogerson SJ, Kose K, et al. Pharmacokinetic properties of azithromycin in pregnancy. Antimicrob Agents Chemother. 2010;54(1):360–366. doi:10.1128/aac.00771-09
26. Coles CL, Mabula K, Seidman JC, et al. Mass distribution of azithromycin for trachoma control is associated with increased risk of azithromycin-resistant Streptococcus pneumoniae carriage in young children 6 months after treatment. Clin Infect Dis. 2013;56(11):1519–1526. doi:10.1093/cid/cit137
27. Sheiner LB, Rosenberg B, Melmon KL. Modelling of individual pharmacokinetics for computer-aided drug dosage. Comput Biomed Res. 1972;5(5):411–459. doi:10.1016/0010-4809(72)90051-1
28. Sasaki T, Tabuchi H, Higuchi S, Ieiri I. Warfarin-dosing algorithm based on a population pharmacokinetic/pharmacodynamic model combined with Bayesian forecasting. Pharmacogenomics. 2009;10(8):1257–1266. doi:10.2217/pgs.09.65
29. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
30. Jamsen KM, McLeay SC, Barras MA, Green B. Reporting a population pharmacokinetic-pharmacodynamic study: a journal’s perspective. Clin Pharmacokinet. 2014;53(2):111–122. doi:10.1007/s40262-013-0114-1
31. Kanji S, Hayes M, Ling A, et al. Reporting guidelines for clinical pharmacokinetic studies: the ClinPK statement. Clin Pharmacokinet. 2015;54(7):783–795. doi:10.1007/s40262-015-0236-8
32. Duffull SB, Wright DF. What do we learn from repeated population analyses? Br J Clin Pharmacol. 2015;79(1):40–47. doi:10.1111/bcp.12233
33. Mao JH, Han L, Liu XQ, Jiao Z. Significant predictors for olanzapine pharmacokinetics: a systematic review of population pharmacokinetic studies. Expert Rev Clin Pharmacol. 2023;16(6):575–588. doi:10.1080/17512433.2023.2219055
34. Christians U, Klawitter J, Clavijo CF. Bioequivalence testing of immunosuppressants: concepts and misconceptions. Kidney Int Suppl. 2010;S1–7. doi:10.1038/ki.2009.504
35. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). doi:10.1136/bmj.b2700
36. Zhang XY, Wang YR, Zhang Q, Lu W. Population pharmacokinetics study of azithromycin oral formulations using NONMEM. Int J Clin Pharmacol Ther. 2010;48(10):662–669. doi:10.5414/cpp48662
37. Muto C, Liu P, Chiba K, Suwa T. Pharmacokinetic-pharmacodynamic analysis of azithromycin extended release in Japanese patients with common respiratory tract infectious disease. J Antimicrob Chemother. 2011;66(1):165–174. doi:10.1093/jac/dkq398
38. Sampson MR, Dumitrescu TP, Brouwer KL, Schmith VD. Population pharmacokinetics of azithromycin in whole blood, peripheral blood mononuclear cells, and polymorphonuclear cells in healthy adults. CPT Pharmacometrics Syst Pharmacol. 2014;3(3):e103. doi:10.1038/psp.2013.80
39. Zhao Q, Tensfeldt TG, Chandra R, Mould DR. Population pharmacokinetics of azithromycin and chloroquine in healthy adults and paediatric malaria subjects following oral administration of fixed-dose azithromycin and chloroquine combination tablets. Malar J. 2014;13:36. doi:10.1186/1475-2875-13-36
40. Zheng S, Matzneller P, Zeitlinger M, Schmidt S. Development of a population pharmacokinetic model characterizing the tissue distribution of azithromycin in healthy subjects. Antimicrob Agents Chemother. 2014;58(11):6675–6684. doi:10.1128/aac.02904-14
41. Wu F, Zhao X, Li X, Cui Y. Population pharmacokinetic modeling of azithromycin eyedrops in tears following single-dose topical administration in healthy volunteers. Eur J Drug Metab Pharmacokinet. 2019;44(3):371–378. doi:10.1007/s13318-018-0522-6
42. Chotsiri P, Tarning J, Hoglund RM, Watson JA, White NJ. Pharmacometric and electrocardiographic evaluation of chloroquine and azithromycin in healthy volunteers. Clin Pharmacol Ther. 2022;112(4):824–835. doi:10.1002/cpt.2665
43. Fischer JH, Sarto GE, Habibi M, et al. Influence of body weight, ethnicity, oral contraceptives, and pregnancy on the pharmacokinetics of azithromycin in women of childbearing age. Antimicrob Agents Chemother. 2012;56(2):715–724. doi:10.1128/aac.00717-11
44. Viscardi RM, Othman AA, Hassan HE, et al. Azithromycin to prevent bronchopulmonary dysplasia in ureaplasma-infected preterm infants: pharmacokinetics, safety, microbial response, and clinical outcomes with a 20-milligram-per-kilogram single intravenous dose. Antimicrob Agents Chemother. 2013;57(5):2127–2133. doi:10.1128/aac.02183-12
45. Merchan LM, Hassan HE, Terrin ML, et al. Pharmacokinetics, microbial response, and pulmonary outcomes of multidose intravenous azithromycin in preterm infants at risk for Ureaplasma respiratory colonization. Antimicrob Agents Chemother. 2015;59(1):570–578. doi:10.1128/aac.03951-14
46. Zheng Y, Liu SP, Xu BP, et al. Population Pharmacokinetics and Dosing Optimization of Azithromycin in Children with Community-Acquired Pneumonia. Antimicrob Agents Chemother. 2018;62(9). doi:10.1128/aac.00686-18
47. Zhang Y, Wang Y, Li J, et al. Population pharmacokinetics and individualized medication of azithromycin for injection in children under 6 years old. J Pharm Sci. 2024;113(5):1351–1358. doi:10.1016/j.xphs.2024.01.012
48. Pene Dumitrescu T, Anic-Milic T, Oreskovic K, et al. Development of a population pharmacokinetic model to describe azithromycin whole-blood and plasma concentrations over time in healthy subjects. Antimicrob Agents Chemother. 2013;57(7):3194–3201. doi:10.1128/aac.02430-12
49. Li J, Cai X, Chen Y, Wang C, Jiao Z. Parametric population pharmacokinetics of isoniazid: a systematic review. Expert Rev Clin Pharmacol. 2023;16(5):467–489. doi:10.1080/17512433.2023.2196401
50. Hundt M, Basit H, Physiology JS, Secretion B. Copyright © 2025. StatPearls Publishing LLC.; 2025.
51. Nahata MC, Koranyi KI, Luke DR, Foulds G. Pharmacokinetics of azithromycin in pediatric patients with acute otitis media. Antimicrob Agents Chemother. 1995;39(8):1875–1877. doi:10.1128/aac.39.8.1875
52. Bourlieu C, Ménard O, Bouzerzour K, et al. Specificity of infant digestive conditions: some clues for developing relevant in vitro models. Crit Rev Food Sci Nutr. 2014;54(11):1427–1457. doi:10.1080/10408398.2011.640757
53. Van Den Abeele J, Rayyan M, Hoffman I, Van de Vijver E, Zhu W, Augustijns P. Gastric fluid composition in a paediatric population: age-dependent changes relevant for gastrointestinal drug disposition. Eur J Pharm Sci. 2018;123:301–311. doi:10.1016/j.ejps.2018.07.022
54. Jahnel J, Zöhrer E, Scharnagl H, Erwa W, Fauler G, Stojakovic T. Reference ranges of serum bile acids in children and adolescents. Clin Chem Lab Med. 2015;53(11):1807–1813. doi:10.1515/cclm-2014-1273
55. Amsden GW, Gregory TB, Michalak CA, Glue P, Knirsch CA. Pharmacokinetics of azithromycin and the combination of ivermectin and albendazole when administered alone and concurrently in healthy volunteers. Am J Trop Med Hyg. 2007;76(6):1153–1157. PMID: 17556628. doi:10.4269/ajtmh.2007.76.1153
56. Leslie KK, Reznikov L, Simon FR, Fennessey PV, Reyes H, Ribalta J. Estrogens in intrahepatic cholestasis of pregnancy. Obstet Gynecol. 2000;95(3):372–376. doi:10.1016/s0029-7844(99)00533-5
57. Sugie M, Asakura E, Zhao YL, et al. Possible involvement of the drug transporters P glycoprotein and multidrug resistance-associated protein Mrp2 in disposition of azithromycin. Antimicrob Agents Chemother. 2004;48(3):809–814. doi:10.1128/aac.48.3.809-814.2004
58. Pinheiro EA, Stika CS. Drugs in pregnancy: pharmacologic and physiologic changes that affect clinical care. Semin Perinatol. 2020;44(3):151221. doi:10.1016/j.semperi.2020.151221
59. McGready R, Stepniewska K, Seaton E, et al. Pregnancy and use of oral contraceptives reduces the biotransformation of proguanil to cycloguanil. Eur J Clin Pharmacol. 2003;59(7):553–557. doi:10.1007/s00228-003-0651-x
60. Ohman I, Luef G, Tomson T. Effects of pregnancy and contraception on lamotrigine disposition: new insights through analysis of lamotrigine metabolites. Seizure. 2008;17(2):199–202. doi:10.1016/j.seizure.2007.11.017
61. Amsden GW. Erythromycin, clarithromycin, and azithromycin: are the differences real? Clin Ther. 1996;18(1):56–72. doi:10.1016/s0149-2918(96)80179-2
62. Girard D, Finegan SM, Dunne MW, Lame ME. Enhanced efficacy of single-dose versus multi-dose azithromycin regimens in preclinical infection models. J Antimicrob Chemother. 2005;56(2):365–371. doi:10.1093/jac/dki241
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.