")
Back to Journals » The Application of Clinical Genetics » Volume 18
Survey of Structural Autosomal Abnormalities and Autosomal Variants in Infertile Patients Treated at Some IVF Centers in Vietnam
Authors Trieu ST , Pham MD, Le H, Vo HV, Nguyen PV , Tran TV , Nguyen NN , Trinh ST
Received 19 December 2024
Accepted for publication 3 April 2025
Published 11 April 2025 Volume 2025:18 Pages 29—40
DOI https://doi.org/10.2147/TACG.S510933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Martin Maurer
Sang Tien Trieu,1 Minh Duc Pham,2 Hoang Le,3 Hien Van Vo,4 Phong Van Nguyen,1 Tuan Van Tran,2 Nhat Ngoc Nguyen,2 Son The Trinh2
1Department of Biology and Medical Genetics, Vietnam Military Medical University, Hanoi, Vietnam; 2Military Institute of Clinical Embryology and Histology, Vietnam Military Medical University, Hanoi, Vietnam; 3IVF Centre, Tam Anh General Hospital, Hanoi, Vietnam; 4Le Huu Trac National Burn Hospital, Vietnam Military Medical University, Hanoi, Vietnam
Correspondence: Son The Trinh, Military Institute of Clinical Embryology and Histology, Vietnam Military Medical University, Hanoi, 12108, Vietnam, Email [email protected]
Background: Chromosomal abnormalities and variations are significant contributors to reproductive challenges. This study aims to investigate the types and incidence of structural autosomal anomalies and autosomal variations in a large Vietnamese population undergoing infertility treatment.
Material and Methods: A retrospective analysis was conducted on 19,191 females and 18,584 males who needed assisted reproductive technology (ART) at the Military Institute of Clinical Embryology and Histology, and Andrology and Fertility Hospital of Hanoi from 2020 to 2023. Karyotyping was conducted using the G-band staining method, and the data were analyzed with STATA 16.0 software.
Results: Males have a higher overall occurrence of structural autosomal anomalies, with a total of 359 cases (1.932%) compared to 306 cases (1.594%) in females, particularly inversions and robertsonian translocations. Chromosome 9 inversions were equally observed in both genders, while robertsonian translocations and reciprocal translocations were more frequent in males (0.183% and 0.468%, respectively) than in females (0.146% and 0.406%, respectively). Deletions and duplications were more prevalent in males, occurring at rates of 0.215% and 0.016%, respectively, versus 0.036% and 0.021% in females. Total autosomal variants were 1478 (7.953%) in males and 1864 (9.7%) in females. Chromosome 9 exhibits the highest occurrence of the q+/qh+ variant, followed by the one of chromosome 1 and chromosome 16. Chromosomes 21 and 22 show notable numbers of ps+ and pstk+ variants.
Conclusion: Structural autosomal anomalies and autosomal variations are common in Vietnamese patients undergoing infertility, highlighting the necessity of genetic testing, particularly karyotyping, in the evaluation and management of infertility.
Keywords: infertility, karyotyping, structural autosomal anomalies, autosomal variations
Introduction
Infertility is characterized by the inability to conceive despite engaging in regular, unprotected sexual intercourse for a period of 12 months. The pooled estimates indicate that the lifetime prevalence of 12-month infertility is 17.5%, while the period prevalence stands at 12.6%.1 There are numerous causes of infertility, and the most common causes of infertility being ovulatory dysfunction, tubal occlusion, endometriosis, diminished ovarian reserve, uterine factors, male factors, and genetic factors.2 Genetic factors account for nearly 30% of infertility cases, including abnormal structures and chromosomal variations affecting both genders. Similar to other multifactorial conditions, genetics is presumed to be a key contributor; however, the specific molecular pathways and genetic determinants are not yet well elucidated.3
In this context, chromosomal abnormalities, such as inversions and translocations, are identified in approximately 3% to 19% of infertile men, particularly those with severe conditions like azoospermia.4 These structural anomalies can disrupt normal spermatogenesis, leading to infertility.5,6 Furthermore, chromosomal variations have a significant impact on male infertility, especially in assisted reproductive technologies such as in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI).7,8 Research shows that certain variations, 9qh+, and Yqh+, are associated with decreased sperm quality and lower fertilization rates.9–11
Similarly, abnormal structures and variations in autosomal chromosomes significantly impact female infertility. Structural abnormalities like translocations can disrupt normal reproductive processes and contribute to miscarriage or infertility. A recent systematic review of chromosomal polymorphism in assisted reproduction revealed an association with increased miscarriage rates that were sex-dependent, showing higher rates in female carriers compared to male carriers.12
The application of genetic testing, particularly karyotyping, is essential in screening and diagnosing infertility in both men and women. Karyotype analysis provides crucial insights into chromosomal abnormalities that may contribute to infertility. Studies indicate that approximately 15% of men with low sperm counts or azoospermia exhibit significant chromosomal abnormalities, such as Klinefelter syndrome and other numerical or structural alterations.13 In women, the prevalence of chromosomal anomalies is similarly concerning; one study found that up to 5% of women with recurrent miscarriages had detectable chromosomal abnormalities, underscoring the importance of karyotyping in this population as well.14 Furthermore, another study highlighted that balanced translocations, often undetected without karyotyping, can lead to infertility or pregnancy loss in couples.15 Karyotype testing allows for the identification of these abnormalities, enabling healthcare providers to offer tailored management plans, including preimplantation genetic testing during IVF procedures.16 By understanding the genetic underpinnings of infertility, couples can make informed decisions about their reproductive options and potential risks to offspring. This study aims to investigate the types and incidences of structural autosomal anomalies and autosomal variations in a Vietnamese population undergoing infertility, thereby providing comprehensive insights into the status of infertility in Vietnam.
Materials and Methods
Study Population
This retrospective descriptive study was carried out at the Military Institute of Clinical Embryology and Histology and the Andrology and Fertility Hospital in Hanoi, between 2020 and 2023. It involved data from 18.584 men and 19.191 women, all of whom were of reproductive age (20–60 years old) and consented to karyotype testing. Individuals with monogenic disorders, cancers, or severe chronic diseases were excluded from the study.
Cytogenetic Analysis (Karyotyping)
Karyotyping was performed using the chromosomal G-band staining technique. Chromosome analysis of peripheral blood was conducted following the College of American Pathologists (CAP) guidelines established in 2010, which stipulate a resolution of 400 bands for routine cases and 550 bands for “inappropriate blood samples” (such as those assessed for intellectual disabilities, dysmorphology, and congenital anomalies) to ensure thorough and precise results. Two-milliliter samples of peripheral blood were collected from patients, anticoagulated with heparin, and cultured in RPMI-1640 medium enriched with fetal calf serum and phytohemagglutinin (PHA) at 37°C for 72 hours. Cell division during metaphase was halted using colcemid. The cells underwent treatment with a hypotonic solution before being fixed in a Carnoy solution. They were then placed on glass slides to expose the chromosomes, treated with trypsin, and stained with Giemsa. Chromosome clusters were examined and documented using an optical microscope, arranged, and analyzed according to ISCN 2020 guidelines. A minimum of 20 metaphases were analyzed for each male participant. All polymorphic variations in the heterochromatin length of chromosomes were recorded, distinguishing between polymorphic variants of the lengths of the stalks (pstk) and satellites (ps) of acrocentric chromosomes.
Statistical Analyses
All parameters were presented as numbers and proportions, along with comparisons of specific types of structural abnormalities. Data analysis was performed using STATA software (Version 16.0; Stata Corporation).
Results
Structural Autosomal Anomalies
Inversions, reciprocal translocations, and robertsonian translocations are more prevalent in males than in females, with 195 cases (1.049%) versus 189 cases (0.985%), 87 cases (0.468%) versus 78 cases (0.406%), and 34 cases (0.183%) versus 28 cases (0.146%), respectively. Deletions and duplications are rare but occur slightly more often in males at 0.215% and 0.016%, respectively, compared to 0.036% and 0.021% in females (Table 1).
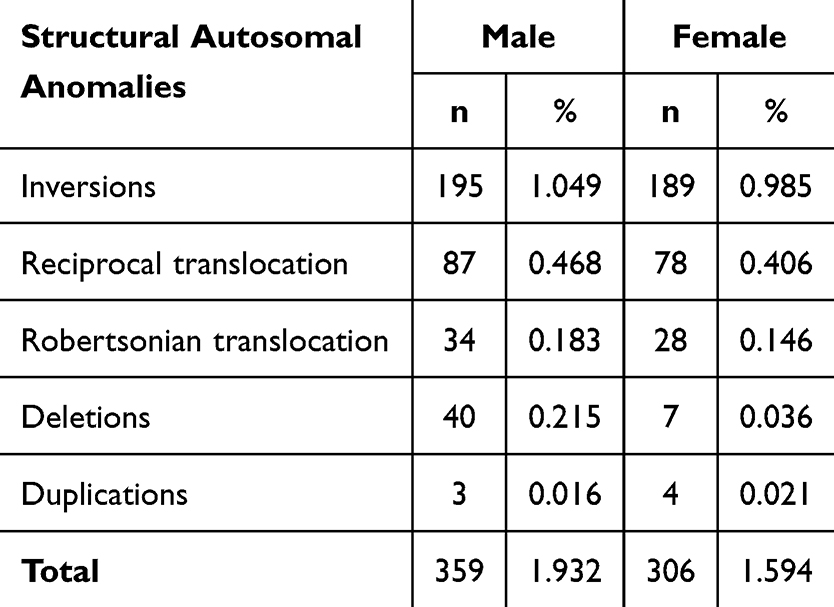 |
Table 1 Structural Autosomal Anomalies |
Chromosome 9 exhibits the highest frequency of inversions, particularly the inv(9)(p11q13) variant, which is seen in 174 females (0.907%) and 176 males (0.947%), suggesting a nearly equal distribution across genders. The occurrences of inv(9)(p11q13) and Yqh+ variant show significant commonality in the group of males carrying inv(9) (with 20 cases). Specifically, one case was documented featuring two distinct inversion variants on chromosome 9 (46,XX,inv(9)(p11q13), inv(9)(p12q13)), two females with inv(9)(p11q13)x2 variant and only one male with inv(9)(p12q13) variant. In contrast, inversions in chromosomes 1, 3, 4, 5, 6, 7, and 13 are far less frequent, often represented by one or two individuals. Notably, chromosome 1 inversions are observed once each in males and females, while chromosome 13 inversions, which are rare, appear in both genders equally (Table 2).
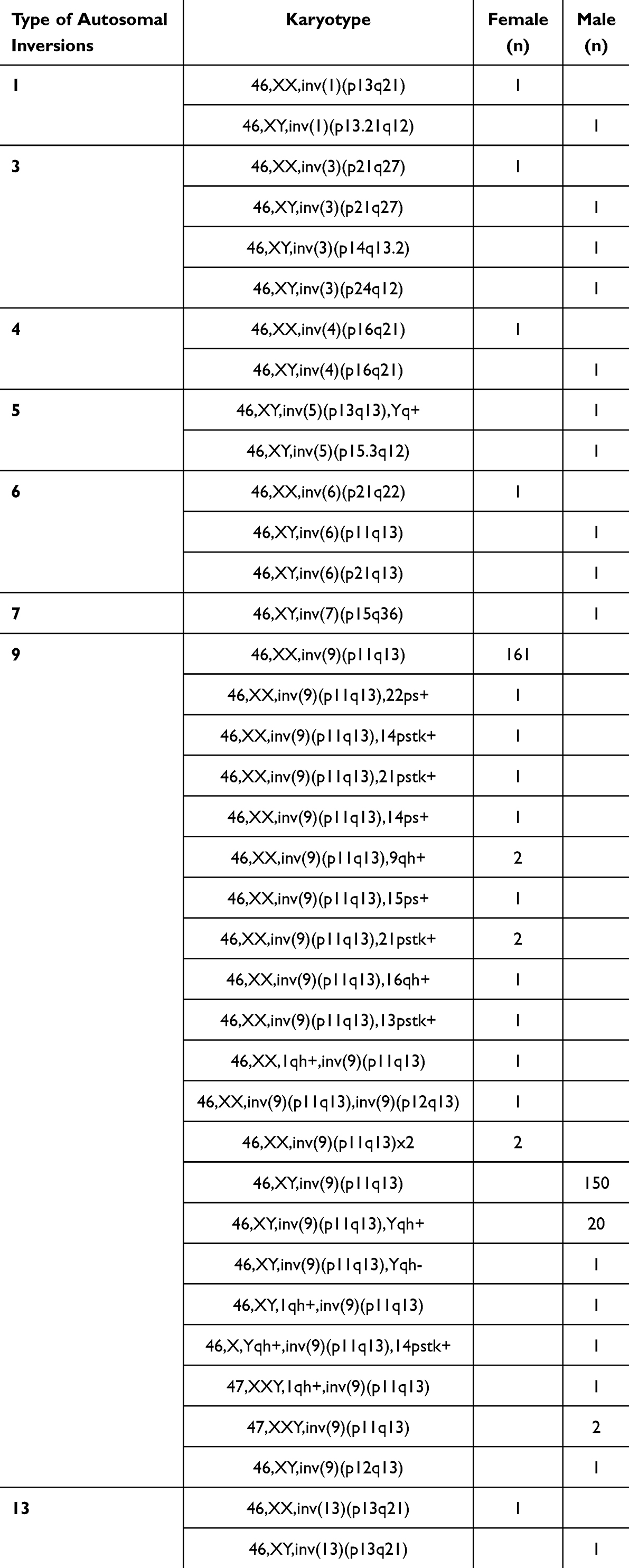 |
Table 2 Autosomal Inversions |
The majority of reciprocal translocations observed in both genders occur as singular events, indicating a high level of diversity among these variations. Regarding robertsonian translocations, a similar pattern is observed in both males and females. The common translocation in females is rob(13;14)(q10;q10) and rob(14;21)(q10;q10), with an occurrence of 19 cases and 5 cases, respectively. Similarly, in males, the same robertsonian translocations are found, with 18 cases of rob(13;14)(q10;q10) and 5 cases of rob(14;21)(q10;q10). Certain robertsonian translocations, such as rob(13;15)(q10;q10), show higher frequencies, particularly among males (Table 3). Specifically, there is one case of a male with a translocation involving three chromosomes with the karyotype 46,XY,t(6;14;11)(q21;q32;p13).
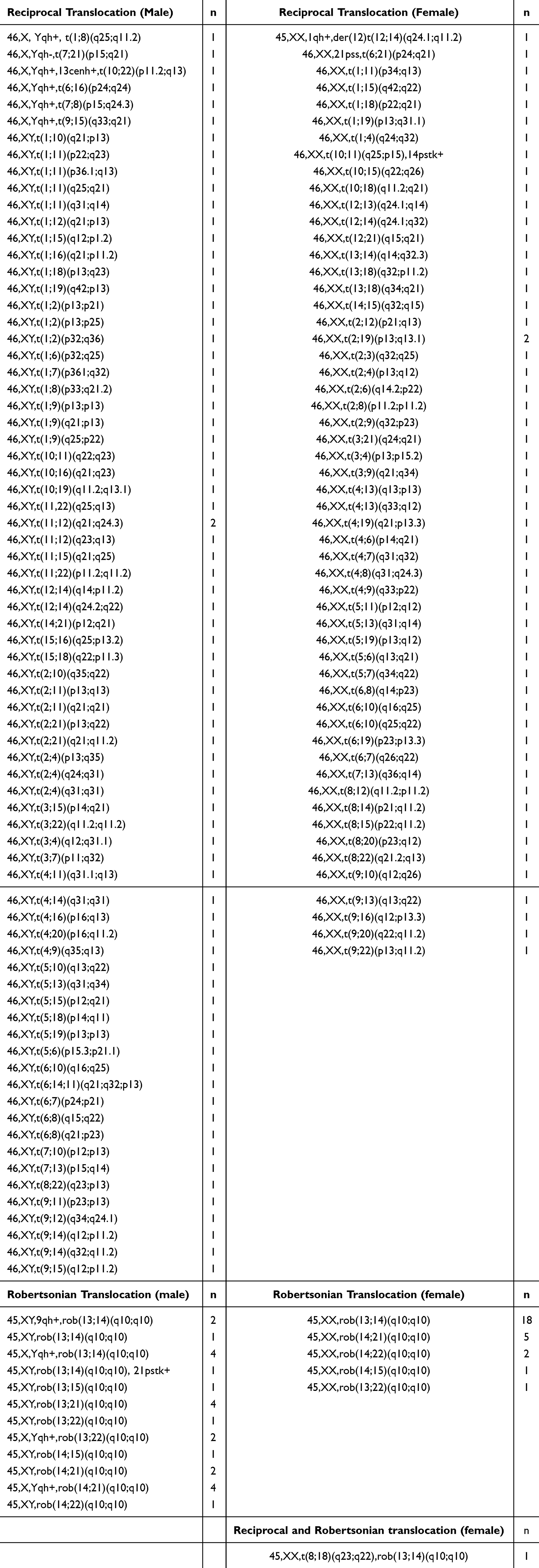 |
Table 3 Autosomal Translocations |
Autosomal Variations
The total number of variants recorded in females is 1864, representing 9.713% of the sample size, indicating the presence of autosomal variations across different chromosomes (Table 4).
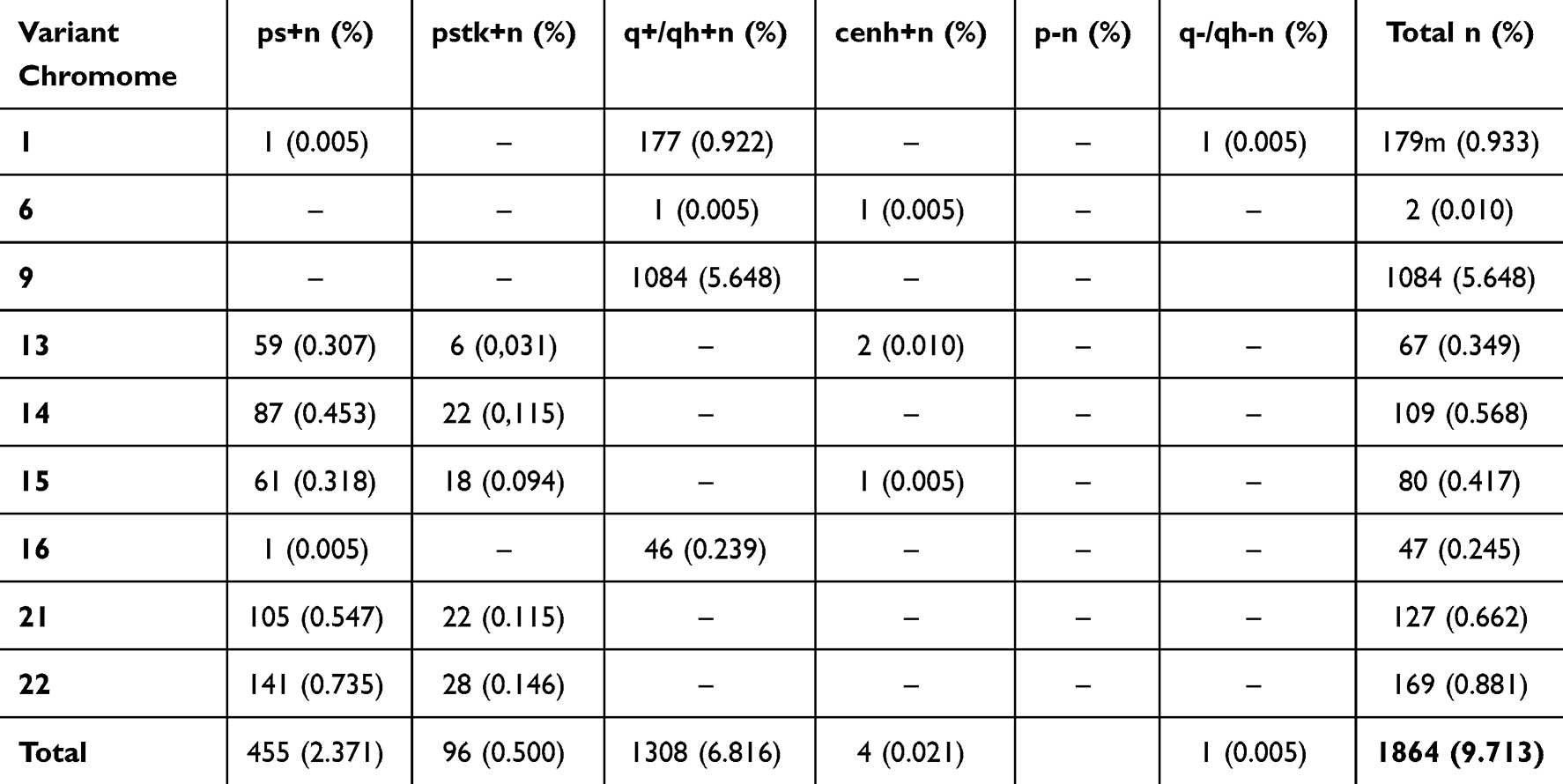 |
Table 4 Autosomal Variations Involving One Autosome in Females |
The most prevalent variant is the q+/qh+ variant on chromosome 9, identified in 1084 cases (5.648%), followed by a notable occurrence of the q+/qh+ variant on chromosome 1 and 16 with 177 cases (0.922%) and 46 cases (0.239%), respectively. Other noteworthy findings reveal a substantial presence of ps+ variants on chromosomes 21 and 22, with 105 occurrences (0.547%) and 141 occurrences (0.735%), respectively. Similarly, pstk+ variants exhibited comparable prevalence rates, with 22 cases (0.115%) on chromosome 21 and 28 cases (0.146%) on chromosome 22. Chromosome 6 has the lowest occurrence, with only 2 total cases across ps+ and cenh+ variants (Table 4).
The total number of autosomal variations documented is 1478, accounting for 7.953% of the sample. The q+/qh+ variant is the most prevalent (5.392%), while other variants such as cenh+ and q-/qh- are rare, each comprising less than 0.02% of the total (Table 5).
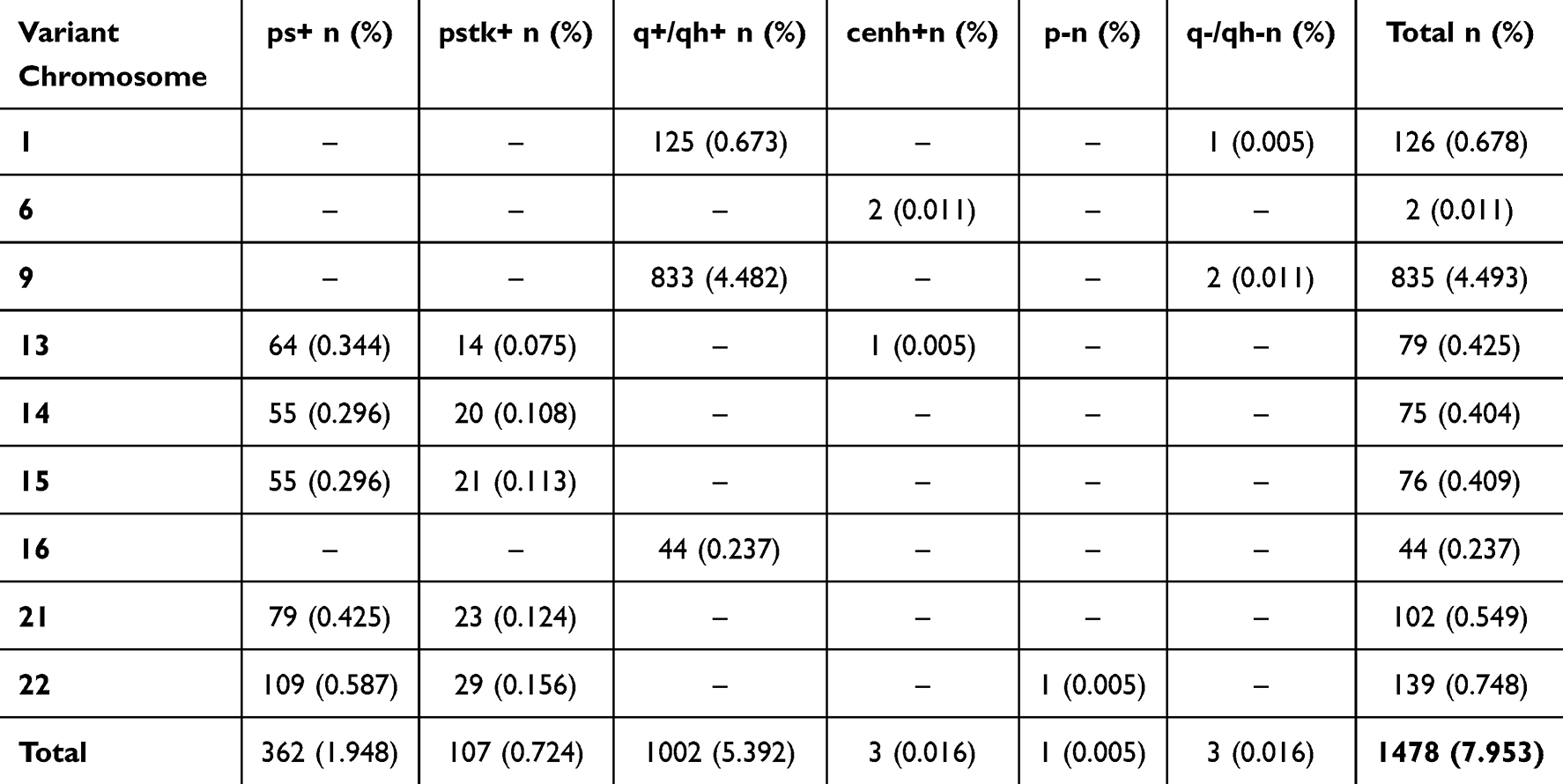 |
Table 5 Autosomal Variations Involving One Autosome in Males |
In males, chromosome 9 shows the highest frequency of the q+/qh+ variant, with 833 occurrences (4.482%). This is followed by a notable occurrence of the q+/qh+ variant on chromosome 1 with 125 cases (0.673%) and chromosome 16 with 44 cases (0.237%). Similar to the female data, chromosomes 21 and 22 reveal a relatively high number of ps+ variants, with 79 and 109 cases, respectively, and pstk+ variants with 23 cases and 29 cases, respectively. In contrast, the rarer variants, cenh+, and p-, are observed sparingly across all chromosomes, appearing in only one to three cases (Table 5).
The combination of variations in autosomes includes 92 cases in females (0.48%) and 56 cases in males (0.301%). Most of the autosomal variations are rare, with percentages typically ranging between 0.005% and 0.038%. The largest frequency in males is the variant 46,XY, 21ps+, and 22ps+ (0.043%). The autosomal variations in females are more variety, with some recurring more frequently such as 46,XX,21ps+,22ps+ (0.073%) (Table 6).
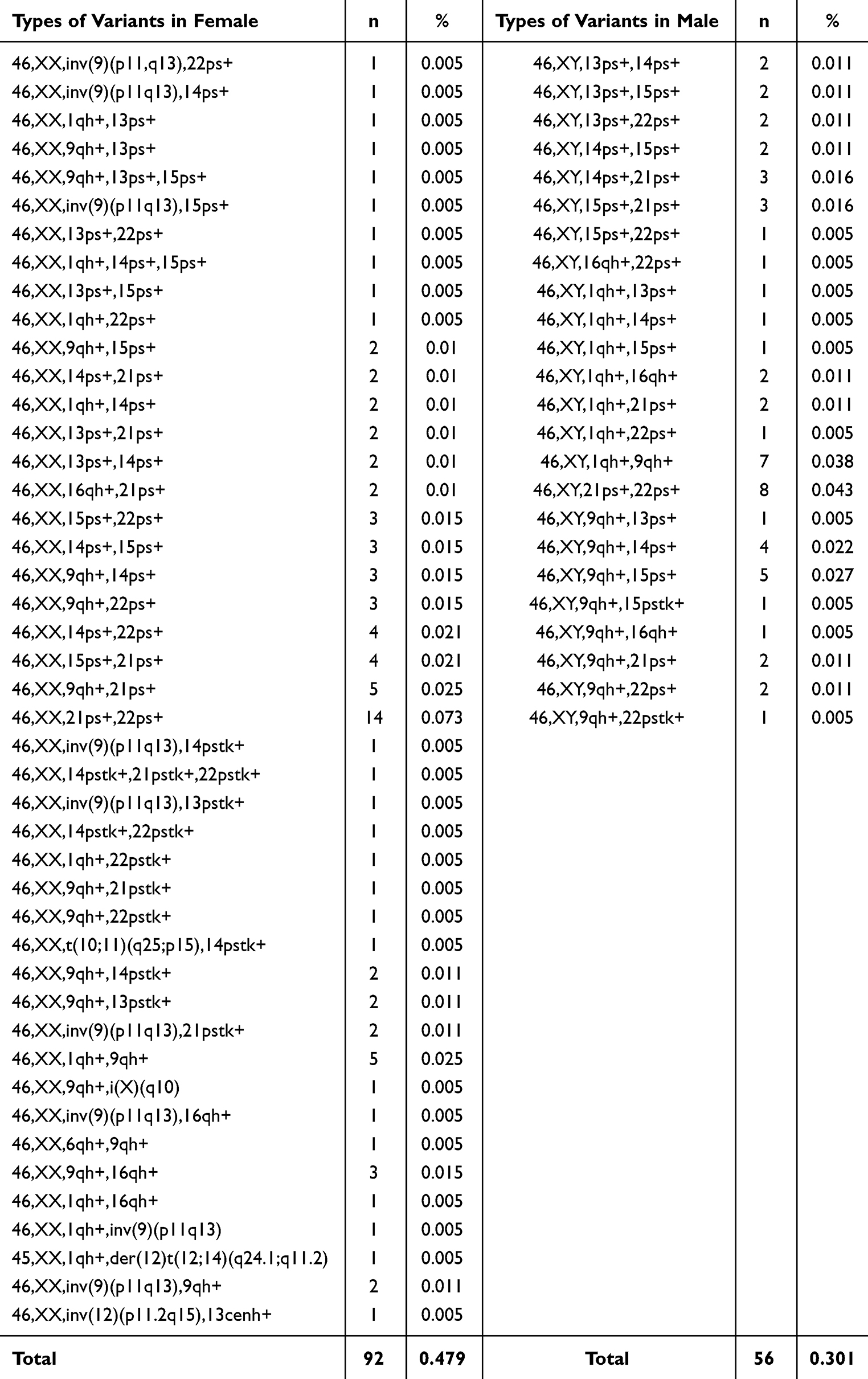 |
Table 6 Combination of Variations in Autosomes in Both Genders |
Discussion
In this study, the inversions, robertsonian translocations, and reciprocal translocations are more common in males than females, with specific prevalence rates of 1.049% for inversions and 0.183% for robertsonian translocations in males compared to 0.985% and 0.146% in females, respectively. These results align with those from a study that reported a significant incidence of structural abnormalities in ART populations, emphasizing the need for comprehensive genetic screening before ART procedures to better understand potential risks associated with chromosomal anomalies.17,18 In contrast, the study by Ogasawara et al found that while the overall rate of chromosomal abnormalities was similar between ART and spontaneous pregnancy groups, the types of abnormalities differed significantly; structural abnormalities were notably higher in the ART group.17 This supports our observation that deletions, although rare, occur slightly more frequently in males (0.215%) than in females (0.036%). The emphasis on understanding these differences is crucial, as structural anomalies can lead to infertility or recurrent miscarriages.19 Moreover, the literature consistently suggests that while both males and females undergoing ART exhibit chromosomal abnormalities, males tend to show a higher prevalence of specific types such as inversions and robertsonian translocations. This has been corroborated by various studies indicating that male infertility is often linked to higher rates of chromosomal anomalies, which can adversely affect sperm quality and overall reproductive outcomes.19 The findings reinforce these observations and highlight the importance of targeted genetic counseling for couples undergoing ART, as understanding these risks can guide treatment decisions and improve success rates.
Our research findings indicate that inversions are more prevalent in males, with 195 cases (1.049%) compared to 189 cases (0.985%) in females, highlighting a slightly higher incidence in the male population. Research by Young et al (2019) indicates that carriers of balanced chromosomal inversions do not exhibit significantly higher rates of aneuploidy compared to controls; however, they may still face reproductive challenges due to the potential for producing unbalanced gametes.20 Pericentric inversions also can disrupt spermatogenesis and are associated with azoospermia and oligospermia in males.21 This highlights the importance of preimplantation genetic testing (PGT) for couples undergoing ART to screen for chromosomal abnormalities and improve the chances of successful pregnancies. Genetic counseling for inversion carriers is crucial due to the varying clinical manifestations associated with different inversion types.22 The most common inversion variant in our data was in chromosome 9, specifically inv(9)(p11q13) variants observed nearly equal distribution across genders, with 174 females (0.907%) and 176 males (0.947%). Research indicates that inversions on chromosome 9 can significantly affect fertility outcomes. Alhalabi et al (2023) highlight that familial pericentric inversions on chromosome 9 are linked to recurrent miscarriages and infertility, emphasizing the need for genetic counseling when such anomalies are identified in couples seeking reproductive assistance. The presence of inversions can lead to unbalanced gametes, which may contribute to adverse reproductive outcomes, including miscarriages and congenital anomalies.23
Most reciprocal translocations are infrequent, with many occurring only once in the studied population. Reciprocal translocations are associated with reproductive challenges. A study by Zhishuo et al (2011) emphasizes that while these translocations can lead to miscarriages and infertility, their occurrence is relatively low in the general population.24 The rarity of reciprocal translocations indicates that they may not be a primary cause of infertility, but they can lead to significant reproductive issues when present. Both males and females exhibit similar frequencies of robertsonian translocations (with rob(13;14)(q10;q10) and rob(14;21)(q10;q10)), while rob(13;22)(q10;q10) is more frequent in males. Males and females display similar frequencies of the most prevalent robertsonian translocations, specifically rob(13;14)(q10;q10) and rob(14;21)(q10;q10), although rob(13;22)(q10;q10) is observed more frequently in males. Research by Scriven et al (2001) highlights that these structural abnormalities can significantly impact reproductive outcomes due to their potential to produce unbalanced gametes. Male carriers of robertsonian translocations often face challenges such as oligospermia or azoospermia, which complicates their fertility potential.25 Moreover, a case report by Almesned et al (2020) discusses how male carriers of robertsonian translocations may still have viable sperm but often require ART to achieve successful pregnancies.26 The authors suggest that preimplantation genetic diagnosis (PGD) can be beneficial for these couples to reduce the risk of miscarriage and improve live birth rates. The clinical implications of these findings are significant for genetic counseling and ART management. Couples with known robertsonian translocations should be counseled about the risks associated with unbalanced gametes and the potential for recurrent pregnancy loss. A study by Poornima et al (2020) emphasizes the importance of comprehensive genetic testing for couples undergoing ART, as identifying chromosomal abnormalities can inform treatment strategies and improve outcomes.18 Furthermore, the role of genetic counseling is crucial in helping couples understand their options when faced with chromosomal abnormalities. As noted by Almesned et al, a multidisciplinary approach involving urologists, reproductive endocrinologists, and genetic counselors is essential to optimize fertility management for couples affected by these translocations.26
Regarding the autosomal variations in females, the frequency of the q+/qh+ variant on chromosome 9 observed in our data aligns with previous reports.27,28 This variant has been associated with an increased risk of miscarriage and infertility, emphasizing the need for further investigation into its clinical significance.29 The result also reveals significant occurrences of ps+ variants in chromosomes 21 and 22, as well as chromosomes 14 and 15. These results are supported by studies that have identified similar patterns of chromosomal variants in infertile individuals.29 The presence of these variants may contribute to meiotic segregation errors and subsequent reproductive failure.
The incidence of autosomal variations in males is 7.953%. This ratio is closely aligned with the prevalence of chromosomal variants in infertile men reported in previous studies, although we do not account for the variations present on the sex chromosomes. A study by Perrin et al (2013) found that chromosomal variants were present in 7.6% of infertile men, with the most common variants being pericentric inversions and heterochromatin variations.30 Similarly, Mierla and Stoian (2012) reported that chromosomal variants were present in 8.3% of infertile men, with the most common variants being pericentric inversions and heterochromatin variations.31 The presence of chromosomal variants in infertile men has been associated with various reproductive outcomes. A study by Li et al (2024) found that chromosomal variants were associated with a higher risk of non-obstructive azoospermia in Chinese men.32 Additionally, a study by Dul et al (2012) found that chromosomal variants had adverse effects on spermatogenesis and negatively influenced the outcome of IVF/ICSI-ET treatment.33
The combination of variations is associated with various health implications for males, particularly concerning fertility and reproductive outcomes. Research indicates that chromosomal polymorphisms, such as those involving heterochromatic regions, can lead to significant issues in spermatogenesis, resulting in conditions like azoospermia and oligozoospermia. Specifically, studies have shown that men with such variants exhibit higher rates of severe oligozoospermia and azoospermia compared to those without these variants, suggesting a detrimental effect on sperm production and quality.34 Moreover, the presence of these chromosomal variants has been linked to increased rates of aneuploidy in sperm cells, which can negatively impact ART outcomes, including IVF success rates.35 The specific variant “46,XY,1qh+” has been noted in studies to correlate with poor sperm morphology and function, further complicating fertility issues and potentially leading to adverse pregnancy outcomes.6 Therefore, individuals carrying this chromosomal variant may face challenges not only in achieving conception but also in the health of potential offspring due to the increased risk of genetic anomalies. The combination of variations can significantly impact female infertility, often leading to various reproductive challenges. Chromosomal variations like inv(9) and 1qh+ have been associated with increased rates of reproductive failure, including miscarriages and failed IVF attempts.36,37
The retrospective design limits data completeness and control over variables, making causal inference challenging. However, it provides valuable insights, especially when prospective studies are impractical or resource-intensive. In our study, it focuses on a specific population group—men and women of reproductive age in Vietnam. Consequently, the dataset includes both patients undergoing assisted reproductive techniques and premarital general health examination. While these data may not be representative of the entire population or solely of patients requiring assisted reproductive technologies, they nonetheless provide a significant and extensive genetic dataset within the Vietnamese population.
Conclusion
In conclusion, structural autosomal anomalies and autosomal variations are relatively common in Vietnamese patients undergoing infertility, with some types being more prevalent than others. The presence of them has been associated with infertility problems in both genders. From a clinical perspective, incorporating genetic testing into routine infertility assessments can facilitate early diagnosis, allowing for personalized treatment strategies and more informed reproductive planning. Identifying specific genetic anomalies enables clinicians to recommend appropriate assisted reproductive technologies (ART) and optimize patient outcomes. Furthermore, these results underscore the significance of genetic counseling in infertility care, providing couples with a clearer understanding of their reproductive risks and potential interventions. By integrating genetic insights into clinical practice, healthcare providers can offer more precise and effective fertility treatments while also addressing the psychological and ethical considerations associated with genetic infertility factors.
Abbreviations
ART, Assisted reproductive technology; IVF, In vitro fertilization; ICSI, Intracytoplasmic sperm injection; PGT, Preimplantation genetic testing; PGD, Preimplantation genetic diagnosis.
Data Sharing Statement
All data supporting the findings of this study can be obtained from the corresponding author upon request.
Ethical Statements
The study received approval from the ethical committee of the Military Institute of Clinical Embryology and Histology at Vietnam Military Medical University (reference number 150224/IRB-VMPLSQĐ) and Andrology and Fertility Hospital of Hanoi (reference number No.8202/2024/IRB-AFHANOI), which was conducted in accordance with the Declaration of Helsinki. Informed written consent was obtained from all patients participating in the study.
Consent For Publication
We are aware that the The Application of Clinical Genetics journal will reach a wider audience through marketing efforts and third-party platforms, and it may be available in both print and online formats. As a result, all published content in the journal will be accessible to everyone. We understand that the readership may include journalists, the general public, academic researchers, and medical professionals. For any inquiries, please email [email protected].
Acknowledgment
This research received support from the Military Institute of Clinical Embryology and Histology, and the Andrology and Fertility Hospital of Hanoi.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work received no funding.
Disclosure
All authors declare that they have no conflicts of interest related to this study and confirm that the research was conducted without any commercial or financial relationships that could be perceived as potential conflicts of interest.
References
1. Cox CM, Thoma ME, Tchangalova N, et al. Infertility prevalence and the methods of estimation from 1990 to 2021: a systematic review and meta-analysis. Hum Reprod Open. 2022;2022(4):hoac051. doi:10.1093/hropen/hoac051
2. Carson SA, Kallen AN. Diagnosis and management of infertility: a review. JAMA. 2021;326(1):65. doi:10.1001/jama.2021.4788
3. Friedrich D Rer Nat C, Tüttelmann UPD Med F. Genetics of female and male infertility. Medizinische Genetik. 2024;36(3):161. doi:10.1515/medgen-2024-2040
4. Naasse Y, Charoute H, El Houate B, et al. Chromosomal abnormalities and Y chromosome microdeletions in infertile men from Morocco. BMC Urol. 2015;15:95. doi:10.1186/s12894-015-0089-3
5. Demirhan O. Chromosome abnormalities related to male infertility. Infertility. 2023;5:1052.
6. Mierla D, Jardan D, Stoian V. Chromosomal Abnormality in Men with Impaired Spermatogenesis. Int J Fertil Steril. 2014;8(1):35–42.
7. Liang L, Zhang X, Zhang Z, et al. Effect of chromosomal polymorphisms on the outcome of in vitro fertilization and embryo transfer. J Obstet Gynaecol Res. 2023;49(9):2351–2360. doi:10.1111/jog.15732
8. Zhang XP, Zhang YF, Liang LX, et al. The effects of chromosome polymorphism on the clinical outcomes of in vitro fertilization/embryo transfer-assisted reproduction. J Matern Fetal Neonatal Med. 2023;36(2):2238863. doi:10.1080/14767058.2023.2238863
9. Mottola F, Santonastaso M, Ronga V, Finelli R, Rocco L. Polymorphic rearrangements of human chromosome 9 and male infertility: new evidence and impact on spermatogenesis. Biomolecules. 2023;13(5):729. doi:10.3390/biom13050729
10. Atli E, Mail Ç, Gurkan H, Yalçintepe S, Demir S, Atli E. Y chromosome polymorphism in Turkish patients with reproductive problems: a genetic centre experience. Eur Res J. 2023;9(4):725–729. doi:10.18621/eurj.1130666
11. Impacts of male chromosomal polymorphisms on semen quality and IVF/ICSI outcomes: a retrospective cohort study - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/38576264/.
12. Ralapanawe MSB, Gajaweera SL, Karunaratne N, et al. Chromosomal polymorphisms in assisted reproduction: an analysis of 942 cycles. Reprod Fertil. 2022;3(3):133–139. doi:10.1530/RAF-21-0116
13. Akgul M, Ozkinay F, Ercal D, et al. Cytogenetic abnormalities in 179 cases with male infertility in Western Region of Turkey: report and review. J Assist Reprod Genet. 2009;26(2–3):119–122. doi:10.1007/s10815-009-9296-8
14. Sugiura-Ogasawara M, Ozaki Y, Sato T, Suzumori N, Suzumori K. Poor prognosis of recurrent aborters with either maternal or paternal reciprocal translocations. Fertil Steril. 2004;81(2):367–373. doi:10.1016/j.fertnstert.2003.07.014
15. Goddijn M, Joosten JHK, Knegt AC, et al. Clinical relevance of diagnosing structural chromosome abnormalities in couples with repeated miscarriage. Hum Reprod. 2004;19(4):1013–1017. doi:10.1093/humrep/deh172
16. Franasiak JM, Forman EJ, Hong KH, et al. The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies evaluated with comprehensive chromosomal screening. Fertil Steril. 2014;101(3):656–663.e1. doi:10.1016/j.fertnstert.2013.11.004
17. Gui J, Ding J, Yin T, Liu Q, Xie Q, Ming L. Chromosomal analysis of 262 miscarried conceptuses: a retrospective study. BMC Pregnancy Childbirth. 2022;22:906. doi:10.1186/s12884-022-05246-1
18. Poornima S, Daram S, Devaki RK, Qurratulain H. Chromosomal abnormalities in couples with primary and secondary infertility: genetic counseling for assisted reproductive techniques (ART). J Reprod Infertil. 2020;21(4):269–274. doi:10.18502/jri.v21i4.4331
19. Bingol B, Abike F, Gedikbasi A, Tapisiz OL, Gunenc Z. Comparison of chromosomal abnormality rates in ICSI for non-male factor and spontaneous conception. J Assist Reprod Genet. 2012;29(1):25–30. doi:10.1007/s10815-011-9646-1
20. Young D, Klepacka D, McGarvey M, Schoolcraft WB, Katz-Jaffe MG. Infertility patients with chromosome inversions are not susceptible to an inter-chromosomal effect. J Assist Reprod Genet. 2019;36(3):509–516. doi:10.1007/s10815-018-1376-1
21. Li R, Fan H, Zhang Q, Yang X, Zhan P, Feng S. Pericentric inversion in chromosome 1 and male infertility. Open Med. 2020;15(1):343–348. doi:10.1515/med-2020-0404
22. Fan H, Liu Z, Zhan P, Jia G. Pericentric inversion of chromosome 6 and male fertility problems. Open Med. 2022;17(1):191–196. doi:10.1515/med-2022-0411
23. Alhalabi MM, Kakaje A, Alhalabi M. Hereditary chromosomal 9 inversion (p22q13) 9 as a cause for recurrent pregnancy loss: a case report. J Med Case Rep. 2023;17(1):427. doi:10.1186/s13256-023-04137-z
24. Ou Z, Stankiewicz P, Xia Z, et al. Observation and prediction of recurrent human translocations mediated by NAHR between nonhomologous chromosomes. Genome Res. 2011;21(1):33–46. doi:10.1101/gr.111609.110
25. Scriven PN, Flinter FA, Braude PR, Ogilvie CM. Robertsonian translocations—reproductive risks and indications for preimplantation genetic diagnosis. Hum Reprod. 2001;16(11):2267–2273. doi:10.1093/humrep/16.11.2267
26. Almesned R, Alsuhaibani S, Alali H, Qubbaj W, Hathal N. Male infertility in robertsonian translocation: a case report. Am J Case Rep. 2020;21. doi:10.12659/AJCR.921616
27. Li SJ, Cheng YX, Null Y-S, et al. Chromosomal polymorphisms associated with reproductive outcomes after IVF-ET. J Assist Reprod Genet. 2020;37(7):1703–1710. doi:10.1007/s10815-020-01793-8
28. Nadeali Z, Salehi P, Derakhshan-Horeh M, et al. Estimating the risk for chromosomal abnormalities and heteromorphic variants in azoospermic and severe oligozoospermic men. Crescent J Med Biol Sci. 2018;5(2):101–106.
29. Yatsenko SA, Rajkovic A. Chromosomal Causes of Infertility. In: Sermon KD, Viville S, editors. Textbook of Human Reproductive Genetics.
30. Perrin A, Caer E, Oliver-Bonet M, et al. DNA fragmentation and meiotic segregation in sperm of carriers of a chromosomal structural abnormality. Fertil Steril. 2009;92(2):583–589. doi:10.1016/j.fertnstert.2008.06.052
31. Mierla D, Malageanu M, Tulin R, Albu D. Prevalence of chromosomal abnormalities in infertile couples in Romania. Balkan J Med Genet. 2015;18(1):23–30. doi:10.1515/bjmg-2015-0002
32. Li JP, Zhang FB, Li LJ, et al. Y chromosome polymorphisms contribute to an increased risk of non-obstructive azoospermia: a retrospective study of 32,055 Chinese men. J Assist Reprod Genet. 2024;41(3):757–765. doi:10.1007/s10815-024-03022-y
33. Dul EC, Groen H, van Ravenswaaij-Arts CMA, Dijkhuizen T, van Echten-Arends J, Land JA. The prevalence of chromosomal abnormalities in subgroups of infertile men†. Hum Reprod. 2012;27(1):36–43. doi:10.1093/humrep/der374
34. Christofolini DM, Mafra FA, Neto RP. Correlation between chromosomal variants and male infertility in a population of Brazilian infertile men. Reprod Sys Sexual Disord. 2012;01(01). doi:10.4172/2161-038X.1000105
35. Poli MN, Miranda LAL, Gil ED, et al. Male cytogenetic evaluation prior to assisted reproduction procedures performed in Mar del Plata, Argentina. JBRA Assisted Reproduction. 2016;20(2). doi:10.5935/1518-0557.20160015
36. Mierla D, Stoian V. Chromosomal polymorphisms involved in reproductive failure in the Romanian population. Balkan J Med Genet. 2012;15(2):23–28. doi:10.2478/bjmg-2013-0003
37. Sahota JS, Sharma B, Guleria K, Sambyal V. Candidate genes for infertility: an in-silico study based on cytogenetic analysis. BMC Med Genomics. 2022;15(1):170. doi:10.1186/s12920-022-01320-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.