")
Back to Journals » Nature and Science of Sleep » Volume 17
The Association Between School Connectedness and Sleep Health in Children and Adolescents: A Systematic Review
Authors Raniti M, Chairilsyah MR , Suma MNI , Sawyer SM
Received 7 October 2024
Accepted for publication 17 January 2025
Published 24 March 2025 Volume 2025:17 Pages 489—504
DOI https://doi.org/10.2147/NSS.S498002
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Valentina Alfonsi
Monika Raniti,1– 3 Muhammad Reza Chairilsyah,2,4,* Muhammad Nur Imaduddin Suma,2,4,* Susan M Sawyer1,2
1Centre for Adolescent Health, Murdoch Children’s Research Institute & Royal Children’s Hospital, Melbourne, Victoria, Australia; 2Department of Paediatrics, Melbourne Medical School, University of Melbourne, Melbourne, Victoria, Australia; 3The ALIVE National Centre for Mental Health Research Translation, University of Melbourne, Melbourne, Victoria, Australia; 4Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
*These authors contributed equally to this work
Correspondence: Monika Raniti, Centre for Adolescent Health, Royal Children’s Hospital and Murdoch Children’s Research Institute, Flemington Road, Parkville, Victoria, 3052, Australia, Tel +61 03 8341 6200, Email [email protected]
Abstract: Schools are key settings for sleep health promotion and interventions. Yet their value as rich social-emotional environments that shape student health and wellbeing has largely been neglected by sleep research. School connectedness reflects students’ engagement with learning and sense of belonging with peers, teachers, and the school environment. Although school connectedness is associated with physical and mental health in children and adolescents, whether it is associated with sleep is unclear. To address this gap, we systematically reviewed the evidence for cross-sectional and prospective associations between school connectedness and sleep. We searched Medline, PubMed, PsycINFO, and ERIC databases for observational and intervention studies published from 1950 to 17th July 2024 that examined relationships between school connectedness and sleep health or sleep problems/disorders in four- to 24-year-olds. We identified ten eligible studies (seven cross-sectional and three longitudinal) for narrative synthesis. Studies were primarily from China and Taiwan (n = 6) and conducted in secondary schools (n = 8). Participants were 14.5 years old, on average. Most of the cross-sectional studies found a positive relationship between school connectedness and sleep health. All longitudinal studies reported at least one significant relationship between school connectedness and sleep health, however two of these studies also reported non-significant relationships. We did not identify any intervention studies. Most studies were rated as ‘fair’ quality representing a moderate risk of bias. The findings of this review suggest that school connectedness is linked to some aspects of sleep health and insomnia in secondary-school aged adolescents. Longitudinal studies are needed to explore prospective relationships in addition to studies conducted in primary and tertiary education settings.
Keywords: pediatric, sleep health, school climate, health promotion, prevention
Introduction
Sleep is important for child and adolescent development, as it influences physical and mental health, cognitive functioning, and academic performance.1 Recognized as a public health priority,2 healthy pediatric sleep is a complex construct, as it is characterised by subjective or caregiver-rated satisfaction, appropriate timing, adequate duration for age, high efficiency, sustained alertness during waking hours, and healthy sleep behaviors.3 It is estimated that approximately a third of children and adolescents experience sleep disturbances (eg, poor quality or inappropriate timing of sleep)4 and over half do not obtain the recommended amount of sleep on school nights.5,6 Sleep disorders such as insomnia disorder and delayed sleep-wake phase disorder are also common.7,8 Identifying novel, modifiable factors that influence pediatric sleep health and which may contribute to the etiology and maintenance of sleep problems, disorders, and their sequelae (eg, depression9) is therefore important to guide population approaches to improving sleep.
Contemporary models conceptualise the factors that contribute to sleep health in children and adolescents using biopsychosocial and socio-ecological frameworks.3,10,11 These models recognise that individual characteristics including one’s biology (eg, age, post-pubertal changes to the sleep homeostatic system),12 behaviors (eg, screen use, bedtimes),13,14 cognitions (eg, beliefs about sleep), and emotions (eg, pre-existing anxiety)15 interact with the wider systems (eg, family, school, neighbourhood) and environments (eg, social-cultural, physical) in which a young person lives, and that these relationships change over the course of development.3,10 Accumulating evidence indicates that social determinants of health such as social ties,16 perceived discrimination,17 and neighbourhood environments18 also influence child and adolescent sleep and may be effective targets in changing sleep health at a population level. However, these contexts, including schools, have received little attention relative to individual factors.
Schools are key settings for sleep health promotion and intervention. Yet their value as rich social-emotional environments that shape student health and wellbeing, particularly since the COVID-19 pandemic,19 has been largely neglected within sleep research.20 Extant evidence is weighted towards the academic correlates of sleep health (eg, the effect of homework and extracurricular activities, academic performance, attendance) and the (largely positive) impact of school scheduling changes to delay school start times in countries such as the USA where school starts early.20 Universal school-based sleep interventions have focused on sleep education and brief cognitive-behavioral sleep interventions, which tend to increase sleep knowledge and improve some aspects of sleep, primarily sleep duration and quality in the short term.21 These interventions typically position schools as platforms for their intervention delivery rather than capitalizing on the wider social context of the school. For example, a growing body of evidence supports the association between peer relationships and sleep. Peer victimization is associated with sleeping problems, particularly in younger children22 and girls,23 while a sense of school belonging has been shown to buffer the negative effects of discrimination on sleep in ethnic minority adolescents.24 One recent study showed that adolescents with higher levels of sleep disturbance had fewer self-rated and peer-rated social connections, even after controlling for sociodemographic and mental health variables.25 Given the developmental importance of the social environment in the transition from childhood to adolescence,26 which is also a vulnerable time for the development of sleep problems,12 interventions that address the school social environment may be a critical piece within holistic strategies that support healthy pediatric sleep.
School connectedness is a multifaceted construct reflecting the quality of the relationships that a student has with their school and the individuals within it.27 School connectedness includes students’ thoughts (eg, perceptions of relationships with teachers and peers, attitudes towards school experiences), feelings (eg, around belonging, acceptance, enjoyment of school), and behaviors (eg, engagement in activities) towards the school environment and learning experiences,28,29 and is usually assessed using self-report measures (example items: I can really be myself at my school,30 You feel like you are a part of the school, Your teachers care about you).31
School connectedness is correlated with greater psychological wellbeing, academic achievement,32 and reduced suicidal thoughts and behaviors,33 and prospectively associated with higher levels of physical activity and reduced substance use,34 and fewer symptoms of depression and anxiety.29 A recent meta-analysis of 90 studies found school connectedness to be protective against poor mental and sexual health, substance use, and violence, and the co-occurrence of these risks in adolescence, suggesting the potential of school connectedness to prevent and mitigate several health risks simultaneously.35 There were particular benefits of school connectedness for sexual and gender minority students, students of color, and older students (ie, middle and high school) for some outcomes (eg, mental health). In addition, interventions that target the social-emotional environment of the school, for example, by aiming to increase a sense of belonging and participation in school life, have been shown to improve student health and related outcomes such as depressive symptoms and self-esteem.36,37
Despite these links to physical and mental health, many of which often co-occur with sleep outcomes,1 it is unclear whether school connectedness is associated with student sleep outcomes, and if so, which specific aspects of sleep and the direction of the effect. It is plausible that school connectedness improves sleep such as sleep-onset latency or subjective sleep quality, potentially through reduced anxiety38 or loneliness.39 Conversely, experiencing sleep problems might make it harder for students to engage in school life leading to a lower sense of connectedness. Alternatively, it is possible that school connectedness worsens some aspects of sleep. For example, school connectedness may increase time spent engaging in school and social activities, which displaces time for sleep, thus reducing sleep duration40 or may increase popularity, which has been linked to poorer sleep, particularly for girls.41 While school connectedness is likely to be associated with the more behavioral and psychological aspects of sleep problems (eg, short sleep duration, prolonged onset latency) than those with a largely biological etiology (eg, circadian rhythm disorders or sleep disordered breathing), it could be that feeling connected to school enhances motivation or organisational skills, which aids treatment adherence, thereby improving sleep.
To this end, we conducted a systematic review that aimed to find the evidence for 1) the cross-sectional and prospective relationships between school connectedness and sleep health and sleep problems/disorders and 2) the effect of interventions to improve school connectedness on sleep health and sleep problems/disorders in children and adolescents aged four to 2442 years in primary, secondary, and tertiary education settings.
Materials and Methods
The review protocol was registered on PROSPERO (CRD42022316182) on 15/04/2022. We did not require ethical approval as these data were obtained from published, peer-reviewed journal articles.
Information Sources and Search Strategy
The final search was conducted on the 17th of July 2024 using MEDLINE, PsycINFO, PubMed, and ERIC electronic databases using free-text and controlled terms related to 1) school connectedness (eg, school belonging, school attachment, school climate); 2) sleep outcomes (eg, insomnia, sleep deprivation, sleep hygiene, sleep-wake); 3) children and adolescents (eg, boy, girl, child, young adult, minor). We also searched the reference lists of included articles for eligible studies. The MEDLINE search strategy was used as the basis of the search for the other databases (see Appendix 1).
Eligibility Criteria
We included peer-reviewed primary observational (cross-sectional and longitudinal) or intervention studies (of any design) published in English since 1950. No other restrictions were applied.
Participants
Participants were children and adolescents aged 4 to 24 years attending primary/elementary, secondary, or tertiary/further education setting in any country and from any population (eg, clinical, community). We planned to include studies that used a wider age range if the mean age fell within our specified age range or where results were presented separately for our specified age range, but this did not apply to any of the identified studies.
Exposure/Intervention
We included observational studies that examined one or more components of school connectedness or defined a synonymous construct such as “school belonging” or “sense of school membership”, and studies of interventions with the objective of improving school connectedness and delivered within a school setting. Interventions could be anything within the spectrum of whole-school approaches19 such as the delivery of an education program, changes to school curriculum, policy or physical to social-emotional environment, or professional development for school staff.
Outcomes
Studies had to include any sleep outcome framed as a measure of sleep health (eg, onset latency, sleep duration, subjective sleep quality) or sleep problem or disorder (eg, insomnia), regardless of how it was measured (eg, single item on a survey, total score on a validated symptom scale, diagnosis made via polysomnography or diagnostic manual such as the DSM-5, actigraphy measured sleep duration). Observational studies had to examine the relationship between school connectedness and sleep outcomes. Intervention studies had to examine change in values or symptom scores or diagnostic status before and after an intervention.
Selection Process
Article deduplication and title, abstract, and full-text screening was conducted in Endnote X9 reference management software by three researchers (MR, MNIS & MRC). Three-quarters of the articles were double screened and discrepancies resolved through discussion with a third researcher (MR and SS).
Data Collection Process and Data Items
Data were extracted separately by three researchers (MR, MNIS & MRC) into an Excel database, with discrepancies resolved through discussion with a third researcher (MR and SS). Extracted information included study design, recruitment and sample method, participant characteristics, exposure and outcome constructs and measures, and relevant findings (eg, negative/positive or no association, effect sizes where possible).
Study Risk of Bias Assessment
Risk of bias assessment was conducted by three researchers separately (MR, MNIS & MRC) with discrepancies resolved through discussion with a third researcher (MR and SS) using the National Institute of Health (NIH) Quality assessment tool for observational and cross-sectional studies and the Quality assessment of controlled intervention studies tool.43 Studies were assessed on 14 criteria and rated as “good”, “fair”, or “poor” per NIH guidance.
Synthesis Methods
We synthesized the data using narrative synthesis and summary tables. Given the small number of studies identified, we did not exclude studies on the basis of study quality. Due to the small number of studies and heterogeneity across studies (eg, measurement of school connectedness and sleep outcomes), we were unable to evaluate overall effect sizes using meta-analysis or compare effect sizes across studies.
Results
The results of the search and selection process are presented in the PRISMA flowchart44 in Figure 1. We identified 866 unique records for screening across all sources, which resulted in 17 potentially eligible articles. After full-text screening, 10 articles met inclusion criteria and were included in the review.
 |
Figure 1 PRISMA flowchart of search results at each step of the systematic review. Note: PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources Source: Page MJ, et al. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. This work is licensed under CC BY 4.0.44 |
Study Characteristics
The study characteristics of the 10 included studies (7 cross-sectional and 3 longitudinal) are summarised in Table 1. No intervention studies were identified. Studies were primarily from China (n = 4)45–48 and Taiwan (n = 2),49,50 followed by Belgium (n = 1),51 France (n = 1),52 Italy (n = 1),53 and the USA (n = 1).54 Seven studies recruited participants from secondary schools,46–50,52,53 one from both primary and secondary schools,51 and one from colleges/universities.45 Another study of late primary to middle secondary school age students recruited participants through their families (who were already part of an existing longitudinal study).54 No studies were conducted in clinical settings. Sample sizes ranged from 888 to 8153 participants; the majority of studies had sample sizes of over 1000 participants. The average mean age of participants was 14.5 years (one study of high school students did not report mean age).50 The three longitudinal studies (two from China45,46 and one from the USA54) had six month,45 nine month,46 and three year54 timed follow-up, respectively. Seven studies46,49–54 designed their statistical analyses to specifically test the relationship between school connectedness and sleep, whereas the remaining three studies45,47,48 examined the role of school connectedness or sleep as part of a larger mediation model. Six studies45,47,50–53 were published in the past five years, two of which collected data during the COVID-19 pandemic.45,52
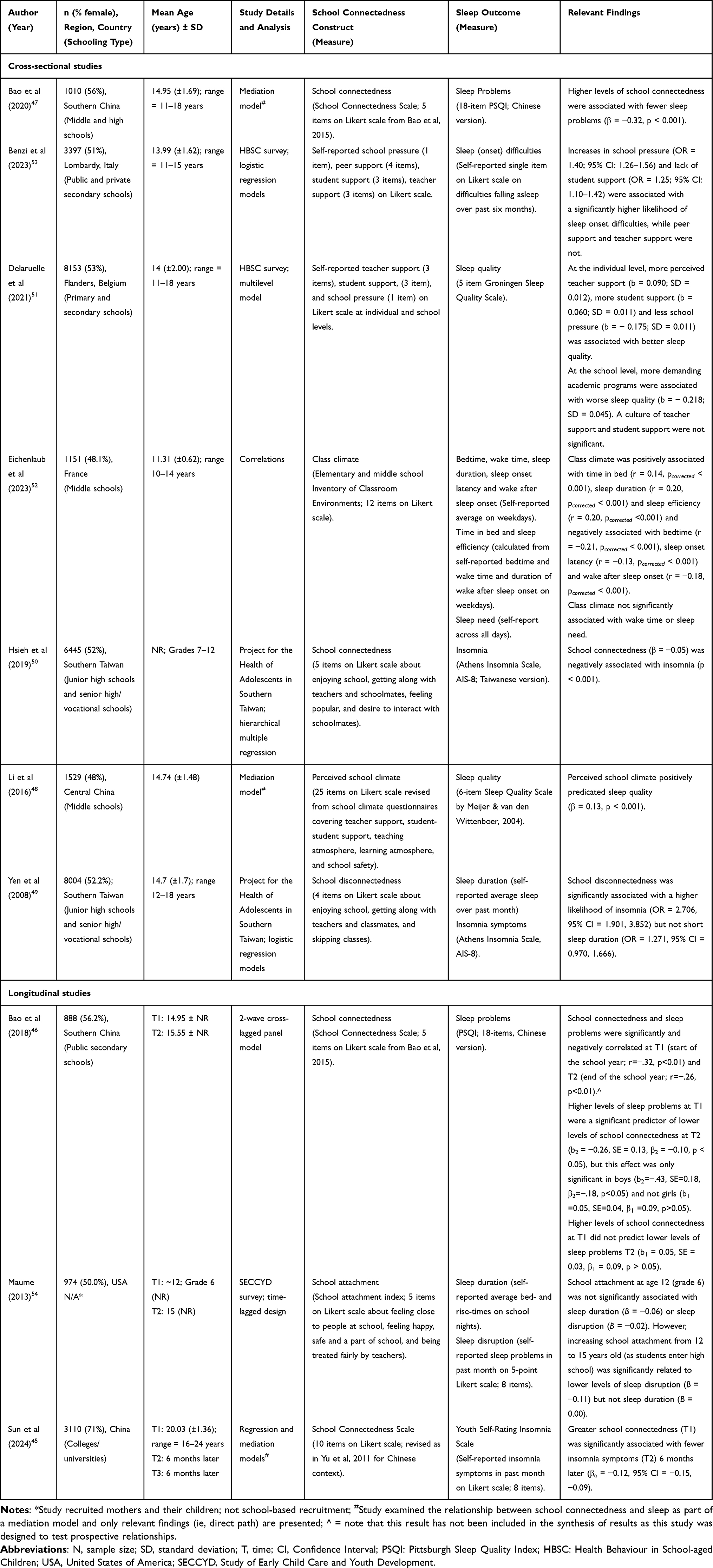 |
Table 1 Study Characteristics and Relevant Findings for the Included Studies |
Measurement of School Connectedness
Studies varied in their conceptualization and measurement of school connectedness. All studies measured school connectedness using student self-report items on a Likert scale. Over half of the studies used an existing or adapted school connectedness scale,45–48,50,52 while the remaining studies used items from existing projects that were developed by the researchers, namely the Health Behaviour in School-aged Children (HBSC) survey,51,53 the Project for the Health of Adolescents in Southern Taiwan,49,50 and the Study of Early Child Care and Youth Development.54 Studies used between 4 and 12 items to assess school connectedness, except for one study48 which used 25 items. All studies measured more than one aspect of school connectedness (eg, teacher or peer support, engagement in school activities, sense of belonging). Eight studies45–48,50,52,54 reported results for a total “global” score, while two studies51,53 reported results for separate components of school connectedness (eg, teacher support). Although many of the studies used similar items (eg, “I like my school”, “I feel I am part of my school”, “Students care about on another”, “I get along well with my teachers”) and/or components (eg, student support, skipping classes) to assess the various aspects of school connectedness, varied terms were used, including “school connectedness”, “school attachment”, and “perceived school climate”. Only one study measured school disconnectedness49 as a construct.
Measurement of Sleep
Studies also varied in their conceptualization and measurement of sleep. Three studies examined sleep duration, all via self-report: one study measured average sleep duration on weekdays but did not report how this was calculated;52 another54 measured average bed and rise times on school nights and calculated the difference in hours to obtain sleep duration but did not report a timeframe (eg, over the past week); while another measured average nightly sleep over the past month.49 Five studies examined sleep quality or problems, which sometimes included daytime impairments such as fatigue. Four of these studies used an existing questionnaire, namely, the Pittsburgh Sleep Quality Index (PSQI; Chinese version),46,47 the Groningen Sleep Quality Scale,51 and the Sleep Quality Scale.48 The remaining study54 used items developed by the researchers as part of the Study of Early Child Care and Youth Development (eg, “How often in the past month have you: had difficulty falling asleep on school nights; felt tired on school days; wished you could get more sleep”). Three studies specifically assessed insomnia symptoms using the Athens Insomnia Scale49,50 or the Youth Self-Rating Insomnia Scale.45 All studies reported multiple sleep outcomes or a total composite score on a questionnaire, except one53 which only reported self-reported sleep onset difficulties over the past six months on a single item.
Study Quality Assessments
The risk of bias assessment ratings for the 10 included studies are presented in Table 2. The three longitudinal studies45,46,54 were rated as “good”, representing a lower risk of bias, and the remaining seven studies47–53 which were cross-sectional were rated as “fair” representing a higher risk of bias.
 |
Table 2 Risk of Bias Assessment for Included Studies |
The majority of studies described their sample well and all recruited from similar populations. However, few studies reported the participation rate, so it was difficult to determine whether the sample adequately represented the target population. Only one study53 provided a sample size justification. Although all studies were rated using measures that were clearly described and used consistently across participants, it should be noted that there was variation in the reliability and validity of these measures. For example, some studies used measures that had been developed by the researchers in previous studies or reported a reliability statistic for that sample, whereas others used measures that have been extensively validated. No study measured sleep using a sleep diary or objective measures such as actigraphy. Most studies controlled for some confounders (sex and age as a minimum), although a couple of studies45,51 were particularly comprehensive, including one45 longitudinal study that controlled for baseline insomnia and depressive symptoms, among other characteristics. All studies used self-report measures in a community setting, some anonymously, which meant that assessors were blinded to participants’ sleep outcome status.
The longitudinal studies measured the exposure of interest (school connectedness) prior to sleep outcomes, all with long enough follow-up to theoretically allow for an effect to emerge (the shortest follow-up was 6 months).45 No studies measured sleep outcomes more than once over time. Only one of these studies46 also measured the reverse relationship of sleep predicting school connectedness. One study reported less than 20% loss to follow-up,46 one greater than 20%,54 and one did not report the number of participants lost to follow-up.45
Given the small number of studies included and that no studies were rated as “poor”, all studies were retained for analysis but have been separated into cross-sectional (fair study quality rating) and longitudinal (good study quality rating) studies in the synthesis of results section below.
Synthesis of Results
Four studies45,47,48,50 reported a significant association between school connectedness and sleep, and six studies46,49,51–54 reported mixed results depending on how school connectedness and sleep were measured. Across all studies, 30 relevant relationships (19 significant and 11 non-significant) between school connectedness and sleep were analysed, which are synthesised below. Six studies examined one45,47,48,50 or two46,49 relationships between school connectedness and sleep, and the remaining four studies examined four,53,54 six,51 and eight52 relationships. Note that Bao et al (2018)46 reported a significant cross-sectional relationship between greater school connectedness and fewer sleep problems at baseline and at 9-month follow-up, but we have not included these findings in this synthesis as the aim of that study was to examine prospective relationships.
Cross-Sectional Studies
Of the seven cross-sectional studies, 23 relationships were analysed (16 significant, seven non-significant). All studies reported at least one significant relationship. Across the significant relationships, higher levels of school connectedness were associated with better sleep and fewer sleep problems, and lower levels of school connectedness or school disconnectedness were associated with worse sleep quality and more sleep problems.
Of the significant relationships, school connectedness was predominately measured using a “global” score (ten relationships47–50,52 which included six relationships analysing class climate, which were all from same study),52 followed by student (two relationships)51,53 and teacher (one relationship)51 support at the individual level, and school pressure at individual (two relationships)51,53 and school (one relationship)51 levels. Sleep was measured as “global” sleep quality (six relationships)47,48,51 or “global” insomnia symptoms (two relationships),49,50 followed by sleep onset difficulties (two relationships)47,48,51 and one study52 which examined single aspects of sleep (six relationships), namely, sleep onset latency, bedtime, time in bed, sleep duration, sleep efficiency, and wake after sleep onset.
Four of the cross-sectional studies reported non-significant relationships.49,51–53 However, none of the studies reported only non-significant associations, that is, results were mixed depending on the sleep outcome analysed in the study. Three relationships were between a “global” score of school connectedness and sleep, specifically the association between school disconnectedness and sleep duration,49 and the association between class climate and wake time and sleep need.52 The remaining non-significant relationships examined a single component of school connectedness (ie, peer support, teacher support) with sleep onset difficulties53 or “higher level” constructs of school-level teacher and peer support with sleep quality.51
Longitudinal Studies
Of the three longitudinal studies,45,46,54 seven relationships were analysed (three significant and four non-significant). All longitudinal studies reported at least one significant relationship. All studies used a “global” measure of school connectedness and examined “global” sleep quality, sleep disruption, or insomnia. One study also examined sleep duration.54 Bao et al (2018) was the only study to examine the bidirectional relationship between school connectedness and sleep.46 They found that school connectedness did not significantly predict sleep problems from the start to the end of the school year (ie, nine-month follow-up). However, the reverse relationship whereby higher levels of sleep problems predicted less school connectedness was significant, but only in boys. Conversely, Sun et al (2024) found that greater school connectedness at baseline significantly predicted fewer insomnia symptoms six months later.45 This was the only study conducted with college students. Finally, Maume (2013) reported mixed results.54 School attachment at baseline did not significantly predict sleep duration or sleep disruption three years later. However, the change in school attachment over those three years, which corresponded to the transition from primary to secondary school, significantly predicted less sleep disruption but not greater sleep duration.
Across both the cross-sectional and longitudinal studies, sleep duration was examined in four relationships (one significant,52 three non-significant).49,54 Insomnia, using a “global” score, was examined in three relationships, and all were significant.45,49,50 Because studies examined different sleep variables, this precluded further synthesis by sleep outcome. We did not discern a clear pattern of results based on whether school connectedness was measured as a “global” score or a single component.
Sub-Group Analyses
Four studies reported results for subgroup analyses or interaction effects.45–47,49 Three studies, all conducted in China, examined the effect of sex/gender: as reported above, Bao et al (2018) found that sleep problems significantly predicted worse school connectedness in boys only;46 Bao et al (2020) found no difference between boys and girls in the association between school connectedness and sleep problems;47 and Sun et al (2024) found no sex differences in the association between school connectedness and insomnia symptoms in a college student sample.45
Yen et al (2008) identified statistically significant interaction effects.49 In depressed adolescents, 48.96% experienced insomnia symptoms who had low levels of school connectedness compared to 34.5% who had high levels of school connectedness (χ2 (df = 1) = 9.829, P < 0.005). In non-depressed adolescents, 14% experienced insomnia symptoms who had low levels of school connectedness compared to 5.2% who had high levels of school connectedness (χ2 (df = 1) = 82.035, P < 0.0001).
Mediation Analyses
No studies conducted mediation analyses to examine how school connectedness and sleep are related. However, three studies from China examined the effect of school connectedness on suicidal ideation/attempts45,48 and deviant peer affiliation47 through sleep (mediator) and all found statistically significant indirect effects (mediation) and direct effects of school connectedness on sleep (as reported in Table 1 and synthesised above).
Discussion
Given how little consideration there has been of the possible role of school social environments on sleep in children and adolescents, we systematically reviewed the evidence for cross-sectional and prospective associations between school connectedness and sleep in primary, secondary, and tertiary education settings. The evidence was weighted towards higher levels of school connectedness being significantly associated with better sleep, and lower levels of school connectedness or school disconnectedness being significantly associated with worse sleep, in middle school adolescents. Notably, we found that school connectedness was more likely to be associated with insomnia than sleep duration. However, given that we only identified a small number of longitudinal studies that reported mixed results and no intervention studies, there was insufficient evidence to determine whether there is a prospective relationship between school connectedness and sleep, and the direction and strength of this effect. We did not find any evidence that greater school connectedness worsens sleep, nor did we identify any studies conducted with children (ie, primary school) or clinical populations (eg, participants with an existing sleep disorder).
These findings are consistent with a growing body of evidence showing that school connectedness is linked to positive health outcomes such as better mental health,29 physical activity,34 and general wellbeing32 in adolescents, and that school-based interventions that aim to improve the social-emotional environment can improve student health outcomes such as depressive symptoms, physical activity, body mass index, fruit and vegetable intake, tobacco use, and being bullied.55 Consistent with biopsychosocial and socio-ecological frameworks3,10,11 and accumulating evidence for the role of social determinants in shaping sleep (eg, social ties),16 this suggests the importance of the school social environment when conceptualising paediatric sleep health. Notably, one of the studies in this review showed that the significant association between social support from peers and better sleep quality in adolescents disappeared once school-related variables (eg, student support) were included in the model.51
Across all studies, we found that school connectedness was more likely to be associated with insomnia symptoms than sleep duration. These findings are congruent with previous evidence in adolescents that show the heterogeneous nature of sleep. For example, one study found that sleep duration and poor subjective sleep quality were associated with depressive symptoms in adolescents but not sleep disturbance, sleep efficiency, or sleep onset latency.56 Although we did not find any studies examining the potential mechanisms through which insomnia is associated with school connectedness, it is possible that low school connectedness increases cognitive, emotional, and physical arousal, which has been implicated in the development and maintenance of insomnia symptoms (ie, frequent difficulties initiating or maintaining sleep or early morning awakenings accompanied by significant distress or impairments to daytime functioning).57 Hyperarousal may occur through school-related stressors, for example, increased worries about relationships with peers and teachers, feelings of loneliness or isolation, being disengaged from learning, or feeling physically or psychologically unsafe at school.58
Further, the relationship between school connectedness and insomnia may also be mediated by mental health problems. Low school connectedness is cross-sectionally and prospectively associated with anxiety and depression,29 both of which are also associated with insomnia (and sleep problems more broadly) in adolescents.59 Interestingly, one of the studies in this review showed that the relationship between school connectedness and insomnia remained significant even after controlling for baseline depression and insomnia, suggesting that the relationship was not fully accounted for by depression,45 while another study found that school connectedness buffered against insomnia symptoms in depressed adolescents.49 In turn, the consequences of poor sleep can further perpetuate hyperarousal, anxiety, and depression,60 and contribute to emotional regulation deficits61 and greater level of negative social evaluative emotions (eg, feeling rejection or embarrassment),62 which can make it harder to connect and socially engage at school. The finding that sleep duration was less likely to be associated with school connectedness may be because students with low school connectedness have more opportunity to sleep as they may participate in fewer school activities and be more disengaged from school relationships and homework, which would otherwise displace time for sleep. Together, these findings suggest the need for future school connectedness studies to examine different aspects of sleep, particularly insomnia, and potential mechanisms of action, especially the links between school connectedness, sleep, and depression and anxiety. It may be that students with elevated insomnia or anxiety and depressive symptoms are good candidates for targeted interventions to enhance school connectedness.
The prospective evidence was limited in this review due to the small number of eligible studies and failure to identify any intervention studies. The mixed results may be a consequence of different sleep outcomes being examined or differences in participant age. It may also be that school connectedness is not sufficiently potent to reliably affect sleep over time. Nonetheless, among the significant prospective associations, we found preliminary evidence to suggest that the relationship is potentially bidirectional. That is, sleep problems significantly predicted less school connectedness and more school connectedness predicted better sleep over time. However, it should be noted that a bidirectional relationship was not found in the only study46 in this review, which explicitly sought to test the bidirectionality hypothesis, suggesting that further investigation is required in future studies that are designed with this question in mind and which control for baseline school connectedness and sleep, among other key confounders (eg, age, mental health).
Future prospective studies will be critical to understanding how the relationship between school connectedness and sleep changes over the course of development and across schooling transitions (eg, from primary to secondary school, and from secondary school to employment or further education). Most studies in this review were conducted with middle school students around 14 years old. This coincides with puberty, a period that is associated with rapid neurobiological and psychosocial changes, which contributes to dramatic alterations to sleep, a rise in the incidence of sleep problems, a steep increase in the prevalence of common mental disorders, and increased salience of peer relationships and group membership.59,63 The relationship between school connectedness and sleep may therefore be particularly strong at this time. Consistent with this, Maume found that the change in school affiliation as students transitioned from primary to secondary school, rather than school affiliation at one point in time, had a significant impact on sleep disruption, even when controlling for pubertal trajectories.54 Interestingly, meta-analyses have shown that school connectedness has a slightly higher protective effect on reducing mental health and violence risks in high school compared to middle school.35 While the relative dearth of studies conducted with primary and tertiary-aged adolescents is consistent with school connectedness studies that examined other health outcomes,29,35 future prospective work should examine the extent to which school connectedness in primary school predicts sleep problems, and vice versa, both in childhood and later in adolescence and young adulthood, as these may guide the ideal timing of interventions.
Previous work has shown that the relationship between school connectedness and some health outcomes (eg, mental health) is stronger for some individuals (eg, sexual and gender minority students)35 and that school connectedness might be a protective factor for sleep problems in some individuals (eg, those experiencing discrimination).24 We found a small number of studies with mixed evidence for the effect of sex/gender on school connectedness and sleep; two longitudinal studies conducted with middle47 and college45 students, respectively, found no significant association and one conducted with middle school students46 found a significant prospective association for boys but only in the direction of sleep problems predicting poorer school connectedness and not vice versa. Although females are typically more likely to report insomnia or sleep problems64 which were the sleep outcomes investigated in these studies, the finding of the latter study is interesting and may indicate that boys who experience sleep problems are vulnerable to impacts on their connection to school.46 Examining whether the relationship between school connectedness and sleep is stronger for particular students will be informative for designing interventions.
To the best of our knowledge, this is the first review on this topic which brings together evidence from sleep and education disciplines. In doing so, it supports a shift in the focus of paediatric sleep health from largely individual-level and biological, psychological, and behavioral factors to also recognising the value of school social environments. The findings of this review can be used to expand existing conceptual models of paediatric sleep health and will be important for informing research aiming to identify sustainable and modifiable targets for the prevention of sleep problems and co-occurring determinants of health, which have historically been difficult at a population level. However, these findings should be considered in the context of some key limitations of the reviewed evidence. Not all studies used validated measures of school connectedness, measured sleep duration in the same way, or adjusted for key confounders (eg, mental health, baseline sleep problems in longitudinal studies), which limits inferences and should be addressed in future studies. Notwithstanding the value and practicality of subjective sleep measures, no studies used an objective measure of sleep. Using consistent and validated measures for both school connectedness (at both the individual and school level) and sleep will be important for future studies. Most studies were conducted with students from China or Taiwan, with the remaining studies conducted across countries in North America and Europe. This potentially limits the generalizability of the findings as these were primarily high-income countries. Further, there are known geographic differences in adolescent sleep characteristics. It is reasonable to assume that there may also be geographic (eg, country or regional level, high-income countries compared to low- and middle-income countries) differences in school connectedness owing to differences in schooling systems (eg, class sizes), resourcing (eg, investment in activities designed to enhance connectedness), teaching approaches (eg, authoritarian or collaborative), and the wider social, cultural, and economic context (eg, the extent to which girls can participate in school life, expectation that students will participate in paid work). For example, there is some evidence that students’ sense of school belonging varies between countries such that students from more egalitarian cultures tend to have a high sense of belonging at school compared to students from more hierarchical cultures.65,66 This suggests that a global health approach is required for future work. In addition, certain limitations of the review methodology should be noted. Issues around the boundaries of the definition of school connectedness have been well described. In this review, we chose to retain the results related to “school pressure” (two relationships) as it was framed alongside teacher and student support in the studies. Although we deemed this to be consistent with our definition of school connectedness, another research team may have chosen to exclude these results. Due to heterogeneity between studies, we could not conduct a meta-analysis or assess publication bias.
Conclusion
This review identified an association between school connectedness and some aspects of sleep, including insomnia, which contributes to the evidence base for the role of school environments on student health. If supported by prospective data, targeting school connectedness has the potential to be an effective primary prevention approach for student sleep. Interventions that aim to improve school connectedness are low in stigma when compared to targeted mental health interventions, accessible by both the health and education workforce, and have the potential to address multiple aspects of health and wellbeing simultaneously. They are consistent with a global movement towards whole-school systems approaches to health and wellbeing in schools that embed programs into the wider policy and social context of the school in an effort to increase the sustainability and scalability of health interventions.19 From a global health lens, the ability to reach large numbers of students may be particularly beneficial in low- and middle-income countries where access to healthcare may be limited and where secondary education systems are quickly expanding.
Trial Registration
PROSPERO (CRD42022316182).
Abbreviations
HBSC, Health Behaviour in School-aged Children; PSQI, Pittsburgh Sleep Quality Index.
Ethical Approval
This study did not require ethical approval as these data were obtained from published, peer-reviewed journal articles.
Acknowldegment
Dr Nilakshi Waidyatillake, Clinical Epidemiologist and Course Convenor: Bachelor Medical Science (Honours) and Associate Director: Clinician Scientist Pathways from the Melbourne Medical School, University of Melbourne, Australia, assisted with the development of the search strategy. This systematic review contributed to the partial fulfilment of the Bachelor of Medical Science research component for authors MNIS and MRC at the Department of Paediatrics, Melbourne Medical School, University of Melbourne, Australia, and Faculty of Medicine, Universitas Indonesia, Indonesia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This review is supported by internal funding from the Melbourne Medical School at the University of Melbourne. Dr Monika Raniti is supported through the Centre of Research Excellence: Driving Global Investment in Adolescent Health funded by the NHMRC (GNT1171981) and the ALIVE National Centre for Mental Health Research Translation (NHMRC Australia Grant GNT2002047). Professor Sawyer is supported by an NHMRC fellowship (GNT1196999) and the Geoff and Helen Handbury Chair of Adolescent Health, Department of Paediatrics, University of Melbourne. Funders were not involved in the review process.
Disclosure
Dr Raniti and Prof Sawyer have previously received consultancy funds from the WHO and UNESCO to produce a body of work related to the ‘Health Promoting Schools’ initiative, and funds from the Wellcome Trust to examine the role of school connectedness in youth depression and anxiety as part of their ‘Active Ingredients’ commission 2021. Mr Suma and Mr Charirilsyah have no known conflicts of interest.
References
1. Matricciani L, Paquet C, Galland B, Short M, Olds T. Children’s sleep and health: a meta-review. Sleep Med Rev. 2019;46:136–150. doi:10.1016/j.smrv.2019.04.011
2. Reynolds AM, Spaeth AM, Hale L, et al. Pediatric sleep: current knowledge, gaps, and opportunities for the future. Sleep. 2023;46(7):zsad060. doi:10.1093/sleep/zsad060
3. Meltzer LJ, Williamson AA, Mindell JA. Pediatric sleep health: it matters, and so does how we define it. Sleep Med Rev. 2021;57:101425. doi:10.1016/j.smrv.2021.101425
4. Cai H, Chen P, Jin Y, et al. Prevalence of sleep disturbances in children and adolescents during COVID-19 pandemic: a meta-analysis and systematic review of epidemiological surveys. Transl Psychiatry. 2024;14(1):12. doi:10.1038/s41398-023-02654-5
5. Kocevska D, Lysen TS, Dotinga A, et al. Sleep characteristics across the lifespan in 1.1 million people from the Netherlands, United Kingdom and United States: a systematic review and meta-analysis. Nat Hum Behav. 2021;5(1):113–122. doi:10.1038/s41562-020-00965-x
6. Buxton OM, Chang A-M, Spilsbury JC, Bos T, Emsellem H, Knutson KL. Sleep in the modern family: protective family routines for child and adolescent sleep. Sleep Health. 2015;1(1):15–27. doi:10.1016/j.sleh.2014.12.002
7. de Zambotti M, Goldstone A, Colrain IM, Baker FC. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12–24. doi:10.1016/j.smrv.2017.06.009
8. Feder MA, Baroni A. Just let me sleep in: identifying and treating delayed sleep phase disorder in adolescents. Child Adolesc Psychiatr Clin North Am. 2024;47(1):163–178. doi:10.1016/j.chc.2020.08.005
9. Gradisar M, Kahn M, Micic G, et al. Sleep’s role in the development and resolution of adolescent depression. Nat Rev Psychol. 2022;1(9):512–523. doi:10.1038/s44159-022-00074-8
10. Becker SP, Langberg JM, Byars KC. Advancing a biopsychosocial and contextual model of sleep in adolescence: a review and introduction to the special issue. J Youth Adolesc. 2015;44:239–270. doi:10.1007/s10964-014-0248-y
11. Crowley SJ, Wolfson AR, Tarokh L, Carskadon MA. An update on adolescent sleep: new evidence informing the perfect storm model. J Adolesc. 2018;67:55–65. doi:10.1016/j.adolescence.2018.06.001
12. Colrain IM, Baker FC. Changes in sleep as a function of adolescent development. Neuropsychol Rev. 2011;21:5–21. doi:10.1007/s11065-010-9155-5
13. Bartel K, Williamson P, van Maanen A, et al. Protective and risk factors associated with adolescent sleep: findings from Australia, Canada, and The Netherlands. Sleep Med. 2016;26:97–103. doi:10.1016/j.sleep.2016.07.007
14. Bauducco S, Gardner L, Champion K, Newton N, Gradisar M. It’s past your bedtime, but does it matter anymore? How longitudinal changes in bedtime rules relate to adolescents’ sleep. J Sleep Res. 2024;33(2):e13940. doi:10.1111/jsr.13940
15. Blake MJ, Trinder JA, Allen NB. Mechanisms underlying the association between insomnia, anxiety, and depression in adolescence: implications for behavioral sleep interventions. Clin Psychol Rev. 2018;63:25–40. doi:10.1016/j.cpr.2018.05.006
16. Tavernier R, Willoughby T. A longitudinal examination of the bidirectional association between sleep problems and social ties at university: the mediating role of emotion regulation. J Youth Adolesc. 2015;44:317–330. doi:10.1007/s10964-014-0107-x
17. Bell AN, Juvonen J. Gender discrimination, perceived school unfairness, depressive symptoms, and sleep duration among middle school girls. Child Dev. 2020;91(6):1865–1876. doi:10.1111/cdev.13388
18. Mayne SL, Mitchell JA, Virudachalam S, Fiks AG, Williamson AA. Neighborhood environments and sleep among children and adolescents: a systematic review. Sleep Med Rev. 2021;57:101465. doi:10.1016/j.smrv.2021.101465
19. Sawyer SM, Raniti M, Aston R. Making every school a health-promoting school. Lancet Child Adolesc Health. 2021;5(8):539–540. doi:10.1016/S2352-4642(21)00190-5
20. Bacaro V, Carpentier L, Crocetti E. Sleep well, study well: a systematic review of longitudinal studies on the interplay between sleep and school experience in adolescence. Int J Environ Res Public Health. 2023;20(6):4829. doi:10.3390/ijerph20064829
21. Albakri U, Drotos E, Meertens R. Sleep health promotion interventions and their effectiveness: an umbrella review. Int J Environ Res Public Health. 2021;18(11):5533. doi:10.3390/ijerph18115533
22. van Geel M, Goemans A, Vedder PH. The relation between peer victimization and sleeping problems: a meta-analysis. Sleep Med Rev. 2016;27:89–95. doi:10.1016/j.smrv.2015.05.004
23. He Y, Chen -S-S, Xie G-D, et al. Bidirectional associations among school bullying, depressive symptoms and sleep problems in adolescents: a cross-lagged longitudinal approach. J Affect Disord. 2022;298:590–598. doi:10.1016/j.jad.2021.11.038
24. Huynh VW, Gillen-O’Neel C. Discrimination and sleep: the protective role of school belonging. Youth Soc. 2016;48(5):649–672. doi:10.1177/0044118X13506720
25. Palmer CA, Powell SL, Deutchman DR, Tintzman C, Poppler A, Oosterhoff B. Sleepy and secluded: sleep disturbances are associated with connectedness in early adolescent social networks. J Adolesc Res. 2022;32(2):756–768. doi:10.1111/jora.12670
26. Nelson EE, Leibenluft E, McClure EB, Pine DS. The social re-orientation of adolescence: a neuroscience perspective on the process and its relation to psychopathology. Psychol Med. 2005;35(2):163–174. doi:10.1017/s0033291704003915
27. García-Moya I, Bunn F, Jiménez-Iglesias A, Paniagua C, Brooks FM. The conceptualisation of school and teacher connectedness in adolescent research: a scoping review of literature. Educ Rev. 2019;71(4):423–444. doi:10.1080/00131911.2018.1424117
28. Hodges A, Cordier R, Joosten A, Bourke-Taylor H, Speyer R. Evaluating the psychometric quality of school connectedness measures: a systematic review. PLoS One. 2018;13(9):e0203373. doi:10.1371/journal.pone.0203373
29. Raniti M, Rakesh D, Patton G, Sawyer S. The role of school connectedness in the prevention of youth depression and anxiety: a systematic review with youth consultation. BMC Public Health. 2022;22(1):2152. doi:10.1186/s12889-022-14364-6
30. Goodenow C. The psychological sense of school membership among adolescents: scale development and educational correlates. Psychol Sch. 1993;30(1):79–90. doi:10.1002/1520-6807(199301)30:1<79::AID-PITS2310300113>3.0.CO;2-X
31. Furlong MJ, O’brennan LM, You S. Psychometric properties of the Add Health School Connectedness Scale for 18 sociocultural groups. Psychol Sch. 2011;48(10):986–997. doi:10.1002/pits.20609
32. Wang M-T, Degol JL. School climate: a review of the construct, measurement, and impact on student outcomes. Edu Psychol Rev. 2016;28(2):315–352. doi:10.1007/s10648-015-9319-1
33. Marraccini ME, Brier ZM. School connectedness and suicidal thoughts and behaviors: a systematic meta-analysis. Sch Psychol. 2017;32(1):5. doi:10.1037/spq0000192
34. Weatherson KA, O’Neill M, Lau EY, Qian W, Leatherdale ST, Faulkner GE. The protective effects of school connectedness on substance use and physical activity. J Adolesc Health. 2018;63(6):724–731. doi:10.1016/j.jadohealth.2018.07.002
35. Rose ID, Lesesne CA, Sun J, Johns MM, Zhang X, hertz M. The relationship of school connectedness to adolescents’ engagement in co-occurring health risks: a meta-analytic review. J Sch Nurs. 2024;40(1):58–73. doi:10.1177/10598405221096802
36. Blossom JB, Adrian MC, Vander Stoep A, McCauley E. Mechanisms of change in the prevention of depression: an indicated school-based prevention trial at the transition to high school. J Am Acad Child Psy. 2020;59(4):541–551. doi:10.1016/j.jaac.2019.05.031
37. Singla DR, Shinde S, Patton G, Patel V. The mediating effect of school climate on adolescent mental health: findings from a randomized controlled trial of a school-wide intervention. J Adolesc Health. 2021;69(1):90–99. doi:10.1016/j.jadohealth.2020.09.030
38. Willis TA, Gregory AM. Anxiety disorders and sleep in children and adolescents. Sleep Med Clin. 2015;10(2):125–131. doi:10.1016/j.jsmc.2015.02.002
39. Arslan G. School belongingness, well-being, and mental health among adolescents: exploring the role of loneliness. Aust J Psychol. 2021;73(1):70–80. doi:10.1080/00049530.2021.1904499
40. Short MA, Gradisar M, Lack LC, et al. A cross-cultural comparison of sleep duration between US and Australian adolescents: the effect of school start time, parent-set bedtimes, and extracurricular load. Health Educ Behav. 2013;40(3):323–330. doi:10.1177/1090198112451266
41. Bauducco S, Boersma K, Gradisar M. Sleepy and popular? The association between popularity, sleep duration, and insomnia in adolescents. Frontiers in Sleep. 2024;3:1346806. doi:10.3389/frsle.2024.1346806
42. Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adoles Health. 2018;2(3):223–228. doi:10.1016/S2352-4642(18)30022-1
43. NHLBI. Study Quality Assessment Tools. NIH National Heart, Lung and Blood Institute. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
44. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. 2021:372. doi:10.1136/bmj.n71.
45. Sun M, Scherffius A, Sun M, Chen C, Wang D. Insomnia symptoms as a mediator between school connectedness and suicidal ideation in Chinese adolescents: a three-wave longitudinal model. Early Interv Psychia. 2024. doi:10.1111/eip.13579
46. Bao Z, Chen C, Zhang W, Jiang Y, Zhu J, Lai X. School connectedness and Chinese adolescents’ sleep problems: a cross‐lagged panel analysis. J Sch Health. 2018;88(4):315–321. doi:10.1111/josh.12608
47. Bao Z, Jiang Y, Zhu J, Zhang W. School connectedness and deviant peer affiliation among Chinese adolescents: the mediating role of sleep problems. Curr Psychol. 2020;1–10. doi:10.1007/s12144-020-00731-2
48. Li D, Bao Z, Li X, Wang Y. Perceived school climate and Chinese adolescents’ suicidal ideation and suicide attempts: the mediating role of sleep quality. J Sch Health. 2016;86(2):75–83. doi:10.1111/josh.12354
49. Yen C-F, Ko C-H, Yen J-Y, Cheng C-P. The multidimensional correlates associated with short nocturnal sleep duration and subjective insomnia among Taiwanese adolescents. Sleep. 2008;31(11):1515–1525. doi:10.1093/sleep/31.11.1515
50. Hsieh Y-P, Lu W-H, Yen C-F. Psychosocial determinants of insomnia in adolescents: roles of mental health, behavioral health, and social environment. Front Neurosci. 2019;13:848. doi:10.3389/fnins.2019.00848
51. Delaruelle K, Dierckens M, Vandendriessche A, Deforche B, Poppe L. Adolescents’ sleep quality in relation to peer, family and school factors: findings from the 2017/2018 hBSC study in Flanders. Qual Life Res. 2021;30(1):55–65. doi:10.1007/s11136-020-02614-2
52. Eichenlaub J-B, Pinelli M, Portrat S. Sleep habits and their relation to self-reported attention and class climate in preteens. Sleep Med. 2023;101:421–428. doi:10.1016/j.sleep.2022.11.032
53. Benzi IMA, Gallus S, Santoro E, Barone L. Psychosocial determinants of sleep difficulties in adolescence: the role of perceived support from family, peers, and school in an Italian HBSC sample. Eur J Pediatr. 2023;182(6):2625–2634. doi:10.1007/s00431-023-04934-0
54. Maume DJ. Social ties and adolescent sleep disruption. J Health Soc Behav. 2013;54(4):498–515. doi:10.1177/0022146513498512
55. Langford R, Bonell C, Jones H, et al. The World Health Organization’s Health Promoting Schools framework: a Cochrane systematic review and meta-analysis. BMC Public Health. 2015;15:1–15. doi:10.1186/s12889-015-1360-y
56. Raniti MB, Allen NB, Schwartz O, et al. Sleep duration and sleep quality: associations with depressive symptoms across adolescence. Behav Sleep Med. 2017;15(3):198–215. doi:10.1080/15402002.2015.1120198
57. Dressle RJ, Riemann D. Hyperarousal in insomnia disorder: current evidence and potential mechanisms. J Sleep Res. 2023;32(6):e13928. doi:10.1111/jsr.13928
58. Maskevich S, Cassanet A, Allen NB, Trinder J, Bei B. Sleep and stress in adolescents: the roles of pre-sleep arousal and coping during school and vacation. Sleep Med. 2020;66:130–138. doi:10.1016/j.sleep.2019.10.006
59. Raniti MB, Trinder J, Allen NB. Sleep, anxiety, and depression in adolescence: a developmental cognitive neuroscience approach. In: Cohen Kadosh K editor. Oxford Handbook of Developmental Cognitive Neuroscience. Oxford University Press; 2021:1019–1048. doi:10.1093/oxfordhb/9780198827474.013.31.
60. Lovato N, Gradisar M. A meta-analysis and model of the relationship between sleep and depression in adolescents: recommendations for future research and clinical practice. Sleep Med Rev. 2014;18(6):521–529. doi:10.1016/j.smrv.2014.03.006
61. Baum KT, Desai A, Field J, Miller LE, Rausch J, Beebe DW. Sleep restriction worsens mood and emotion regulation in adolescents. J Child Psychol Psychiatr. 2014;55(2):180–190. doi:10.1111/jcpp.12125
62. Tavernier R, Choo SB, Grant K, Adam EK. Daily affective experiences predict objective sleep outcomes among adolescents. J Sleep Res. 2016;25(1):62–69. doi:10.1111/jsr.12338
63. Vijayakumar N, Husin HM, Dashti SG, et al. Characterization of puberty in an Australian population-based cohort study. J Adolesc Health. 2024;74(4):665–673. doi:10.1016/j.jadohealth.2023.08.035
64. Baker FC, Yűksel D, de Zambotti M. Sex differences in sleep. Sleep Disorders Women. 2020;55–64. doi:10.1007/978-3-030-40842-8_5
65. Allen KA, Gallo Cordoba B, Ryan T, et al. Examining predictors of school belonging using a socio-ecological perspective. J Child Fam Stud. 2023;32(9):2804–2819. doi:10.1007/s10826-022-02305-1
66. Chiu MM, Chow BWY, McBride C, mol ST. Students’ sense of belonging at school in 41 countries: cross-cultural variability. J Cross-Cultural Psychol. 2016;47(2):175–196. doi:10.1177/0022022115617031
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.