")
Back to Journals » Journal of Pain Research » Volume 18
The Effect of Postoperative Tranexamic Acid and Dexamethasone on Quality of Recovery After Arthroscopic Rotator Cuff Repair: a Double-Blinded, Randomized Controlled Trial
Authors Jiang X, Xu C , Yuan C, Gao W, Liu W, Wang Y, Wang H, Yu W, He Y
Received 17 October 2024
Accepted for publication 13 January 2025
Published 20 January 2025 Volume 2025:18 Pages 259—270
DOI https://doi.org/10.2147/JPR.S497297
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Xiping Jiang,1,* Cheng Xu,2,* Chenrui Yuan,1,* Wenliang Gao,3 Wencai Liu,1 Yifei Wang,1 Haiming Wang,1 Weilin Yu,1 Yaohua He1,4
1Department of Orthopedic Surgery, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200233, People’s Republic of China; 2Department of Anesthesiology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200233, People’s Republic of China; 3Department of Orthopedics, Longyan First Affiliated Hospital of Fujian Medical University, Longyan, Fujian, 364000, People’s Republic of China; 4Department of Orthopedic Surgery, Jinshan District Central Hospital Affiliated to Shanghai University of Medicine & Health Sciences, Jinshan Branch of Shanghai Sixth People’s Hospital, Shanghai, 201500, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weilin Yu; Yaohua He, Department of Orthopedic Surgery, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200233, People’s Republic of China, Tel +86 021 64369181, Email [email protected]; [email protected]
Purpose: Arthroscopic rotator cuff repair (ARCR) commonly results in significant postoperative pain. Adjuncts like dexamethasone (DEX) and tranexamic acid (TXA) are used to enhance postoperative recovery. This study aimed to determine whether the combined application of TXA and DEX could improve postoperative recovery during the first 24 hours in ARCR patients. Our goal is to relieve the acute postoperative pain and promote fast recovery and rapid discharge for ARCR patients.
Patients and Methods: Ninety-six patients who underwent ARCR from December 2023 to March 2024 were enrolled in this double-blinded, randomized control trial (Registration number, ChiCTR2300078507). Patients were randomized to intravenously receive 200mL of normal saline (control group), 200mL of 1g TXA in saline (TXA group), or 200 mL of 1g TXA and 5mg DEX in saline (TXA+DEX group) within 2 hours postoperatively. The primary outcome was the Quality of Recovery-15 (QoR-15) score at 24 hours post-surgery. Secondary outcomes included mean visual analog scale (VAS) scores every four hours within 24 hours, postoperative blood test results the day after surgery, and American Shoulder and Elbow Surgeons (ASES) score at 3 months postoperatively.
Results: No significant differences in QoR-15 scores at 24 hours were observed among the groups [control, 127.0 (112.8, 138.0); TXA, 125.0 (116.5, 136.8); TXA+DEX, 132.0 (120.3, 140.8), p = 0.176]. VAS scores at 5– 8 (placebo vs TXA+DEX, p = 0.014; TXA vs TXA+DEX, p = 0.002), 9– 12 (placebo vs TXA+DEX, p = 0.008; TXA vs TXA+DEX, p < 0.001), and 13– 16 (placebo vs TXA+DEX, p = 0.035; TXA vs TXA+DEX, p = 0.013) hours postoperatively showed a significant decrease for the TXA+DEX group compared with the control or TXA group. There were no significant differences in postoperative blood test results and ASES score at 3 months postoperatively.
Conclusion: Postoperative application of TXA alone could not facilitate postoperative recovery during the first 24 hours in ARCR patients. Although the combination of TXA and DEX presented better levels of postoperative pain between 5 and 16 hours than the control and TXA alone, it did not significantly improve postoperative recovery quality. Further large-scale and multi-center investigation is required to determine if the combined application of TXA and DEX or TXA alone is beneficial for postoperative recovery in ARCR patients.
Keywords: postoperative pain, arthroscopy, rotator cuff tear, QoR-15, TXA, DEX
Introduction
Rotator cuff tendon tear is one of the most common diseases afflicting the shoulder, with more than 250,000 RCR operated annually in the United States alone.1 The number of ARCRs being performed continued to rise due to the aging population, elevated patient activity levels, and advances in arthroscopic techniques.2,3 Although arthroscopic shoulder surgery is a minimally invasive operation, the postoperative pain can be severe and intolerant, which results in delayed recovery and discharge.4,5 Perioperative pain management aims to alleviate suffering, achieve early mobilization and rapid discharge, and improve patient satisfaction. Traditional opioid pain management increases the incidence of side effects like over-sedation, respiratory depression, postoperative nausea and vomiting, and impaired recovery quality. Therefore, multimodal analgesia strategies are preferred to achieve adequate pain control while minimizing opioid-related side effects.6
Surgical adjuvants like dexamethasone (DEX) and tranexamic acid (TXA) are used in orthopedic surgeries to reduce blood loss, postoperative inflammation, and pain levels, potentially benefiting this setting.7 Dexamethasone, a potent corticosteroid, is used with other antiemetics to enhance their effect. Its mechanism is not fully understood, but it seems to act synergistically with serotonin receptor antagonists to reduce nausea and provide analgesic benefits.8 TXA, a synthetic lysine derivative, competitively inhibits plasminogen activation, blocking the fibrinolysis pathway to stabilize thrombi and reduce bleeding.9 Recently, intravenous administration of TXA has shown the promise to improve visual clarity during arthroscopic surgery and reduce postoperative pain,10,11 but other studies reported no benefits to relieve postoperative pain after arthroscopic RCR.12,13 The DEX has also been widely used to decrease postoperative pain in various surgical procedures,14–16 and recommended to apply after arthroscopic RCR.17 The combined application of TXA and DEX has been proven effective to relieve the postoperative pain in both total knee and hip arthroplasty.18–20 Although previous studies showed the administration of DEX and TXA postoperatively could alleviate pain, their effect on postoperative recovery quality is still unknown.
Postoperative recovery after surgery and anesthesia is a complex, multidimensional process. Poor recovery quality negatively impacts both patients and medical teams. With advances in surgical techniques, sedation, and pain management, current perioperative care focuses on patients’ subjective postoperative experience rather than morbidity endpoints alone.21 The quality of recovery (QoR) score objectively measures patient-centered health status after surgery and anesthesia. The latest version, QoR-15, is time-efficient with high response and completion rates, validated in various surgical procedures.22
Therefore, we hypothesized that combined postoperative administration of TXA and DEX could improve recovery quality in ARCR patients. The primary outcome was to evaluate the effectiveness of postoperative TXA and DEX on recovery quality after ARCR during the first 24 hours using the QoR-15 questionnaire. We aim to relieve the acute postoperative pain and promote fast recovery and rapid discharge for ARCR patients.
Materials and Methods
Ethics Approval and Registration
This study was approved by the Institutional Review Board of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China, with the approval number, 2023–141-(1), dated 20 November 2023. This trial was registered with the Chinese Clinical Trial Registry with approval number, ChiCTR2300078507, dated 11 December 2023. The study was a prospective, double-blinded, randomized control trial. All patients (or their proxies/legal guardians) provided written informed consent to participate in the study and for their data to be published. This trial conforms to the provisions of the Declaration of Helsinki (as revised in Brazil in 2013). We adhered to the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement.23 The full trial protocol could be obtained from the corresponding authors upon request.
Inclusion and Exclusion Criteria
The inclusion criteria were, (1) age 40 to 80 years old; (2) body mass index (BMI) < 35 kg/m2; (3) American Society of Anesthesiologists (ASA) physical status I to II; (4) unilateral RCR with small to medium tear size; (5) rotator cuff tears repaired with suture anchors.
The exclusion criteria were, (1) coagulation defect or recent use of anti-coagulation or anti-platelet drugs; (2) psychological or neurological diseases, or long-term use of sedative, analgesic, and psychotropic drugs; (3) opioid or corticosteroids use two weeks before surgery; (4) epidural or articular corticosteroids injection three months before surgery; (5) allergy or contraindications to TXA or DEX; (6) missed postoperative blood test.
Randomization and Blinding
Patients who provided informed consent and met eligibility criteria were randomized (1:1:1) in blocks of 6 to control, TXA, and TXA+DEX groups. An uninvolved individual prepared the computer-generated randomization sequence and sequentially numbered and sealed opaque envelopes to maintain blinding and allocation concealment. Eligible participants were randomized on the day of surgery using the next numbered envelope in sequence. The randomization list was kept secure, inaccessible to investigators or study personnel. The study medication [TXA (ReYoung Pharmaceutical Co., Ltd, Shangdong, China), 1g, and DEX (HeNan RunHong Pharmaceutical Co. Ltd, Henan, China), 5mg] was intravenously administrated and assigned based on randomization by an anesthetic nurse not involved in the rest of the study. The drug was diluted to 200 mL with normal saline before administration. Placebo of normal saline (control group), 1g TXA (TXA group), or 1g TXA + 5mg DEX (TXA+DEX group) was administered at a maintenance dose of 100 mL hourly, starting 2 hours after surgery.
Standard General Anesthesia, Surgical Procedure, and Postoperative Care
None of the subjects took preemptive analgesics before surgery. After establishing intravenous access and applying standard monitors (electrocardiogram, noninvasive blood pressure cuff, continuous oxygen saturation), the participants were sedated with intravenous midazolam (1–2 mg). The lateral neck and supraclavicular fossa on the same side as the surgical site were cleansed with an isopropyl alcohol/chlorhexidine gluconate solution. An ultrasound-guided low-volume ISB (0.5% ropivacaine, 10 mL) was performed under sterile conditions by a staff regional anesthesiologist or a supervised regional anesthesia fellow using a 13–6 MHz 38 mm linear probe (MTurbo®; SonoSite Inc., Bothell, WA, USA) at the C5 and C6 nerve root level via a posterior approach and a 22-gauge insulated 50 mm regional needle. Once the needle tip was correctly positioned and aspiration was negative, the local anesthetic was injected. General anesthesia was induced using a standardized technique with sufentanil 0.2μg/kg and propofol 1–3mg/kg. Tracheal intubation was facilitated with 0.6mg/kg rocuronium. Anesthesia was maintained with sevoflurane at an end-tidal concentration of 1.4–2 vol%. During surgery, 5μg aliquots of sufentanil were administered when blood pressure or heart rate increased more than 20% from preoperative baseline values. Standard antiemetic prophylaxis with 4 mg ondansetron was intravenously administered before emergence.
All patients who underwent ARCR were performed by one of the three senior orthopedic surgeons (I, II, III). Standard posterior and anterior portals were created to inspect the glenohumeral joint. A lateral portal was established for acromioplasty, bursectomy, and rotator cuff repair. The average surgery duration for all patients was 55.4 ± 11.6 minutes. One or two suture anchors was applied during surgery. Single-row or double-row rotator cuff repair technique was utilized for all patients. Postoperatively, participants received 1 g oral paracetamol, 50 mg intravenous flurbiprofen axetil every 8 hours, and 100 mg intravenous tramadol every 12 hours. The nurses checked all the postoperative medications had been applied and followed by all patients. The patients were hospitalized for all the medications. The medications were administrated for 24 hours after surgery for all patients.
Outcome Measurements
All patients completed the QoR-15 questionnaire twice, on the morning of the operation in the preoperative holding area and 24 hours after surgery. The primary outcome was the quality of recovery 24 hours after surgery, assessed using the QoR-15 questionnaire. Δ Total QoR-15 score was calculated as preoperative QoR-15 score minus postoperative QoR-15 score. The QoR-15 is a multidimensional patient-reported outcome measure validated in the perioperative setting through extensive psychometric evaluation and systematic review.24,25 This questionnaire evaluates overall recovery by assessing five domains of health status: pain, physical comfort, physical independence, psychological support, and emotional state.26,27 It consists of 15 statements covering these domains, with patients indicating their level of agreement on a scale of 0–10. The total QoR-15 score ranges from 0 to 150, with higher scores indicating better recovery quality. Each question was scored from 0 (none of the time) to 10 (all the time), except for questions 11–15, which were inversely scored, from 10 (none of the time) to 0 (all the time).27 We applied Chinese version of QoR-15 questionnaire in this study which has been previously validated for assessing the quality of postoperative recovery.28
Secondary outcomes included mean visual analogue scale (VAS) scores every four hours within 24 hours postoperatively, and blood test results including C-reactive protein (CRP), D-Dimer, hemoglobin (Hb), prothrombin time (PT), activated partial thromboplastin time (APTT), international normalized ratio (INR), fibrinogen, platelet (PLT) the day after surgery. ASES scores were obtained from all patients via telephone 3 months post-surgery. Δ ASES score was calculated as ASES score at 3 months postoperatively minus ASES score preoperatively.
The potential pain-relieving effect of TXA and DEX was due to reduced blood loss and postoperative inflammation. The preoperative and postoperative blood tests were utilized to validate the safety and potential effectiveness of TXA and DEX on fibrinolysis, inflammation, coagulation, and blood loss. The preoperative blood tests were applied to ensure the comparability among groups. The parameters of blood test were selected based on previous published literatures.7,18,19 Since arthroscopic surgeries were minimally invasive without large amount of blood loss and tissue damage, we did not expect to find significant differences among groups for blood test results after the application of TXA or TXA+DEX. Since it was impossible to distinguish the shoulder function right after surgery, we chose to evaluate the clinical outcome at 3 months after ARCR, which was the important prognostic factor for full shoulder functional recovery for ARCR.29,30
Sample Size and Statistical Analysis
The QoR-15 score was the primary outcome. In our preliminary study conducted with nine patients (three in each group), the mean QoR-15 score was 102 ± 20, 110 ± 19, and 120 ± 16 for the control, TXA, and TXA+DEX groups, respectively. Sample size calculation was performed with PASS V.11.0 (PASS, NCSS, USA) for Windows. One-way analysis of variance (ANOVA) was selected and grouped into three groups. Group allocation ratios were equal. Hypothesized means were 102, 110, and 120, and SD were 20, 19, and 16, respectively. At a power of 0.80 and an alpha error of 0.05, the required sample size for each group was calculated to be 25. Considering the dropouts and incomplete follow-up, 32 patients per group and a total of 96 patients were suggested for this study.
The data were analyzed using GraphPad Prism version 9.5.0 (GraphPad Software, San Diego, CA, USA). Normality was checked for all data using Kolmogorov–Smirnov test. Quantitative data with normal distribution were reported as mean ± standard deviation. Quantitative data with non-normal distribution were presented as median (25 percentile, 75 percentile). ANOVA was applied to compare differences among groups with normally distributed data. Kruskal–Wallis test was utilized for nonparametric data comparison among groups, and Dunn’s test was applied to compare the mean rank of each group with the mean rank of every other group. Qualitative variables were assessed for significance using the chi-squared test. The statistical significance was set as p < 0.05.
Results
Of the 132 patients assessed for eligibility, 32 failed to meet the inclusion criteria and 4 declined to participate. These patients were excluded from the study. Patients who underwent ARCR from December 12th 2023 to March 15th 2024 at our institution were enrolled in this study and followed up to June 18th 2024. Ninety-six patients were randomized into three groups, 32 patients in the control group, 32 patients randomized to the TXA group, and 32 patients in the TXA+DEX group (Figure 1). No one was lost to follow-up in these three groups at the day after surgery and at 3 months after surgery for ASES assessment. For placebo, TXA, and TXA+DEX groups, the mean ages of enrolled patients were 61.08 ± 7.90, 60.94 ± 6.82, and 60.89 ± 8.45, respectively. 11, 10, 10 male patients were included in each group. The median symptom duration was 4 months for patients in each group. The ratios of high and medium demand to low demand types of work were 6/26, 10/22, 7/25 for placebo, TXA, and TXA+DEX groups. The mean BMI were 23.96 ± 2.70, 23.64 ± 2.51, and 24.37 ± 2.91 for each group. 10, 8, and 9 patients had hypertension in placebo, TXA, and TXA+DEX groups. The ratios of single-row to double-row technique were 15/17, 10/22, and 12/20 for placebo, TXA, and TXA+DEX groups. The ratios of surgeon I to II and III who performed the surgeries were 21/11, 20/12, and 22/10 in each group. The average preoperative ASES scores were 53.80 ± 22.13, 47.55 ± 19.62, and 55.00 ± 19.53 for placebo, TXA, and TXA+DEX groups, respectively. There were no significant differences among groups with regard to mean age (p = 0.994), sex (p = 0.954), symptom duration (p = 0.786), type of work (p = 0.476), BMI (p = 0.562), hypertension (p = 0.857), surgical method of RCR (p = 0.437), surgeon (p = 0.871), and preoperative ASES scores (p = 0.300) (Table 1). No significant differences were shown for the preoperative total QoR-15 scores among groups (control group, 137.5 ± 7.3; TXA group, 135.5 ± 9.1; TXA+DEX group, 136.4 ± 8.6, p = 0.606). There were no differences among groups with the five dimensions of preoperative QoR-15 scores (Table 2). No significant differences were found in preoperative blood test results (Table 3).
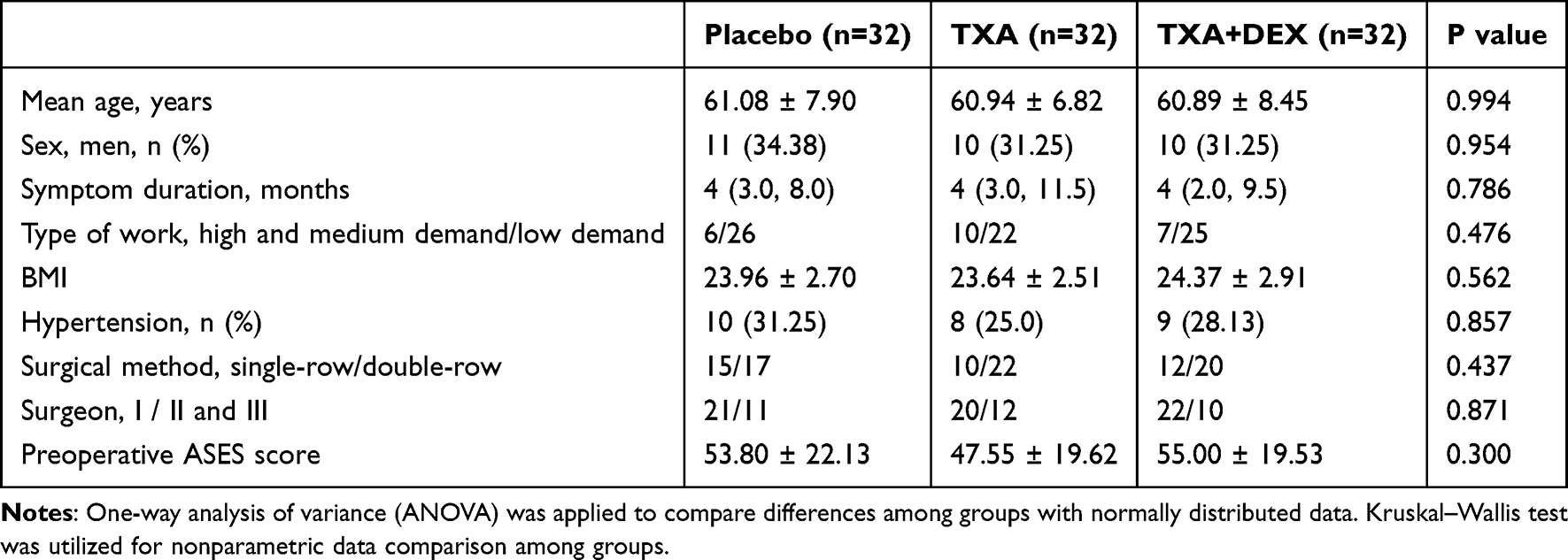 |
Table 1 Patient Demographic Characteristics |
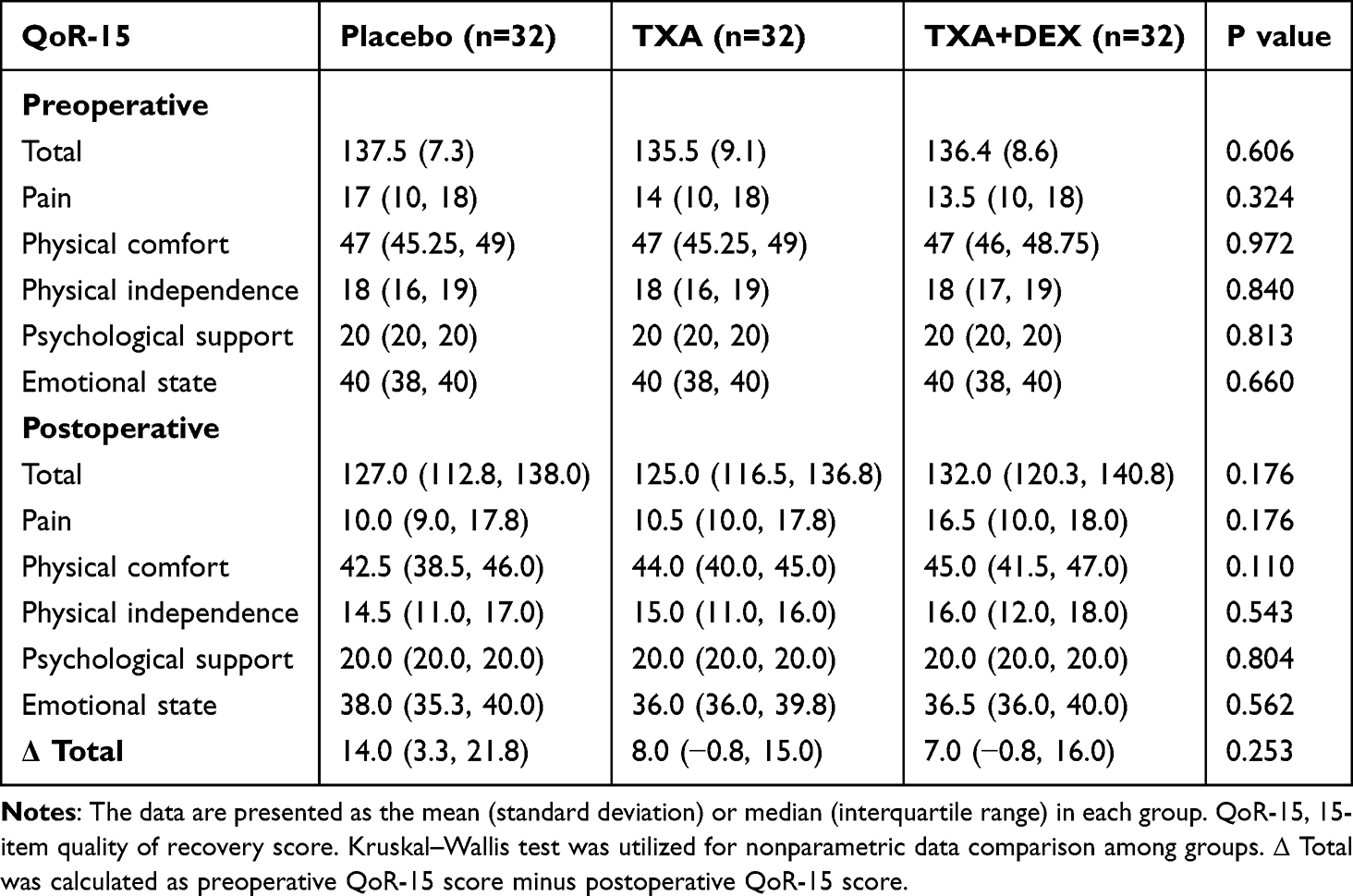 |
Table 2 Total and Dimensional QoR-15 Scores of the Participants |
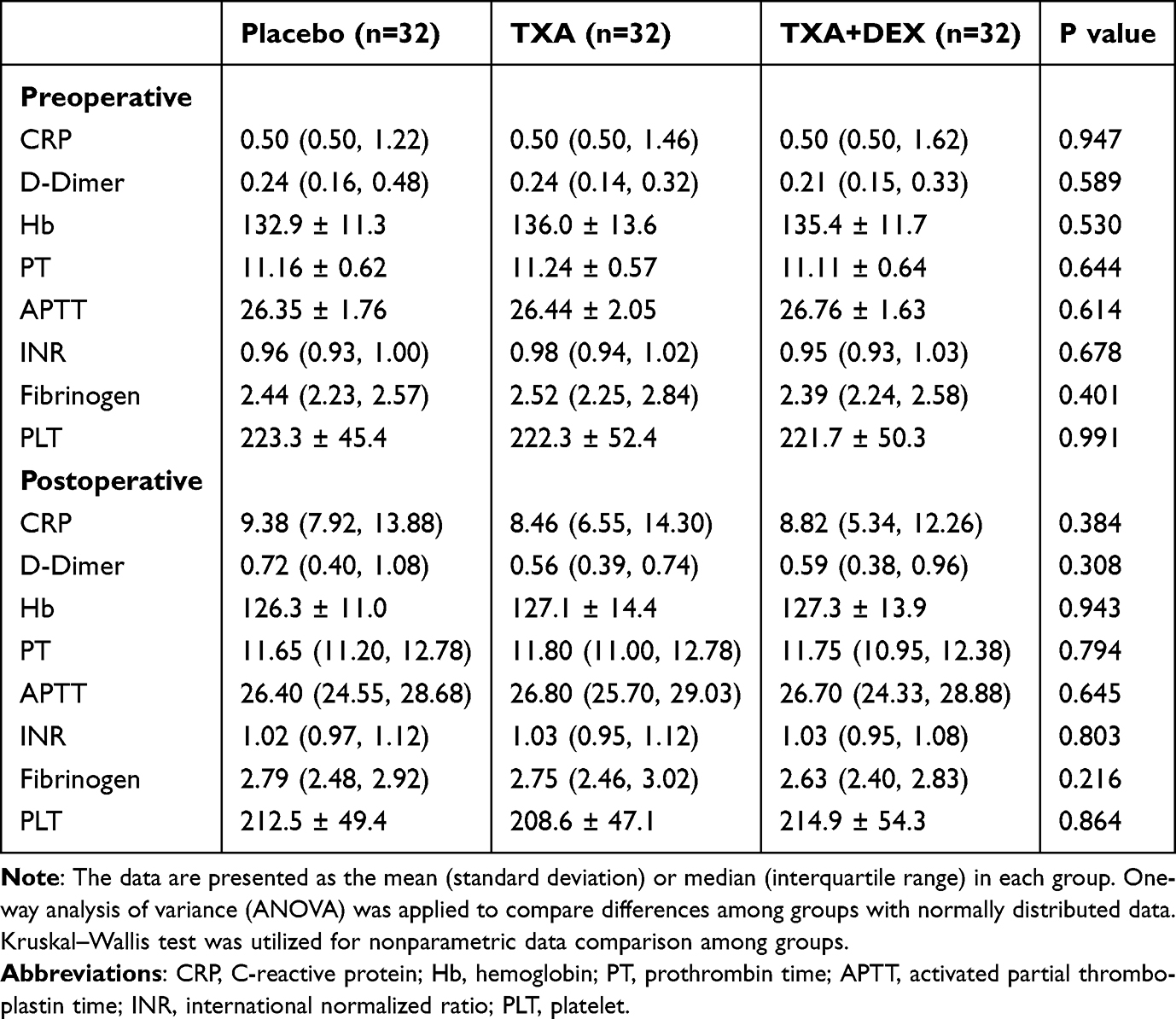 |
Table 3 Comparison of Blood Tests Among Three Groups |
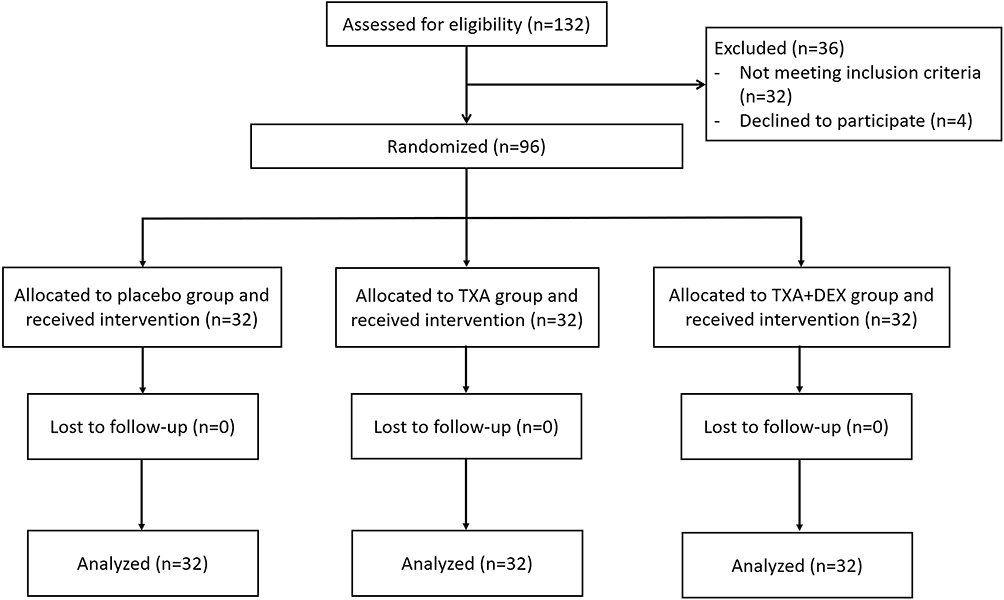 |
Figure 1 Flow diagram of patient enrollment. |
The Quality of Recovery-15
For the primary outcome, the total QoR-15 scores were 127.0 (112.8, 138.0), 125.0 (116.5, 136.8), and 132.0 (120.3, 140.8) for placebo, TXA, and TXA+DEX groups. The TXA+DEX group had the highest score but without statistical significance (p = 0.176). The five dimensions of postoperative QoR-15 scores were also analyzed. For the dimension of postoperative pain, the scores were 10.0 (9.0, 17.8), 10.5 (10.0, 17.8), and 16.5 (10.0, 18.0) for placebo, TXA, and TXA+DEX groups. The scores of physical comforts were 42.5 (38.5, 46.0), 44.0 (40.0, 45.0), and 45.0 (41.5, 47.0) for each group. For physical independence, the scores were 14.5 (11.0, 17.0), 15.0 (11.0, 16.0), and 16.0 (12.0, 18.0) in each group. The median score of psychological support was 20.0 for all three groups. The scores of emotional states were 38.0 (35.3, 40.0), 36.0 (36.0, 39.8), and 36.5 (36.0, 40.0) for placebo, TXA, and TXA+DEX groups. There were also no differences among groups with the five dimensions of postoperative QoR-15 scores. Δ Total QoR-15 scores were 14.0 (3.3, 21.8), 8.0 (−0.8, 15.0), and 7.0 (−0.8, 16.0) for placebo, TXA, and TXA+DEX groups. No significant differences were found among groups (p = 0.253) (Table 2).
Visual Analogue Scale
The VAS values at postoperative 0–4 hours were 0.0 (0.0, 1.0), 0.0 (0.0, 1.3), and 0.0 (0.0, 1.0) for placebo, TXA, and TXA+DEX groups, respectively, and no significant differences were found among groups (placebo vs TXA, P = 0.340; placebo vs TXA+DEX, p = 0.173; TXA vs TXA+DEX, p=0.788). For placebo, TXA, and TXA+DEX groups at postoperative 5–8 hours, the VAS values were 3.5 (2.0, 4.0), 3.0 (2.0, 5.0), and 2.0 (1.0, 3.0). No significance was found between placebo and TXA groups at postoperative 5–8 hours, but the VAS value of TXA+DEX group was significantly higher than the placebo and TXA groups (placebo vs TXA, p = 0.464; placebo vs TXA+DEX, p = 0.014; TXA vs TXA+DEX, p = 0.002). The VAS values at postoperative 9–12 hours were 5.0 (4.0, 7.0), 5.5 (4.0, 8.0), and 3.5 (2.0, 5.0) for placebo, TXA, and TXA+DEX groups. There was no significance between placebo and TXA groups at postoperative 9–12 hours, but the VAS value of TXA+DEX group was significantly higher than the placebo and TXA groups (placebo vs TXA, p = 0.268; placebo vs TXA+DEX, p = 0.008; TXA vs TXA+DEX, p < 0.001). For placebo, TXA, and TXA+DEX groups at postoperative 13–16 hours, the VAS values were 4.5 (3.0, 6.0), 5.0 (3.0, 6.0), and 3.0 (2.0, 5.0). No significance was found between placebo and TXA groups at postoperative 13–16 hours, but the VAS value of TXA+DEX group was significantly higher than the placebo and TXA groups (placebo vs TXA, p = 0.793; placebo vs TXA+DEX, p = 0.035; TXA vs TXA+DEX, p = 0.013). The VAS values at postoperative 17–20 hours were 3.0 (1.8, 5.0), 4.0 (2.0, 5.0), and 3.0 (2.0, 5.0) for placebo, TXA, and TXA+DEX groups, and no significant differences were demonstrated among groups (placebo vs TXA, p = 0.207 placebo vs TXA+DEX, p = 0.941; TXA vs TXA+DEX, p = 0.235). The VAS values at postoperative 21–24 hours were 2.0 (2.0, 4.0), 3.0 (2.0, 4.0), and 2.0 (1.0, 4.0) for placebo, TXA, and TXA+DEX groups, and significant difference was found between TXA and TXA+DEX groups (placebo vs TXA, p = 0.334 placebo vs TXA+DEX, p = 0.259; TXA vs TXA+DEX, p = 0.043). In summary, there were significant differences among groups with regard to mean VAS values at postoperative 5–8 hours (placebo vs TXA+DEX, p = 0.014; TXA vs TXA+DEX, p = 0.002), 9–12 hours (placebo vs TXA+DEX, p = 0.008; TXA vs TXA+DEX, p < 0.001), 13–16 hours (placebo vs TXA+DEX, p = 0.035; TXA vs TXA+DEX, p = 0.013), 21–24 hours (TXA vs TXA+DEX, p = 0.043) (Figure 2).
 |
Figure 2 Mean VAS value every four hours within 24 hours postoperatively. Data were expressed as median (horizontal bar), interquartile range (box), the maximum and minimum values (upper and lower edges) and the outliers (circles). * P<0.05. **P<0.01. ***P<0.001. Kruskal–Wallis test was utilized for data comparison among groups, and Dunn’s test was applied to compare the mean rank of each group with the mean rank of every other group. Abbreviation, PO, postoperative. |
Perioperative Data
No differences were found for postoperative blood test results (Table 3). This indicated the safety of TXA and DEX utilized postoperatively. The application of TXA and DEX did not significantly alter the levels of fibrinolysis, inflammation, coagulation, and blood loss. ASES scores at 3 months after surgery demonstrated no significant differences among the three groups (placebo group, 76.33 ± 10.74; TXA group, 71.29 ± 15.42; TXA+DEX group, 72.66 ± 12.67, p = 0.243). There were also no significant differences among the groups for Δ ASES (placebo group, 21.71 ± 19.76; TXA group, 22.58 ± 20.24; TXA+DEX group, 19.60 ± 19.12, p = 0.805) (Table 4).
 |
Table 4 Comparison of ASES Score at 3 Months After Surgery |
Discussion
In this prospective, double-blinded, randomized control trial, we investigated the effect of combined intravenous (iv) administration of TXA and DEX on the quality of recovery during the first 24 hours after ARCR. The application of iv. TXA and DEX resulted with no statistical significance (p = 0.176). TXA and DEX could relieve acute postoperative pain between 5 and 16 hours, while TXA demonstrated no quantifiable benefits for promoting quality of recovery and pain relief. In this study, we used QoR-15 as the primary outcome, which focused on the patient’s subjective well-being and satisfaction after surgery, encompassing physical, mental, and emotional health.26 Higher QoR-15 scores indicate a better quality of recovery.31 The preoperative measurements of QoR-15 score, blood tests, and ASES scores were to ensure the comparability among groups and also to make comparison with the postoperative results. Our studies revealed that the acute postoperative pain and quality of recovery status were even worse than the patients’ preoperative levels. This might be due to the intense pain and temporary loss of shoulder ROM caused by surgical operation. Thus, we calculated the Δ total QoR-15 score as preoperative score minus postoperative score. Lower Δ total QoR-15 score indicates a better quality of recovery during the first 24 hours postoperatively.
As for the application of TXA in arthroscopy, several systematic reviews and meta-analyses have summarized that the administration of TXA could improve visual clarity during surgery, decrease operation time, and reduce postoperative pain.9,32–35 However, these studies included arthroscopic knee and shoulder surgeries simultaneously, and most of the enrolled experiments focused on knee surgeries. DEX is also investigated for pain management in arthroscopic RCR. Several studies showed that the combination of DEX with interscalene blocks could prolong the analgesic duration after shoulder arthroscopy.36–39
To our knowledge, this study is the first to investigate the combined application of TXA and DEX in arthroscopic shoulder surgery. Previous study showed mixed outcomes of TXA on arthroscopic shoulder RCR. One randomized control trial (RCT) and one retrospective study reported favorable outcomes of TXA on postoperative pain after arthroscopic RCR.10,40 However, two other RCT studies demonstrated no measurable improvement in postoperative pain scores after arthroscopic RCR.12,13 The combined administration of TXA and DEX was mostly employed in total knee or hip arthroplasty with favorable outcomes. Previous studies showed that the combined application could relieve postoperative pain, reduce blood loss, and promote fast recovery.7,41,42 In our study, we observed significant postoperative pain relief in the TXA+DEX group between 5 and 16 hours after ARCR surgery compared to all other groups. No differences in VAS scores were noted between the control and TXA groups at any four-hour interval within the first 24 hours post-surgery. This suggested that while TXA alone did not alleviate postoperative pain in ARCR patients, the combination of TXA and DEX enhanced pain relief. Since the intravenous administration of DEX postoperatively has been proven to be effective in prolonging the analgesic duration of interscalene brachial plexus block and recommended for arthroscopic rotator cuff repair pain management,17 we did not repeatedly evaluate the efficacy of DEX alone in improving postoperative recovery and pain relief. Based on our findings, we do not recommend the application of TXA alone or DEX in conjunction with TXA for ARCR patients due to limited benefits for postoperative recovery. The QoR-15 questionnaire, which assessed postoperative pain levels, focused on moderate and severe pain within 24 hours after surgery, rather than at multiple time points as in our study. This method provided an average pain level over the 24-hour period, which revealed no statistically significant differences in the pain domain of the QoR-15 scores among the three groups. Additionally, there were no significant differences in the overall QoR-15 scores, which encompassed physical comfort, physical independence, psychological support, and emotional state.
No side effects of TXA and DEX administration were observed during the three-month postoperative follow-up. However, the application of TXA and DEX is not without risks, particularly for patients with underlying health conditions. Potential side effects of these medications can outweigh their benefits, making alternative management strategies necessary to mitigate risks and ensure patient safety.
There are several limitations of this study. First, we evaluated the QoR-15 score at 24 hours postoperatively, and more timepoints, like at 48 hours or more postoperatively, should be considered in future studies to determine the effectiveness of TXA and DEX. Second, the patient samples are regional since most patients were from areas located in or close to Shanghai, China. A larger and multicenter study should be carried out to validate the effectiveness of TXA and DEX. Third, the appropriate dose and timing of the administration of TXA and DEX should be investigated.
Conclusion
The application of TXA alone or combined administration of TXA and DEX could not significantly improve the quality of recovery during the first 24 hours in ARCR patients. The combination of TXA and DEX presented better levels of postoperative pain between 5 and 16 hours than the control and TXA alone. Further large-scale and multi-center investigation is required to determine if the combined application of TXA and DEX or TXA alone is beneficial for postoperative recovery in ARCR patients.
Abbreviations
ARCR, arthroscopic rotator cuff repair; DEX, dexamethasone; TXA, tranexamic acid; QoR-15, Quality of Recovery-15; VAS, visual analog scale; ASES, American Shoulder and Elbow Surgeons; PONV, postoperative nausea and vomiting; IRB, Institutional Review Board; CONSORT, Consolidated Standards of Reporting Trials; BMI, body mass index; ASA, American Society of Anesthesiologists; CRP, C-reactive protein; Hb, hemoglobin; PT, prothrombin time; APTT, activated partial thromboplastin time; INR, international normalized ratio; PLT, platelet; ANOVA, one-way analysis of variance; RCT, randomized control trial.
Data Sharing Statement and Data Availability
The authors intend to share individual deidentified participant data, including patient characteristics, QoR-15 questionnaire score, VAS square, blood test results, and ASES scores. The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was reviewed and approved by the Institutional Review Board (IRB) of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine with the approval number, 2023-141-(1), dated November 20th 2023. This trial was registered with the Chinese Clinical Trial Registry with approval number, ChiCTR2300078507, dated December 11th 2023. This trial conforms to the provisions of the Declaration of Helsinki (as revised in Brazil in 2013).
Consent for Publication
All patients (or their proxies/legal guardians) provided written informed consent to participate in the study and for their data to be published. Patients who cannot read or write had their legal guardians provide informed consent.
Acknowledgments
The authors want to thank Yilin Liu and Qiuhua Chen for the help during the experiment. This work was supported by the Clinical Project of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (No. ynts202002).
Funding
This work was supported by the Clinical Project of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (No. ynts202002), and Key Research and Development Plan of the Ministry of Science and Technology (SQ2023YFC240014605).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gulotta LV, Kovacevic D, Ehteshami JR, Dagher E, Packer JD, Rodeo SA. Application of bone marrow-derived mesenchymal stem cells in a rotator cuff repair model. Am J Sports Med. 2009;37(11):2126–2133. doi:10.1177/0363546509339582
2. Colvin AC, Egorova N, Harrison AK, Moskowitz A, Flatow EL. National trends in rotator cuff repair. J Joint Bone Surg. 2012;94(3).
3. Ensor KL, Kwon YW, DiBeneditto MR, Zuckerman JD, Rokito AS. The rising incidence of rotator cuff repairs. J Shoulder Elbow Surg. 2013;22(12):1628–1632. doi:10.1016/j.jse.2013.01.006
4. Bang SR, Yu SK, Kim TH. Can gabapentin help reduce postoperative pain in arthroscopic rotator cuff repair? A prospective, randomized, double-blind study. Arthroscopy. 2010;26(9):S106–S11. doi:10.1016/j.arthro.2009.11.010
5. Oh JH, Kim WS, Kim JY, Gong HS, K-y R. Continuous intralesional infusion combined with interscalene block was effective for postoperative analgesia after arthroscopic shoulder surgery. J Shoulder Elbow Surg. 2007;16(3):295–299. doi:10.1016/j.jse.2006.04.015
6. Uquillas CA, Capogna BM, Rossy WH, Mahure SA, Rokito AS. Postoperative pain control after arthroscopic rotator cuff repair. J Shoulder Elbow Surg. 2016;25(7):1204–1213. doi:10.1016/j.jse.2016.01.026
7. Jiang W, Wang X, Xu H, et al. Tourniquets can further reduce perioperative blood loss in patients on dexamethasone and tranexamic acid during cemented total knee arthritis: a single-center, double-blind, randomized controlled trial. J Orthop Traumatol. 2023;24(1):17. doi:10.1186/s10195-023-00698-3
8. Huang L, Li P, Zhang L, Kang G, Zhou H, Zhao Z. Analgesic comparison between perineural and intravenous dexamethasone for shoulder arthroscopy: a meta-analysis of randomized controlled trials. J Orthopaedic Surg Res. 2022;17(1):103. doi:10.1186/s13018-022-02952-6
9. Goldstein K, Jones C, Kay J, Shin J, de Sa D. Tranexamic acid administration in arthroscopic surgery is a safe adjunct to decrease postoperative pain and swelling: a systematic review and meta-analysis. Arthroscopy. 2022;38(4):1366–77.e9. doi:10.1016/j.arthro.2021.10.001
10. Liu Y, Hong C, Hsu K, et al. Intravenous administration of tranexamic acid significantly improved clarity of the visual field in arthroscopic shoulder surgery. a prospective, double-blind, and randomized controlled trial. Arthroscopy. 2020;36(3):640–647. doi:10.1016/j.arthro.2019.10.020
11. Bildik C, Pehlivanoglu T. Arthroscopic rotator cuff repair performed with intra-articular tranexamic acid: could it provide improved visual clarity and less postoperative pain? A prospective, double-blind, randomized study of 63 patients. J Shoulder Elbow Surg. 2023;32(2):223–231. doi:10.1016/j.jse.2022.10.007
12. Mackenzie SP, Spasojevic M, Smith M, et al. The effect of single-dose, preoperative intravenous tranexamic acid on early postoperative pain scores after rotator cuff repair: a double-blind, randomized controlled trial. J Shoulder Elbow Surg. 2022;31(7):1399–1408. doi:10.1016/j.jse.2022.02.023
13. Nicholson TA, Kirsch JM, Churchill R, Lazarus MD, Abboud JA, Namdari S. The effect of tranexamic acid for visualization on pump pressure and visualization during arthroscopic rotator cuff repair: an anonymized, randomized controlled trial. J Shoulder Elbow Surg. 2022;31(11):2211–2216. doi:10.1016/j.jse.2022.06.027
14. Gasbjerg KS, Hägi-Pedersen D, Lunn TH, et al. Effect of dexamethasone as an analgesic adjuvant to multimodal pain treatment after total knee arthroplasty: randomised clinical trial. BMJ. 2022;376:e067325. doi:10.1136/bmj-2021-067325
15. Vieth MP, Deas DE, Archontia Palaiologou A, Diogenes A, Mader MJ, Mealey BL. Effect of intravenous dexamethasone on postoperative pain and swelling following periodontal flap surgery: a randomized controlled trial of patient-centered outcomes. J Periodontol. 2022;93(2):239–247. doi:10.1002/JPER.21-0153
16. Steinthorsdottir KJ, Awada HN, Abildstrøm H, Kroman N, Kehlet H, Kvanner Aasvang E. Dexamethasone dose and early postoperative recovery after mastectomy: a double-blind, randomized trial. Anesthesiology. 2020;132(4):678–691. doi:10.1097/ALN.0000000000003112
17. Toma O, Persoons B, Pogatzki-Zahn E, Van de Velde M, Joshi GP, The PWGc. PROSPECT guideline for rotator cuff repair surgery: systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2019;74(10):1320–1331. doi:10.1111/anae.14796
18. An Y, Xu M, An Y, Liu H, Zheng M, Jiang D. Combined application of dexamethasone and tranexamic acid to reduce the postoperative inflammatory response and improve functional outcomes in total hip arthroplasty. Orthop Surg. 2020;12(2):582–588. doi:10.1111/os.12664
19. Xu H, Xie J, Yang J, Huang Z, Wang D, Pei F. Synergistic effect of a prolonged combination course of tranexamic acid and dexamethasone involving high initial doses in total knee arthroplasty: a randomized controlled trial. J Knee Surg. 2021;36(05):515–523. doi:10.1055/s-0041-1739197
20. Tan TK, Gopal Subramaniam A, Hau R. Effects of combined dexamethasone and tranexamic acid in lower limb total arthroplasty: a systematic review and meta-analysis of randomized clinical trials. Eur J of Orthop Surg and Traumatol. 2023;33(8):3327–3335. doi:10.1007/s00590-023-03612-z
21. Myles PS, Shulman MA, Reilly J, Kasza J, Romero L. Measurement of quality of recovery after surgery using the 15-item quality of recovery scale: a systematic review and meta-analysis. Br J Anaesth. 2022;128(6):1029–1039. doi:10.1016/j.bja.2022.03.009
22. Campfort M, Cayla C, Lasocki S, Rineau E, Léger M. Early quality of recovery according to QoR-15 score is associated with one-month postoperative complications after elective surgery. J Clin Anesth. 2022;78:110638. doi:10.1016/j.jclinane.2021.110638
23. Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. doi:10.1136/bmj.c332
24. Finnerty DT, McMahon A, McNamara JR, Hartigan SD, Griffin M, Buggy DJ. Comparing erector spinae plane block with serratus anterior plane block for minimally invasive thoracic surgery: a randomised clinical trial. Br J Anaesth. 2020;125(5):802–810. doi:10.1016/j.bja.2020.06.020
25. Moorthy A, Ní Eochagáin A, Dempsey E, et al. Postoperative recovery with continuous erector spinae plane block or video-assisted paravertebral block after minimally invasive thoracic surgery: a prospective, randomised controlled trial. Br J Anaesth. 2023;130(1):e137–e47. doi:10.1016/j.bja.2022.07.051
26. Choi JY, Lee HS, Kim JY, et al. Comparison of remimazolam-based and propofol-based total intravenous anesthesia on postoperative quality of recovery: a randomized non-inferiority trial. J Clin Anesth. 2022;82:110955. doi:10.1016/j.jclinane.2022.110955
27. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
28. Bu X-S, Zhang J, Zuo Y-X. Validation of the Chinese version of the quality of recovery-15 score and its comparison with the post-operative quality recovery scale. Patient - Patient-Centered Outcomes Res. 2016;9(3):251–259. doi:10.1007/s40271-015-0148-6
29. Nakamura Y, Gotoh M, Mitsui Y, et al. Prognostic factors affecting clinical outcomes after arthroscopic rotator cuff repair: importance of functional recovery by 3 months after surgery. J Orthopaedic Surg Res. 2018;13(1):310. doi:10.1186/s13018-018-1014-8
30. Ito Y, Ishida T, Matsumoto H, et al. Passive shoulder abduction range of motion at 3 months postoperatively is the most important prognostic factor for achieving full recovery of range of motion at 6 months after arthroscopic rotator cuff repair. JSES Int. 2024;8(4):806–814. doi:10.1016/j.jseint.2024.03.010
31. Hao C, Xu H, Du J, et al. Impact of opioid-free anesthesia on postoperative quality of recovery in patients after laparoscopic cholecystectomy-a randomized controlled trial. Drug Des Devel Ther. 2023;17:3539–3547. doi:10.2147/DDDT.S439674
32. Belk JW, McCarty EC, Houck DA, Dragoo JL, Savoie FH, Thon SG. Tranexamic acid use in knee and shoulder arthroscopy leads to improved outcomes and fewer hemarthrosis-related complications: a systematic review of level i and ii studies. Arthroscopy. 2021;37(4):1323–1333. doi:10.1016/j.arthro.2020.11.051
33. Han C, Liu M, Lian X, et al. Tranexamic acid use in arthroscopic rotator cuff repair is an effective and safe adjunct to improve visualization: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2023;32(11):2389–2399. doi:10.1016/j.jse.2023.06.013
34. Hurley ET, Rodriguez K, Karavan MP, et al. Tranexamic acid for rotator cuff repair, a systematic review and meta-analysis of randomized controlled trials. Am J Sports Med. 2024;2024:03635465231216336.
35. Tan TK, Tan P, Wang K, Hau R. Effect of tranexamic acid on shoulder surgery: an updated meta-analysis of randomized studies. J Shoulder Elbow Surg. 2024;33(2):e97–e108. doi:10.1016/j.jse.2023.09.024
36. Woo JH, Lee HJ, Oh H-W, Lee JW, Baik HJ, Kim YJ. Perineural dexamethasone reduces rebound pain after ropivacaine single injection interscalene block for arthroscopic shoulder surgery: a randomized controlled trial. Reg Anesth Pain Med. 2021;46(11):965. doi:10.1136/rapm-2021-102795
37. Kahn RL, Cheng J, Gadulov Y, Fields KG, YaDeau JT, Gulotta LV. Perineural low-dose dexamethasone prolongs interscalene block analgesia with bupivacaine compared with systemic dexamethasone: a randomized trial. Reg Anesth Pain Med. 2018;43(6):572. doi:10.1097/AAP.0000000000000817
38. Holland D, Amadeo RJJ, Wolfe S, et al. Effect of dexamethasone dose and route on the duration of interscalene brachial plexus block for outpatient arthroscopic shoulder surgery: a randomized controlled trial. Can J Anaesth. 2018;65(1):34–45. doi:10.1007/s12630-017-0989-7
39. Chalifoux F, Colin F, St-Pierre P, Godin N, Brulotte V. Low dose intravenous dexamethasone (4 mg and 10 mg) significantly prolongs the analgesic duration of single-shot interscalene block after arthroscopic shoulder surgery: a prospective randomized placebo-controlled study. Can J Anaesth. 2017;64(3):280–289. doi:10.1007/s12630-016-0796-6
40. Zhu R, Jiang H, Xu W, Shen L, Jin G. Impact of intra-articular injection with tranexamic acid on total blood loss and postoperative pain after arthroscopic rotator cuff repair surgery. Front Surg. 2023;10:1052039.
41. Li F, Huang X, Liu W, Huang W, Wang C, Yin D. Application of dexamethasone combined with tranexamic acid in perioperative period of total hip arthroplasty. Medicine. 2022;101(42):e31223.
42. Yu Y, Lin H, Wu Z, Xu P, Lei Z. Perioperative combined administration of tranexamic acid and dexamethasone in total knee arthroplasty—benefit versus harm? Medicine. 2019;98(34):e15852. doi:10.1097/MD.0000000000015852
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.