")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Subject Modeling-Based Analysis of the Evolution and Intervention Strategies of Major Emerging Infectious Disease Events
Authors Guo H, Zhao T , Zou Y , Zhang B, Cheng Y
Received 10 December 2024
Accepted for publication 2 April 2025
Published 11 April 2025 Volume 2025:18 Pages 1257—1278
DOI https://doi.org/10.2147/RMHP.S507704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kyriakos Souliotis
Haixiang Guo,1,2 Tiantian Zhao,1 Yuzhe Zou,1 Beijia Zhang,1 Yuyan Cheng1
1School of Economics and Management, China University of Geosciences, Wuhan, People’s Republic of China; 2The Laboratory of Natural Disaster Risk Prevention and Emergency Management, China University of Geosciences, Wuhan, People’s Republic of China
Correspondence: Haixiang Guo, Email [email protected]
Objective: Due to the popularity of the Internet and the extensive use of new media, after the occurrence of infectious diseases, the spread of social media information greatly affects the group’s opinion and cognition and even the health behaviors they take, thus affecting the spread of infectious diseases. Therefore, this paper studies the event evolution from multiple dimensions.
Methods: To address this gap, we developed a three-layer model framework of major infectious disease event evolution based on subject modeling. This framework integrates three key factors—health transmission, perspective interaction, and risk perception—to analyze group perspective evolution, behavioral change, and virus transmission processes. The model’s effectiveness was evaluated through simulation and sensitivity analysis. In addition, we conducted an empirical analysis by constructing a social media health transmission effect index system to identify the critical factors affecting health transmission.
Results: Simulation results reveal that among the three factors, health transmission has the most significant impact on the evolution of group perspectives during infectious disease events. Moreover, the dynamics of public viewpoint evolution influence individual decisions regarding the adoption of non-pharmacological interventions, which are shown to effectively reduce both the transmission rate of the virus and the peak number of infections.
Conclusion: The findings of this study enhance our understanding of the complex mechanisms and evolutionary pathways in infectious disease events. By integrating multiple dimensions of event evolution, the proposed model offers valuable insights for the design of effective countermeasures and strategies in emergency management and response to infectious disease outbreaks.
Keywords: infectious disease events, viewpoint evolution, behavior change, subject modeling, simulation
Introduction
Since the beginning of the 21st century, major outbreaks of infectious diseases have frequently occurred, significantly impacting economic and social development, as well as normal public life. Infectious diseases caused by viruses are one of the major infectious diseases that have a profound impact on human society.1 Among these, COVID-19 stands out as a global public health crisis that has had the most profound repercussions in the 21st century.2 Following the emergence of the novel coronavirus, the virus swiftly proliferated worldwide, leading to a sustained high number of infections. Concurrently, navigating through the plethora of information during the pandemic became arduous, with a proliferation of misinformation and false narratives giving rise to an “infodemic”.3 This phenomenon severely impeded efforts to combat the outbreak and control the spread of infectious diseases, posing a grave threat to social cohesion and stability.On November 11, 2022, the Comprehensive Group of the State Council’s Joint Prevention and Control Mechanism issued the “Report on Further Enhancing the Management of the COVID-19 Pandemic”. This report underscored the importance of monitoring public sentiment and underscored the necessity of promptly addressing public concerns to effectively optimize prevention and control measures. Guiding public opinion is paramount in responding to infectious disease crises.4 Consequently, enhancing the comprehensive response mechanism and bolstering the capacity to mitigate risks during major infectious disease outbreaks has emerged as a critical priority.
The progression of an infectious disease event encompasses not only the transmission of the virus but also the intricate process of information dissemination. Central to this process is the pivotal role of health communication in shaping collective perspectives during infectious disease outbreaks. Health communication involves translating complex medical research findings into easily digestible health information for the general public. Through inducing changes in attitudes and behaviors, the primary goal is to mitigate disease prevalence and mortality rates, ultimately enhancing the overall quality of life and health standards within a community or nation. An essential component of health communication lies in the dissemination of health knowledge via various media channels to influence people’s emotions, attitudes, knowledge, and behaviors towards diseases. In recent years, there has been a notable surge in the implementation of health communication strategies during infectious disease events. This has led to the widespread dissemination of crucial health information, including disease specifics, prevention and control guidelines, which, in turn, significantly impact public perceptions regarding the transmission risks of infectious diseases, attitudes towards such events, and decision-making processes concerning behavioral responses.5 With health transmission, the public’s risk perception of an event evolves, and when it reaches a certain level, it leads to a change in behavioural decision-making, with the public spontaneously adopting preventive and control behaviours to combat viral infections.6 The acceptance of prevention and control behaviours in a population can directly influence the spread of the virus.7 The large-scale implementation of preventive and control behaviours can effectively reduce the infection rate and the negative impact of the spread of infectious diseases. In the case of the New Crown outbreak, for example, through the dissemination of knowledge about the transmissibility of the disease and recommended precautions by the media and opinion leaders, the population may become aware of the risk of being infected and change their behaviour by adopting self-protective measures, which will further influence the spread of the disease.6 Thus, there is a significant chain of influence between group opinion evolution, behavioural change and the corresponding viral spread process, which together constitute the infectious disease event evolutionary system.
The existing body of research on the mechanisms influencing the evolution of infectious disease events has predominantly focused on the impact of cognitive shifts in group perspectives or the dynamics of information dissemination on disease spread.4 However, the mediating role of group behavior change has received comparatively less attention. Moreover, in studies that do consider the influence of group behavior change, the depiction of the evolution of group perspectives on infectious disease events tends to be oversimplified, often overlooking the significant contribution of factors such as health communication to viewpoint evolution. To address these gaps, this paper aims to construct a comprehensive three-layer model framework for understanding the evolution of major infectious disease events. Drawing on subject-based modeling, this framework aims to elucidate the multifaceted evolution process of infectious disease events in a nuanced manner. By intervening in the evolutionary system of infectious disease events through enhancing the efficacy of health communication, the paper seeks to guide public perspectives, promote health-conscious behaviors, curb virus transmission, and offer theoretical underpinnings for a holistic response to and emergency management of infectious disease events.
Research Status
Research on the Evolutionary Mechanisms of Major Infectious Disease Events
Sudden major infectious disease events fall under the category of public health emergencies. Numerous scholars have adopted a macro-level approach, simulating the intricate evolution process of infectious disease events by integrating various factors such as environmental conditions, psychological elements, and political economy considerations.8
Methodologically, the states of nodes within multilayer networks are typically discrete and finite. Nonetheless, in real-world scenarios, individuals’ perceptions of events exhibit dynamic and continuous characteristics, varying in degrees.9,10 And subject-based modelling can better portray and simulate the complex system interaction evolution process in real situations. The subject-based modelling approach can also be used to analyse the interactive evolution process of views between different subjects in a group.11,12 In terms of model construction, the “group cognitive change-virus spread” multilayer network and the “viewpoint-behaviour-virus” evolutionary model are mainly used to simulate the spreading mechanism of infectious diseases. The former model mainly focuses on the influence of group cognitive change on virus spread,13,14 while the latter incorporates the influence of group behavioural change in the evolution of infectious disease events, but does not take into account both cognitive and behavioural changes in groups, and less consideration is given to the influence of internal and external factors, such as group risk perception and governmental intervention, on the evolution of group viewpoints on infectious disease events.
Research on the Evolution of Group Viewpoints on Major Infectious Disease Events
In a major infectious disease event, the group’s perspective on the event is a dynamic process influenced by a combination of internal and external factors.14,15 Major external factors, such as the effects of health transmission as well as environmental noise, can have an impact on group views.16 In addition, according to the health belief model, the public’s risk perception of the severity of an infectious disease event can also influence their views and perceptions of the event.14 In the process of group viewpoint evolution, internal factors refer to the process of viewpoint interaction within the group. Individuals in a group are often influenced by other individuals, and the influence of different individuals varies considerably.
In terms of research methodology, the study of viewpoint dynamics is often combined with complex networks to study the interplay of different opinions among individuals in a social group, the evolution of public opinion, and the process of reaching consensus.17 Viewpoint dynamics is divided into two models, continuous and discrete, depending on whether the opinion values are continuous or discrete.10 Continuous viewpoint dynamics models are able to portray the dynamic evolution of opinions, and one of the more classic models is the bounded trust model, which assumes that individuals only interact with individuals whose opinions are similar to their own.
Bounded trust models include the Deffuant-Weisbuch (DW) model18 and the Hegselmann-Krause (HK) model.19 The main difference between the two models is that the DW model uses two pairs of individuals to interact with each other, whereas in the HK model, each individual moves to the average view of all the individuals in its confidence level, the individual’s view in the DW model is updated asynchronously at each moment, whereas the individual’s view in the HK model is updated synchronously. In the 21st century, with the rapid development of information technology and the massive and rapid dissemination of information, when individuals interact with each other, they often do not have one-to-one interactions, but are directly confronted with massive and complex information sources, therefore, the HK model is more in line with the real situation as well. The above studies mainly innovate the structure of the viewpoint dynamics model and the application scenarios, but less for the specific scenario of the infectious disease event, considering the multiple influencing factors in the evolution of the event to analyse the group viewpoint evolution process in depth.
Research on the Group Behavior Change in Major Infectious Disease Events
After the occurrence of a major infectious disease event, the public’s views on the event continue to evolve interactively, influencing public behaviour, especially the decision-making process of preventive and control behaviours, which in this paper mainly refers to the evolution of the individual’s viewpoints that will ultimately affect the individual’s behavioural decision-making to accept Non-pharmaceutical Intervention (NPI). Common NPIs such as wearing masks, home isolation, and reducing going out can reduce the likelihood of infection by reducing physical contact or increasing protection. As the public becomes more aware of infectious disease events and the prevention and control of viruses, health behaviours in the population change and more individuals adopt preventive and control behaviours.20–22
The main purpose of current research on infectious disease infections is to provide recommendations to policy makers to improve emergency response and emergency management. However, the impact of infectious disease infections, as well as policy effectiveness, is limited by the behaviours adopted by groups during infectious disease events.23 This highlights the importance of behavioural change of groups in the evolution of infectious disease events. Scholars have studied such issues extensively, with the threshold model being the most classic model for studying behavioural change. Most of the existing studies preset threshold conditions, and behavioural change occurs only when an individual reaches a certain condition.24–26 All of the above studies show that individuals will start to take preventive and control behaviours only when the information related to infectious disease events and the degree of risk perception they obtain meet certain conditions and reach a certain threshold. However, risk perception is not the only factor that influences behavioral adoption in infectious disease events; external factors as well as the individual’s perceived viewpoint of an infectious disease event also influence the decision-making process of individual behavioral adoption.25
Research on the Spread of Viruses in Major Infectious Disease Events
How to contain the spread of viruses in the early stages of a major infectious disease event in a timely manner and as soon as possible, and to effectively control the rate of its spread has been a hot research topic.27 Infectious disease transmission is a complex process of viral diffusion in a population, and modelling this process can help to improve the understanding and knowledge of the transmission mechanism and the regularities of infectious disease spread, which is the basis for predicting the epidemic trend and making decisions on prevention and control.28,29 Currently, infectious disease transmission models are divided into two categories: network dynamics models and deterministic models. Network dynamics models, on the other hand, are some of the recently emerged models that apply cutting-edge technologies and research,30 which include metacellular automata, artificial neural networks, scale-free network models and so on. The deterministic models, on the other hand, are mainly based on differential equations, including several models such as Susceptible-Infectious (SI), Susceptible-Infectious-Susceptible (SIS), Susceptible-Infectious-Recovered (SIR), and susceptible-exposed-infective-recovered (SEIR), which are the most widely used and influential infectious disease models.31,32 In order to make the model simulation process closer to reality, some scholars have improved the SEIR model, such as considering the state of the infected person in the process of infectious disease transmission, constructing an infectious disease model containing multiple compartments33 or susceptible-exposed-infective-vigilant (SEIV) model, which takes into account that the behaviour of an individual may change after infection.34
When responding to public health emergencies, the preventive and control measures taken can be divided into medical measures and non-pharmacological interventions (NPIs). Medical measures mainly refer to vaccination and other medical-related measures, while NPIs have a wider scope of application in comparison. Some studies have pointed out that NPI will continue to be an indispensable and important initiative in the fight against new crown outbreaks until medical measures are widely used.35 Due to the large impact of NPI on the infection rate of virus spread as well as the speed of transmission.36 Many scholars have introduced NPIs into the simulation of infectious disease transmission in an attempt to understand, analyse and quantify the effects of different NPIs and combinations of NPIs on the spread of infectious diseases, and compared them with the original model, and have found that the proposed model is able to better simulate the process of infectious disease transmission in real-life situations.37–39
In summary, existing studies have mainly adopted the multilayer network approach to study the influence of group perception on the virus spreading process, but have not explained the role of behavioural change as an intermediate process. Some studies have also improved on this foundation by constructing a framework based on subject-based modelling to combine the evolution of group views, behavioural change and the spread of viruses, and to study the influence of the relationship between “viewpoints-behaviour-viruses”, but they often do not provide an in-depth portrayal of the process of the evolution of group views. Therefore, in this paper, the important factor of behavioural change is included in the evolution process of major infectious disease events, and a subject-based model of group viewpoint evolution-behavioural change-virus diffusion in infectious disease events is constructed. At the same time, multiple influencing factors, such as health transmission, are considered to help decision makers understand the process of group view evolution in infectious disease events more deeply, so as to provide scientific prevention and control strategies for infectious disease event response.
Methods and Material
Modelling the Evolution of Group Viewpoints on Major Infectious Disease Events
Analysis of factors influencing the evolution of group viewpoints on major infectious disease events
After an emergency, the public will spontaneously express their personal views and opinions, which will then develop and spread through the Internet, media, and other dissemination channels.12 According to viewpoint dynamics, different viewpoints interact with each other and coalesce in the process of spreading and spreading in the group according to individual decision-making styles, leading to the evolution of group viewpoints. Especially in the context of an infectious disease event, the public’s viewpoint perception of the event is also influenced by external factors, including the interaction of viewpoints with other individuals and the perceived risk of disease spread, in addition to health transmission factors.16 The relationships influencing the evolution of their group viewpoints are shown in Figure 1.
 |
Figure 1 Factors influencing the evolution of group views. |
Health transmission impacts
This paper quantitatively analyses the role that health transmission initiatives play in the evolution of group viewpoints on infectious disease events by incorporating health transmission factors into the evolution of group perspectives on infectious disease events. The extent to which individual  is affected by health transmission at moment
is affected by health transmission at moment  is denoted by
is denoted by  , which refers to the degree of influence of health transmission received by individuals through different media channels. In order to reduce the complexity of the model, it is assumed that all individuals in the
, which refers to the degree of influence of health transmission received by individuals through different media channels. In order to reduce the complexity of the model, it is assumed that all individuals in the  moment are affected by health transmission in the same way, ie
moment are affected by health transmission in the same way, ie  .
.
Viewpoint interaction impacts
The confidence level in an opinion dynamics model reflects the degree of trust that individuals in a group have in other individuals, and can greatly influence the process and final outcome of the group’s opinion evolution. Bounded confidence models are mainly composed of the DW model and the HK model, which are commonly used to simulate the opinion evolution among different subjects. There are subtle differences between these two models: the subjects in the DW model are randomly paired, whereas the subjects in the HK model are influenced by all neighbours who satisfy the opinion thresholds, which is more suitable for large-scale group interactions. At this stage, the process of information dissemination and opinion evolution in groups mainly uses social media as a platform, so the HK opinion dynamics model is used to represent the influence of inter-individual interactions on opinion evolution:

 indicates the extent to which individual i’s own viewpoint changes after interacting with another person’s viewpoint at moment
indicates the extent to which individual i’s own viewpoint changes after interacting with another person’s viewpoint at moment  . Where
. Where  denotes the subject
denotes the subject  ’s confidence interval within which an individual will interact with the
’s confidence interval within which an individual will interact with the  engage in viewpoint interactions.
engage in viewpoint interactions.  denotes the viewpoint value of individual
denotes the viewpoint value of individual  at moment
at moment  . The expression for the weight
. The expression for the weight  for
for  to interact with other individuals is as follows:
to interact with other individuals is as follows:

The setting of the confidence interval indicates that individual  interacts with individual
interacts with individual  only when the difference between the opinion values of individual
only when the difference between the opinion values of individual  and individual
and individual  is less than a fixed threshold
is less than a fixed threshold  , ie
, ie  , and
, and  denotes the threshold of trust between subject
denotes the threshold of trust between subject  and individual
and individual  .
.  denotes the number of individuals in the confidence interval. In the base model individuals
denotes the number of individuals in the confidence interval. In the base model individuals  views are only influenced by the views of other individuals whose difference with their view value is less than a fixed threshold, and regardless of the influence of other individuals in the network, the
views are only influenced by the views of other individuals whose difference with their view value is less than a fixed threshold, and regardless of the influence of other individuals in the network, the  the influence of other individuals’ views is the same.
the influence of other individuals’ views is the same.
Risk perception impacts
Risk perception refers to the subjective judgements people make about the characteristics and severity of a particular risk. This paper refers to existing research34 that view the degree of risk perception as a function of the spread of the infectious disease in question to describe the effect of the level of risk perception on the evolution of the view. Infectious disease transmission is represented by the proportion of people infected
as a function of the spread of the infectious disease in question to describe the effect of the level of risk perception on the evolution of the view. Infectious disease transmission is represented by the proportion of people infected  in the SEIR model. This value represents the number of infected persons as a proportion of the total number of infected persons at the moment
in the SEIR model. This value represents the number of infected persons as a proportion of the total number of infected persons at the moment  , with a value closer to 1 indicating a more severe current infection situation and vice versa, a less severe infectious disease spread. The formula is expressed as follows:
, with a value closer to 1 indicating a more severe current infection situation and vice versa, a less severe infectious disease spread. The formula is expressed as follows:

Where  denotes the function of the current infection situation on the value of the subject’s
denotes the function of the current infection situation on the value of the subject’s  viewpoint, taking the interval [0.9, 0.95].34
viewpoint, taking the interval [0.9, 0.95].34
Improved Viewpoint Dynamics Modelling Under the Influence of Multiple Factors
Based on the above analysis of influencing factors, this paper adds the influence of health transmission, viewpoint interaction and risk perception factors to construct a group viewpoint evolution model for infectious disease events. The framework of the influence of group viewpoint evolution formula is as follows:

 denote the weights of health transmission, viewpoint interaction, and risk perception influences respectively.
denote the weights of health transmission, viewpoint interaction, and risk perception influences respectively.  denote respectively the extent to which the views held by individual
denote respectively the extent to which the views held by individual  about an infectious disease event at moment
about an infectious disease event at moment  are influenced by health transmission, viewpoint interactions, and risk perception factors during group viewpoint evolution.
are influenced by health transmission, viewpoint interactions, and risk perception factors during group viewpoint evolution.
Further, taking into account the effects of the above factors, a model of viewpoint evolution in an infectious disease event scenario is constructed with the following formula for individual viewpoint updating:

where  denotes individual
denotes individual  ’s perception of own view of the infectious disease event at moment
’s perception of own view of the infectious disease event at moment  ,
,  denotes the degree to which individual
denotes the degree to which individual  is firm in the view it holds, and
is firm in the view it holds, and  denotes the degree to which individual
denotes the degree to which individual  trusts the other influences. It is generally believed that the firmer the attitude of the viewpoint held by an individual, the more it tends to stick to its own viewpoint and accepts less influence from other factors. On the contrary, the more inclined they are to accept the influence of other factors and change their views.40
trusts the other influences. It is generally believed that the firmer the attitude of the viewpoint held by an individual, the more it tends to stick to its own viewpoint and accepts less influence from other factors. On the contrary, the more inclined they are to accept the influence of other factors and change their views.40
Models of Group Behaviour Change in Major Infectious Disease Events
According to cognitive-behavioural theory,41 of the three, cognition, emotion and behaviour, cognition plays the most important role, cognition generates emotion, emotion leads to behaviour, and behaviour continues to influence cognition, thus forming a triangular cycle, as shown in Figure 2. This is also true in the context of infectious disease events, where the accuracy of people’s cognitive perceptions of their views on the spread of the virus’s postures and the dangers of the virus greatly influences the behaviour they receive.
 |
Figure 2 Cognitive Behavioural Theory. |
Threshold Model Construction for Behaviour Change Under the Influence of Viewpoint Evolution
In the process of infectious disease event evolution, the group’s acceptance of prevention and control behaviours is mainly influenced by their viewpoints, and then their behavioural decision-making process will keep changing with the evolution of viewpoints. Therefore, in the behavioural change model of infectious disease events, this paper proposes to use the threshold model as the base model, and the probability ( ) of accepting NPI is expressed as:
) of accepting NPI is expressed as:

Of these,  is the viewpoint threshold at which subject
is the viewpoint threshold at which subject  makes a behavioral change in response to an infectious disease. Below a certain threshold, subjects do not see the need to adopt NPI; however, when the value of the subject’s viewpoint exceeds the threshold, they reach a certain level of severity and awareness of the infectious disease, which in turn triggers the acceptance of NPI, thus reducing the probability of being infected. We will count the acceptance rate of NPI in the group, denoted as
makes a behavioral change in response to an infectious disease. Below a certain threshold, subjects do not see the need to adopt NPI; however, when the value of the subject’s viewpoint exceeds the threshold, they reach a certain level of severity and awareness of the infectious disease, which in turn triggers the acceptance of NPI, thus reducing the probability of being infected. We will count the acceptance rate of NPI in the group, denoted as  , and finally introduced
, and finally introduced  into the infection rate formula of the SEIR model.
into the infection rate formula of the SEIR model.
Model of Viral Spread in Major Infectious Disease Events Under the Influence of NPI
The group’s viewpoint perception of infectious disease events can largely influence the group’s NPI acceptance, and the group’s adoption of preventive and control measures can subconsciously influence the transmission posture of infectious diseases. Therefore, this paper improves the infection rate formula in the traditional SEIR model by adding the willingness of the group to accept NPI and the NPI acceptance rate as factors affecting the infection rate in the model.The effect of NPI preventive and control measures on the groups of contacts and infected persons is most significant. Therefore, the infection rate formula in the SEIR model was adjusted as follows:

Among them,  and
and  denote respectively the rate of conversion from susceptible to exposed and from susceptible to infected without receiving any NPI.
denote respectively the rate of conversion from susceptible to exposed and from susceptible to infected without receiving any NPI.  denotes the rate of NPI acceptance in the group, ie, the ratio of the number of people receiving NPI to the total number of people in the group. Based on the simulation results of the group viewpoint evolution and behavioural change model, the group NPI acceptance rate was statistically obtained as
denotes the rate of NPI acceptance in the group, ie, the ratio of the number of people receiving NPI to the total number of people in the group. Based on the simulation results of the group viewpoint evolution and behavioural change model, the group NPI acceptance rate was statistically obtained as  . Then
. Then  indicates the effectiveness of the group accepting NPI.
indicates the effectiveness of the group accepting NPI.  and
and  denote respectively the rate of conversion from susceptible to exposed and infected, after taking into account the population NPI acceptance rate. In summary, the improved SEIR model considering group NPI acceptance is shown in Eq:
denote respectively the rate of conversion from susceptible to exposed and infected, after taking into account the population NPI acceptance rate. In summary, the improved SEIR model considering group NPI acceptance is shown in Eq:

Modelling the Evolution of Group Viewpoint Evolution-Behavioural Change-Virus Spread Evolution on Infectious Disease Events
In this paper, we construct a major infectious disease event evolution system based on the subject, and convert the influence relationship between the above three into a formulaic expression, and the connection between the three layers of the model is shown in Equation 2.9:

Firstly, under the influence of multiple factors such as health transmission, viewpoint interaction and risk perception, individuals’ viewpoints on infectious disease events are constantly evolving, and the final viewpoint evolution value  will affect the individual’s behavioural decision to accept the NPI, the individual viewpoint value will be inputted into the behavioural change threshold model, the NPI acceptance rate in the group will be counted
will affect the individual’s behavioural decision to accept the NPI, the individual viewpoint value will be inputted into the behavioural change threshold model, the NPI acceptance rate in the group will be counted  , and finally introduced
, and finally introduced  into the infection rate formula of the SEIR model to get the infection rate that considers the influence of viewpoint evolution and behaviour change process. The connection between the three layers of the model is shown schematically in Figure 3.
into the infection rate formula of the SEIR model to get the infection rate that considers the influence of viewpoint evolution and behaviour change process. The connection between the three layers of the model is shown schematically in Figure 3.





Data Collection
Following the simulation experiments, this paper will further validate and discuss the effect of health communication in the spread and evolution of major infectious diseases based on social media data.
On 7 December 2022, the prevention and control of the new crown epidemic will be fully liberalised, the health code and trip code service will be taken offline, and the nucleic acid certificate and trip code will no longer be checked for traffic and travel. Therefore, 7 December 2022 was chosen as the time point, and the top 50 users in the healthcare category of the Weibo “V Influence List” from 7 December 2022 to 7 January 2023 were selected as the data source for their relevant information and microblog content. By excluding users who have not posted for more than a month and those who have nothing to do with healthcare, the basic information of 41 users and their 7,811 tweets were obtained.
Simulation Verification Results
Group Viewpoint Evolution Simulation
Suppose that there exists a scale-free network which has a population size of  , the degree distribution of nodes in the network approximately obeys a power law distribution, while new nodes joining with an edge number of 2 will preferentially connect with nodes of higher degree in the network. Each subject in the model interacts with other subjects with viewpoints. The viewpoint of the subject
, the degree distribution of nodes in the network approximately obeys a power law distribution, while new nodes joining with an edge number of 2 will preferentially connect with nodes of higher degree in the network. Each subject in the model interacts with other subjects with viewpoints. The viewpoint of the subject  at the moment
at the moment  is
is  . Initially each subject is given a confidence level with the same value between
. Initially each subject is given a confidence level with the same value between  , and viewpoint interaction occurs when the difference between the subject’s viewpoints and other subjects’ viewpoints is less than this threshold.
, and viewpoint interaction occurs when the difference between the subject’s viewpoints and other subjects’ viewpoints is less than this threshold.
In this paper, it is assumed that all subjects have the same confidence level, which takes the value of 0.5. The Networkx library for Python is used to construct scale-free networks to obtain random network graphs obeying the Barabási-Albert preference connection. The version of Networkx used in this study is 2.5 and Python version 3.8 was used for running the simulations. The initial viewpoint values are randomly generated by the software. The initial viewpoint evolution network graph is shown in Figure 4.
 |
Figure 4 Initial network diagram. |
The degree distribution of the initial network is shown in Figure 5.
 |
Figure 5 Initial network degree distribution: The (a) shows the distribution of degrees and the (b) shows the histogram of degrees. |
The initial settings of the basic parameters are shown in Table 1.
 |
Table 1 Parameter Settings for the Group View Evolution Model |
Based on the model simulation parameter settings above, the program was run to obtain the simulation results of group viewpoint evolution and plotted as shown in Figure 6. As can be seen from Figure 6a–c, the convergence value of viewpoint evolution in the group is the highest when focusing on the role of health transmission in the model, between [0.5, 0.6]; the convergence value of group viewpoint evolution is the second highest when focusing on the effect of viewpoint interactions; and the convergence value of the group’s viewpoint evolution is the lowest when focusing on the effect of risk perception, located between [0.3, 0.4]. The picture below Figure 6 then shows the final network diagram of the group’s viewpoint evolution. According to the colour bar on the right, when the nodes in the network converge to a warmer colour, it indicates that the final viewpoint value converges to 1, and vice versa, it indicates that the final viewpoint evolution value converges to 0. According to the model results, the health transmission factor plays the largest role in the group viewpoint evolution process of infectious disease events, and can significantly influence the group viewpoint evolution process and the final convergence value.







Group Behaviour Change Simulation
For the value of the viewpoint in the group at each moment, applying the behavioural threshold model proposed in the previous section, set the threshold of behavioural change at this time set to 0.5, reflecting the degree of tolerance of the individual for the risk. The NPI acceptance rate, that is, the number of individuals adopting the NPI as a proportion of the total number of the group, and similarly for the combination of weights for different influencing factors to draw a curve diagram of the acceptance rate of the control and prevention behaviours, and the results shown in Figure 7.








In Figure 7, three different scenarios are set up, and the blue, orange and green curves represent the group NPI acceptance rate when the role of health transmission, views interaction and risk perception factors are highlighted in the group viewpoint evolution process, respectively. It can be seen that in the initial stage, the group NPI acceptance rate of the three scenarios is about 0.5. And as the number of iterations increases, the group NPI acceptance rate of the first scenario, ie, increasing the health dissemination, increases gradually until it converges to 1. In the second scenario, ie, highlighting the viewpoint interactions, the group NPI acceptance rate increases and then decreases, and then converges to 0. The third scenario, ie, highlighting the influence of the risk perception, the group NPI acceptance rate decreases until the group NPI acceptance rate decreases. NPI acceptance rate decreases until it approaches 0.
In summary, it can be seen that in the process of the evolution of the group’s views on the infectious disease event, if the external health transmission is small, mainly relying on the spontaneous interaction of the group’s viewpoints or the role of risk perception, the final evolution of the group’s viewpoints and the acceptance rate of the NPI tend to be low. This suggests that the group’s knowledge and attitude towards the event and related prevention and control behaviours did not reach the expected results, and that there may be problems such as insufficient in-depth knowledge of the viewpoints and insufficient support for prevention and control. The results of the model also reflect the importance of health transmission in the evolution of group views on infectious disease events. Effective and widely used health transmission measures can greatly improve the group’s view of infectious disease events, promote the dissemination of information about infectious diseases and the adoption of related prevention and control behaviours, and ultimately increase the proportion of the group that adopts prevention and control behaviours to resist the spread of the virus.
In the behavioural change threshold model, whether an individual accepts NPI or not depends on whether the value of his/her viewpoint reaches a particular threshold. Therefore, further simulation of the effect of behavioural thresholds on NPI adoption rate was conducted and the results were obtained as shown in Figure 8.


In Figure 8, the behavioural change threshold is set to vary between 0.2 and 0.8, from which it can be seen that when the behavioural change threshold exceeds 0.6, the NPI acceptance rate of the group decreases; while if the value is less than 0.6, the NPI acceptance rate of the group rises continuously, and finally approaches 1. This indicates that lowering the threshold of the group’s behavioural change can help to increase the acceptance rate of the NPI in the group. When the behavioural change threshold is 0.6, the initial group NPI acceptance rate keeps increasing and decreasing after reaching the peak value. The reason may be that the viewpoint value of the group in the initial situation is randomly distributed and varies greatly, and in the process of evolution most of the individuals are influenced by multiple factors viewpoint value continues to rise and exceeds the behavioural change threshold, so the NPI acceptance rate of the group in the early stage continues to rise. However, due to the high threshold of behavioural change, there are always some individuals with lower viewpoint values who maintain their original state and lower the group’s viewpoint value during viewpoint interactions with other individuals, resulting in a decrease in the NPI acceptance rate in the later stage.
Virus Spreading Simulation
The influence of NPI is not considered in the traditional SEIR model, and this paper proposes an improved SEIR model by taking into account the influence of the willingness to accept NPI in the group and the effect of NPI implementation. The basic parameter settings are shown in Table 2.
 |
Table 2 Viral Diffusion Layer Parameter Settings |
The results of the SEIR model as well as the model proposed in this paper are first compared, where the NPI validity is assumed to be 0.9 and the NPI acceptance rate of the group is 0.5. The results obtained are shown in Figure 9.
 |
Figure 9 Comparison of virus spreading simulations. The (a) is the simulation result of virus spread under the traditional SEIR model, and the (b) is the simulation result of virus spread under the improved SEIR model in this paper. The blue, yellow, red and green lines are susceptible, exposed, infected and recovered persons, respectively. |
In Figure 9a, it can be seen that the number of contacts as well as infected persons climbed rapidly shortly after the outbreak of the virus, reaching a peak very quickly. In Figure 9b, which takes into account the acceptance of NPI by the population, the number of contacts as well as infected persons peaked almost twice as long as in the case of no NPI acceptance. The population of infected and contacted persons declines significantly, with the most pronounced fall in the population of contacted persons. Through these results, we can get that considering the NPI acceptance rate during virus transmission can significantly prolong the time for the population to reach the peak of infection as well as reduce the peak of population infection, thus providing more time for the emergency response to the infectious disease event, and effectively reducing the hazardousness and negative impacts of the infectious disease event. This suggests that by improving the traditional SEIR model and considering the acceptance rate of NPI in the model, our infectious disease group opinion-behaviour change-virus transmission model is more responsive to the reality of the law than the infectious disease model that simply uses the traditional SEIR model.
Impact of Group Viewpoint Evolution and Behavioural Change on Virus Diffusion
Figure 10 shows the results of the evolution of the group view under the weights of different influencing factors and the corresponding simulation results of the virus spread. The comparison graph of results reveals distinct patterns across scenarios in the virus spreading process. In the first scenario, the peak number of infected individuals is observed to be the lowest, accompanied by the longest time taken to reach this peak infection level. Conversely, the second and third scenarios exhibit higher rates of infection spread and peak values compared to the initial scenario. These findings underscore the potential impact of offering comprehensive guidance to groups during viewpoint evolution and enhancing the efficacy of health communication. By doing so, it is possible to delay the peak of viral infection, reduce the overall infection rate within the group, and thereby create a window for more effective emergency management and response strategies during the onset of an infectious disease event.







In the model simulations above, the NPI acceptance rate in the improved SEIR model was set to 0.5 across the board in order to highlight the influence of other factors, and the model simulations below are based on this aspect of the effect of the NPI acceptance rate on virus infection.
The vertical coordinate in Figure 11 is the number of infected people simulated by the improved SEIR model, which shows that when the NPI acceptance rate of the group increases, the higher the support of the group for the related prevention and control behaviours, and that the number of infected people in the group decreases and the rate of infection decreases, all other things being equal. In the above results, the influence of group NPI acceptance rate on virus transmission is more obvious, indicating that group NPI acceptance can effectively influence the virus infection situation of the group, which also shows the importance of strengthening the guidance of the viewpoints to enhance the group’s knowledge of the virus and the related prevention and control behaviours.
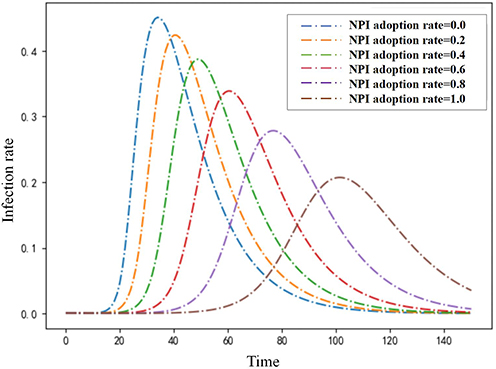 |
Figure 11 Effect of NPI acceptance rate on infection rates. |
Model Sensitivity Analysis
This paper focuses on the exploration of uncertainty in viewpoint evolution models using Sobol sensitivity analysis.42 The results are shown in Figure 12. From Figure 12b, it can be seen that when the value of individual viewpoints is less than 0.5, the health transmission weights  has a higher sensitivity to the model results, and as the individual’s cognitive viewpoint on infectious diseases is deepening, the
has a higher sensitivity to the model results, and as the individual’s cognitive viewpoint on infectious diseases is deepening, the  value gradually decreases. It shows that the health transmission factor is most effective when the individual’s cognition of infectious disease events is less adequate, which greatly influences the individual’s final viewpoint evolution value. Figure 12c shows that as the value of an individual’s view of an infectious disease event increases, the sensitivity of view interaction factor
value gradually decreases. It shows that the health transmission factor is most effective when the individual’s cognition of infectious disease events is less adequate, which greatly influences the individual’s final viewpoint evolution value. Figure 12c shows that as the value of an individual’s view of an infectious disease event increases, the sensitivity of view interaction factor  to the viewpoint evolution results also increases. It shows that as the individual’s perception of the infectious disease event continues to deepen, the viewpoint interaction factor plays an increasingly significant role in it. Figure 12d shows that the sensitivity of the risk perception factor tends to be close to 0, indicating that its influence on the outcome of viewpoint evolution is small. Figure 12e shows that when the value of an individual’s view of an infectious disease event is small, the sensitivity of
to the viewpoint evolution results also increases. It shows that as the individual’s perception of the infectious disease event continues to deepen, the viewpoint interaction factor plays an increasingly significant role in it. Figure 12d shows that the sensitivity of the risk perception factor tends to be close to 0, indicating that its influence on the outcome of viewpoint evolution is small. Figure 12e shows that when the value of an individual’s view of an infectious disease event is small, the sensitivity of  is higher, indicating that the role of individual recalcitrance on viewpoint evolution is more significant at this time. And when the value of the individual’s viewpoint is increasing, the sensitivity of
is higher, indicating that the role of individual recalcitrance on viewpoint evolution is more significant at this time. And when the value of the individual’s viewpoint is increasing, the sensitivity of  sensitivity decreases, the effect of individual recalcitrance on the outcome of viewpoint evolution decreases.
sensitivity decreases, the effect of individual recalcitrance on the outcome of viewpoint evolution decreases.
 |
Figure 12 Model sensitivity analysis. The (a) illustrates the results of the sensitivity analysis of the viewpoint evolution model. The (b–e) respectively represent the sensitivity curves of the health transmission factor, the viewpoint interaction factor, the risk perception factor, and the degree of firmness of an individual to the viewpoint held to the results of the viewpoint evolution model. |
In summary, we firstly obtain that health transmission factors play an important role in the evolution of group views, which can enhance the group’s awareness of infectious disease events and influence their willingness to accept preventive and control measures, so as to intervene in the process of virus spread in the group, and effectively reduce the rate of infection in the group and the negative impacts brought about by the spread of the virus. Secondly, the acceptance of NPI by the group can also effectively influence the viral infection of the group, which also indicates the importance of strengthening the viewpoint guidance in infectious disease events, and improving the group’s viewpoint awareness of the virus and related prevention and control behaviours. Therefore, improving the effectiveness of health transmission can significantly influence group views, behaviours and infectious disease transmission dynamics during infectious disease events.
Empirical Analysis and Discussion
The model constructed in the previous section only includes the abstract quantification of health transmission factors into the model formula, which is still insufficient for how to improve the actual effect of health transmission. Therefore, this section takes health transmission in social media platforms as the theme to explore the important factors affecting the effectiveness of health transmission in social media.
Selection of Indicators
According to the definition of health transmission, an important part of health transmission is to disseminate health knowledge through the media, so as to change people’s feelings, attitudes, knowledge and behaviours towards diseases. Therefore, research on the effectiveness of health transmission focuses on the measurement of changes in the cognitive, affective, attitudinal, and behavioural phases of the messages received by the audience.43,44 At the same time, the existing research on health transmission effects of social media platforms mostly selects specific health official accounts, and constructs an index system to measure the health transmission effects of social media accounts from the dimensions of breadth and depth of communication, and discovers the key factors affecting the effects of health transmission.44 The key factors affecting the effect of health transmission are found.
Therefore, this paper constructs a health transmission effect index system based on microblog accounts to measure the breadth and depth of health transmission in social media, in order to reflect the cognitive, emotional attitudes and behavioural changes of the audience when receiving health information, to more comprehensively measure the effect of health transmission and to discover its key influencing factors. Because the Micro-blog Communication Index (BCI) is an indicator that reflects the communication ability and effect of microblog accounts through the activity and communication degree of microblogs, the BCI contains comprehensive and scientific data to compare the effectiveness of health transmission with that of microblogs. This index contains comprehensive scientific data and is more objective, so it is added to the communication effect measurement index system as a reference.
Referring to the existing studies, the second and third level indicators of this paper’s microblog account-based health transmission effectiveness indicator system and the related descriptions are shown in Table 3.
 |
Table 3 Description of the Indicator System of Health Transmission Effect of Microblog Account |
Analysis of Influencing Factors of Health Transmission Based on Microblogging Platforms
Statistical methods are used to construct a multiple regression model to analyse the causal relationship between the breadth and depth of communication and its influencing factors and the magnitude of their influence in the effect of health transmission, and to find out the key factors affecting the effect of communication, so as to provide theoretical support for the enhancement of the effect of health transmission.
Factors Influencing the Breadth of Health Transmission
Firstly, we make descriptive statistics on the number of fans, authentication status, and topic status of the collected data, as shown in Figure 13.
 |
Figure 13 Statistical Distribution of Breadth Evaluation Indicators. The (a) shows the distribution of account followers, the (b) shows the account authentication, and the (c) shows the statistics of microblogging with topics. |
Then, a health propagation span model is constructed, with the number of fans, authentication state and topic state as independent variables and the number of retweets as dependent variables. The results are shown in Table 4.
 |
Table 4 Regression Model of the Number of Retweets Against Each Evaluation Indicator |
The analysis of Table 4 and Figure 13 shows that the three indicators of number of followers, authentication status and whether or not to bring topics are all significant at the 0.1% significance level, in which the number of followers and whether or not to bring topics are positive, and the higher the number of followers is, the higher the dissemination of the blog post is. If the microblogs come with topics, the retweets of the blog posts are higher. This is mainly due to the fact that microblogging is a social media platform based on the relationship between following and being followed, so the number of followers of a microblog account is an important factor affecting the breadth of health communication, which can greatly influence the number of times the information is viewed and the probability of secondary dissemination. Secondly, the authentication status of the account can also affect the retweeting behaviour of the public to a certain extent. The authentication status is related to the professionalism and authority of the blogger, and professional authentication information can bring a higher degree of trust to the blogger, which can help the secondary dissemination of information. In addition, the number of retweets of blog posts is also affected by the topic of microblogging. Blog posts with popular topics, especially those with microblogging popular search list topics, are more likely to be retweeted, and the popular topics are equivalent to providing another communication channel for the blog posts in addition to focusing on the visible, and can therefore play an important role in promoting the dissemination of information.
Factors Influencing the Depth of Health Communication
The source credibility, topic selection and expression form in the collected data were counted, and the results were shown in Figure 14.
 |
Figure 14 Statistical Distribution of Depth Evaluation Indicators. (a), (b) and (c) are the statistical distributions of the number of microblog posts and the average number of likes under different subject types, different expression forms and different credibility of information sources, respectively. |
The results of the multiple linear regression model with source credibility, topic selection and expression form as independent variables and the number of microblog likes as dependent variables are as Table 5.
 |
Table 5 Regression Model of the Number of Likes and Each Evaluation Indicator |
Combined with Table 5 and Figure 14, it can be seen that both topic choice and form of expression are significant at the 0.1% level of significance and have a positive effect. It indicates that topic selection and expression form of blog posts can significantly affect the depth of blog communication. Health communication-related blog posts in Weibo are generally divided into three aspects: medical science, treatment methods, and disease prevention, and the number of science blog posts is the highest, and the degree of recognition by the audience is also the highest. At the same time, the BCI index of microblog accounts was counted, and among 41 microblog accounts, there were two accounts with a BCI index of more than 1,300, and the main content was medical and health knowledge-related popular science. This shows that the audience has a higher degree of recognition and interest in popular knowledge information, and the actual dissemination effect of this type of information is better. Compared with easy-to-understand medical knowledge popularisation microblogs, microblogs on treatment methods are more esoteric and obscure, requiring a certain degree of professional knowledge and general medical knowledge, and are therefore accepted by the general public to a lesser extent.
Secondly, the mode of expression significantly impacts the reception of health communication messages. Analysis of microblog data revealed that posts predominantly featured images and videos, with image-based microblogs enjoying higher recognition compared to videos. This preference can be attributed to the contemporary online habit of consuming fragmented information, where images require less time and effort than videos. Consequently, image-based microblogs prove most effective in facilitating deep engagement in health communication. Lastly, the credibility of the information source, whether labeled or not, does not notably influence overall message acceptance. Likewise, there is no significant difference in the number of likes between microblogs with and without source labels.
Conclusions
In this study, we developed a framework to model the evolutionary dynamics of major infectious disease events using subject modeling. Our approach simulated the evolution of group viewpoints, behavioral changes, and the spread of viruses within this framework. By analyzing the interrelationships among these factors, we aimed to quantify their respective impacts on the progression and outcomes of infectious disease events.
Based on our simulations, we found that health communication factors play a crucial role in shaping public perception, influencing behavioral responses, and effectively mitigating virus transmission. As a result, we extended our analysis to focus on Weibo as a case study of social media platforms. We proposed a Social Media Health Communication Effect Index System, designed to identify key factors influencing health communication effectiveness on Weibo accounts. This system aims to provide evidence-based recommendations for enhancing the efficacy of health communication efforts during infectious disease outbreaks.
Key conclusions and policy recommendations derived from our findings include:
- Through the two simulation experiments of group viewpoint evolution and group behaviour change, it is found that among the three influencing factors of health communication, viewpoint interaction and risk perception, health communication can significantly influence the process of group viewpoint evolution in infectious disease events, and substantially increase the acceptance rate of group NPI. Therefore, it is necessary for the relevant departments to promote the effective implementation of health communication, which on the one hand can help to construct correct public health concepts and make the public more aware of the hazards of infectious diseases, their transmission routes and prevention methods; On the other hand, it can enhance the public’s willingness to accept NPI, which means that when implementing prevention and control measures such as quarantine, wearing masks, hand cleaning, etc., it will be able to gain the support and cooperation of a wider range of people. This will reduce the spread of the virus infection rate and alleviate the impact of infectious diseases on people’s lives and socio-economics.
- In this paper, the improved SEIR model considering the NPI acceptance rate is closer to the real situation, and the time for the number of infected people to reach the peak is prolonged and the peak number of infected people decreases after considering the NPI acceptance of the group in the traditional SEIR model. This suggests that after an infectious disease event, large-scale implementation of NPI measures to improve the acceptance rate of group NPI can effectively slow down the spread of the virus, buying valuable time for vaccine development, drug treatment, and deployment of medical resources, thus reducing the impact of the epidemic on the healthcare system. In addition, it is also possible to increase public awareness and acceptance of NPI measures by strengthening the dissemination of health information and popularisation of science, thereby promoting the implementation of NPI measures and further slowing down the rate of virus transmission. Therefore, the government should formulate and implement targeted NPI policy regimes, such as social distancing, travel restrictions, wearing of masks, etc., in accordance with the spreading dynamics and epidemiological characteristics of the virus, in order to prevent the further spread of the virus.
- In the empirical analysis of social media health communication, we found that when posting microblogs, we can get higher viewership than ordinary microblogs by attaching microblogging topics, especially the current hot topics or topics on the popular search list. In terms of the content of the tweets, it is easier for the audience to recognise and accept health-related information by choosing popular science topics that are easy to understand. In the form of microblogs, it is necessary to avoid the pure text form of microblogs, and can be accompanied by pictures and videos, which can help to attract the audience’s attention and enhance their interest in the content of microblogs, so as to achieve a better dissemination effect. Therefore, health information disseminators should consider three key factors to further enhance the effectiveness of social media health communication: First, they should pay close attention to social hotspots and popular trends, and cleverly combine health information with popular topics to increase the exposure and dissemination range of the information; Second, the scientific and accurate content of the messages should be ensured, and easy-to-understand language and expressions should be used to ensure that the health messages can convey professional knowledge as well as be accepted by the general public; Thirdly, making full use of multimedia means such as pictures and videos, and designing clear and concise visual elements so as to quickly convey the core message.
Although the model in this paper can provide theoretical value and practical significance, in practice, there may still be costs such as model maintenance and updating, data collection and processing, computational resources and expert hiring, etc., and the cost limitations will further restrict the feasibility and generalisability of the model in future major infectious disease events. Therefore, future research will optimise and improve the overall structure of the model and the resources required, taking into account the cost issue while maintaining the model performance.
Additionally, its application across different populations or regions may face challenges due to varying socio-cultural backgrounds, public health policies, and information dissemination environments. These factors could affect model assumptions and parameters, influencing the accuracy and generalizability of the results. Future research should explore the model’s adaptability to diverse contexts and account for local or cultural variations.
Furthermore, the model assumes uniform confidence levels among individuals, but in reality, these levels vary due to differences in cognitive processes, environmental influences, and trust in others’ viewpoints. Future work should incorporate this variability into group opinion dynamics, enhancing the model’s accuracy in reflecting real-world complexities.
Ethics Approval and Consent to Participate
This study follows the principles of the Declaration of Helsinki. The study was an independent investigation and was approved by the School of Economics and Management of China University of Geosciences (Wuhan). Each participant was informed of the purpose, benefits, and confidentiality of the study, and consent was obtained from each survey participant prior to inclusion in the study (eligible children under 18 years of age were required to obtain their guardian’s consent). The data collected were stored securely to prevent unauthorised access.
Funding
This study was funded by the National Natural Science Foundation of China under the Grant 72074198, and The National Social Science Fund of China under the Grant No.23AZD072, and the Foundation for Innovative Research Groups of Hubei Province of China (Grant No.2024AFA015), and the Fundamental Research Funds for the Central Universities, China University of Geosciences (Wuhan) under the Grant CUG2642022006.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
References
1. Li X, Jiang H, Liang X. Early stage risk identification and governance of major emerging infectious diseases: a double-case study based on the Chinese context. Risk Manag Healthc Policy. 2023;Volume 16:635–653. doi:10.2147/RMHP.S400546
2. Du E, Chen E, Liu J, et al. How do social media and individual behaviors affect epidemic transmission and control? Sci Total Environ. 2021;761:144114. doi:10.1016/j.scitotenv.2020.144114
3. Mheidly N, Fares J. Leveraging media and health communication strategies to overcome the covid-19 infodemic. J Public Health Policy. 2020;41(4):410–420. doi:10.1057/s41271-020-00247-w
4. Ye Y, Zhang Q, Ruan Z, et al. Effect of heterogeneous risk perception on information diffusion, behavior change, and disease transmission. Phys Rev E. 2020;102(4):042314. doi:10.1103/PhysRevE.102.042314
5. Serena L, Marzolla M, D’Angelo G, et al. A review of multilevel modeling and simulation for human mobility and behavior. Simul Modell Pract Theory. 2023;127:102780. doi:10.1016/j.simpat.2023.102780
6. Lorenz J. CONTINUOUS opinion dynamics under bounded confidence: a survey. Int J Mod Phys C. 2007;18(12):1819–1838.
7. Dong Y, Zhan M, Kou G, et al. A survey on the fusion process in opinion dynamics. Information Fusion. 2018;43:57–65.
8. Dong J, Hu J, Zhao Y, et al. Opinion formation analysis for Expressed and Private Opinions (EPOs) models: reasoning private opinions from behaviors in group decision-making systems. Expert Syst Appl. 2024;236:121292.
9. Shen Y, Ma X, Xu Z, et al. Opinion evolution and dynamic trust-driven consensus model in large-scale group decision-making under incomplete information. Inf Sci. 2024;657:119925.
10. Granell C, Gómez S, Arenas A. Dynamical interplay between awareness and epidemic spreading in multiplex networks. Phys Rev Lett. 2013;111(12):128701. doi:10.1103/PhysRevLett.111.128701
11. Ep F, Castillo-Chavez C, G CM, et al. Adaptive human behavior in epidemiological models. Proc Natl Acad Sci. 2011;108(15):6306–6311. doi:10.1073/pnas.1011250108
12. K KAP, Yan M, T HY, et al. What shapes people’s willingness to wear a face mask at the beginning of a public health disaster? A qualitative study based on COVID-19 in China. Int J Disaster Risk Reduct. 2021;65:102577. doi:10.1016/j.ijdrr.2021.102577
13. Kim DKD, Kreps GL. An analysis of government communication in the United States during the covid‐19 pandemic: recommendations for effective government health risk communication. World Med Health Policy. 2020;12(4):398–412. doi:10.1002/wmh3.363
14. Rosenstock IM. Health Belief Model[M]//Encyclopedia of Psychology. Vol. 4. Washington, DC, US: American Psychological Association; 2000:78–80.
15. Chen T, Yin X, Yang J, et al. Modeling multi-dimensional public opinion process based on complex network dynamics model in the context of derived topics. Axioms. 2021;10(4):270. doi:10.3390/axioms10040270
16. Deffuant G, Neau D, Amblard F, et al. Mixing beliefs among interacting agents. Adv Complex Syst. 2000;03(01n04):87–98. doi:10.1142/S0219525900000078
17. Hegselmann R. OPINION dynamics and bounded confidence models, analysis, and simulation. 2002.
18. Zelič Ž, Berič M, Kobal Grum D. Examining the role of covid-19 conspiracy beliefs in predicting vaccination intentions, preventive behavior and willingness to share opinions about the coronavirus. Studia Psychologica. 2022;64(1):136–153. doi:10.31577/sp.2022.01.844
19. Bernardes AT, Ribeiro LC. Information, opinion and pandemic. Physica a Stat Mech Appl. 2021;565:125586. doi:10.1016/j.physa.2020.125586
20. Chawla Y, Radziwon A, Scaringella L, et al. Predictors and outcomes of individual knowledge on early-stage pandemic: social media, information credibility, public opinion, and behaviour in a large-scale global study. Inf Process Manag. 2021;58(6):102720. doi:10.1016/j.ipm.2021.102720
21. Verelst F, Willem L, Beutels P. Behavioural change models for infectious disease transmission: a systematic review (2010–2015). J Royal Soc Interface. 2016;13(125):20160820. doi:10.1098/rsif.2016.0820
22. Xiao Y, Xu X, Tang S. Sliding mode control of outbreaks of emerging infectious diseases. Bull Math Biol. 2012;74(10):2403–2422. doi:10.1007/s11538-012-9758-5
23. Shaw LB, Schwartz IB. Enhanced vaccine control of epidemics in adaptive networks. Phys Rev E. 2010;81(4):046120. doi:10.1103/PhysRevE.81.046120
24. Wu Q, Liu H, Small M. Dynamical diversity induced by individual responsive immunization. Physica a Stat Mech Appl. 2013;392(12):2792–2802. doi:10.1016/j.physa.2013.02.014
25. Kendall PC, Hollon SD. Cognitive-behavioral interventions: theory, research, and procedures[C]. 1979.
26. Cao Y, Shan J, Gong Z, et al. Status and challenges of public health emergency management in China related to COVID-19. Front Public Health. 2020;8:250. doi:10.3389/fpubh.2020.00250
27. Grassly NC, Fraser C. Mathematical models of infectious disease transmission. Nat Rev Microbiol. 2008;6(6):477–487. doi:10.1038/nrmicro1845
28. Vynnycky E, White R. An Introduction to Infectious Disease Modelling[M]. OUP oxford; 2010.
29. Heesterbeek H, M AR, Andreasen V, et al. Modeling infectious disease dynamics in the complex landscape of global health. Science. 2015;347(6227):aaa4339. doi:10.1126/science.aaa4339
30. Waku J, Oshinubi K, Demongeot J. Maximal reproduction number estimation and identification of transmission rate from the first inflection point of new infectious cases waves: COVID-19 outbreak example. Math Comput Simul. 2022;198:47–64. doi:10.1016/j.matcom.2022.02.023
31. Hu Z, Wu Y, Su M, et al. Population migration, spread of COVID-19, and epidemic prevention and control: empirical evidence from China. BMC Public Health. 2021;21:1–12. doi:10.1186/s12889-021-10605-2
32. S ZX, Vynnycky E, Charlett A, et al. Transmission dynamics and control measures of COVID-19 outbreak in China: a modelling study. Sci Rep. 2021;11(1):2652. doi:10.1038/s41598-021-81985-z
33. Bhowmick S, Panja S. Influence of opinion dynamics to inhibit epidemic spreading over multiplex network. IEEE Control Syst Lett. 2021;5(4):1327–1332. doi:10.1109/LCSYS.2020.3035873
34. Mp K, L CM, Becker AD, et al. Chopping the tail: how preventing superspreading can help to maintain covid-19 control. Epidemics. 2021;34:100430. doi:10.1016/j.epidem.2020.100430
35. Ayouni I, Maatoug J, Dhouib W, et al. Effective public health measures to mitigate the spread of covid-19: a systematic review. BMC Public Health. 2021;21(1):1015. doi:10.1186/s12889-021-11111-1
36. Prem K, Liu Y, W RT, et al. The effect of control strategies to reduce social mixing on outcomes of the covid-19 epidemic in Wuhan, China: a modelling study. Lancet Public Health. 2020;5(5):e261–e270. doi:10.1016/S2468-2667(20)30073-6
37. Tang B, Wang X, Li Q, et al. Estimation of the transmission risk of the 2019-ncov and its implication for public health interventions. J Clin Med. 2020;9(2):462. doi:10.3390/jcm9020462
38. Lio CF, Cheong HH, Lei CI, et al. Effectiveness of personal protective health behaviour against covid-19. BMC Public Health. 2021;21(1):827. doi:10.1186/s12889-021-10680-5
39. Friedkin NE, Johnsen EC. Social influence and opinions. J. Math Sociol. 1990;15(3–4):193–206. doi:10.1080/0022250X.1990.9990069
40. Sameni R. Mathematical modeling of epidemic diseases; a case study of the COVID-19 Coronavirus. arXiv. 2020.
41. Hou C, Chen J, Zhou Y, et al. The effectiveness of quarantine of Wuhan city against the corona virus disease 2019 (COVID-19): a well-mixed SEIR model analysis. J Med Virol. 2020;92(7):841–848. doi:10.1002/jmv.25827
42. Saltelli A. Making best use of model evaluations to compute sensitivity indices. Comput Phys Commun. 2002;145(2):280–297. doi:10.1016/S0010-4655(02)00280-1
43. Zhou C, Xiu H, Wang Y, et al. Characterizing the dissemination of misinformation on social media in health emergencies: an empirical study based on COVID-19. Inf Process Manag. 2021;58(4):102554. doi:10.1016/j.ipm.2021.102554
44. Shen L, Wang S, Chen W, et al. Understanding the function constitution and influence factors on communication for the WeChat official account of top tertiary hospitals in China: cross-sectional study. J Med Int Res. 2019;21(12):e13025. doi:10.2196/13025
45. Wang G, Wang Y, Liu K, et al. Multidimensional influencing factors of public opinion information dissemination in social media: evidence from Weibo dataset. Int J Modern Phys B. 2019;33(31):1950375. doi:10.1142/S0217979219503752
46. Katz E, Blumler JG, Gurevitch M. USES and gratifications research. The Public Opinion Quarterly. 1973;37(4):509–523. doi:10.1086/268109
47. Houts PS, Doak CC, Doak LG, et al. The role of pictures in improving health communication: a review of research on attention, comprehension, recall, and adherence. Patient Educ Couns. 2006;61(2):173–190. doi:10.1016/j.pec.2005.05.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.