")
Back to Journals » Open Access Emergency Medicine » Volume 17
Spontaneous Spinal Epidural Hematoma Under Rivaroxaban and Clopidogrel: A Case Report and Literature Review
Authors Schoenmaekers B , Derraz I, Tahhan N, Metrailler P
Received 30 August 2024
Accepted for publication 31 January 2025
Published 21 February 2025 Volume 2025:17 Pages 129—135
DOI https://doi.org/10.2147/OAEM.S489072
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Bruno Schoenmaekers,1 Imad Derraz,2 Nadim Tahhan,3 Pierre Metrailler1
1Emergency Department, Centre Hospitalier du Valais Romand (CHVR), Sion, Switzerland; 2Department of Radiology, Centre Hospitalier du Valais Romand (CHVR), Sion, Switzerland; 3Neurosurgery Department, Centre Hospitalier du Valais Romand (CHVR), Sion, Switzerland
Correspondence: Bruno Schoenmaekers, Centre Hospitalier du Valais Romand (CHVR), Emergency Department, Avenue du Grand-Champsec 80, Sion, 1951, Switzerland, Email [email protected]
Abstract: Spontaneous spinal epidural hematoma (SSEH) is a rare pathology with potentially severe consequences for the patient. Given its uncommon incidence and frequent atypical presentation, SSEH can easily be misdiagnosed. The association between anticoagulation or antiplatelet therapy and SSEH has been described in multiple case reports and literature reviews. We present a case of a 61-year-old man on anticoagulation and antiplatelet therapy (Rivaroxaban and Clopidogrel respectively), diagnosed with spinal SSEH with good recovery after laminectomy and hematoma evacuation. However, treatment guidelines for SSEH are difficult to find and there is no clear strategy about management of anticoagulation and antiplatelet therapy. The aim of this report is to highlight the importance of rapid diagnosis and surgical therapy in selected cases and to give an insight on the anticoagulation and antiplatelet management in these patients and their prognosis.
Keywords: neurosurgery, anticoagulation, platelet inhibitors, treatment, prognosis
Introduction
Spontaneous spinal epidural hematoma (SSEH) is a rare pathology with an incidence of 0.1 in 100000 per year.1 Patients typically present with back pain and neurological deficits, which might lead to a first suspicion of stroke or cardiac event. In the era of direct oral anticoagulants (DOAC), bleeding complications are a concern and SSEH seems to be one of them. Several case reports describe patients with SSEH under either anticoagulation2–10 or antiplatelet therapy.11–16 But we did not find cases of both, except in the acute setting of myocardial infarction on DAPT (double antiplatelet therapy) and enoxaparin.17 We present the case of a 61-year-old male patient, on anticoagulation treatment for atrial fibrillation and antiplatelet therapy for coronary disease, who was diagnosed with SSEH, and had good recovery after laminectomy.
Case
A 61-year-old male patient, known for atrial fibrillation and stented ischemic heart disease, treated by rivaroxaban, clopidogrel, metoprolol, candesartan and atorvastatin/ezetimib, consulted at our emergency department with acute onset of an intense cervico-thoracic pain with intermittent paresthesia of the fingers of both hands. The pain appeared while resting and worsened with cervical extension. There was no thoracic or abdominal pain. The blood pressure was symmetric at 143/100 mmHg, the heart frequency was 103 bpm, saturation 99% at room air, respiratory frequency of 15 breaths/min and body temperature of 36.8°C. Detailed neurological examination revealed a paresis at the lower limbs (right: M2 proximal, M1 distal, left: M4 proximal, M2 distal, according to the Medical Research Council power scale (see Table 1)), hypoesthesia of the lower limbs right > left, and hypoesthesia in the left upper limb. Babinski sign was positive bilateral.
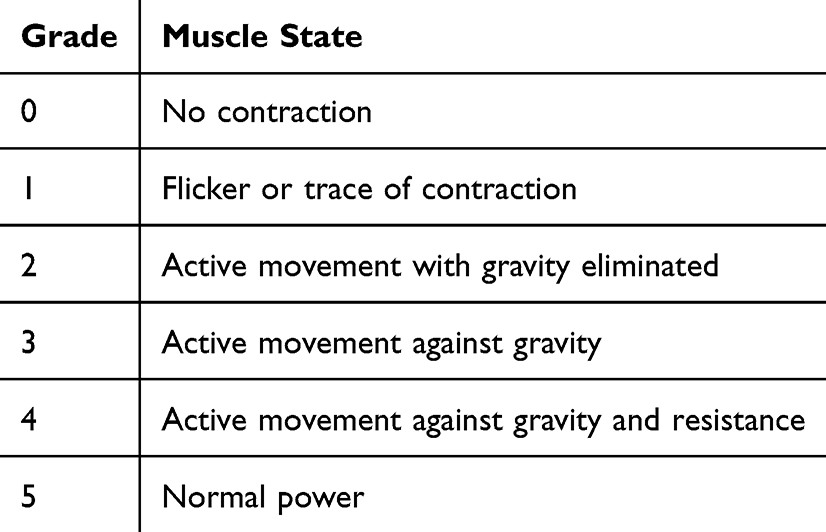 |
Table 1 Grading on Muscle Force According to the Medical Research Council (MRC) |
Electrocardiogram (ECG) showed sinus rhythm without any signs of acute ischemia. Blood samples showed a normal formula (leucocytes 7.4 G/L, thrombocytes 185 G/L, hemoglobin 146 g/l), electrolytes were normal, C-reactive protein (CRP) was negative (<0.3 mg/l), and creatinine was slightly elevated without meeting KDIGO (Kidney Disease: Improving Global Outcomes) criteria of acute kidney injury (121 mcmol/l). PT (prothrombin time) was at 61% with an INR (International Normalized Ratio) of 1.2 and PTT (Partial thromboplastin time) was 41 sec., explained by rivaroxaban and clopidogrel treatment.
The patient received 1g of paracetamol and 15 mg of morphine in 4 hours for pain therapy.
A cervico-thoraco-abdominal computed tomography (CT) scan with contrast injection was initially performed and showed a posterior cervical epidural mass of 7.5 cm long and 7 mm wide, extending from C5 to T1 with a spot sign, representing focal extravasation of contrast containing blood within the lesion (Figure 1). Magnetic Resonance Imaging (MRI) identified a posterior epidural hematoma from C2 to D5 with signs of medullary compression at C6/7 (Figure 2).
 |
Figure 1 Contrast injected CT scan of de cervical spine. Axial (A and B) and sagittal (C) CT angiography showing a posterior cervico-thoracic epidural mass (head arrow) with a spot sign (arrow), representing focal extravasation of contrast containing blood within the lesion. |
 |
Figure 2 MRI of the cervical and upper thoracic spine. Sagittal (A–C) and axial (D and E) MRI showing a spinal cord compression by a spontaneous epidural hematoma, isointense on T1W (C; head arrow), heterogeneously hyperintense with hypointense foci on T2W (A, B, and D; head arrow), and with a blooming artifact on GRE (gradient recalled echo)T2*-weighted MRI (E; black arrow). A fluid-fluid level (yellow arrow) is seen, that may be associated with bleeding by coagulation disorders. |
Rivaroxaban and clopidogrel were discontinued. After correction of coagulation (TP 80%, INR 1.1) with perfusion of coagulation factors (3000 U of Octaplex (factors II, VII, IX, X)) and 2 platelet concentrates, a laminectomy C6-C7 with drainage of the hematoma has been performed urgently. Neurological status rapidly normalized within four hours after intervention. The patient left the hospital at day 6 without neurological deficits. Renal function and coagulation parameters had normalized at discharge. Clopidogrel could be stopped definitely, since cardiac stent implantation was over 6 month and rivaroxaban was restarted 3 weeks after the operation. After two months, neurological status was still normal, and MRI showed complete resorption of the hematoma.
Discussion
Epidemiology
SSEH is a rare pathology with an incidence around 0.1 in 100,000 per year with a slight male predominance (1,4:1). Typically, patients are within the fourth or fifth decade of their life. SSEH accounts for less than 1% of all spinal canal masses and 1/3 of all spinal hematomas.1,18 Around 22% of spinal hematomas are associated with coagulopathy including anticoagulant use, which is identified as important risk factor. It mostly occurs in the cervicothoracic level, but can present at any level.7 Other identified risk factors are anticoagulant therapy, therapeutic thrombolysis, coagulopathy, platelet aggregation inhibitor, cocaine abuse, arteriovenous malformations, vertebral hemangiomas, minor trauma, pregnancy, hemophilia, and leukemia.1,19
Clinical Presentation
SSEH is a rare cause of spinal cord compression. It typically presents with acute onset of back pain, and is accompanied by partial or complete nerve root signs or full neurological deficit,1 however neurological signs are not always present.20 Neurological symptoms are typically lower motor neuron pathologies with hyporeflexia and flaccid paralysis1 but sensory neurons can also be touched. Dependent on localization, even Brown Séquard syndrome (hemisection of the spinal cord) has been described.21 Upper motor neuron lesions can also be seen due to profound compression. A positive Babinski sign bilaterally can be seen when there is a damage to pyramidal tract, as it was seen in our patient. Severity of neurologic signs are classified by Frankel classification, or its revised version, the ASIA (American Spinal Injury Association) impairment scale (AIS), shown in Table 2.
 |
Table 2 ASIA Grading of Neurological Function After Spinal Cord Injury |
Diagnosis
Diagnosis of SSEH remains a challenge in the emergency department. Differential diagnosis is wide, including disc herniation, cerebral infarction, spinal cord infarction, transverse myelitis, subarachnoid hemorrhage, aortic dissection, vertebral artery dissection, and acute myocardial infarction.20 This diagnosis can easily be missed, especially in atypical presentation or absence of neurological symptoms. In case of neurological signs, especially when present unilaterally, misdiagnosis as stroke is frequent and causes a therapeutic problem.22 Nevertheless, quick diagnosis and decision-making are primordial for patient’s prognosis.18 In our case, a cervico-thoraco-abdominal CT scan with contrast was initially performed. A space occupying mass was identified with a hyperintense blush, suspicious of epidural hematoma, later confirmed by MRI. The gold standard imaging modality is MRI of the spine. It outperforms CT myelography, which had been used before MRI was readily available. MRI allows for identification of the type, location, and age of the lesion, as imaging features can change over time (see Table 3).23
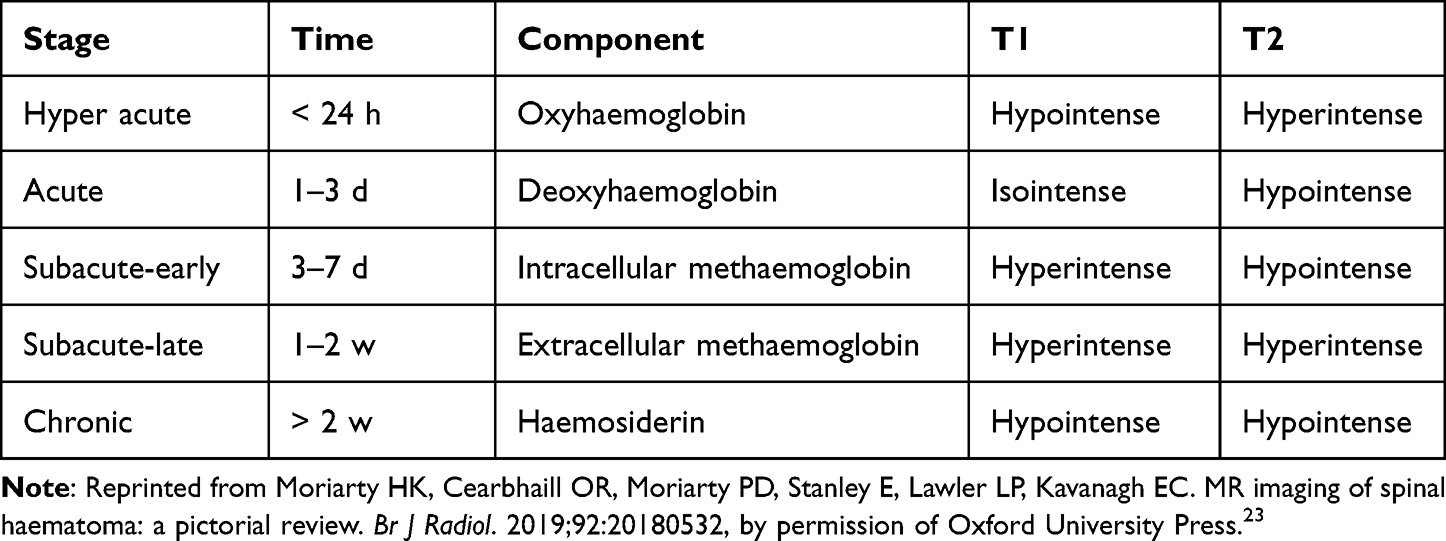 |
Table 3 Imaging Features of MRI Over Time |
Treatment
Treatment depends on hematoma localization, severity and onset of neurological deficit. Treatment options are observance, stopping or reversal of anticoagulation therapy, and emergent or delayed decompressive surgery by laminectomy or hemilaminectomy and hematoma removal.
Fukui et al compared the prognosis of surgical versus conservative treatment. In their study, patients with ASIA grade A and B were included in the surgery group and those with ASIA grade D and E in the conservative group, so that comparison only is reliable in patients with ASIA grade C (N = 31). In this group, there was no significant difference in outcome between surgical (N = 19) and non-surgical treatment (N = 12). If surgical treatment is chosen, rapid action is important, as patients operated after a timeframe of 24 hours had worse outcome.24 Kim et al compared 10 operated patients to 5 non-operated patients. In their study, conservative management consisted of administration of 10 mg Dexamethasone after admission (except 1 patient). 4×4 mg of dexamethasone was administered over an average time range of two days in all patients. Again, all ASIA A and B patients were in the surgical group. For Asia C patients there was no significant difference in outcome between surgical and conservative treatment.25
It seems reasonable to operate as soon as possible in ASIA A and B patients or ASIA C patients with bad evolution (preferably within 24 hours), and to try conservative treatment in ASIA D and E patients or ASIA C patients with good evolution.
When an operative treatment is chosen, open laminectomy and hemilaminectomy with hematoma evacuation is generally used, but some case-reports show good results with minimally invasive techniques.26,27
In case of anticoagulation or antiplatelet therapy, these treatments should be discontinued. The goal is to avoid an aggravation of bleeding and to facilitate a surgical intervention if necessary. The administration of anticoagulant reversal remains controversial and needs further investigation. Some even hypothesize that with continuation of anticoagulant therapy the blood remains liquid with a more homogeneous distribution without medullary compression.11
In some cases surgery was delayed because of anticoagulant use.2 This strategy seems to be more harmful, as rapid surgical intervention remains the main factor for good prognosis.2 Cases have been reported where surgical and conservative treatment were performed without anticoagulation reversal, with good result.28 Stetkarova et al describe in their cohort 10 of 14 patients receiving anticoagulant (n = 8) or antiplatelet (n = 2) therapy. Only one patient (INR > 5 on Warfarin treatment) received reversal by fresh frozen plasma. El Alaya et al collected a series of 11 anticoagulated patients. Eight Patients underwent operative treatment, of which 3 patients received reversal therapy and one patient received aminocaproic acid. Conservatively treated patients did not receive procoagulant therapy.2
To date, there is no clear answer to the question if we should reverse anticoagulant therapy. It seems logical to correct coagulation before a surgical intervention, to minimize hemorrhagic operative complications. If there is an operative indication, intervention should not be delayed because of anticoagulation.
For antiplatelet therapy, there are no clear recommendations. Guidelines for neurosurgical interventions are divergent and propose continuation or stopping Clopidogrel 5–7 days before elective surgery, dependent on indication.29
Laminectomy and hematoma evacuation have been performed without platelet administration after stopping Clopidogrel13,15 or DAPT.12,30 Platelets were generally not given to reverse platelet dysfunction.
Timing for restarting antiplatelet drugs is not standardized and depends on its indication. In some cases clopidogrel was stopped definitely,15 in other cases it was interrupted between 112,21 and 14 days.30 There have been cases without interruption of clopidogrel at all.11 A prescribing specialist (neurologist, cardiologist) should be involved in the decision making.
Several case reports and reviews describe the use of Corticosteroids. To date, corticoid therapy for spinal cord injury seems to be more harmful than beneficial and is thus not recommended.31
Prognosis
SSEH is a pathology with potentially severe consequences. Prognosis ranges from complete recovery (about 40%) over mild to severe impairment or even death (about 5%).18 Fukui et al identified age, hematoma location, preoperative Frankel score and time from onset to diagnosis to be significant factors for prognosis. Older age, longer time from onset to diagnosis, presence of a hematoma in the thoracic spine, and the need for surgical treatment were associated with poor prognosis. Short time to develop full neurologic symptoms would logically be a negative prognostic factor, but could not be identified as such, probably because they are diagnosed and treated more rapidly. Whereas Kreppel et al could not show craniocaudal extension to influence outcome, Fukui et al identified vertical size of the hematoma as a factor for poor prognosis in non-operated patients.18,24 In patients needing surgery, time from onset to surgery was a prognostic factor.24 Kim et al did not find age, sex or premorbid medication of antiplatelets or anticoagulants to affect complete recovery.25
Conclusion
SSEH is a rare pathology with potentially severe consequences for the patient. Rapid diagnosis and treatment in patients with SSEH are critical for prognosis. Clinical suspicion should be raised in patients with acute onset of spinal pain and neurological deficits, especially in patients with coagulopathy. Prompt MRI should be performed for diagnosis. In case this is not possible, CT scan can help identify spinal lesions. Treatment options vary from conservative treatment in patients with ASIA D and E and patients with ASIA C who experience spontaneous symptom regression. Patients with ASIA C experiencing symptom progression, as well as patients with ASIA A and B should undergo surgical treatment. Options range from minimal invasive techniques to full laminectomy and hematoma removal. Anticoagulation and antiplatelet therapy are risk factors for SSEH, but it remains unclear how to handle these medications after diagnosis. It seems logical to interrupt this treatment to prevent further bleeding. Due to the rare prevalence, prospective clinical trials are difficult to set up, but are important to resolve questions concerning conservative vs surgical treatment and correction of coagulopathy.
Informed Consent
Written patient informed consent to publish was obtained from the patient for publication of case details and images.
Funding
No external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Figueroa J, DeVine JG. Spontaneous spinal epidural hematoma: literature review. J Spine Surg. 2017;3:58–63. doi:10.21037/jss.2017.02.04
2. El Alayli A, Neelakandan L, Krayem H. Spontaneous spinal epidural hematoma in a patient on apixaban for nonvalvular atrial fibrillation. Case Rep Hematol. 2020;2020:7419050. doi:10.1155/2020/7419050
3. Feret WB, Kwiatkowska E, Domański L. Paraplegia caused by spontaneous spinal hemorrhage in a patient undergoing rivaroxaban therapy. Am J Case Rep. 2020;21:e923607. doi:10.12659/AJCR.923607
4. Goldfine C, Glazer C, Ratzan RM. Spontaneous spinal epidural hematoma from rivaroxaban. Clin Pract Cases Emerg Med. 2018;2:151–154. doi:10.5811/cpcem.2018.2.37096
5. Jaeger M, Jeanneret B, Schaeren S. Spontaneous spinal epidural haematoma during factor xa inhibitor treatment (Rivaroxaban). Eur Spine J. 2012;21(Suppl 4):S433–435. doi:10.1007/s00586-011-2003-3
6. Mathais Q, Esnault P, Cruc M, Bernard C, Prunet B, Gaillard PE. Spontaneous cervical spinal epidural hematoma associated with dabigatran. World Neurosurg. 2018;112:264–266. doi:10.1016/j.wneu.2018.01.199
7. Raasck K, Habis AA, Aoude A, et al. Spontaneous spinal epidural hematoma management: a case series and literature review. Spinal Cord Ser Cases. 2017;3:16043. doi:10.1038/scsandc.2016.43
8. Raeouf A, Goyal S, Van Horne N, Traylor J. Spontaneous spinal epidural hematoma secondary to rivaroxaban use in a patient with paroxysmal atrial fibrillation. Cureus. 2020;12:e10417. doi:10.7759/cureus.10417
9. Rahimizadeh A, Malekmohammadi Z, Williamson WL, Rahimizadeh S, Amirzadeh M, Asgari N. Rivaroxaban-induced acute cervical spine epidural hematoma: report of a case and review. Surg Neurol Int. 2019;10:210. doi:10.25259/SNI_390_2019
10. Tawk C, El Hajj Moussa M, Zgheib R, Nohra G. Spontaneous epidural hematoma of the spine associated with oral anticoagulants: 3 case studies. Int J Surg Case Rep. 2015;13:8–11. doi:10.1016/j.ijscr.2015.05.022
11. Abu-Abaa M, Jumaah O, Mousa A, Al-Qaysi G. A spontaneous spinal epidural hematoma secondary to long-term low-dose aspirin and clopidogrel use: a case report. Cureus. 2023;15:e34537. doi:10.7759/cureus.34537
12. Alahmadi MJ, Almolky KS, Rezai DM. Spontaneous spinal epidural hematoma associated with short-term dual antiplatelet therapy: a case report. Cureus. 2022;14:e29415. doi:10.7759/cureus.29415
13. Bhat KJ, Kapoor S, Watali YZ, Sharma JR. Spontaneous epidural hematoma of spine associated with clopidogrel: a case study and review of the literature. Asian J Neurosurg. 2015;10:54. doi:10.4103/1793-5482.151521
14. Seet RC, Lim EC, Wilder-Smith EP, Ong BK. Spontaneous epidural haematoma presenting as cord compression in a patient receiving clopidogrel. Eur J Neurol. 2005;12:811–812. doi:10.1111/j.1468-1331.2005.01057.x
15. Sung JH, Hong JT, Son BC, Lee SW. Clopidogrel-induced spontaneous spinal epidural hematoma. J Korean Med Sci. 2007;22:577–579. doi:10.3346/jkms.2007.22.3.577
16. Wang L, Liu G, Subramaniam S, Wong TA, Kumar N. Spontaneous spinal epidural haematoma after antiplatelet treatment: a report of two cases. J Orthop Surg. 2012;20:386–390. doi:10.1177/230949901202000326
17. Özyurtlu F, Çetin N, Pekel N, Özpelit ME. Spontaneous spinal epidural hematoma developing after percutaneous coronary intervention: early diagnosis, early intervention, and good outcome. Turk Kardiyol Dern Ars. 2016;44:158–160. doi:10.5543/tkda.2015.68957
18. Kreppel D, Antoniadis G, Seeling W. Spinal hematoma: a literature survey with meta-analysis of 613 patients. Neurosurg Rev. 2003;26:1–49. doi:10.1007/s10143-002-0224-y
19. Wang M, Zhou P, Jiang S. Clinical features, management, and prognostic factors of spontaneous epidural spinal hematoma: analysis of 24 cases. World Neurosurg. 2017;102:360–369. doi:10.1016/j.wneu.2017.02.058
20. Eto F, Tatsumura M, Iwabuchi S, Ogawa T, Mammoto T, Hirano A. Clinical features of spontaneous spinal epidural hematoma. J Rural Med. 2019;14:206–210. doi:10.2185/jrm.3005
21. Riaz S, Jiang H, Fox R, Lavoie M, Mahood JK. Spontaneous spinal epidural hematoma causing brown-sequard syndrome: case report and review of the literature. J Emerg Med. 2007;33:241–244. doi:10.1016/j.jemermed.2007.02.032
22. Hu Y, Su J, Cui X, Pan L, Jin L, Teng F. How to avoid misdiagnosing spontaneous cervical spinal epidural hematoma as ischemic stroke: 3 case reports and literature review. Cerebrovasc Dis. 2023;52:597–606. doi:10.1159/000527705
23. Moriarty HK, Cearbhaill OR, Moriarty PD, Stanley E, Lawler LP, Kavanagh EC. MR imaging of spinal haematoma: a pictorial review. Br J Radiol. 2019;92:20180532. doi:10.1259/bjr.20180532
24. Fukui H, Kamei N, Fujiwara Y, et al. Prognostic factors for spontaneous spinal epidural hematoma: a multicenter case-control study. Acta Neurochir. 2022;164:1493–1499. doi:10.1007/s00701-022-05130-z
25. Kim T, Lee CH, Hyun SJ, Yoon SH, Kim KJ, Kim HJ. Clinical outcomes of spontaneous spinal epidural hematoma: a comparative study between conservative and surgical treatment. J Korean Neurosurg Soc. 2012;52:523–527. doi:10.3340/jkns.2012.52.6.523
26. Lisheng H, Dong Z, Xuedong B, et al. Successful treatment of thoracic myelopathy caused by spontaneous spinal epidural hematoma (SSEH) combined with calcification of the ligamentum flavum (CLF) by posterior percutaneous endoscopic surgery (PPES): a case report. Front Surg. 2022;9:1077343. doi:10.3389/fsurg.2022.1077343
27. Fu CF, Zhuang YD, Chen CM, et al. Spontaneous spinal epidural hematoma management with minimally invasive surgery through tubular retractors: a case report and review of the literature. Medicine. 2016;95:e3906. doi:10.1097/MD.0000000000003906
28. Stetkarova I, Ehler E, Brabec K, et al. Spontaneous spinal epidural haematoma: management and main risk factors in era of anticoagulant / antiplatelet treatment. Neurologia i Neurochirurgia Polska. 2021;55:574–581. doi:10.5603/PJNNS.a2021.0066
29. Kaye AD, Manchikanti L, Novitch MB, et al. Responsible, safe, and effective use of antithrombotics and anticoagulants in patients undergoing interventional techniques: American Society of Interventional Pain Physicians (ASIPP) guidelines. Pain Physician. 2019;22:S75–s128. doi:10.36076/ppj/2019.22.s75
30. Yang SM, Kang SH, Kim KT, Park SW, Lee WS. Spontaneous spinal epidural hematomas associated with acute myocardial infarction treatment. Korean Circ J. 2011;41:759–762. doi:10.4070/kcj.2011.41.12.759
31. Thomas AX, Riviello JJ Jr, Davila-Williams D, et al. Pharmacologic and acute management of spinal cord injury in adults and children. Curr Treat Options Neurol. 2022;24:285–304. doi:10.1007/s11940-022-00720-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.