")
Back to Journals » Journal of Pain Research » Volume 18
The Applications and Prescriptions of Motion Style Acupuncture Treatment for Musculoskeletal Pain: A Scoping Review of Clinical Controlled Trials
Authors Chen Y , Zhu F , Zhu Y , Duan Y, Bai Z
Received 21 March 2025
Accepted for publication 24 June 2025
Published 28 June 2025 Volume 2025:18 Pages 3275—3287
DOI https://doi.org/10.2147/JPR.S529676
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yetong Chen,1 Fenglin Zhu,1 Yang Zhu,1 Yucheng Duan,1,2 Zhenmin Bai1
1School of Sports Medicine and Rehabilitation, Beijing Sport University, Beijing, People’s Republic of China; 2Research Laboratory of Physical Training, Beijing Research Institute of Sport Science, Beijing, People’s Republic of China
Correspondence: Yucheng Duan, Email [email protected] Zhenmin Bai, Email [email protected]
Purpose: Motion style acupuncture treatment (MSAT) is a new treatment which comprises acupuncture therapy and exercise therapy. Musculoskeletal pain is highly prevalent and a significant contributor to global disability and disease. In recent years, an increasing number of studies have applied MSAT to the management of musculoskeletal pain. This scoping review systematically collected clinical studies on the use of MSAT in the management of different musculoskeletal pain conditions and identified any adverse events.
Methods: Seven databases were searched from their inception through to 2024. RCTs and CCTs on MSAT for pain conditions meeting the inclusion criteria were identified. Data were extracted on patients, interventions, details of MSAT, control treatments and outcomes.
Results: This review included 36 clinical studies. These included, 27 (75%) RCTs and 9 (25%) CCTs, treating 2620 patients with 16 different pain-related diseases or symptoms. The most frequently reported conditions were acute lumbar sprain (8, 22.22%), adhesive capsulitis (5, 13.89%). Selection of movement and acupuncture was different in the treatment of different musculoskeletal pain conditions. MSAT was used alone in about one-third of the studies and of the remaining studies it was combined with other treatment. All studies reported relevant outcomes of pain and 9 (25%) adverse events.
Conclusion: MSAT, which seems to be a promising intervention used in the management of diverse musculoskeletal pain conditions, has been gradually studied in China and Korea. However, given the variety of study designs and reported treatment outcomes, conclusions about the evidence for MSAT for specific conditions are not possible at this stage.
Keywords: motion style acupuncture treatment, musculoskeletal pain, scoping review
Introduction
Musculoskeletal pain, defined as “persistent or recurrent pain that arises as part of a disease process directly affecting bone(s), joint(s), muscle(s), or related soft tissue(s)”,1 is the most common cause of disability with significant economical and societal implications globally.2 The prevalence of musculoskeletal pain was approximately 30% (range of 13.5–47%) from 23 population studies conducted in 15 different countries.3 Considering the different aetiologies and underlying physiopathological mechanisms, musculoskeletal pain is categorized into nociceptive pain, neuropathic pain, and nociplastic pain.4 Clinically, there are different manifestations of pain, such as burning sensations, stabbing pains, electric shock-like sensations, and sharp pains.2 Musculoskeletal pain can effect sleep5 and mood.6 Moreover, it can significantly limit one’s mobility and participation in regular physical activities, thereby increasing the risk of developing chronic diseases.7 In the management of musculoskeletal pain, pharmacotherapy is common used.8 However, the effectiveness of the currently available pharmacotherapy in the treatment of musculoskeletal pain conditions is unsatisfactory.9 In addition, the potential for adverse effects needs to be taken into account. Accordingly, the implementation of preventative strategies and physical tools are recommended in recent guidelines to minimize the use of pharmacotherapy.8 Non-pharmacological therapy includes manual therapy,10 therapeutic exercise,11 acupuncture12 and so on. As for acupuncture, many clinical trials have validated the effectiveness of acupuncture in the treatment of musculoskeletal pain.13 After the development of acupuncture, a novel acupuncture treatment which is named motion style acupuncture treatment has emerged. MSAT, the combination of acupuncture therapy and exercise therapy, requests the patient to exercise actively or passively, while needles are left in the body. The analgesic effects of acupuncture are mediated through the modulation of neuronal activity in the central nervous system (CNS). Specifically, the release of endogenous opioids, 5-hydroxytryptamine (5-HT), and norepinephrine in the CNS, which are induced by peripheral stimuli, is thought to play a crucial role in the regulation of both inflammatory and neuropathic pain. MSAT reinforces the stimulus quantity of acupuncture by moving the needled muscles.14 Through extensive activation of the brain,15 it provides a greater analgesic effect with neuronal modulation in the CNS than conventional acupuncture therapy.14 Due to this mechanism, MSAT is suitable for a wide range of musculoskeletal disorders, with the effect of relieving pain, improving the range of motion of joints and aiding in the recovery of functions.16 Furthermore, in the clinical application, MSAT is widely used to reduce musculoskeletal pain.17 However, MSAT used in the management of musculoskeletal pain is different.
Data of scoping review can be used to inform future clinical trials in order to prioritize conditions or treatment regimens. Scoping reviews can also be precursors to conducting systematic review and therefore may be an appropriate approach to explore existing evidence for MSAT and its use in reducing musculoskeletal pain. This review comprehensively searched multiple databases to provide a thorough overview of the current applications of MSAT in the management of different musculoskeletal pain conditions. The study aimed to explore which specific musculoskeletal pain conditions MSAT has been applied to, and what the movement therapy and acupuncture prescriptions in MSAT are for these conditions. By listing and analyzing the commonly used prescriptions for each type of musculoskeletal pain conditions, this review offers valuable references for the clinical application of MSAT.
Materials and Methods
Study Registration
This review was registered in OSF (OSF registration DOI:https://doi.org/10.17605/OSF.IO/5MDX2). It is reported to follow methodological guidance for the conduct of scoping reviews.18,19
Eligibility Criteria
This scoping review used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the PRISMA Extension for Scoping Reviews (PRISMA-ScR) guidelines.20,21
Types of Studies
Relatively published clinical studies included randomized controlled trials (RCTs), clinical controlled trials (CCTs) in Chinese or English.
Types of Patients
Patients with any musculoskeletal pain-related diseases/symptoms were eligible. Both primary and associated symptoms were included.
Types of Interventions
Experimental interventions involving a combination of acupuncture and movement therapy were eligible. Those studies in which acupuncture therapy and movement therapy were considered separate strategies were excluded. Control interventions excluding MSAT, such as manual therapy and pharmacological therapy, were eligible.
Types of Outcome Measures
Studies were included if they reported outcomes of any pain-related symptom as either a primary or a secondary outcome.
Literature Search
Four English and three Chinese databases were searched from their inception through to 5 December 2024. An supplementary file provides the complete search strategy and results for all searched databases (see Supplementary file). In addition, relevant literature cited in the searched literature was also included in this research. All the clinical controlled studies finally included in this review were listed in the supplementary file.
Databases were following:
- MEDLINE (https://pubmed.ncbi.nlm.nih.gov/)
- Cochrane Library (https://www.cochranelibrary.com/library)
- Web of Science (https://webofscience.com/wos/alldb/basic-search)
- EBSCO (https://www.ebsco.com/)
- China Network Knowledge Infrastructure (CNKI) (http://www.cnki.net/)
- VIP Database (https://qikan.cqvip.com/)
- Wangfang Data (https://www.wanfangdata.com.cn/)
The first stage of literature screening was screening of titles and abstracts by using Zotero. The second stage of literature screening was reading potentially eligible literature in full to determine whether they met the eligible criteria.
Data Extraction and Analysis
Data was extracted into a pre-designed electronic form by using Microsoft Excel 2016.
The data extraction form was followed the PRISMA and PICO framework.22 The extracted data included bibliometric data (published year, authors, journal, origin, published language, study type), patients (sample size, gender, age, pain area, disease/symptom), interventions (movement, acupoints, duration, frequency, treatment period, comparisons) and outcomes (symptom reduction, adverse events).
These data were analyzed descriptively by calculating frequencies and percentages. After being integrated into Microsoft Excel 2016, data were represented graphically using GraphPad 10. All tables were made using Microsoft Word 2016.
Results
Literature Search
A total of 2,927 records were retrieved from literature search. Any duplicates were excluded, and the remaining studies were assessed for eligibility. The flowchart shows the selection process (Figure 1). At the end, 36 full-text articles were included in this review.23–58
 |
Figure 1 Flowchart of literature search. |
Bibliometric Information
The supplementary file shows the figures of bibliometric information (see Supplementary file). Firstly, the 36 studies included 27 (75%) RCTs and 9 (25%) CCTs. The second earliest RCT was published in 2011. The range of published year was from 2011 to 2024. From 2011 to 2018, 10 (27.78%) clinical studies were published. From 2019 to 2024, 26 (72.22%) clinical studies were published. There was an increasing overall trend in the number of publications year by year. In addition, 30 (83.33%) articles were published in Chinese, and 6 (16.67%) articles were published in English. Furthermore, all these article were conducted in two countries-China (32, 88.89%), Korea (4, 11.11%).
Patients
In total, 2,620 patients participated in the 36 studies. For trials (RCTs n=27 and CCTs n=9), study sample sizes ranged from 46 to 164 (median: 72; average: 73). Among the 36 studies, a total of 32 (88.89%) studies reported gender (male: 1196, 45.65%; female: 1152, 43.97%) and 34 (94.44%) studies reported age. Thirty-four (94.44%) studies reported the duration of disease, and the duration of disease reported in 11 (30.56%) studies was within 7 days. All these studies reported the duration of treatment with the range from 1 day to 6 weeks, 3 (8.33%) studies applied one-off treatment, and 34 (94.44%) studies applied treatment within 1 month.
There were 6 pain areas in the 36 studies which covered 16 different diseases/symptoms. And the number of pain areas were counted in Figure 2. Low back pain (LBP) (18, 50%) was the most frequently reported, followed by shoulder pain (7, 19.44%), neck pain (4, 11.11%), knee pain (4, 11.11%), heel pain (2, 5.56%) and wrist pain (1, 2.78%).
 |
Figure 2 Pain area and disease/symptom. |
Interventions
Selection of Acupoints and Duration
All studies reported their selection of acupoints and duration which was shown in Figure 3. In neck pain, the most frequently chosen acupoint was SI3 (2, 40%), and the selected duration was 20min (n=2). In shoulder pain, the most frequently chosen acupoints were ST38 (2, 28.57%) for 20min (n=1) and 40min (n=1), GB34 (2, 28.57%) for 10min (n=1) and 20min (n=1), Ashi point (2, 28.57%) for 10min (n=1) and 30min (n=1). In LBP, the most frequently chosen acupoints were EX-UE7 (6, 33.33%) for 5min (n=1), 10min (n=1), 15–20min (n=1), 20min (n=2), 30min (n=1), SI3 (5, 27.78%) for 20min (n=1), 20–30min (n=1), 30min (n=3), LR2 (3, 16.67%) for 10min (n=1), 15min (n=1), 20min (n=1), LI11 (3, 16.67%) for 15min (n=1), 20min (n=1), 30min (n=1), GV16 (2, 11.11%) for 15min (n=1), 20min (n=1), LI10 (2, 11.11%) for 10min (n=1), 30min (n=1), DU26 (2, 11.11%) for 15–20min (n=1), 20–30min (n=1), Ashi point (2, 11.11%) for 15min (n=1) and 30min (n=1). In knee pain, the most frequently chosen acupoints were GB34 (2, 50%) for 30min (n=2), SP9 (2, 50%) for 30min (n=2), ST36 (2, 50%) for 30min (n=2), Ashi point (2, 50%) for 20min (n=1) and 30min (n=1).
 |
Figure 3 Conditions, selection of acupoints and movement. |
Selection of Movement
Movement selection for each disease/symptom was shown in Figure 3. Overall, all studies applied active movement therapy, one of these studies applied rehabilitation technique. In neck pain, active movement of the head and neck in all directions was included. As for shoulder pain, active movement of the shoulder in adduction and abduction, internal and external rotation was included. In LBP, McKenzie therapy, one of rehabilitation techniques, was applied in the treatment of nonspecific LBP, walking was applied in all studies of acute LBP. In the treatment of knee osteoarthritis, 2 (66.67%) studies applied isometric contraction of the quadriceps femoris. In heel pain, heel stomping and walking were applied in all these studies of heel pain.
Frequency and Treatment Period
In the study on wrist pain, the treatment frequency was set at three times per week, with the treatment period of two weeks. In the studies on shoulder pain, the most commonly used treatment frequencies were once every two days (2, 28.57%) and once a day (2, 28.57%), and the most commonly used treatment periods were 10 days (2, 28.57%) and 2 weeks (2, 28.57%). In the studies on neck pain, the most commonly used treatment frequency was once a day (3, 75%), and the treatment periods were 3 days (1, 25%), 6 days (1, 25%), 2 weeks (1, 25%), 30 days (1, 25%). In the studies on low back pain, the most commonly used treatment frequencies were once a day (9, 50%), one-off (3, 16.67%), once every two days (2, 11.11%), five times per week (2, 11.11%), and the most commonly used treatment periods were 3 days (4, 22.22%), 2 weeks (4, 22.22%), one-off (3, 16.67%), 14 days (2, 11.11%). In the studies on knee pain, the most commonly used treatment frequency was once every two days (2, 50%), and the most commonly used treatment period was 4 weeks (2, 50%). In the studies on heel pain, the most commonly used treatment frequency was once every two days (2, 100%), and the treatment periods were 14 days (1, 50%), 20 days (1, 50%).
Treatments and Comparators
The specific components of the treatment and intervention are shown in Table 1. In the terms of treatments used in the 36 studies, 13 (36.11%) used MSAT alone and the others used MSAT combined with other treatments. And it is shown that there are 3 kinds of MSAT included MSAT, T-MSAT (1, 4.2%), PL-MSAT (1, 4.2%). T-MSAT refers to the treatment in which patients exercise with inserted acupuncture needles after traction is applied to the body using a device.30 PL-MSAT is the combination of MSAT and progressive loading exercise.31 CAT (12, 33.33%), pharmacological therapy including capsule intake (5, 13.89%) and IKM (3, 8.33%) were the most commonly used control treatments. In the included studies, it is found that MSAT is composed of two elements, acupuncture and movement, and there are various kinds of each element. In the element of acupuncture, eye acupuncture (1, 2.78%), scalp acupuncture (1, 2.78%), fire needling (2, 5.56%) and warm - needling moxibustion (2, 5.56%) are included. In the element of movement, rehabilitation technique such as McKenzie therapy (1, 2.78%) is included.
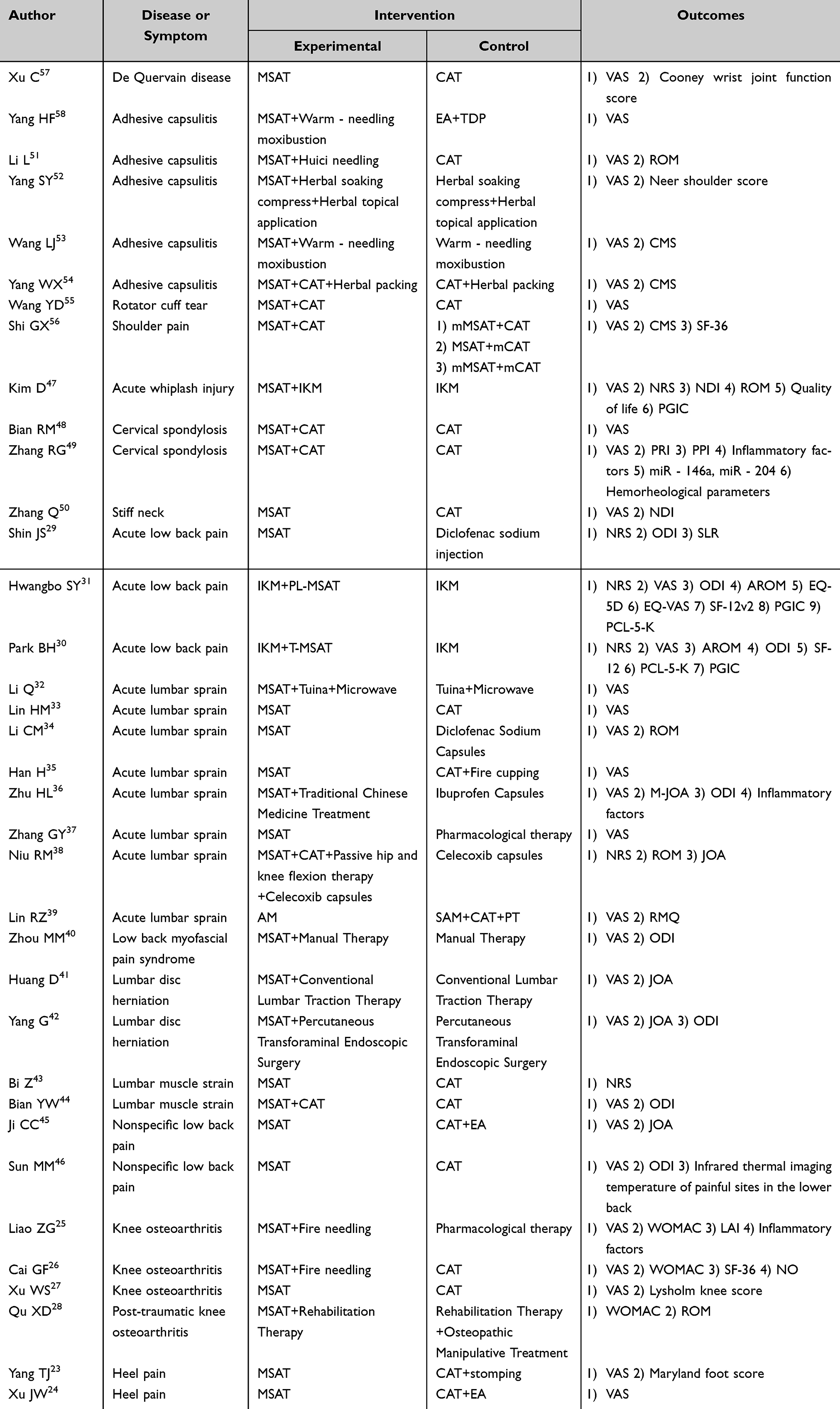 |
Table 1 Details of interventions and Outcomes |
Treatment Effects and Side Effects
Thirty-two (88.89%) studies used VAS as an index to measure the efficacy of pain. Among them, 19 (59.38%) studies reported the within-group differences. Seven (21.88%) studies had a P value of less than 0.01, and 12 (37.5%) studies had a P value of less than 0.05. Among the 32 studies that reported between-group differences, 1 (3.13%) study had a P value of 0.01, 16 (50%) studies had P value <0.01, 14 (43.75%) studies had P value <0.05, and 1 (3.13%) study had a P value >0.05. Six (16.67%) studies used NRS as an index to measure the efficacy of pain. Among these, 1 (16.67%) study reported within-group differences with a P value <0.01. All 6 studies reported statistically significant between-group differences in pain assessment. Specifically, 4 (66.67%) studies demonstrated strong significance (p < 0.01), and 2 (33.33%) studies showed conventional significance (p < 0.05).
Nine (25%) studies reported outcomes on adverse events, 2 (22.22%) studies found no adverse events. Three (33.33%) studies reported patients in the intervention group having dizziness. The remaining 4 studies reported adverse events from MSAT as well as events from other interventions during the treatment, which are shown in Table 2.
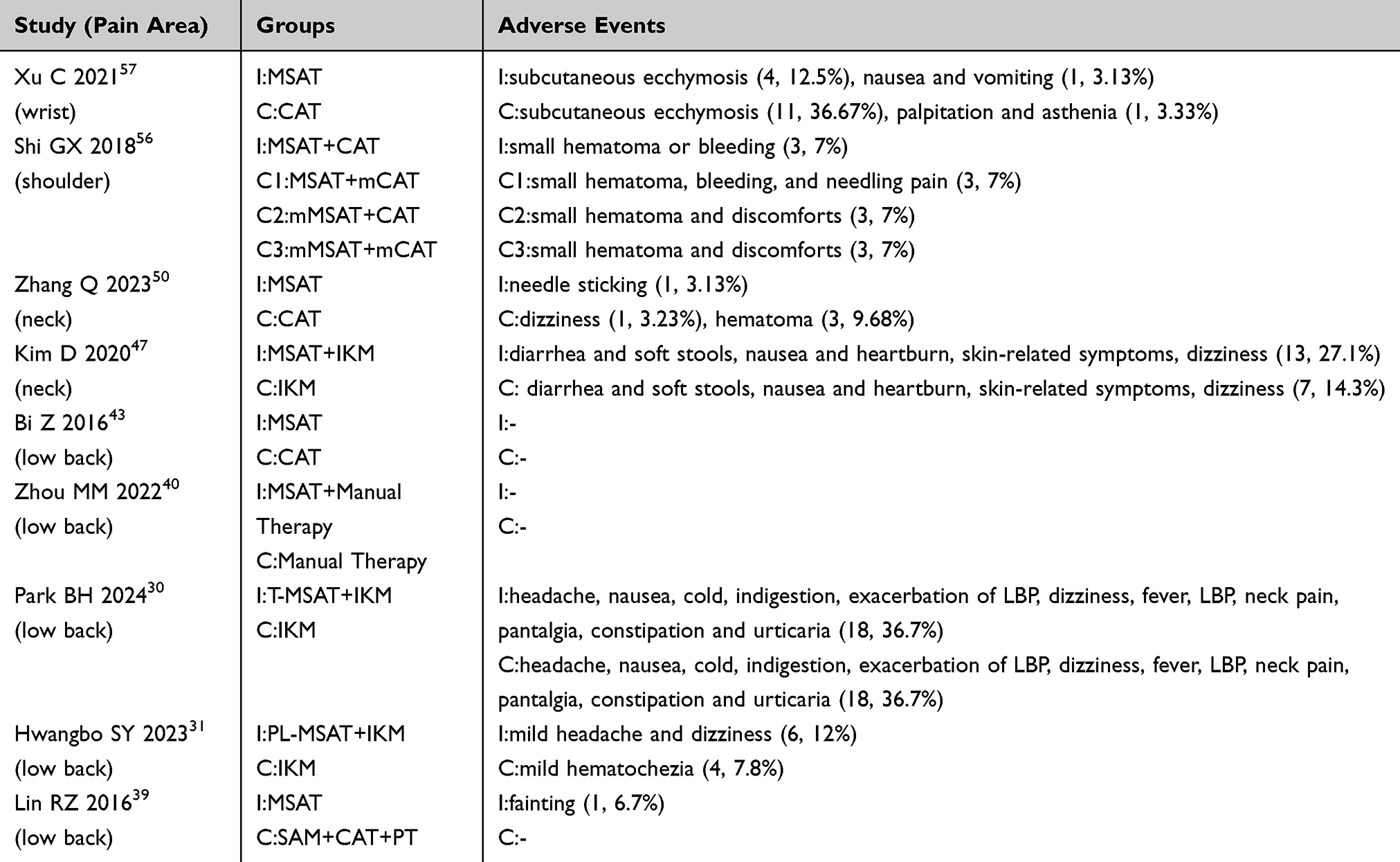 |
Table 2 Adverse Events |
Discussion
Main Findings
A total of 36 clinical studies using MSAT were included and an increasing publication trend from 2019 to 2024, culminating in 27 (75%) RCTs and 9 (25%) CCTs. The analyzed studies had a total of 2,620 patients with 16 different pain-related diseases/symptoms, representing both genders. The most commonly included conditions were acute lumbar sprain (8, 22.22%), adhesive capsulitis (5, 13.89%). In the treatment of acute LBP, 2 different kinds of MSAT, T-MSAT and PL-MSAT, were applied and showed immediate analgesic effects. MSAT was used alone in 11 (30.56%) studies and the others used MSAT combined with other treatment. Nine (25%) studies reported on the outcome of adverse events. Outcomes were measured by multidimensional scales of pain symptoms, quality of life, and mental health, with the VAS being the most frequently used instrument. In the 32 studies that used VAS as one outcome, 31 (96.88%) studies demonstrated significant differences.
In the included studies, it is found that MSAT is composed of two elements, acupuncture and movement, and there are various kinds of each element. In the element of acupuncture, eye acupuncture (1, 2.78%), scalp acupuncture (1, 2.78%), fire needling (2, 5.56%) and warm-needling moxibustion (2, 5.56%) are included. In the element of movement, rehabilitation technique such as McKenzie therapy (1, 2.78%) is included.
Limitations
There are three main limitations in this study. Firstly, MSAT has been gradually researched in the last decade, leading to the insufficient sample size. Secondly, most of included studies were published in Chinese. The last is that this report is unable to present information on the long-term outcomes and patients’ quality of life due to lack of enough data on follow-up in the included studies.
Implications
There are the following three points: 1) This study systematically searched seven databases to comprehensively collect research pertaining to musculoskeletal pain interventions using MSAT, thereby establishing an evidence base to elucidate research advancements and clinical application status in this therapeutic domain. 2) The included studies were classified according to the sites of musculoskeletal pain, diseases/symptoms, etc. This classification may assist researchers in more precisely and intuitively understanding the clinical applications of MSAT in various types of musculoskeletal pain and identifying which types of musculoskeletal pain still lack relevant research on MSAT. 3) In these studies, T-MSAT, PL-MSAT and McKenzie therapy were used in the treatment of LBP, which showed that MSAT can take many different forms, and acupuncture can be combined with different forms of exercise and even rehabilitation techniques. This study provides a detailed description of the various MSAT methods selected for different types of musculoskeletal pain, offering a comprehensive reference for the clinical application of MSAT.
Conclusion
MSAT which seems to be a promising intervention used in the management of diverse musculoskeletal pain conditions has been gradually studied in China and Korea. However, so far, few related studies have been published. Given the variety of study designs and reported treatment outcomes, conclusions about the evidence for MSAT for specific conditions are not possible at this stage. There is a need for more high-quality studies to address the issue of optimal acupuncture treatments of different pain conditions. In addition, the mechanism of remains unclear. Therefore, research on the mechanism of MSAT is necessary to elucidate the pathophysiological pathways through which it alleviates musculoskeletal pain.
MSAT refers to a treatment method in which acupuncture and movement therapy are administered concurrently rather than sequentially, and active/passive movements are applied to a patient under the assistance/supervision of a physician with the needle retained. According to different type of acupuncture and movement therapy, there are different kinds of MSAT. In addition to this, MSAT has been named differently in different studies. Therefore, the establishment of a classification system and a clear concept of MSAT is required.
Abbreviations
MSAT, motion style acupuncture treatment; CNKI, China Network Knowledge Infrastructure; CNS, central nervous system; 5-HT, 5-hydroxytryptamine; LBP, low back pain; EA, electroacupuncture; RCTs, randomized controlled trials; CCTs,controlled clinical trials; IKM, integrative Korean medicine (a comprehensive treatment, consists of acupuncture, pharmacopuncture, chuna, and herbal medicine); CAT, conventional acupuncture treatment; mMSAT, minimal MSAT; mCAT, minimal CAT; T-MSAT, MSAT using traction; PL-MSAT, Progressive Loading-MSAT; AM, acupuncture-movement; SAM, sham acupuncture-movement; TDP, electromagnetic spectrum therapeutic device; PT, physical therapy; VAS, Visual Analog Scale; NRS, pain numeric rating scale; NDI, neck disability index; ROM, range of motion; Quality of life, PGIC, patient global impression of change; SF-36, Short Form 36 Questionnaire; JOA, Japanese Orthopaedic Association Scores; CMS, ConstantMurley score; AROM, active range of motion; SLR, degree of straight leg raising; PPI, present pain intensity; PRI, pain rating index; LAI, Lequesne Algofunctional Index; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; NO, Nitric oxide; ODI, Oswestry Disability Index; SLR, degree of straight leg raising; AROM, active range of motion; SF-12, 12-item short-form survey; EQ-5D, EuroQol 5-Dimension; EQ-VAS, EuroQol Visual Analogue Scale; SF-12v2, Short Form‐12 health survey version 2; PCL-5-K, posttraumatic stress disorder checklist for DSM-5; RMQ, Roland Morris Questionnaire; M-JOA, Modified Japanese Orthopaedic Association low back Pain score; MFS, Maryland foot score.
Funding
This research was supported by the Winter Sports Management Center of General Administration of Sport of China 2024 Figure Skating Team Fitness Enhancement Service (0773-2441GNOEFWGK4888).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
2. Moretti A, Snichelotto F, Liguori S, et al. The challenge of pharmacotherapy for musculoskeletal pain: an overview of unmet needs. Ther Adv Musculoskelet Dis. 2024;16:1759720X241253656. doi:10.1177/1759720X241253656
3. Elma Ö, Yilmaz ST, Deliens T, et al. Chronic musculoskeletal pain and nutrition: where are we and where are we heading? PM R. 2020;12(12):1268–1278. doi:10.1002/pmrj.12346
4. Shraim MA, Sluka KA, Sterling M, et al. Features and methods to discriminate between mechanism-based categories of pain experienced in the musculoskeletal system: a delphi expert consensus study. Pain. 2022;163(9):1812–1828. doi:10.1097/j.pain.0000000000002577
5. Abeler K, Bergvik S, Sand T, et al. Daily associations between sleep and pain in patients with chronic musculoskeletal pain. J Sleep Res. 2021;30(4):e13237. doi:10.1111/jsr.13237
6. Amiri S. Exercise training and depression and anxiety in musculoskeletal pain patients: a meta-analysis of randomized control trials. Neuropsychiatr. 2023;37(2):88–100. doi:10.1007/s40211-022-00431-2
7. Dzakpasu FQS, Carver A, Brakenridge CJ, et al. Musculoskeletal pain and sedentary behaviour in occupational and non-occupational settings: a systematic review with meta-analysis. Int J Behav Nutr Phys Act. 2021;18(1):159. doi:10.1186/s12966-021-01191-y
8. El-Tallawy SN, Nalamasu R, Salem GI, et al. Management of musculoskeletal pain: an update with emphasis on chronic musculoskeletal pain. Pain Ther. 2021;10(1):181–209. doi:10.1007/s40122-021-00235-2
9. Curatolo M, Bogduk N. Pharmacologic pain treatment of musculoskeletal disorders: current perspectives and future prospects. Clin J Pain. 2001;17(1):25–32. doi:10.1097/00002508-200103000-00005
10. Bialosky JE, Bishop MD, Price DD, et al. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14(5):531–538. doi:10.1016/j.math.2008.09.001
11. Li Z, Zhuang J, Zhang S, et al. Therapeutic effects of traditional Chinese exercises on musculoskeletal pain: a systematic review and meta-analysis. Pain Res Manag. 2021;2021:5584997. doi:10.1155/2021/5584997
12. Zhang Y, Wang C. Acupuncture and chronic musculoskeletal pain. Curr Rheumatol Rep. 2020;22(11):80. doi:10.1007/s11926-020-00954-z
13. Wright A, Sluka KA. Nonpharmacological treatments for musculoskeletal pain. Clin J Pain. 2001;17(1):33–46. doi:10.1097/00002508-200103000-00006
14. Kim DY, Ha IH, Kim JY. Graded exercise with motion style acupuncture therapy for a patient with failed back surgery syndrome and major depressive disorder: a case report and literature review. Front Med. 2024;11:1376680. doi:10.3389/fmed.2024.1376680
15. Park JW, Jeong WJ, Huh HS, et al. Combination of MSAT and Korean medicine for managing foot drop due to lumbar disc herniation: case report. Korean J Acupunct. 2021;38(3):189–195. doi:10.14406/acu.2021.012
16. Jong-Hyeok J, Hyeon-Jun W, Won-Bae H, et al. Domestic clinical research trends of motion-style acupuncture treatment: a scoping review. J Korean Med Rehabil. 2022;32(4):19–32. doi:10.18325/jkmr.2022.32.4.19
17. Kim D, Lee YJ, Ha I-H. In-Hyuk Ha. A scoping review of clinical research on motion style acupuncture treatment. Perspect Integr Med. 2023;2(2):65–76. doi:10.56986/pim.2023.06.001
18. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
19. Peters MDJ, Godfrey CM, Khalil H, et al. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13(3):141–146. doi:10.1097/XEB.0000000000000050
20. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
21. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
22. Stone PW. Popping the (PICO) question in research and evidence-based practice. Appl Nurs Res. 2002;15(3):197–198. doi:10.1053/apnr.2002.34181
23. Yang TJ, Wen FF, Wan QQ. Clinical efficacy observation of giant spur exercise therapy in the treatment of painful heel syndrome. Acta Chin Med Pharmacol. 2022;50:78–81. doi:10.19664/j.cnki.1002-2392.220255
24. Xu JW. Therapeutic observation on acupuncture at the second metacarpal holographic point plus exercise with needles for heel. J Acupunct Tuina Sci. 2013;32:755–756. doi:10.3969/j.issn.1005-0957.2013.09.755
25. Liao ZG, Xu XY, Chen S, et al. Therapeutic effect on knee osteoarthritis treated with combination of filiform-fire needling, muscular region-acupuncture and kinematic-acupuncture. J Liaoning Univ Traditional Chin Med. 2022;24:137–141. doi:10.13194/j.issn.1673-842x.2022.09.030
26. Cai GF, Cai GL, Zhuang Z, et al. Clinical effect of fire needling combined with exercise therapy on serum NO in the treatment of KOA of early stage. J Clin Acup Moxib. 2020;36:20–25. doi:10.3969/j.issn.1005-0779.2020.07.007
27. Xu WS, Dong BQ, Liu T. Clinical study of eye acupuncture kinesitherapy combined with body acupuncture in the treatment of KOA. J Clin Acup Moxib. 2020;36:23–27. doi:10.3969/j.issn.1005-0779.2020.06.007
28. Qu XD, Zhou JJ, Zhai HW, et al. Therapeutic effect of exercise acupuncture and osteopathy on traumatic knee arthritis. Chin J Orthop Traumatol. 2019;32(6):493–497. doi:10.3969/j.issn.1003-0034.2019.06.002
29. Shin JS, Ha IH, Lee J, et al. Effects of motion style acupuncture treatment in acute low back pain patients with severe disability: a multicenter, randomized, controlled, comparative effectiveness trial. Pain. 2013;154(7):1030–1037. doi:10.1016/j.pain.2013.03.013
30. Park BH, Han JH, Park JH, et al. Effectiveness and safety of motion-style acupuncture treatment using traction for inpatients with acute low back pain caused by a traffic accident: a randomized controlled trial. Medicine. 2024;103:e38590. doi:10.1097/MD.0000000000038590
31. Hwangbo SY, Kim YJ, Shin DG, et al. Effectiveness and safety of progressive loading-motion style acupuncture treatment for acute low back pain after traffic accidents: a randomized controlled trial. Healthcare. 2023;11(22):2939. doi:10.3390/healthcare11222939
32. Li Q, Xu CY, Zhu L, et al. Treatment of 48 cases of acute lumbar sprain with sports acupuncture combined with massage and microwave physiotherapy. World Latest Med Info. 2019;19:184–186.
33. Lin HM. Clinical observation of acupuncture at houxi points plus exercise therapy in treating acute lumbar sprain. Clin J Chinese Med. 2022;14:82–84. doi:10.3969/j.issn.1674-7860.2022.24.030
34. Li CM, Pan Z, Xie Z, et al. Clinical efficacy observation on acupuncture at Shousanli and Yaotongdian combined with exercise therapy in treating acute lumbar sprain in grassroots officers and soldiers. J Emergency Traditional Chin Med. 2024;33:884–887. doi:10.3969/j.issn.1004-745X.2024.05.033
35. Han H, Li M. Clinical observation on the efficacy of acupuncture at the lumbago points combined with exercise therapy in the treatment of acute lumbar sprain. Lishizhen Medicine Materia Medica Res. 2012;23:244–245. doi:10.3969/j.issn.1008-0805.2012.01.109
36. Zhu HL, Zhou ZB, Wu XG, et al. Clinical research of using Shentong Zhuyu decoction combined with acupuncture kinesitherapy and traditional Chinese application therapy in the treatment of acute lumbar sprain. J Trad Chin Med. 2022;40:148–151. doi:10.3969/j.issn.1000-3649.2022.5.sczy202205044
37. Zhang GY, Kang LH, Yu M. Randomized parallel controlled study of acupuncture combined with lumbar exercise in the treatment of acute lumbar sprain. J Pract Traditional Chin Int Med. 2019;33:55–57.
38. Niu RM, Pan XH. Clinical analysis of acupuncture exercise therapy combined with passive hip flexion and knee flexion in the treatment of acute lumbar sprain. Chin Med Treat. 2023;42:21–24. doi:10.13729/j.issn.1671-7813.Z20190041
39. Lin RZ, Zhu N, Liu J, et al. Acupuncture-movement therapy for acute lumbar sprain: a randomized controlled clinical trial. J Tradit Chin Med. 2016;36(1):19–25. doi:10.1016/S0254-6272(16)30003-6
40. Zhou MM, Xie B, Guo L, et al. Clinical observation on 30 cases of myofascial pain syndrome treated by manipulation combined with motion acupuncture. Chin J Ethnomedicine Ethnopharm. 2022;31:101–106. doi:10.3969/j.issn.1007-8517.2022.13.zgmzmjyyzz202213024
41. Huang D, Lai JY, He SH. Clinical observation of motion acupuncture combined with lumbar traction therapy in the treatment of lumbar disc herniation. J GuangZhou Univ Tradit Chin Med. 2022;39:2048–2052. doi:10.13359/j.cnki.gzxbtcm.2022.09.015
42. Yang G, Tian YF, Yu J, et al. Observation on the clinical effect of percutaneous transforaminal endoscopic discectomy combined with acupuncture-movement therapy on lumbar intervertebral disc herniation. Hebei J Trad Chin Med. 2020;42:1369–1373. doi:10.3969/j.issn.1002-2619.2020.09.020
43. Bi Z, Zhu YC. Clinical observation of shallow needling at Fuliu combined with exercise therapy on lumbar muscle strain. Clin J Tradit Chin Med. 2016;28 doi:10.16448/j.cjtcm.2016.0352
44. Bian YW, Zhang Y. Efficacy observation of needling-exercise therapy on lumbar muscle strain. Shanxi J Tradit Chin Med. 2024;40:27–28. doi:10.20002/j.issn.1000-7156.2024.12.011
45. Ji CC, Zhao JY. Observation on the efficacy of acupuncture movement therapy in the treatment of acute non - specific low back pain. J Shaanxi Coll Tradit Chin Med. 2018;41:86–87,91.
46. Sun MM, Mao X, Liu JT, et al. Head acupuncture combined with exercise therapy for nonspecific low back pain: a randomized controlled trial. Chin Acupuncture Moxibustion. 2022;42:511–514. doi:10.13703/j.0255-2930.20210613-k0002
47. Kim D, Park KS, Lee JH, et al. Intensive Motion Style Acupuncture Treatment (MSAT) is effective for patients with acute whiplash injury: a randomized controlled trial. J Clin Med. 2020;9(7):2079. doi:10.3390/jcm9072079
48. Bian RM. Clinical observations on the efficacy of acupuncture kinesitherapy plus conventional acupuncture in treating cervical spondylosis. Shanghai J Acupuncture Moxibustion. 2015;1216–1218. doi:10.13460/j.issn.1005-0957.2015.12.1216
49. Zhang RG, Gao M, Li JL, et al. Research on the efficacy and safety of acupuncture combined with exercise therapy in the treatment of nerve root type cervical spondylosis. Acta Chin Med Pharmacol. 2024;52:51–56.
50. Zhang Q, Liu ML, Shao P, et al. Clinical efficacy of penetrating acupuncture at houxi combined with exercise therapy in the treatment of stiff neck. World J Integr Tradit West Med. 2023;18:1453–1456. doi:10.13935/j.cnki.sjzx.230732
51. Li L, Sheng JK, Zhang W. Hui-acupuncture combined with Ju—sports acupuncture in the treatment of acute scapulohumeral periarthritis. J Clin Acup Moxib. 2011;27:32–34. doi:10.3969/j.issn.1005-0779.2011.09.015
52. Yang SY. Clinical study on treating scapulohumeral periarthritis with acupuncture - movement therapy combined with traditional Chinese medicine compress and topical application of traditional Chinese medicine. Modern Diagnosis Treatment. 2021;32:1861–1863.
53. Wang LJ, Luo HP, Ding Y, et al. Randomized controlled trial of acupuncture movement and warm round sharp needle acupuncture for scapulohumeral periarthritis of wind cold dampness pattern. World J Tradit Chin Med. 2021;34:120–123. doi:10.12174/j.issn.2096-9600.2021.07.31
54. Yang WX, Guo SS. Chinese herbal medicine encapsulation combined with acupuncture exercise in the treatment of periarthritis of shoulder. Guangming J Chin Med. 2024;39:1595–1597. doi:10.3969/j.issn.1003-8914.2024.08.036
55. Wang YD, Wan HM. Efficacy observations of Qiuxu through Zhaohai motility acupuncture combined with shouIder five-needle acupuncture in treating rotator cuff injury. J Emergency Traditional Chin Med. 2022;31:1970–1972. doi:10.3969/j.issn.1004-745X.2022.11.023
56. Shi GX, Liu BZ, Wang J, et al. Motion style acupuncture therapy for shoulder pain: a randomized controlled trial. J Pain Res. 2018;11:2039–2050. doi:10.2147/JPR.S161951
57. Xu C, Gao YN. Therapeutic effect of contralateral puncture combined with acupuncture exercise therapy on early stenosing tenosynovitis of radius styloid. Med Inf. 2021;34:170–172. doi:10.3969/j.issn.1006-1959.2021.11.048
58. Yang HF. Effective observation on treating periarthritis of shoulder in warmed needle and moxibustion plus exercise needling therapy. Clin J Chinese Med. 2011;3:4–5. doi:10.3969/j.issn.1674-7860.2011.01.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.