")
Back to Journals » Journal of Pain Research » Volume 18
Spectral Analysis of Bioelectrical Activity in Experimentally Provoked Referred Pain – Motor Alterations Related to the Network of Trigger Points
Authors Konieczny M , Matuska J, Domaszewski P , Pakosz P, Herrero P , Santafe MM , Wotzka D , Zmarzły D, Skorupska E
Received 20 June 2024
Accepted for publication 25 February 2025
Published 26 March 2025 Volume 2025:18 Pages 1657—1666
DOI https://doi.org/10.2147/JPR.S475606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Mariusz Konieczny,1 Jakub Matuska,2 Przemysław Domaszewski,3 Paweł Pakosz,1 Pablo Herrero,4 Manel M Santafe,5 Daria Wotzka,6 Dariusz Zmarzły,6 Elżbieta Skorupska2
1Faculty of Physical Education and Physiotherapy, Opole University of Technology, Opole, Poland; 2Department of Physiotherapy, Poznan University of Medical Sciences, Poznan, Poland; 3Department of Health Sciences Institute of Health Sciences, University of Opole, Opole, Poland; 4Faculty of Health Sciences, IIS Aragon, University of Zaragoza, Zaragoza, Spain; 5Unit of Histology and Neurobiology, Department of Basic Medical Sciences, Faculty of Medicine and Health Sciences, Rovira I Virgili University, Reus, Spain; 6Faculty of Electrical Engineering, Automatic Control and Informatics, Opole University of Technology, Opole, Poland
Correspondence: Mariusz Konieczny, Email [email protected]
Purpose: This study investigates bioelectrical changes in thigh muscles associated with referred pain following noxious stimulation of the gluteus minimus, focusing on understanding motor alterations related to the network of trigger points. While previous research suggested atypical autonomic activity, motor alterations in referred pain areas remain understudied. Thus, our aim was to investigate motor alternations using spectral analysis.
Methods: Sixty-three participants were selected based on tests for atypical autonomic reactivity within the referred zone. The control group (CON) comprised 15 out of 48 healthy volunteers with negative test results, while the experimental group (EXP) included 13 out of 15 Polish national Short Track athletes with positive test results. They underwent a 10-minute surface electromyography session during gluteus minimus dry needling. Power spectral density analysis was then applied to assess the obtained signals.
Results: Significant statistical differences in power spectral density were observed between the EXP and CON groups in thigh muscles, while no statistical differences were found in the pelvic girdle muscles. The most notable atypical bioelectrical activity was observed in the vastus lateralis, semitendinosus, and rectus femoris muscles.
Results Importance: Visualization of motor alterations related to the trigger point network in the thigh due to noxious stimulation of the gluteus minimus trigger points.
Conclusion: Noxiously provoked referred pain from the gluteus minimus muscle, confirmed by abnormal autonomic activity, is characterized by motor alternations of the thigh muscles, suggesting a network of latent trigger points. Further studies exploring this observed phenomenon for both active and latent trigger points can provide new insights into myofascial pain syndrome.
Keywords: myofascial pain syndrome, trigger points, surface electromyography, satellite trigger point
Introduction
Myofascial pain syndrome (MPS), provoked by trigger points (TrPs) is classified as a subtype of soft tissue rheumatism.1 For years, this syndrome has been overlooked or ignored. Nowadays, it is becoming more widely accepted, even by the WHO.2 Referred pain is a phenomenon related to MPS for both types of TrPs: active, defined as spontaneous referred pain recognized by pain patients, and latent, where referred pain must be mechanically or noxiously provoked.3 In Travell’s concept,3 both latent and active TrPs can cause three types of alterations present in the area of referred pain: autonomic, motor and sensory. Additionally, she postulated a network of trigger points found in patients with active TrPs, eg gluteus minimus, characterized by an extensive number of satellite TrPs.
Our previous studies demonstrated atypical autonomic nervous system (ANS) involvement in the referred pain zone for both active and latent trigger points, manifested by amplified vasomotor activity due to noxious stimulation of the gluteus minimus muscle exclusively.4–8 We find it interesting to explore whether subjects with referred pain confirmed by atypical ANS activity might also exhibit additional phenomena, such as motor disturbances related to the referred pain. Our purpose was to determine whether atypical motor activity could first be observed in latent trigger points due to noxious gluteus minimus stimulation to detect the hypothetically posited motor alterations. The hypothesis of a network of latent trigger points in individuals with highly overloaded muscles was also postulated.3 Its existence, accompanied by motor alterations, is supported by empirical studies from other authors, who have confirmed that, for example, latent trigger points are characterized by altered kinematics, muscle activation, muscle fatigue, and decreased strength.9–13 It is further supported by Fernandez-Carnero et al, who indicated that noxious stimulation of latent TrPs in the infraspinatus increased motor activity in TrPs of distant muscles at the same segmental level.14 Moreover, it has been confirmed that the lower extremities of athletes are more affected by an extensive number of latent trigger points compared to people with a sedentary lifestyle.15 Short-track athletes who overuse lower limbs (mainly left) muscles and short hip rotators that stabilize the hips during skating (eg gluteus minimus) are particularly suited for this study.16–18 Moreover, our previous research confirmed an increased prevalence of latent TrPs in the left leg of Short Track athletes.19 As a control group, we selected young individuals not engaged in sports, who are unlikely to exhibit TrPs network related to gluteus minimus.
Spectral analysis breaks down bioelectric signals into frequency components to identify specific patterns of muscle activity patterns. In this study, for the very first time we used this method to visualize motor changes by analyzing sEMG signals during noxious stimulation of the gluteus minimus, exploring bioelectrical activity in response to induced referred pain. We hypothesize that bioelectrical activity is connected with a network of trigger points. Hence, the aim of this study is to investigate motor alterations in individuals with experimentally induced referred pain, confirmed by an atypical ANS response.
Materials and Methods
Study Design
The study was conducted from January to March 2023 in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Poznan University of Medical Sciences (Resolution No 110/22 of 10 March 2022). Trial registration: 20/07/2022, Trial Id: ACTRN12622001016729. Before the examination, all participants expressed written informed consent to participate in the study. At the same time, a detailed description of all tests was provided to participants with the right to refuse to undergo the dry needling procedure and withdraw from the study at any time.
Referred pain of the gluteus minimus muscle was defined by Travell and Simons20 and can be elicited from the trigger point, usually by dry needling, but less often through deep palpation.20 The mechanically evoked-referred pain/sensation can be confirmed by a newly established test (Skorupska Protocol – SP® test) being positive if abnormal autonomic phenomenon (amplified vasomotor response defined as percentage size intensive vasodilatation above the cut-off at rest) within the muscle referred zone is confirmed.7 SP® test was conducted according to the protocol outlined in Skorupska et al paper.8 Noxiously provoked referred pain is necessary for a positive SP test®, which in turn is associated with the occurrence of vasomotor reaction. The thigh was confirmed as a diagnostic zone to establish positive/negative results of the autonomic abnormal activity for the gluteus minimus muscle.5 Hence, we decided to use the SP® test to confirm the presence of the referred pain objectively. Regarding this, participants were included or excluded into groups based on the SP test® results, as we aim to assess motor reaction in individuals with confirmed referred pain.
Short-track athletes with a positive SP test® were chosen because they are prone to having a network of TrPs, which we hypothesize to be a potential source of bioelectrical activity. To provide a meaningful comparison, we included healthy non-athletes who tested negative on the SP test® as the control group, as they did not present either referred pain or a TrPs network. This group selection allowed us to examine the conditions under which motor responses occur effectively.
At first we examined the thigh zone towards abnormal autonomic activity, mainly vasodilatation, due to dry needling of the gluteus minimus. Based on the result of the SP test®, participants were included or excluded from the EXP (experimental) and CON (control) groups. The second examination was the surface EMG (sEMG) assessment of the thigh with dry needling of the gluteus minimus muscle, which was stimulated to examine the existence of abnormal motor activity in the thigh area, as well as if any referred pain/sensations were associated to it. The flow chart presenting the study design is shown in Figure 1.
 |
Figure 1 Flow diagram of the study design. |
Participants
At first, recruited participants were asked to fill out the form that allowed us to exclude those who did not meet the criteria. Then, during the in-person meeting, the criteria were verified. Sixty-three healthy subjects (n=63), divided into an EXP group formed by members of the Polish national Short-Track team (n=15), and a CON group formed by healthy volunteers (n=48) were assessed for eligibility. The inclusion criteria were as follows: (1) general good health condition (pain-free, without any medical diagnosis of permanent disease or surgery in the past, current fever, or infection); 2) age between 18 and 30 (inclusive); 3) both lower limbs present 4) SP test results: (i) positive for EXP and (i) negative for CON.
Subjects were excluded if they presented any lower limb injuries, scoliosis, inflammation, autoimmune diseases, anxiety due to needles, previous back surgery, spinal tumors or pregnancy.
Finally, thirteen elite athletes (n=13) aged 18.5 ± 1.5 years, participated in the EXP group study. The athletes had at least ten years of competitive experience and were participating in professional training at the time of the study. The CON group comprised fifteen (n=15) young healthy volunteers aged 19.5 ± 1.6 years (Figure 1).
Testing Procedure of the Surface EMG in the Thigh Muscles During 10 minutes of Dry Needling in the Gluteus Minimus Muscle
The left limb underwent diagnostic examination for EXP and CON groups, as per previous studies regarding the asymmetric overload disorder of the Short Track athletes’ left lower limb.19 Then, another researcher prepared the skin, and electrodes and sensors were attached. A 16-channel sEMG system (NORAXON DTS) was used to record signals at a sampling rate of 1500 hz. During the signal recording, a Lowpass 500 filter was used, designated by the manufacturer in the hardware setup of the NORAXON DTS – Belt Receiver. Signal processing was performed using NORAXON MR-XP 1.07 Master Editions software. The signal processing in the presented software involved saving files in the MATLAB system, and no normalization was applied, as the raw sEMG signal was analyzed for Power Spectral Density. The processing procedure is described in the section “Power Spectral Density analysis of the sEMG signal”.
The signal and the procedure were performed by an experienced researcher. The skin was cleaned to prepare the muscles for analysis, and electrodes (Ag/AgCl) were applied according to the SENIAM method21. Sensors and electrodes were placed on the following muscles: gluteus medius, gluteus maximus, vastus lateralis, rectus femoris, vastus medialis, adductor longus, biceps femoris and semitendinosus. Then, the bioelectrical activity of the eight mentioned muscles was measured during the ten minutes of dry needling in the gluteus minimus. The initiation of dry needling coincided with the commencement of EMG signal recording. Both dry needling and EMG signal measurements were conducted by two independent specialists with extensive experience. Furthermore, the physiotherapists who performed dry needling did not have real-time access to the EMG signal. After 10 minutes, when the needle was stopped, the EMG measurement was terminated.
Dry Needling Procedure
The participants received dry needling (DN) stimulation in the gluteus minimus muscle. The other extremity did not receive any intervention. The presence of trigger points using conservative clinical criteria is impossible for the gluteus minimus muscle due to the deep location. Then, according to Travel&Simons and the Delphi criteria, TrPs spot tenderness (which can be clearly localized) and referred pain/sensation were selected for trigger points diagnosis.22
For the EXP and the CON groups, the gluteus minimus was examined towards motor response from the two most painful sensitive spots with/without referred pain presence examined previously by SP® test. All participants received diagnostic long-lasting dry needling according to the fast-in fast-out technique by Hong23 with 0.30 mm diameter, 60 mm long sterile acupuncture needles SEL (Serin Corp, Shizuoka, Japan). The skin was disinfected with an antiseptic. Then, each of the examined points was needled for 5 minutes, resulting in a total stimulation of 10 minutes for each participant.
Power Spectral Density Analysis of the sEMG Signal
A set of scripts were developed in the Matlab environment to analyse data measurement. In particular, sEMG data were analyzed in both the CON and EXP groups. The sampling frequency was 1500 hz. Samples are designated into 10 segments corresponding to specific activities, activities, and subsequent SP-test stages. A periodogram was determined for each of the 10 segments. The periodogram is an estimate of the spectral density of a signal. It’s derived from the Fourier Transform, specifically the Discrete Fourier Transform (DFT) for digital signals. The basic formula for a periodogram I(f) of a signal EMG with N samples is:

where S(f) is the DFT of EMG
Window of length 64 was used. In each window the estimated spectrum was scaled by the equivalent noise bandwidth (in Hz) of the window to estimate of the power at each frequency.
DFT converts a sequence of values, representing a time-domain signal, into components of different frequencies, providing a frequency-domain representation of the signal.

or k=0,1,2,…,N−1
S[k] represents the DFT output and is a sequence of complex numbers.
EMG[n] is the input time-domain sequence of EMG data
Obtained power values were limited to 100 dB before averaging and to 30 dB for averaged spectra.
As a result of the conducted signal analysis, the average power spectral density (PSD) value presented on the spectrograms for each muscle in individual groups was determined.
Statistical Analysis
The normality of the distribution of the PSD variables was assessed using the Shapiro–Wilk test. Due to the non-normal distribution of the data, the Mann–Whitney U-test was employed to evaluate statistically significant differences between the values of the PSD variable across all muscles. The significance level was set at P ≤ 0.05. The data collected was analysed using StatsCloud software (https://statscloud.app/beta/).
Due to the innovative character of the study (without previous data), the sensitivity power analysis was conducted in GPower 3.1.9.7. The sample size of 28 (EXP = 13 and CON = 15) participants in 2 groups is sensitive enough to detect effect size r = 0.5 or larger (with 80% power and 5% significance level, two-sided) was calculated. The effect size values calculated for each variable are presented in Table 1.
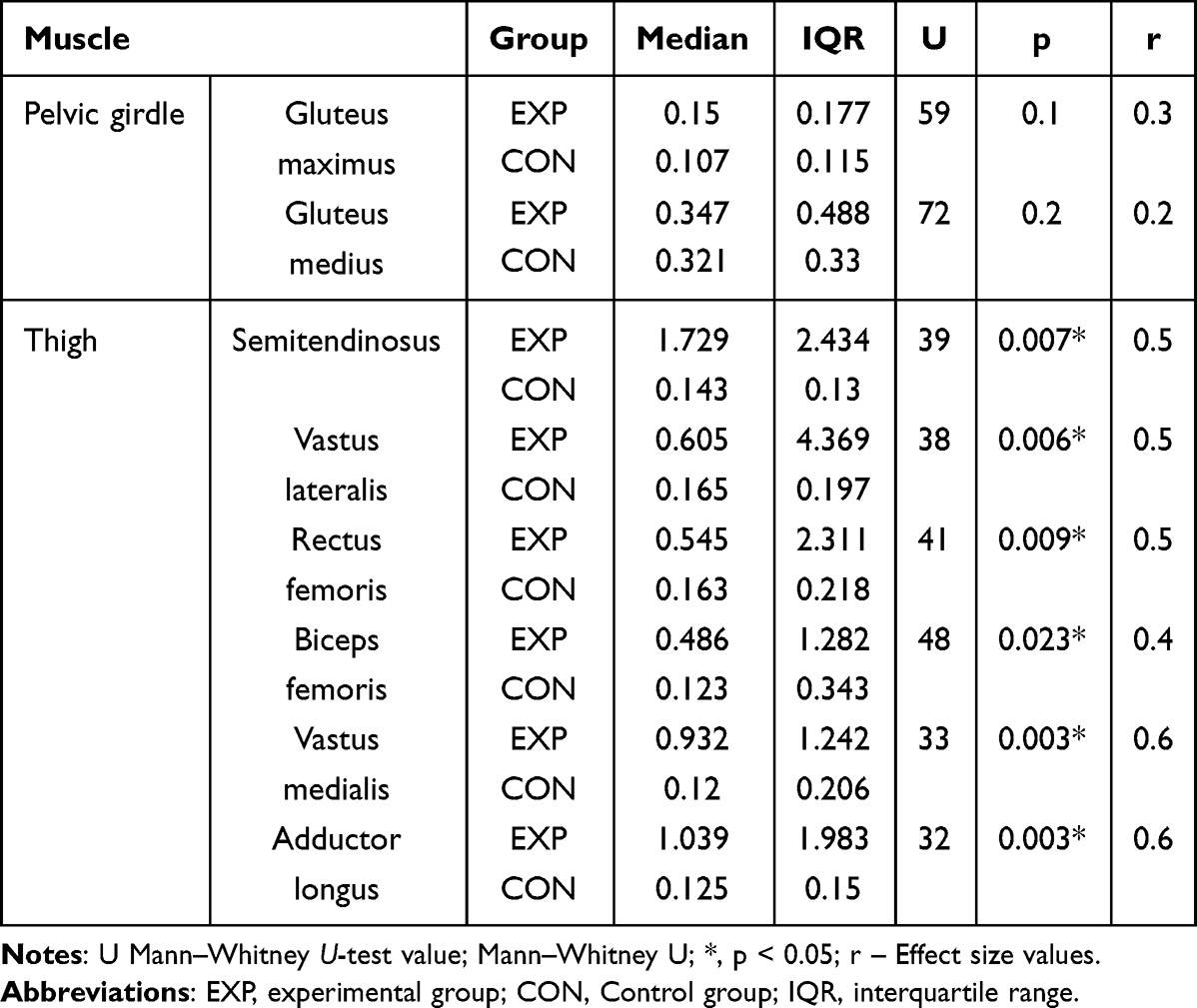 |
Table 1 Estimation of the Power Spectral Density of sEMG Muscles Response Signals in the Thigh in Response to Gluteus Minimus Muscle Noxious Stimulation |
Results
The EXP group showed statistically significant differences in the level of PSD in the thigh muscles compared to the control group (Table 1), with no statistically significant differences in the pelvic girdle muscles (gluteus maximus and gluteus medius). In the EXP group, the highest median and interquartile range SPD values (visible in the spectrograms - Figure 2) were observed in the semitendinosus and the vastus lateralis muscles. The detailed description of the PSD of individual muscles presented below (paragraph 3.1) can be observed on the spectrograms placed in Figure 2.
 |
Figure 2 Power spectral density spectrograms reflected the presence of the referred motor phenomenon within thigh muscles due to long-lasting dry needling of the gluteus minimus muscle. The figure illustrates changes in the Power Spectral Density (PSD) over time in response to needle mechanical stimulation of the gluteus minimus across eight different muscles: gluteus maximus, gluteus medius, semitendinosus, vastus lateralis, rectus femoris, biceps femoris, vastus medialis, and adductor longus. (PSD - is the measure of signal’s power content versus frequency and reflects changes in the power of the bioelectric signal produced by mechanical stimulation of referred pains). The Y-axis represents the frequency at which the PSD values occur. The X-axis indicates the time of the intervention during which electromyography was conducted. A colour bar on the right side of the figure provides a scale for the PSD values, which are indicated on the spectrogram. In the experimental group (labeled EXP, which includes individuals with positive referred pain), there are notable changes in the average PSD over time. Conversely, in the control group (labeled CON, consisting of individuals without referred pain), there are minimal or no changes in the average PSD. |
Detailed Power Spectral Density Analysis of the Examined Muscles
Pelvic Girdle Area
For the gluteus maximus muscle, very weak activity was observed for frequencies below 10 hz in both groups, without significant differences between them (Table 1; U = 59, p = 0.076).
For the gluteus medius muscle, in the EXP group, a PSD was observed from minute 5 to 9 extending to about 50 hz, whereas, in the CON group, very weak activity was observed for frequencies below 10 hz, without significant differences between groups (Table 1; U = 72, p = 0.240).
Thigh Area
In the CON group, very weak activity was observed for frequencies below 10 hz in all muscles. Across the remaining frequencies (from 0 to 750 hz), there was an absence of activity.
For the semitendinosus muscle, in the EXP group, a PSD reflected the presence of the referred motor phenomenon since the start to the minute 7 for frequencies ranging from 0 to 150 hz, whereas for frequencies around 50 hz only weak energy was observed at minute 10, showing significant differences with the CON group (Table 1; U = 39, p = 0.007).
For the vastus lateralis muscle, in the EXP group, a PSD reflected the presence of the referred motor phenomenon from minute 0 to 5 for frequencies ranging from 0 to 110 hz and from minute 6 to 9 for irregular frequencies ranging from 0 to 80 hz, with significant differences between groups (Table 1; U = 38, p = 0.006).
For the rectus femoris muscle, in the EXP group a PSD reflected the presence of the referred motor phenomenon from minute 2 to 5 for frequencies ranging from 0 to 80 hz and at minute 7 for frequencies around 10 hz, with significant differences between groups (Table 1; U = 41, p = 0.009).
For the biceps femoris muscle, in the EXP group, a PSD reflected the presence of the referred motor phenomenon from minute 0 to 6 for frequencies ranging from 0 to 100 hz, with significant differences between groups (Table 1; U = 48, p = 0.023).
For the vastus medialis muscle, in the EXP group, a PSD reflected the presence of the referred motor phenomenon from minute 0 to 3 and about minute 5 for frequencies ranging from 0 to about 25 hz, with significant differences between groups (Table 1; U = 33, p = 0.003).
For the adductor muscle, in the EXP group, a PSD reflected the presence of the referred motor phenomenon from minute 3 to 5 and from minute 7 to 10 for frequencies ranging from 0 to 50 hz, with significant differences between groups (Table 1; U = 32, p = 0.003).
Discussion
This is the first study presenting an objective confirmation of the atypical, distant motor phenomenon in the thigh area, provoked by mechanical stimulation of trigger points in the gluteus minimus muscle. The observed abnormal motor phenomenon was characterised by selective and time variable values of the PSD during the procedure, but solely for those cases with referred pain. Vastus lateralis, semitendinosus and rectus femoris, which are located in the area of referred pain of the gluteus minimus muscle, presented the highest intensity of the power spectrum density among all examined thigh muscles.
In previous studies, EMG research focused solely on changes in bioelectrical activity within trigger point locations and therefore it is not possible to compare our results directly with previous studies. In earlier studies, mechanical trigger point stimulation under sEMG control was aimed to acquire signals in the immediate vicinity of the dry needling input13 The differences in the magnitude of bioelectrical activity near LTrPs compared to non-TrPs areas in healthy individuals were confirmed.24 Correlation between spontaneous electrical activity (SEA) at the TrPs indicates focal muscle fiber contraction and/or muscle cramp potentials within taut bands.24 Barbero et al25 utilized high-density surface EMG to examine the upper trapezius muscles in both patients with myofascial pain (with active trigger points) and asymptomatic subjects. Those authors generated topographical maps of the EMG average rectified value and peak EMG amplitude, finding that individuals with myofascial pain (active TrPs) exhibited a shift in the distribution of muscle activity compared to asymptomatic individuals. They demonstrated that the location of peak muscle activity is not correlated with the location of the TrPs, which is aligned with our results, which significantly expand the understanding of this phenomenon by revealing increased muscle activity not directly associated with the location of the TrPs.
The Probable Explanation of the Referred Motor Phenomenon
According to Travell, sensory, autonomic and motor phenomena can be observed within trigger points referred pain area. Bin Pai et al26 indirectly confirmed TrPs’ impact on sensory phenomena using QST to show that TrP therapy reduces hyperalgesia in referred pain areas. Amibte-Quesada et al27 also used QST to identify sensory disturbances in asymptomatic volunteers’ TrPs-related zones, finding pinprick and vibration hypoesthesia in the area of referred pain. Regarding autonomic alterations, our previous study confirmed abnormal autonomic activity solely due to mechanically induced referred pain from both active and latent TrPs.6,8 Thus, our current study sheds light on a new aspect: the latent TrPs’ motor responses.
The motor phenomenon observed in the presented cases can reflect the link between the TrPs and the so-called satellite TrPs.3 Autonomic response to DN showed dependency between the DN duration and the intensity of the phenomenon, which was not observed for the motor response since the bioelectrical muscle activity was only observed immediately at the moment of the reported referred pain. We also registered that the signal’s power significantly decreased at the moment of intervention interruption in the fifth minute, associated with a needle change, demonstrating the discontinuous occurrence of the described phenomenon. Similarly, irregularities associated with fluctuations in the level of PSD that reflected the presence of the referred motor phenomenon in individuals’ muscles were observed, which we refer to in the limitations section. These results may suggest specific sensory-motor control alterations related to TrPs, implying that TrPs-related pain is associated with increased activity of motor units and/or excitability of motor units.
All of these findings support the hypothesis regarding the possible involvement of the central nervous system in the referred sensation and/or pain from trigger points. Further studies exploring motor phenomena associated with both latent and active trigger points are demanded on a larger group of subjects.
Clinical Importance
Current findings together with abnormal autonomic activity can allow the development of new diagnostic protocols for objective trigger point diagnosis in the future. Apart from the obvious target group of patients with myofascial pain, we can find other results that can be translated into clinical practice. Lastly, the clinical relevance of the latent trigger points for the athletes was suggested,13,28 since they can provoke muscle motor alternations, fatigue or pain in case they are activated through many different reasons. The EXP group, comprising Short Track athletes was chosen due to the confirmed overrepresentation of latent TrPs in the lower extremities.19 Regarding the highest PSD activity observed in the thigh muscles of the EXP group, it is clinically relevant to consider the vastus lateralis muscle, since this is involved in leg control during asymmetric movement on the ice. Additionally, we can speculate that the athletes´ position and movement on the ice, which overuse the short hip rotators, can provoke similar motor activity to the gluteus minimus muscle, leading to the development of satellite TrPs and therefore provoking fatigue and other muscle alternations.
Furthermore, the objective confirmation of the latent TrPs can enhance the medical service for athletes. Trybulski et al investigated martial arts athletes and proposed that targeted therapy for latent TrPs could enhance muscle power. These findings support Devereux et al28 who observed an increase in vertical jump height up to 48 hours post-intervention. Additionally, certain authors have reported enhanced gluteus medius force and reduced muscle fatigue in the general healthy population.13,29 Das et al9 demonstrated that latent trigger points can restrict range of motion, while Haser et al30 found that DN treatment of TrPs in elite soccer players led to increased hip flexion range of motion and greater knee extensor force after a 4-week follow-up. However, the influence of trigger points localized in the hip girdle on the lower limb remains to be established.
The motor phenomenon observed in our study suggests the potential for objectively assessing alterations caused by TrPs-related referred pain, particularly in elite athletes. This holds the promise for analysing whether the cause of motor dysfunction extends beyond the affected muscle and might predispose to injury due to changes in sports performance.
Limitations
Despite being innovative, our study has some limitations. First of all, the sample size group was small. However, due to the experimental nature of the study and the robust, indisputable results of spectral analysis, we decided to include as small a sample as possible. We conducted sensitivity power analyses to justify our results. The calculations proved that our group was large enough to detect a large effect, which we indicated. The group should be larger in the future, and its size will be calculated a priori based on the obtained results. Secondly, we have not measured the exact time of the reported referred pain, eg decline and reoccurrence in time during the procedure, so we cannot make a statement if the referred motor sensation occurred at the same time as the referred pain. Lastly, the position where the participants were tested and the pain stimulation was performed could have induced activity in the adductor longus muscle.
Conclusion
Noxiously provoked referred pain from the gluteus minimus muscle, confirmed by abnormal autonomic activity, is characterized by motor alterations in the thigh muscles, indicating the presence of a network of latent trigger points. Future studies should include larger sample sizes and consider simultaneously tracking both patient sensations and motor responses, focusing on both active and latent trigger points to confirm the current findings. This approach could provide new insights into myofascial pain syndrome (MPS) and open opportunities for objectifying its assessment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Benzon H, N. Raja S, Fishman SM, S Liu S, P Cohen S. Essentials of Pain Medicine.
2. WHO guideline for non-surgical management of chronic primary low back pain in adults in primary and community care settings. 2023. https://www.ncbi.nlm.nih.gov/books/NBK599212/.
3. Travell JG, Simons DG. Travell, Simons & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual.
4. Skorupska E, Dybek T, Rychlik M, Jokiel M, Zawadziński J, Dobrakowski P. Amplified vasodilatation within the referred pain zone of trigger points is characteristic of gluteal syndrome{\textemdash}a type of nociplastic pain mimicking sciatica. J Clin Med. 2021;10(21):5146. doi:10.3390/jcm10215146
5. Skorupska E, Dybek T, Rychlik M, Jokiel M, Dobrakowski P. The automatization of a new thermography method using invasive nociceptive stimulation to confirm an autonomic phenomenon within a trigger point referred pain zone. Brain Sci. 2021;11(7):893. doi:10.3390/brainsci11070893
6. Skorupska E, Jokiel M, Rychlik M, Łochowski R, Kotwicka M. Female overrepresentation in low back-related leg pain: a retrospective study of the autonomic response to a minimally invasive procedure. J Pain Res. 2020;13:3427–3435. doi:10.2147/JPR.S282233
7. Skorupska E, Rychlik M, Samborski W. Validation and test-retest reliability of new thermographic technique called thermovision technique of dry needling for gluteus minimus trigger points in sciatica subjects and {TrPs}-negative healthy volunteers. Biomed Res Int. 2015;2015:1–11. doi:10.1155/2015/546497
8. Skorupska E, Dybek T, Rychlik M, et al. A potential objective sign of central sensitization: referred pain elicited by manual gluteus minimus muscle exploration is coincident with pathological autonomic response provoked by noxious stimulation. Pain Res Manag. 2023;2023:1–11. doi:10.1155/2023/4030622
9. Das R, Jhajharia B, Ciocan VC, Majumdar I, Sharma A. The relationship between latent myofascial trigger point and range of motion of knee flexor and extensor muscles. Physical Educ Theory Methodol. 2023;23(2):192–198. doi:10.17309/tmfv.2023.2.06
10. Ge HY, Monterde S, Graven-Nielsen T, Arendt-Nielsen L. Latent myofascial trigger points are associated with an increased intramuscular electromyographic activity during synergistic muscle activation. J Pain. 2014;15(2):181–187. doi:10.1016/j.jpain.2013.10.009
11. Ibarra JM, Ge HY, Wang C, Martínez Vizcaíno V, Graven-Nielsen T, Arendt-Nielsen L. Latent myofascial trigger points are associated with an increased antagonistic muscle activity during agonist muscle contraction. J Pain. 2011;12(12):1282–1288. doi:10.1016/j.jpain.2011.09.005
12. Ge HY, Arendt-Nielsen L, Madeleine P. Accelerated muscle fatigability of latent myofascial trigger points in humans. Pain Med. 2012;13(7):957–964. doi:10.1111/j.1526-4637.2012.01416.x
13. Sánchez-Infante J, Bravo-Sánchez A, Esteban-García P, Jiménez F, Abián-Vicen J. Changes in electromyographic activity of latent trigger points after a dry needling intervention: a randomised controlled trial. Physiotherapy. 2022;117:72–80. doi:10.1016/J.PHYSIO.2022.09.002
14. Fernández-Carnero J, Ge HY, Kimura Y, Fernández-De-Las-Peñas C, Arendt-Nielsen L. Increased spontaneous electrical activity at a latent myofascial trigger point after nociceptive stimulation of another latent trigger point. Clin J Pain. 2010;26(2):138–143. doi:10.1097/AJP.0b013e3181bad736
15. Zuil-Escobar JC, Martínez-Cepa CB, Martín-Urrialde JA, Gómez-Conesa A. The prevalence of latent trigger points in lower limb muscles in asymptomatic subjects. PM & R. 2016;8(11):1055–1064. doi:10.1016/j.pmrj.2016.03.005
16. Konieczny M, Pakosz P, Witkowski M. Asymmetrical fatiguing of the gluteus maximus muscles in the elite short-track female skaters. BMC Sports Sci Med Rehabil. 2020;12(1). doi:10.1186/S13102-020-00193-W
17. Pakosz P, Konieczny M. Training induced fatigability assessed by sEMG in Pre-Olympic ice-skaters. Sci Rep. 2020;10(1). doi:10.1038/S41598-020-71052-4
18. Konieczny M, Matuska J, Pakosz P, et al. Resting muscle tension and trigger points in elite junior short-track athletes and healthy non-athletes: a cross-sectional examination. Front Sports Act Living. 2024;6:1412412. doi:10.3389/FSPOR.2024.1412412/BIBTEX
19. Konieczny M, Skorupska E, Domaszewski P, Pakosz P, Skulska M, Herrero P. Relationship between latent trigger points, lower limb asymmetry and muscle fatigue in elite short-track athletes. BMC Sports Sci Med Rehabil. 2023;15(1):1–6. doi:10.1186/S13102-023-00719-Y/FIGURES/2
20. Travell JG, Simons DG. Myofascial Pain and Dysfunction: The Trigger Point Manual; Vol. 2. The Lower Extremities.
21. Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. 2000;10(5):361–374. doi:10.1016/S1050-6411(00)00027-4
22. Fernández-de-las-Peñas C, Dommerholt J. International consensus on diagnostic criteria and clinical considerations of myofascial trigger points: a delphi study. Pain Med. 2018;19(1):142–150. doi:10.1093/PM/PNX207
23. Hong CZ. Lidocaine injection versus dry needling to myofascial trigger point: the importance of the local twitch response. Am J Phys Med Rehabil. 1994;73(4):256–263. doi:10.1097/00002060-199407000-00006
24. Ge HY, Fernández-de-las-Peñas C, Yue SW. Myofascial trigger points: spontaneous electrical activity and its consequences for pain induction and propagation. Chin Med. 2011;6:13. doi:10.1186/1749-8546-6-13
25. Barbero M, Falla D, Mafodda L, Cescon C, Gatti R. The location of peak upper trapezius muscle activity during submaximal contractions is not associated with the location of myofascial trigger points: new insights revealed by high-density surface EMG. Clin J Pain. 2016;32(12):1044–1052. doi:10.1097/AJP.0000000000000373
26. Yu M, Pai B, Toma JT, et al. General Section Dry needling has lasting analgesic effect in shoulder pain: a double-blind, sham-controlled trial. 2021. doi:10.1097/PR9.0000000000000939.
27. Ambite-Quesada S, Arias-Bur\’\ia JL, Courtney CA, Arendt-Nielsen L, Fernández-de-las-Peñas C. Exploration of quantitative sensory testing in latent trigger points and referred pain areas. Clin J Pain. 2018;34(5):409–414. doi:10.1097/ajp.0000000000000560
28. Devereux F, O’rourke B, Byrne PJ, Byrne D, Kinsella S. EFFECTS OF MYOFASCIAL TRIGGER POINT RELEASE ON POWER AND FORCE PRODUCTION IN THE LOWER LIMB KINETIC CHAIN. J Strength Cond Res. 2019;33(9):2453–2463. doi:10.1519/JSC.0000000000002520
29. Schneider E, Moore ES, Stanborough R, Slaven E. Effects of trigger point dry needling on strength measurements and activation levels of the gluteus medius: a quasi-experimental randomized control study. Int J Sports Phys Ther. 2022;17(7). doi:10.26603/001C.55536
30. Haser C, Stöggl T, Kriner M, et al. Effect of dry needling on thigh muscle strength and hip flexion in elite soccer players. Med Sci Sports Exerc. 2017;49(2):378–383. doi:10.1249/MSS.0000000000001111
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.