")
Back to Journals » Eye and Brain » Volume 16
Spotlight on Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC)
Authors Kozak I, Mochida GH, Lin DD, Ali SM, Bosley TM
Received 16 July 2024
Accepted for publication 20 October 2024
Published 23 October 2024 Volume 2024:16 Pages 55—63
DOI https://doi.org/10.2147/EB.S419663
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rustum Karanjia
Igor Kozak,1,2 Ganeshwaran H Mochida,3,4 Doris DM Lin,5 Syed M Ali,2,6 Thomas M Bosley7
1Department of Ophthalmology and Vision Science, University of Arizona, Tucson, AZ, USA; 2Research Department, Moorfields Eye Hospital Center, Abu Dhabi, United Arab Emirates; 3Division of Genetics and Genomics and The Manton Center for Orphan Disease, Boston Children’s Hospital, Department of Pediatrics, Harvard Medical School, Boston, MA, USA; 4Pediatric Neurology Unit, Department of Neurology, Massachusetts General Hospital, Boston, MA, USA; 5Division of Neuroradiology, Russel H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 6Department of Ophthalmology, Kanad Hospital, Al Ain, United Arab Emirates; 7Wilmer Eye Institute, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Igor Kozak, Department of Ophthalmology and Vision Science, University of Arizona, Tucson, AZ, USA, Tel +1-520-626-2010, Email [email protected]
Abstract: Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC) is a rare syndrome caused by biallelic mutations in the JAM3 gene with significant intrafamilial variability in clinical presentation and brain imaging phenotypes. The clinical presentation of HDBSCC includes severe recurrent hemorrhages involving the brain parenchyma and the ventricles beginning in utero and continuing in infancy together with dense central cataracts present at birth. This comprehensive review documents reported cases on this unique condition and describes its genetic, neuroradiologic and ophthalmic features. It should be included in the differential diagnosis of children with congenital cataracts and neurodevelopmental abnormalities. Unique clinical, imaging findings and genetic testing can help the diagnosis.
Keywords: hemorrhagic destruction of the brain, subependymal calcification, and congenital cataracts, junctional adhesion molecule 3 gene, neuroradiology, imaging, eye
Introduction
Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC, MIM# 613730) is a rare autosomal recessive genetic disorder caused by variants in the Junctional Adhesion Molecule 3 (JAM3) gene that contributes a major structural element to tight junctions in the brain and elsewhere. The clinical presentation of HDBSCC includes severe recurrent hemorrhages involving the brain parenchyma and the ventricles beginning in utero and continuing in infancy together with dense central cataracts present at birth. This disorder is unique among tight junction-associated genetic disorders because it presents with severe hemorrhagic destruction of the brain, a process not previously associated with tight junction genetic problems. This highlights the critical role of tight junctions, which are composed of proteins like claudins, occludins, and JAMs, in the development of cerebrovascular endothelium of the human brain and in maintaining the integrity of the blood brain barrier. HDBSCC is also marked by bilateral congenital central cataracts that hinder assessment of the eye’s posterior segment, potentially masking other vision-impairing lesions.1,2
JAM3 is a transmembrane glycoprotein that is part of the immunoglobulin superfamily and plays a critical role in tight junction assembly, angiogenesis, and various inflammatory processes. Its malfunction has broad implications, affecting not only the brain and eyes but also other parts of the body, potentially influencing tumor development. JAM3 knockout mice models have provided insights into the wide-ranging functions of JAM3, including its role in spermatid differentiation, myelin sheath integrity, nerve conduction, lens development, and esophagus innervation. These knockout models have exhibited symptoms like megaesophagus, failure to thrive, jitteriness, pneumonia, brain hemorrhages, and hydrocephalus, mirroring the complex clinical presentation seen in HDBSCC patients.2
In this review, the first and second sections describe various clinical presentations and genetics of this condition, respectively. The new ophthalmic findings are summarized in the section on ophthalmic characteristics and the final section will detail neuroradiologic description of previously published cases.
Clinical Description
To date, only approximately 20 patients have been reported globally with probable or definite HDBSCC, emphasizing the rarity of this disorder.
Mochida et al2 in 2010 were the first to produce a comprehensive clinical and genetic description of HDBSCC (OMIM:613730) in eight individuals from a large consanguineous family with its origin in Baluchistan that had been partially described previously. These individuals all displayed hemorrhagic destruction of the brain parenchyma, subependymal calcification, congenital cataracts, facial dysmorphism, severe developmental delay, infantile seizures, and generalized spasticity. Several patients also had renal anomalies and an enlarged liver, but testing for TORCH infections was negative. Only one segment of homozygosity on chromosome 11q25 was shared by all affected individuals, and sequence analysis of the nine protein-coding genes in this region revealed only one candidate mutation in the Junctional Adhesion Molecule 3 (JAM3) gene at the first base position of intron 5 (c.747+1G>T) that is predicted to remove the wild-type splice donor site and to reveal a cryptic splice donor site 19 base pairs downstream. Three of the affected children died within days to months of birth; three had seizures; two had renal anomalies; one had a cardiac anomaly; all had dense central cataracts; and one was noted to have slightly pale optic disks.
Akawi et al3 in 2013 reported three additional families with HDBSCC. The parents in Family 1 were normal individuals who were second cousins of Turkish origin. Their first child was preterm and born with intracranial bleeding and died in the neonatal period. Their second child was born at term with bilateral cataracts and facial dysmorphism consisting of a slopping forehead, bulging anterior fontanelle, and bitemporal grooving. She was admitted on day 5 of life with tonic seizures that were difficult to control, and brain imaging showed subependymal calcifications and multifocal brain hemorrhages. This child developed hydrocephalus and died at age two months. The affected children had a homozygous missense variant in exon 6 of the JAM3 gene (c.656G>A; p.C219Y NM_032801.4), and the parents were carriers of that variant. Family 2 was Afghani in origin. Their first child was born by emergency caesarian section. He had bilateral cataracts and was small (<10th centile) with feeding difficulties. At two weeks of age he developed vomiting and a high-pitched cry, and an MRI scan showed a large intraventricular hemorrhage with severe ventricular dilation. He died shortly thereafter. The second child in this family was normal. The third child initially had normal tone and reflexes with bilateral cataracts and no obvious seizures, but an EEG on day 3 of life revealed bilateral epileptiform activity. Cranial ultrasound showed bilateral intracerebral hemorrhages, and he died on the fifth day of life. The affected children had homozygous missense mutations in exon 4 of the JAM3 gene (c.346G>A; p.E116K, NM_032801.4). The parents were non-consanguineous, but both were carriers of this same variant. The parents of Family 3 were Moroccan first cousins. Their first child was born at 36 weeks with a cerebral hemorrhage and hydrocephalus and died at 10 days of age. They then had two normal children, but their fourth child was stillborn with hydrocephalus and necrotic areas of the brain. Their fifth child was delivered by caesarian section after fetal tachycardia was noted. She had both central and nuclear cataracts. She became irritable on her second day of life with a bulging anterior fontanelle, and brain ultrasound showed an intraventricular hemorrhage on the right with dilated lateral ventricles bilaterally and frontal periventricular cysts. EEG documented status epilepticus despite the absence of clinical seizures. Head circumference gradually enlarged, and she died at home at the age of 39 days. A homozygous mutation of JAM3 in this family changed the initiator codon (c.346G>A; p.E116K, NM_032801.4); the parents were both carriers of the mutation. All of these children died within two months of birth, and at least two had documented seizure activity.
De Rose et al4 in 2021 reported a consanguineous Italian family with no prior neurologic or visual history who delivered their first child, a baby boy, at term. An MRI scan at 20 weeks gestational age showed no cerebral abnormalities. At 12 hours of life he became irritable with excessive startle, hypotonia, and apnea. Focal seizures began on the second day of life and gradually became more frequent until the child had status epilepticus resistant to medications. Eye exam early in life revealed bilateral central cataracts and eventually bilateral microphthalmia. Cranial ultrasound showed periventricular leukomalacia, and a subsequent brain MRI showed multiple intraventricular and intraparenchymal hemorrhages as well as multiple periventricular calcifications. Brain lesions progressed, and his clinical condition eventually required a percutaneous endoscopic gastrostomy tube and a ventriculoperitoneal shunt. The child was documented to have a novel homozygous JAM3 variant in exon 6 (c.690T>G; p.C230W, NM_1205329.1), of which his parents were heterozygous carriers. The child also had myocardial hypertrophy.
Xu et al5 in 2022 reported three siblings with severe ventriculomegaly noted in utero from China. The first female child died during the newborn period. The second fetus (gender not described) had dilated ventricles by fetal cranial MRI at 29th week of gestation. At the 31st week, an ultrasound revealed skin edema, bilateral pleural effusion and ascites (observations not typical of HDBSCC), in addition to severe ventriculomegaly, and the pregnancy was terminated. The third fetus (gender not described) had dilated ventricles and intraventricular hemorrhage noted by fetal cranial MRI at the 24th week, and the pregnancy resulted in termination. Ophthalmological findings were not documented. Genetic analysis of the second and third child revealed compound heterozygous variants in JAM3, a maternally inherited nonsense variant (c.813C>G; p.Y271*) and a paternally inherited canonical splice-site variant (c.712+2T>A).
Kozak et al1 in 2023 reported a consanguineous family from Pakistan who had a 14-year-old daughter with developmental delay and severe disability with spastic quadriplegia, and poor vision associated with bilateral cataracts. She was found to have the same intron 5 variant (c.747+1G>T, NM 1205329.1) in the JAM3 gene that was the same as reported previously by Mochida et al,2 and it was assumed that this was another branch of the same large consanguineous family. The focus of the Kozak report was a younger sister with intrauterine growth restriction, enlarged head, dysmorphic appearance with frontal bossing, and seizures beginning at 12 hours post-partum. She had very poor vision and inability to fix and follow associated with bilateral dense central cataracts. In addition, she had attenuated retinal vessels, bilateral optic atrophy with no disk edema, poorly reactive pupils with no afferent pupillary defect, and a retinal hemorrhage inferiorly in the right eye. This scenario implied that at least this variant of the JAM3 gene can affect the development of structures in the globe. Serial head ultrasonography showed early multifocal hemorrhagic destruction of the brain that progressed rapidly over the first month of life to include cystic encephalomalacia with marked loss of brain parenchyma. She was subsequently moved to a rehabilitation center.
Moady et al6 in 2023 reported a new male patient from a consanguineous Bedouin family in Israel. Fetal ultrasonography at 14 weeks gestation revealed a single umbilical artery, and the child was followed carefully subsequently. Ultrasonography at 23 weeks of gestation showed bilateral central cataracts and calcification in periventricular regions bilaterally. Lateral ventricles were dilated at 30 weeks of gestation; serologic testing for TORCH and parvovirus were negative. The child had a small head and body at birth, and subsequent evaluation revealed a thin corpus callosum, dilated lateral ventricles, and a hemorrhage in the left thalamus. The child subsequently developed numerous foci of bleeding in the brain parenchyma and ventricles with periventricular leukomalacia. A CT scan at age 12 months showed small third and lateral ventricles and enlargement of the subarachnoid spaces compatible with brain atrophy. The child developed severe microcephaly, episodes of severe restlessness, severe generalized hypertonia, diffuse hyperreflexia, intractable seizures, and an abnormal EEG. He had dysmorphic facial features and very delayed cognitive development. The child proved to have a novel pathogenic homozygous frameshift variant in the JAM3 gene (c.745dupG; p(V249Gfs*28); both parents were heterozygous for the same mutation. The child was alive at 30 months post-partum, at the time of the clinical report cited here.
Alshammari et al7 in 2024 reported an affected male from a consanguineous family in Saudi Arabia who presented with profound global developmental delay, multiple joint contractures, epilepsy, and cataracts. Brain MRI showed intraparenchymal hemorrhage and extensive cystic encephalomalacia, with parenchymal volume loss and ex vacuo dilatation of the lateral ventricles. A homozygous missense variant in JAM3 (c.346G>A; p.E116K), which was previously reported in Akawi et al3 was identified and was interpreted as likely pathogenic.
In addition to the publications above, there are reports of JAM3 variants identified as part of large-scale sequencing efforts, and clinical information is somewhat limited (Bertoli-Avella et al8 and Al-Kasbi et al9).
Patients with HDBSCC sometimes exhibit a variety of brain and somatic anomalies in addition to recurrent brain hemorrhages and cataracts. Thin corpus callosum and white matter abnormalities have been described in several patients,3,6 quite likely as the result of brain injury from recurrent hemorrhages. This recurrent brain injury with tissue damage, cystic degeneration, and liquefaction likely leads to progressive microcephaly noted in a number of patients. Hepatomegaly, renal anomalies,1 cardiac hypertrophy, and megaesophagus4 have also been reported, possibly as independent effects of tight junction abnormalities elsewhere in the body.
Genetic Characteristics
HDBSCC is an autosomal recessive disorder caused by biallelic mutations in the JAM3 gene. Heterozygous carriers have not been reported to show any clinical manifestations. Several types of JAM variants, including splicing, nonsense, frameshift, missense, and start-loss, have been reported in the literature. There is no clear genotype-phenotype correlation. For example, the missense variants do not seem to be associated with a milder phenotype than truncating variants. However, significant intrafamilial variability in brain imaging phenotypes can be observed.1 Further, due to the small number of reported cases to date, it is possible that the full clinical spectrum of the condition is not yet delineated. Loss-of-function is the most likely pathogenetic mechanism, and this is supported by the observation that the knockout mice for Jam3 (also known as Jam-C) may develop hydrocephalus accompanied by intracranial hemorrhage.10
Human tight junctions are composed of a complex of transmembrane proteins consisting of claudins, occludins, and JAMs. Several other human genetic syndromes have been reported to result from autosomal recessive variants of the genes encoding tight-junction proteins, including familial hypercholanemia (MIM 607748),11 autosomal recessive deafness 29 (DFNB29; MIM 605608),12 and 49 (DFNB49; MIM 610153),13 and Nance-Horan Syndrome (MIM 302350).14 These syndromes cause a variety of clinical symptoms, but none of them are recognized to cause severe brain hemorrhages. Pseudo-TORCH syndrome 1 (OMIM#251290) is an autosomal recessive disorder due to variants in the OCLN gene (MIM#602876) encoding occludin. This disorder causes brain calcification, cortical dysgenesis, severe developmental delay, and thrombocytopenia, but it does not cause brain hemorrhages or cataracts.15,16 In fact, it seems that the combination of cataracts and brain hemorrhage (often beginning in utero and continuing into infancy) is almost pathognomonic for HDBSCC once a TORCH infection has been excluded.17,18
Variants in JAM2 cause autosomal recessive idiopathic basal ganglia calcification-8, a progressive neurological disorder characterized by extensive calcifications in deep brain regions, including basal ganglia, thalamus, and cerebellum.19,20 The onset of neurological symptoms is later than that of JAM3 or OCLN variants and ranges from childhood to adulthood.
Ophthalmic Characteristics
The most prominent ocular abnormality in this syndrome is a congenital cataract which can be either an isolated finding or in conjunction with other ocular features. These include dysmorphic features such as high forehead with low anterior hair line, thin nasal bridge, high arched eyebrows and epicanthus with upper slanting eyes.5 There may be microphthalmia with horizontal and rotary nystagmus jerks.4 A recent report described attenuated retinal vessels, optic atrophy, and a retinal hemorrhage in a child with HDBSCC.1
Mice deficient for the mouse ortholog of JAM3 (Jam3; also known as JAM-C) have been reported to develop nuclear cataracts.14 Congenital cataracts, however, may have different patterns of opacification. Reports also describe cataract as an isolated ocular abnormality. De Rose et al describe bilateral congenital cataracts which underwent vitrectomy surgery at 2 months of life.4 Abdallah Moady et al describe normal ophthalmic examination except for the cataracts.6 At 6 weeks, the neonate underwent lens aspiration with posterior capsulotomy and anterior vitrectomy in his left eye, and a month later in the right eye. After 1 month, he was re-operated due to bilateral central opacification resembling Elschnig pearls. This opacification recurred one more time before mechanical excision with scissors. Re-opacification of the lens capsule is very rare especially if the posterior capsule or anterior hyaloid does not exist.15 A new study regarding lens development in knockdown mice with JAMC deficiency showed abnormal lens morphology and defective degradation of nuclei and organelles in lens fiber cells. Cell death and abnormal lens development was accompanied by the activation of unfolded protein response (UPR).16 As such the role of JAM in cataract formation seems to be crucial in these patients. Visual rehabilitation should follow clearing the visual axis but that may be limited by pathology.
Neuroradiological Appearance
Neuroimaging findings show variable stages and severity of early onset, progressive brain destruction consisting of multifocal parenchymal and intraventricular hemorrhage, subependymal calcification, periventricular white matter volume loss, cystic porencephaly and ventriculomegaly, together with manifest congenital cataract, this syndrome is given its descriptive name of HDBSCC. Cerebral abnormalities may occur in utero, at birth, or postnatally. The syndrome carries a high mortality, with a number of affected individuals die in utero or within days or months of life.2,4,5,7 Similar findings of brain necrosis in a stillborn (4) indicates that the destructive process can commence early during fetal life. A number of reported cases show extensive cerebral hemorrhages early in life; for example, multifocal parenchymal and intraventricular hemorrhages depicted in Figure 1A by neonatal sonography in an affected child born at near term (36 weeks) without complication of pregnancy or delivery but presenting with seizures at 12 hours of life.1 The location of parenchymal hemorrhage is typically in the periventricular zone with almost invariably concomitant intraventricular hemorrhage, in a pattern akin to the most severe germinal matrix hemorrhage occurring in the preterm infants following hypoxic ischemic injury, except that in HDBSCC intracranial hemorrhage occurs in full-term newborns without evidence of perinatal infection or other complications, more massive and destructive, and the sequence of events appear to take place as early as in utero with rapid progression in infancy.
 |
Figure 1 Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC). (A) Coronal neonatal head ultrasound on day 1 of life shows multifocal parenchymal and intraventricular hemorrhages with increased echogenicity, and dilatation of the lateral ventricles. (B) Coronal head CT without contrast at 5 weeks of age demonstrates profound parenchymal rarefaction, marked ventricular dilation and porencephaly, with only thin strands of soft tissue remaining (arrows). Scattered calcifications are seen along the ventricular margin (curved arrow). (C) Photograph of this child at birth shows macrocephaly (circumference 46 cm, >99 percentile) and frontal bossing. |
Parenchymal volume loss, ventriculomegaly and porencephalic cysts ensue progressively in response to cerebral injury. The degree of cerebral volume loss can be profound, such as seen in Figure 1B of the same child at 5 weeks of age. As shown in Figure 1C, at birth this child appeared dysmorphic with a large head and bulging fontanels suggesting underlying hydrocephalus. The CT finding of marked ventriculomegaly at week 5 was likely reflective of an element of communicating hydrocephalus superimposed on parenchymal volume loss. There were multiple similarly reported cases of ventriculomegaly including one that required ventriculoperitoneal shunting for post-hemorrhagic hydrocephalus;5 however, there were also a number of cases that predominantly presented with microcephaly.2,7
Characteristic findings of multi-compartment hemorrhages, at times at different stages of evolution, and periventricular tissue injury with volume loss are best demonstrated on MRI (Figure 2), while subependymal calcifications are most readily depicted by CT. The rapid progression of cerebral destruction and tissue loss has been well documented in serial ultrasound1 and MRI5 within the first few months of life. Phenotypic expression may vary, however, even with the same mutation within the same consanguineous family reported in Mochida et al,2 as demonstrated in Figure 3. In addition, dystrophic calcification develops, frequently in the periventricular or subependymal regions most probably because these sites reflect the vulnerable, watershed zones in the perinatal period. Dystrophic calcifications can, however, also be seen in the cerebral cortex and cerebellum (Figures 2–4).2,3
 |
Figure 2 Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC). A newborn female with bilateral congenital cataract and JAM3 mutation at day 1 of life, reported by Mochida et al (ref 2) as individual VIII-21. (A) Sagittal T1, (B) coronal T1 and (C) coronal T2 weighted MR images show intraventricular blood within a dilated cavum septum pellucidum (arrowheads) and third ventricle, as well as multifocal globular parenchymal hemorrhages in the right frontal lobe (arrows). Parenchymal blood shows predominantly T1 hyperintensity and T2 hypointensity consistent with intracellular methemoglobin (early subacute blood products; ~3-7 days old) with central regions of T1 isointensity consistent with deoxyhemoglobin (acute blood products; ~1-3 days). In addition, curvilinear and gyriform intrinsic T1 hyperintensity is seen in the cortex and subcortical regions (curve arrows in (B) suggestive of cortical laminar necrosis or hemorrhage. Reduced craniofacial ratio on sagittal image (A) suggests microcephaly. The lateral ventricles are dilated. Image courtesy of Dr. Lihadh Al-Gazali. |
 |
Figure 3 Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC). Variation of characteristic neuroimaging findings in HDBSCC of 5 siblings with JAM3 mutation, in the same family reported by Mochida et al (ref 2). (A) Axial head CT of VIII-21, same individuals as in Figure 2, on day 1 of life shows intraventricular hemorrhage, left parietal parenchymal hemorrhage of different attenuations, dilated lateral ventricles with chunky periventricular/subependymal calcifications. She died soon after birth. (B) Axial head CT of individual VIII-22 (male), on day 4 of life, demonstrates similar findings of multifocal intraventricular and parenchymal hemorrhages of varying ages, encephalomalacia, ventricular dilation and subependymal calcification. (C) Axial head CT of individual VIII-29 (female), day 1 of life, shows ventriculomegaly and subependymal calcification without the evidence of acute or recent hemorrhage. (D) Sagittal T1-weighted MRI of VIII-27 (male) at 3 weeks of age demonstrates large porencephalic cysts in the cerebrum and posterior fossa, associated with marked thinning of the cortical mantle. He died at 2 months. (E) Sagittal T1-weighted MRI of VIII-10 (female) at 3 weeks 4 days of age shows extensive parenchymal and intraventricular hemorrhages with ventricular dilatation and developing porencephaly. Image courtesy of Dr. Lihadh Al-Gazali. |
 |
Figure 4 Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC). Axial head CT without contrast of a 14-year-old girl (the older sister of the index case presented in reference 1 and in Figure 1) with homozygous mutation in the JAM3 gene. Multifocal destruction of the cerebrum with porencephalic cysts, some appearing to communicate with the dilated temporal horns. The brainstem and cerebellum are small but mostly spared in this case. Multiple foci of dystrophic calcification are present in the parenchyma within the cerebrum, cerebellum and along the ependymal lining. |
The Relevance of HDBSCC Syndrome
HDBSCC syndrome is a serious clinical condition with a high level of morbidity and mortality. It expands a clinical spectrum of congenital defects that can present with neurodevelopmental abnormalities with cataracts (Table 1). As such, it should be differential from similar conditions such as developmental and epileptic encephalopathy with cataract,21–23 or brain calcifications.24–26
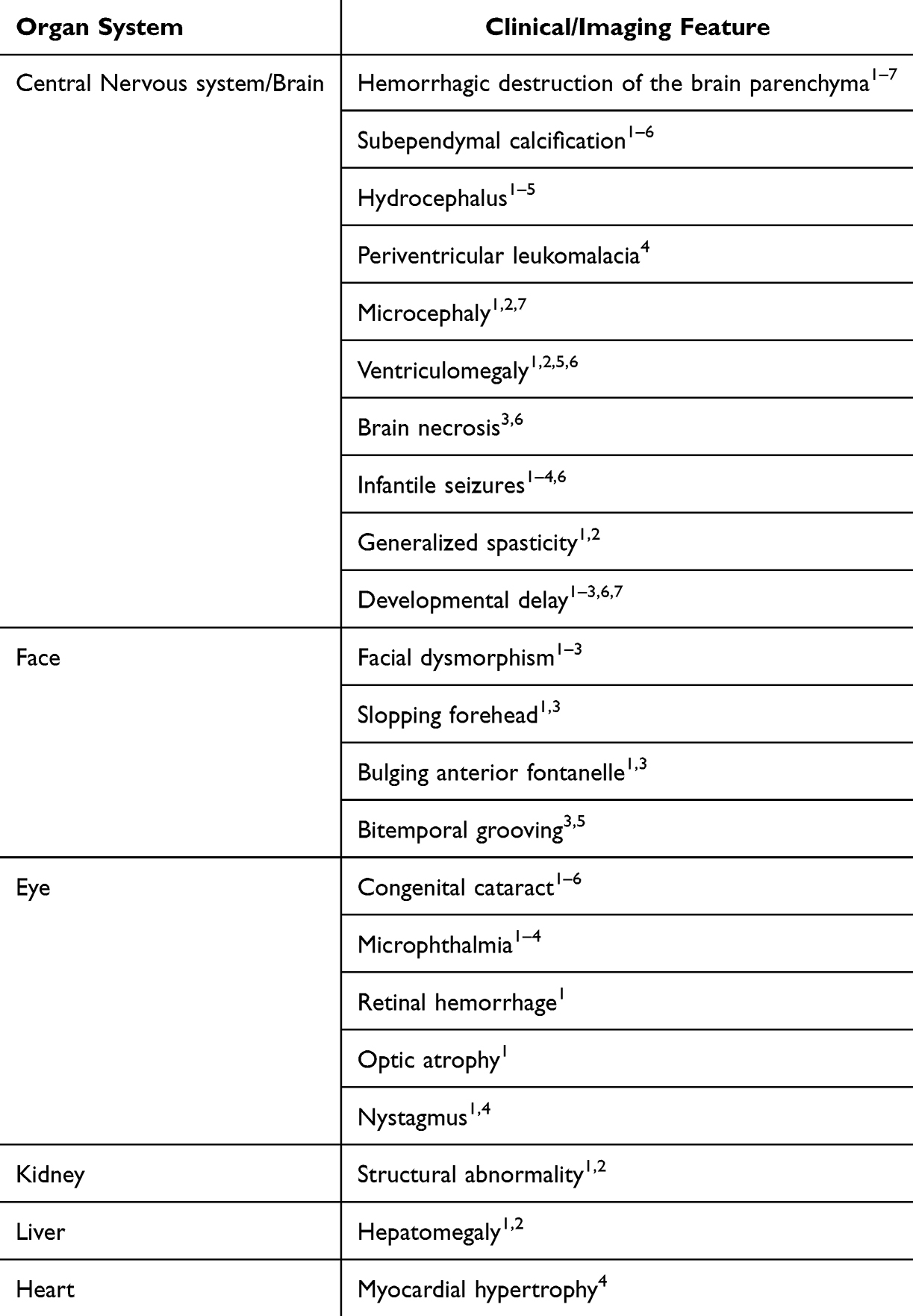 |
Table 1 A Summary of the Most Relevant Clinical and Neuroimaging Features in Patients with Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC) Syndrome |
Conclusion
Hemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC) is a rare syndrome caused by biallelic variants in the JAM3 gene with significant intrafamilial variability in clinical presentation and brain imaging phenotypes. It should be included in the differential diagnosis of children with congenital cataracts and neurodevelopmental abnormalities. Unique neuroradiologic findings and genetic testing can help the diagnosis.
Acknowledgments
We thank Dr. Lihadh Al-Gazali for providing original images included in Figures 2 and 3, and Jennifer E. Neil for her assistance in selection and deidentification.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kozak I, Ali SM, Hoque N, Lin D, Bosley TM. Retinal findings in Haemorrhagic Destruction of the Brain, Subependymal Calcification, and Congenital Cataracts (HDBSCC): case report and review. Neuroophthalmology. 2023;47(1):11–19. doi:10.1080/01658107.2022.2072517
2. Mochida GH, Ganesh VS, Felie JM, et al. A homozygous mutation in the tight-junction protein JAM3 causes hemorrhagic destruction of the brain, subependymal calcification, and congenital cataracts. Am J Hum Genet. 2010;87(6):882–889. doi:10.1016/j.ajhg.2010.10.026
3. Akawi NA, Canpolat FE, White SM, et al. Delineation of the clinical, molecular and cellular aspects of novel JAM3 mutations underlying the autosomal recessive hemorrhagic destruction of the brain, subependymal calcification, and congenital cataracts. Hum Mutat. 2013;34(3):498–505. doi:10.1002/humu.22263
4. De Rose DU, Gallini F, Battaglia DI, et al. A novel homozygous variant in JAM3 gene causing hemorrhagic destruction of the brain, subependymal calcification, and congenital cataracts (HDBSCC) with neonatal onset. Neurol Sci. 2021;42(11):4759–4765. doi:10.1007/s10072-021-05480-z
5. Xu M, Jin P, Huang Y, et al. Case report: prenatal diagnosis of fetal intracranial hemorrhage due to compound mutations in the JAM3 gene. Front Genet. 2022;13:1036231. doi:10.3389/fgene.2022.1036231
6. Abdallah Moady T, Odeh M, Fedida A, et al. Case report: novel insights into hemorrhagic destruction of the brain, subependymal calcification, and cataracts disease. Front Pediatr. 2023;11:1178280. doi:10.3389/fped.2023.1178280
7. Alshammari MJ, Shamseldin HE, Essbaiheen F, et al. Genomic analysis of presumed perinatal stroke in Saudi Arabia reveals a strong monogenic contribution. Hum Genet. 2024;143(1):59–69. doi:10.1007/s00439-023-02621-6
8. Bertoli-Avella AM, Beetz C, Ameziane N, et al. Successful application of genome sequencing in a diagnostic setting: 1007 index cases from a clinically heterogeneous cohort. Eur J Hum Genet. 2021;29(1):141–153. doi:10.1038/s41431-020-00713-9
9. Al-Kasbi G, Al-Murshedi F, Al-Kindi A, et al. The diagnostic yield, candidate genes, and pitfalls for a genetic study of intellectual disability in 118 Middle Eastern families. Sci Rep. 2022;12(1):18862. doi:10.1038/s41598-022-22036-z
10. Wyss L, Schafer J, Liebner S, et al. Junctional adhesion molecule (JAM)-C deficient C57BL/6 mice develop a severe hydrocephalus. PLoS One. 2012;7(9):e45619. doi:10.1371/journal.pone.0045619
11. Carlton VE, Harris BZ, Puffenberger EG, et al. Complex inheritance of familial hypercholanemia with associated mutations in TJP2 and BAAT. Nat Genet. 2003;34(1):91–96. doi:10.1038/ng1147
12. Wilcox ER, Burton QL, Naz S, et al. Mutations in the gene encoding tight junction claudin-14 cause autosomal recessive deafness DFNB29. Cell. 2001;104(1):165–172. doi:10.1016/S0092-8674(01)00200-8
13. Riazuddin S, Ahmed ZM, Fanning AS, et al. Tricellulin is a tight-junction protein necessary for hearing. Am J Hum Genet. 2006;79(6):1040–1051. doi:10.1086/510022
14. Burdon KP, McKay JD, Sale MM, et al. Mutations in a novel gene, NHS, cause the pleiotropic effects of Nance-Horan syndrome, including severe congenital cataract, dental anomalies, and mental retardation. Am J Hum Genet. 2003;73(5):1120–1130. doi:10.1086/379381
15. LeBlanc MA, Penney LS, Gaston D, et al. A novel rearrangement of occludin causes brain calcification and renal dysfunction. Hum Genet. 2013;132(11):1223–1234. doi:10.1007/s00439-013-1327-y
16. O’Driscoll MC, Daly SB, Urquhart JE, et al. Recessive mutations in the gene encoding the tight junction protein occludin cause band-like calcification with simplified gyration and polymicrogyria. Am J Hum Genet. 2010;87(3):354–364. doi:10.1016/j.ajhg.2010.07.012
17. Goncalves FG, Caschera L, Teixeira SR, et al. Intracranial calcifications in childhood: part 1. Pediatr Radiol. 2020;50(10):1424–1447. doi:10.1007/s00247-020-04721-1
18. Goncalves FG, Caschera L, Teixeira SR, et al. Intracranial calcifications in childhood: part 2. Pediatr Radiol. 2020;50(10):1448–1475. doi:10.1007/s00247-020-04716-y
19. Cen Z, Chen Y, Chen S, et al. Biallelic loss-of-function mutations in JAM2 cause primary familial brain calcification. Brain. 2020;143(2):491–502. doi:10.1093/brain/awz392
20. Schottlaender LV, Abeti R, Jaunmuktane Z, et al. Bi-allelic JAM2 variants lead to early-onset recessive primary familial brain calcification. Am J Hum Genet. 2020;106(3):412–421. doi:10.1016/j.ajhg.2020.02.007
21. Scala M, Wortmann SB, Kaya N, et al. Clinico-radiological features, molecular spectrum, and identification of prognostic factors in developmental and epileptic encephalopathy due to inosine triphosphate pyrophosphatase (ITPase) deficiency. Hum Mutat. 2022;43(3):403–419. doi:10.1002/humu.24326
22. Schoch K, Meng L, Szelinger S, et al. A recurrent de novo variant in NACC1 causes a syndrome characterized by infantile epilepsy, cataracts, and profound developmental delay. Am J Hum Genet. 2017;100(2):343–351. doi:10.1016/j.ajhg.2016.12.013
23. Buchert R, Tawamie H, Smith C, et al. A peroxisomal disorder of severe intellectual disability, epilepsy, and cataracts due to fatty acyl-CoA reductase 1 deficiency. Am J Hum Genet. 2014;95(5):602–610. doi:10.1016/j.ajhg.2014.10.003
24. Efthymiou S, Scala M, Nagaraj V, et al. Novel loss-of-function variants expand ABCC9-related intellectual disability and myopathy syndrome. Brain. 2024;147(5):1822–1836. doi:10.1093/brain/awae010
25. Carecchio M, Mainardi M, Bonato G. The clinical and genetic spectrum of primary familial brain calcification. J Neurol. 2023;270(6):3270–3277. doi:10.1007/s00415-023-11650-0
26. D’Onofrio G, Scala M, Severino M, et al. Expanding the phenotype associated with biallelic SLC20A2 variants. Eur J Hum Genet. 2023;31(7):725–729. doi:10.1038/s41431-023-01349-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.