")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Study on the Combined Application of Occlusal Splint and Intra-Articular Injection of Hyaluronic Acid in the Treatment of Non-Reducible Anterior Disc Displacement of the Temporomandibular Joint
Authors Bi K, Cheng G, Wu X, Lv Z
Received 30 January 2025
Accepted for publication 6 April 2025
Published 23 April 2025 Volume 2025:21 Pages 523—532
DOI https://doi.org/10.2147/TCRM.S518989
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Ke Bi, Gang Cheng, Xiuyin Wu, Zhijun Lv
Department of Stomatology, Affiliated People’s Hospital of Shandong First Medical University, Jinan, People’s Republic of China
Correspondence: Zhijun Lv, Email [email protected]
Objective: To investigate the effect of combining intra-articular injection of hyaluronic acid (HA) with occlusal splint therapy in the treatment of non-reducible anterior disc displacement of the temporomandibular joint (ADDWoR).
Methods: A retrospective analysis was conducted on the clinical data of 62 patients with ADDWoR admitted to our hospital from April 2023 to June 2024. According to the treatment method received, patients were divided into a control group (n=31, treated with occlusal splints) and an observation group (n=31, treated with occlusal splints combined with intra-articular injection of HA). The clinical treatment effects, pain levels (Visual Analog Scale [VAS]), temporomandibular joint dysfunction (Friction Temporomandibular Joint Dysfunction Index [CMI]), mandibular movement function (maximum mouth opening [MMO], left lateral excursion [LLE], right lateral excursion [RLE], protrusive movement [PM]), clinical aesthetic indicators (condylar height, joint space width), and adverse reactions were compared between the two groups.
Results: (1) Clinical Efficacy: The observation group had a higher total effective rate (90.32% vs 67.74%, P < 0.05). (2) Pain & Dysfunction: Both groups showed significant improvement in VAS and CMI scores over time, with the observation group exhibiting greater reductions (P < 0.05). (3) Mandibular Function & Aesthetic Indicators: The observation group had greater improvements in MMO, LLE, RLE, PM, condylar height, and joint space width (P < 0.05). (4) Adverse Reactions: No significant difference in adverse reaction rates (P > 0.05).
Conclusion: The combination of intra-articular injection of HA with occlusal splint therapy can further improve the treatment outcomes for ADDWoR patients, alleviate pain, improve temporomandibular joint dysfunction and mandibular movement function, promote aesthetic recovery, and does not increase the risk of adverse reactions.
Keywords: occlusal splint, intra-articular injection of HA, non-reducible anterior disc displacement of the temporomandibular joint, ADDWoR, treatment efficacy
Introduction
The temporomandibular joint (TMJ) is one of the most complex synovial joints in the human body, and its normal function plays a crucial role in daily activities such as chewing, speaking, and facial expressions.1 However, due to the complex anatomy and the interaction of various etiological factors, temporomandibular joint disorders (TMDs) have become one of the most common oral and maxillofacial diseases.2 Among these disorders, non-reducible anterior disc displacement of the temporomandibular joint (ADDWoR) is a typical and severe pathological condition.3 The main characteristic of ADDWoR is the permanent displacement of the articular disc, which cannot be spontaneously repositioned during mandibular movements. Patients typically present with limited mouth opening, joint pain, the absence of joint clicking, and chewing dysfunction. In severe cases, asymmetric changes in the jaw and face may occur, significantly affecting the patient’s quality of life and psychological well-being.4,5
In recent years, intra-articular therapies have gained prominence as minimally invasive options for TMDs, particularly when conservative treatments fail. Hyaluronic acid (HA) injections are increasingly recommended for patients with persistent pain, synovitis, or degenerative changes, aiming to restore joint lubrication and reduce inflammation.6 However, the timing of intervention remains debated; HA is typically administered after failed splint therapy or as an adjunct to physical modalities.7 Notably, intra-articular drug administration carries risks such as transient pain, infection (incidence <1%), and rare hypersensitivity reactions.8
Recent advancements in TMD management also include emerging modalities like photobiomodulation (PBM) and low-intensity pulsed ultrasound (LIPUS). PBM utilizes light therapy to reduce inflammation and promote tissue repair, while LIPUS enhances cartilage regeneration through mechanical stimulation.9,10 Despite their potential, these therapies lack robust evidence for ADDWoR-specific efficacy compared to established approaches like HA injection.
Currently, the treatment of ADDWoR is divided into conservative and surgical approaches. Conservative treatments include pharmacotherapy, physical therapy, occlusal splints, and intra-articular injections. In this study, patients were required to discontinue other therapies (eg, analgesics, physiotherapy) during the trial period to eliminate confounding effects. Occlusal splints are widely used for mild-to-moderate cases due to their ability to redistribute joint loading and improve disc position.11 However, their efficacy diminishes in chronic or severe cases, necessitating adjunct therapies.12
Intra-articular HA injection addresses these limitations by supplementing synovial fluid viscosity, reducing friction between displaced discs and condyles.13 Notably, our protocol involved lower joint compartment injections guided by ultrasound, as upper compartment access may risk articular eminence perforation.14 Prior to HA administration, joints were lavaged with 1 mL of 2% lignocaine—a choice based on its dual anesthetic and diagnostic utility: pain relief during lavage confirms accurate needle placement.15 While multi-electrolyte solutions are common, lignocaine’s immediate analgesic effect may enhance patient tolerance without altering HA’s therapeutic outcomes.16
Given the individual advantages of occlusal splints and HA injections, their combined use may synergistically improve outcomes. This study aims to evaluate this hypothesis. By elucidating the efficacy of combined therapy, we seek to optimize ADDWoR management strategies.
Materials and Methods
Study Design and Participants
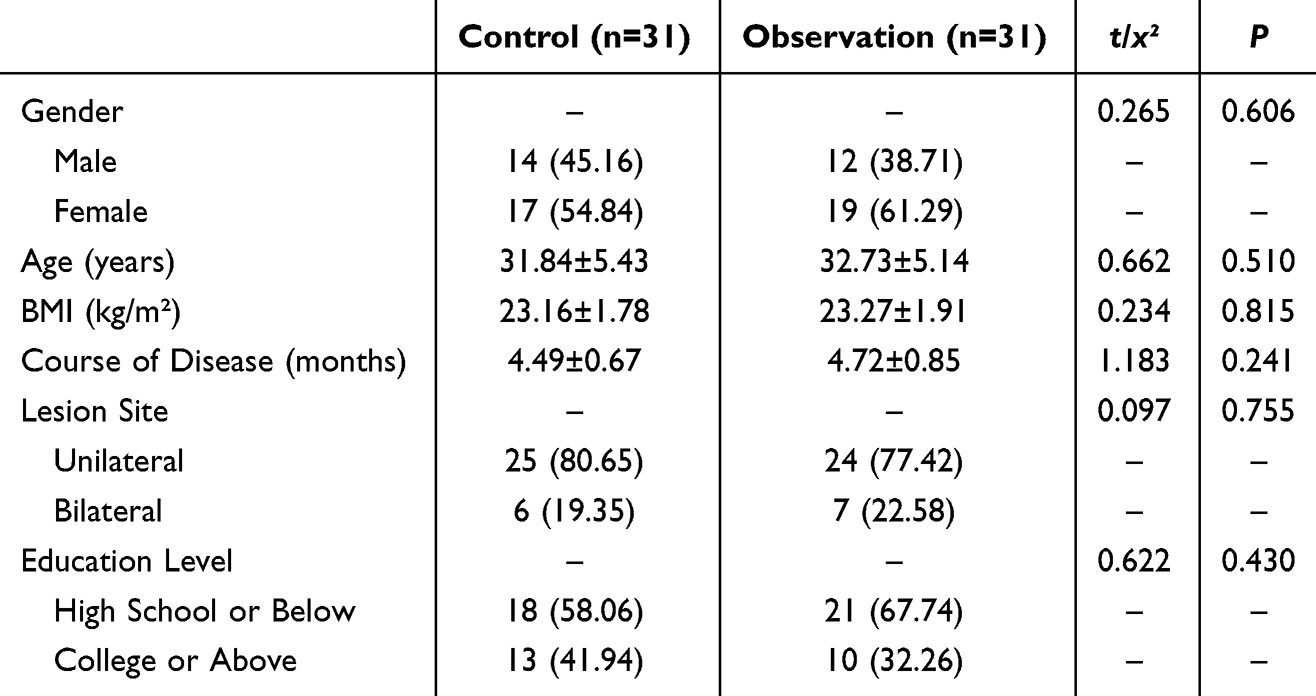
This retrospective cohort study analyzed 62 patients diagnosed with non-reducible anterior disc displacement (ADDWoR) at our hospital between April 2023 and June 2024. Sample size was determined based on historical case availability and feasibility, as retrospective studies often lack formal power calculations.15 Patients were divided into two groups: the control group (n=31, occlusal splint only) and observation group (n=31, splint + HA injection). Group allocation was based on the initial treatment received, as recorded in medical charts. To address potential selection bias, baseline demographic and clinical characteristics (eg, gender, age, body mass index (BMI), course of disease, lesion site, and education level) were statistically compared between groups (Table 1).
 |

Inclusion and Exclusion Criteria
Inclusion criteria: (1) Diagnosis of ADDWoR confirmed by MRI (disc displacement without reduction on dynamic imaging);16 (2) ≥2 symptoms: pain (VAS ≥4), limited mouth opening (<35 mm), joint clicking, or jaw dysfunction; (3) No prior TMD treatment; (4) patients were aged ≥18 years and ≤65 years, regardless of sex; (5) the patients and their families were fully informed and provided written consent to participate in the study.
Exclusion criteria: (1) Active oral infections, systemic arthritis, or acute TMJ trauma; (2) Contraindications to HA/splint therapy (eg, allergy, severe malocclusion); (3) history of mental illness or cognitive dysfunction; (4) inability to cooperate with the study due to any reason.
This study was approved by the People’s Hospital Affiliated to Shandong First Medical University Medical Ethics Committee (approval number: 24-KQ00013), and all procedures followed the ethical guidelines of the Declaration of Helsinki.
Interventions
Control Group
Occlusal Splint: Custom-made hard acrylic splints (3 mm thickness) fabricated from upper/lower arch impressions. Thickness was standardized to minimize vertical dimension changes while redistributing occlusal forces.17 Patients wore splints ≥10 h/day for 3 months. Adjustments were made biweekly by a single clinician using articulating paper to eliminate premature contacts.
Observation Group
Combined Therapy: Splint + two HA injections (Hylan G-F 20, 1 mL) into the lower joint compartment (superior joint space injections avoided due to perforation risks).18
Injection Protocol:
Patient Positioning: Seated with head tilted contralaterally.
Landmark-Guided Technique: 25-gauge needle inserted 2 mm inferior to the tragus-condylar depression. Real-time confirmation via mandibular manipulation (needle movement synchronized with condyle).
Lavage: 2% lidocaine (1 mL) was injected first for diagnostic confirmation (pain relief ≤2 min indicated correct placement) and lavage.19 Rationale: Lidocaine’s immediate analgesic effect improved procedural tolerance without altering HA efficacy.
HA Administration: Post-lavage, 1 mL HA injected slowly. Repeat injection at 2 weeks.14
Observation Indicators
(1) Clinical Treatment Effectiveness: The evaluation was conducted 3 months after treatment. The criteria were as follows: Effective: Mouth opening range 3–3.4 cm, normal mouth opening type and jaw movement, no joint clicking, and absence of pain. Improved: Mouth opening <3 cm, normal mouth opening type, no joint clicking or pain, but occasional tenderness in the joint area and surrounding muscles. Ineffective: No significant improvement or even worsening of clinical symptoms and signs. The total effective rate = 100% - (number of ineffective cases / total number of cases × 100%).
(2) Pain Assessment: Pain was evaluated using the Visual Analog Scale (VAS) at baseline, 1 month, and 3 months after treatment. The VAS score ranged from 0 to 10, with higher scores indicating more severe pain (Cronbach’s α = 0.863, validity = 0.841).20
(3) Temporomandibular Joint Disorder Assessment: The Friction Temporomandibular Joint Disorder Index (CMI) was used to assess the temporomandibular joint disorder at baseline, 1 month, and 3 months post-treatment. The CMI score ranged from 0 to 1, with lower scores indicating better temporomandibular joint function (Cronbach’s α = 0.879, validity = 0.856).21
(4) Jaw Movement Function: The following four measures were assessed: maximum active mouth opening (MMO), left lateral excursion (LLE), right lateral excursion (RLE), protrusive movement (PM). Measurements were taken at baseline and 3 months post-treatment. Larger values indicated better function. MMO was measured using a caliper by recording the distance between the upper and lower incisors when the patient opened their mouth as wide as possible. LLE, RLE, and PM were measured using a T-scanIII occlusal force meter. The patient was seated upright, and the occlusal strip was placed between the upper and lower dental arches, ensuring it was parallel to the occlusal plane. The patient was instructed to perform left and right lateral movements and protrusion movements, and measurements were recorded. After a 3-minute rest, a second set of measurements was taken, and the average of three measurements was used for analysis.
(5) Clinical Aesthetic Indicators: Condylar height and joint space width were measured using magnetic resonance imaging at baseline and post-treatment, and the data were recorded.
(6) Adverse Reactions: Adverse reactions including occlusal splint discomfort, dizziness, headache, nausea, vomiting, local swelling, and joint inflammation were recorded by the hospital’s medical staff.
Additional Notes: No electromyography (EMG) was performed due to retrospective design limitations. Splint compliance monitored via patient logs and intraoral scans for wear patterns.
Statistical Analysis
GraphPad Prism 8 was used for graphing, and SPSS 22.0 was used for data analysis. For categorical data, percentages (%) were reported, and chi-square tests were used for analysis. For continuous data, the ( ) was reported, and independent t-tests were used for comparison between two groups. Paired t-tests were used for comparisons within the same group, and repeated measures ANOVA was used for comparisons at different time points within groups. A p-value < 0.05 was considered statistically significant.
) was reported, and independent t-tests were used for comparison between two groups. Paired t-tests were used for comparisons within the same group, and repeated measures ANOVA was used for comparisons at different time points within groups. A p-value < 0.05 was considered statistically significant.
Results
Comparison of Baseline Data
The comparison of baseline data, including gender, age, body mass index (BMI), course of disease, lesion site, and education level between the two groups showed no significant differences (P > 0.05), indicating comparability, see Table 1.
Clinical Efficacy
The observation group demonstrated superior clinical outcomes compared to the control group (total effective rate: 90.32% vs 67.74%, P < 0.05, Figure 1). Notably, the combined therapy group showed a 2.3-fold higher rate of “markedly effective” outcomes (35.5% vs 19.4%), suggesting synergistic effects of HA injection and splint therapy, as shown in Figure 1.
 |
Figure 1 Comparison of Clinical Treatment Effects [n(%)]. Note: Comparison between groups, *P < 0.05. |
Comparison of Pain Levels
The group (F=6.284), time (F=8.031), and interaction (F=7.396) comparisons of VAS scores between the two groups were significant (P < 0.05). Within-group: VAS scores were lower at 1 month and 3 months after treatment compared to pre-treatment, and the VAS score at 3 months was lower than at 1 month (P < 0.05). Between groups: There were no significant differences in VAS scores before treatment (P > 0.05), but at 1 month and 3 months after treatment, the VAS scores in the observation group were lower than those in the control group (P < 0.05), as shown in Figure 2.


Comparison of Temporomandibular Joint Dysfunction
The group (F=4.976), time (F=6.843), and interaction (F=5.897) comparisons of CMI scores between the two groups were significant (P < 0.05). Within-group: CMI scores were lower at 1 month and 3 months after treatment compared to pre-treatment, and the CMI score at 3 months was lower than at 1 month (P < 0.05). Between groups: No significant difference was found in CMI scores before treatment (P > 0.05), but at 1 month and 3 months after treatment, the CMI scores in the observation group were lower than those in the control group (P < 0.05), as shown in Figure 3.


Comparison of Mandibular Movement Function
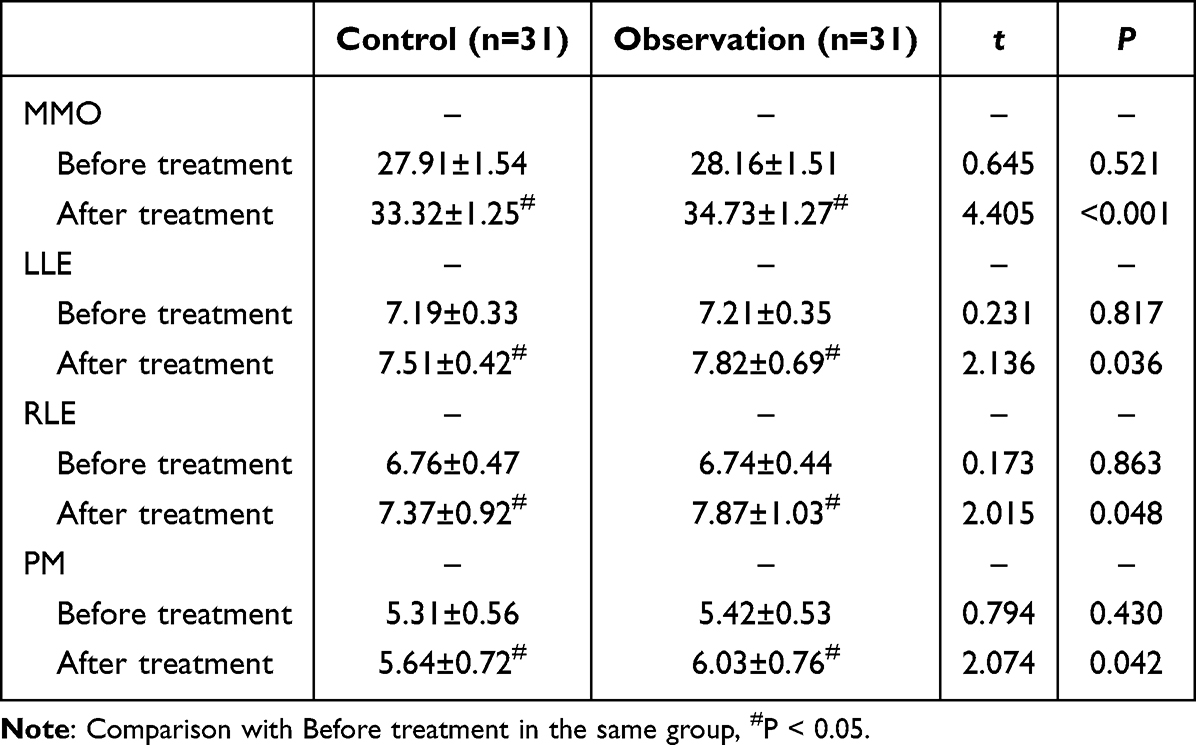
Both groups showed increased MMO, LLE, RLE, and PM after treatment compared to pre-treatment, with a greater change observed in the observation group (P < 0.05), as shown in Table 2.
 |

Comparison of Clinical Aesthetic Indicators
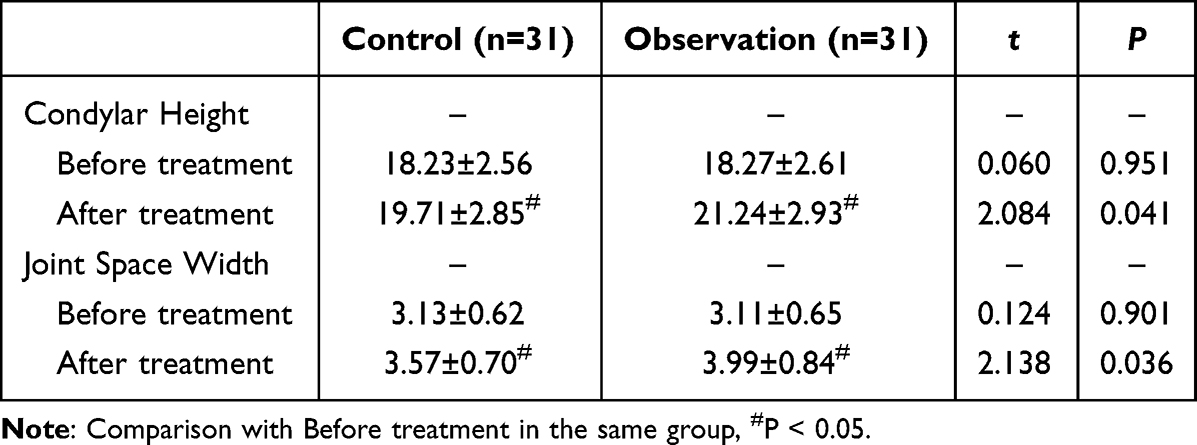
Both groups showed increased condylar height and joint space width after treatment compared to pre-treatment, with a greater change observed in the observation group (P < 0.05), as shown in Table 3.
 |

Comparison of Adverse Reactions
The adverse reaction rates were 12.90% in the control group and 19.35% in the observation group, with no significant difference between the groups (P > 0.05), as shown in Table 4.
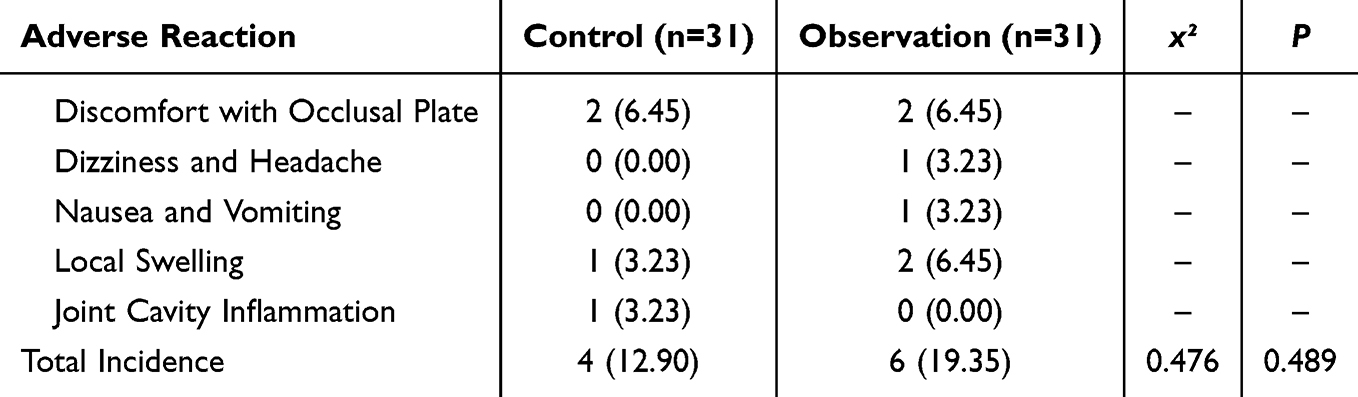 |
Table 4 Comparison of Adverse Reactions [n(%)] |
Discussion
ADDWoR is a common and complex TMJ disorder, primarily characterized by the anterior displacement of the articular disc, which cannot return to its normal position during mandibular movement.22 This disease is often associated with symptoms such as pain, restricted mouth opening, and joint clicking, significantly affecting the patient’s daily life and mental health.23 Although various treatment methods are currently available, conservative treatments (such as occlusal splint therapy) remain the most widely used. However, relying solely on occlusal splint therapy often fails to meet the full therapeutic needs of ADDWoR patients, especially in those with a longer disease duration or more severe joint damage. Therefore, this study explored the efficacy of combined intra-articular HA injection on the basis of occlusal splint therapy for ADDWoR patients, aiming to provide a new treatment approach for clinical practice and further validate the advantages of combination therapy in pain relief, improving joint function, and promoting joint structure recovery.This study demonstrates that combining occlusal splint therapy with intra-articular HA injection significantly improves clinical outcomes in ADDWoR patients, achieving a 90.32% efficacy rate compared to 67.74% with splint alone. The synergy likely stems from HA’s dual mechanical and biological effects: (1) reducing disc-condyle friction via viscoelastic lubrication,24 and (2) suppressing synovial inflammation through CD44 receptor-mediated inhibition of IL-6/NF-κB pathways.25 These mechanisms complement the splint’s ability to unload the joint by redistributing occlusal forces,26 providing a multi-targeted approach to address both structural and inflammatory aspects of ADDWoR; however, in some patients, relying solely on the splint cannot fully restore the biomechanical function of the joint, particularly when the disc displacement is severe. While novel modalities like photobiomodulation (PBM) and low-intensity pulsed ultrasound (LIPUS) show promise in TMD management, their efficacy in ADDWoR remains uncertain. PBM primarily targets pain via mitochondrial cytochrome C oxidase activation,27 and LIPUS enhances cartilage repair through mechanotransduction.28 However, neither directly addresses the biomechanical derangement of disc displacement—a critical advantage of HA’s lubricating action. The results of this study indicate that at 1 month and 3 months post-treatment, the VAS scores of the observation group were significantly lower than those of the control group. Furthermore, within-group comparisons showed that the VAS score at 3 months post-treatment was lower than at 1 month (P < 0.05), suggesting that combined therapy can relieve pain in the short term, with further pain reduction as treatment continues. The reason for this may be that HA injection, through its lubricating effect, reduces joint friction and alleviates pain caused by the anterior displacement of the articular disc. Moreover, HA has certain anti-inflammatory effects, helping to reduce inflammation within the joint and further improve pain perception.29 Our results align with recent study showing HA injections yield superior pain reduction (ΔVAS −2.8 vs −1.3 for PBM) and functional improvement in disc displacement disorders.30 Temporomandibular joint dysfunction is one of the main manifestations of ADDWoR, typically presenting as chewing dysfunction, limited mandibular range of motion, and joint locking.31 In this study, at both 1 month and 3 months post-treatment, the CMI scores of the observation group were significantly lower than those of the control group, with the scores at 3 months post-treatment further reduced compared to 1 month (P < 0.05). This suggests that combined therapy can effectively improve the functional state of the TMJ in patients. Intra-articular HA injection can improve the viscoelasticity of synovial fluid and promote the repair of articular cartilage, effectively reducing joint damage caused by the anterior displacement of the disc, thereby alleviating joint dysfunction.32 The occlusal splint works by adjusting the mandibular position, reducing the pressure on the articular disc, and improving the biomechanical state of the joint.33 The synergistic effect of both therapies helps restore normal joint function and relieve clinical symptoms. In addition, this study also evaluated the recovery of mandibular movement function. The results indicated that, compared with the control group, the observation group showed significant improvements in MMO, LLE, RLE, and PM levels (P < 0.05). This suggests that combined therapy is more effective in improving joint mobility compared to using the occlusal splint alone. Combined therapy reduces joint friction through HA’s lubricating effect, facilitates disc repositioning, and, at the same time, the occlusal splint alleviates joint overloading by adjusting the occlusion, helping to restore the normal range of mandibular movement. Furthermore, the restoration of TMJ function not only helps relieve pain and movement dysfunction but also improves the patient’s facial appearance.34,35 The results of this study show that, post-treatment, the condylar height and joint space width in the observation group were significantly greater than those in the control group (P < 0.05), indicating that combined therapy has a greater advantage in improving the biomechanical function of the TMJ and facial aesthetics. The potential reason for this is that HA injection helps restore joint structure and promotes disc repositioning and soft tissue repair through its lubricating effect,36 ultimately contributing to the recovery of normal TMJ function and facial appearance. Finally, regarding adverse reactions during treatment, the study results showed no significant difference in the incidence of adverse reactions between the two groups (P > 0.05), indicating that combined therapy did not significantly increase the risk of adverse reactions. HA injection, as a treatment method with a relatively high safety profile, has been widely used in various joint diseases, with most adverse reactions being mild and localized, such as transient pain and swelling at the injection site, which are generally well tolerated by patients.37,38 In this study, the safety of combined therapy was further validated, providing strong support for clinical practice.Although this study draws positive conclusions through retrospective analysis, some limitations still exist. Single-center retrospective design with potential selection bias (eg, healthier patients opting for combined therapy). Prospective RCTs using stratified randomization by disc displacement severity are needed to confirm causality. Short follow-up (3 months) precludes assessment of HA’s durability. Studies show HA effects peak at 6 months, warranting longer-term tracking. Subjective endpoints (VAS, CMI) dominate outcomes. Future work should integrate quantitative MRI biomarkers (eg, synovial fluid volume) and serum inflammatory markers (IL-1β, TNF-α) for objective validation. Lack of active comparators (eg, PBM, LIPUS). Head-to-head trials could clarify HA’s relative value in multimodal TMD algorithms.
Conclusion
In conclusion, combining intra-articular HA injection with occlusal splint therapy significantly improves the treatment outcomes for ADDWoR patients, alleviates pain, improves joint function, restores facial aesthetics, and demonstrates a high level of safety. Combined HA-splint therapy offers a safe, effective strategy for ADDWoR by synergizing mechanical stabilization (splint) with biological modulation (HA). While emerging therapies like LIPUS/PBM target specific pain pathways, our approach addresses the disorder’s biomechanical core—a paradigm warranting further exploration in precision TMD management.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ma MQ, Shang T, Mao Y, et al.. Research advances of complications regarding temporomandibular joint prosthesis replacement. Zhonghua Kou Qiang Yi Xue Za Zhi. 2024;59(10):1059–1064. doi:10.3760/cma.j.cn112144-20240611-00237
2. Li CX, Song ZQ, Jin X, et al.. Interpretation of a clinical practice guideline on the management of chronic pain associated with temporomandibular joint disorders. Zhonghua Kou Qiang Yi Xue Za Zhi. 2024;59(10):988–997. doi:10.3760/cma.j.cn112144-20231229-00313
3. Li CX, Liu X, Gong Z-C, et al.. Effects of condyle on disc status of the reducing and nonreducing anterior disc displacement of the temporomandibular joint based on 3D reconstructive imaging: a pilot study. Quintessence Int. 2023;54(2):156–166. doi:10.3290/j.qi.b3512027
4. Dong M, Sun Q, Yu Q, Tao X, Yang C, Qiu W, et al.. Determining the optimal magnetic resonance imaging sequences for the efficient diagnosis of temporomandibular joint disorders. Quant Imaging Med Surg. 2021;11(4):1343–1353. doi:10.21037/qims-20-67
5. Igarashi C, Kobayashi K, Ito H, et al.. Clinical and magnetic resonance imaging findings in patients with and without improvement after mandibular manipulation and conservative physical therapy for temporomandibular joint disorders. Oral Surg Oral Med Oral Pathol Oral Radiol. 2023;135(2):294–302. doi:10.1016/j.oooo.2022.09.008
6. Heo HA, Park S, Pyo SW, Yoon HJ, et al.. Clinical outcomes of patients with unilateral internal derangement of the temporomandibular joint following arthrocentesis and stabilization splint therapy. Maxillofac Plast Reconstr Surg. 2024;46(1):24. doi:10.1186/s40902-024-00436-7
7. Deregibus A, Ferrillo M, Piancino MG, Domini MC, de Sire A, Castroflorio T, et al.. Are occlusal splints effective in reducing myofascial pain in patients with muscle-related temporomandibular disorders? A randomized-controlled trial. Turk J Phys Med Rehabil. 2021;67(1):32–40. doi:10.5606/tftrd.2021.6615
8. Rabel K, Lüchtenborg J, Linke M, et al.. 3D printed versus milled stabilization splints for the management of bruxism and temporomandibular disorders: study protocol for a randomized prospective single-blinded crossover trial. Trials. 2024;25(1):589. doi:10.1186/s13063-024-08437-7
9. Zhang ZW, Zhao JY, Feng Y, et al.. Study on the mechanism of cross-linked hyaluronic acid-dexamethasone hydrogelin post-traumatic osteoarthritis. Zhonghua Yi Xue Za Zhi. 2024;104(9):695–703. doi:10.3760/cma.j.cn112137-20231008-00672
10. Béret M, Barry F, Garcia-Fernandez M-J, et al.. Efficacy of intra-articular injection of botulinum toxin type A (IncobotulinumtoxinA) in temporomandibular joint osteoarthritis: a three-arm controlled trial in rats. Toxins. 2023;15(4):261. doi:10.3390/toxins15040261
11. Yao Y, Wei G, Ding J, et al.. Injectable hydrogel microspheres experimental research for the treatment of osteoarthritis. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2023;37(8):918–928. doi:10.7507/1002-1892.202302105
12. Chęciński M, Chęcińska K, Turosz N, Brzozowska A, Chlubek D, Sikora M. Current clinical research directions on temporomandibular joint intra-articular injections: a mapping review. Journal of Clinical Medicine. 2023;12(14):4655. doi:10.3390/jcm12144655
13. Chęciński M, Chęcińska K, Turosz N, Sikora M, Chlubek D. Intra-articular injections into the inferior versus superior compartment of the temporomandibular joint: a systematic review and meta-analysis. Journal of Clinical Medicine. 2023;12(4):1664. doi:10.3390/jcm12041664
14. Lubecka K, Chęcińska K, Bliźniak F, et al.. Intra-articular local anesthetics in temporomandibular disorders: a systematic review and meta-analysis. Journal of Clinical Medicine. 2023;13(1):106. doi:10.3390/jcm13010106
15. Chęciński M, Chlubek D, Sikora M. (2024) effects of Hyaluronic Acid (HA) and Platelet-Rich Plasma (PRP) on mandibular mobility in temporomandibular joint disorders: a controlled clinical trial. Biomolecules. 1216;14(10). doi:10.3390/biom14101216
16. Zheng L, Gao L, Hu Y, Zhang L, Guan Y. Progress in the study of temporomandibular joint lavage in temporomandibular joint disorder. Journal of Multidisciplinary Healthcare. 2024;Volume 17(17):2175–2184. doi:10.2147/JMDH.S458227
17. Hu M, Yang C, Liu HH, et al.. Experts consensus on standard items of the cohort construction and quality control of temporomandibular joint diseases (2024). Zhonghua Kou Qiang Yi Xue Za Zhi. 2024;59(10):977–987. doi:10.3760/cma.j.cn112144-20240725-00293
18. Lubecka K, Chęcińska K, Bliźniak F, et al.. Update on evidence and directions in temporomandibular joint injection techniques: a rapid review of primary research. Journal of Clinical Medicine. 2024;13(14):4022. doi:10.3390/jcm13144022
19. Goiato MC, da Silva EV, de Medeiros RA, Túrcio KH, Dos Santos DM. Are intra-articular injections of hyaluronic acid effective for the treatment of temporomandibular disorders?A systematic review. International Journal of Oral and Maxillofacial Surgery. 2016;45(12):1531–1537. doi:10.1016/j.ijom.2016.06.004
20. Baron D, Baron H, Baerer C, Bodere C, Conrozier T. (2022).Predictors for patient satisfaction of a single intra-articular injection of crosslinked hyaluronic acid combined with mannitol (HANOX-M-XL) in patients with temporomandibular joint osteoarthritis. results of a prospective open-label pilot study (HAPPYMINI-ARTEMIS trial). BMC Musculoskeletal Disorders. 2022;23(1). doi:10.1186/s12891-022-05352-3
21. Li YQ, Wang GG, Wang YJ, et al.. A meta-analysis of the efficacy and safety of genicular artery embolization for the treatment of pain secondary to knee osteoarthritis. Zhonghua Yi Xue Za Zhi. 2024;104(45):4162–4170. doi:10.3760/cma.j.cn112137-20240825-01960
22. Liu S, Zhang L, Guo L, et al.. Effectiveness of modified temporomandibular joint disc reduction and suture with tragus incision assisted by arthroscopy. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024;38(11):1352–1358. doi:10.7507/1002-1892.202407071
23. Etöz M, Çabuk DS, Kütük N, et al.. Association between articular eminence structure and joint spaces in temporomandibular joints with anterior disc displacement. Niger J Clin Pract. 2024;27(3):408–414. doi:10.4103/njcp.njcp_710_23
24. Heo HA, Yoon HJ. Clinical outcomes of patients with bilateral anterior disc displacement without reduction and erosive change of the temporomandibular joint after performance of unilateral arthrocentesis and stabilisation splint therapy. J Oral Rehabil. 2020;47(3):307–312. doi:10.1111/joor.12897
25. Dhiman NK, Jaiswara C, Hirani MS, et al.. Efficacy of arthrocentesis with intra-articular injection of hyaluronic acid and corticosteroid in the treatment of internal derangement of temporomandibular joint. Natl J Maxillofac Surg. 2023;14(1):93–100. doi:10.4103/njms.njms_8_22
26. Kukreja P, Kukreja BJ, Marrapodi MM, et al.. Efficacy of hyaluronic acid in temporomandibular disorders evaluated with diagnostic criteria for temporomandibular disorders (DC / TMD). J Oral Rehabil. 2025;52(2):254–265. doi:10.1111/joor.13840
27. Al-Dboush R, Esfahani AN, El-Bialy T. Impact of photobiomodulation and low-intensity pulsed ultrasound adjunctive interventions on orthodontic treatment duration during clear aligner therapy. The Angle Orthodontist. 2021;91(5):619–625. doi:10.2319/112420-956.1
28. Gul Amuk N, Kurt G, Guray E. Effects of photobiomodulation and ultrasound applications on orthodontically induced inflammatory root resorption; transcriptional alterations in OPG, RANKL, Cox-2: an experimental study in rats. Photomedicine and Laser Surgery. 2018;36(12):653–659. doi:10.1089/pho.2018.4508
29. Fan X, Hua J, Lu C, et al.. Comparison between disc repositioning by open surgery versus occlusal splint in the treatment of temporomandibular joint anterior disc displacement without reduction: a retrospective cohort trial of short-term results. J Craniomaxillofac Surg. 2023. doi:10.1016/j.jcms.2023.04.009
30. Shamel M, Raafat S, El Karim I, Saber S. Photobiomodulation and low-intensity pulsed ultrasound synergistically enhance dental mesenchymal stem cells viability, migration and differentiation: an invitro study. Odontology. 2024;112(4):1142–1156. doi:10.1007/s10266-024-00920-6
31. Topaloglu Yasan G, Adiloglu S, Tuz HH, et al.. Evaluation of clinical signs and magnetic resonance imaging findings in patients with temporomandibular disorders. J Craniomaxillofac Surg. 2023;51(7–8):441–447. doi:10.1016/j.jcms.2023.08.013
32. Goker F, Russillo A, Taschieri S, et al.. Evaluation of Arthrocentesis with hyaluronic acid injections for management of temporomandibular disorders: a systematic review and case series. J Biol Regul Homeost Agents. 2021;35(2 Suppl. 1):21–35. doi:10.23812/21-2supp1-3
33. Albagieh H, Alomran I, Binakresh A, et al.. Occlusal splints-types and effectiveness in temporomandibular disorder management. Saudi Dent J. 2023;35(1):70–79. doi:10.1016/j.sdentj.2022.12.013
34. Xie Q, Li P, Yang C, et al.. Feasibility of simultaneous TMJ arthroscopy in ADDwoR patients undergoing orthognathic surgery for jaw deformity. J Craniomaxillofac Surg. 2024;52(3):347–354. doi:10.1016/j.jcms.2024.01.019
35. Zhang D, Shen P, Zhang Y, et al.. Influence of local factors on the condylar growth after arthroscopic discopexy in adolescents with temporomandibular joint anterior disc displacement without reduction: a retrospective longitudinal study. Int J Oral Maxillofac Surg. 2023. doi:10.1016/j.ijom.2023.10.005
36. Romero-Tapia P, Sedano-Balbin G, Mayta-Tovalino F, et al.. Therapeutic effect of sodium hyaluronate and corticosteroid injections on pain and temporomandibular joint dysfunction: a quasi-experimental study. J Contemp Dent Pract. 2020;21(10):1084–1090. doi:10.5005/jp-journals-10024-2890
37. Xu J, Ren H, Zhao S, et al.. Comparative effectiveness of hyaluronic acid, platelet-rich plasma, and platelet-rich fibrin in treating temporomandibular disorders: a systematic review and network meta-analysis. Head Face Med. 2023;19(1):39. doi:10.1186/s13005-023-00369-y
38. Miranda DG, Ramos LDP, Lopes NFDS, et al.. Ketoprofen associated with hyaluronic acid hydrogel for temporomandibular disorder treatment: an in vitro study. Gels. 2024;10(12):811. doi:10.3390/gels10120811
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.