")
Back to Journals » Infection and Drug Resistance » Volume 18
The Advance and Clinical Practice on Lung Disease Caused by Mycobacterium abscessus
Authors Zhang L, Rao Y, Li Z, Fan M, Xiang Z, Wang J
Received 27 February 2025
Accepted for publication 18 June 2025
Published 25 June 2025 Volume 2025:18 Pages 3103—3115
DOI https://doi.org/10.2147/IDR.S524214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Lijun Zhang,1 Yao Rao,2 Zhongyan Li,2 Mei Fan,3 Zongjun Xiang,3 Jingsong Wang3
1Department of Clinical Pharmacy, Dazhou Central Hospital, Dazhou, Sichuan, People’s Republic of China; 2Department of Respiratory, Dazhou Central Hospital, Dazhou, Sichuan, People’s Republic of China; 3Department of Pharmacy, Guangyuan Central Hospital, Guangyuan, Sichuan, People’s Republic of China
Correspondence: Jingsong Wang, Department of Pharmacy, Guangyuan Central Hospital, Guangyuan, Sichuan, People’s Republic of China, Email [email protected]
Abstract: Mycobacterium abscessus (M. abscessus) lung disease has gradually become a common clinical condition, with its incidence rate continuously rising, especially among patients with weakened immune function or those with chronic lung diseases. Given the high resistance of M. abscessus to antibiotics, the options for antibiotics are very limited. Additionally, long treatment times and poor patient compliance lead to low cure rates and high recurrence rates, making it one of the significant public health challenges threatening global health. This article presents two cases of patients diagnosed with M. abscessus lung disease using next-generation metagenomic sequencing technology. It reviews and analyzes the current research on M. abscessus along with details from these cases. Furthermore, this article emphasizes the necessity of timely, regular, and comprehensive treatment for M. abscessus lung disease. Meanwhile, we call for the formulation of robust prevention strategies, the optimization and innovation of treatment regimens, and the enhancement of follow-up management after cure to improve the understanding and handling capabilities of M. abscessus lung disease, thereby addressing the increasing clinical challenges.
Keywords: nontuberculous mycobacteria, Mycobacterium abscessus lung disease, clinical manifestations, diagnosis, treatment, prevention
Introduction
Nontuberculous mycobacteria (NTM) refer to a large group of mycobacteria excluding the Mycobacterium tuberculosis complex and Mycobacterium leprae.1 So far, more than 190 strains of NTM have been discovered,2 and a small number of NTM are pathogenic, which can lead to infections in various tissues of the human body, including skin soft tissue, breast, eyes, musculoskeletal system, heart, lymphatic system, and tendon sheaths.3–6 Lung infections are particularly common.3 In the state of Hawaii, USA, the prevalence can be as high as 396 cases per 100,000 people.7 According to the growth rates of NTM, they are divided into two main categories: slow-growing and fast-growing species. Among the fast-growing species, M. abscessus is considered the most pathogenic.8 It is known that M. abscessus has three subspecies: Mycobacterium abscessus subspecies abscessus (MAB), Mycobacterium abscessus subspecies massiliense (MMA), and Mycobacterium abscessus subspecies bolletii (MAO).9 According to some reports, lung infections caused by M. abscessus make up 2.6–13% of NTM lung infections,10,11 especially in patients with weakened immune systems or chronic lung diseases, who face a higher risk of infection. The clinical manifestations of lung infection caused by M. abscessus are very similar to those of pulmonary tuberculosis, including cough, producing sputum, weight loss, pleural effusion, dyspnea, and hemoptysis. Additionally, due to a previous lack of understanding about this strain and the lack of easy and practical ways to identify the strain, it is easy to miss or misdiagnose the disease,12 which can result in treatment failures. Simultaneously, M. abscessus exhibits complex resistance mechanisms encompassing target site modification, mutations at target loci, β-lactamase-mediated drug inactivation, activation of efflux pump systems, and cell wall permeability barriers.13,14 Consequently, the American Thoracic Society (ATS) recommends combination therapy with 3–4 active agents selected through in vitro susceptibility testing to prevent acquired resistance during treatment, particularly against macrolides.9 However, specific regimens require comprehensive integration of pharmacokinetic/pharmacodynamic (PK/PD) characteristics, drug synergism, adverse effects, and multidimensional considerations including patient-specific factors (advanced age, obesity), comorbidities, and disease severity. Therefore, no standardized combination therapy protocol currently exists. Additionally, the treatment duration is long, and patient compliance is poor, making clinical treatment extremely challenging.12,15 M. abscessus lung disease has become one of the significant public health issues threatening human health.12,16,17
Due to factors such as the unique biological characteristics of the pathogenic bacteria, the immune status of the host, the external environment, destruction of lung structure, and incomplete treatment,18 the recurrence rate of patients infected with M. abscessus may be as high as 40%,19 with a co-infection rate of aspergillus between 3.9% and 16.7%,18 which increases patient mortality. Therefore, it is essential to place a high emphasis on follow-up management after recovery. The purpose of this article is to explore the clinical characteristics, diagnosis, treatment, follow-up, prevention, and future research directions of M. abscessus lung disease through clinical practice and literature review, in order to help clinicians gain a comprehensive understanding of M. abscessus pulmonary disease and provide a useful reference for similar cases.
Cases Presentation
Case 1
A 58-year-old female was admitted to our hospital on November 3, 2022, due to “persistent cough with purulent sputum for 2 years, worsening for 10 d”. She has a history of pulmonary tuberculosis for over 30 years and has been cured. A chest CT at the outpatient showed widespread small patchy spots in both lungs, particularly prominent in the basal segments of the lower lobes of both lungs and the middle lobe of the right lung, with local bronchial dilatation (Figure 1A). Next-generation metagenomic sequencing (mNGS) of sputum and bronchoalveolar lavage fluid (BALF) revealed MAB, inducing macrolide-resistant strains (Table 1). But the treatment was delayed because of the COVID-19 pandemic. Four months later, the patient visited another hospital, where auscultation revealed wet rales in both lungs. Her white blood cell count was 5.58 × 109 cells/L (reference range: 3.5–9.5), C-reactive protein (CRP) was 18.60 mg/L (0–8.2), Procalcitonin (PCT) was 0.059 ug/L (<0.064), FEV1/FVC was 76.08%. Liver and kidney function tests, Serum (1-3)-β-D-glucan test (G test, to detect fungal infections); Galactomannan Test (GM test, to assess invasive aspergillosis), and tumor markers CA125/CA153/CA724 showed no significant abnormalities. DNA of Mycobacterium in the sputum, tuberculosis X-pert, and tuberculosis RNA tests were negative. Acid-fast bacilli smear of sputum was positive. The Matrix-Assisted Laser Desorption/Ionization Time of Flight Mass Spectrometry (MALDI-TOF MS) test on the sputum indicates that MAB and MMA are present.
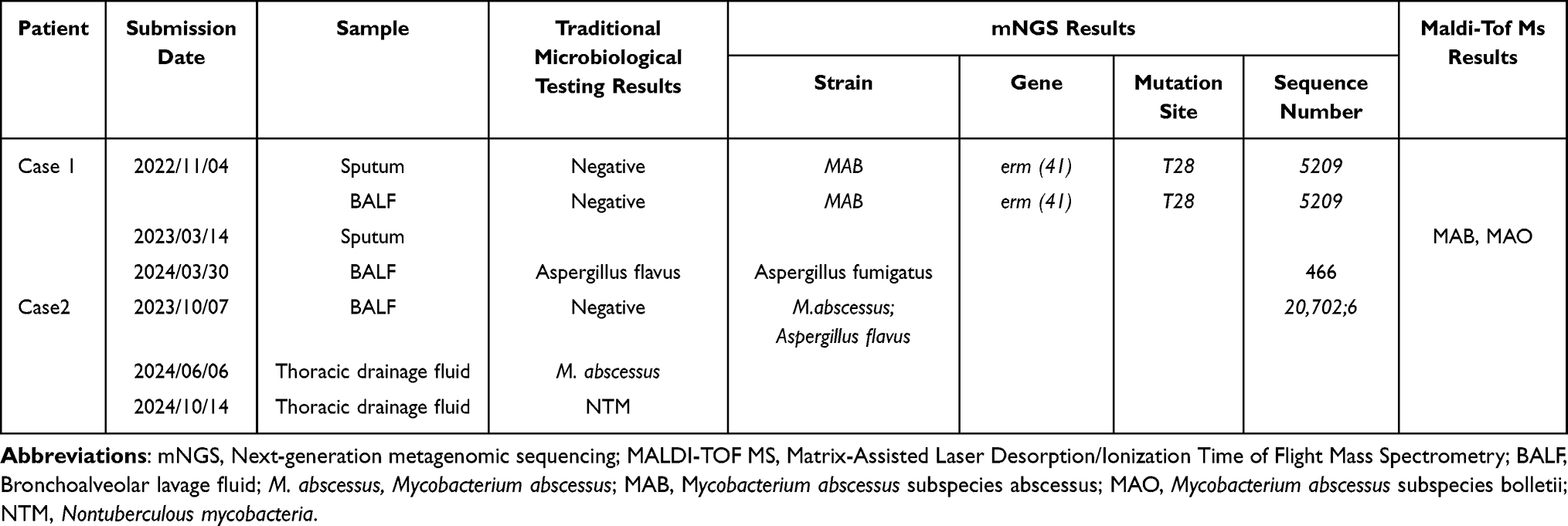 |
Table 1 Summary of Results from Traditional Tests, mNGS and MALDI-TOF MS |
 |
Figure 1 The chest CT pulmonary imaging of Case 1. (A) On October 30, 2022, lung CT showed widespread small patchy spots in both lungs, particularly prominent in the basal segments of the lower lobes of both lungs and the middle lobe of the right lung, with local bronchial dilatation; (B) On March 25, 2024, lung CT showed scattered patches, nodules, and strip-like shadows in both lungs, with mild dilation of some bronchi; (C) On June 20, 2024, lung CT showed the M. abscessus lesion in the middle lobe of the right lung has absorbed; (D) On June 20, 2024, lung CT showed the aspergillosis lesion has absorbed more than before. |
The diagnosis of M. abscessus lung disease was confirmed. On April 19, 2023, the drug therapy started. In the initial phase, the patient experienced thrombocytopenia from linezolid and an allergic reaction to cefoxitin. Consequently, the final treatment regimen included intravenous (IV) amikacin and imipenem-cilastatin, along with oral moxifloxacin, minocycline, and clarithromycin. During the maintenance phase, the patient continued oral moxifloxacin, minocycline, and clarithromycin. On September 12, 2023, sputum mycobacterial culture converted to negative. On March 25, 2024, the patient experienced a recurrence of cough and sputum production after catching a cold, accompanied by wheezing. Auscultation revealed scattered moist rales in both lungs. Chest CT showed scattered patches, nodules, and strip-like shadows in both lungs, with mild dilation of some bronchi (Figure 1B). mNGS of BALF indicated Aspergillus fumigatus. Microscopic examination revealed a small number of white blood cells and Aspergillus-like hyphae. Mycobacterium tuberculosis DNA and acid-fast staining of sputum were negative. CRP was 14.92 mg/L (reference range: 0–8.2). White blood cells were 8.73 × 109 cells/L (reference range: 3.5–9.5). PCT, and liver and kidney function tests showed no abnormalities. The diagnosis of invasive pulmonary aspergillosis was confirmed. Clarithromycin was discontinued, and oral isavuconazole sulfate capsules were added for more than two months of treatment. A follow-up chest CT showed that the M. abscessus lesions were completely absorbed (Figure 1C), and the aspergillosis lesions looked better than before (Figure 1D). On July 7, 2024, the patient had no cough, sputum, or wheezing. Isavuconazole was discontinued. On September 24, 2024, FEV1/FVC was 78.86%. Laboratory indicators showed CRP 7.15 mg/L (0–8.2), white blood cells 8.73 × 109 cells/L (reference range: 3.5–9.5), TBIL 7.13 μmol/L (3.4–17.1), ALT 15 U/L (5–40), AST 18 U/L (8–40), and serum creatinine 49 μmol/L (59–104). Minocycline and moxifloxacin were also discontinued. The patient was monitored for four months after recovery with no recurrence. The detailed therapeutic course of Case 1 is illustrated in Figure 2.
 |
Figure 2 The treatment process of Case 1. |
Case 2
A 54-year-old male patient had recurrent blood-streaked sputum over the past year. On October 7, 2023, he was admitted to the hospital due to massive hemoptysis. He had lost 15 kg in weight in the past year. He had a history of emphysema and pulmonary tuberculosis for over 30 years, with the previous tuberculosis having been cured. Chest CT showed bilateral emphysema, bilateral lung infection, possible cavity formation in the upper lobe of the right lung, accompanied by partial bronchial dilatation (Figure 3A). Laboratory test white blood cell count was 14.62 × 109 cells/L (reference range: 3.5–9.5), CRP was 186.6 mg/L (reference range: 0–8.2), PCT was 0.285 μg/L (reference range: <0.064), and liver and kidney functions were normal. mNGS of BALF showed M. abscessus and Aspergillus flavus (Table 1). He expressed a reluctance to participate in strain identification and drug susceptibility testing. On October 12, 2023, thoracoscopic resection of the upper lobe of the right lung was performed, followed by the placement of a drainage tube. Lung tissue pathology revealed purulent lesions in the right lung, accompanied by microabscess formation and chronic granulomatous inflammation.
 |
Figure 3 The chest CT pulmonary imaging of Case 2. (A) On October 11, 2023, Lung CT showed Cavity in the right upper lobe, accompanied by bronchiectasis; (B) On February 27, 2024, Lung CT showed the right upper lobe is missing, with cavitary shadows and air-fluid levels, and the lesions in the right middle lobe have increased. |
He was diagnosed with M. abscessus lung disease. After surgery, he was started on IV imipenem cilastatin sodium, linezolid, and amikacin, combined with oral moxifloxacin therapy. The patient has no hemoptysis. His white blood cell count was 9.67 × 109 cells/L (reference range: 3.5–9.5), CRP was 19.87 mg/L (0–8.2), and liver and kidney functions show no abnormalities. He was requested to continue treatment at the local hospital. The local hospital did not follow the recommended medical advice but instead administered oral anti-tuberculosis treatment with isoniazid, rifampicin, pyrazinamide, and ethambutol for four months. His cough, phlegm, and shortness of breath did not improve, and the drainage tube continued to discharge yellowish-green fluid daily. Chest CT scan on February 27, 2024, showed absence of the upper lobe of the right lung, accompanied by cavity shadows and air-fluid levels. Lesions in the middle lobe of the right lung increased, and segmental atelectasis and bronchiectasis appeared in the posterior segment of the upper lobe of the left lung, with exacerbated emphysema in both lungs (Figure 3B). After discontinuing anti-tuberculosis drugs. He went to several hospitals to get checked, but they did not give him any treatment. On June 6, 2024, an outpatient NTM culture (thoracic drainage fluid) revealed a small amount of M. abscessus. Antimicrobial susceptibility test (cultured for 12 d): amikacin is sensitive, cefoxitin (MIC 64 μg/L) and clarithromycin (MIC 4 μg/L) are moderately sensitive, the rest are resistant. But he refused hospitalization and planned to take the test report back to our hospital for continued treatment. On October 13, 2024, he was readmitted to our hospital. Laboratory tests showed white blood cell count of 8.94 × 109 cells/L (reference range: 3.5–9.5), CRP of 67.22 mg/L (reference range: 0–8.2), total bilirubin (TBIL) of 23.08 μmol/L (reference range: 3.4–17.1), alanine aminotransferase (ALT) of 19 U/L (reference range: 5–40), aspartate aminotransferase (AST) of 21 U/L (reference range: 8–40), alkaline phosphatase (ALP) 47 U/L (reference range: 45–125 U/L), and serum creatinine of 52.4 μmol/L (reference range: 59–104). The culture of thoracic drainage fluid for NTM shows a positive result in small amounts. The treatment plan includes iv amikacin, tigecycline, and cefoxitin, along with oral clarithromycin and clofazimine for combination therapy. Two days later, the patient developed nausea, vomiting, and diarrhea ten times a day, along with scattered rashes on the chest and shoulders. After symptomatic treatment, nausea, vomiting and rash improved, and diarrhea decreased to two to three times a day. On November 2, 2024, nausea, vomiting, and diarrhea have worsened again, with diarrhea increasing to 8 times a day. Laboratory tests showed white blood cell count of 7.43 × 109 cells/L (reference range: 3.5–9.5), CRP of 69.04 mg/L (reference range: 0–8.2), TBIL of 40.54 μmol/L, ALT at 65 U/L, and AST at 63 U/L, and ALP at 358U/L. The patient requested to stop treatment and be discharged. Unfortunately, he passed away one month later. The detailed therapeutic course of Case 2 is illustrated in Figure 4.
 |
Figure 4 The treatment process of Case 2. |
Diagnosis
The diagnosis of NTM disease should be based on a comprehensive assessment of microbiological, clinical, imaging, and pathological examination results.
Microorganisms
In recent years, M. abscessus lung disease has gradually become a clinically frequent disease. The increase in incidence can be attributed not only to increased environmental exposure, an aging population, and a rise in chronic lung disease but also to advancements in microbiological diagnostic techniques. With the development of molecular biology technologies, mNGS and MALDI-TOF MS have been widely used in the diagnosis and treatment of NTM lung disease due to its higher sensitivity, faster sequencing speed.3,15,20 Guidelines recommend that a single positive culture of NTM from bronchial washings or bronchoalveolar lavage fluid and/or molecular biological testing is sufficient;9 however, this standard may be somewhat rough in cases with very few sequences, potentially leading to misdiagnosis or overdiagnosis.9 It is suggested that both NTM culture and molecular biological detection of bronchial washings or bronchoalveolar lavage fluid should be positive simultaneously. Case 2 utilized traditional microbial culture combined with mNGS to discover the pathogenic bacteria M. abscessus, while Case 1 employed mNGS and MS to identify the pathogenic MAB and MAO. Modern molecular biology techniques provide a basis for precise diagnosis in pathogen identification.
Imaging and Clinical Symptoms
The guidelines recommend that individuals with respiratory symptoms and/or systemic symptoms, who show cavitary shadows, multifocal bronchiectasis, and multiple small nodular lesions on chest imaging, and meet the criteria for microbiological evidence while excluding other pulmonary diseases, can be diagnosed with NTM lung disease.9 Case 1 showed bronchiectasis on chest CT, with symptoms of cough and phlegm. Case 2 exhibited fibrous cavities on chest CT, with symptoms of hemoptysis, while excluding other diseases such as pulmonary tuberculosis and lung cancer. The clinical manifestations and imaging features of these two patients are consistent with the guidelines.
Pathology
The lung tissue biopsy in Case 2 revealed granulomatous inflammation, which is a histopathological characteristic change of mycobacteriosis.
Based on the clinical manifestations, etiology, imaging, and pathological results of both cases, the diagnosis of M. abscessus lung disease is confirmed.
Treatment
Drug treatment and Adverse Reaction Monitoring of M. abscessus Lung Disease
Drug treatment
M. abscessus demonstrates formidable multidrug resistance characterized by three distinct patterns: intrinsic (constitutive) resistance, acquired resistance, and inducible resistance.21 The intrinsic resistance primarily stems from its low-permeability cell wall22 (composed of peptidoglycan, arabinogalactan, and long-chain mycolic acids) and efflux systems.23 High-expression efflux pumps such as MmpL and Tap in the outer membrane substantially reduce intracellular antibiotic concentrations through active efflux mechanisms. Specifically, the MmpL efflux pump mediates cross-resistance between clofazimine and bedaquiline,24 while the Tap pump contributes to amikacin resistance.25 Efflux pump inhibitors including thioridazine, verapamil, and MmpL3 inhibitors may enhance antibiotic efficacy through efflux inhibition or cellular metabolic interference, presenting promising therapeutic strategies.21,23 Acquired resistance typically arises from genetic mutations (eg, in rrl (23S rRNA)26 and rrs (16S rRNA)27 and production of β-lactamase (BlaMab),28 conferring resistance to macrolides, aminoglycosides, and β-lactams. β-lactamase inhibitors such as avibactam,28 vaborbactam,29 durlobactam30 and relebactam31 can suppress BlaMab activity and potentiate β-lactam antibiotics (eg, meropenem, ceftaroline, sulopenem, imipenem-cilastatin and ceftazidime),28,29,31 though clinical validation remains pending. Inducible resistance is particularly prevalent with macrolides, associated with thymine at position 28 of the erm (41) gene (T28 genotype).32,33 Therefore, erm (41), rrl, and rrs gene testing are strongly recommended when administering macrolides or aminoglycosides.
In Case 1, the genetic characterization of M. abscessus revealed the erm (41) T28 genotype. In Case 2, while M. abscessus was cultured pre- and post-operatively, the absence of species identification and genetic testing precluded differentiation between persistent infection and disease recurrence. And there is currently study indicates that regardless of whether it is a recurrence or reinfection, the treatment plan remains the same as the initial treatment, depending on the susceptibility of the isolated strain to macrolide antibiotics.34 According to CLSI standards, the minimum inhibitory concentration (MIC) for macrolide-sensitive strains should be ≤2 μg/mL, but the MIC of this strain for clarithromycin is 4 μg/mL. Meanwhile, most isolates of MAB and MAO have active erm genes, which make them resistant to macrolides.35 However, almost all isolates of the MMA do not have active erm genes and are sensitive to macrolides. Based on this, we speculate that the cases of 1 and 2 may have been infected with MAB and/or MAO with active erm genes, and therefore both adopted treatment regimens targeting inducible macrolide-resistant M. abscessus.
Clinical guidelines and study suggested that for patients with infection-induced macrolide-resistant M. abscessus, the initial treatment regimen should include at least four combined drugs, including a macrolide and amikacin.9,36,37 Other optional drugs include imipenem/cilastatin, cefoxitin, tigecycline, clofazimine, and linezolid. The duration of this phase should be at least a month, with a recommendation to extend it to 3 to 6 months. The maintenance phase should include at least three orally active drugs, such as linezolid, minocycline, ciprofloxacin, moxifloxacin, rifabutin, or clofazimine, or the option of nebulized amikacin. The treatment should continue until the sputum culture results are negative and should be maintained for at least one year. Case 1 ultimately chose amikacin, imipenem and cilastatin sodium, moxifloxacin, minocycline, and clarithromycin for treatment for over 6 months in the initial phase, and in the maintenance phase, moxifloxacin, minocycline, and clarithromycin were used for 5 months, followed by moxifloxacin and minocycline for over 5 months. The treatment was ultimately successful, with no recurrence during the 4-month follow-up. Case 2 restarted treatment one year after surgery. In the initial phase, the patient was treated with amikacin, cefoxitin, tigecycline, clofazimine, and clarithromycin. However, treatment was discontinued due to intolerance from adverse drug reactions. Unfortunately, the patient passed away a month after discharge.
Both Case 1 and Case 2 included clarithromycin and amikacin in their treatment regimens. Clarithromycin is a macrolide antibiotic. However, it is not considered an effective antibacterial agent in this context, but rather as an immunomodulator,38 inhibiting inflammatory factors, reactive oxygen species (ROS), the formation of neutrophil extracellular traps, and leukotriene synthesis, thereby enhancing bactericidal effects. And some studies have shown that clarithromycin used in a multi-drug combination regimen for patients with macrolide-resistant infections has achieved good therapeutic outcomes,39,40 consistent with the results of Case 1. Amikacin is currently considered the second most important drug for treating M. abscessus,10,36 and its resistance is clearly correlated with the efficacy of treatment for mycobacteriosis. In addition, amikacin is usually sensitive and can significantly improve treatment success rates when combined with other antibiotics such as imipenem, cefoxitin, clarithromycin, ciprofloxacin, and linezolid.37,41 Furthermore, the inhaled formulation of amikacin (ALIS) has shown promising prospects in the treatment of drug-resistant M. abscessus infections, enhancing drug concentration at the site of infection while reducing systemic toxicity, providing a new treatment approach.42 Due to drug availability, we did not select ALIS for the maintenance phase.
Apart from the two core drugs, macrolides and amikacin, there is currently no standard combination regimen. There is currently evidence indicate that the combination of two β-lactam antibiotics (cefoxitin/imipenem, ceftolozane/imipenem, and ceftazidime/ceftolozane) can better inhibit D, D-transpeptidase,43 thereby inhibiting the synthesis of the mycobacterial cell wall, which is beneficial for killing NTM and provides a new direction for future treatments. However, our patient was initially treated with imipenem-cilastatin combined with cefoxitin.
Moxifloxacin shows relatively weak antibacterial activity against M. abscessus and is mainly used for maintenance therapy or as an alternative treatment in cases of drug allergy. Minocycline is a tetracycline drug, with tigecycline and doxycycline being its counterparts. Weihe Zhang found extremely high resistance rates of M. abscessus to doxycycline and minocycline in vitro, at 93% and 87.2%, respectively, but increased susceptibility to tigecycline with a resistance rate of only 7.2%.44 YongSoo Kwon also found that treatment regimens containing tigecycline showed significant improvements in symptoms and imaging results in M. abscessus lung disease, but the rate of microbiological improvement was poor, and adverse reactions were common.45 Therefore, caution is advised when selecting tigecycline for treatment. In Case 1, we chose a combination regimen of minocycline during the maintenance treatment phase, which showed good efficacy, but its effectiveness was inconsistent with the literature reports.41 On the other hand, in Case 2, we selected a combination regimen of tigecycline during the initial phase, resulting in intolerable adverse reactions, which were consistent with the safety reported.41
Monitoring of Adverse Drug Reactions
Due to the numerous types and quantities of medications for treating M. abscessus lung disease, as well as the long duration of treatment, nearly 80% of patients experience adverse reactions during treatment.46 Therefore, monitoring of adverse drug reactions is particularly important.
In the Case 1, the patient experienced thrombocytopenia from linezolid and an allergic reaction from cefoxitin while on medication. Tedizolid, a novel oxazolidinone antibiotic, might be a good alternative to linezolid.47 It has advantages in terms of antibacterial activity, side effects, and drug interactions. However, our patient did not choose tedizolid due to price and drug accessibility issues. After 18 d of using cefoxitin, the patient developed a fever and respiratory distress that were unbearable, leading to stopping the medication. This is consistent with reports stating that cefoxitin has poor tolerability, with an average use of only 22 d.48 However, the regimen also contained imipenem, which is also a β-lactam medcation. We could not determine whether imipenem was involved in the allergic reaction, but we still caution that the risk of adverse reactions may increase when similar drugs are used in combination, and close monitoring is required.
In Case 2, the patient developed gastrointestinal symptoms, including diarrhea, vomiting, and nausea, accompanied by liver injury. YongSoo Kwon reported that tigecycline, cefoxitin, amikacin, clarithromycin, and clofazimine can all cause gastrointestinal reactions such as nausea, vomiting, and diarrhea, but tigecycline has the highest incidence rate, reaching 85%–94.2%.49 Even after using antiemetic medications like ondansetron to help with tigecycline tolerance, gastrointestinal reactions still occurred at a rate of 77.1%, resulting in a 57.1% rate of stopping or reducing the dosage.45,50 Our patient initially showed improvement in diarrhea and vomiting symptoms after using tropisetron hydrochloride tablets, esomeprazole enteric-coated capsules, and bifidobacterium triple viable capsules. However, as the treatment duration extended, the improvement in symptoms was not significant, which is consistent with the above literature reports.45,50 Clarithromycin, clofazimine, and tigecycline can all cause liver injury. Clarithromycin can cause mild asymptomatic elevations in serum alanine aminotransferase (ALT) levels in about 1–2% of the population48 and can also lead to acute liver failure,51 especially when used concurrently with certain hepatotoxic antibiotics, which can exacerbate clarithromycin-induced liver injury.48,51 Tigecycline-induced liver injury is characterized by elevated serum ALT/AST and bilirubin levels, as well as hepatic failure.52 This is especially common in patients with high maintenance doses (200 mg/d), long treatment durations (more than 14 d), and the use of multiple hepatotoxic drugs, with an incidence rate as high as 5%–10.3%.50,53,54 Clofazimine itself is not associated with elevated serum aminotransferase levels or clinically significant acute liver injury during treatment, but its combined use with other hepatotoxic drugs such as clarithromycin and tigecycline can increase the risk of hepatotoxicity.55,56 Therefore, we conclude that the gastrointestinal reactions and liver damage in this patient are likely caused by the combined effects of several drugs.
In summary, when deciding on treatment for M. abscessus lung disease, clinicians must comprehensively consider multiple factors such as the type of NTM subspecies, the severity of the disease, the drug of sensitivity, pharmacokinetics/pharmacodynamics (PK/PD) characteristics, adverse reactions and interactions, patient tolerability, treatment costs, drug accessibility, etc. They should weigh the pros and cons and make comprehensive judgments.
Surgical Treatment
Surgical treatment has demonstrated significant effectiveness in the management of many diseases, especially in dealing with complex cases. Lung resection can serve as an adjuvant therapy for drug in specific patients with M. abscessus lung disease. Such patients should meet the following criteria: good cardiopulmonary function, able to tolerate surgery, with localized or isolated lesions, and with poor response to medical treatment or complications requiring surgical intervention, such as hemoptysis.9,57,58 Surgical options include segmentectomy, lobectomy, and pneumonectomy. After lung resection surgery, 99.5% of patients had negative sputum results, while 8.2% experienced microbial recurrence.59 Therefore, it is recommended to continue anti-NTM treatment until sputum culture results are continuously negative for at least one year. Surgical options include segmentectomy, lobectomy, and pneumonectomy. After lung resection surgery, it is still recommended to provide NTM treatment until the sputum culture results remain negative for more than a year.57,58 In Case 2, the patient had massive hemoptysis, which met the surgical indications. However, after the surgery, the patient did not get timely drug sensitivity testing or continue treatment for the mycobacterial infection as advised by the doctor, which led to the condition getting worse. One year later, a five-drug combination therapy including clarithromycin was chosen based on the drug sensitivity results, but the treatment still did not work. Therefore, although lung resection can effectively remove the lesion, it cannot completely guarantee the elimination of potential sources of infection in the body in patients with complex conditions, and surgical treatment should still be approached with caution.60 Postoperative combination with sensitive drug therapy is very necessary, and the duration of drug use should be based on the patient’s overall health, the extent of the infection, the type of surgery, the doctor’s skill level, how well the lesions were cleared, and how the patient is recovering.
Follow-Up Management
Management of Recurrence
A recurrence of NTM is a second episode of NTM occurring after a first episode had been considered cured. In particular, patients with a longer interval between initial diagnosis and treatment, multiple lung lobes affected, and failure to convert to negative sputum culture within 6 months after the initiation of treatment, as well as those with nodular bronchiectatic type, have a higher recurrence rate,61 ranging from 9–33%.62,63 Recurrence mainly occurs within one year after cure.64 Most recurrences are attributed to reinfection with new genotypes rather than recurrent infection with not the same strain. And data indicates that 78% of recurrences after the clearance of M. abscessus are caused by reinfection with different strains.63 Case 1 is about a bronchiectasis patient who did not get timely treatment after their initial diagnosis and has high recurrent risk factors. Four months after the initial diagnosis, the patient experienced reinfection with MAO. After treatment, there was no relapse in the 4 months following treatment, but they need close monitoring, and it is a good idea to do sputum mycobacterial cultures every 6 months.
Management of Complications
Patients with NTM lung disease often exhibit abnormal host defense functions and immunodeficiency. Additionally, their lung tissue structure is often damaged, accompanied by airflow obstruction. These factors create a favorable environment for fungal survival, making it easy to lead to secondary or concurrent Aspergillus infections.16,65 According to the onset time, Case 1 detected Aspergillus at the time of NTM lung disease diagnosis, while Case 2 was discovered 1.4 years later, and both findings occurred earlier than the 1.5–7 years reported in the literature.18 When two diseases coexist, the imaging usually presents as thickening of the lung cavity, surrounding infiltration, and fungal ball or aspergilloma. However, the imaging findings of Case 1 show interstitial changes in both lungs, which are inconsistent with the descriptions in the literature.65 In the treatment, the clinical improvement of patients is more related to the response to antifungal therapy, suggesting that antifungal treatment should be prioritized before treating NTM to avoid unnecessary interactions. In Case 1, to avoid delaying the condition, we added the antifungal agent voriconazole and discontinued clarithromycin. In Case 2, the sequence count of Aspergillus is relatively low, and we do not consider it a pathogenic organism at this time. Instead, we will enhance the monitoring of sputum fungal smears and cultures, serum G and GM tests, and Aspergillus IgG antibodies. Once Aspergillus infection is detected, azithromycin, which has less interaction with voriconazole, can be chosen as a substitute for clarithromycin.66
Preventive Measures
Environmental Control
Reducing exposure to NTM can decrease the risk of primary infection and recurrence after treatment.61 Therefore, high-risk individuals should minimize exposure to environments that may contain NTM, such as house dust, acidic and damp soil, water supply systems13,67–69 like showerheads, sink faucets, underground water pipes, indoor swimming pools, hot tubs, continuous positive airway pressure machines, humidifiers, and medicated bathtubs.15 Additionally, ventilation and disinfection should be enhanced.
Monitoring of High-Risk Populations
Early monitoring of high-risk populations is a key strategy for preventing NTM infections. In addition, the chronic obstructive pulmonary disease, bronchiectasis, cystic fibrosis, pneumoconiosis, pulmonary tuberculosis, alveolar proteinosis, gastroesophageal reflux, cystic fibrosis genotypes, and abnormal alpha-1 antitrypsin phenotypes can all predispose individuals to NTM disease,3,15,65,70,71 especially among patients with post-tuberculosis bronchiectasis and fibrotic cavity diseases, where NTM infections are more prominent.72 Therefore, screening for NTM should be strengthened among these populations to promptly identify NTM lung disease. For patients diagnosed with NTM lung disease, they should receive timely treatment with sensitive antibiotics in a sufficient variety, adequate dosage, and for the appropriate duration to prevent complications.
Strategies for Enhancing the Immune System
After an infection occurs, host factors seem to be key determinants of progression. Therefore, enhancing the body’s immunity is crucial. First, the use of medications that affect immunity should be minimized. Since tumor necrosis factor-α (TNF-α) is protective in NTM infections, which means TNF-α inhibitors like infliximab, etanercept, and adalimumab should be used less frequently.15,73,74 Drugs that affect immunity also include hormones, proton pump inhibitors, methotrexate.15,72
Secondly, reasonable nutrition, appropriate exercise, rehabilitation training, and good living habits can significantly improve an individual’s immune system.75 Furthermore, immune intervention measures for specific populations, such as vaccination and the use of immunomodulators, may also play a positive role in preventing NTM infections.
Patient Education and Self-Management
Patient education and self-management are important components in preventing NTM infections.76,77 It is essential to actively carry out a series of health science training with the theme of “NTM lung disease cognition-prevention-treatment-rehabilitation” to help patients master self-management methods, thereby enhancing their understanding and coping abilities towards the disease.
Conclusion and Prospect
Through clinical practice in M. abscessus lung disease, this article found that molecular biology technology mNGS has significant diagnostic value in species identification of NTM lung disease and detection of drug-resistance genes. Early initiation of standardized antimicrobial therapy upon diagnosis is crucial to prevent reinfection and disease progression. The treatment protocol should closely monitor adverse drug reactions, with routine tests including complete blood count, kidney function (urea nitrogen, creatinine), liver enzymes, and gastrointestinal symptoms (nausea, diarrhea); special drug monitoring includes aminoglycosides (vestibular function and hearing), chloramphenicol (skin and mucosal pigmentation), macrolides (hearing, QT interval), quinolones (photosensitivity, tendon damage), and β-lactams (allergic reactions). For complex cases, a combined treatment regimen of surgery and medication should be considered when necessary. Meanwhile, this article also emphasizes that follow-up management after the cure of NTM lung disease cannot be ignored.
By reviewing the literature, this article proposes further research directions for the diagnosis and treatment of M. abscessus lung disease. Future research should focus on new explorations of drug-resistance mechanisms and the discovery of new genes to promote the development of related fields. At the same time, efforts should be made to preserve the activity of existing antibacterial drugs, especially macrolide antibiotics and amikacin. Furthermore, the future work should also include the development of new therapeutic drugs, vaccines, natural products, or plant extracts, as well as the research and development of targeted agents for genes such as erm (41), whiB7, and MmpL3. Finally, the effectiveness of existing novel drugs (such as omadacycline, tedizolid, double β-lactam combinations, and bacteriophages) should be verified to address the challenges of NTM lung disease.
Consent for Publication
Written informed consent was obtained from the patient’s family of the deceased patient or the patient himself for the publication of any data included in this work. The cases’ details are open access and can be browsed without institutional approval.
Author Contributions
All authors made substantial contributions to the conception, study design, execution, acquisition of data, analysis, and interpretation; participated in drafting the manuscript or critically revising it for intellectual content; gave final approval of the version to be published; agreed to submit to the current journal; and take responsibility for all aspects of the work, ensuring integrity and accuracy.
Funding
The authors declare that no financial support has been received for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Prevots DR, Marshall JE, Wagner D, Morimoto K. Global epidemiology of nontuberculous mycobacterial pulmonary disease. Clinics Chest Med. 2023;44(4):675–721. doi:10.1016/j.ccm.2023.08.012
2. Nguyen MH, Haas MK, Kasperbauer SH, et al. nontuberculous mycobacterial pulmonary disease: patients, principles, and prospects. Clin Infect Dis. 2024;79(4):e27–e47. doi:10.1093/cid/ciae421
3. Liu Y, Ma X, Chen J, Wang H, Yu Z. Nontuberculous mycobacteria by metagenomic next-generation sequencing: three cases reports and literature review. Front Public Health. 2022. doi:10.3389/fpubh.2022.972280
4. Hindman H, Venkateswaran N, Yeaney G, Chung M. Recurrent nontuberculous mycobacterial endophthalmitis: a diagnostic conundrum. Clin Ophthalmol. 2014;837. doi:10.2147/opth.S56670
5. Kwan M, Tupler R. Recurrent nontuberculous mycobacterial tenosynovitis. Ochsner J. 2021;21(1):86–89. doi:10.31486/toj.19.0010
6. Yoo H, Choi SH, Yj K, Sj K, Yu C, Sj C. Recurrent bilateral breast abscess due to nontuberculous mycobacterial infection. J Breast Cancer. 2014;17(3):295. doi:10.4048/jbc.2014.17.3.295
7. Adjemian J, Olivier KN, Seitz AE, Holland SM, Prevots DR. Prevalence of nontuberculous mycobacterial lung disease in U.S. Medicare beneficiaries. Am J Respir Crit Care Med. 2012;185(8):881–886. doi:10.1164/rccm.201111-2016OC
8. Touré H, Durand N, Guénal I, Herrmann JL, Girard-Misguich F, Szuplewski S. Mycobacterium abscessus opsonization allows an escape from the defensin bactericidal action in drosophila. Microbiol Spectr. 2023;11(4):e0077723. doi:10.1128/spectrum.00777-23
9. Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Clin Infect Dis. 2020;71(4):905–913. doi:10.1093/cid/ciaa1125
10. Dedrick RM, Abad L, Storey N, et al. The problem of Mycobacterium abscessus complex: multi-drug resistance, bacteriophage susceptibility and potential healthcare transmission. Clin Microbiol Infect. 2023;29(10):1335.e9–1335.e16. doi:10.1016/j.cmi.2023.06.026
11. Lee MR, Sheng WH, Hung CC, Yu CJ, Lee LN, Hsueh PR. Mycobacterium abscessus complex infections in humans. Emerg Infect Dis. 2015;21(9):1638–1646. doi:10.3201/2109.141634
12. Gopalaswamy R, Shanmugam S, Mondal R, Subbian S. Of tuberculosis and non-tuberculous mycobacterial infections – a comparative analysis of epidemiology, diagnosis and treatment. J Biomed Sci. 2020;27(1). doi:10.1186/s12929-020-00667-6
13. Johansen MD, Herrmann JL, Kremer L. Non-tuberculous mycobacteria and the rise of Mycobacterium abscessus. Nat Rev Microbiol. 2020;18(7):392–407. doi:10.1038/s41579-020-0331-1
14. Lopeman RC, Harrison J, Desai M, Cox JAG. Mycobacterium abscessus: environmental Bacterium Turned Clinical Nightmare. Microorganisms. 2019;7(3). doi:10.3390/microorganisms7030090
15. Pathak K, Hart S, Lande L. Nontuberculous mycobacteria lung disease (NTM-LD): current recommendations on diagnosis, treatment, and patient management. Int J Gene Med. 2022;15:7619–7629. doi:10.2147/ijgm.S272690
16. Takeda K, Imamura Y, Takazono T, et al. The risk factors for developing of chronic pulmonary aspergillosis in nontuberculous mycobacteria patients and clinical characteristics and outcomes in chronic pulmonary aspergillosis patients coinfected with nontuberculous mycobacteria. Med Mycol. 2016;54(2):120–127. doi:10.1093/mmy/myv093
17. Tan Y, Su B, Shu W, et al. Epidemiology of pulmonary disease due to nontuberculous mycobacteria in Southern China, 2013-2016. BMC Pulm Med. 2018;18(1):168. doi:10.1186/s12890-018-0728-z
18. Phoompoung P, Chayakulkeeree M. Chronic pulmonary aspergillosis following nontuberculous mycobacterial infections: an emerging disease. J Fungi. 2020;6(4):346. doi:10.3390/jof6040346
19. Pasipanodya JG, Ogbonna D, Ferro BE, et al. Systematic review and meta-analyses of the effect of chemotherapy on pulmonary Mycobacterium abscessus outcomes and disease recurrence. Antimicrob Agents Chemother. 2017;61(11). doi:10.1128/aac.01206-17
20. Yao L, Gui X, Wu X, et al. Rapid Identification of nontuberculous mycobacterium species from respiratory specimens using nucleotide MALDI-TOF MS. Microorganisms. 2023;11(8). doi:10.3390/microorganisms11081975
21. Sethiya JP, Sowards MA, Jackson M, North EJ. MmpL3 inhibition: a new approach to treat nontuberculous mycobacterial infections. Int J Mol Sci. 2020;21(17):6202. doi:10.3390/ijms21176202
22. Guallar-Garrido S, Luquin M, Julián E. Analysis of the lipid composition of mycobacteria by thin layer chromatography. J Vis Exp. 2021;170. doi:10.3791/62368.
23. Mudde SE, Schildkraut JA, Ammerman NC, et al. Unraveling antibiotic resistance mechanisms in Mycobacterium abscessus: the potential role of efflux pumps. J Global Antimicrob Resist. 2022;31:345–352. doi:10.1016/j.jgar.2022.10.015
24. Gutiérrez AV, Richard M, Roquet-Banères F, Viljoen A, Kremer L. The TetR family transcription factor MAB_2299c regulates the expression of two distinct MmpS-MmpL efflux pumps involved in cross-resistance to clofazimine and bedaquiline in Mycobacterium abscessus. Antimicrob Agents Chemother. 2019;63(10). doi:10.1128/aac.01000-19
25. Wu M, Li B, Guo Q, et al. Detection and molecular characterisation of amikacin-resistant Mycobacterium abscessus isolated from patients with pulmonary disease. J Global Antimicrob Resist. 2019;19:188–191. doi:10.1016/j.jgar.2019.05.016
26. Bastian S, Veziris N, Roux AL, et al. Assessment of clarithromycin susceptibility in strains belonging to the Mycobacterium abscessus group by erm(41) and rrl sequencing. Antimicrob Agents Chemother. 2011;55(2):775–781. doi:10.1128/aac.00861-10
27. Prammananan T, Sander P, Brown BA, et al. A single 16S ribosomal RNA substitution is responsible for resistance to amikacin and other 2-deoxystreptamine aminoglycosides in Mycobacterium abscessus and Mycobacterium chelonae. J Infect Dis. 1998;177(6):1573–1581. doi:10.1086/515328
28. Andersson V, Fröberg G, Dahl VN, et al. The in vitro activity of carbapenems alone and in combination with β-lactamase inhibitors against difficult-to-treat mycobacteria; Mycobacterium tuberculosis, Mycobacterium abscessus, and Mycobacterium avium complex: a systematic review. Int J Mycobacteriol. 2023;12(3):211–225. doi:10.4103/ijmy.ijmy_131_23
29. Chen L, Shashkina E, Kurepina N, Calado Nogueira de Moura V, Daley CL, Kreiswirth BN. In vitro activity of cefoxitin, imipenem, meropenem, and ceftaroline in combination with vaborbactam against Mycobacterium abscessus. Antimicrob Agents Chemother. 2024;68(5):e0017424. doi:10.1128/aac.00174-24
30. Dousa KM, Shin E, Kurz SG, et al. Synergistic effects of sulopenem in combination with cefuroxime or durlobactam against Mycobacterium abscessus. mBio. 2024;15(6):e0060924. doi:10.1128/mbio.00609-24
31. Vogiatzoglou AI, Hadji Μitrova M, Papadaki E, et al. Combination of imipenem-cilastatin-relebactam and amoxicillin in the antibiotic regimen in two cases of Mycobacterium abscessus lung infection. Cureus. 2024. doi:10.7759/cureus.65112
32. Richard M, Gutiérrez AV, Kremer L. Dissecting erm(41)-mediated macrolide-inducible resistance in Mycobacterium abscessus. Antimicrob Agents Chemother. 2020;64(2). doi:10.1128/aac.01879-19
33. Yoshida S, Tsuyuguchi K, Kobayashi T, Inoue Y, Suzuki K. Comparison of drug-susceptibility patterns and gene sequences associated with clarithromycin and azithromycin resistance in Mycobacterium abscessus complex isolates and evaluation of the accumulation of intrinsic macrolide resistance. J Med Microbiol. 2021;70(3). doi:10.1099/jmm.0.001326
34. Diel R, Nienhaus A, Ringshausen FC, et al. Microbiologic outcome of interventions against mycobacterium avium complex pulmonary disease: a systematic review. Chest. 2018;153(4):888–921. doi:10.1016/j.chest.2018.01.024
35. Nash KA, Brown-Elliott BA, Wallace RJ. A novel gene, erm(41), confers inducible macrolide resistance to clinical isolates of Mycobacterium abscessus but is absent from mycobacterium chelonae. Antimicrob Agents Chemother. 2009;53(4):1367–1376. doi:10.1128/aac.01275-08
36. Griffith DE, Daley CL. Treatment of Mycobacterium abscessus Pulmonary Disease. Chest. 2022;161(1):64–75. doi:10.1016/j.chest.2021.07.035
37. Rahi MS, Reyes SP, Parekh J, Gunasekaran K, Amoah K, Rudolph D. Disseminated Mycobacterium abscessus infection and native valve endocarditis. Respir Med Case Rep. 2021;32:101331. doi:10.1016/j.rmcr.2020.101331
38. Pohl K, Grimm XA, Caceres SM, et al. Mycobacterium abscessus clearance by neutrophils is independent of autophagy. Infect Immun. 2020;88(8). doi:10.1128/iai.00024-20
39. Safe IP, Macedo V, Marcelo W, et al. Nontuberculous mycobacterial infections after aesthetic procedures: comparison of clinical features and treatment. J Clin Aesthet Dermatol. 2021;14(3):46–49.
40. Yoshida S, Tsuyuguchi K, Suzuki K, et al. Rapid identification of strains belonging to the Mycobacterium abscessus group through erm(41) gene pyrosequencing. Diagn Microbiol Infect Dis. 2014;79(3):331–336. doi:10.1016/j.diagmicrobio.2014.04.001
41. Duan HF, Chu NH, Qf W, Wang J, Huang HR, Liang Q. Mycobacterium abscessus group lung disease: case reports and review of the literature. Zhonghua Jie He He Hu Xi Za Zhi. 2013;36(9):671–674.
42. Siegel SAR, Griffith DE, Philley JV, et al. Open-label trial of amikacin liposome inhalation suspension in Mycobacterium abscessus lung disease. Chest. 2023;164(4):846–859. doi:10.1016/j.chest.2023.05.036
43. Longo BM, Trunfio M, Calcagno A. Dual β-lactams for the treatment of Mycobacterium abscessus: a review of the evidence and a call to act against an antibiotic nightmare. J Antimicrob Chemother. 2024;79(11):2731–2741. doi:10.1093/jac/dkae288
44. Zhang W, Dong L, Men P, et al. In vitro antimicrobial activity of doxycycline, minocycline, and tigecycline against Mycobacterium abscessus complex: a meta-analysis study. Diagn Microbiol Infect Dis. 2024;110(2):116435. doi:10.1016/j.diagmicrobio.2024.116435
45. Wallace RJ, Dukart G, Brown-Elliott BA, Griffith DE, Scerpella EG, Marshall B. Clinical experience in 52 patients with tigecycline-containing regimens for salvage treatment of Mycobacterium abscessus and Mycobacterium chelonae infections. J Antimicrob Chemother. 2014;69(7):1945–1953. doi:10.1093/jac/dku062
46. Chen J, Zhao L, Mao Y, et al. Clinical efficacy and adverse effects of antibiotics used to treat Mycobacterium abscessus pulmonary disease. Front Microbiol. 2019;10:1977. doi:10.3389/fmicb.2019.01977
47. Gao X, Ding C, Xie D, et al. Contezolid-containing regimen successfully treated multiple drug resistance Mycobacterium abscessus complex infection of skin: a case report and literature review. Infect Drug Resist. 2024;17:1243–1249. doi:10.2147/idr.S453541
48. Woodhead JL, Yang K, Oldach D, et al. Analyzing the mechanisms behind macrolide antibiotic-induced liver injury using quantitative systems toxicology modeling. Pharm Res. 2019;36(3):48. doi:10.1007/s11095-019-2582-y
49. Dalcolmo M, Gayoso R, Sotgiu G, et al. Effectiveness and safety of clofazimine in multidrug-resistant tuberculosis: a nationwide report from Brazil. Eur Respir J Mar. 2017;49(3). doi:10.1183/13993003.02445-2016
50. Shi X, Zuo C, Yu L, et al. Real-world data of tigecycline-associated drug-induced liver injury among patients in China: a 3-year retrospective study as assessed by the updated RUCAM. Front Pharmacol. 2021;12:761167. doi:10.3389/fphar.2021.761167
51. Sharma NR, Wagle A, Bist M, et al. Clarithromycin-induced acute liver injury in a patient with positive Helicobacter pylori: a case report and review of the literature. Ann Med Surg. 2023;85(9):4629–4632. doi:10.1097/ms9.0000000000001135
52. Wei C, Liu Y, Jiang A, Wu B. A pharmacovigilance study of the association between tetracyclines and hepatotoxicity based on Food and Drug Administration adverse event reporting system data. Int J Clin Pharmacy. 2022;44(3):709–716. doi:10.1007/s11096-022-01397-5
53. Kwon YS, Levin A, Kasperbauer SH, Huitt GA, Daley CL. Efficacy and safety of tigecycline for Mycobacterium abscessus disease. Respir Med. 2019;158:89–91. doi:10.1016/j.rmed.2019.10.006
54. Yu Z, Zhao Y, Jin J, Zhu J, Yu L, Han G. Prevalence and risk factors of tigecycline-induced liver injury: a multicenter retrospective study. Int J Infect Dis. 2022;120:59–64. doi:10.1016/j.ijid.2022.04.024
55. Clofazimine. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. National Institute of Diabetes and Digestive and Kidney Diseases; 2012.
56. Saint-Marc T, Marneff E, Touraine JL. Mycobacterium avium intracellulare infections. Treatment with a clarithromycin-clofazimine combination. 18 cases. Presse Med. 1993;22(38):1903–1907.
57. Huang HL, Liu CJ, Lee MR, et al. Surgical resection is sufficient for incidentally discovered solitary pulmonary nodule caused by nontuberculous mycobacteria in asymptomatic patients. PLoS One. 2019;14(9):e0222425. doi:10.1371/journal.pone.0222425
58. Mitchell JD. Surgical treatment of pulmonary nontuberculous mycobacterial infections. Thorac surg clin. 2019;29(1):77–83. doi:10.1016/j.thorsurg.2018.09.011
59. Togo T, Atsumi J, Hiramatsu M, et al. Residual destructive lesions and surgical outcome in mycobacterium avium complex pulmonary disease. Ann Thorac Surg. 2020;110(5):1698–1705. doi:10.1016/j.athoracsur.2020.04.034
60. Haworth CS, Banks J, Capstick T, et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax. 2017;72(Suppl 2):ii1–ii64. doi:10.1136/thoraxjnl-2017-210927
61. Lee BY, Kim S, Hong Y, et al. Risk factors for recurrence after successful treatment of Mycobacterium avium complex lung disease. Antimicrob Agents Chemother. 2015;59(6):2972–2977. doi:10.1128/aac.04577-14
62. Kang N, Jhun BW. Long-term outcomes of adjunctive lung resection for nontuberculous mycobacteria pulmonary disease. Open Forum Infect Dis. 2024;11(7):ofae345. doi:10.1093/ofid/ofae345
63. Kim JY, Lee HW, Yim JJ, Kwak N. Outcomes of adjunctive surgery in patients with nontuberculous mycobacterial pulmonary disease: a systematic review and meta-analysis. Chest. 2023;163(4):763–777. doi:10.1016/j.chest.2022.09.037
64. Li Q, Li H, An J, et al. Transition between Mycobacterium tuberculosis and nontuberculous mycobacteria in recurrent “tuberculosis” patients. Eur J Clin Microbiol Infect Dis. 2022. doi:10.1007/s10096-022-04477-6
65. Fayos M, Silva JT, López-Medrano F, Aguado JM. non-tuberculous mycobacteria and aspergillus lung co-infection: systematic review. J Clin Med. 2022;11(19):5619. doi:10.3390/jcm11195619
66. Purkins L, Wood N, Ghahramani P, Kleinermans D, Layton G, Nichols D. No clinically significant effect of erythromycin or azithromycin on the pharmacokinetics of voriconazole in healthy male volunteers. Br. J. Clin. Pharmacol. 2003;56(s1):30–36. doi:10.1046/j.1365-2125.2003.01996.x
67. Carter KK, Lundgren I, Correll S, et al. First United States outbreak of Mycobacterium abscessus hand and foot disease among children associated with a wading pool. J Pediatric Infect Dis Soc. 2019;8(4):291–296. doi:10.1093/jpids/piy036
68. Honda JR, Hasan NA, Davidson RM, et al. Environmental nontuberculous mycobacteria in the Hawaiian Islands. PLoS Negl Trop Dis. 2016;10(10):e0005068. doi:10.1371/journal.pntd.0005068
69. Feazel LM, Baumgartner LK, Peterson KL, Frank DN, Harris JK, Pace NR. Opportunistic pathogens enriched in showerhead biofilms. Proc Natl Acad Sci U S A. 2009;106(38):16393–16399. doi:10.1073/pnas.0908446106
70. Adjemian J, Olivier KN, Prevots DR. Epidemiology of pulmonary nontuberculous mycobacterial sputum positivity in patients with cystic fibrosis in the United States, 2010–2014. Ann Am Thoracic Soc. 2018;15(7):817–826. doi:10.1513/AnnalsATS.201709-727OC
71. Furuuchi K, Morimoto K, Yoshiyama T, et al. Interrelational changes in the epidemiology and clinical features of nontuberculous mycobacterial pulmonary disease and tuberculosis in a referral hospital in Japan. Respir Med. 2019;152:74–80. doi:10.1016/j.rmed.2019.05.001
72. McShane PJ, Glassroth J. Pulmonary disease due to nontuberculous mycobacteria. Chest. 2015;148(6):1517–1527. doi:10.1378/chest.15-0458
73. Catherinot E, Roux A-L, Vibet M-A, et al. Inhaled therapies, azithromycin and Mycobacterium abscessus in cystic fibrosis patients. Eur Respir J. 2013;41(5):1101–1106. doi:10.1183/09031936.00065612
74. Binder AM, Adjemian J, Olivier KN, Prevots DR. Epidemiology of nontuberculous mycobacterial infections and associated chronic macrolide use among persons with cystic fibrosis. Am J Respir Crit Care Med. 2013;188(7):807–812. doi:10.1164/rccm.201307-1200OC
75. Zhan QY, Xie LX, Wang C. Promoting critical care system and capacity building in pulmonary and critical care medicine subspecialties. Zhonghua Yi Xue Za Zhi. 2023;103(40):3149–3151. doi:10.3760/cma.j.cn112137-20230602-00919
76. Kapnadak SG, Hisert KB, Pottinger PS, Limaye AP, Aitken ML. Infection control strategies that successfully controlled an outbreak of Mycobacterium abscessus at a cystic fibrosis center. Am J Infect Control. 2016;44(2):154–159. doi:10.1016/j.ajic.2015.08.023
77. Wang XY, Jia QN, Li J. Treatment of non-tuberculosis mycobacteria skin infections. Front Pharmacol. 2023;14:1242156. doi:10.3389/fphar.2023.1242156
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nanotechnology: A Promising Approach for Cancer Diagnosis, Therapeutics and Theragnosis
Dessale M, Mengistu G, Mengist HM
International Journal of Nanomedicine 2022, 17:3735-3749
Published Date: 26 August 2022
Updated Perspectives on the Diagnosis and Management of Onychomycosis
Falotico JM, Lipner SR
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1933-1957
Published Date: 15 September 2022
Nontuberculous Mycobacteria Lung Disease (NTM-LD): Current Recommendations on Diagnosis, Treatment, and Patient Management
Pathak K, Hart S, Lande L
International Journal of General Medicine 2022, 15:7619-7629
Published Date: 1 October 2022
Challenges in the Early Diagnosis and Treatment of Chronic Inflammatory Demyelinating Polyradiculoneuropathy in Adults: Current Perspectives
van Doorn IN, Eftimov F, Wieske L, van Schaik IN, Verhamme C
Therapeutics and Clinical Risk Management 2024, 20:111-126
Published Date: 14 February 2024
Managing Opioid Withdrawal Symptoms During the Fentanyl Crisis: A Review
Weber AN, Trebach J, Brenner MA, Thomas MM, Bormann NL
Substance Abuse and Rehabilitation 2024, 15:59-71
Published Date: 10 April 2024