")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
The ADHD Assessment Quality Assurance Standard for Children and Teenagers (CAAQAS)
Authors Young S , Absoud M , Al-Attar Z, Ani C, Colley W, Cortese S, Crame J, Gudjonsson G, Hill P, Hollingdale J, Mukherjee RAS, Ozer S, Partridge G, Smith J, Woodhouse EL, Lewis A
Received 17 August 2024
Accepted for publication 4 December 2024
Published 24 December 2024 Volume 2024:20 Pages 2603—2628
DOI https://doi.org/10.2147/NDT.S472923
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
CAAQAS for children and young people – Video abstract [472923]
Views: 128
Susan Young,1,2 Michael Absoud,3 Zainab Al-Attar,4,5 Cornelius Ani,6,7 William Colley,8 Samuele Cortese,9– 13 Jo Crame,14 Gisli Gudjonsson,2,15 Peter Hill,16 Jack Hollingdale,17 Raja AS Mukherjee,18,19 Susan Ozer,20 Gavin Partridge,21 Jade Smith,22 Emma Louise Woodhouse,17,23 Alexandra Lewis24
1Independent Practice, Psychology Services Limited, London, UK; 2Department of Psychology, Reykjavik University, Reykjavik, Iceland; 3Department of Children’s Neurosciences, Evelina London Children’s Hospital, Guys and St Thomas’ NHS Foundation Trust, London, UK; 4Independent Practice, Psychiatry UK, London, UK; 5Department of Psychiatry, University of Oxford, Oxford, UK; 6Division of Psychiatry, Imperial College London, London, UK; 7Neurodevelopmental Team, Children and Young People’s Service, Surrey and Borders Partnership NHS Foundation Trust, Leatherhead, UK; 8Independent Practice, CLC Consultancy, Dunkeld, UK; 9Centre for Innovation in Mental Health, School of Psychology, Faculty of Environmental and Life Sciences, University of Southampton, Southampton, UK; 10Clinical and Experimental Sciences (CNS and Psychiatry), Faculty of Medicine, University of Southampton, Southampton, UK; 11Child and Adolescent Mental Health Service, Solent NHS Trust, Southampton, UK; 12Hassenfeld Children’s Hospital at NYU Langone, New York University Child Study Center, New York City, NY, USA; 13DiMePRe-J-Department of Precision and Regenerative Medicine-Jonic Area, University of Bari “Aldo Moro”, Bari, Italy; 14Service-User Representative, Surrey, UK; 15Department of Psychology, Institute of Psychiatry, Psychology & Neuroscience, King’s College London, London, UK; 16Independent Practice, London, WC1N 3HB, UK; 17Independent Practice, Compass Psychology Services Ltd, London, UK; 18ASD and ADHD Service, Horizon, Epsom, UK; 19University of Surrey Medical School, Guildford, UK; 20Child Development Centre, East and North Hertfordshire NHS Trust, Stevenage, UK; 21Partridge ADHD Clinic, Oxford, UK; 22Children and Young People’s Neurodevelopmental Service, Humber NHS Foundation Trust, Hull and East Riding, UK; 23Department of Forensic & Neurodevelopmental Sciences, Institute of Psychiatry, Psychology & Neuroscience, King’s College London, London, UK; 24Fulbourn Hospital, Cambridgeshire and Peterborough Foundation NHS Trust, Cambridge, UK
Correspondence: Susan Young, Email [email protected]
Abstract: Around 5% of the children and teenagers worldwide are affected by Attention-Deficit/Hyperactivity Disorder [ADHD], making it a major public health concern. Recently, demand for assessments has substantially increased, putting strain on healthcare and waiting lists. There is concern that pressure to clear service bottlenecks is leading to variable quality and reliability of ADHD assessments in this population. The ADHD Assessment Quality Assurance Standard for Children and Teenagers [CAAQAS] aims to address this by proposing a quality framework for ADHD assessments in this population. CAAQAS is intended to complement formal training, provide support to clinicians, inform commissioners, and empower children, teenagers, and caregivers on what to expect from an assessment and assessment report. Our goal is to promote evidence-based high-quality assessments, improve diagnostic accuracy, and reduce the risks of overdiagnosis, misdiagnosis, and underdiagnosis. Seven key topics were identified by authors which guided the development of this expert consensus statement. It was agreed that a high-quality diagnostic assessment of ADHD in this population commences with advance preparation to facilitate engagement of the child or teenager and caregivers. The consensus agreed that the minimum/essential standards for assessing and diagnosing ADHD adopt a systematic approach from pre-assessment through assessment to post-diagnostic stage, enabling ADHD to be disentangled from differential diagnoses. The process applies multi-source information to inform an assessment of development history and early risk factors, history of physical, mental health and other neurodevelopmental conditions, family, educational, and social histories. Assessment of core ADHD symptoms should include specific developmentally appropriate examples of associated difficulties and impairments. Neuropsychiatric and physical comorbidities should be assessed and identified. Recommendations for report writing are intended to facilitate effective communication between ADHD specialists and other services, and we highlight the importance of linking the diagnosis to an appropriate post-diagnostic discussion. Further, we discuss core competencies required to conduct a diagnostic assessment of ADHD in children and teenagers.
Keywords: attention deficit hyperactivity disorder, practice guidelines, diagnosis, children, teenagers, assessment
Introduction
In the clinical assessment and diagnosis of Attention-Deficit/Hyperactivity Disorder [ADHD] in children and teenagers, the importance of quality assurance standards cannot be overstated. ADHD is one of the most common neurodevelopmental conditions affecting children and teenagers, with a significant impact on academic, social, and emotional functioning. Prevalence rates suggest that around 5% of the children and teenagers worldwide are affected by ADHD, making it a major public health concern.1,2 However, the transdiagnostic nature of ADHD symptoms (inattentiveness, restlessness, impulsivity) are features of many conditions, creating a higher risk of diagnostic errors and consequent erroneous or ineffective interventions.3 The quality of the diagnostic assessment process is key to achieving accurate diagnosis of ADHD.
While classification systems such as the Diagnostic and Statistical Manual of Mental Disorders Text Revision DSM-5-TR4 or the International Classification of Diseases ICD-115 provide criteria for diagnosing ADHD, they offer limited guidance on the process of obtaining an accurate diagnosis.
In the United Kingdom, the National Institute of Health and Care Excellence (NICE) offers guidelines for the diagnosis and management of ADHD6,7, but these guidelines do not specify detailed procedures for clinical practice. This gap in guidance leaves practitioners without clear direction on how to conduct assessments effectively. Recognising the need for more specific guidance, the UK Adult ADHD Network (UKAAN) has developed comprehensive guidance for assessing adults with ADHD - the Adult ADHD Assessment Quality Assurance Standard (AQAS).8 This document has been welcomed, with demands from professionals and people with lived experience for similar guidance tailored to the assessment of those aged 19 or younger. Hence, we present the ADHD Assessment Quality Assurance Standard for Children and Teenagers [CAAQAS], a quality framework for ADHD assessments of individuals between the age of 5–19 (although tertiary services may see younger children at age 4), developed through a process of expert consensus.
Why Guidance on ADHD Assessment for Children and Teenagers is Necessary
The necessity for detailed guidance in assessing children and teenagers with ADHD stems from several factors. It is a guiding principle that children, teenagers, and adults need different approaches to healthcare. The presentation of physical and mental health conditions in children and teenagers may differ considerably from that in adults; often being less clear-cut and requiring input from multiple sources (eg parents/caregivers, teachers).9 A further complexity is that children and teenagers are developing in a range of different areas (eg cognitive, emotional, and social development) and they can therefore grow out of difficulties as well as into them. The unique considerations in diagnosing ADHD in children and teenagers (such as developmental differences) necessitate specific recommendations. Thus, the use of AQAS to guide ADHD assessments is inappropriate, and tailored child-centred guidance is required.
Establishing agreed quality standards for ADHD diagnostic assessments and reports in children and teenagers can reduce variability in quality and improve overall care, ensuring those with ADHD receive support and interventions at the earliest opportunity. This means that appropriate resources can be directed towards this population, preventing ineffective and cost-ineffective treatments, potential harmful side-effects from medications and non-pharmacological treatments, unnecessary costs associated with misdiagnosis, and other treatable conditions being overlooked. Misdiagnosis could also mislead caregivers and children/adolescents, increasing the likelihood of psychological distress.
CAAQAS aims to serve as a benchmark, ensuring children and teenagers receive reliable and valid diagnostic assessments, reflecting high quality in clinical practice and standards of care. The guidance will be helpful for four groups:
- Clinicians: Clarification of best practice will increase clinicians’ confidence and competence in diagnostic accuracy. It will limit potential harm from inappropriate treatment and support them to resist managerial pressures to prioritise speed over quality of assessment.
- Commissioners of ADHD services: The guidance will provide a benchmark regarding “what good looks like”, which can guide specifications for providers and ensure realistic allocation of resources to ADHD pathways.
- Policy-makers: Improved accuracy in ADHD diagnoses will advance the quality of population-based data which in turn has the potential to inform health strategies and allocation of budgets.
- Parents/caregivers, children, and teenagers: The guidance can educate parents and caregivers about ADHD and what to expect from an assessment. An ADHD assessment that follows these guidelines will increase confidence in the accuracy of an ADHD diagnosis and the value of a proposed management plan, empowering them to advocate for their child or teenager and participate meaningfully in their care.
Terminology
We are aware of the importance of clarity of language and the debates around terminology. We have used the UK NHS Digital Service Manual standards definitions of children and adolescents in this paper. These standards specify that a ‘child’ is aged between 4 and 12 years old and a ‘teenager’ is aged between 13 and 19 years old. We are also sensitive to individual preferences within autistic communities when referring to Autism Spectrum Disorder or Autism Spectrum Condition, and the use of identity versus person-first language.10 For the purposes of this paper, we will use ‘autistic individuals’ or “autism”.
Methods
The UK ADHD Partnership (UKAP)
Authors of this guideline are the UKAP executive committee members and guest authors who have worked with UKAP on consensus statements in the past. In total 16 authors, recognised as having extensive experience specialising in the assessment and treatment of ADHD in children and teenagers, were invited to contribute to this consensus. They represented a multidisciplinary panel of expertise working across a range of services and disciplines. Eight authors had medical qualifications/appointments (six child and adolescent psychiatrists and one paediatrician), five had clinical psychology qualifications/appointments and eight had academic qualifications/appointments. There was also representation by a service-user and an educational/occupational specialist.
The consensus group incorporated evidence from a broad range of sources. However, this largely reflects clinical practice, terms, and legislations in the United Kingdom, which may differ in other countries.
Development of CAAQAS
CAAQAS was developed through discussion of a series of agreed assessment-related questions and themes. These discussions used the UK NICE ADHD Clinical Guideline on “recognising, diagnosing and managing ADHD in children, young people and adults”7 which CAAQAS is designed to support. An iterative process was followed through drafting and redrafting, culminating in the formulation of a set of quality standards, or consensus statements, supported by all authors.
Seven key areas were agreed by all authors for ADHD assessments of children and teenagers, as follows:
- Setting the scene for the assessment ADHD.
- Minimum/essential standards for assessing and diagnosing ADHD.
- Reduced functioning or impairment required to make a diagnosis of ADHD.
- Common differential diagnoses and comorbidity.
- The information that should be included in the assessment report.
- The post-diagnosis discussion.
- The core competencies required to conduct a diagnostic assessment of ADHD.
Following email discussions about topics and content, an initial draft was circulated to authors for their review and comments, with the aim of achieving a broad consensus. Drawing on their clinical experience, each author submitted responses to the first draft; these were collated by the lead author and an amended second draft produced. Following a series of rigorous reviews of several iterations (including a video-conference), a final draft of CAAQAS was produced and authors came to an agreement by consensus, by approving the final version.
In developing this quality standard, CAAQAS identifies three levels of recommendations:
- Essential: These are non-negotiable. They include existing recommendations from the NICE guidelines and the application of DSM-5-TR or ICD-11 criteria.
- Highly recommended: These represent what the authors believe to be a minimum standard of quality care that should be followed in most assessments.
- Optional: These are highly desirable but not considered essential for practice.
At the end of each section, these are presented in a summary box of quality standard guidance for each topic.
No funding was requested or provided in preparation of this paper, and none of the authors were compensated for their time in any way. This study was not pre-registered, and no primary data was collected or analysed for this paper.
Results: Outcomes of the Expert Consensus on CAAQAS
Table 1 provides an overview of the structure of the manuscript.
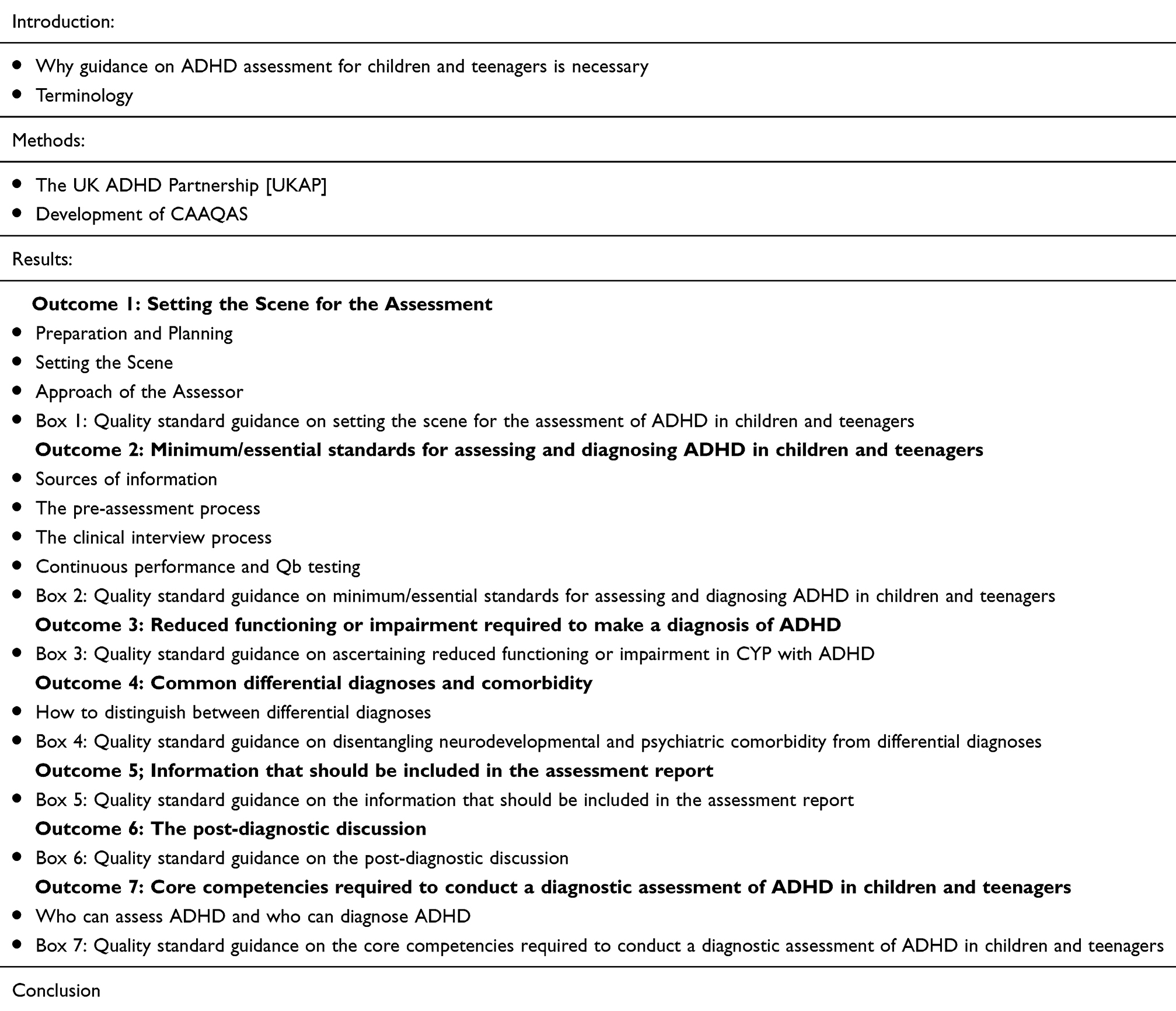 |
Table 1 Overview of Manuscript Structure |
Outcome 1: Setting the Scene for the Assessment
Preparing for a clinical assessment with a child or teenager requires careful planning and consideration to optimise its success. The aim of the assessment is for clinicians to gather the information necessary to inform interventions that will support the child or teenager’s well-being and development. Thorough preparation is essential and involves several factors, including carefully reviewing background information, selecting appropriate assessment tools, creating a conducive assessment environment, building rapport with the child or teenager and caregivers and explaining what will happen, and considering cultural and developmental factors.
Preparation and Planning
Obtain and review as much background information as possible about the child or teenager. This involves a “depth and breadth” approach, drawing on both longitudinal data (such as birth and early development records) and data from multiple systems (such as physical and mental health, educational, social services). It includes information obtained from the initial referral source, pre-assessment questionnaires, medical history, developmental milestones, family dynamics, any previous assessments or interventions, and any relevant education or social information. Any complex queries or clarifications that arise from this documentation should be dealt with prior to the interview.
Aside from the obvious need to assess the presence of ADHD symptoms, comorbidities, and potential differential diagnoses and impairment, it is helpful to consider whether any additional factors may need to be assessed, such as cognitive functioning, memory and other neuropsychological functions, social-emotional development, behavioural concerns, specific learning disabilities, intellectual disabilities, or other neurodevelopmental conditions such as autism. These assessments may need to be conducted by multidisciplinary professionals as required.
Ensure that appropriate assessment tools are selected taking age, developmental level, and presenting concerns into consideration. This may include standardised tests, observational measures, behaviour rating scales, and interviews with caregivers and teachers. Ensure that the selected tools are culturally and linguistically appropriate, and guidelines about their use are carefully followed.
Of note, legally, at least in the UK, mothers automatically have parental responsibility from birth, and fathers have parental responsibility if they were married to the mother or are named on the birth certificate. Step-parents may acquire parental responsibility through a court Parental Responsibility Order, and local authorities have parental responsibility for a child who is in care. Parental responsibility confers responsibility for a child’s wellbeing up to age 18. This responsibility persists even if the parents divorce, although it may be restricted by a court. Most divorced or separated parents continue to co-parent in a harmonious and child-centred way. However, when disagreements occur, parental consent for an assessment is only required from one person with parental responsibility11 (and none, if a child or teenager is competent to give this themselves).12
In terms of disclosure of the diagnostic assessment report, anyone with parental responsibility has a right to seek access to that child’s medical records, although a child or teenager may have capacity to decide if they want the records disclosed. There is no obligation to seek permission from or inform other holders of parental responsibility of a request for access to the records. However, doing so may allow them to explain any objection they may have. If there is third party information in the report, consent should be sought regarding sharing this information before disclosure. It may be necessary to anonymise or redact third party information if consent to share it is not given.13 It is recommended that advice is sought from an indemnity provider in such circumstances.
In most circumstances, offering both parents/caregivers the opportunity to contribute to the assessment (separately or jointly) is likely to be in the best interests of the child and will maximise the chance that the ultimate diagnostic opinion will be accurate and accepted.
Setting the Scene
The clinician needs to build rapport with parents/caregivers as well as the child or teenager. This is especially important with teenagers, who will be interviewed independently. To do this effectively it is important to clarify the parameters of the assessment, including specific goals and objectives, duration, format, and break times. This should preferably be done in advance by providing a standard pre-assessment information leaflet, but it could also be specified at the start of the session. This will help to manage everyone’s expectations and ensure they are reasonable.
The clinician must consider any obstacles that could prevent the child or teenager from fully participating in the assessment, including the fact that they can struggle to sit still or to see a motive for engagement. Determining why a child or teenager might be hesitant to engage can be difficult, but stigma, oppositionality, demand avoidance, and parental conflict about the value of the assessment should be considered. It is important to reassure children and teenagers that an assessment conducted for clinical purposes is confidential and that it is not a test that results in a “pass” or a “fail”. In cases of an assessment being undertaken as part of a court report, the individual and caregivers should be informed that the diagnosis may be disclosed more widely.
If the assessment is being conducted in-person, ensure the physical space is welcoming and comfortable. It should meet the needs of more restless children and teenagers who may wish to leave their seat, walk around, sit on the floor and/or play with toys. This can be agreed at the start of the assessment. Frequent breaks must be offered, if required. Minimise distractions and create a friendly atmosphere with age-appropriate toys, games, and activities available to engage the child or teenager and facilitate rapport-building.
If the assessment (ie the interview) is being conducted online (by video)14 check that the child or teenager is in a confidential place and cannot be overheard. Explicit acceptance should be expressed about periodic moving around if needed and/or for the use of fiddle toys. Younger children should be encouraged to bring a toy, book, blanket, etc to help them feel comfortable. Frequent breaks should be offered during online assessments. The assessor should explicitly ask teenagers to refrain from playing with their phones as this may not be visible onscreen. Provide explicit permission for children, teenagers, and caregivers to ask for information to be repeated and clarified (caregivers may be neurodivergent).
When engaging directly with a child or teenager (either online or in person) take time to introduce yourself, explain the purpose of the assessment using appropriate language, and establish trust and rapport through friendly interaction and active listening. Encourage children and teenagers to ask questions and express any concerns they may have. It can be helpful to ask why they think they are being assessed and what the outcome might be (for example, is the assessment perceived to be a punishment or a “last chance” before something else happens). It is important to clarify that the assessment will discuss differences and difficulties and that this is not a reflection of their faults. Explain that the assessment will also explore their strengths (ie, emphasise that it is not just a deficit focused assessment). Importantly, set up expectations of the assessment process (eg sometimes more than one appointment may be required) and the outcome process (ie whether the diagnostic outcome will be fed back at the end of the assessment or whether this will be fed back in a separate appointment).
The well-being of the child or teenager and their relationship with their caregivers is the top priority. Therefore, if the child or teenager becomes distressed, refuses to participate and/or demands to leave, then they should not be asked to continue.
Approach of the Assessor
Due to the chronicity of ADHD and the potential need for further appointments, a positive first appointment will encourage the child or teenager to attend future appointments. Approach the assessment with empathy and warmth, demonstrating genuine interest in the individual’s and family’s well-being. The use of neuro-affirming language, together with a compassionate and non-judgmental tone, will create a safe space for everyone to express themselves.
Every child and teenager is unique and may require different strategies for engagement, so it is important to be flexible and adaptable. The clinician should tailor their communication style and assessment techniques to suit the child’s or teenager’s individual needs and preferences. Be mindful of cultural differences and developmental considerations that may influence the assessment process and interpretation. It is also important to be mindful of the heritability of ADHD and other neurodevelopmental conditions when working with parents/caregivers. It is possible that the informants may also have characteristics of ADHD and/or other neurodevelopmental or mental health conditions.
Whilst engaging child or teenager and caregivers in a friendly and open demeanour, it is essential to maintain professionalism and integrity in all interactions. Obtain informed consent from the caregivers (and where appropriate, the child or teenager) and consider confidentiality and privacy regarding assessment outcome.
Box 1: Quality Standard Guidance on Setting the Scene for the Assessment of ADHD in Children and Teenagers
1.1 Manage the expectations of the interviewees by “setting the scene” and providing an overview of the assessment process. This could be sent out in advance or be given at the beginning of the assessment [essential].
1.2 In advance of the assessment obtain and review background and other relevant information (eg pre-assessment questionnaires, school and medical reports) from multiple sources, as appropriate [essential].
1.3 If required, select appropriate validated assessment tools for administration during the assessment taking account of age and developmental level [highly recommended].
1.4 Consider obstacles to engagement, reassure confidentiality (where appropriate), allow periodic movement, minimise distractions where possible, and offer frequent breaks [essential].
1.5 Be flexible and adaptable in engagement strategies, tailor communication style and assessment techniques to the individual child’s or teenager’s needs and consider cultural and developmental differences [essential].
Outcome 2: Minimum/Essential Standards for Assessing and Diagnosing ADHD in Children and Teenagers
Presently, there are no biomarkers, cognitive, or neuroimaging tests with sufficient specificity and sensitivity to diagnose ADHD.15 This is also the case for other mental health conditions. Therefore, we are reliant on the systematic collation of information to inform our diagnostic decision. It is widely recognised that when assessing ADHD in children and teenagers, a comprehensive semi-structured diagnostic interview should be administered to explore their clinical and behavioural presentation and associated difficulties,16 along with background developmental, medical, family, and social histories, and mental state and risk assessments. The assessment should include information from educational settings and other supplementary information.
Sources of Information
The primary interviewee must have had a close relationship with the child or teenager for a considerable time (ie, from pre-school period onwards) and be familiar with their functioning in different settings. Usually, this is a parent, caregiver, or family member (in the latter case the person must be older than the child/teenager). If it is not possible to interview someone who has known the individual for a considerable amount of time (eg in the case of an adopted or looked after child or teenager), current information can be gleaned from an informant and/or historical information from alternative sources, such as school and/or social services (if possible). When working with an interpreter, it is important to specify that an accurate translation from language to language is required, not an “interpretation” which may change the meaning.
The clinical interview should include a joint discussion with the interviewee/primary carer and the child or teenager, as well as separate discussions on their own (both ensuring privacy). The separate meetings allow for the carer’s and the child or teenager’s respective perspectives to be explored without either party being concerned about upsetting each other. This approach can facilitate open discussions about difficult topics without the potential for aggravating family relationships that may already be fraught.
It is important to enquire whether both/all of the child or teenager’s parents/caregivers hold the same view that ADHD could be a possible explanation for their difficulties. If different views are held (especially if one parent/carer is strongly opposed to a possible diagnosis of ADHD) it is necessary to explore the option of speaking to both parents/caregivers (separately or together) to enable both perspectives to be fully considered. Each parent’s/caregiver’s perspectives will be based on their familiarity with the child or teenager and the contexts in which they observe them.17,18 Variation between parental/caregiver’s perceptions regarding symptoms is not uncommon, especially for inattentiveness and less externalizing symptoms.19–21
It is essential to understand whether there are any other contextual factors that may be influencing parental perspectives of difficulties or motivations for participating (or not) in the ADHD assessment process, eg perceived stigma, child residency disputes, and allegations about parenting abilities.
Consideration of all available information will be needed to inform clinical judgment regarding whether any informant discrepancies may reflect true contextual and situational differences in symptom expression or are likely to be a consequence of perceptual differences.
In most circumstances, offering both parents/caregivers the opportunity to contribute to the assessment (separately or jointly) is likely to be in the best interests of the child and will maximise the chance that the ultimate diagnostic opinion will be accurate and accepted.
It is important to observe the child or teenager’s behaviour and to assess their mental state. However, the assessor should be aware that a cross-sectional presentation in an unfamiliar setting (such as the assessment environment) may not reflect their usual behaviour. In some cases, an additional observation of the child or teenager in an educational setting may be required. A generalised protocol may be utilised, such as a functional assessment of behaviour, as there are no validated observations for use in children or teenagers with ADHD. Independent evidence should be obtained from previous and current educational settings (eg, teacher questionnaires and/or interview, school/SEN reports, examination results). Children and teenagers in secondary schools and colleges typically have several teachers, and their behaviour may vary across subjects. Therefore, reports and questionnaires should be obtained from someone with an appropriate overview (such as the school SENCo and/or personal tutor) and/or from several teachers. If the child or teenager is not in education, an alternative professional who knows them well may be available to provide relevant information.
If a child or teenager has had previous contact with mental health services, it is good practice to review clinical records, including GP letters, previous assessment and medico-legal reports. Additional reports from social services, practitioner psychologists, psychotherapists, and occupational therapists can be helpful. This can be time-consuming but essential for children and teenagers presenting with greater complexity.
The Pre-Assessment Process
Rating scales are commonly used in services to screen for ADHD symptoms (eg, 18-point ADHD symptom scales). These scales assess the frequency of symptoms, not severity. They typically consist of a list of leading questions that follow a closed-question format (ie, yes or no answers, or a Likert scale). Most are not standardised by sex and may under-represent ADHD symptoms among those with more internalised presentations. A meta-analysis conducted by Mulraney et al22 concluded “most tools have excellent overall diagnostic accuracy as indicated by the area under the curve (AUC). However, a single measure completed by a single reporter is unlikely to have sufficient sensitivity and specificity for clinical use or population screening”. For these reasons, there have been concerns about the reliability of rating scales (especially if they are being used as a triage system to exclude people from services). The consensus group agreed that rating scales are helpful for monitoring treatment, but they should not be used as diagnostic screening tools unless supplemented with qualitative information about symptoms.
If used for screening purposes, it is essential that rating scales are supplemented with qualitative information, by giving a narrative and/or specific examples of difficulties and impairment associated with ADHD symptoms. These can be completed by parents/caregivers, teachers, and self-reported by teenagers (if appropriate). Pre-assessment information can also be used to elicit background information and current concerns, which can help to shorten the length of the clinical interview. However, this should not replace a comprehensive clinical interview. In cases where there is a lengthy gap between initial screening and appointment for assessment (eg, six months or more), the pre-assessment process needs to be repeated.
It is not unusual for information about the frequency and severity of ADHD symptoms to differ between respondents. For example, the child or teenager may behave differently when they are expected to settle, focus, and learn in a noisy class environment (especially when they lack interest in the subject) compared with when they are engaged in selected activities of interest in a more unstructured home environment. However, if differences are substantial, the clinician needs to carry out a more extensive and in-depth exploration of the evidence to try and resolve the conflicting data. As discussed above, this may require obtaining more information from other caregivers (eg, the other parent who was not present at the interview or other relatives who have a substantial care giving role). If the uncertainty relates to school information provided by one teacher (eg, the SENCo), additional direct feedback can be sought from subject teachers.
One important consideration will be to identify whether specific adjustments (strategies) are being applied by parents/caregivers and/or teachers to minimise impairments and/or optimise achievement. A further consideration may be whether the child or teenager is camouflaging or masking their symptoms; they are more likely to do this at school rather than at home (eg to “fit in”, to avoid being criticised).23 However, varying presentations across different contexts should not automatically be attributed to camouflaging. This possibility should be explored with the individual to determine whether there is evidence to support this explanation.
The Clinical Interview Process
The assessment must be conducted in face-to-face format (preferably “in person”). As direct observations during the assessment are important, purely audible format should not be used. Given recent advances in technology and a shift to remote communication during COVID-19, interviews with parents/caregivers or family members can be conducted online. However, an individual’s preference for “in person” appointments should be accommodated where possible or necessary for clinical reasons. It is important to record whether the child or teenager has taken any prescribed medication on the day of the assessment which may impact on their engagement.
For video-based online assessments, the clinician should satisfy themselves that the format affords sufficient opportunity to observe the child or teenager. The clinician should be mindful of the possibility of atypical presentation in unfamiliar settings, and a lack of observable ADHD symptoms during the assessment should not automatically lead to exclusion of a diagnosis of ADHD. Additional formal “in person” observations of the child or teenager at home, in class or alternative settings (if not in education) may be required, especially when assessing younger children. The observation should include activities that have the potential to elicit the presence of ADHD symptoms.
The clinical assessment should be undertaken using a semi-structured clinical interview (such as the ADHD Child Evaluation)24 to systematically evaluate the presence or absence of each of the 18 DSM-5-TR or ICD-11 symptoms. Several symptoms must have been present by age 12 and must be pervasive and persistent (ie, they must occur across settings over time). The interview should be a systematic qualitative enquiry about the presence of symptoms using open questions, with specific examples to illustrate difficulties. It is also helpful to ask about any adjustments that have been made to manage or prevent problems. These adjustments might include compensatory strategies applied by the child or teenager or by the people around them (eg, family, school, or occupational). Sufficient information needs to be obtained for the assessor to make a clinical judgment on whether a core symptom of ADHD is present or absent; this should not rely on the sole endorsement of prescribed categories (eg yes, no, never, sometimes, often). In addition, symptoms are required to be associated with significantly reduced functioning or impairments across social, educational, and/or occupational domains compared with the average neurotypical child or teenager of the same age.
It is important to be mindful of potential sex differences; a recent meta-analysis25 comparing severity of ADHD symptoms in males and females found that rating scale data (predominantly drawn from community samples) indicated that girls present with significantly less severe hyperactivity/impulsivity symptoms than boys. In adulthood, men were rated to have significantly more severe inattention than women with no difference in the hyperactivity/impulsivity dimension. All significant differences were of small effect size. By contrast, there were no significant differences between sexes when they were assessed using clinical diagnostic interview data. Hence, rating scale data suggests that ADHD symptoms present differently in males and females, whereas there is no significant difference when they are assessed by a clinical interview which is likely to be a more comprehensive and reliable method. While there is heterogeneity between sexes and age (with hyperactivity reducing as children and teenagers get older), the assessor must identify a number of core symptoms that are “trait-like” rather than episodic, the latter reflecting change from a pre-morbid baseline (such as an episode of depression in adolescence) rather than ADHD.
Due to developmental differences in key skills, it is essential that clinicians are familiar with realistic expectations of different age and ability ranges. Symptoms may vary throughout the day, depending on the individual’s ‘level of interest in the task and the task demands. Children and teenagers may learn strategies to compensate for their ADHD symptoms, making them less salient behaviourally. When assessing individuals with suspected or diagnosed intellectual disability, clinicians must be aware that rating scales are not usually normed on this population.
A detailed physical and mental health history must be obtained, as this information will be used to evaluate whether the presenting symptoms may be better explained by another condition. This requires a good understanding of both ADHD and overlapping conditions. This will include the individual’s ‘developmental history and possible early risk factors (use of alcohol/prenatal alcohol exposure, illicit drugs during pregnancy, birth complications, premature birth, low birth weight, developmental milestones, early temperament, and experiences of childhood adverse life experiences and trauma). There may be some instances when this information is not available, such as for children and teenagers in care.
It is essential to enquire about the child or teenager’s history of existing physical health conditions that may mimic (eg, thyroid disorders, epilepsy, sleep apnea, iatrogenic effects of medications such as corticosteroids, substance misuse) or be comorbid (eg obesity, heart disease, epilepsy, or diabetes, obesity, asthma).26–28 Additionally, enquiring about any vision or hearing issues is crucial for the differential diagnosis.
Enquiries must be made regarding the child or teenager’s current mental state, mental health, intellectual functioning, learning difficulties, and neurodevelopmental conditions. The latter includes autism, tic disorders, dyslexia, dyscalculia, and dyspraxia/developmental co-ordination disorder. Clinicians should also enquire about adverse childhood events, protective factors, and symptoms of trauma (PTSD, complex PTSD). Due to the impact on education and understanding, enquiries should be made about receptive or expressive language difficulties.
The assessor should specifically enquire about the risk of harm to self or others or harm from misadventure. Topics of enquiry may include antisocial behaviour, aggression, deliberate self-harm, substance use, sexual health, and victimisation/exploitation. Risk in both physical and digital contexts should be considered. The risk assessment should document the nature of the risk, precipitating, perpetuating, and protective factors, and a risk management plan.
NICE Guidelines recommend that a baseline physical assessment should be conducted before starting medication, hence medical practitioners may include this in their diagnostic assessment. This should involve a review of physical health (including centiles to aid interpretation) including height, weight, pulse, blood pressure, and heart rate. As sensory organ deficits can impair academic and social functioning, they should enquire about hearing and visual acuity and advise parents/caregivers to discuss any suspected problems with their GP and/or optician.
Continuous Performance and Qb Testing
To date, no guidelines have recommended continuous performance tests (CPTs) (including the Qb Test, which combines a CPT with a motion track system) to be an essential component of the assessment process. A meta-analysis of studies of commercially available CPT concluded:
At the clinical level, CPTs as a stand-alone tool have only a modest to moderate ability to differentiate ADHD from non-ADHD samples. Hence, they should be used only within a more comprehensive diagnostic process.29
Regarding more specifically the Qb Test, a meta-analysis30 concluded that
When used on their own, Qb Test scores available to clinicians are not sufficiently accurate in discriminating between ADHD and non-ADHD clinical cases. Therefore, the Qb Test should not be used as stand-alone screening or diagnostic tool, or as a triage system for accepting individuals on the waiting-list for clinical services. However, when used as an adjunct to support a full clinical assessment, QbTest can produce efficiencies in the assessment pathway and reduce the time to diagnosis.
Of note, there is no evidence for the Qb Test or other devices to be used as a tool to monitor treatment response.
The literature on other neuropsychological tests, delivered mainly via digital technologies, has recently been comprehensively reviewed by NICE. With the exception of the QbTest, which is indicated as an option to support the diagnostic process in children, other tests (ie, EFSim Test, EFSim Test Web Version, Nesplora Attention Adults Aquarium, Nesplora Attention Kids Aula, QbCheck), as well as the QbTest in individuals aged 18 years and over are not endorsed by NICE in the diagnostic process for ADHD due to insufficient evidence.31
Box 2: Quality Standard Guidance on Minimum/Essential Standards for Assessing and Diagnosing ADHD in Children and Teenagers
2.1 There are many pre-assessment (baseline) rating scales that focus on the individual’s presenting problems and it is for the clinician to decide which they prefer. Rating scales are helpful for monitoring treatment, but they should not be used as diagnostic screening tools unless supplemented with qualitative information about symptoms [highly recommended].
2.2 Pre-assessment questionnaires that ask for qualitative information and provide specific examples of difficulties associated with core ADHD symptoms are helpful and can reduce the time required for the interview, eg the ADHD Child Evaluation v.2 self and informant questionnaires24 [highly recommended].
2.3 If there is a lengthy gap (ie 6 months or more) between initial screening and the assessment, the pre-assessment process should be repeated [highly recommended].
2.4 Validated questionnaires for co-morbidities are helpful to screen for other mental and physical health disorders [optional].
2.5 The clinical interview must be conducted in face-to-face format (preferably “in person”). Given recent advances in technology and a shift to remote communication during COVID-19, interviews with parents/caregivers or family members can be conducted online. However, an individual’s preference for an “in person” appointment should be accommodated where possible or necessary for clinical reasons [highly recommended].
2.6 Medical practitioners must include a baseline physical assessment for diagnostic purposes and before starting medication. This should include measures of height, weight, pulse, blood pressure, heart rate. The physical examination should be carried out in person [essential].
2.7 Information gathering: all relevant information obtained during the assessment needs to be noted in detail and includes specific examples [essential].
2.8 Where there is missing information or conflicting data between informants, this should be explored. This may reflect adjustments being made in the home and/or school setting to minimise presenting problems, differing thresholds for concern among informants, or differing attitudes of informants towards the value of diagnostic labels. Divorced or separated parents/caregivers can give different accounts and discrepancies need to be understood [highly recommended].
2.9 A systematic evaluation must be undertaken of each ADHD symptom and additional diagnostic criteria using a comprehensive and systematic approach. If a symptom is identified as occurring “often”, it is essential to elicit and document clear examples of this, along with and any adjustments being made (by the individual, family, and/or school) to avoid or prevent difficulties [essential].
2.10 Consider the degree of impairment associated with each symptom present and evaluate this against what would be expected of a typically developing young person of the same age [essential].
2.11 Assessment must employ a semi-structured clinical interview eg the ADHD Child Evaluation [ACE];24 Young-DIVA;32 K-SADS-PL33; MINI34. Alternatively, an experienced ADHD assessor may follow an interview style that follows diagnostic criteria, ensuring that all 18 symptoms, impairments, and additional criteria are fully explored. Leading questions must not be used [essential].
2.12 Assess ADHD specific developmental history and early risk factors. There may be some instances when this information is not fully available, such as for children or teenagers in care [essential].
2.13 By clinical enquiry or direct observation, consider other possible neurodevelopmental conditions and learning difficulties. Document concern and consider further investigation [essential].
2.14 Assess education and social history: academic progress, exclusions/expulsions, behaviour in class, peer group relationships, antisocial behaviour, personal relationships [essential].
2.15 Assess current mental state together the individual’s mental health history to identify common mental health problems/disorders (both current and previous), particularly those that can mimic ADHD, or are commonly comorbid with ADHD (eg anxiety, depression, obsessional compulsive disorder, conduct disorder, eating disorder, attachment disorder, substance use, self-harm) [essential].
2.16 Assess physical health history to identify any history of existing medical conditions (eg heart disease, diabetes, epilepsy, head injury) and common comorbidities such as obesity, asthma, hypermobility. Ask directly about sleep, vision, or hearing issues. Enquire about current and past medications and medication allergies [essential].
2.17 Assess risk, including risk of harm to self, to others, from others and/or harm from misadventure. Enquire about adverse childhood events, protective factors, and symptoms of trauma [essential].
2.18 Triangulate different perspectives: gather information from two or more sources (parents/caregivers, collateral information from educational, healthcare and/or social services reports, clinical and/or school observation) [essential].
2.19 The clinician must document whether or not they observed ADHD symptoms and/or other features (eg depressed affect, anxiety, tics) during the assessment whilst being mindful that symptoms may be less apparent in an atypical situation. Notably, the lack of observable ADHD symptoms during the assessment should not automatically lead to an exclusion of a diagnosis of ADHD [essential].
2.20 Additional formal “in person” observations’ of the child or teenager at home, in class or alternative settings (if not in education) may be required, especially when assessing younger children. The observation should include activities that have the potential to elicit the presence of ADHD symptoms [optional].
2.21 Continuous performance tests should not be used as stand-alone screening or diagnostic tools, or as a triage system for accepting individuals on the waiting-list for clinical services. They may be helpful when used as an adjunct to support a full clinical assessment [optional].
Outcome 3: Reduced Functioning or Impairment Required to Make a Diagnosis of ADHD
Symptoms of ADHD can interfere with or reduce the quality of the child or teenager’s academic, social, and/or occupational functioning, highlighting the importance of early intervention and support to address unique needs and challenges.35 Hence, diagnosing ADHD is not solely a matter of assessing the presence of ADHD symptoms; their severity and impact on daily functioning must be considered.
ICD-11 specifies that symptoms must be sufficiently severe that they have a direct negative impact on academic, occupational, or social functioning, referred to as “impairment” in DSM-5-TR. How to establish “impairment”, however, is not clearly defined. It can be helpful to consider whether some form of intervention is warranted. NICE Guidelines6,7 suggest that impairment from symptoms of ADHD should be at least of moderate severity and fall across at least two domains or settings based on interview and/or direct observation. The Weiss Functional Impairment Rating Scale – Parent Report or the Vineland-3 are helpful tools to support this assessment.36,37
ADHD symptoms exist on a spectrum within the broader population, with many individuals displaying some degree of these traits. Therefore, this is not a “one-size-fits-all” process. Children and teenagers with ADHD can present with a wide range of symptoms and levels of impairment, manifesting in various ways across multiple areas of life, including school behaviour and academic performance; extra-curricular, leisure and social activities; family and peer relationships; risk-taking behaviours (often associated with emotional and behavioural dysregulation), daily tasks, and psychological functioning (eg self-image and self-esteem). Clinicians should be mindful that the child or teenager’s experiences may be influenced by various factors, including individual differences, co-occurring conditions, and environmental factors.
It is crucial not to dismiss the possibility of ADHD solely based on high achievements in specific areas, such as academic success or “islands of excellence”. Some might label such individuals to have intellectual strengths, sometimes referred to as a “high-functioning” with ADHD, but this term can overlook significant challenges and burdens they face in other domains. Despite apparent success, the child or teenager may still be underperforming compared to their potential, with other areas of impairment being overshadowed by an islet of achievement. These could include struggles with social interactions, disruptions in family life, sleep disturbances, emotional dysregulation, or internalising symptoms such as a lack of confidence, low self-esteem, and heightened stress levels. Furthermore, the area of achievement may require the individual to exert substantial effort to sustain attention, suppress hyperactivity, and regulate their impulsivity leading to performance being maintained in one domain of life at the cost of fatigue, decompensation, and/or accentuation of symptoms in other domains. In turn, this may also lead to secondary mental and physical health challenges.
Family accommodations can inadvertently mask impairment in the functioning of children and teenagers with ADHD in several ways:
- Compensatory Strategies: Families may develop compensatory strategies to help the individual cope with their ADHD symptoms. These strategies could include providing constant reminders, structuring routines, or simplifying tasks. While these accommodations can temporarily alleviate some difficulties, they may also obscure the true extent of the child or teenager’s impairment by artificially smoothing over challenges.
- Overcompensation: In efforts to support the individual, families might overcompensate by taking on responsibilities that the child or teenager would otherwise be learning to manage independently. For instance, parents/caregivers might excessively monitor homework completion or organise their belongings. This overinvolvement can mask the child or teenager’s struggles and delay their development of essential skills for independent functioning.
- Normalisation of symptoms: Over time, families may become accustomed to the child or teenager’s ADHD symptoms and adjust their expectations accordingly. Behaviours that would typically be seen as problematic or indicative of impairment may be perceived as normal within the family context. This normalization can lead to a lack of recognition of the individual’s ongoing difficulties in other settings, such as school or social environments. Other family members may also have ADHD, rendering the child or teenager’s challenges normative within the family, which may lead to underreporting during assessment.
Overall, while family accommodations and adjustments are often well intentioned and can provide valuable support for a child or teenager with ADHD, they can also inadvertently obscure the true extent of impairment, making it challenging to accurately assess and address the individual’s needs.
Socio-cultural norms and environmental factors can also mask ADHD. For example, hyperactivity and impulsivity may be channelled through culturally normative activity (eg, a very active outdoor or rural lifestyle, hyperactive-led practical task responsibilities; impulsive-led antisocial behaviour, or nomadic lifestyle). In such instances, family may not report any “unexpected” levels of impairments or consider the individual to be more impaired than their peers, and the assessor may need to focus on how symptoms manifested earlier in childhood when the child or teenager was not embarking on such normative activities (eg during sedentary periods or periods of solitude). In the modern age, much of childhood and adolescence is being lived “digitally” and academic, social, and emotional functioning (including impairments) may play out through digital activity. Therefore, it is important to explore proxies of hyperactivity, impulsivity, and inattention or attention regulation challenges within digital spaces.
Box 3: Quality Standard Guidance on Ascertaining Reduced Functioning or Impairment in Children and Teenagers with ADHD
3.1 The interviewer should obtain specific examples of how core ADHD symptoms have interfered with or reduced the quality of the individual’s functioning across psychological, social, academic, and/or occupational functioning. This should include the exploration of digital activity [essential].
3.2 Impairment should be of at least moderate severity and in at least two domains or settings. It can be helpful to consider the following areas: school behaviour and academic performance; extra-curricular, leisure and social activities; family and peer relationships; risk taking behaviours (often associated with emotional and behavioural dysregulation), daily tasks, and psychological functioning (eg self-image and self-esteem) [essential].
3.3 When assessing impairment, be mindful that high achievements in specific areas and/or family support and accommodations may obscure impairments. Compensation by the individual, as well as socio-cultural and environmental norms that channel ADHD symptoms, may also mask impairments [highly recommended].
Outcome 4: Common Differential Diagnoses and Comorbidity
When assessing for possible ADHD, it is essential to consider other disorders which may “mimic” ADHD. These disorders may provide a better explanation for the child or teenager’s presentation than ADHD. (For a list of the range of conditions that can mimic ADHD symptoms of inattention, hyperactivity, and impulsivity see38).
Complexity can arise because these same disorders can also co-occur with ADHD and need to be identified and managed alongside ADHD. Early identification and intervention for comorbid conditions can help mitigate their impact on developmental trajectories and improve overall outcomes for individuals with ADHD. A comprehensive approach (which may require multi-disciplinary input) that accurately assesses for ADHD and comorbidities is essential. Conditions that must be considered within an ADHD assessment in children and teenagers include:
- Disruptive behaviour and dissocial disorders: Most commonly seen in males, children, and teenagers with ADHD often exhibit Oppositional defiant behaviours and/or Conduct-dissocial disorder. These conditions involve persistent patterns of disobedience, hostility, and aggression toward authority figures or peers.
- Anxiety Disorders: Worry, fear, distractibility, and restlessness can be symptoms of anxiety, but may be misattributed to ADHD and/or exacerbated by inappropriate stimulant treatment. Therefore, anxiety-related disorders (including Obsessive-compulsive disorder and Post-traumatic stress disorder) need to be considered as possible differential diagnoses as well as common comorbidities.
- Trauma: Early trauma can impact children and teenager’s development and presentations including their capacity to attend and engage. Trauma associated anxiety, hypervigilance, and the presence of fight/flight responses can mimic restlessness and impulsivity.
- Mood Disorders: Depression and (to a lesser extent) bipolar disorder may present as a persistent sadness, irritability, mood swings, and changes in energy levels, further impacting emotional well-being and functioning. They may also be associated with difficulty concentrating, impulsive behaviour, and excessive reward seeking. However, mood disorders are typically episodic compared to ADHD.
- Developmental Language Disorders: This is a condition where children and teenagers have long-term challenges talking and/or understanding words. They may have lots of ideas but find it hard to put their ideas into words and understand what other people say to them. Receptive processing problems can produce inattention.
- Learning Difficulties: Individuals with ADHD often struggle with academic performance and may have specific learning difficulties, such as dyslexia or dyscalculia. These can exacerbate the challenges associated with ADHD and require targeted interventions to address them. Those who have a significant discrepancy in their verbal-performance intellectual abilities (where verbal skills are superior to performance skills) are sometimes thought to have ADHD as they appear to be presenting with inexplicable academic underperformance (eg, bright and chatty in class but poor on written work).
- Intellectual Disability: A more generalised intellectual disability characterised by a Full Scale IQ of 70 and under plus adaptive skills difficulties can present alongside or mimic ADHD.
- Weak Cognitive Executive Function: Working memory and executive functioning problems (eg “scratchpad memory”, defining goals, setting priorities, task planning, initiation, evaluating progress, self-organisation, and time management) can exist independently of (and mimic) ADHD, especially in children and teenagers with brain injury or autism.
- Sleep Disorders: Poor quality sleep can cause inattentiveness, irritability, and restlessness and should be considered as a possible differential diagnosis. However, sleep problems, such as insomnia, restless leg syndrome, or sleep-disordered breathing, are commonly reported in individuals with ADHD. Disrupted sleep patterns can exacerbate ADHD symptoms and impair cognitive functioning, attention, and behaviour during the day.
- Substance Use Disorders: Teenagers with ADHD are at increased risk of developing substance use disorders,39 including alcohol and substance abuse. Impulsivity, risk-taking behaviour, and difficulties with self-regulation contribute to this heightened risk. Substance use can also mask ADHD symptoms, and withdrawal symptoms can be mistaken for ADHD symptoms. Therefore, it is inadvisable to conduct an assessment with a young person who is thought to be under the influence of substances or withdrawing from substances. The interplay between substance use and ADHD symptoms is important to consider during assessment. For example, some forms of substance use may appear to temporarily improve cognitive functioning and reduce agitation, masking the ADHD challenges and making the intoxication less apparent. Substance use in the long-term can impact cognitive functioning and hence exacerbate ADHD symptoms.
- Foetal Alcohol Spectrum Disorder: FASD remains the single most common aetiological cause of damage to the developing foetus.40 This is especially true in populations such as those in care.41 The complex interplay between the prenatal lifestyle of parents, especially the mother, pregnancy-related impact on the developing brain and body, alongside the postnatal traumas experienced, all increase the predisposition to ADHD. The profile, however, is not typical of other cases of ADHD. An inattentive/impulsive subtype is more common, with associated cognitive and communicatory challenges. Identifying the condition, both in terms of diagnosis and delimiting complexity of presentation, and also changes to management approaches, it is important to consider this common aetiological factor as explaining the variability in profile and medication response.42
- Autism: Social communication challenges associated with autism, as well as pre-occupying interests and sensory sensitivities, can give rise to impairments or differences in interaction, motivation, focusing and learning, and/or trigger agitation. Sensory-motor features of autism may also lead to repetitive or stimulation-seeking motor behaviours. These can all accentuate the attentional regulation and hyperactivity/restlessness symptoms of ADHD and/or be mistaken for ADHD. Social and sensory challenges associated with autism can also contribute to behavioural difficulties and affect the individual’s ability to regulate their emotions and behaviours. Autistic children and teenagers may find some environments intensely anxiety-provoking and exhausting and may engage in externalising behaviours in order to release tension that feels unbearable, or else to engineer removal from the distressing environment. Children and teenagers with comorbid ADHD and autism often present with substantially greater complexity, with autism and ADHD each accentuating the impairments of the other. Inversely, autism and ADHD may also reciprocally mask one another, for example, by creating a need for novelty interspersed with a need for predictability/sameness, and by creating intense sustained focus on some detailed tasks interspersed with difficulty paying attention to other tasks. Abilities generated by each condition may also be used to mask the impairments generated by the other (eg, ADHD-related social impulsivity may over-ride autism-related anxiety in social situations; an autism-related need to adhere to rules may lead an individual to exert sufficient effort to overcome inattention and suppress hyperactivity associated with ADHD). Finally, ADHD may interact with autism to manifest in a hybrid way. For example, the impulsivity and novelty-seeking of ADHD could manifest within the realm of intense interests related to autism, resulting in risky and stimulation-seeking perseverative interests. The co-existence of autism and ADHD often necessitates comprehensive assessments and interventions tailored to the unique strengths and support needs brought about by the interaction and the reciprocal impact of the two neurodevelopmental conditions.
While modern influences like gaming and social media offer opportunities for learning and socialization, they also pose risks to children and teenager’s cognitive, social, and emotional development due to their pervasive nature and immersive characteristics. They can affect cognitive development, socialisation, emotional regulation, sleep patterns, and influence risk-taking behaviour.
While some comorbidities may be common across both age groups, there are differences in comorbidity patterns between young children and teenagers with ADHD. In younger children, common comorbidities include autism, developmental language disorder, oppositional defiant disorder (ODD), conduct-dissocial disorder (CDD), intellectual disabilities and other specific learning difficulties, sensory processing difficulties, anxiety disorders, and sleep disturbances.
As children with ADHD transition into adolescence, the pattern of comorbidities may shift. The assessor should be mindful that children and teenagers are still developing which means they can grow in and out of problems. Teenagers may or may not continue to struggle with oppositional behaviour and conduct problems. However, the nature and severity of these challenges may evolve as they navigate the demands of adolescence, including peer relationships, academic expectations, and increasing independence. Mood disorders may emerge or become more pronounced during this developmental stage. Hormonal changes generated by puberty may also interact with ADHD symptoms and self-regulation. Substance use disorders may emerge during adolescence, as young people are at increased risk of engaging in risky behaviours and substance experimentation. Later, adolescence may also bring with it a loosening of external structures, where the individual leaves school or attends college and university where they are required to rely increasingly on their self-organisational skills and executive frontal abilities. Therefore, different developmental challenges may impact ADHD and the manifestation of such impact.
How to Distinguish Between Differential Diagnoses
Assessing children and teenagers for ADHD while considering both differential diagnoses and comorbidities presents a multifaceted challenge. The transdiagnostic nature of inattention, impulsivity, and restlessness provides the first issue. The obscuring effect of comorbidities provides the second issue, as symptoms may intertwine or exacerbate each other, leading to diagnostic ambiguity. To address this, clinicians need to conduct thorough assessments, considering the individual’s symptom presentation, developmental history, and family context to untangle overlapping symptoms and identify underlying conditions accurately. Variability in symptom severity and expression among children and teenagers with ADHD poses a further challenge. Symptoms may manifest differently across individuals and fluctuate in intensity over time, making it difficult to establish a clear diagnostic threshold.
As multiple conditions interact with each other in complex, non-linear ways, it is not solely an issue of formulating “primary” and “secondary” conditions, it is important to understand the presenting problems and how they interact. A “primary” condition typically manifests first or co-occurs with ADHD symptoms from an early age; it is typically associated with significant impairment in specific domains of functioning. “Secondary” conditions may develop later, in response to or as a consequence of ADHD symptoms. However, a condition may have chronological primacy (such as autism) but not functional primacy in terms of the distress they may cause (eg depression). Response to treatment may be a further consideration. Primary conditions often require targeted interventions specific to their underlying pathology, whereas secondary conditions may improve or resolve with effective management of ADHD symptoms. However, it can be hard to assess the effectiveness of ADHD treatment when other untreated disorders are present.
ADHD may mimic other conditions, and vice versa. To delineate which conditions are present, it is important to explore the subjective “experience” of the symptom or presentation, as well as the context and triggers. For example, distractibility (as with all ADHD symptoms) may be driven by ADHD as well as a number of other conditions. Where an individual is describing difficulty concentrating, the assessor may explore the triggering context (eg a more rewarding/novel stimulus in the room triggering distractibility away from a low-stimulation, under-arousing task) and subjective experience (eg the under-arousing task being experienced as boring, agitating, and difficult to hold attention on, and then attention wandering and being snagged by a more mesmerising, novel, arousing stimulus). This ADHD feature may be mimicked by other conditions, such as when attention is difficult to sustain on a task due to anxiety, interest, negative ideation, intrusive thoughts, hypervigilance, attachment fears, pain, or anaemia. In such a scenario, exploring the experience and triggers to attention wandering can assist with differential diagnosis between ADHD and anxiety, depression, OCD, PTSD, attachment disorders, and/or physical health conditions.
Box 4: Quality Standard Guidance on Common Differential Diagnoses and Comorbidity
4.1 Assess current mental state and take a detailed developmental history, enquiring about, mental health and neurodevelopmental conditions, lifestyle risk, and family history. The information should be used to evaluate whether the presenting symptoms may be better explained by another condition. This requires a good understanding both of ADHD and overlapping conditions, an awareness of normal parameters for symptoms (attention, restlessness, impulsivity) at different developmental stages and for the cultural background of the individual being assessed [essential].
4.2 Assess for common comorbidities include disruptive behaviour and dissocial disorders, anxiety disorders, mood disorders, learning disorders, autism, sleep disorders, and substance use disorders [essential].
4.3 Be aware of the impact of modern influences like gaming and social media on cognitive, social, and emotional development, and consider their role in mimicking ADHD symptoms or exacerbating or masking comorbid conditions in individuals with ADHD [highly recommended].
4.4 Recognise differences in comorbidity patterns between young children and teenagers with ADHD, understanding that comorbid conditions may shift as children transition into adolescence. Children and teenagers are still developing which means they can grow in and out of problems [highly recommended].
4.5 To determine whether symptoms are primary or secondary to ADHD, consider the chronological and functional presentation of symptoms (ie assess their temporal relationship, severity, frequency, and persistence over time) [essential].
4.6 Consider the range of alternative explanations for ADHD-like attentional/cognitive, hyperactivity, and impulsivity symptoms and challenges. To assist with such differential diagnostic questioning, explore the trigger/context for the symptom and its subjective experience [essential].
Outcome 5: Information That Should Be Included in the Assessment Report
A clear overview of the method and diagnostic criteria should be specified in the report. The assessor must cover and detail the assessment domains outlined previously in Sections 2–4. Where “essential” information is not available, it should be made clear that it was discussed and/or considered. Assessing clinicians should give careful thought as to whether they can justify making a diagnosis of ADHD in the context of missing or contradictory information and in such cases, there should be an exploration of the issue and its impact on the validity of the conclusion.
The report must specify the following topics: diagnostic criteria applied, pre-assessment process, sources of information, documents reviewed, materials used (structured interview and/or other tests), physical and mental health history, current mental state, developmental and personal history, family history, educational/occupational history, inattention and hyperactive/impulsive symptom domains, behavioural observations, psychometric results and interpretation (if administered), impact on daily functioning (including risk behaviours and impairment), strengths and resources, conclusions, recommendations, and follow-up plan/options. It is not acceptable to bulk out a brief report with generic tables, graphs, appendices, references, and/or information about treatment.
A detailed description of the symptoms endorsed in the inattention and hyperactive-impulsive domains and an explanation of how these symptoms align with the diagnostic criteria should be clearly specified. This should include real-life examples of how symptoms cause difficulties, the context in which they occur and whether accommodations are made to mitigate these difficulties. This section should include verbatim self- or informant-narrative.
The report may comment on the absence of relevant conditions and/or risk factors associated with ADHD and its treatment (eg, “no evidence of previous head injuries or seizures; no evidence of blood pressure or cardiovascular problems past or present; no history of joint hypermobility/orthostatic symptoms/allergy etc”).
The report must include a diagnostic formulation that specifies how all diagnostic criteria for ADHD are met (or not). This includes:
- The precise number of symptoms identified from each of the inattentive and/or hyperactive-impulsive symptom domains should be explicitly specified.
- Whether “several” inattentive or hyperactive-impulsive symptoms were present (or not) prior to age 12 years.
- Whether “several” inattentive or hyperactive-impulsive symptoms are present (or not) in two or more settings (eg at home, school, or work; with friends or relatives; in other activities).
- Whether there is clear evidence (or not) that the symptoms interfere with or reduce the quality of social, academic, or occupational functioning.
- Whether symptoms are (or not) better explained by another disorder.
If ADHD diagnostic criteria are met, the report should explicitly state that the clinical presentation subtype (eg, ADHD–combined presentation, ADHD–predominantly inattentive presentation, ADHD–predominantly hyperactive-impulsive presentation).
If ADHD diagnostic criteria are not met, the report should comment whether symptoms of inattentiveness, impulsivity, and/or restlessness are present that fall subthreshold of an ADHD diagnosis (eg symptoms and/or impairments may have diminished with age, or the child/teenager may fall just below the diagnostic threshold). Alternatively, the report should comment on whether these symptoms are considered to be secondary to a different mental, medical, or neurodevelopmental condition. In some cases, this may require a further assessment (eg autism might be suspected but there may be insufficient information from the ADHD assessment to diagnose it).
The report must explicitly state the child or teenager’s history of comorbidity and/or whether a comorbid condition(s) is present at the time of the assessment. In the latter case, it should be stated how these condition(s) may be impacting or contributing to the ADHD presentation (or vice versa), as in some cases the comorbidity may need to be addressed first. If there is a risk of harm to self or others, this should be explicitly stated, documenting the nature of the risk, precipitating, perpetuating, and protective factors, and a risk management plan.
The report should summarise the resources (strengths, talents, and functional coping strategies) of the individual and caregivers and suggest recommendations for “next steps”, including options for intervention and support (irrespective of whether the child or teenager meets ADHD diagnostic criteria or not).
Aside from the full clinical report, it is helpful to generate a shorter, more accessible summary report. The full report may contain very personal information that the family is not comfortable sharing more widely. Children and teenagers and/or their family may feel more comfortable sharing a summary report, written in user-friendly language, with other professionals (eg teachers, social workers).
Box 5: Quality Standard Guidance on the Information That Should Be Included in the Assessment Report
5.1 The report should be organised under the key assessment headings described above [highly recommended].
5.2 It must report what collateral information has been reviewed, eg school reports (and other relevant assessment reports), and whether they support the diagnostic outcome [essential].
5.3 All the relevant information obtained during the assessment needs to be recorded and described in detail to demonstrate that a robust and valid diagnostic assessment has been undertaken [essential].
5.4 Missing or contradictory information must be specified [essential].
5.5 A detailed account of the inattention and hyperactive/impulsive domain symptoms that are present (including scores) must be provided, together with real-life examples of how they cause difficulties, the context in which they occur, and whether accommodations are made to mitigate these difficulties [essential].
5.6 A summary of the previous and current mental and physical health comorbidities [essential].
5.7 The report must have a section on diagnostic formulation where the clinician should specify which diagnostic classification system has been applied and provide evidence from the assessment that shows how the diagnostic criteria for ADHD are met (or not) [essential].
5.8 The report should report quantitative data giving the precise number of symptoms within each domain that have been identified [essential].
5.9 If ADHD diagnostic criteria are met, the clinical presentation subtype must be stated (eg, ADHD–combined presentation, ADHD–predominantly inattentive presentation, ADHD–predominantly hyperactive-impulsive presentation) [essential].
5.10 Specify DSM-5-TR category of severity of symptoms (mild, moderate, severe) [essential].
5.11 The evidence for any comorbid diagnosis should be specified [essential].
5.12 If ADHD diagnostic criteria are not met, the report should clarify whether any inattentive, impulsive, restless symptoms are secondary to a different mental, physical, or neurodevelopmental condition or better explained by any other factors [essential].
5.13 Include protective factors and strengths (within the individual’s and the caregiver environment, such as support networks, compensatory strategies, environmental accommodations) and how to harness and direct them at positive opportunities [highly recommended].
5.14 Summarise the resources of the individual and caregivers and suggest recommendations for “next steps”, including options for intervention and support (irrespective of whether the child or teenager meets ADHD diagnostic criteria or not) [highly recommended].
5.15 Generate a shorter, more accessible summary report with a user-friendly language to meet the needs of the child/teenager and/or parent/caregiver [optional].
Outcome 6: The Post-Diagnostic Discussion
Following a diagnosis of ADHD in children and teenagers, NICE Guidelines suggest a post-diagnostic discussion to support both the caregivers and individual themselves. This discussion is not about outlining a formal treatment plan but rather giving them space to process the diagnosis and address any immediate concerns, worries, or questions in a supportive atmosphere.
Whether at the end of the assessment or in a dedicated follow-up session, the post-diagnostic discussion should be tailored to the needs of both the child or teenager and their caregivers, providing information, support, and reassurance. If the diagnosis of ADHD has not been made, the reasons for this need to be carefully explained. It is important to be mindful that this is a child or teenager and family who have presented with difficulties and struggles. They will value guidance about their next steps and future options.
For those who are given the diagnosis, this marks the beginning of their journey of discovery in the management of their ADHD. For adolescents and caregivers, it’s essential to give reassurance that the diagnosis does not define them but can open doors to support and adjustments that can greatly improve their quality of life. This includes access to resources, accommodations in education, and understanding from peers and educators. However, it is also important to emphasise that ADHD is just one aspect of their identity and to discuss potential negative aspects such as stigma and labelling.
It is crucial to empower children and teenagers by involving them in discussions about their diagnosis and its implications, when appropriate. This might include talking about how ADHD could affect their life, both positively and negatively. They may have questions or worries about how it will impact their school performance, relationships, and daily activities. Acknowledging their concerns and providing information and support can help them navigate these challenges.
It is important to explain that pharmacological and psychosocial treatments (such as therapy or behavioural interventions) are available and to enquire about attitudes to treatment. A brief and clear review of the current evidence for interventions will foster an informed decision about the intervention. For prescribing clinicians, this might include discussions about medication options, their potential benefits, and any associated risks or side effects. If the post-diagnostic discussion is not being held with a prescribing clinician, the individual and caregivers should be signposted or referred directly to discuss this with a qualified prescribing clinician.
With young children and/or when speaking with caregivers independently, there may be more focus on practical strategies for managing ADHD symptoms in the home. This could include techniques for improving communication, regulating mood, setting clear expectations, establishing supportive routines and environmental modifications to optimise attention when doing homework. If risky behaviours have been identified, discussing strategies to address these and keep the child or teenager safe is crucial.
With consent from the individual/family, it may also be helpful to provide feedback to other professionals in education, residential settings, social care, and/or youth justice.
If appropriate, provide signposting and referrals to other services, either within the NHS or other organisations. This might include referrals to mental health services, educational support services, or community organisations that offer support to individuals with ADHD and their families. Regarding supplementary resources, there are vast amounts of books, podcasts, and other materials online. If signposting to these resources, be sure that these materials have been screened and approved.
Box 6: Quality Standard Guidance on the Post-Diagnostic Discussion
6.1 Either immediately following or in a dedicated follow-up assessment offer a post-diagnostic discussion to address questions and alleviate anxiety [highly recommended].
6.2 Customise the discussion to meet the needs of both the individual and caregivers. Empower children and teenagers by involving them in the discussion about their diagnosis and its implications [essential].
6.3 Highlight the ongoing nature of managing ADHD with discussion about positive aspects (access to resources, accommodations) and potential negatives (stigma, labelling) [highly recommended].
6.4 Discuss treatment options (pharmacological and psychosocial) and ensure that the individual and/or caregivers have an opportunity to discuss medication options with a qualified prescribing clinician [essential].
6.5 Consider if feedback to other professionals in the system is required with consent [highly recommended].
6.6 Discuss practical strategies for home such as communication techniques, setting clear expectations, establishing routines, and optimising the environment for homework [highly recommended].
6.7 Address risky behaviours with strategies to keep the young person safe [essential].
6.8 Provide information and/or referrals to other services as appropriate (mental health, educational support, community organizations) [highly recommended].
Outcome 7: Core Competencies Required to Conduct a Diagnostic Assessment of ADHD in Children or Teenagers
There are complexities involved in accurately diagnosing ADHD in children and young people, which emphasise the importance of including skilled practitioners in the assessment process. It is an established principle that all adults have a duty to ensure that children and teenagers are safe, that their welfare is protected, and that all safeguarding concerns are reported and subsequently addressed. Mental health professionals undertaking assessments should have a good understanding of typical development for children and young people. They should be well informed regarding cultural norms for the individual being assessed and be aware that presentations in children and teenagers may be less clear cut than in adults.9
Accurate diagnosis of ADHD requires a practitioner who understands when not to diagnose, as well as a sound understanding of ADHD and other related conditions. However, the transdiagnostic nature of inattention, impulsivity, and restlessness creates complexities in accurately diagnosing ADHD in children and young people, which emphasises the importance of including skilled practitioners in the assessment process across psychopathology.
In line with the general approach to all mental health conditions, the diagnosis of neurodevelopmental conditions is dependent on clinical judgment as to the presence or absence of symptoms and whether a required threshold for reduced quality of functioning and/or impairment has been reached. This requires clinicians to consider a range of differential diagnoses in children and teenagers, including other mental and physical health conditions that may present similarly to ADHD and mimic its symptoms. This is further complicated by a range of comorbid conditions that are present alongside ADHD. Adequate data collection during assessment is crucial for informed decision-making by trained clinicians. However, many clinicians lack confidence in assessing neurodevelopmental conditions (including ADHD), and this can be missed and/or misdiagnosed.
There is growing recognition of the utility of educational-led reviews of ADHD symptoms in educational settings.43 Typically, these focus on educational needs arising from inattention, impulsivity, or restlessness, and they may lead to educational support and accommodations for children/teenagers. They may expedite referral for clinical diagnostic assessments so the children/teenagers can access clinical support.
Who Can Assess ADHD and Who Can Diagnose ADHD
Regarding the clinical pathway, junior clinicians with a specialist understanding of ADHD may be involved in aspects of comprehensive clinical assessment. They may not be proficient in differential diagnosis, but with appropriate training and supervision they can gather pertinent information using a semi-structured clinical interview for consideration by an experienced clinician who does have training in differential diagnoses. This has the potential to support under-resourced clinicians to reliably gather information to assess diagnostic criteria in a trustworthy and systematic way.
Healthcare professionals assessing AND diagnosing ADHD in children and teenagers need to have received clinical training and acquired a core competency in working with this group. This training needs to be part of a formal training course that is recognised by healthcare regulators, rather than simply involving attending modular courses. They must also have a firm understanding of normal levels of attention, impulsivity, and hyperactivity for typically developing children and teenagers and the cultural background of the individuals being assessed. This will enable an informed decision to be made as to whether the young person’s presentation differs from what would typically be expected.
As a guide, we have noted what we consider to be the qualification and competence required to undertake assessment and diagnosis of ADHD in children and teenagers. Note that the lists below are not exhaustive and all practitioners are expected to maintain their clinical competencies and access supervision in line with their governing bodies:
Category A: The specialities that generally have the necessary experience, expertise, and competence to assess and diagnose ADHD in children and teenagers must be (1) clinical practitioners who have been trained to work with children and teenagers and (2) who have a minimum of three years expertise in working with children and teenagers with ADHD under supervision. This group includes:
- Consultant child and adolescent psychiatrists.
- Consultant paediatricians.
- Clinical psychologists (senior level).
- Practitioner neuropsychologists who completed the clinical psychology training route (senior level).
- Associate specialist doctors.
- Advanced nurse practitioners and Nurse Consultants.
Category B: Specialities that will typically require direct supervision to assess and diagnose ADHD in children and teenagers must be (1) clinical practitioners who have been trained to work with children and teenagers but who are yet to meet criteria for a Category A practitioner and (2) who are receiving clinical supervision in the assessment of ADHD in children and teenagers (at a minimum of once per month) from a Category A practitioner. This group includes:
- Clinical psychologists.
- Practitioner neuropsychologists who completed the clinical psychology training route.
- Specialist psychiatric trainees.
- Mental Health Nurses.
- Specialist pharmacists with appropriate post qualification training.
Category C: Other healthcare professionals working within the clinical field and who have an interest in learning more about ADHD in children and teenagers who can assist clinical practitioners in the assessment process (ie they can complete a semi-structured interview, but they cannot diagnose) must receive robust oversight and supervision for each case from a Category A or Category B practitioner. This group includes:
- Core psychiatric trainees.
- Clinical psychology trainees.
- Junior mental health nurses.
- Associate mental health workers.
- Assistant psychologists.
- Primary care general medical practitioners.
Practitioners working in other professional areas who have an interest in learning more about ADHD in children and teenagers and who have acquired an extensive knowledge of mental health and neurodevelopmental conditions may acquire the specialist skills and competencies required to be a Category C (or in some circumstances a Category B) assessor of ADHD in this group, provided they have received training and acquired a core competency in working with children and teenagers. Examples might include specialists in neurology, counselling psychology, educational psychology, forensic psychology, occupational psychology, occupational therapy, speech and language therapy, practitioner neuropsychology with completion of the counselling psychology or educational psychology training route, and assistant/associate general practitioners working in primary care.
Box 7: Quality Standard Guidance on the Core Competencies Required to Conduct a Diagnostic Assessment of ADHD in Children and Teenagers
7.1 NICE guidelines stipulate that a diagnosis of ADHD should only be made by “a specialist psychiatrist, paediatrician or other appropriately qualified healthcare professional with training and expertise in the diagnosis of ADHD”. It is stipulated that “they should undertake training so that they are able to diagnose ADHD and provide treatment and management in accordance with this guideline” [essential].
7.2 Healthcare professionals assessing and diagnosing ADHD in children and teenagers need to have received clinical training and acquired a core competency in working with children and teenagers. This training needs to be part of a formal training course that is recognised by healthcare regulators, rather than simply involving attending modular courses [essential].
7.3 It is essential assessors have a firm understanding of normal levels of attention, impulsivity, and hyperactivity for typically developing children and young people and the cultural background of the individual being assessed. This will enable an informed decision to be made as to whether the child or teenager’s presentation differs from what would typically be expected [essential].
7.4 Following initial training, clinicians will need to arrange formal supervision for their ADHD cases (at least monthly). Supervision should be provided by someone who is experienced in assessing and managing ADHD in children and teenagers [essential].
Conclusion
The manuscript emphasises the importance of establishing quality assurance standards and guidance for diagnosing ADHD in children and teenagers to address challenges faced by practitioners, reduce delays in diagnosis and intervention, and ensure proper support for children and teenagers with ADHD. The development of the AQAS8 and its childhood counterpart, CAAQAS (this document), aims to support this process by offering clear, practical, and detailed guidance for assessments. Recommendations for report writing are intended to facilitate effective communication between ADHD specialists and other services, including primary care and education sectors.
While neither the AQAS nor CAAQAS aims to replace formal training and supervision, they provide a framework for those who have undergone training to follow. The intention is not to be overly prescriptive but to offer sensible recommendations to support high-quality clinical care.
Our goal is to promote high-quality assessments, improve diagnostic accuracy, and reduce the risks of overdiagnosis, misdiagnosis, and underdiagnosis, ultimately aiming to enhance outcomes for children and teenagers with ADHD. The development of quality assurance standards and the provision of this guidance will enhance outcomes for children and teenagers with ADHD by ensuring they receive the support they need.
The limitations of these consensus guidelines for ADHD assessment stem from their reliance on expert opinion and drawing on their knowledge of empirical evidence. While the guidelines offer a comprehensive framework, they are shaped by clinical experience, which can introduce variability in practice. This reliance on subjective judgment makes it harder to ensure consistency and replicability across different clinical settings. Additionally, the guidance is focused on UK practices, which may not apply in other countries with different healthcare systems, cultural norms, and legal frameworks. This limits their international relevance and could lead to difficulties in adapting the recommendations for global use. Another limitation is the lack of biomarkers for ADHD, meaning the guidelines rely on subjective clinical assessments, which can vary in accuracy.
Future research should focus on advancing biomarker research, which could enhance the objectivity and precision of ADHD diagnosis, improving diagnostic accuracy. Cross-cultural validation is also needed, as the guidelines are UK-centred and may be less relevant in other countries. Research comparing the effectiveness of different assessment tools across various settings would help ensure the guidelines apply to diverse populations. Additionally, studying the role of digital tools and telemedicine in ADHD assessments could determine how technology can complement traditional diagnostic methods.
Abbreviations
ADHD, Attention-Deficit/Hyperactivity Disorder; CAAQAS, ADHD Assessment Quality Assurance Standard for Children and Young People; NICE, National Institute of Health and Care Excellence; UKAAN, UK Adult ADHD Network; UKAP, UK ADHD Partnership; AUC, area under the curve; SENCo, Special Educational Needs Coordinator; PTSD, post-traumatic stress disorder; CPTs, continuous performance tests; ACE, ADHD Child Evaluation; FASD, Foetal Alcohol Spectrum Disorder; ODD, oppositional defiant disorder; CDD conduct-dissocial disorder; SASC, SpLD Assessment Standards Committee; AQAS, Adult ADHD Assessment Quality Assurance Standard; ACAMH, Association for Child and Adolescent Central Health.
Acknowledgments
We are grateful to Tanya Palmer for support with referencing the manuscript.
Disclosure
In the last 5 years: S.Y. has received honoraria for consultancy and educational talks from Medice, Janssen and Takeda. She is the author of the ADHD Child Evaluation (ACE), ACE+ for adults and R&R2ADHD.
R.M.’s clinical service has received honoraria for his educational talks and project work from Flynn-Pharma, Takeda, and Medice.
C.A, has received honoraria from Flynn-Pharma and Takeda for educational presentations.
S.O. received an educational grant to develop information for children and young people with ADHD.
S.C. NIHR Research Professor (NIHR303122), is funded by the NIHR for research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS or the UK Department of Health and Social Care. He has received reimbursement for travel and accommodation expenses from the Association for Child and Adolescent Central Health (ACAMH) in relation to lectures delivered for ACAMH, the Canadian AADHD Alliance Resource, and the British Association of Psychopharmacology, for educational activity on ADHD, and has received honoraria from Medice.
A.L. has received an honorarium from Takeda in 2023 for participating in a consultation about Adult ADHD Service Provision in the UK.
Z.A., W.C., G.H.G., J.S., G.P., E.W., P.H., J.H., J.C., MA, W.A. declare no conflict of interest.
References
1. Polanczyk GV, Willcutt EG, Salum GA, Kieling C, Rohde LA. ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. Int J Epidemiol. 2014;43(2):434–442. doi:10.1093/ije/dyt261
2. Cortese S, Song M, Farhat LC, et al. Incidence, prevalence, and global burden of ADHD from 1990 to 2019 across 204 countries: data, with critical re-analysis, from the global burden of disease study. Mol Psychiatry. 2023;28(11):4823–4830. doi:10.1038/s41380-023-02228-3
3. Bradford A, Meyer AND, Khan S, Giardina TD, Singh H. Diagnostic error in mental health: a review. BMJ Qual Saf. 2024;33(10):663–672. doi:10.1136/bmjqs-2023-016996
4. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. 2022.
5. World Health Organization. International classification of diseases 11th revision [ICD–11]. 2022. Available from: https://www.who.int/standards/classifications/classification-of-diseases.
6. National Institute for Health and Care Excellence. Attention deficit hyperactivity disorder: Quality Standard [QS39]. 2013. Available from: https://www.nice.org.uk/guidance/qs39.
7. National Institute for Health and Care Excellence. Attention deficit hyperactivity disorder: diagnosis and management [NG87]. 2018. Available from: www.nice.org.uk/guidance/ng87.
8. Adamou M, Arif M, Asherson P et al. The adult ADHD assessment quality assurance standard. Front Psychiatry. 2024;15:1380410. doi:10.3389/fpsyt.2024.1380410
9. Vos M, Rommelse NNJ, Franke B, et al. Characterizing the heterogeneous course of inattention and hyperactivity-impulsivity from childhood to young adulthood. Eur Child Adolesc Psychiatry. 2022;31(8):1–11. doi:10.1007/s00787-021-01764-z
10. Botha M, Hanlon J, Williams GL. Does language matter? Identity-first versus person-first language use in autism research: a response to vivanti. J Autism Dev Disord. 2023;53(2):870–878. doi:10.1007/s10803-020-04858-w
11. Care Quality Commission. Brief guide BG004: brief guide: capacity and competence in under 18s. 2019.
12. National Health Service (2022). Children and Young People, Consent to Treatment. Available from: https://www.nhs.uk/conditions/consent-to-treatment/children/.
13. Medical Defence Union (2024). Children whose Parents are Separated. Available from: https://www.themdu.com/guidance-and-advice/guides/children-whose-parents-are-separated.
14. Santosh P, Cortese S, Hollis C, et al. Remote assessment of ADHD in children and adolescents: recommendations from the European ADHD guidelines group following the clinical experience during the COVID-19 pandemic. Eur Child Adolesc Psychiatry. 2023;32(6):921–935. doi:10.1007/s00787-023-02148-1
15. Cortese S, Solmi M, Michelini G, et al. Candidate diagnostic biomarkers for neurodevelopmental disorders in children and adolescents: a systematic review. World Psychiatry. 2023;22(1):129–149. doi:10.1002/wps.21037
16. Coghill D, Banaschewski T, Cortese S, et al. The management of ADHD in children and adolescents: bringing evidence to the clinic: perspective from the European ADHD Guidelines Group (EAGG). Eur Child Adolesc Psychiatry. 2023;32(8):1337–1361. doi:10.1007/s00787-021-01871-x
17. De Los Reyes A, Kazdin AE. Measuring informant discrepancies in clinical child research. Psychol Assess. 2004;16(3):330–334. doi:10.1037/1040-3590.16.3.330
18. De Los Reyes A. Introduction to the special section: more than measurement error: discovering meaning behind informant discrepancies in clinical assessments of children and adolescents. J Clin Child Adolesc Psychol. 2011;40(1):1–9. doi:10.1080/15374416.2011.533405
19. Caye A, Machado JD, Rohde LA. Evaluating parental disagreement in ADHD diagnosis: can we rely on a single report from home? J Atten Disord. 2017;21(7):561–566. doi:10.1177/1087054713504134
20. Mayfield AR, Parke EM, Barchard KA, et al. Equivalence of mother and father ratings of ADHD in children. Child Neuropsychol. 2018;24(2):166–183. doi:10.1080/09297049.2016.1236186
21. Langberg JM, Epstein JN, Simon JO, et al. Parent agreement on ratings of children’s attention deficit/hyperactivity disorder and broadband externalizing behaviors. J Emot Behav Disord. 2010;18(1):41–50. doi:10.1177/1063426608330792
22. Mulraney M, Arrondo G, Musullulu H, et al. Systematic review and meta-analysis: screening tools for attention-deficit/hyperactivity disorder in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2022;61(8):982–996. doi:10.1016/j.jaac.2021.11.031
23. van der Putten WJ, Mol AJJ, Groenman AP, et al. Is camouflaging unique for autism? A comparison of camouflaging between adults with autism and ADHD. Autism Res. 2024;17(4):812–823. doi:10.1002/aur.3099
24. Young S. ADHD child evaluation [ACEv.2]. London, UK: Psychology Services Limited. Available from: https://www.psychology-services.uk.com/adhd.
25. Young S, Uysal O, Kahle J, et al. A systematic review and meta-analysis comparing the severity of core symptoms of attention deficit hyperactivity disorder in females and males. Psychol Med. 2024;1–22. doi:10.1017/S0033291724001600
26. Arrondo G, Solmi M, Dragioti E, et al. Associations between mental and physical conditions in children and adolescents: an umbrella review. Neurosci Biobehav Rev. 2022;137:104662. doi:10.1016/j.neubiorev.2022.104662
27. Cortese S, Sun S, Zhang J, et al. Association between attention deficit hyperactivity disorder and asthma: a systematic review and meta-analysis and a Swedish population-based study. Lancet Psychiatry. 2018;5(9):717–726. doi:10.1016/s2215-0366(18)30224-4
28. Cortese S. The association between ADHD and obesity: intriguing, progressively more investigated, but still puzzling. Brain Sci. 2019;9(10):256. doi:10.3390/brainsci9100256
29. Arrondo G, Mulraney M, Iturmendi-Sabater I, et al. Systematic review and meta-analysis: clinical utility of continuous performance tests for the identification of attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2024;63(2):154–171. doi:10.1016/j.jaac.2023.03.011
30. Bellato A, Hall CL, Groom MJ, et al. Practitioner review: clinical utility of the QbTest for the assessment and diagnosis of attention-deficit/hyperactivity disorder - A systematic review and meta-analysis. J Child Psychol Psychiatr. 2024;65(6):845–861. doi:10.1111/jcpp.13901
31. National Institute for Health and Care Excellence: Diagnostics Guidance [DG60]. (2024) Digital Technologies for Assessing Attention Deficit Hyperactivity Disorder. Available from: https://www.nice.org.uk/guidance/dg60.
32. Curran SA, Kooij JJ. Young-DIVA. DIVA Foundation. 2019;56:14––34.
33. Kaufamn JB, Axelson D. K-SADS-PL DSM-5, Pittsburg, USA Available from: https://pediatricbipolarpittedu/sites/default/files/assets/Clinical%20tools/KSADS/KSADS_DSM_5_SCREEN_Finalpdf.
34. Sheehan D. MINI 7.0.2 for ADHD Studies. Harm Research Institute. Available from: https://harmresearch.org/product/mini-international-neuropsychiatric-interview-mini-for-attention-deficit-hyperactivity-disorder-studies-7-0-2-13/.
35. Wanni Arachchige Dona S, Badloe N, Sciberras E, Gold L, Coghill D, Le HND. The impact of childhood attention-deficit/hyperactivity disorder (ADHD) on children’s health-related quality of life: a systematic review and meta-analysis. J Atten Disord. 2023;27(6):598–611. doi:10.1177/10870547231155438
36. Thompson T, Lloyd A, Joseph A, Weiss M. The Weiss functional impairment rating scale-parent form for assessing ADHD: evaluating diagnostic accuracy and determining optimal thresholds using ROC analysis. Qual Life Res. 2017;26(7):1879–1885. doi:10.1007/s11136-017-1514-8
37. Cicchetti DS, Sparrow CS. Vineland adaptive behavior scales (Third Edition). Available from: https://www.pearsonclinical.ca/store/caassessments/en/Store/Professional-Assessments/Behavior/Interventions/Vineland-Adaptive-Behavior-Scales-%7C-Third-Edition/p/P100008010.html.
38. Al-Attar Z. ADHD and Differential Diagnosis in Children and Adults. Psychology Services Limited. Available from: https://www.psychology-services.uk.com/adhd.htm.
39. Young S, Abbasian C, Al-Attar Z, et al. Identification and treatment of individuals with attention-deficit/hyperactivity disorder and substance use disorder: an expert consensus statement. World J Psychiatry. 2023;13(3):84–112. doi:10.5498/wjp.v13.i3.8
40. McCarthy R, Mukherjee RAS, Fleming KM, et al. Prevalence of fetal alcohol spectrum disorder in Greater Manchester, UK: an active case ascertainment study. Alcohol Clin Exp Res. 2021;45(11):2271–2281. doi:10.1111/acer.14705
41. Gregory G. Children who are looked after: the impact of FASD. In: Mukherjee RAS, Aiton N, (eds) Prevention, Recognition and Management of Fetal Alcohol Spectrum Disorders. Cham: Springer; 2021. doi:10.1007/978-3-030-73966-9_17
42. Young S, Absoud M, Blackburn C, et al. Guidelines for identification and treatment of individuals with attention deficit/hyperactivity disorder and associated fetal alcohol spectrum disorders based upon expert consensus. BMC Psychiatry. 2016;16(1):324. doi:10.1186/s12888-016-1027-y
43. SASC. SASC guidance on the assessment and identification of the characteristics of an Attention Deficit Hyperactivity Disorder (ADHD). Available from: https://sasc.bykayo.digital/sasc-downloads/.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Brain Function Characteristics of Children with Attention-Deficit/Hyperactivity Disorder Aged 4-9 Years During a GO/NOGO Task: An Functional Near-Infrared Spectroscopy Study
Cui Z, Liang A, Huang H, Ni X
Neuropsychiatric Disease and Treatment 2024, 20:2507-2516
Published Date: 13 December 2024