")
Back to Journals » Infection and Drug Resistance » Volume 18
Stenotrophomonas Maltophilia Necrotizing Soft Tissue Infection in an Acute Myeloid Leukemia Patient
Authors Xu H, Xu Y, He H, Huang D, Su G, Huang D
Received 7 January 2025
Accepted for publication 21 April 2025
Published 3 June 2025 Volume 2025:18 Pages 2837—2844
DOI https://doi.org/10.2147/IDR.S512466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Hao Xu,1 Youhai Xu,1 Hesheng He,1 Dexi Huang,2 Guiping Su,1 Dongping Huang1
1Department of Hematology, The First Affiliated Hospital of Wannan Medical College, Yijishan Hospital, Wuhu, People’s Republic of China; 2Department of Laboratory Medicine, Tongling City Hospital, Tongling, People’s Republic of China
Correspondence: Dongping Huang, Department of Hematology, The First Affiliated Hospital of Wannan Medical College, Yijishan Hospital, West Zheshan Road 2, Wuhu, 241000, People’s Republic of China, Tel/Fax +86-0553-5739176, Email [email protected] Guiping Su, Department of Hematology, The First Affiliated Hospital of Wannan Medical College, Yijishan Hospital, West Zheshan Road 2, Wuhu, 241000, People’s Republic of China, Tel/Fax +86-0553-5739176, Email [email protected]
Abstract: We present a case of Stenotrophomonas maltophilia-induced soft tissue infection in a patient with acute myeloid leukemia (AML), who exhibited atypical symptoms and lab findings. The patient fully recovered following ultrasound-guided drainage and appropriate medical intervention. Due to Stenotrophomonas maltophilia’s multi-drug resistance and high mortality rate, we share this case to highlight the importance of timely diagnosis and treatment for this aggressive infection in immunocompromised individuals.
Keywords: acute myeloid leukaemias, stenotrophomonas maltophilia, drug resistance
Case
A 39-year-old male presented to our hematology emergency department with 7-day history of progressive lethargy and intermittent low-grade fever (38.2–38.9°C). Initial laboratory evaluation revealed leukocytosis (WBC 15.7×109/L) with 30% circulating blasts, normocytic anemia (Hb 100 g/L), and severe thrombocytopenia (platelets 5×109/L). The combined diagnosis of bone marrow morphology and flow cytometry confirmed acute myeloid leukemia (AML, FAB M2 subtype according to WHO classification), and he was treated with induction chemotherapy at our institution. Two days later, he developed high-grade fever (39.6°C) with profound neutropenia (ANC 0.1×109/L) and elevated CRP (15.77 mg/L, ref: <5 mg/L). Initiated first-line empirical therapy with cefoperazone-sulbactam (3g q8h) per institutional protocol. On the 5th day, recrudescent fever (38.8°C) occurred with worsening cytopenias (WBC 0.2×109/L, ANC 0×109/L) and progressive CRP (25.82 mg/L), and procalcitonin elevation (10.26 ng/mL; normal <0.5 ng/mL). The regimen was escalated to imipenem (1000 mg q6h), etimicin (200 mg qd), and posaconazole (200 mg tid) prophylaxis, after which his fever subsided. On the 14th day, the treatment was adjusted to piperacillin-tazobactam (4.5 g q8h) with continued etimicin and posaconazole for agranulocytosis. On the 17th day, new-onset left thigh pain emerged alongside febrile episodes (peak 39.2°C), with CRP rising to 17.91 mg/L. Vancomycin (1 g q12h) was added for suspected Gram-positive breakthrough infection. However, the clinical condition continued to progress, the patient manifested septic progression (peak temperature 40.1°C) with paradoxical CRP surge (123.0 mg/L) and elevated procalcitonin (0.556 ng/mL) on the 19th day. No organisms were identified on Gram stain or blood culture. Physical examination revealed mild left thigh swelling without cutaneous erythema or fluctuance (Figure 1). He then received empirical antimicrobial therapy with tigecycline (Initial Dose: 100 mg, Maintenance Dose: 50 mg, every 12 hours), imipenem, posaconazole (200 mg tid), and caspofungin (Loading Dose: 70 mg, on Day 1. Maintenance Dose: 50 mg, once daily starting from Day 2). Contrast-enhanced MRI demonstrated multifocal intramuscular edema in the vastus lateralis muscles suggesting pyogenic collection (Figure 2). On day +23, ultrasound-guided aspiration retrieved 18 mL of hemorrhagic exudate (Figure 3) for metagenomic sequencing and microbial culture. His clinical condition and lab results have gradually improved following empirical antimicrobial therapy. On day 26, lab results were: WBC 3.8 × 10^9/L (neutrophils 51.5%), platelets 209 × 10^9/L, CRP 32.27 mg/L, procalcitonin 0.097 ng/mL. Serum β-D glucan levels were within normal limits, and the galactomannan antigen test was negative, he was switched to vancomycin and cefoperazone-sulbactam for anti-infective treatment. Two day later, metagenomic next-generation sequencing detected Stenotrophomonas maltophilia-specific sequences at 18.72% relative abundance (CCAGCCGGGTGACGGCGGGGGCGTGTGAGGTCATGGGGGTACCGCTGGAG). Concurrent aerobic culture on 5% sheep blood agar grew non-hemolytic, yellow-pigmented colonies (Figure 4A). Definitive identification via VITEK-2 system (BioMérieux, France) confirmed S. maltophilia. He was subsequently transitioned to empirical therapy with trimethoprim-sulfamethoxazole (TMP-SMZ) (800 mg q12h of trimethoprim component) and cefoperazone-sulbactam. Before long, antimicrobial susceptibility testing (Table 1) and The Kirby-Bauer test (Figure 5) revealed susceptibility to TMP-SMZ, cefoperazone-sulbactam, tigecycline, levofloxacin hydrochloride, and ceftazidime. Consequently, the patient continued to receive TMP-SMZ and cefoperazone-sulbactam for therapy, which led to a swift improvement in local symptoms. Enhanced MRI also demonstrated a reduction in muscle and soft tissue edema and effusion (Figure 6). The chronology of the patient’s hospital courses is described in Figure 7.
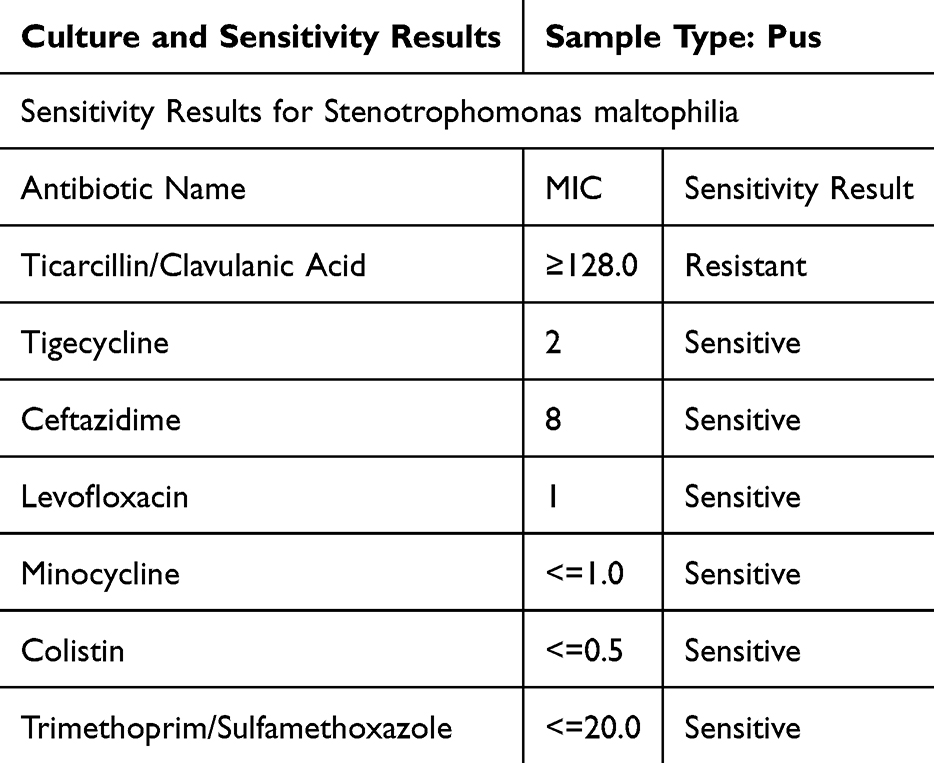 |
Table 1 The Drug Sensitivity Test Results for the Patient’s Pus |
 |
Figure 1 Appearance of the patient’s legs throughout the duration of the treatment. |
 |
Figure 2 In the early stages, enhanced magnetic resonance imaging (MRI) revealed swelling in the anterolateral muscles of the left femur. |
 |
Figure 3 Appearance of abscess drainage fluid. |
 |
Figure 4 The microbial agar culture results of the drainage fluid: (A) left is the macroscopic view. (B) right shows the microbial morphology under oil immersion. |
 |
Figure 5 Disk diffusion method for testing drug sensitivity in drainage fluid. |
 |
Figure 6 After symptomatic treatment., the anterolateral muscles of the left femur of MRI. |
 |
Figure 7 Timeline of the patient’s hospitalization. |
Discussion
Stenotrophomonas maltophilia is a gram-negative bacillus that infects immunocompromised individuals, notably those with neutropenia or receiving chemotherapy and broad-spectrum antibiotics.1 This pathogen has been implicated in a wide range of infections, including pneumonia, bloodstream infections, catheter-related infections, and complicated biliary infections. Less commonly, it has been associated with skin and soft tissue infections (SSTIs).2,3 Herin, we report the first locally recorded case of S. maltophilia-induced soft tissue infection in a hematological malignancy patient.
Stenotrophomonas maltophilia infections often coexist with other pathogens (such as Enterococcus spp., coagulase-negative staphylococci, and Pseudomonas aeruginosa), complicating antibiotic selection and increasing the complexity of diagnosis and treatment,4 besides, S. maltophilia exhibits intrinsic resistance to a wide range of antibiotics, including beta-lactams, aminoglycosides, and carbapenems,5 which closely linked to S. maltophilia’s expression of L1 metallo-β-lactamase and L2 extended-spectrum β-lactamase, the L1 enzyme can hydrolyze carbapenems, while the L2 enzyme has broad hydrolytic activity against cephalosporins and penicillins.6 This resistance resulted a significant mortality rate, with a systematic review indicating an attributable mortality rate of 37.5%.7 Moreover, diagnosing STIs in immunocompromised patients is challenging, as they often lack the typical symptoms like pain, erythema, edema, and fever seen in immunocompetent individuals8 which can result in delayed diagnosis and treatment, adversely affecting outcomes. Therefore, early and accurate diagnosis of STIs by S. maltophilia, along with timely intervention, is crucial for improving patient outcomes.
For this patient, his left thigh was mildly swollen and tense, limiting walking, yet without any signs of erythema, ulceration, and subcutaneous crepitus. Blood tests showed neutropenia, and there was no abscess evident at the infection site initially. His severe condition worsened despite receiving broad-spectrum antibiotics. To differentiate the source of symptoms as leukemic infiltration or soft tissue infection, he underwent enhanced MRI, which facilitated the diagnosis of a STI. The abscess did not form until neutrophil counts rebounded. Following, ultrasound-guided drainage was performed. Both the pus culture and metagenomic sequencing identified Stenotrophomonas maltophilia, and antibiotic therapy was adjusted based on the susceptibility results. Fortunately, he had fully recovered.
The excessive use of broad-spectrum antibiotics has contributed to an increase in Stenotrophomonas maltophilia infections among cancer patients.2 When cancer patients display atypical symptoms of muscular soft tissue following treatment with carbapenem antibiotics, it is crucial to maintain a high level of suspicion for S. maltophilia-induced soft tissue infections (STIs) and to initiate prompt empirical treatment. Enhanced MRI facilitates swift and conclusive diagnosis.9 Trimethoprim-sulfamethoxazole is recognized as the preferred empirical therapy for S. maltophilia infections.10,11 Once neutrophil counts rebound, ultrasound-guided drainage should be performed, and antibiotic treatment should be tailored to the drug sensitivity profile. This approach can significantly improve patient outcomes and reduce mortality.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation. For data inquiries, please contact [email protected].
Ethics Approval and Consent to Participate
All procedures performed in the study involving human participants were in accordance with the ethical standards of the Ethics Committee of the Yijishan Hospital, and no institutional approval is needed to publish the details of this case.
Consent for Publication
Written informed consent was obtained from the individual, for the publication of any potentially identifiable images or data included in this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Anhui Provincial University Scientific Research Project (Number: 2023AH040255).
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Sayed HA, El AA, Ismail A. Development of mortality statistics at governmental hospitals, Egypt. J Egypt Public Health Assoc. 2003;78(5–6):397–415.
2. Safdar A, Rolston KV. Stenotrophomonas maltophilia: changing spectrum of a serious bacterial pathogen in patients with cancer. Clin Infect Dis. 2007;45(12):1602–1609. doi:10.1086/522998
3. Gales AC, Jones RN, Forward KR, Linares J, Sader HS, Verhoef J. Emerging importance of multidrug-resistant Acinetobacter species and stenotrophomonas maltophilia as pathogens in seriously ill patients: geographic patterns, epidemiological features, and trends in the sentry antimicrobial surveillance program (1997-1999). Clin Infect Dis. 2001;32(Suppl 2):S104–13. doi:10.1086/320183
4. Brooke JS. Stenotrophomonas maltophilia: an emerging global opportunistic pathogen. Clin Microbiol Rev. 2012;25(1):2–41. doi:10.1128/CMR.00019-11
5. Chang YT, Lin CY, Chen YH, Hsueh PR. Update on infections caused by stenotrophomonas maltophilia with particular attention to resistance mechanisms and therapeutic options. Front Microbiol. 2015;6:893. doi:10.3389/fmicb.2015.00893
6. Okazaki A, Avison MB. Induction of L1 and L2 beta-lactamase production in Stenotrophomonas maltophilia is dependent on an AmpR-type regulator. Antimicrob Agents Chemother. 2008;52(4):1525–1528. doi:10.1128/AAC.01485-07
7. Wang X, Yang Z, Miu W, et al. A simple and convenient synthesis of 3-salicyloylquinoline-4-carboxylic esters from chromone and isatin. Rsc Adv. 2019;9(63):37057–37060. doi:10.1039/C9RA08124K
8. Keung EZ, Liu X, Nuzhad A, Adams C, Ashley SW, Askari R. Immunocompromised status in patients with necrotizing soft-tissue infection. JAMA Surg. 2013;148(5):419–426. doi:10.1001/jamasurg.2013.173
9. Weaver JS, Omar IM, Mar WA, et al. Magnetic resonance imaging of musculoskeletal infections. Pol J Radiol. 2022;87:e141–62. doi:10.5114/pjr.2022.113825
10. Sarzynski SH, Warner S, Sun J, et al. Trimethoprim-sulfamethoxazole versus levofloxacin for stenotrophomonas maltophilia infections: a retrospective comparative effectiveness study of electronic health records from 154 us hospitals. Open Forum Infect Dis. 2022;9(2):ofab644. doi:10.1093/ofid/ofab644
11. Peng Y, Xu S, Chen G, Wang L, Feng Y, Wang X. L-3-n-butylphthalide improves cognitive impairment induced by chronic cerebral hypoperfusion in rats. J Pharmacol Exp Ther. 2007;321(3):902–910. doi:10.1124/jpet.106.118760
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.