")
Back to Journals » Clinical Ophthalmology » Volume 19
Subfoveal Choroidal Thickness After Successful Retinal Detachment Repair with Persistent Subretinal Fluid at the Macula
Authors Mansour AM , Parodi MB, Uwaydat SH, Lima LH , Charbaji S, Casella AM , López-Guajardo L, Belotto S , Wu L, Schwartz SG , Smiddy WE , Hassoun MM, Pérez-Salvador García E, Mansour HA, Elnahry AG , Hamam RN
Received 18 February 2025
Accepted for publication 5 June 2025
Published 11 June 2025 Volume 2025:19 Pages 1847—1854
DOI https://doi.org/10.2147/OPTH.S520076
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ahmad M Mansour,1,2,* Maurizio Battaglia Parodi,3,* Sami H Uwaydat,4 Luiz H Lima,5 Suzanne Charbaji,6 Antonio Marcelo Casella,7 Lorenzo López-Guajardo,8 Silvana Belotto,9 Lihteh Wu,10 Stephen G Schwartz,11 William E Smiddy,11 Mahdi M Hassoun,1 Eduardo Pérez-Salvador García,12 Hana A Mansour,13 Ayman G Elnahry,14,15 Rola N Hamam1
1Department of Ophthalmology, American University of Beirut, Beirut, Lebanon; 2Department of Ophthalmology, Rafic Hariri University Hospital, Beirut, Lebanon; 3Department of Ophthalmology, University Vita-Salute Milan, Milan, Italy; 4Jones Eye Institute, University of Arkansas Medical School, Little Rock, Arkansas, USA; 5Department of Ophthalmology and Visual Sciences, Federal University of Sao Paulo, Sao Paulo, Brazil; 6Department of Epidemiology and Population Health, American University of Beirut, Beirut, Lebanon; 7Department of Ophthalmology, Londrina State University, Londrina, Paraná, Brazil; 8Department of Ophthalmology, Hospital Clinico San Carlos, Madrid, Spain; 9Institut Català de Retina, Barcelona, Spain; 10Asociados de Macula Vitreo y Retina de Costa Rica, San José, Costa Rica; 11Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, Florida, USA; 12Servicio de Oftalmología del Hospital Universitario de Burgos, Burgos, Spain; 13Wills Eye Hospital, Thomas Jefferson Medical Center, Philadelphia, Pennsylvania, USA; 14Department of Ophthalmology, Kasr Al-Ainy Hospitals, Cairo University, Cairo, Egypt; 15BayCare Clinic Eye Specialists, Greenbay, Wisconsin, USA
*These authors contributed equally to this work
Correspondence: Ahmad M Mansour, Department of Ophthalmology, American University of Beirut, Beirut, Lebanon, Tel +9613377633, Email [email protected]
Objective: To explore the relationship between subfoveal choroidal thickness (SFCT) and persistent subretinal fluid (pSRF) at the macula after successful rhegmatogenous retinal detachment (RRD) surgery.
Methods: This is a retrospective multicenter comparative study of Caucasian subjects with successful RRD repair. SFCT was measured in 2 groups: Group 1 with persistent subretinal fluid (pSRF) 1 month after repair, and Group 2 with absence of pSRF. SFCT was measured by a masked observer based on ImageJ. Multiple regression analyses were implemented to control for age, refraction, and gender.
Results: Surgery type was as follows: Group 1 (24 scleral buckle SB, 23 pars plana vitrectomy PPV, 9 SB+PPV, and 5 pneumoretinopexy), and Group 2 (68 PPV). Adjusted mean 1-month SFCT was thicker in Group 1 than in Group 2 by 41.0 μm (p = 0.049). Within Group 1, PPV subgroup tended to have thinner SFCT than the other subgroups by: SB (117.4 μm), SB-PPV (9.3) and pneumoretinopexy (1.2 μm) (all p> 0.05). SFCT at 1-month was not different between pSRF (237.5± 77.2 μm) and no pSRF (213.7± 72.1 μm) in PPV groups (p=0.2).
Conclusion: SFCT post PPV appeared similar in eyes with or without pSRF. In eyes with pSRF, SFCT tended to be thicker following SB compared to PPV.
Plain Lanugage Summary: What was known before:Persistent subretinal fluid one month after successful retinal detachment surgery is associated with a thicker choroid and pachychoroid.
What this study adds:Persisting subretinal fluid one month after successful retinal detachment repair by pars plana vitrectomy is not influenced by the subfoveal choroidal thickness.Scleral buckle leads to increased subfoveal choroidal thickness due to compression of the choroid.
Keywords: choroid, choroidal thickness, optical coherence tomography, pars plana vitrectomy, persistent subretinal fluid, pneumoretinopexy, rhegmatogenous retinal detachment, scleral buckling, subfoveal choroidal thickness
Introduction
Visual recovery is often incomplete after a successful repair of macula-off rhegmatogenous retinal detachment (RRD) from persistent subretinal fluid (pSRF) at the macula.1 Long duration of pSRF in any retinal location appears multifactorial: high viscosity of SRF, long-standing RRD, protracted breakdown of the blood-retinal barrier from surgical trauma to the retinal pigment epithelium. In most cases, pSRF disappears spontaneously within 1 year. However, delayed absorption of SRF at the macula may not occur in some cases resulting in photoreceptor damage with visual loss. Little is known why some cases have pSRF at the fovea, and this may relate to a disturbed RPE function.1 The highly vascularized choroid plays an important role in ocular metabolism with some ocular disorders being associated with choroidal thickening or hyperpermeability. Chantarasorn et al1 demonstrated an intriguing link between pSRF and increased subfoveal choroidal thickness (SFCT) (one biomarker of choroidal thickening), suggesting pachychoroidopathy as a cause of delayed resorption of pSRF. Our goal was to assess SFCT in a cohort of surgical eyes with pSRF and to compare it with a surgical group without pSRF.
Materials and Methods
This was a retrospective multicenter comparative case series consisting of 2 groups: Group 1 included cases of pSRF 1 month after a straightforward, successful primary RRD repair (pars plana vitrectomy PPV, scleral buckle SB, combined PPV-SB, or pneumoretinopexy); Group 2 included consecutive cases from the same contributing centers and same time frame and exam schedule (between 10 am and 2 pm) but with absence of pSRF documented 1 month after successful PPV for RRD repair. Anatomical success was defined as the complete resolution of RRD as observed with binocular indirect ophthalmoscopy. This retrospective cross-sectional study followed the tenets of the Declaration of Helsinki. The study was approved by the Ethics Committee of Rafik Hariri University Hospital. A waiver of patient consent was granted to review medical records per Ethics Committee approval as this research involved very minimal risk to subjects. Patient data confidentiality was maintained by making sure that only authorized persons collected data and that data was accessible and stored through secure storage outlets for research data.
Criteria for inclusion included: persistence of SRF at the 1 month after RRD surgery (mostly PPV and/or SB) confirmed by OCT and successful RRD surgery (PPV) controls without pSRF; high-quality OCT horizontal foveal scan that delineates the whole choroidal contour; Caucasian race; age 16 years and above; OCT machines were restricted to SpectralisR using 815nm (Heidelberg Engineering, Heidelberg, Germany), TritonR using 1,050nm wavelength (Topcon, Tokyo, Japan) and Cirrus 600R using 840nm (Zeiss, Oberkochen, Germany). Criteria for exclusion included: previous retinal surgery; need for subsequent retina surgery; presence of a giant retinal tear; presence of tractional rhegmatogenous retinal detachment or silicone oil use; presence of proliferative vitreoretinopathy, glaucoma or ocular hypertension; history of ocular trauma; preexisting ocular diseases such as high myopia (<-8 diopters) or high hyperopia (>+6 diopters), uveitis, cystoid macular edema, retinal vascular disorder, optic disc pit or coloboma, macular degeneration, retinal pigment epithelial detachment, central serous retinopathy (CSR),2,3 pachychoroid, vitreomacular traction, macular hole (lamellar or full-thickness); and presence of systemic illness (diabetes mellitus, Alzheimer’s disease, cirrhosis, kidney disease, and uncontrolled systemic hypertension).
Choroidal Imaging
SFCT was defined as the height from the Bruch’s membrane to the choroid–scleral interface based on the best horizontal foveal cut. OCT images of the three groups were imported into Image J (Bethesda, Maryland, USA). Measurements of the choroidal thickness were done in a masked fashion with no knowledge of clinical information. Each image was measured two times independently by a single rater (SHU) with the mean being recorded for final analysis. SFCT was further adjusted for the OCT machine used based on established algorithms: (1) SFCT values are quite equivalent between Spectralis and Cirrus;4 (2) SFCT values using Spectralis SD-OCT were 7.31 μm thinner than that obtained with the DRI SS-OCT.5
Statistical Analysis
Continuous data were presented as means±standard deviations. Statistical analyses were performed using one-way analysis of variance (ANOVA). Pearson correlation coefficient was used to measure the covariance between variables. Multiple regression analysis was carried out using SPSS 22 (IBM SPSS, Armonk, New York, USA) to control for age, gender, and spherical equivalence to SFCT.6–8 The measures of association were expressed as odds ratios (OR) with 95% confidence intervals (CI). P values of less than 0.05 were considered statistically significant.
Results
Ocular exam and history for Group 1 are detailed in Table 1. Group 1 included 24 eyes that underwent SB (with SRF drainage), 23 that had PPV, 9 that had combined SB+PPV, and 5 that had pneumoretinopexy (SF6 or C3F8 gas without SRF drainage). In that group, 56 eyes had macula-off RRD, while 5 had macula-on RRD. Group 2 included 68 eyes that underwent successful PPV for RRD with no pSRF. Data on gender, age, race, refractive error (automated refractometer) and OCT machine used for the 2 groups are presented in Table 2. Adjusted mean SFCT was thicker in Group 1 than in Group 2 by 41.0 microns (p=0.049) (Table 3) by multiple regression analysis. Within group 1, PPV subgroup had SFCT thinner than the other subgroups by: SB (117.4 microns) (p=0.52), SB-PPV (9.3 microns) (p=1.0) and pneumoretinopexy (1.2 microns) (p=1.0) after controlling for gender, age, and spherical equivalent (Tables 3 and 4).
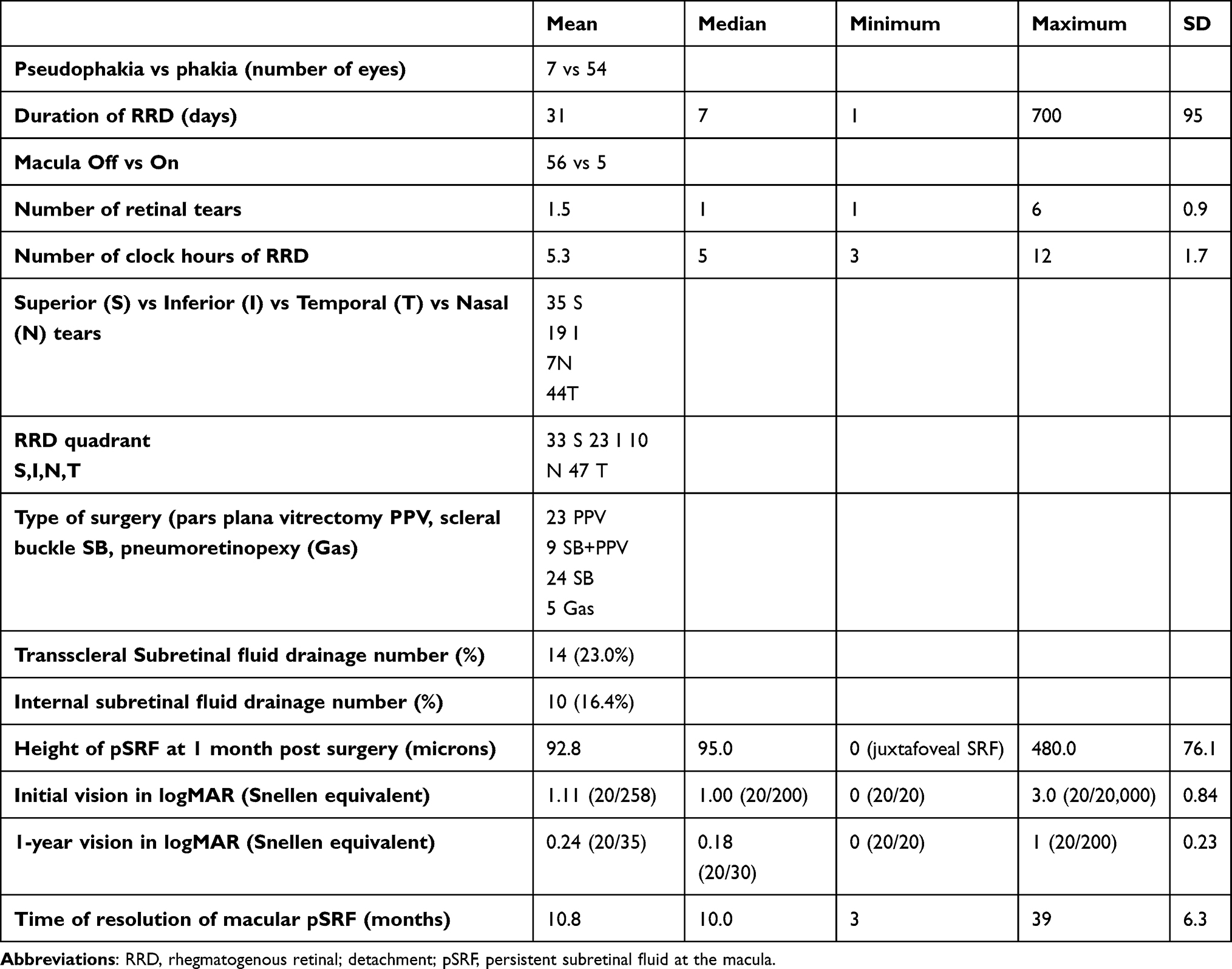 |
Table 1 Clinical Data of Group 1 |
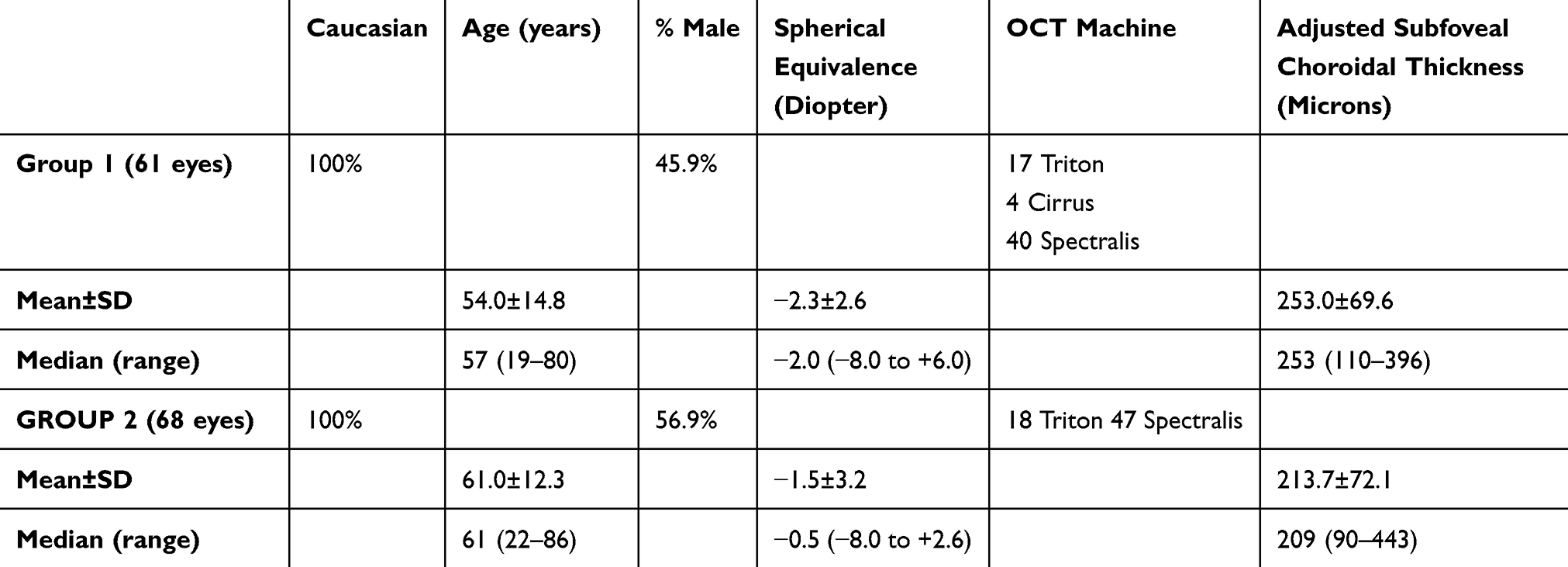 |
Table 2 Demographics of groups 1 and 2. Adjusted subfoveal choroidal thickness SFCT= corrected for differences in optical coherence tomography OCT machines. |
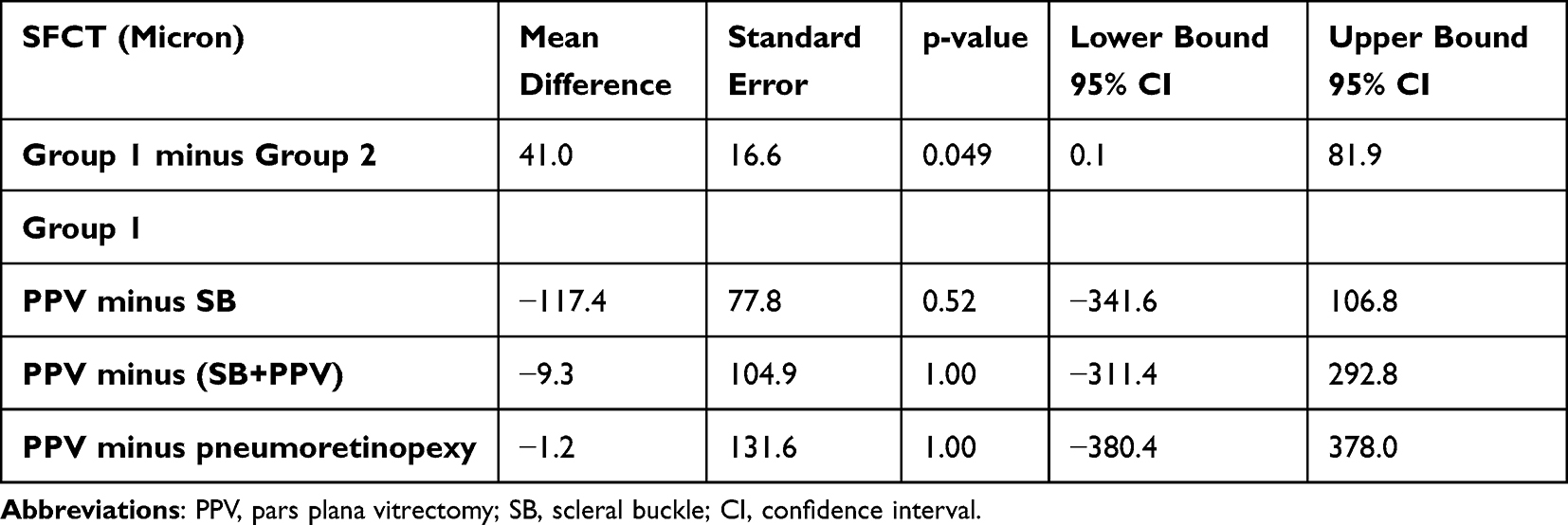 |
Table 3 Comparison of Subfoveal Choroidal Thickness (SFCT) Between the Group 1 and 2 (Top) and Subgroups of Group 1 After Adjusting for Age, Gender and Spherical Equivalence |
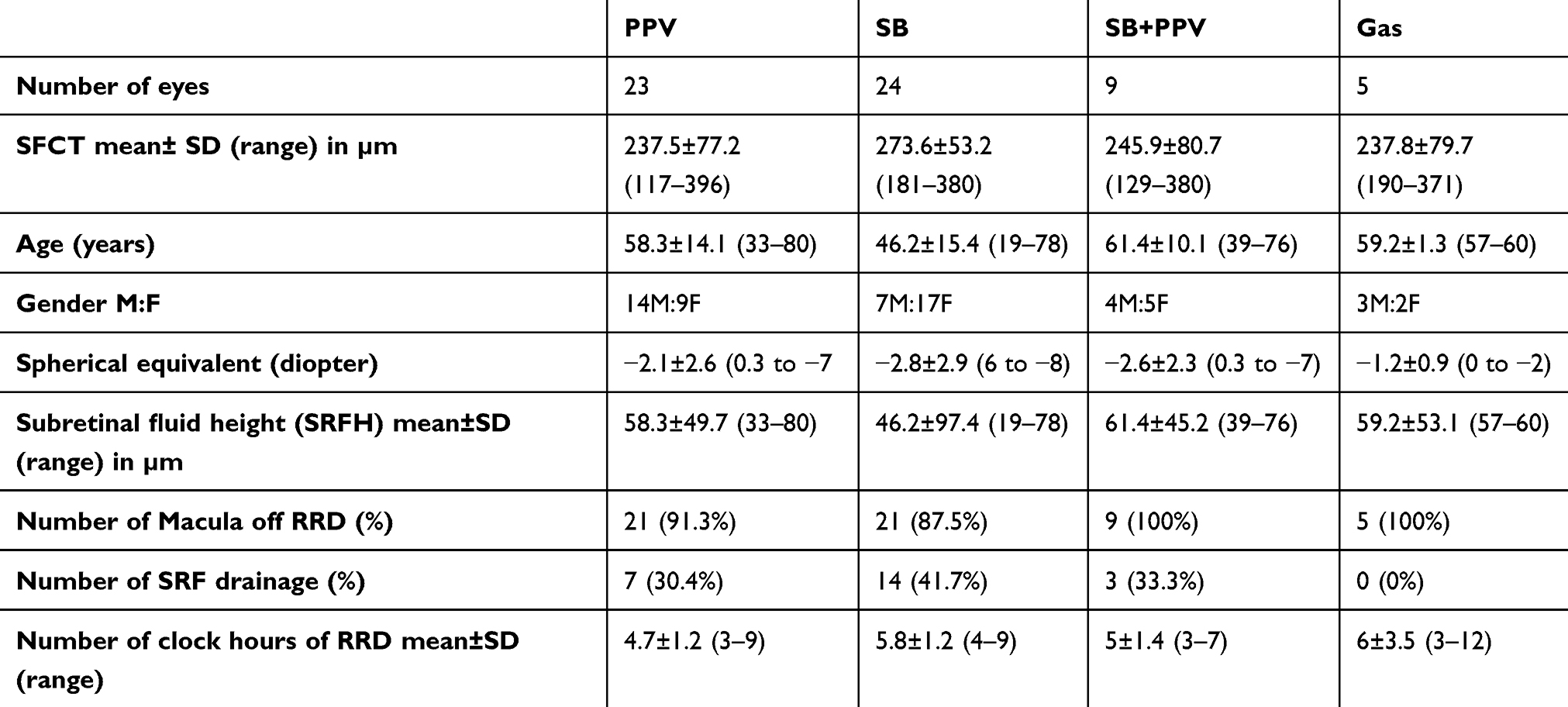 |
Table 4 Demographics of the 4 Subgroups with Persistent Subretinal Fluid at Macula pSRF (SFCT=Subfoveal Choroidal Thickness; RRD=Rhegmatogenous Retinal Detachment; M=Male; F=Female). PPV Subgroup Had SFCT Thinner Than the Other Subgroups By: SB (117.4 Microns) (p=0.52), SB-PPV (9.3 Microns) (p=1.0) and Pneumoretinopexy (1.2 Microns) (p=1.0) After Controlling for Gender, Age, and Spherical Equivalent |
SFCT was larger in eyes with SB and pSRF (273.6±53.2 µm) versus control PPV without pSRF (213.7±72.1 µm) (p=0.04 by univariate analysis; p=0.011 after controlling for age, gender and spherical equivalence). SFCT in eyes with PPV and pSRF was not different from control PPV (p=0.067) before and p=0.098 after controlling for age, gender and spherical equivalence. There was a positive correlation between subretinal fluid height (SRFH) and SFCT with Pearson correlation r=0.26 (p=0.046). Of note, the interclass correlation coefficient (ICC) between the 2 SFCT measures (per eye) was 0.988 (95% CI 0.984 to 0.991).
Discussion
The current paper evaluated some of the possible associations of pSRF after successful repair of RRD.9–31 SFCT was thicker (by 117.4 µm µm) in SB eyes with pSRF vs PPV eyes with pSRF, but the difference was not significant. Also, PPV eyes with pSRF had equivalent choroidal thickness to control PPV eyes. SFCT was significantly larger in eyes with SB and pSRF versus control PPV eyes without pSRF (by 59.9 µm). From these findings, it appears that SB has a direct effect on the choroidal circulation unlike PPV. Odrobina et al19 found a long-lasting thickening of the choroid after an encircling buckle (up to a mean of 22 months), while there was a transient choroidal thickening (lasting a few weeks) after a radial buckle18,20 and no thickening after PPV (Table 5).22,24,25 Encircling SB (considering that the width and size of materials) have long-lasting effect on SFCT vs segmental SB or PPV.19 Besides, cryopexy that accompanies SB leads to inflammation and choroidal thickening but this effect only lasts a few weeks.21 SB is thought to be more associated with residual SRF for several reasons: incomplete drainage of subretinal fluid, use of cryopexy which disrupts the blood retinal barrier, and compression of vortex veins. On the other hand, PPV in most studies does not alter SFCT.
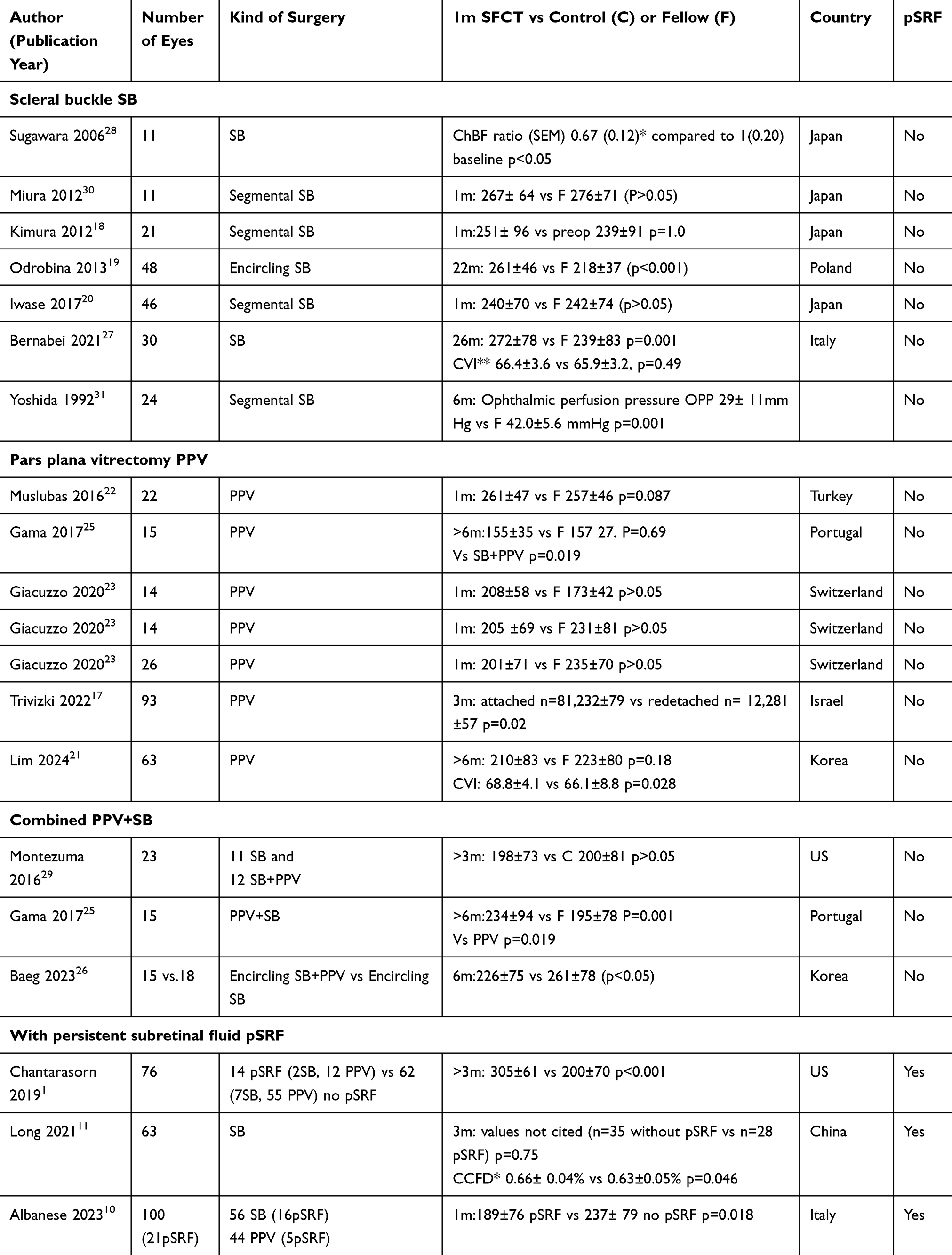 |
Table 5 Literature review1,10,11,17–23,25–31 of One-month (1m) Subfoveal Choroidal Thickness (SFCT) or Other Biomarkers (Choriocapillaris Flow Density (CCFD) or Choroidal Vascularity Index (CVI) or Choroidal Blood Flow Ratio (ChBF Ratio) After Successful RRD Repair Comparing Pars Plana Vitrectomy (PPV), Scleral Buckle (SB) or Combination to Fellow Non-Operated Eye (F) or Control Eye (C)). (CCFD=choriocapillaris Flow Density Within 3×3 mm Macular Fovea; Choroidal Vascularity Index (CVI)=luminal Area Divided by Choroidal Area. ChBF ratio = ChBF of Surgical Eye/ChBF of the Fellow Control Eye; SEM=Standard Error of the Mean) |
At 1-month post-surgery, pSRF can impact at least the time course of visual recovery and suggested causes include incomplete SRF drainage (not using perfluorocarbon), poor retinal pigment epithelium (RPE) pump (membrane pumps, endocytosis, passive diffusion, hydrostatic pressure, and oncotic pressure), long duration of RRD (high protein content of SRF), macula-off RRD, advanced age (age-related hydrophobic barrier formed by accumulated sub-RPE lipoproteins), persistent choroidal inflammation or ocular hypotony and type of surgery.9–16 The choroid plays an important role in ocular metabolism with thickening involved in the pathophysiology of various ocular diseases.17 The inclusion criteria in the current study excluded cases of CSR, pachychoroid, high hyperopia and high myopia in all the 2 groups. Thereafter, there was no difference in SFCT comparing PPV with pSRF vs PPV without pSRF. The literature gives controversial results about choroidal thickness in pSRF due to differences in timing of the OCT after surgery, combining SB with PPV, and inclusion of cases with diabetes mellitus, CSR or high ametropia.1,9–11
SFCT may not be the best biomarker of choroidal health. There is considerable interindividual variation in SFCT in healthy individuals,32 Also there is diurnal variation and can also be influenced by intake of caffeine. Higher SFCT correlated with younger age,6 hyperopia7 and male gender,8 hence we did multiple regression to account for these variables.
The main limitations of this study are its retrospective nature, the inclusion of patients from different centers and use of different OCT protocols, the wide variations in surgical techniques, non-inclusion of fellow eyes measurements, and not accounting for other potential risk factors such as systemic hypertension, dyslipidemia and caffeine intake. Another drawback is the absence of measurements related to the choriocapillaris flow density of the macular fovea or to the choroidal vascular index. The study is limited to the 1-month post-surgery values not studying serial changes view the dynamic nature of SFCT changes following an ongoing choroidal remodeling. Another limitation is the choice to compare eyes operated using a variety of techniques (PPV with or without SB, SB alone, pneumoretinopexy in Group 1) versus eyes operated with only PPV (in Group 2). This decision was made because OCT was readily available in this group. However, because this is a retrospective, multicenter series, there were no predetermined criteria for which patients received which surgical modalities. It is possible that eyes operated with PPV were somehow different from eyes operated with other techniques, which may have introduced bias into the results.
In conclusion, based on current findings, SFCT was not different between eyes with PPV and pSRF vs PPV without pSRF but was higher after SB than PPV. Omitting eyes having either CSR or pachychoroid, increased choroidal thickness was not associated with pSRF in PPV eyes.
Abbreviations
BCVA, best-corrected visual acuity; log MAR, logarithm of the minimum angle of resolution; SRF, subretinal fluid; RRD, rhegmatogenous retinal detachment.
Funding
There is no funding to report.
Disclosure
Professor Lihteh Wu reports personal fees from Roche, Bayer, Apellis, Lumibird Medical, and Ocular Therapeutix, outside the submitted work. The authors declare no other conflicts of interest in this work.
References
1. Chantarasorn Y, Oellers P, Eliott D. Choroidal thickness is associated with delayed subretinal fluid absorption after rhegmatogenous retinal detachment surgery. Ophthalmol Retina. 2019;3(11):947–955. doi:10.1016/j.oret.2019.05.009
2. Oellers P, Eliott D. Overloaded dysfunctional RPE leads to delayed absorption of subretinal fluid after retinal detachment repair. Ophthalmic Surg Lasers Imaging Retina. 2017;48(10):852–855. doi:10.3928/23258160-20170928-12
3. Moreno-López M, Pérez-López M, Casas-Llera P, et al. Persistent subretinal fluid due to central serous chorioretinopathy after retinal detachment surgery. Clin Ophthalmol. 2011;5:1465–1467. doi:10.2147/OPTH.S21331
4. Branchini L, Regatieri CV, Flores-Moreno I, et al. Reproducibility of choroidal thickness measurements across three spectral domain optical coherence tomography systems. Ophthalmology. 2012;119(1):119–123. doi:10.1016/j.ophtha.2011.07.002
5. Matsuo Y, Sakamoto T, Yamashita T, et al. Comparisons of choroidal thickness of normal eyes obtained by two different spectral-domain OCT instruments and one swept-source OCT instrument. Invest Ophthalmol Vis Sci. 2013;54(12):7630–7636. doi:10.1167/iovs.13-13135
6. Spaide R, Koizumi H, Pozzoni M, Pozonni M. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol. 2008;1464(4):496–500. doi:10.1016/j.ajo.2008.05.032
7. Bhayana A, Kumar V, Tayade A, et al. Choroidal thickness in normal Indian eyes using swept-source optical coherence tomography. Ind J Ophthalmol. 2019;67(2):252–255. doi:10.4103/ijo.IJO_668_18
8. Wang W, He M, Zhong X. Sex-dependent choroidal thickness differences in healthy adults: a study based on original and synthesized data. Curr Eye Res. 2018;43(6):796–803. doi:10.1080/02713683.2018.1428995
9. Kim JM, Lee EJ, Cho GE, et al. Delayed absorption of subretinal fluid after retinal reattachment surgery and associated choroidal features. Korean J Ophthalmol. 2017;31(5):402–411. doi:10.3341/kjo.2016.0033
10. Albanese GM, Visioli G, Iannetti L, et al. Does choroidal thickness predict persistent subretinal fluid after rhegmatogenous retinal detachment repair? A retrospective study with fellow eye comparison. Acta Ophthalmologica. 2023;101(4):413–421. doi:10.1111/aos.15298
11. Long K, Meng Y, Chen J, Luo J. Multifactor analysis of delayed absorption of subretinal fluid after scleral buckling surgery. BMC Ophthalmol. 2021;21(21):86. doi:10.1186/s12886-021-01853-2
12. Veckeneer M, Derycke L, Lindstedt EW, et al. Persistent subretinal fluid after surgery for rhegmatogenous retinal detachment: hypothesis and review. Graefes Arch Clin Exp Ophthalmol. 2012;250(6):795–802. doi:10.1007/s00417-011-1870-y
13. Hagimura N, Iida T, Suto K, Kishi S. Persistent foveal retinal detachment after successful rhegmatogenous retinal detachment surgery. Am J Ophthalmol. 2002;133(4):516–520. doi:10.1016/S0002-9394(01)01427-1
14. Otsuka Y, Oishi A, Suda K, et al. Multiple subretinal fluid blebs after pars plana vitrectomy for rhegmatogenous retinal detachment repair. Graefes Arch Clin Exp Ophthalmol. 2019;257(5):921–929. doi:10.1007/s00417-018-04231-9
15. Mimouni M, Jaouni T, Ben-Yair M, et al. Persistent loculated subretinal fluid after rhegmatogenous retinal detachment surgery. Retina. 2020;40(6):1153–1159. doi:10.1097/IAE.0000000000002565
16. Fu Y, Chen S, Gu ZH, et al. Natural history of persistent subretinal fluid following the successful repair of rhegmatogenous retinal detachment. Int J Ophthalmol. 2020;13(13):1621–1628. doi:10.18240/ijo.2020.10.17
17. Trivizki O, Eremenko R, Au A, et al. Association of choroidal thickness with rhegmatogenous retinal detachment repair. Retina. 2022;42(7):1254–1261. doi:10.1097/IAE.0000000000003455
18. Kimura M, Nishimura A, Yokogawa H, et al. Subfoveal choroidal thickness change following segmental scleral buckling for rhegmatogenous retinal detachment. Am J Ophthalmol. 2012;154(154):893–900. doi:10.1016/j.ajo.2012.05.010
19. Odrobina D, Laudańska-Olszewska I, Gozdek P, et al. Influence of scleral buckling surgery with encircling band on subfoveal choroidal thickness in long-term observations. Biomed Res Int. 2013;2013:586894. doi:10.1155/2013/586894
20. Iwase T, Kobayashi M, Yamamoto K, et al. Change in choroidal blood flow and choroidal morphology due to segmental scleral buckling in eyes with rhegmatogenous retinal detachment. Sci Rep. 2017;7(1):5997. doi:10.1038/s41598-017-05126-1
21. Lim G, Kim K, Jo K, et al. Choroidal vascularity and visual outcomes in macula-off rhegmatogenous retinal detachment. Retina. 2024;44(2):261–268. doi:10.1097/IAE.0000000000003944
22. Muslubas S, Karacorlu M, Hocaoglu M, et al. Subfoveal choroidal thickness change after pars plana vitrectomy in recent onset rhegmatogenous retinal detachment. Retina. 2016;36(12):2371–2376. doi:10.1097/IAE.0000000000001096
23. Giacuzzo C, Bergin C, Potic J, et al. Evolution and patterns of choroidal thickness changes in rhegmatogenous retinal detachment. Retina. 2020;40(1):47–55. doi:10.1097/IAE.0000000000002345
24. Akkoyun I, Yılmaz G. Choroidal thickness after sclera buckling surgery versus pars plana vitrectomy in macula-off rhegmatogenous retinal detachment [in German]. Aderhautdicke nach buckelchirurgie versus pars-plana-vitrektomie bei makula-off-rhegmatogener ablatio retinae. Klin Monbl Augenheilkd. 2014;231(10):1029–1033. doi:10.1055/s-0034-1368375
25. Gama I, Proença H, Gonçalves A, et al. Macular choroidal thickness after vitreoretinal surgery: long-term effect of pars plana vitrectomy with and without encircling scleral buckling surgery. Archivos de la Sociedad Española de Oftalmología. 2017;92(12):577–584. doi:10.1016/j.oftal.2017.03.011
26. Baeg JY, Han JW. Long-term comparison of choroidal thickness between scleral encircling and combined with trans-pars plana vitrectomy in retinal detachment. J Korean Ophthalmol Soc. 2023;64(6):473–481. doi:10.3341/jkos.2023.64.6.473
27. Bernabei F, Pellegrini M, Taroni L, et al. Choroidal vascular changes after encircling scleral buckling for rhegmatogenous retinal detachment. Eye (Lond). 2021;35(9):2619–2623. doi:10.1038/s41433-020-01307-x
28. Sugawara R, Nagaoka T, Kitaya N, et al. Choroidal blood flow in the foveal region in eyes with rhegmatogenous retinal detachment and scleral buckling procedures. Br J Ophthalmol. 2006;90(11):1363–1365. doi:10.1136/bjo.2006.097485
29. Montezuma SR, Tang PH, Miller CJ, et al. The effect of scleral buckling surgery on choroidal thickness measured by enhanced depth optical coherence tomography: a cross-sectional study. Ophthalmol Ther. 2016;5(2):215–222. doi:10.1007/s40123-016-0060-8
30. Miura M, Arimoto G, Tsukahara R, et al. Choroidal thickness after scleral buckling. Ophthalmology. 2012;119(7):1497–1498. doi:10.1016/j.ophtha.2012.02.038
31. Yoshida A, Hirokawa H, Ishiko S, et al. Ocular circulatory changes following scleral buckling procedures. Br J Ophthalmol. 1992;76(9):529–531. doi:10.1136/bjo.76.9.529
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Scleral Buckling: A Look at the Past, Present and Future in View of Recent Findings on the Importance of Photoreceptor Re-Alignment Following Retinal Re-Attachment
Cruz-Pimentel M, Huang CY, Wu L
Clinical Ophthalmology 2022, 16:1971-1984
Published Date: 16 June 2022
Peripapillary and Subfoveal Choroidal Thickness in Retinal Vein Occlusions
Moleiro AF, Godinho G, Madeira C, Faria Pereira A, Brandão E, Falcão-Reis F, Beato JN, Penas S
Clinical Ophthalmology 2022, 16:3775-3783
Published Date: 16 November 2022
Spotlight on Lattice Degeneration Imaging Techniques

Maltsev DS, Kulikov AN, Shaimova VA, Burnasheva MA, Vasiliev AS
Clinical Ophthalmology 2023, 17:2383-2395
Published Date: 16 August 2023
A Comparison of Adjustable Positioning and Free Positioning After Pars Plana Vitrectomy for Rhegmatogenous Retinal Detachment: A Prospective Randomized Controlled Study
Liang Q, Sun D, Xue S, Li X, Liu X, Du Q, Zhang Z, Ma X, Li J
Clinical Ophthalmology 2023, 17:3389-3396
Published Date: 6 November 2023
Outcomes in Recurrent Rhegmatogenous Retinal Detachment Repair: Does Scleral Buckling at Primary or Secondary Surgery Impact Results?
Hébert M, Garneau J, Doukkali S, Bourgault S, Caissie M, Tourville É, Dirani A
Clinical Ophthalmology 2025, 19:949-956
Published Date: 17 March 2025