")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
The Effects of the Multi-Hospital Global Budget Payment on Medical Expenditure and Service Volume: The Evidence from Dangyang County, China
Received 28 March 2024
Accepted for publication 23 July 2024
Published 30 July 2024 Volume 2024:17 Pages 1875—1887
DOI https://doi.org/10.2147/RMHP.S471212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kyriakos Souliotis
Kunhe Lin,1 Li Xiang1,2
1Department of Health Management, School of Medicine and Health Management, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2HUST Base of National Institute of Healthcare Security, Wuhan, People’s Republic of China
Correspondence: Li Xiang, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Email [email protected]
Background: Global budget payment is currently the prevailing payment strategy internationally. In China, the concept of multi-hospital global budget payment has been proposed with the aims of achieving cost control effects while also encouraging hospital collaboration and optimising allocation of healthcare resources. This study seeks to analyse the impact of multi-hospital global budget payment in China on healthcare expenditure and service volume.
Materials and Methods: A retrospective comparative study was carried out in Dangyang County, China. The exposure cases were migrants who were not locally registered in the residence registration system. The study period encompassed January 1, 2017, to December 31, 2019. Including 3,246,164 outpatient medical records and 242,685 inpatient medical records. The key variables are medical expenditure and service volume indicators. Continuous variables were reported as mean and tested by t-test. We used interrupted time series analysis models to estimate the changes in the level and trend of each outcome measure after the policy.
Results: After the outpatient global budget payment reform, the monthly medical expenditure of the hospital alliance has transitioned from a discernible upward trajectory to a deceleration in the rate of growth. The outpatient volume in public and private high-level hospitals decreased at a rate of − 419.26 person/month and − 137.04 person/month, respectively. In terms of inpatient service volume, only private high-level hospitals reported a decrease, with a reduction rate of − 15.38 individuals per month.
Conclusion: This study presents new evidence demonstrating that the multi-hospital global budget payment can effectively control costs and promote resource reallocation when implemented jointly with hospital alliance policies. However, overly lenient budget caps risk counterproductive effects.
Keywords: global budget payment, multi-hospital, medical expenditure, service volume, China
Introduction
The growth rate of medical expenditure has exceeded the growth rate of national income, which is a global challenge seen in countries or regions like the United States, France, the Netherlands, and Tunisia.1–4 China faces the similar issue.5 Medical expenditure has increased more than tenfold in the past 15 years, from $10.572 billion in 2005 to $104.514 billion in 2020.6 A growing number of Chinese, particularly in rural areas, cannot afford the added burden of medical costs as the rise in medical expenditure outpaces income growth. Containing medical expenditure inflation has become an increasingly important policy priority.
Until 2016, Fee-for-service (FFS) serves as a prevalent payment method in China, wherein the remuneration is based on the quantity of services rendered. Several articles have revealed that doctors, operating under the FFS model, exhibit a tendency to engage in excessive procedures and accommodate a larger number of patients to augment their income.7,8 Regrettably, this inclination towards maximizing revenue has resulted in the squandering of valuable medical resources and an irrational escalation of medical expenditure.9,10 The absence of collaboration among hospitals at different levels contributes to the issue at hand.11 In their pursuit of maximizing benefits, high-level hospitals persist in expanding their patient base.11 Consequently, Chinese patients increasingly gravitate towards these high-level hospitals.12
To address this issue and curtail medical expenditure, it is imperative to seize the optimal moment for provider payment reform, thereby veering away from FFS.13 Provider payment reform holds the potential to shape provider behavior and indirectly guide patients towards seeking medical treatment in a more rational manner. Global budget payment is one of the most common provider payment reform strategies.3,14 One source of confusion about the impact of “global budget payment” is that the term has been used to refer to a wide variety of schemes used in different contexts.14 There are two budget models implemented in hospitals: the single-hospital global budget and the multi-hospital global budget.
Under the single-hospital global budget model, a budget is allocated to a specific hospital. It enabling the hospital to effectively manage its resources and expenditures within the provided budgetary constraints. The United States employs the single-hospital global budget model in certain regions. An example of this can be found in Maryland, where the implementation of a single-hospital global budget has demonstrated effective control over medical expenses. Heather Beil’s evaluation, utilizing the double difference method, supports this observation.15 However, it is important to acknowledge that internally, challenges persist in avoiding the expansion of patient numbers as hospitals compete for the next year’s budget quota. This phenomenon arises from the desire to secure a higher budget allocation for the upcoming year.
The multi-hospital global budget payment involves the allocation of a consolidated budget to a group or network of hospitals. This model aims to foster collaboration and coordination among the participating hospitals, allowing for a more efficient distribution and utilization of resources. The shared budget enables the hospitals to collectively address healthcare needs, optimize resource allocation, and enhance overall healthcare delivery across the network. In certain regions such as outpatient clinics in Germany, Taiwan, and certain parts of Canada, the multi-hospital global budget model has been adopted. However, it is worth noting that several articles have confirmed a tendency among healthcare providers to increase service volume within the given year under this payment model, as hospitals engage in fierce competition. For example, in Germany, while the global budget payment model has effectively controlled medical expenditure, there has been a notable surge in the volume of outpatient services provided.16,17 Similar observations have been made in Taiwan, where an unreasonable escalation in the number of outpatient services rendered to hypertension patients has been observed.18
Similar to many other countries, hospitals in China operate independently, while high-level hospitals oppress primary hospitals, leading to waste and inefficiency. Recognizing the challenges arising from hospital independence and the resulting excessive competition, China has taken steps to address this issue. By integrating independent hospitals into hospital alliances, China aims to mitigate the negative effects of competition and foster a more collaborative and coordinated approach to healthcare delivery. Medical expenditure comes from patient payments and health insurance payments. China’s medical insurance system is government-led social basic medical insurance. Therefore, government policies can jointly reform insurance payments and hospital alliances. The actual compensation level of China’s medical insurance system reaches 60–80%, making insurance payments the main source of hospital income. Reforms in the health insurance payment model will significantly impact hospital services. In 2016, the Chinese government has taken a proactive stance by implementing global budget payment for regional hospital alliances in certain counties. The implementation of global payments in China is based on the establishment of hospital alliances. This involves the formation of hospital alliances through the integration of all hospitals within a county, with unified medical insurance payment for these alliances.19,20 Regrettably, the model in various regions of China is not without its flaws. This imperfection has resulted in inadequate institutional cooperation.21 In China’s research landscape, current studies primarily concentrate on exploring how the hospital alliance promotes integration, but fail to highlight the pivotal role that integrated payments play in this process.21,22 Furthermore, there is limited exploration of the varying effects on different types of hospitals.21–23 Consequently, it remains challenging to draw definitive conclusions regarding the impacts of the China multi-hospital global budget payment. Hence, this article selects Dangyang, a county in central China, as the research subject to delve into the specific impact of the China multi-hospital global budget payment.
Context: The Reform of the Multi-Hospital Global Budget Payment in Dangyang County
Dangyang County, with medium economic level, is located in in Hubei Province, central China. The total population is 418 thousand. Among them, the rural population is 213 thousand, accounting for over 50%. The number of hospital beds per thousand people in the county was 4.78, and the number of healthcare professionals was 5.78 per thousand people. In comparison, the national average for county-level healthcare resources in the same year stood at 4.56 beds and 4.63 professionals per thousand people. These figures indicate that the county’s healthcare resources are at a moderate level nationwide. Moreover, Dangyang County has gained recognition as a national model city for the development of hospital alliances. Therefore, the reform effect of this county is more conducive to providing reference for other counties.
Similar to various regions across China, Dangyang County grapples with the issue of rapid growth in medical expenditure. In an ardent endeavor to tackle these challenges, Dangyang County undertook a reform initiative in April 2018, which entailed the implementation of the multi-hospital global budget payment and the establishment of a hospital alliance. This proactive approach aims to address the issues of escalating medical expenditure and inefficiencies in the delivery of healthcare services within the county.
Step 1: Establish the Hospital Alliance
Under the guidance of the government, Dangyang County has taken a decisive step by integrating all hospitals within the county to form a robust alliance. In this organizational structure, independent hospitals have transformed into functional or business departments, operating under the umbrella of the hospital alliance. The board of directors of the alliance consists of leaders from each participating hospital, with core directors appointed from high-level hospitals. Notably, the government has boldly bestowed the directors with authoritative powers encompassing management, personnel, finance, and other crucial aspects.
This unified approach enables comprehensive planning, decision-making, management, and equitable distribution of benefits across all business functions. The departmental structure fosters a high degree of interdependence and strong correlation among the hospitals. It addresses the issue of high-level hospitals exerting dominance over primary hospitals due to personal interests. When allocating resources, the leaders of high-level hospitals are required to consider the needs and circumstances of the primary hospitals.
Step 2: Implement the Multi-Hospital Global Budget Payment
Social medical insurance serves as the primary source of hospital income in Dangyang County. To maintain the structure of the hospital alliance and guide the transformation of provider services, the global budget payment is implemented as a vital economic incentive measure. In Dangyang County, the global budget amount is allocated into two categories: outpatient global budget amount and inpatient global budget amount. Each year, these allocated amounts experience a 10% increase. These funds are utilized to cover the costs associated with medical services within the scope of social medical insurance reimbursement.
Throughout the year, there are two scenarios where a discrepancy arises between the actual consumption amount and the budgeted amount: (a) when the budget amount exceeds the actual consumption amount, resulting in a profit for the hospital alliance, and (b) when the budget amount falls short of the actual consumption amount, resulting in a loss for the hospital alliance. This policy utilizes profit as an incentive to compel the hospital alliance to exercise control over medical expenditure, service volume, and resource allocation adjustments. By utilizing this approach, the hospital alliance is motivated to optimize resource utilization, curtail unnecessary medical expenditure, and ensure efficient service delivery.
However, there are still fundamental problems that are difficult to solve during the operation process. While the multi-hospital global budget payment sets an annual aggregate budget target at the beginning of the year, the actual allocation for each healthcare organization is still determined based on end-of-year performance evaluation. Even though some administrative integration is implemented, each hospitals remain independently operated legal entities. The government hopes to promote internal cooperation within institutions through administrative bundling, but in reality, it is difficult to achieve. More importantly, the key metrics in the year-end evaluation are the service volume performance of each hospital during that year, which provides strong incentives for hospitals to compete for more budget allocation in the following year. Meanwhile, hospitals risk having their baseline budgets reduced or face financial penalties if service and performance targets are not met. We concern that hospitals in hospital alliance may compete to increase their service volumes under this budget system.
Utilizing data extracted from the medical insurance information system of Dangyang County, we have obtained relevant indicators pertaining to medical expenditure and service volume for the years 2017 to 2019. This article aims to provide an analysis of the policy concerning the multi-hospital global budget payment in Dangyang County. By examining the reform measures on medical expenses and service volume, we seek to address two key questions. Firstly, does the implementation of the multi-hospital global budget payment effectively control medical expenditure and service volume? Secondly, are there discernible differences in the effects of these measures between high-level hospitals and primary hospitals, as well as between public and private hospitals? Through this study, we endeavor to shed light on these inquiries and deepen our understanding of the implications of the multi-hospital global budget payment in Dangyang County.
Materials and Methods
Study Design and Data Sources
We have conducted a retrospective comparative study using data obtained from the medical insurance information system of Dangyang County. The hospital alliance consists of 16 hospitals, including 3 public high-level hospitals, 3 private high-level hospitals, and 10 primary public hospitals. The study period encompassed January 1, 2017, to December 31, 2019, during which we collected data from a comprehensive database comprising 3,246,164 outpatient medical records and 242,685 inpatient medical records. This dataset provided valuable insights into outpatient and inpatient medical expenditure per visit, as well as the number of outpatients and inpatients.
Our study design involved comparing outpatient and inpatient medical expenditure before and after the implementation of the reform measures, as well as analyzing any variations in the number of outpatients and inpatients. Furthermore, we conducted a comparative analysis between high-level hospitals and primary hospitals. Within the high-level hospitals category, there are 3 public hospitals and 3 private hospitals. To ensure a comprehensive analysis, we also performed heterogeneity analysis to examine any distinctions between public and private hospitals.
Variables and Outcomes
The key variables in our study include outpatient and inpatient medical expenditure per month, outpatient and inpatient medical expenditure per visit, as well as the number of outpatients and inpatients per month. The implementation of the reform measures commenced in April 2018, and thus, we have selected this period as the boundary for the reform, utilizing it as an indicator variable (0 represents the period before the reform, spanning from January 2017 to March 2018; 1 represents the period after the reform, covering April 2018 to December 2019).
We conducted separate analyses to examine the levels and trends of both outpatient and inpatient medical expenditure per visit before and after the reform. Moreover, we focused on the levels and trends of public and private hospitals within the high-level hospital category, as mentioned earlier.
Furthermore, we analyzed the number of outpatients and inpatients, assessing their levels and trends before and after the reform. In line with our previous approach, we also examined the levels and trends of public and private hospitals within the high-level hospital category.
Through these comprehensive analyses, our study aims to gain valuable insights into the impact of the reform measures on medical expenditure and service volume. Additionally, we seek to explore any variations observed among different types of hospitals and ownership structures, thus contributing to a deeper understanding of the reform’s effects.
Statistical Analysis
Using SPSS 24.0 software, Continuous variables were reported as mean and tested by t-test.
We used interrupted time series analysis (ITSA) models, which are the quasi-experimental method, to estimate the changes in the level and trend of each outcome measure after the policy.24 After Gillings introduced ITSA into health services research, it has been widely used in assessing the effects of health services and policy interventions.25
Using Stata 14 software, we included the indicators in ITSA from January 2017–December 2019. The indicators include outpatient and inpatient medical expenditure per visit, as well as the number of outpatients and inpatients per month. To further explore the effect of reform on high-level hospitals, Separate public and private hospitals into ITSA. ITSA modeled the association of the indicators with the reform using the ordinary least-squares method. Considering factors such as seasonality and autocorrelation, we conducted the regression with Newey–West standard errors for autocorrelation and carried out a seasonal adjustment.
Statistical significance was determined at the 1%, 5%, and 10% levels.
Results
Outpatient
Table 1 presents data on the outpatient medical expenditure and outpatient volume across hospital types within the hospital alliance before and after the reform. Specifically, it includes information for: 3 public high-level hospitals, 3 private high-level hospitals, and 10 primary public hospitals. According to the results of t-test, the outpatient medical expenditure under the hospital alliance post-reform was $2609633.84 per month, exceeding the pre-reform expenditure of $2152476.04 (t = −8.028, P < 0.001). There are significant differences in these two factors among some types of hospitals before and after the reform. The average outpatient medical expenditure under the hospital alliance post-reform was $27.73 per visit, exceeding the pre-reform expenditure of $25.69 (t = −2.72, P = 0.010). High-level hospitals were the main contributor to this difference. Both public and private high-level hospitals experienced significantly increased medical expenditure post-reform relative to pre-reform levels (t = −2.37, P = 0.024. t = −6.10, P < 0.001). Specifically, expenditure rose by $7.60 and $4.10 respectively. Following the implementation of the reform, there remains a notable disparity in the number of outpatients per month compared to the pre-reform period (t = −4.19, P < 0.001). The outpatient volume increased from 84,357.67 person/month to 94,323.77 person/month. Both high-level hospitals and primary hospitals experienced remarkable growth, with a notable increase of 3422.06 patients and 6544.03 patients respectively (t = −2.29, P = 0.029. t = −4.09, P < 0.001). Furthermore, it is worth noting that there was a significant increase observed in both public and private high-level hospitals (t = −2.03, P = 0.050. t = −2.13, P = 0.041).
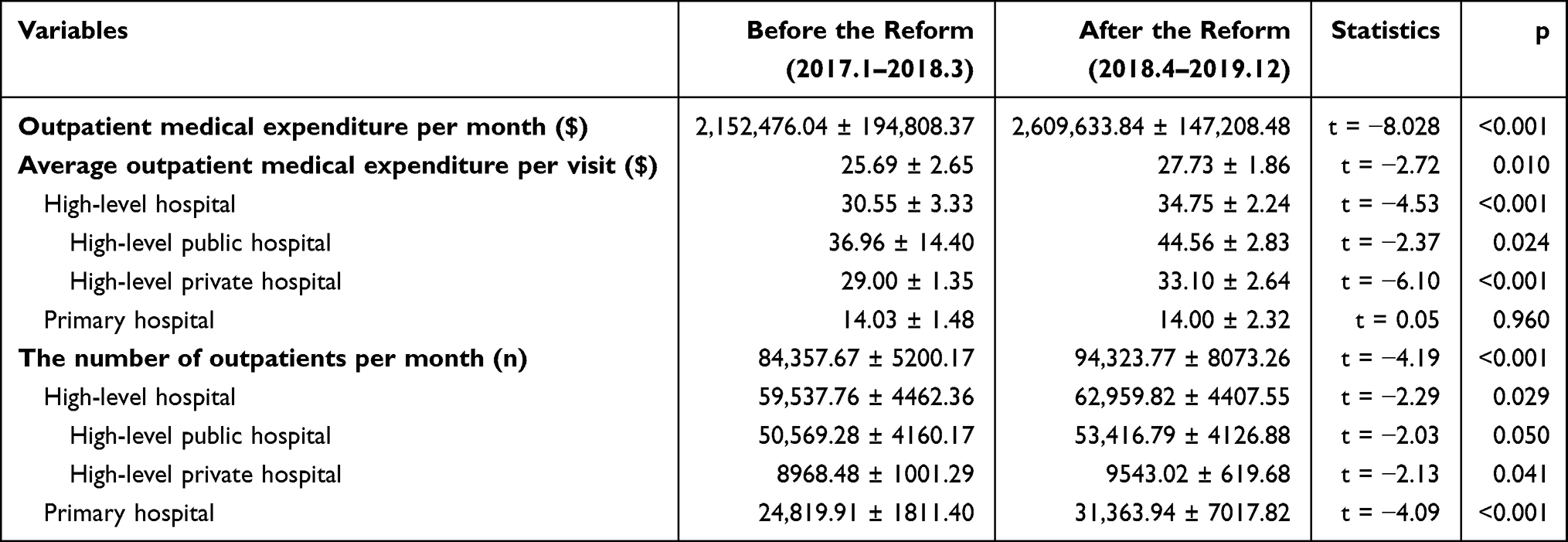 |
Table 1 Changes in the Average Outpatient Medical Expenditure per Visit and the Number of Outpatients per Month Before and After the Reform |
Figures 1 and 2 and Table 2 exhibit the ITSA results of the outpatient medical expenditure within the hospital alliance and its various hospital types, both before and after the reform. Prior to the reform, the outpatient medical expenditure in the hospital alliance demonstrated an upward trend with a slope of 36837.03 $/month (t = 5.99, P<0.001). However, following the reform, the trend experienced a decline at a rate of −21482.75 $/month (t = −3.21, P = 0.003). The average outpatient medical expenditure per visit showed the same trend of change. Prior to the reform, the average outpatient medical expenditure per visit in the hospital alliance demonstrated an upward trend with a slope of 0.46 $/month (t = 5.20, P<0.001). However, following the reform, the trend experienced a decline at a rate of 0.42 $/month (t = −3.83, P = 0.001). Specifically, both public and private high-level hospitals showed an upward trend before the reform, with growth rates of 0.16 and 1.48 $/month, respectively (t = −2.33, P = 0.026. t = −2.24, P = 0.032). No significant difference was observed in the changes after the reform (t = −0.13, P = 0.107. t = −0.99, P = 0.143). However, it is worth noting that the average outpatient medical expenditure in primary hospitals displayed an upward trend with a slope of 0.28 $/month (t = 7.74, P < 0.001) before the reform, and the trend experienced a decline at a rate of 0.41 $/month (t = −4.46, P < 0.001) after the reform. Figure 1 also shows that the trend changes of the average outpatient medical expenditure per visit in primary hospitals declines after the reform.
 |
Table 2 The ITSA Results of the Average Outpatient Medical Expenditure per Visit and the Number of Outpatients per Month Before and After the Reform |
 |
Figure 1 Segmented regression model showing the outpatient/inpatient medical expenditure per month before and after the reform. |
 |
Figure 2 Segmented regression model showing the average outpatient medical expenditure per visit and the number of outpatients per month before and after the reform. |
Figure 2 and Table 2 also show the ITSA results of the number of outpatients per month before and after the reform. Compared to before the reform, there has been no significant change in the trend of the number of outpatients per month in the hospital alliance (t = −0.16, P = 0.876). High-level hospitals and primary hospitals show two opposite trends after the reform (Figure 2). The number of outpatients in high-level hospitals experienced a significant decline at a rate of −556.30 person/month after the reform (t = −2.51, P = 0.017). Specifically, After the reform, there was a significant change in the regression slope of the number of outpatient patients in public and private high-level hospitals. The rate of change in levels is −419.26 and −137.04 person/month, respectively (t = −1.89, P = 0.068. t = −3.20, P = 0.003). On the contrary, after the reform, the number of outpatients in primary hospitals increased significantly at a rate of 614.05 person/month (t=2.66, P=0.012).
Inpatient
Table 3 displays data regarding the inpatient medical expenditure per visit and inpatient volume across various hospital types within the hospital alliance before and after the reform. According to the results of t-test, there are significant differences in these two factors among some types of hospitals before and after the reform. The average inpatient medical expenditure under the hospital alliance post-reform was $653.34 per visit, lower than the pre-reform expenditure of $607.31 (t = 4.35, P < 0.001). All types of hospitals played a significant role in contributing to this disparity. Both high-level hospitals and primary hospitals witnessed a reduction in average inpatient expenditure per visit compared to the pre-reform period (t = 6.00, P < 0.001. t = 2.14, P = 0.040). Specifically, expenditure decreased by $76.95 and $16.23 respectively. Following the implementation of the reform, there remains a notable disparity in the number of outpatients per month compared to the pre-reform period (t = −2.08, P = 0.045). The inpatient volume increased from 6446.11 person/month to 6801.80 person/month. High-level hospitals were the main contributor to this difference. Both public and private high-level hospitals witnessed a significant increase in the number of inpatients after the reform, surpassing the levels observed prior to the reform (t = −2.98, P = 0.008. t = −2.43, P = 0.021). Specifically, the number of inpatients rose by 132.34 person and 241.08 person respectively.
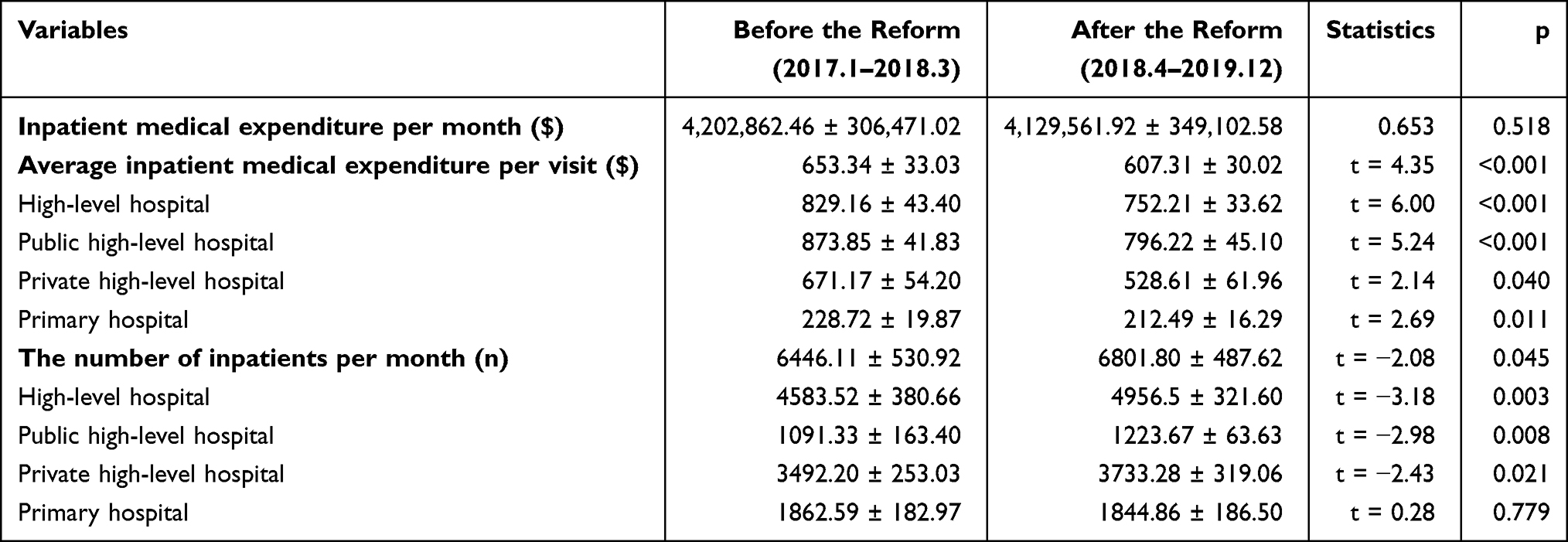 |
Table 3 Changes in the Average Inpatient Medical Expenditure per Visit and the Number of Inpatients per Month Before and After the Reform |
Figure 3 and Table 4 show the ITSA results of the inpatient medical expenditure within the hospital alliance and its various hospital types, both before and after the reform. The average inpatient medical expenditure per visit in hospital alliance had an upward trend with a slope of 4.19 $/month after the reform (t= 2.38, P = 0.024). Public high-level hospitals were the main contributor to this difference. The average inpatient medical expenditure per visit in Public high-level hospitals had a downward trend with a slope of −4.49 $/month before the reform (t= −2.50, P = 0.018). After the reform, it decreased −70.97 $ (t= −2.75, P = 0.010). Compared with the pre-reform periods, the trend changes rise at a rate of 7.66$/month after the reform (t= 3.05, P = 0.005). Figure 3 and Table 4 also show the ITSA results of the number of inpatients per month before and after the reform. Both public and private high-level hospitals showed an upward trend before the reform, with growth rates of 23.90 and 11.88 person/month, respectively (t = 2.20, P = 0.025. t = 2.01, P = 0.035). After the reform, only private high-level hospitals experienced a significant decline in the number of inpatients at a rate of 15.38 individuals per month (t = −2.49, P = 0.018).
 |
Table 4 The ITSA Results of Average Inpatient Medical Expenditure per Visit and the Number of Inpatients per Month |
 |
Figure 3 Segmented regression model showing the average inpatient medical expenditure per visit and the number of inpatients per month before and after the reform. |
Discussion
We have analyzed the impact of the multi-hospital global budget payment on medical expenditure and service volume within the hospital alliance. After the outpatient global budget payment reform, the monthly medical expenditure of the hospital alliance has transitioned from a discernible upward trajectory to a deceleration in the rate of growth. There was a notable shift in the trend of average outpatient expenditure per visit in primary hospitals, transitioning from an upward trajectory to a downward trend. The outpatient volume in public and private high-level hospitals decreased at a rate of −419.26 person/month and −137.04 person/month, respectively. However, the outpatient volume in primary hospitals witnessed an upward trend. There is no significant difference in the medical alliance, which indicates a certain degree of outpatient volume transfer from high-level hospitals to primary hospitals. Regarding the inpatient global budget payment reform, we observed that the average inpatient expenditure per visit in public high-level hospitals initially experienced a momentary decline, followed by a subsequent upward trend. In terms of inpatient service volume, only private high-level hospitals reported a decrease, with a reduction rate of −15.38 individuals per month.
The multi-hospital global budget payment for outpatient has prominently impacted the hospital alliance in Dangyang County. The monthly medical expenditure of the hospital alliance has undergone a significant transformation, shifting from a noticeable upward trend to a gradual deceleration in the growth rate. The implementation of the multi-hospital global budget payment has demonstrated its efficacy in effectively controlling medical expenditures. The conclusions drawn by Kilaru, Lin, and Song regarding the ability of global budget payment to effectively control the increase in healthcare expenses remain consistent with the current study’s results.26–28 This consistency across studies reinforces the value and significance of implementing global budget payment as a viable approach to managing and constraining medical expenditure.
Primary hospitals have effectively controlled average outpatient expenditure and taken on more patients diverted from high-level hospitals, which is consistent with policy expectations. China’s social health insurance provides more generous reimbursement for inpatient care relative to outpatient care.29,30 The outpatient reimbursement amounts place greater emphasis on chronic patients.31 Thus, the global budget for outpatient often operates under tight constraints. On the hand, to obtain more surplus in outpatient budgets, high-level hospitals will transfer unnecessary chronic patients to primary hospitals to avoid overspending medical insurance funds. On the other hand, the medical alliance has promoted hospital integration. High-level hospitals sink resources to primary hospitals through workforce training and skills transfer. This improves the ability of primary hospitals to attract and treat more outpatients.32,33 In summary, the reforms have redistributed the outpatient workload, with primary care now handling a larger share of chronic and general cases and helping control medical expenditure.
The multi-hospital global budget payment for hospitalization has not achieved the goal of cost control as intended, and may have even produced the opposite effect: the average inpatient medical expenditure of public high-level hospitals have shown a significant upward trend after the reform. The obtained results, however, do not align with the conclusions drawn in other articles that mention the effectiveness of global budget payment reform in effectively controlling medical expenditure.26–28 This may be attributed to overly generous budget ceilings and the dominant leadership role of public high-level hospitals within the hospital alliance. The global budget for hospitalization is increased by 10% annually in Dangyang County. Such expansions in funding fell short of sufficiently tight budgetary constraints.
It is worth mentioning that this global payment is made to the entire hospital alliance rather than to a single hospital. The hospital alliance in Dangyang county is not an independent legal entity; instead, each hospital within the alliance is an independent legal entity. They are all working towards the development of their own hospital’s interests. Inpatient services constitute the primary revenue stream for high-level hospitals, offering wider profit margins relative to outpatient care. While hospitals are managed collectively under the hospital alliance, self-interested incentives still exist for each.34,35 Given their largest scale and core position within the hospital alliance, public high-level hospitals can compete for more insurance funds by raising inpatient medical expenditure. Additionally, the result of ITSA of inpatient volume at private high-level hospitals indicates that they have faced some degree of constraint following the reform. This may be attributed to public high-level hospitals leveraging their leadership position within the hospital alliance to weaken inpatient services offered by private hospitals, thereby expanding their own market share. The impact on primary hospitals remains relatively limited due to their smaller number of inpatients and the typically milder symptoms exhibited by patients.
Why does the cost control effect of the outpatient global budget payment and the inpatient global budget payment have the opposite result? This could be attributed to the fact that the historical foundation of the inpatient budget is indeed substantial. The annual growth rate of 10% in Dangyang County exceeds the upper limit set by global budget payment standards in other countries. Take the Netherlands as an example, where the global budget payment mandates that hospitals’ medical expenditure should not surpass an annual growth rate of 2.5%.3 This stringent constraint ensures more effective financial management and control over medical expenditures. However, the relatively lax upper limit of the inpatient budget in Dangyang County results in insufficient constraints. Public high-level hospitals are more likely to prioritize their own interests in competing for market share when budget constraints are lax. Therefore, the inpatient global budget payment has failed to effectively control costs as intended. The global budget payment should impose stricter parameters on budget amounts.36 In addition, the hospital alliance does indeed facilitate resource allocation among hospitals, as evidenced by changes to outpatient services. However, in the case of inpatient services, loose budget constraints could inspire large hospitals to advance their own interests through leveraging alliance power. On the other hand, there is still a possibility that hospitalization services have high technical requirements, and patients are more inclined to choose high-value services for their health.
This study has several strengths. Firstly, it utilizes a retrospective design based on monthly data from official organizations, ensuring data quality. Secondly, to examine the impact of the reform, we conducted an interrupted ITSA on key indicators. Thirdly, hospitals were categorized into different types to further examine the impact of the reform on medical expenditure and service volume across hospital categories.
This study has several limitations. Firstly, This study primarily focuses on the impact of the multi-hospital global budget payment on healthcare expenditures and service volume. Consequently, it lacks an examination of healthcare quality and patient experience. This is also an important dimension that the payment model may impact. Secondly, the data used in this study is from January 2017 to January 2019, which is relatively outdated. This is primarily because China entered the COVID-19 pandemic period in 2020, which had a profound impact on the healthcare sector, making it difficult to investigate the results of various reforms. Therefore, the long-term effects of the reforms remain inadequately assessed. Thirdly, The study lacks a control group, which would enhance the credibility of the results. Fourthly, since this study only analyzed data from one county, there is a regional and biased nature to the data, limiting the generalizability of the conclusions. Additionally, due to limitations in the available data, the findings of this study can only be representative of regions comparable to the sampled areas. The results are not able to reflect the actual situation in more economically developed urban centers.
Conclusion
This study presents new evidence demonstrating that the multi-hospital global budget payment can effectively control costs and promote resource reallocation when implemented jointly with hospital alliance policies. However, overly lenient budget caps risk counterproductive effects. The research findings in Dangyang County serve to illustrate the impact of implementing the multi-hospital global budget payment for outpatient within the constraints of a relatively tight budget. This approach has effectively facilitated the redirection of less severe outpatient cases from high-level hospitals to primary hospitals. As a result, outpatient medical expenditure has been controlled, and the overall efficiency of outpatient services has witnessed improvement. Conversely, the budget allocated to the multi-hospital global budget payment for inpatient is notably more generous, leading to high-level hospitals increasing their provision of inpatient services in an effort to expand their profits. On the one hand, high-level hospitals, as the core managers of the medical alliance, guide other hospitals within the alliance to refer patients for higher-level treatment. On the other hand, due to their superior medical services and facilities, high-level hospitals are more attractive to patients. Moreover, the structure of the medical alliance has created a situation where public high-level hospitals may misuse their authority to attract patients from other hospitals. These findings suggest Chinese local governments should further examine budget caps and design them reasonably when deploying this policy combination.
Data Sharing Statement
The data-set used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study design was approved by the ethics institutional review board of Huazhong University of Science and Technology, Wuhan, China (approval number: 20210630-S170). All the methods were carried out in accordance with relevant guidelines and regulations. The need for informed consent was waived by the ethics institutional review board of Huazhong University of Science and Technology because of the retrospective nature of the study. All authors confirm that this research caused no harm (physical or mental) to any participants. The research process complies with the Declaration of Helsinki. The health data was anonymously provided by Dangyang Medical Insurance Bureau and the medical alliance.
Acknowledgment
We thank Dangyang County Medical Insurance Bureau and the medical alliance for providing historical data in the study, and those who reviewed drafts of this paper.
Funding
LX was supported by the National Natural Science Foundation of China (grant 72174068 to LX). KL was supported by Fundamental Research Funds for the Central Universities (grant YCJJ20242228 to KL).
Disclosure
The authors declare that there were no competing interests in this work.
References
1. Dieleman JL, Templin T, Sadat N, et al. National spending on health by source for 184 countries between 2013 and 2040. Lancet. 2016;387(10037):2521–2535. doi:10.1016/S0140-6736(16)30167-2
2. Vuagnat A, Yilmaz E, Roussot A, et al. Did case-based payment influence surgical readmission rates in France? A retrospective study. BMJ open. 2018;8(2):e018164. doi:10.1136/bmjopen-2017-018164
3. Gaspar K, Portrait F, van der Hijden E, Koolman X. Global budget versus cost ceiling: a natural experiment in hospital payment reform in the Netherlands. Eur J Health Econ. 2020;21(1):105–114. doi:10.1007/s10198-019-01114-6
4. Ben Abdelaziz A, Haj Amor S, Ayadi I, Khelil M, Zoghlami C, Ben Abdelfattah S; Financing health care in Tunisia. Current state of health care expenditure and socialization prospects, on the road to Universal Health Coverage. Tunis Med. 2018;96(10–11):789–807.
5. Zhang T, Lu B, Yan Z, Huang X, Lu W. Impacts of a new episode-based payment scheme on volume, expenditures, and efficiency in Public Hospitals: a Quasi-Experimental Interrupted Time-Series Study in Jinhua, China. Risk Manag Healthc Policy. 2022;15:1659–1669. doi:10.2147/RMHP.S376516
6. China NBoSo. China Statistical Yearbook. Beijing: China Statistics Press; 2021.
7. Miller-Breslow AJ, Raizman NM. Physician reimbursement: fee-for-service, accountable care, and the future of bundled payments. Hand Clin. 2020;36(2):189–195. doi:10.1016/j.hcl.2019.12.002
8. Ginsburg PB. Fee-for-service will remain a feature of major payment reforms, requiring more changes in Medicare physician payment. Health Aff. 2012;31(9):1977–1983. doi:10.1377/hlthaff.2012.0350
9. Tang X, Zhang X, Chen Y, Yan J, Qian M, Ying X. Variations in the impact of the new case-based payment reform on medical costs, length of stay, and quality across different hospitals in China: an interrupted time series analysis. BMC Health Serv Res. 2023;23(1):568. doi:10.1186/s12913-023-09553-x
10. Quinn K. The 8 basic payment methods in health care. Ann Intern Med. 2015;163(4):300–306. doi:10.7326/M14-2784
11. Yip W, Hsiao W. Harnessing the privatisation of China’s fragmented health-care delivery. Lancet. 2014;384(9945):805–818. doi:10.1016/S0140-6736(14)61120-X
12. Li C, Hou Y, Sun M, et al. An evaluation of China’s new rural cooperative medical system: achievements and inadequacies from policy goals. Bmc Public Health. 2015;15(1). doi:10.1186/s12889-015-2410-1
13. Ginsburg PB. Achieving health care cost containment through provider payment reform that engages patients and providers. Health Aff. 2013;32(5):929–934. doi:10.1377/hlthaff.2012.1007
14. Chen B, Fan VY. Strategic Provider Behavior Under Global Budget Payment with Price Adjustment in Taiwan. Health Econ. 2015;Nov;24(11):1422–36. doi: 10.1002/hec.3095
15. Beil H, Haber SG, Giuriceo K, et al. Maryland’s global hospital budgets: impacts on medicare cost and utilization for the first 3 years. Med Care. 2019;57(6):417–424. doi:10.1097/MLR.0000000000001118
16. Schmitz H. Practice budgets and the patient mix of physicians – the effect of a remuneration system reform on health care utilization. J Health Econ. 2013;32(6):1240–1249. doi:10.1016/j.jhealeco.2013.09.013
17. Busse R, Blumel M. Germany: health system review. Health Syst Transit. 2014;16(2):1.
18. Chang RE, Tsai YH, Myrtle RC. Assessing the impact of budget controls on the prescribing behaviors of physicians treating dialysis-dependent patients. Health Policy Plann. 2015;30(9):1142–1151. doi:10.1093/heapol/czu119
19. Xu J, Pan R, Pong RW, Miao Y, Qian D. Different models of hospital-community health centre collaboration in selected cities in china: a cross-sectional comparative study. Int J Integr Care. 2016;16(1). doi:10.5334/ijic.2456
20. Yip W, Fu H, Chen AT, et al. 10 years of health-care reform in China: progress and gaps in Universal Health Coverage. Lancet. 2019;394(10204):1192–1204. doi:10.1016/S0140-6736(19)32136-1
21. Cai M, Liu E, Tao H, et al. Does A medical consortium influence health outcomes of hospitalized cancer patients? An integrated care model in Shanxi, China. Int J Integr Care. 2018;18(2). doi:10.5334/ijic.3588
22. Wang X, Sun X, Gong F, et al. The Luohu model: a template for integrated urban healthcare systems in China. Int J Integr Care. 2018;18(4). doi:10.5334/ijic.3955
23. Zhong Z, Yao Q, Chen S, et al. China promotes Sanming’s Model: a National template for integrated medicare payment methods. Int J Integr Care. 2023;23(2):15. doi:10.5334/ijic.7011
24. Petrou P. An interrupted time-series analysis to assess impact of introduction of co-payment on emergency room visits in Cyprus. Appl Health Econ Health Policy. 2015;13(5):515–523. doi:10.1007/s40258-015-0169-2
25. Gillings D, Makuc D, Siegel E. Analysis of interrupted time series mortality trends: an example to evaluate regionalized perinatal care. Am J Public Health. 1981;71(1):38–46. doi:10.2105/AJPH.71.1.38
26. Kilaru AS, Crider CR, Chiang J, Fassas E, Sapra KJ. Health care leaders’ perspectives on the Maryland all-payer model. JAMA Health Forum. 2022;3(2):e214920. doi:10.1001/jamahealthforum.2021.4920
27. Lin LK. Effects of a global budget payment scheme on medical specialty workforces. Soc Sci Med. 2022;309:115254. doi:10.1016/j.socscimed.2022.115254
28. Song Z, Rose S, Safran DG, Landon BE, Day MP, Chernew ME. Changes in health care spending and quality 4 years into global payment. N Engl J Med. 2014;371(18):1704–1714. doi:10.1056/NEJMsa1404026
29. Li X, Lu J, Hu S, et al. The primary health-care system in China. Lancet. 2017;390(10112):2584–2594. doi:10.1016/S0140-6736(17)33109-4
30. Miao Y, Qian D, Sandeep S, et al. Exploring the characteristics of the high-cost population from the family perspective: a cross-sectional study in Jiangsu Province, China. BMJ Open. 2017;7(11):e017185. doi:10.1136/bmjopen-2017-017185
31. Du W, Liu P, Xu W. Effects of decreasing the out-of-pocket expenses for outpatient care on health-seeking behaviors, health outcomes and medical expenses of people with diabetes: evidence from China. Int J Equity Health. 2022;21(1):162. doi:10.1186/s12939-022-01775-5
32. Ran Y, Gao H, Han D, Hou G, Chen Y, Zhang Y. Comparison of inpatient distribution amongst different medical alliances in a county: a longitudinal study on a healthcare reform in rural China. Int J Equity Health. 2020;19(1):142. doi:10.1186/s12939-020-01260-x
33. Pan J, Zhao H, Wang X, Shi X. Assessing spatial access to public and private hospitals in Sichuan, China: the influence of the private sector on the healthcare geography in China. Soc Sci Med. 2016;170:35–45. doi:10.1016/j.socscimed.2016.09.042
34. Casalino LP. Which type of medical group provides higher-quality care? Ann Intern Med. 2006;145(11):860–861. doi:10.7326/0003-4819-145-11-200612050-00012
35. Kralewski JE, Zink T, Boyle R. Factors influencing electronic clinical information exchange in small medical group practices. J Rural Health. 2012;28(1):28–33. doi:10.1111/j.1748-0361.2011.00372.x
36. Ciarametaro M, Houghton K, Wamble D, Dubois R. The dollar or disease burden: caps on healthcare spending may save money, but at what “Cost” to patients? Value Health. 2021;24(3):388–396. doi:10.1016/j.jval.2020.10.024
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.