")
Back to Journals » Research Reports in Clinical Cardiology » Volume 16
Simultaneous Multivessel Coronary Artery Spasm Leading to Acute Myocardial Infarction: A Case Report
Authors Ahmed SA , Aden AS , Hassan MO , Abdi IA , Waberi MM , Abdi AE, Mohamud MA , Hassan Fujeyra AM, Ali AA , Ahmed MA, Adam BA , Hassan MS , Aksu F , Dahir OF
Received 12 March 2025
Accepted for publication 3 June 2025
Published 8 June 2025 Volume 2025:16 Pages 15—19
DOI https://doi.org/10.2147/RRCC.S527812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Said Abdirahman Ahmed,1 Ahmed Shafie Aden,1 Mohamed Omar Hassan,1 Ishak Ahmed Abdi,1 Mohamud Mire Waberi,1 Ahmed Elmi Abdi,1 Mohamed Abdullahi Mohamud,2 Abdullahi Mohamed Hassan Fujeyra,3 Abdijalil Abdullahi Ali,4 Mohammed AM Ahmed,5,6 Bakar Ali Adam,7 Mohamed Sheikh Hassan,7 Feyza Aksu,8 Osman Farah Dahir1
1Department of Cardiology, Mogadishu Somali-Turkish Training and Research Hospital, Mogadishu, Somalia; 2Department of Cardiology, Jazeera Specialist Hospital, Mogadishu, Somalia; 3Dean College of Medicine and Health Science, Abrar University, Mogadishu, Somalia; 4Cardiovascular Surgery Department, Mogadishu Somali-Turkish Training and Research Hospital, Mogadishu, Somalia; 5Faculty of Medicine, Mogadishu University, Mogadishu, Somalia; 6Department of Pediatric cardiology, Mogadishu Heart Center, Mogadishu, Somalia; 7Neurology Department, Mogadishu Somali-Turkish Training and Research Hospital, Mogadishu, Somalia; 8Department of Cardiology, Göztepe Prof. Dr. Süleyman Yalçın City Hospital, Istanbul, Türkiye
Correspondence: Osman Farah Dahir, Mogadishu Somalia Turkish Training and Research Hospital, Digfer Road, Mogadishu, Somalia, Tel +252615963164, Email [email protected]
Background: Coronary artery spasm (CAS) refers to a sudden and intense narrowing of the coronary arteries caused by vasoconstriction, which can result in myocardial ischemia and potentially lead to acute myocardial infarction (AMI), even in individuals without significant atherosclerotic risk factors. Simultaneous multivessel coronary spasm is a rare clinical presentation that poses significant diagnostic and therapeutic challenges, with the potential for life-threatening complications.
Case Report: We report a case of a 42-year-old male with no history of hypertension, diabetes, or dyslipidemia who presented with sudden-onset retrosternal chest pain radiating to the left arm and jaw, associated with diaphoresis. The electrocardiography (ECG) demonstrated ST-segment elevation in the inferior leads with reciprocal changes, while cardiac biomarkers confirmed myocardial injury. Urgent coronary angiography revealed diffuse spasm in both the right coronary artery and obtuse marginal artery without significant atherosclerotic lesions, which resolved after intracoronary nitrate administration. Management included sublingual nitroglycerin, calcium channel blockers, and lifestyle modifications. The patient remained thermodynamically stable during hospitalization, with no recurrence of symptoms.
Conclusion: Simultaneous multivessel CAS is a rare but important cause of AMI, particularly in younger patients without typical risk factors. Early diagnosis and treatment are key, and this case underscores the need for greater awareness and research into its management.
Keywords: coronary vasospasm, coronary arteries, ECG, calcium channel blockers, vasodilators
Introduction
Acute myocardial infarction (AMI) is most commonly caused by atherosclerotic plaque rupture leading to coronary artery occlusion.1 However, coronary artery spasm (CAS) is a less common but significant cause of acute myocardial infraction (AMI), capable of triggering severe myocardial ischemia, arrhythmias, and even sudden cardiac death.2,3 While CAS usually affects a single coronary artery, simultaneous multivessel involvement is rare and can lead to extensive myocardial injury.4,5 This case report presents a 42-year-old male who developed AMI due to simultaneous multivessel coronary spasm, emphasizing the clinical presentation, diagnostic challenges, and management of this uncommon condition.
Case Presentation
A 42-year-old male with no prior history of hypertension, diabetes, or dyslipidemia, presenting with sudden-onset, severe retrosternal chest pain that occurred at rest and lasted for approximately 20 minutes which radiating to the left arm and jaw, accompanied by diaphoresis and mild shortness of breath. His social history revealed occasional smoking and tobacco consumption, with no significant family history of coronary artery disease.
On examination, he appeared alert but in discomfort due to chest pain. His blood pressure was 135/85 mmHg, heart rate 72 bpm, respiratory rate 18 breaths per minute, and oxygen saturation 98% on room air. Cardiovascular examination revealed normal heart sounds without murmurs, and there was no jugular venous distension. Respiratory examination was unremarkable with clear breath sounds bilaterally. Neurological examination showed no focal deficits.
An initial ECG (Figure 1) demonstrated ST-segment elevation in the inferior leads (II, III, aVF) with reciprocal changes in leads I and aVL. Cardiac biomarkers were mildly elevated, with troponin-I suggesting myocardial injury and an increase in CK-MB levels. Bedside echocardiography showed mild hypokinesia of the inferior wall, but overall left ventricular function remained preserved with an estimated ejection fraction of 55%. In light of the ECG findings and elevated cardiac biomarkers, urgent coronary angiography was performed. The patient received a loading dose of aspirin (300 mg) and atorvastatin (40 mg). Intravenous fluids were administered for hydration, and oxygen was provided as needed. Angiography revealed diffuse coronary artery spasm in both the right coronary artery (Figure 2A) and the obtuse marginal artery (Figure 2B), which resolved after intracoronary nitrate administration (Figure 2C).
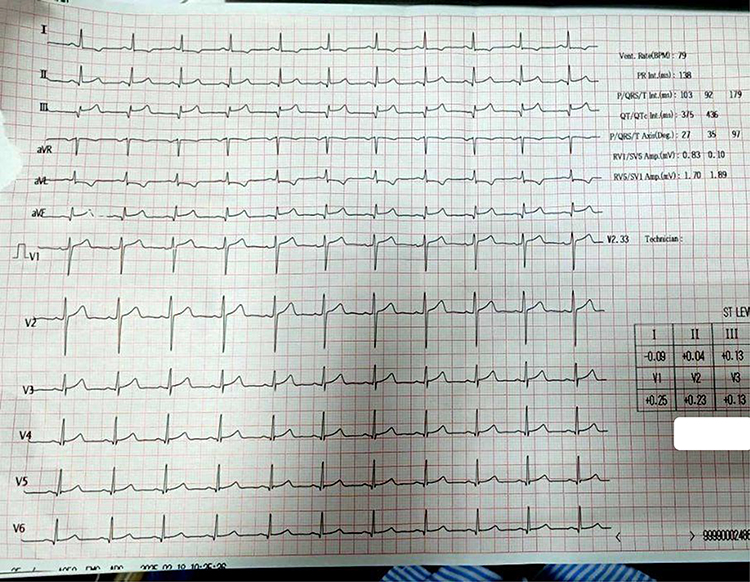 |
Figure 1 ECG showing ST-segment elevation in inferior leads (II, III, aVF) with reciprocal changes in leads I and aVL. |
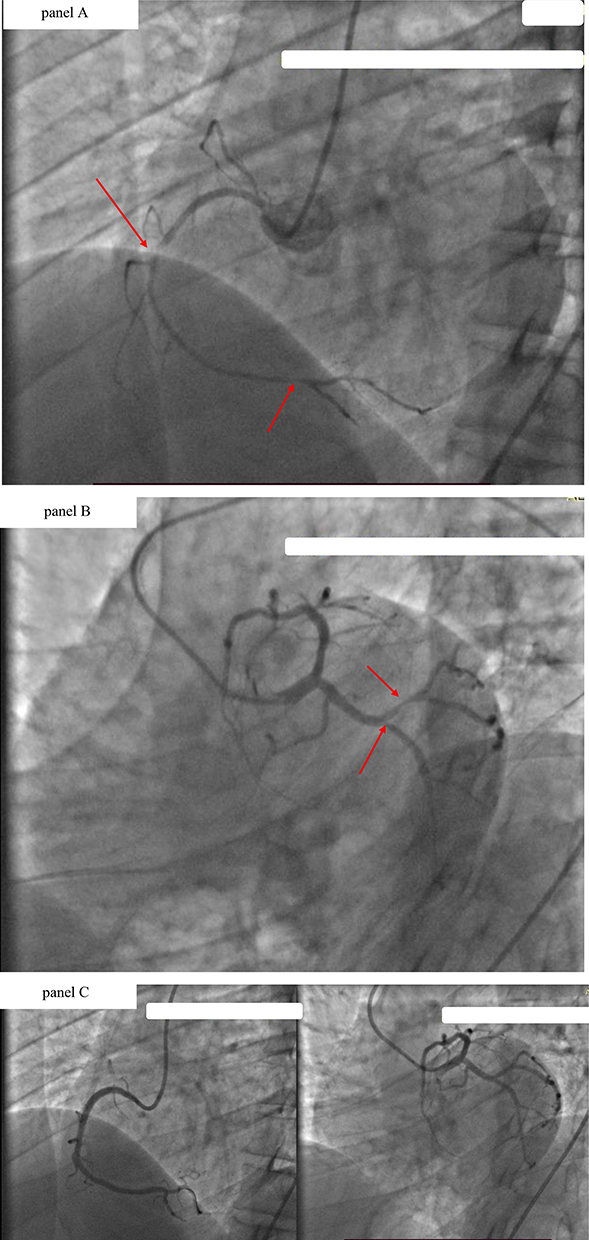 |
Figure 2 (A) Coronary angiography showing diffuse spasm in the right coronary artery. (B) Coronary angiography showing diffuse spasm in the obtuse marginal artery. (C) Post-nitrate angiography showing normal coronary arteries without significant stenosis. |
The patient was diagnosed with an acute myocardial infarction due to simultaneous multivessel coronary spasm. He was promptly treated with sublingual nitroglycerin for immediate symptom relief, followed by an intravenous infusion of the calcium channel blocker diltiazem to prevent further vasospasm.
The patient was advised to adopt lifestyle modifications, including smoking cessation, stress management, and regular exercise, while avoiding triggers such as cold exposure, stimulants, and excessive alcohol. He remained hemodynamically stable during hospitalization and was discharged after 24 hours of monitoring, with a favorable prognosis contingent on treatment adherence. His discharge medications included diltiazem 60 mg three times daily, sublingual nitroglycerin 0.5 mg as needed for chest pain, and pantoprazole 40 mg once daily.
This case emphasizes recognizing coronary vasospasm as a cause of AMI in low-risk patients and the importance of early vasodilator treatment and risk factor control to improve outcomes.
Discussion
Coronary artery spasm (CAS) is a transient, intense vasoconstriction of the coronary arteries that can lead to myocardial ischemia, arrhythmias, and, in severe cases, acute myocardial infarction (AMI).6 While CAS typically affects a single vessel, simultaneous multivessel coronary spasm is a rare occurrence with significant clinical implications.7 The presented case of a 42-year-old male experiencing AMI due to simultaneous multivessel coronary spasm underscores the importance of recognizing this condition in patients presenting with chest pain, especially when traditional risk factors for atherosclerosis are absent.4
The pathophysiology of CAS involves hyperreactivity of the vascular smooth muscle in the coronary arteries, leading to transient occlusion.8 Factors contributing to this hyperreactivity include endothelial dysfunction, oxidative stress, and autonomic nervous system imbalances. In some cases, external triggers such as cold exposure, stress, or certain medications can precipitate spasms.1 Interestingly, our patient had a history of occasional smoking, which is a known risk factor for CAS due to its impact on endothelial function and promotion of vasoconstriction.9
It was differentiated from thrombosis and catheter-induced spasm based on several key findings: the diagnosis of simultaneous multivessel coronary spasm (SMCS) was supported by complete resolution of diffuse narrowing in the right coronary and obtuse marginal arteries after intracoronary nitrate administration—uncharacteristic of thrombotic occlusion. Angiography revealed smooth, segmental constrictions without signs of plaque rupture, thrombus, or dissection. The patient’s lack of major cardiovascular risk factors further favored a vasospastic mechanism. Moreover, the simultaneous involvement of non-contiguous vessels and resolution without catheter repositioning made catheter-induced vasospasm unlikely.
Diagnosing CAS, particularly when multiple vessels are involved, poses a significant challenge. Standard diagnostic tools like coronary angiography may reveal normal or near-normal arteries between episodes, as spasms are transient.6 Provocative testing using agents such as acetylcholine or ergonovine during angiography can induce spasms, aiding in diagnosis.8 However, these tests carry risks and are not routinely performed. In our case, the diagnosis was confirmed during angiography by the observation of diffuse spasms in the right coronary artery (RCA) and left anterior descending (LAD) artery, which were relieved by intracoronary nitrates.4
Management of CAS involves both acute and long-term strategies. Acute episodes are typically managed with sublingual nitroglycerin, which acts as a potent vasodilator.6 For long-term prevention, calcium channel blockers (CCBs) are the mainstay of therapy, as they reduce the frequency and severity of spasms by inhibiting calcium influx into vascular smooth muscle cells. Long-acting nitrates can be added if CCBs alone are insufficient.4 Lifestyle modifications, including smoking cessation, stress management, and avoidance of known triggers, are also crucial components of management.6
The management of CAS includes both acute and long-term approaches. Acute episodes are treated with sublingual nitroglycerin, a potent vasodilator. For long-term prevention, calcium channel blockers (CCBs) are the first-line therapy, reducing spasm frequency and severity by inhibiting calcium influx into vascular smooth muscle cells. If CCBs are insufficient, long-acting nitrates may be added. Lifestyle modifications, such as smoking cessation, stress management, and avoiding known triggers, play a vital role in preventing recurrence.
The prognosis for patients with CAS is generally favorable when appropriately managed. However, the occurrence of simultaneous multivessel spasm, as seen in our patient, may portend a higher risk of adverse outcomes, including life-threatening arrhythmias and sudden cardiac death.3 Therefore, it is imperative to recognize this condition promptly and initiate appropriate therapy. Regular follow-up is essential to monitor treatment efficacy and adherence to lifestyle modifications.
Conclusion
This case highlights the importance of considering CAS in the differential diagnosis of AMI, especially in younger patients without significant atherosclerotic risk factors. Early recognition and appropriate management are vital to prevent serious complications. Further research is needed to better understand the mechanisms underlying multivessel CAS and to develop targeted therapies for this condition.
Abbreviations
RCA, Right Coronary Artery; LAD, Left Anterior Descending (coronary artery); CCB, Calcium Channel Blocker; CAS, Coronary artery spasm; ECG, electrocardiography.
Consent
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. All identifying information has been removed to protect patient confidentiality.
EthicalApproval
This case report has been thoroughly described within the article, and therefore, additional approval from the Ethics Committee was not considered necessary.
Funding
We confirm that no external funding or institutional assistance was provided for the development of this case report.
Disclosure
The authors declare no conflicts of interest related to this case report.
References
1. DIEČKUS L, Rodevič G, Baranauskas A. et al. Case report: a rare manifestation of vasospasm induced myocardial infarction with ST-segment elevation in a young male patient. Front CardiovascMed. 2023;9:1017107. doi:10.3389/fcvm.2022.1017107
2. WONG K-T, Tam C-CF, Chung T-S, et al. Coronary vasospasm presenting in a catastrophic way. Case Reports. 2024;29(18):102554. doi:10.1016/j.jaccas.2024.102554
3. Iranirad L, Sadeghi MS. A rare case of spontaneous and simultaneous multivessel coronary artery spasm leading to multisite myocardial infarction and ventricular fibrillation. ARYA Atheroscler. 2018;14(1):41–43. doi:10.22122/arya.v14i1.1683
4. Takagi Y, Yasuda S, Tsunoda R, et al. Clinical characteristics and long-term prognosis of vasospastic angina patients who survived out-of-hospital cardiac arrest: multicenter. Circulation: Arrhythmia and Electrophysiology. 2011;4(3):295–302. doi:10.1161/CIRCEP.110.959809
5. Cai H, Chen S, Wang D. Sudden diffuse spasm of multiple coronary arteries: a case report. Medicine. 2024;103(2):e36889. doi:10.1097/MD.0000000000036889
6. Diečkus D, Rodevič V, Baranauskas A, Davidavičius G, Budrys P. A rare manifestation of vasospasm-induced myocardial infarction in a young male: a case report. Front Cardiovasc Med. 2023;10:1061234.
7. Wong KT, Tam CC, Chung TS, Lau TK, Wong SF. Coronary vasospasm presenting in a catastrophic way. JACC Case Rep. 2024;6(18):102554.
8. Beltrame JF, Crea F, Kaski JC, et al. International standardization of diagnostic criteria for vasospastic angina. Eur Heart J. 2017;38(33):2565–2568. doi:10.1093/eurheartj/ehv351
9. Hung M-J, Hu P, Hung M-Y. Coronary artery spasm: review and update. Int J Med Sci. 2014;11(11):1161–1171. doi:10.7150/ijms.9623
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.