")
Back to Journals » Journal of Inflammation Research » Volume 18
The Association of Polymorphisms in Interleukin-6 (IL-6), Interleukin-10 (IL-10), IL-6 Receptor, and IL-10 Receptor Genes with the Risk of Pediatric Inflammatory Bowel Disease
Authors Krawiec P , Lejman M, Pac-Kożuchowska E
Received 7 March 2025
Accepted for publication 27 May 2025
Published 26 June 2025 Volume 2025:18 Pages 8389—8397
DOI https://doi.org/10.2147/JIR.S524632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nadia Andrea Andreani
Paulina Krawiec,1 Monika Lejman,2 Elżbieta Pac-Kożuchowska1
1Department of Pediatrics and Gastroenterology, Medical University of Lublin, Lublin, 20-059, Poland; 2Independent Laboratory of Genetic Diagnostics, Medical University of Lublin, Lublin, 20-059, Poland
Correspondence: Paulina Krawiec, Department of Pediatrics and Gastroenterology, Medical University of Lublin, Racławickie 1, Lublin, 20-059, Poland, Tel +48817185420, Email [email protected]
Purpose: Inflammatory bowel disease (IBD) results from a complex interplay between genetic, immune, and environmental factors. Despite a significant advancement in genetic studies, until now, little is known about genotype–phenotype correlations in children with IBD. Thus, we aimed to evaluate if polymorphisms in the Interleukin-6 (IL-6), Interleukin-10 (IL-10), IL-6 receptor, and IL-10 receptor genes are associated with the risk for pediatric IBD, its phenotype and severity.
Patients and Methods: We enrolled 50 children with IBD in the study group and 20 healthy children to the control group. Demographic and clinical data of the subjects were collected from available electronic medical records. The DNA was extracted from peripheral blood samples of all individuals. TaqMan® single nucleotide polymorphism (SNP) genotyping assays were used to detect IL-10 variants RS3024505 and RS1800872, IL-10RA RS3135932, IL-10RB RS2834167, IL-6 RS10499563, and IL-6R RS4537545. A binary logistic regression model was used to evaluate the association between SNP’s and the risk of IBD, IBD onset, phenotype, and the need to use of steroids or biologics.
Results: There was a significant difference in the genotype distribution of IL-6 RS10499563 between patients with IBD and control group (χ 2 = 10.96, p = 0.004). The distribution of genotype CT at IL-6 RS10499563 was higher, whereas the distribution of genotype CC and TT at IL-6 RS10499563 was lower in children compared to controls. There were no significant differences in the distribution of the other SNPs between the study and control groups. We found a significant association between the genotype CT at IL-6 RS10499563 and the risk of ulcerative colitis (OR 13.41; 95% CI: 1.58– 114.26; p = 0.02), but not Crohn’s disease (OR 7.60; 95% CI: 0.82– 70.16; p = 0.07).
Conclusion: In this study, we found a significant association between the genotype CT at IL-6 RS10499563 and the risk of ulcerative colitis in children.
Keywords: Crohn’s disease, ulcerative colitis, children, genetics
Introduction
Recent epidemiological studies have indicated an increasing prevalence and incidence of inflammatory bowel disease (IBD), particularly in children and adolescents.1,2 The disease tends to have a more severe course and behavior in the pediatric population compared to adults.3 Thus, there is a need to identify predictive factors of aggressive course of IBD to optimize the decision-making process regarding the treatment strategies in individuals.
The complex pathogenesis of IBD is determined by the tissue damage due to an aberrant mucosal immune response to commensal bacteria in a genetically susceptible host.4,5 Genome-wide association (GWAS) studies have detected more than 240 susceptibility genes related to an increased risk of IBD.6,7 The majority of these genes code molecules involved in various mechanisms critical for the maintenance of intestinal homeostasis including in particular the innate and adaptive immune response, regulation of epithelial function, autophagy, and reactive oxygen species generation.8 Crucial role in the orchestration of the mucosal homeostasis plays cytokines and cytokines’ receptors.4 Disruption of these precise mechanisms results in the inflammatory cascade and development of IBD4. Despite significant advancement in genetic studies, until now little is known about the genetic background of IBD and genotype–phenotype correlations in pediatric patients.9,10
The aim of the study was to explore whether polymorphisms in Interleukin-6 (IL-6), Interleukin-10 (IL-10), IL-6 receptor, and IL-10 receptor genes are associated with risk for IBD in children. The second aim was to evaluate if these polymorphisms were associated with IBD phenotype and severity.
Materials and Methods
A total of 50 children with inflammatory bowel disease were enrolled in this study from inpatients of the Department of Pediatrics and Gastroenterology, Medical University of Lublin, Poland, between May 2018 and March 2020.
Inflammatory bowel disease was diagnosed based on a combination of clinical evaluation, results of laboratory and imaging studies, and esophagogastroduodenoscopy and ileocolonoscopy with histology according to the European Society of Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) revised Porto criteria.11 The IBD phenotype at disease onset was categorized according to the Paris classification.12 The clinical activity of Crohn’s disease was assessed using the Pediatric Crohn’s Disease Activity Index (PCDAI),13 while the clinical activity of ulcerative colitis was scored using the Pediatric Ulcerative Colitis Activity Index (PUCAI).14 Clinical remission of Crohn’s disease was defined as the PCDAI of 10 or less points, and an active phase as the PCDAI of more than 10 points.13 Clinical remission of ulcerative colitis was categorized as the PUCAI of less than 10 points, and n active phase as the PUCAI of 10 or more points.14
Demographic and clinical data of subjects including patients’ age at the IBD onset, gender, IBD severity, location, and the required treatment were retrieved from available electronic medical records.
The control group comprised healthy children. Healthy children were selected from a group of patients hospitalized due to foreign body ingestion. The exclusion criteria were as follows: ongoing or previous history of any chronic organic disease, any clinical or laboratory signs of acute or chronic inflammation at the time of recruitment, and lack of informed consent for the participation in the study.
The genetic analysis was performed at the Independent Laboratory of Genetic Diagnostics, Medical University of Lublin. The DNA was extracted from EDTA-stabilized peripheral blood samples from all patients and healthy controls by using a QIAamp DNA Blood Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s recommendations. The SNPs were chosen from the literature studies.15–18 IL-10 variants RS3024505 and RS1800872, IL-10RA variant RS3135932, IL-10RB variant RS2834167, IL-6 variant RS10499563, and IL-6R variant RS453754513 were genotyped using pre-developed allelic discrimination assays (Applied Biosystems). Genotyping reaction was performed in a final volume of 25 μL consisting of 12.5 μL TaqMan Genotyping Master Mix, 1.25 μL 20 × TaqMan SNP Genotyping Assays and 11.25 μL genomic DNA. Genotyping was performed by TaqMan real-time PCR on Quant Studio 5 (ThermoFisher Scientific), using Allelic Discrimination. Ten nanograms of DNA was genotyped in 25 μL containing 1 × Mastermix (Applied Biosystems, Nærum, Denmark), 250 nM probes, and 900 nM primers or as recommended by the manufacturer for predesigned assays. Controls for known genotypes were included in each run, and repeated genotyping of a random 10% subset yielded 100% identical genotypes.
Statistical Analysis
Continuous variables were presented as means, standard deviation, median, and range. Categorical variables were described as frequencies, percentages, and proportions. Differences between groups for continuous variables were evaluated using the t-test for normally distributed data, the Wilcoxon rank-sum test for non-normally distributed data. Differences between the groups for categorical variables were evaluated using the chi-square test. Binary logistic regression model was used to evaluate the association between SNP’s and the risk of IBD, and the association between SNP’s and IBD onset, phenotype, and the need to use steroids or biologics. The p-value below 0.05 was considered statistically significant. The statistical analysis was performed using STATA 18.0 StataCorp.
Since there are limited number of studies in the existing literature providing data on examined SNP’s and pediatric inflammatory bowel disease, our study is of preliminary nature, allowing sample size estimation for potential future studies.
Results
The study group consisted of 50 children with inflammatory bowel disease including 29 (52%) children with ulcerative colitis and 21 (42%) with Crohn’s disease. The basic characteristics of the study group are presented in Table 1.
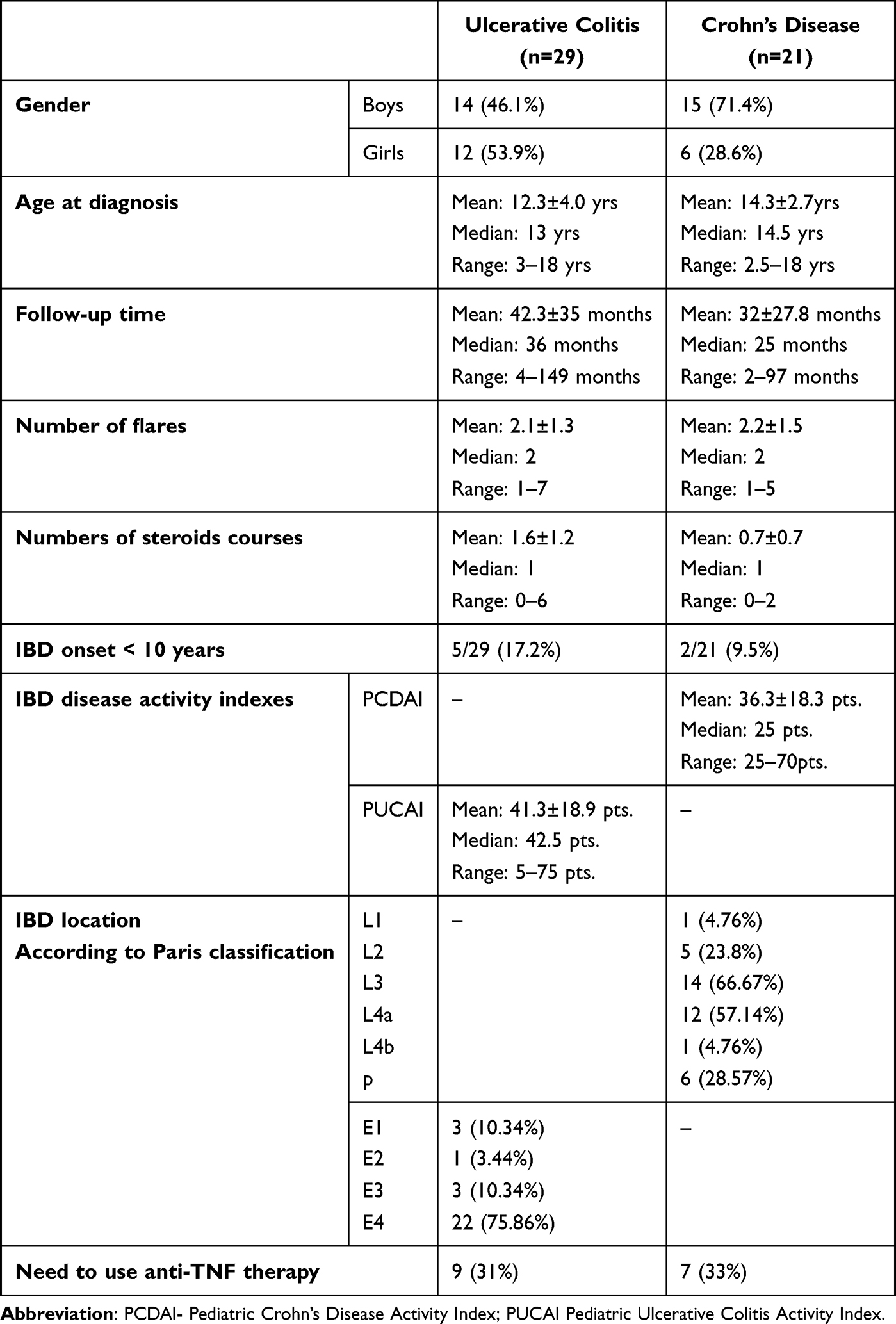 |
Table 1 Demographic and Clinical Characteristics of Children with IBD |
We recruited 20 healthy children for the control group, including 13 girls (65%) and 7 boys (35%). The age of the children in the control group ranged from 4 to 16 years old, the mean age was 11.9 ± 3.4 years old, and the median was 13.25 years.
The genotype distribution and allele frequencies of the examined polymorphisms are presented in Table 2. There was a significant difference in the genotype distribution of IL-6 RS10499563 between patients with IBD and control group (χ2 = 10.96, p = 0.004). The distribution of genotype CT at IL-6 RS10499563 was higher, whereas the distribution of genotype CC and TT at IL-6 RS10499563 was lower in children with IBD compared to controls. No other significant differences were observed among the groups.
 |
Table 2 Comparison of Genotypes’ Distribution Between Patients with IBD and Controls |
Analysis of the association of the examined polymorphisms and IBD risk in our study group is presented in Table 3. There was a significant association between genotype CT in IL-6 RS10499563 and the risk of IBD (OR 10.69; 95% CI 1.31–86.59; p = 0.03). A detailed analysis revealed a significant association between the genotype CT at IL-6 RS10499563 and the risk of ulcerative colitis (OR 13.41; 95% CI 1.58–114.26; p = 0.02), but not Crohn’s disease (OR 7.60; 95% CI 0.82–70.16; p = 0.07).
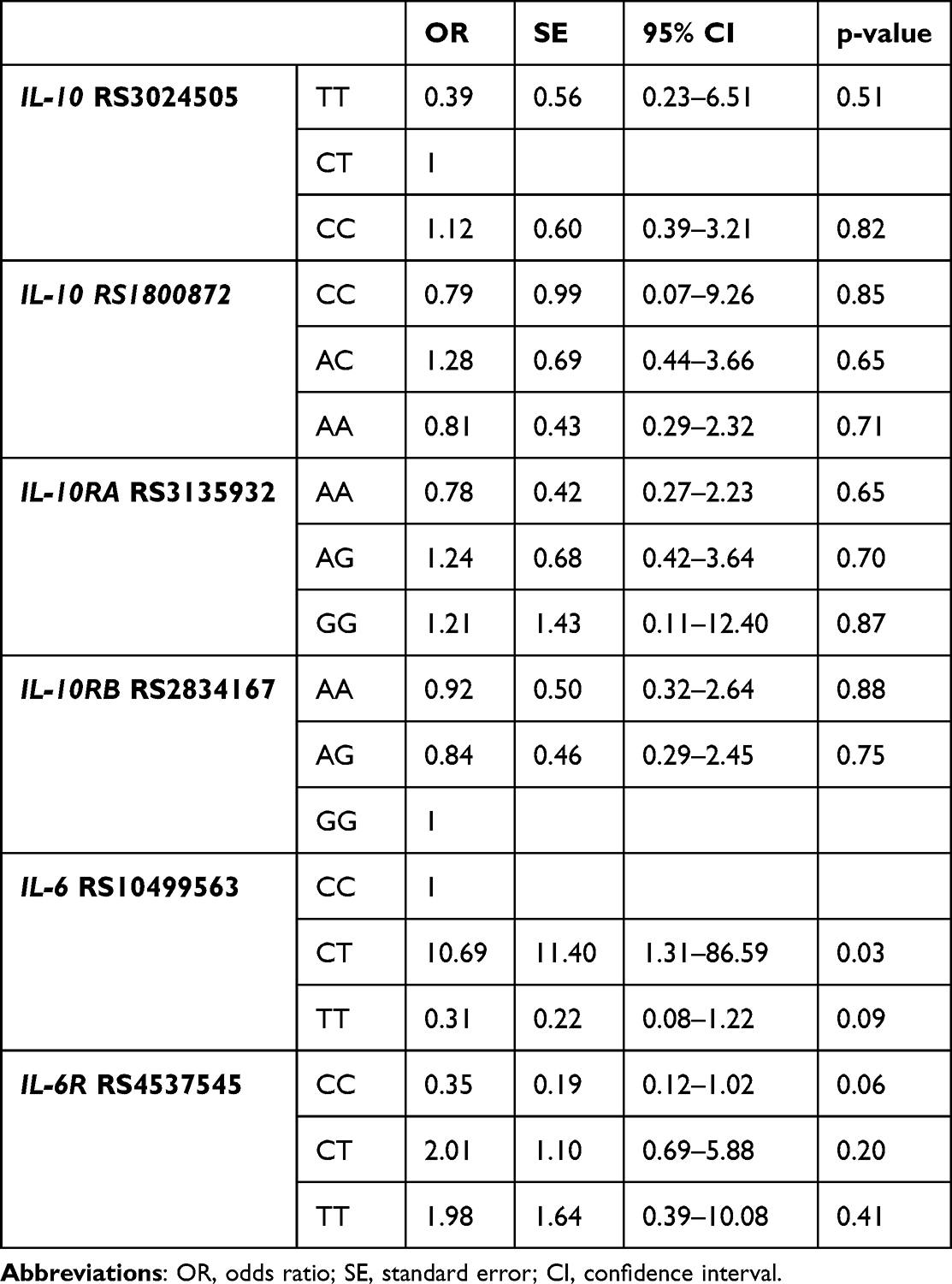 |
Table 3 Logistic Regression Analysis of the Association Between Studied SNP’s and the Risk of IBD |
In our group of patients, we did not find any association between the studied SNP’s and the risk of IBD onset below 10 years of age (Supplementary Table 1). None of the SNP’s were associated with the need to use any anti-tumor necrosis factor (anti-TNF) drugs or steroids within the follow-up period (Supplementary Tables 2 and 3).
Discussion
This study, for the first time, revealed an association between the genotype CT of IL-6 RS10499563 and the risk of ulcerative colitis. The distribution of genotypes at IL-10 RS3024505, IL-10 RS1800872, IL-10RA RS3135932, IL-10RB RS2834167, and IL-6R RS4537545 did not differ significantly between the children with IBD and the control group. There was no association between the studied polymorphisms of Interleukin-10, IL-10 receptor, and IL-6 receptor genes and the risk of IBD. This may reflect the general concept of IBD pathogenesis, assuming the contribution of various environmental factors and genetic susceptibility to IBD development.
Contrary results were reported by Bank et al in a Danish cohort of patients with IBD. In this study, there was no association between IL-6 RS10499563 and the risk for IBD.16 However, in the previous studies among patients with IBD the significance of IL-6 RS10499563 in predicting treatment response has been evaluated.15,19,20 Salvador-Martin et al found that this variant of the IL-6 gene was significantly associated with a response to anti-tumor necrosis factor (anti-TNF) drugs in children with Crohn’s disease.20 Moreover, the C allele in the IL-6 (RS10499563) was associated with supratherapeutic trough levels of infliximab (>7ug/mL) and was predictive of a longer response time to anti-TNF therapy20 in children with Crohn’s disease.19,20 Similar observations were reported in an adult population of patients with IBD. Variant RS10499563 was associated with a beneficial response to anti-TNF treatment in adults with ulcerative colitis and in IBD in general.15 These findings may imply a significant impact in the development of a personalized treatment approaches tailored to individuals with IBD.
Although the association between the IL-6 RS10499563 and the risk of IBD has not been widely explored, another polymorphism in IL-6 gene was found to be strongly related to IBD. A recent meta-analysis of nine studies including 1249 cases and 2804 controls showed a significant association between IL-6 RS1800795 and the risk of IBD in the general population and Caucasians.21
In our study, we did not demonstrate an association between the other analyzed SNPs; however, in the current literature, there are research studies reporting the relationship among these polymorphisms and IBD susceptibility.
Lin et al presented that two IL-10 SNP’s RS1800872 and RS3024496, and SNP’s in IL-10 pathway genes ie, IL-10RA RS3135932 and IL-10RB RS2834167 were not associated with pediatric IBD.18 The only polymorphism associated with IBD was IL-10 RS3024496 (OR 1.487; 95% CI 1.055–2.099; p = 0.022).18 However, the epistasis analysis detected interactions between two SNP’s in the IL-10 gene ie, RS1800872 and RS3024496, and between SNP’s in IL-10 RS1800872, IL-10 RS3024496 and IL-10RA RS3135932, that are associated with an increased risk of IBD in childhood.18
In a Danish case–control study performed among adults with IBD, it has been also demonstrated that the polymorphism IL-10 RS3024505 increased the risk of ulcerative colitis (OR 1.43; 95% CI 1.12–1.82; p = 0.004) and Crohn’s disease (OR 1.40; 95% CI 1.06–1.85; p = 0.02).17 The risk of IBD was not associated with IL-10 RS1800872, IL-10 RS1800871 or IL-10 RS1800896.17
Moreover, a variant of IL-6R RS4537545 was identified as a susceptibility polymorphism for Crohn’s disease (OR: 1.73, 95% CI: 1.12–2.66, p = 0.01).16
A possible explanation for the inconsistency between the studies on the genetic polymorphisms linked to the susceptibility of IBD may be heterogeneity of studied groups. This may also be a consequence of various magnitude effects of environmental factors on IBD development in different populations.
Our study has several limitations including a relatively small sample size and homogenous group of patients that may affect the findings of genotype–phenotype relationships in this group of patients. This limitation hinders the generalizability of our results and confines extrapolation of our results to other populations. Moreover, it should be highlighted that genetic polymorphisms contribute to the susceptibility for inflammatory bowel disease. However, the development of inflammatory bowel disease results from a complex interplay between genetic and environmental factors. The lack of data on exposure to various environmental factors in our study group limits the ability to explore interactions between genetic polymorphisms and environment underlying the development of IBD. Future studies should incorporate analysis of gene-environment links in pediatric IBD.
Conclusion
To conclude, our study revealed an association between the genotype CT of IL-6 RS10499563 and the development of ulcerative colitis. However, further research is needed to validate replication of our findings in other populations of patients with IBD. Interleukin-6 is a central cytokine involved in promoting and sustaining chronic intestinal inflammation.22 Thus, it appears that the IL-6 signaling pathway should be considered as a therapeutic target for pediatric IBD. Recent studies have shown that IL-6 trans-signaling mode, via IL-6, and its soluble receptor IL-6R, and two molecules of the transmembrane protein gp130 acting as the signal transducer, plays a primary role in orchestrating gut inflammation.22–24 Until now, a growing body of evidence suggests the efficacy of blockade of IL-6 trans-signaling in adults with IBD.23,24 However, further studies are required to explore the interplay between genetic susceptibility and environmental factors in the development of IBD and genotype–phenotype associations in patients with IBD.
Ethics
The study was approved by the Bioethical Committee of the Medical University of Lublin (KE-0254/97/2018) and conducted in accordance with the principles of the Declaration of Helsinki. Written informed parental consent for participation in this research study was required, and in the case of a child older than 16 years of age simultaneously signed by a patient.
Acknowledgments
The manuscript preparation was supported during the Harvard Medical School’s Polish Clinical Scholars Research Training Program, organized by the Agencja Badań Medycznych (ABM, English: Medical Research Agency, Warsaw, Poland). Paulina Krawiec participated in this program.
Funding
This study was funded by the Medical University of Lublin; Grant No. DS406 to Elżbieta Pac-Kożuchowska and DS411 to Monika Lejman.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ye Y, Manne S, Treem WR, Bennett D. Prevalence of inflammatory Bowel Disease in pediatric and adult populations: recent estimates from Large National Databases in the United States, 2007–2016. Inflamm Bowel Dis. 2020;26(4):619–625. doi:10.1093/ibd/izz182
2. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769–2778. doi:10.1016/S0140-6736(17)32448-0
3. Malham M, Jakobsen C, Vester-Andersen MK, et al. Paediatric onset inflammatory bowel disease is a distinct and aggressive phenotype—a comparative population-based study. GastroHep. 2019;1(6):266–273. doi:10.1002/ygh2.368
4. Magyari L, Kovesdi E, Sarlos P, Javorhazy A, Sumegi K, Melegh B. Interleukin and interleukin receptor gene polymorphisms in inflammatory bowel diseases susceptibility. World J Gastroenterol. 2014;20(12):3208–3222. doi:10.3748/wjg.v20.i12.3208
5. Schirmer M, Garner A, Vlamakis H, Xavier RJ. Microbial genes and pathways in inflammatory bowel disease. Nat Rev Microbiol. 2019;17(8):497–511. doi:10.1038/s41579-019-0213-6
6. El Hadad J, Schreiner P, Vavricka SR, Greuter T. The genetics of inflammatory Bowel Disease. Mol Diagnosis Ther. 2024;28(1):27–35. doi:10.1007/s40291-023-00678-7
7. Kakuta Y, Naito T, Kinouchi Y, Masamune A. Current status and future prospects of inflammatory Bowel Disease genetics. Digestion. 2022;104(1):7–15. doi:10.1159/000527340
8. Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis of inflammatory bowel disease. Nature. 2011;474(7351):307–317. doi:10.1038/nature10209
9. Shaw KA, Cutler DJ, Okou D, et al. Genetic variants and pathways implicated in a pediatric inflammatory bowel disease cohort. Genes Immun. 2019;20(2):131–142. doi:10.1038/s41435-018-0015-2
10. Li X, Song P, Timofeeva M, et al. Systematic meta-analyses and field synopsis of genetic and epigenetic studies in paediatric inflammatory bowel disease. Sci Rep. 2016;6:34076. doi:10.1038/srep34076
11. Levine A, Koletzko S, Turner D, et al. ESPGHAN revised Porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr. 2014;58(6):795–806. doi:10.1097/MPG.0000000000000239
12. Levine A, Griffiths A, Markowitz J, et al. Pediatric modification of the Montreal classification for inflammatory bowel disease: the Paris classification. Inflamm Bowel Dis. 2011;17(6):1314–1321. doi:10.1002/ibd.21493
13. Hyams JS, Ferry GD, Mandel FS, et al. Development and validation of a pediatric Crohn’s disease activity index. J Pediatr Gastroenterol Nutr. 1991;12(4):439–447.
14. Turner D, Otley AR, Mack D, et al. Development, validation, and evaluation of a pediatric ulcerative colitis activity index: a prospective multicenter study. Gastroenterology. 2007;133(2):423–432. doi:10.1053/j.gastro.2007.05.029
15. Bank S, Andersen PS, Burisch J, et al. Associations between functional polymorphisms in the NFκB signaling pathway and response to anti-TNF treatment in Danish patients with inflammatory bowel disease. Pharmacogenomics J. 2014;14(6):526–534. doi:10.1038/tpj.2014.19
16. Bank S, Skytt Andersen P, Burisch J, et al. Polymorphisms in the inflammatory pathway genes TLR2, TLR4, TLR9, LY96, NFKBIA, NFKB1, TNFA, TNFRSF1A, IL6R, IL10, IL23R, PTPN22, and PPARG are associated with susceptibility of inflammatory bowel disease in a Danish cohort. PLoS One. 2014;9(6):e98815. doi:10.1371/journal.pone.0098815
17. Andersen V, Ernst A, Christensen J, et al. The polymorphism rs3024505 proximal to IL-10 is associated with risk of ulcerative colitis and Crohns disease in a Danish case-control study. BMC Med Genet. 2010;11:82. doi:10.1186/1471-2350-11-82
18. Lin Z, Wang Z, Hegarty JP, et al. Genetic association and epistatic interaction of the interleukin-10 signaling pathway in pediatric inflammatory bowel disease. World J Gastroenterol. 2017;23(27):4897–4909. doi:10.3748/wjg.v23.i27.4897
19. Salvador-Martín S, López-Cauce B, Nuñez O, et al. Genetic predictors of long-term response and trough levels of infliximab in Crohn’s disease. Pharmacol Res. 2019;149:104478. doi:10.1016/j.phrs.2019.104478
20. Salvador-Martín S, Bossacoma F, Pujol-Muncunill G, et al. Genetic predictors of long-term response to antitumor necrosis factor agents in pediatric inflammatory Bowel Disease. J Pediatr Gastroenterol Nutr. 2020;71(4):508–515. doi:10.1097/MPG.0000000000002840
21. Liu W, Wang C, Tang L, Yang H. Associations between gene polymorphisms in pro-inflammatory cytokines and the risk of inflammatory Bowel Disease: a meta-analysis. Immunol Invest. 2021;50(8):869–883. doi:10.1080/08820139.2020.1787438
22. Alhendi A, Naser SA. The dual role of interleukin-6 in Crohn’s disease pathophysiology. Front Immunol. 2023;14:1295230. doi:10.3389/fimmu.2023.1295230
23. Schreiber S, Aden K, Bernardes JP, et al. Therapeutic Interleukin-6 trans-signaling inhibition by Olamkicept (sgp130Fc) in patients with active inflammatory Bowel Disease. Gastroenterology. 2021;160(7):2354–2366.e11. doi:10.1053/j.gastro.2021.02.062
24. Zhang S, Chen B, Wang B, et al. Effect of induction therapy with Olamkicept vs Placebo on clinical response in patients with active ulcerative colitis: a randomized clinical trial. JAMA. 2023;329(9):725–734. doi:10.1001/jama.2023.1084
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Biosimilars in Pediatric IBD: Updated Considerations for Disease Management
Dipasquale V, Cucinotta U, Romano C
Biologics: Targets and Therapy 2022, 16:57-66
Published Date: 13 June 2022
Atypical Forms of Pyoderma Gangrenosum in Inflammatory Bowel Disease: Report of Four Cases and Literature Review
Martinelli VF, Martinelli Barbosa P, Dantas de Oliveira LS, Melo LALV, Casa Nova JM, Brito CAA
International Medical Case Reports Journal 2022, 15:449-456
Published Date: 26 August 2022
A Review on Inflammatory Bowel Diseases: Recent Molecular Pathophysiology Advances
Abdulla M, Mohammed N
Biologics: Targets and Therapy 2022, 16:129-140
Published Date: 12 September 2022
Paediatric Pyodermatitis-Pyostomatitis Vegetans Without Underlying Inflammatory Bowel Disease: A Case Report of a 3-Year-Old African Girl
Maruma F, Makuru H
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2363-2367
Published Date: 3 November 2022
The Association Between Inflammatory Bowel Disease and Exposure to Tobacco Smoking: A Case-Control Study in Qatar
Abdallah B, Arif M, Al-Malki M, Hourani R, Al-Maadeed T, Khodr N, Al-Kuwari G, Al-Siddiqi M, Kane T, Chivese T
International Journal of General Medicine 2023, 16:233-242
Published Date: 21 January 2023