")
Back to Journals » Journal of Pain Research » Volume 18
The Efficacy and Brain Network Mechanism of Acupuncture for Knee Osteoarthritis: A Study Protocol for Randomized Controlled Neuroimaging Trial
Authors Sun YY, Wang ML, Zhao RH, Hao MY, Song S, Zhou Y, Zhang N
Received 9 October 2024
Accepted for publication 7 January 2025
Published 23 January 2025 Volume 2025:18 Pages 391—404
DOI https://doi.org/10.2147/JPR.S500024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yi-Yang Sun,1 Ming-Lin Wang,2 Ruo-Han Zhao,1 Ming-Yao Hao,3 Shuai Song,3 Yue Zhou,3 Na Zhang1
1Department of Acupuncture-Moxibustion and Tuina, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China; 2Traditional Chinese Medicine Comprehensive Treatment Center, Shengli Oilfield Central Hospital, Jinan, Shandong, People’s Republic of China; 3External Treatment Center of Traditional Chinese Medicine, Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China
Correspondence: Na Zhang, Email [email protected]
Purpose: Knee osteoarthritis (KOA) is a prevalent degenerative bone and joint disease observed in clinical practice. While acupuncture has demonstrated efficacy in treating KOA, the central mechanisms underlying its effects remain ambiguous. Recently, functional magnetic resonance imaging (fMRI) has been extensively applied in studying the brain mechanisms of acupuncture analgesia. Currently, network analysis based on brain connectomics is a focal point in acupuncture imaging research. Therefore, this study uses KOA as the research vehicle, focuses on the abnormal connectivity patterns of brain functional networks, and integrates clinical pain assessments to thoroughly investigate the central mechanisms of acupuncture therapeutic effects on KOA.
Patients and Methods: In this parallel, randomized, sham-controlled neuroimaging trial, 60 KOA patients will be randomly divided into the acupuncture group and sham acupuncture group in a 1:1 ratio, treated three times weekly for a total of 12 sessions. Patients will undergo clinical symptom assessments and cranial fMRI scans at baseline (− 1– 0 weeks), post-treatment (4 weeks), and at the follow-up (16 weeks). Forty healthy subjects will be recruited for observation, with a single MRI scan conducted only at baseline (− 1– 0 week). The primary efficacy indicator will be the change in NRS score after four weeks of treatment, with secondary outcomes including WOMAC, STAI, and safety assessments. fMRI observations will employ independent component analysis, brain network construction, and functional connectivity, complemented by Pearson correlation analysis to explore the relationship between brain responses and clinical improvements.
Conclusion: This study will initially uncover how acupuncture intervention for chronic KOA pain centrally regulates and exerts therapeutic effects through the modulation of abnormal brain network functional connectivity patterns, with a demonstrated long-term effect.
Ethics and Dissemination: This study has been approved by the ethics committee of Shandong University of Traditional Chinese Medicine Affiliated Hospital ((2024) Lunshen No. (028) - KY).
Clinical Trial Registration: This study has been approved by registered in the Chinese Clinical Trial Registry (ChiCTR2400083695).
Keywords: acupuncture, knee osteoarthritis, neuroimaging, RCT, protocol
Introduction
Knee osteoarthritis (KOA) is a prevalent and enduring joint ailment characterized by inflammation and degeneration of joint tissues, leading to pain and limited mobility.1 The pathogenesis of KOA represents a complex interplay of physiological and pathological processes resulting from the interaction of multiple factors.2 It involves not only the degeneration of cartilage and alterations in joint structure but also a series of other intricate changes.3 Specific tissues, such as the infrapatellar fat pad, may serve as a potential source of chronic knee pain in osteoarthritis and can undergo fibrotic changes that disrupt the normal physiological function and biomechanics of the knee joint.4 The most commonly associated risk factors for knee osteoarthritis (KOA) include advanced age, genetic predisposition, obesity, repetitive joint use, abnormal bone density, muscle weakness, and joint laxity.5–8 KOA is considered a disabling condition, and research from a meta-analysis indicates that the prevalence of symptomatic KOA in China is high, with 21 studies involving a total of 74,908 participants.9 Additionally, the overall estimated lifetime risk was found to be 13.83%.8 With the global population aging and obesity rates on the rise, it is widely anticipated that the burden of osteoarthritis will continue to grow, placing a heavier burden on healthcare systems.5,10
Currently, the management of KOA primarily focuses on symptom management, with treatment recommendations typically divided into non-pharmacological intervention, pharmacological intervention, and surgical intervention.11–13 While certain medications have demonstrated pain relief and enhanced joint function, the effectiveness of a considerable number of these drugs remains uncertain.14 Surgical treatment is not widely accepted by most people due to its inherent risks and substantial costs.15 Therefore, effective non-surgical treatment strategies for KOA, such as acupuncture, have gradually gained recognition in many countries.
In October 2022, the National Institute for Health and Care Excellence (NICE) in the UK released the new osteoarthritis guideline, giving a weak recommendation for acupuncture intervention.16 The “Chinese Guidelines for Diagnosis and Treatment of Osteoarthritis (2021 Edition)” released in September 2021 emphasized the efficacy and safety of acupuncture in ameliorating joint pain and function for osteoarthritis patients.17 Multiple randomized controlled trials (RCT) have shown that patients with KOA can benefit from acupuncture treatment.18–21 A meta-analysis published in 2016 (including 10 RCTs) revealed that acupuncture treatment is more effective than sham acupuncture in improving knee pain in the short term.22 However, currently there are still few studies on the mechanism of the central role of acupuncture in improving chronic pain in KOA, and further in-depth exploration is needed.
Functional Magnetic Resonance Imaging (fMRI) studies have implicated metabolic alterations in brain networks associated with sensation, motor function, emotion, and cognition in chronic pain conditions.23–25 The central regulatory effect of acupuncture on KOA involves different brain responses. Relevant studies have proved that acupuncture can enhance the functional connection between the dorsal raphe and the striatum, as well as in the right frontoparietal neural network (rFPN) and the executive control network (ECN) with the anterior cingulate cortex/medial prefrontal cortex.26,27 Our preliminary research aimed to predict the efficacy of acupuncture in alleviating chronic pain associated with knee osteoarthritis (KOA) by analyzing psychological and neurological factors prior to treatment. We observed that the functional indicators such as posterior cingulate cortex (PCC)/precuneus fractional amplitude of low-frequency fluctuation (fALFF), striatal fALFF related to the effectiveness of acupuncture in improving chronic pain showed changes, whereas the structural indicators such as striatal volume, thickness of the PCC remained relatively stable.28 However, existing studies lack comprehensive investigations into abnormal brain networks linked to chronic KOA pain or the long-term mechanisms of acupuncture-induced pain relief. Despite some recent fMRI studies on chronic KOA pain and acupuncture analgesia, further research is necessary to clarify the role of brain functional networks in the development of chronic KOA pain and the regulatory role of acupuncture analgesia.
Therefore, investigating the central effects of acupuncture analgesia mechanisms based on the abnormal connectivity patterns of KOA brain functional networks is currently a crucial task in acupuncture research. This study aims to preliminarily explore the central mechanism of how acupuncture enhances abnormal brain functional network connectivity patterns in KOA patients through the RCT design combined with fMRI technology. The main objective is to provide scientific evidence and insights for the clinical efficacy and central mechanisms of acupuncture treatment for KOA.
Methods
Study Design
This study is a single-center, parallel control, randomized controlled trial. Sixty KOA patients will be randomly assigned to either the true acupuncture group (TA) or the sham-acupuncture group (SA) in a 1:1 allocation ratio, with 30 patients in each group. The total observation period for KOA patients is 16 weeks, including a 1-week baseline period, a 4-week clinical treatment period, and a follow-up period on the 16th week. Before the treatment, all KOA patients (n = 60) will undergo clinical indicator assessments and magnetic resonance scans. After the treatment and in the follow-up period, the patients will be reassessed on these indicators. 40 healthy people will also be included as matched healthy controls (HC) and will only undergo baseline fMRI scans. The study flow chart is presented in Figure 1, and the schedule of enrolment, interventions, and assessments is shown in Table 1.
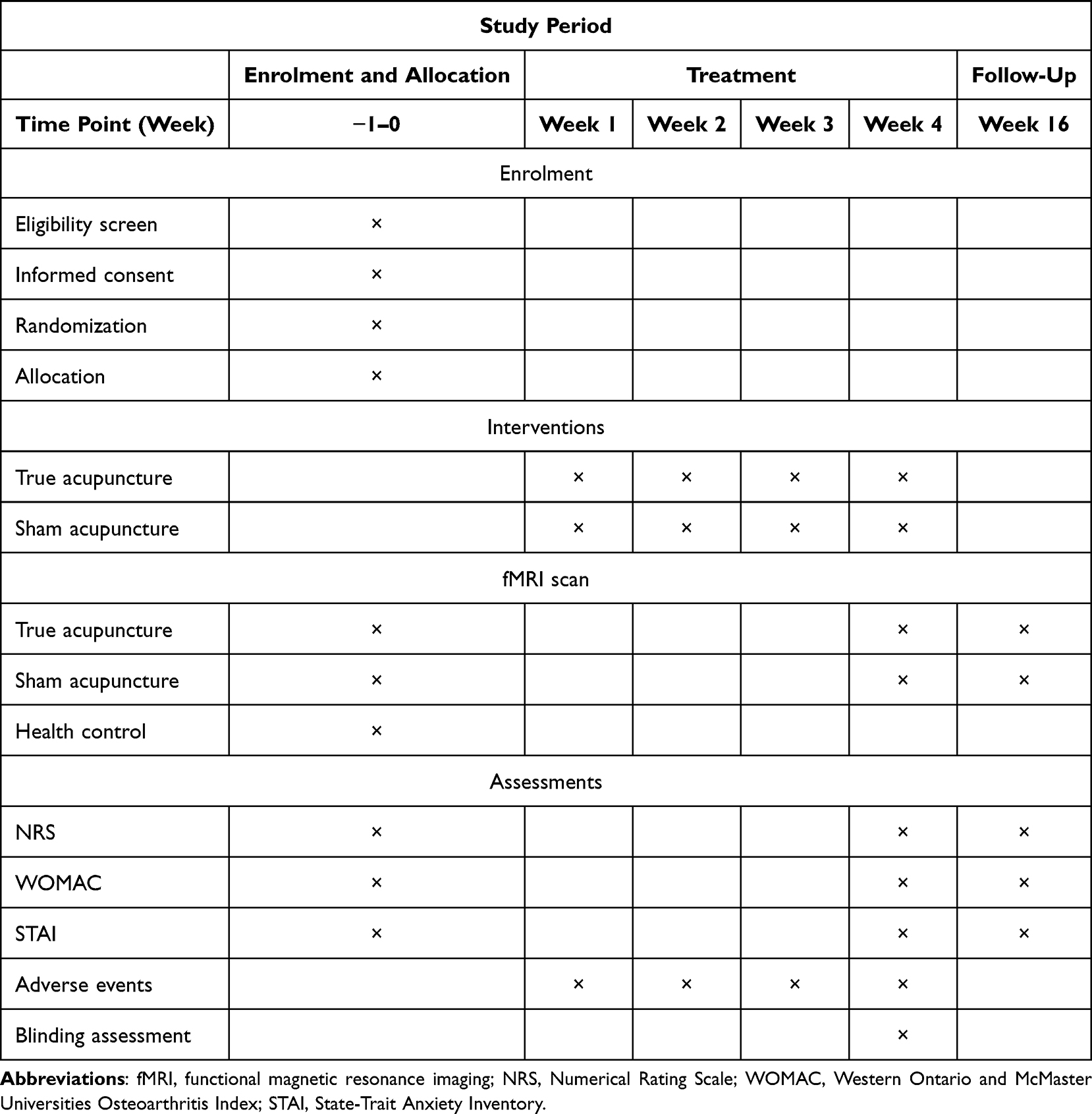 |
Table 1 The Schedule of Enrollment, Intervention and Assessments in This Study |
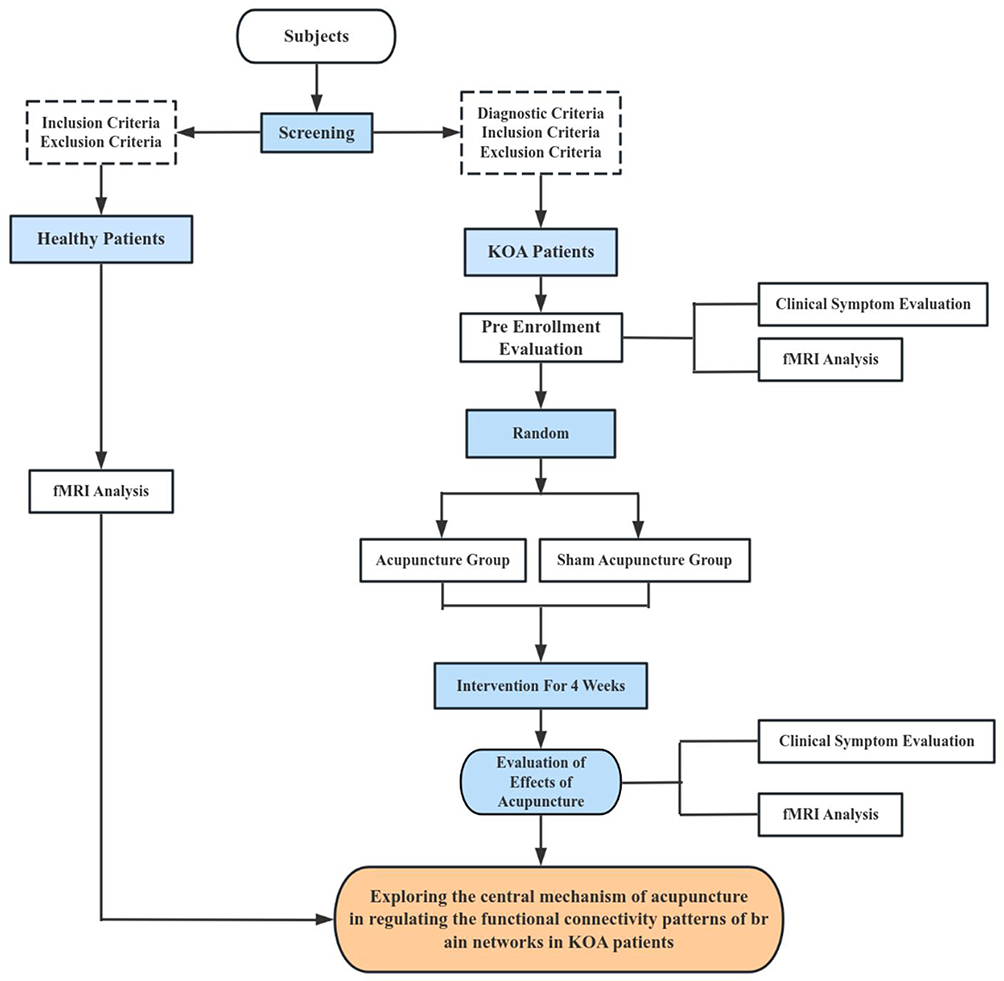 |
Figure 1 The study flow chart. |
This study will be reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statements and Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) statements. This protocol is reported following the Standard Protocol Items: Recommendations for Intervention Trials (SPIRIT) guidelines (shown in Supplementary Table S1).
Participants and Recruitment
A total of 60 eligible patients diagnosed with KOA will be recruited from the Affiliated Hospital of Shandong University of Traditional Chinese Medicine. The recruitment advertisement will be mainly published to the public on WeChat (a Chinese social media platform) and also placed on bulletin boards or other places in the hospital to promote recruitment. Voluntary patients need to undergo diagnosis and assessment by certified clinicians according to inclusion and exclusion criteria, then the eligible 60 patients will be randomly allocated at a balanced ratio (1:1) into the acupuncture group and the sham acupuncture group after signing the informed consent. They will be not only informed of the whole procedure, benefits, and potential risks via receiving information sheets before the trial begins but also made aware that they could withdraw at any moment without any reason or benefit loss during the study period. In addition, 40 healthy subjects will be recruited for comparison so as to conduct observation research.
Inclusion Criteria
Inclusion Criteria for TA and SA Groups
According to the diagnostic criteria in the guideline for KOA of ACR (American College of Rheumatology Subcommittee) (1995),29 the inclusion criteria for patients with KOA are as follows:
1) Age between 40 and 70 and right-handed;
2) Duration of symptoms exceeding 6 months;
3) Kellgren-Lawrence (K-L) graded as II or III;
4) Numerical Rating Scale (NRS) score ≥ 4.
Inclusion Criteria for HC Group
1) Aged 40–70, right-handed;
2) Absence of knee discomfort such as pain, limited function, or stiffness;
3) Good physical condition;
4) No presence of organic or severe functional diseases;
5) No MRI contraindications such as claustrophobia;
6) No involvement in other clinical studies.
Exclusion Criteria
The patients will be excluded if they meet any of the following criteria:
1) History of knee surgery or waiting for knee surgery such as total knee replacement (TKR) and arthroscopic knee surgery (AKS);
2) History of arthroscopy within 1 year or intra-articular injection within 6 months when screened;
3) Knee pain attributed to other conditions (eg, loose bodies, severe joint effusion, inflammation, malignant tumors, autoimmune diseases, trauma, fracture, or gout);
4) Severe acute or chronic organic and psychiatric diseases;
5) Blood coagulation disorders such as hemophilia;
6) Preparing for pregnancy, being pregnant or lactating;
7) Contraindications for MRI scans, such as claustrophobia, cardiac defibrillators, or metallic objects implanted in the body;
8) Organic lesions or severe abnormality of anatomical asymmetry in MRI scanning;
9) Treatment of acupuncture or moxibustion during the past 1 month;
10) Allergy to needles and alcohol, fear of acupuncture;
11) Involved in other clinical trials during the previous 3 months.
Dropout and Suspension Criteria
Patients failing to complete treatment or follow the study protocol will be considered dropouts. Researchers will contact dropouts to determine the reasons for incomplete treatment, and efforts will be made to complete the assessments. Details of all dropped-out patients such as acupuncture frequency and the last time for treatment should be recorded in the case report files (CRF) to ensure subsequent analysis.
The observation should be discontinued promptly upon the occurrence of serious adverse events or the development of any unexpected illnesses that render the patient’s condition inappropriate for continued monitoring, and the latter will be considered invalid cases. Additionally, suspension may also occur if significant non-compliance results in a loss of efficacy evaluation.
Randomization and Concealment
Block randomization will be applied in this study, with a length of 4. Sixty patients will be randomly allocated to the acupuncture group and the sham acupuncture group at a 1:1 ratio. Random number sequences will be generated using SPSS software (version 26.0, SPSS Inc., Chicago, IL, United States) by independent statisticians not involved in the study. The allocation of random numbers will be entrusted to a predetermined specialized researcher, who will securely store them. Once the eligible participants have been randomly assigned, the researchers will then inform the acupuncturists of the respective random numbers via a brief message, ensuring a transparent and unbiased process.
Blinding
During the entire procedure, patients will not be informed of the treatment that they will receive, with outcome assessors and statisticians also being kept blind to the allocations through the use of random numbers instead of actual labels to prevent bias. However, the acupuncturists cannot be blinded due to the proprietary treatment characteristics of acupuncture. They will not disclose any information regarding treatment to participants and not be involved in assessing outcomes to ensure blinding integrity.
Unblinding will only be required after study completion except if the researchers must be notified regarding related information of the group when the participant has a serious adverse event (SAE) or needs rescue. Reasons, time, and staff involved in emergency unblinding should be promptly recorded in CRFs, with a security incident report to be submitted to the ethics committee. Information on frequency, reasons, extent, and timing of emergency unblinding should also be included in the final statistical analysis for reference in evaluating efficacy and safety.
The credibility of blinding procedures will be assessed by independent researchers not involved in patient allocation or treatment during the acupuncture intervention phase at week 4.
Sample Size Calculation
For fMRI research, different from clinical trials, there are no standardized methods for determining sample sizes. Based on previous studies, referring to the Type I error rate α=0.005, we recommend 20 patients.30 When α=0.000002, approximately 25 patients are required.31 Considering a 20% dropout rate and potential data loss due to head movements during scanning, a maximum of 25 patients per group is adopted for the KOA patient group, with plans to recruit 30 patients in each group.
Intervention
Acupoint selection is based on the traditional Chinese medicine acupuncture theory, combined with the clinical experience of acupuncture physicians, and culminates in establishing a fundamental consensus.21,32 Acupuncture physicians must obtain a license from the Ministry of Health of the People’s Republic of China and have at least 5 years of clinical practice experience. Acupuncture group and sham acupuncture group will receive treatment in different small rooms for 4 weeks and 3 times per week. We will use the needles (Hwato, Suzhou, China, 0.30 × 40 mm or 0.30 × 25 mm) in both groups. Locations of all acupoints will adhere to the National Standard of the People’s Republic of China (GB/T12346-2010). Prior to commencing the trial, clinicians will undergo specialized training encompassing basic clinical methods, follow-up procedures, and treatment protocols. The research overview diagram is shown in Figure 2.
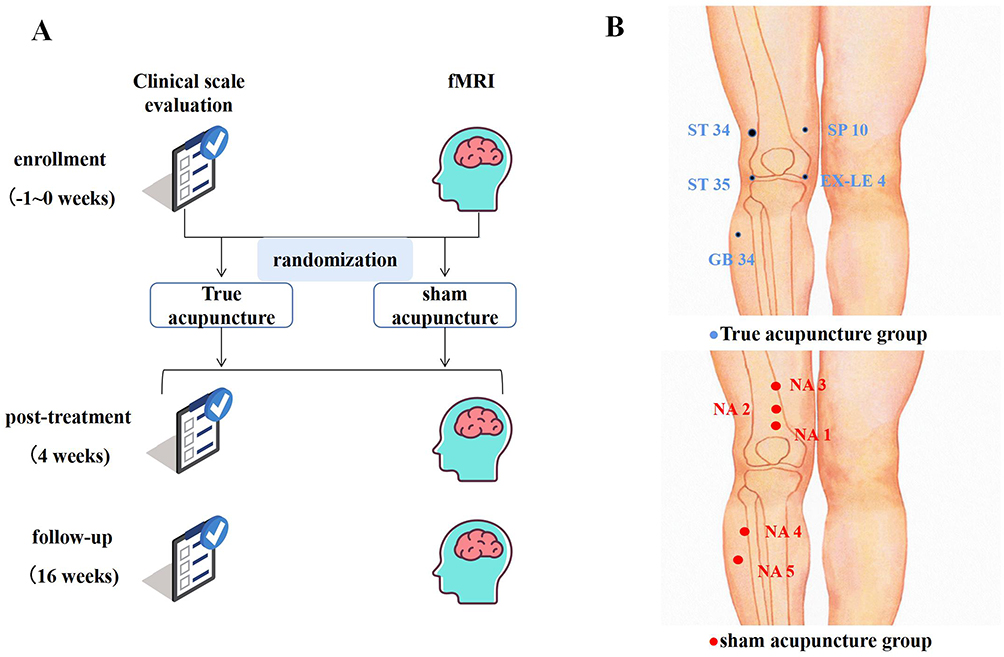 |
Figure 2 The research overview diagram and the location of acupoints. (A) The research overview diagram. (B) The location of acupoints in true acupuncture group and sham acupuncture group. Notes: The blue dots represent the location of real acupoints in the true acupuncture group. The red dots represent the location of sham acupoints in the sham acupuncture group. |
True Acupuncture Group
The patients will be treated with a supine position at real acupoints (Figure 2 and Table 2) including bilateral Du Bi (ST35), Nei Xi-yan (EX-LE4), Xue Hai (SP10), Liang Qiu (ST34), Yang Ling-Quan (GB34), and Ashi acupoints (painful spots confirmed by patients or palpation points33). After the skin is disinfected with alcohol, needles will be inserted into acupoints at a depth of 5–20mm and then twisted or lifted to generate a Deqi sensation. After Deqi, the needles will be retained for 30 minutes followed by the needles’ withdrawal.
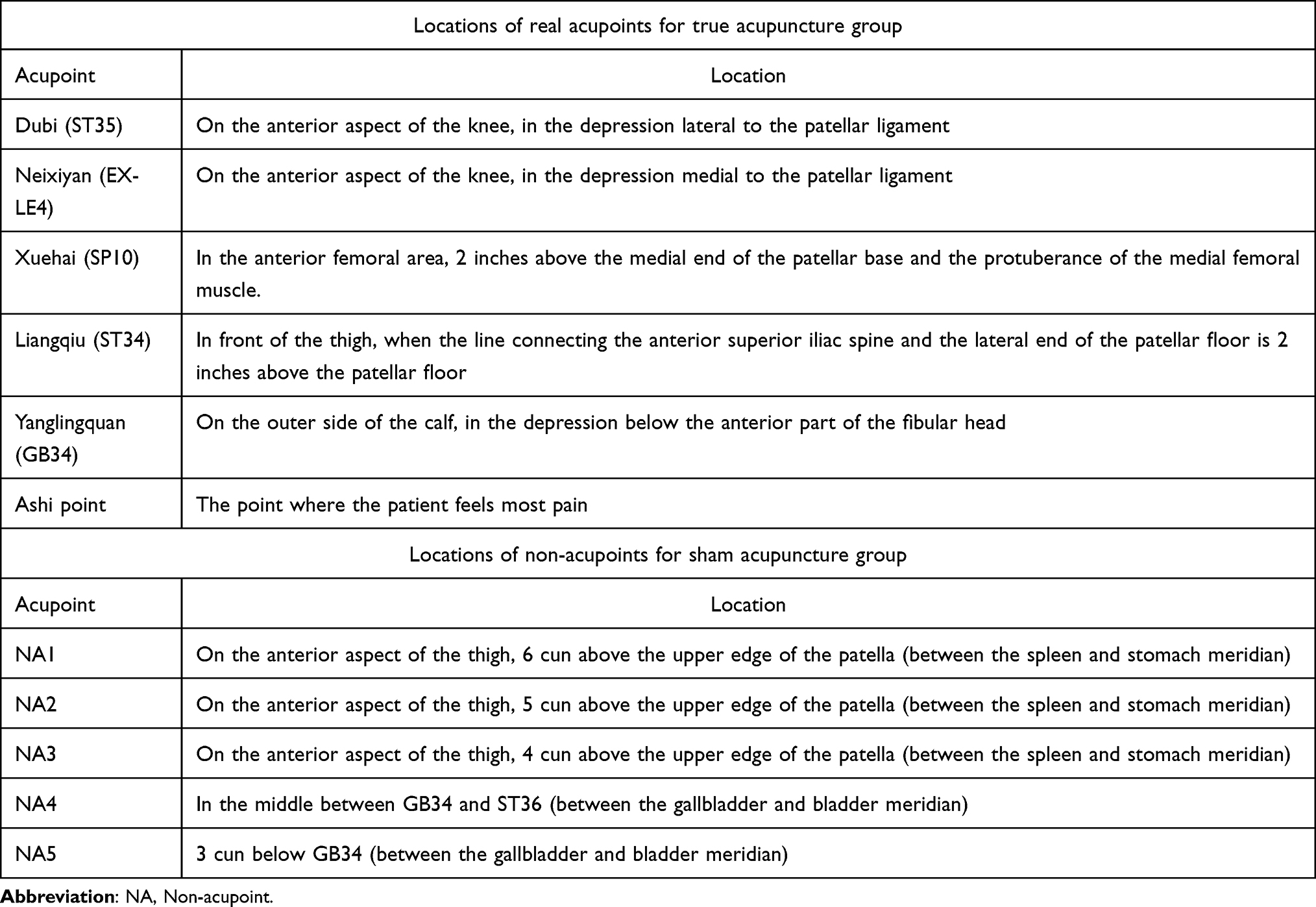 |
Table 2 Locations of Acupoints and Non-Acupoints for True Acupuncture and Sham Acupuncture Groups |
Sham Acupuncture Group
The patients will receive superficial skin penetration at sham acupoints without Deqi sensation, following a methodology commonly employed in randomized controlled trials.34 In our study, needles will be inserted into the skin for approximately 1mm at 5 non-acupoints following disinfection. The location of the sham acupoints is shown in Figure 2 and Table 2. Needles will be retained for 30 minutes without Deqi sensation.
Temporary Oral Painkiller Regulations
Before enrollment, patients will be informed that they should try not to use other drugs related to the treatment of KOA during the entire observation and treatment period. In compliance with the Declaration of Helsinki ethical principles, patients experiencing severe pain (NRS > 8) will be instructed to promptly notify the investigator for temporary treatment with oral non-steroidal analgesics. Detailed records will be maintained by the investigator regarding the drug’s name, administration method and dosage, and timing. Moreover, the proportion of people taking temporary painkillers should be calculated. If a patient consumes other medications exceeding 1/4 of the prescribed intervention amount during the study period, their data will be excluded during final data processing.
MRI Protocol
fMRI scans will be performed at the First Rongjun Youfu Hospital of Shandong Province using a 3.0 Tesla MR scanner (GE Discovery MR750, GE Healthcare, Chicago, IL, United States). To ensure imaging quality, a designated radiological technician will operate the scanner consistently using the same machine each time. Prior to the research commencement, training sessions will be organized for the relevant personnel to grasp the research design and MRI safety measures. Before entering the MRI operating console, our researcher will once again confirm with the patient if they have any metal items, ask the patient to put on earplugs in advance, lie down relaxed on the MRI table, and stabilize the patient’s head through a head mask and sponge to prevent large head movements during the scan. The patients will hold a ball and can signal discomfort by squeezing it, prompting immediate halt of the scan. A professional researcher in radiology will check the quality of the images and program compliance after each scan to detect any brain injury or structural abnormalities.
Participants in the acupuncture group and the sham acupuncture group will undergo scans at pre-grouping, post-treatment, and after follow-up. HC subjects will only undergo one scan after enrollment.
For resting-state fMRI, echo planar imaging (EPI) sequence will be used with parameters: repetition time (TR) = 2000 ms, echo time (TE) = 30ms, field of view (FOV) = 220 mm × 220 mm, flip angle (FA) = 90°, layer thickness = 3.0mm, number of layers = 40, voxel size = 2.3 mm × 2.3 mm × 3.0 mm, and scanning duration = 10 min. Registration structural images will be obtained using 3D T1-weighted MPRAGE sequence with: TR = 2300 ms, TE = 2.32ms, FOV = 240 mm × 240 mm, flip angle = 8°, layer thickness = 0.9 mm, matrix = 256 × 256, number of layers = 192, voxel size = 0.9 mm × 0.9 mm × 0.9 mm.
T1 weighted 3D magnetization preparatory gradient echo sequence (3D T1-weighted MPRAGE) will be utilized with specific parameters: TR = 2530 ms, TE = 2.98 ms, magnetic field (FOV) =240mmx240 mm, FA = 7°, level thickness = 1.0 mm, matrix (Matrix) =256 × 256, layers =192, voxel size =1.0 mm × 1.0 mm × 1.0 mm.
Outcome Measures
Primary Outcome Measures
Numerical Rating Scale, NRS
The Numerical Rating Scale (NRS) is a single 11-point numeric scale commonly utilized to assess pain intensity, ranging from 0 for “no pain” to 10 for “worst pain imaginable”.35,36 As the score increases, it indicates that the pain becomes more severe.
Secondary Outcome Measures
Osteoarthritis Index
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) is a comprehensive system for evaluating knee conditions across three subscales: pain, stiffness, and physical function, involving a total of 24 questions.37 The severity of pain, stiffness, and physical function will be represented by increased scores.
State-Trait Anxiety Inventory, STAI
The State-Trait Anxiety Inventory (STAI) is an identified questionnaire to evaluate the association between anxiety and stress level, comprising state anxiety (STAI S-A) for emotional and transitory anxiety condition and trait anxiety (STAI T-A) for stable propensity on anxiety.38,39 The STAI will be used in this trial to assess the severity of anxiety with a higher score representing more anxiety.
fMRI Outcome Measures
fMRI will be used to meticulously track alterations in brain network activity via an array of indicators, including low-frequency fluctuation amplitude (ALFF), regional homogeneity (ReHo), seed-based functional connectivity (FC), and independent component analysis (ICA), providing a comprehensive understanding of neural dynamics, and further reveal the association between clinical outcome and brain activity via statistical methods such as Pearson correlation analysis. These indicators show the specific neuroimaging changes in the brain. FC indicates synchronicity and functional connectivity between different regions, while amplitude of low-frequency fluctuation and ReHo are applied to determine the regional change of the local brain area.40 And the ICA algorithm is employed to extract and match the information with interconnected and closely related functional networks for further comparison and analysis.41
All clinical indicators through scales filling and fMRI scanning will be detected 1 week before inclusion, week 4, and week 16.
Safety Assessments
Adverse Events (AEs) will be documented by participants and acupuncturists collaboratively to determine if they are related to acupuncture treatment. In cases of observed AEs, appropriate actions, such as treatment discontinuation or hemostasis, will be promptly taken by acupuncturists. Detailed documentation including event occurrence, symptoms, duration, severity, causal analysis, and treatment response will be conducted. Serious Adverse Events (SAE) will involve events causing death, posing a life-threatening situation, leading to hospitalization or extending hospital stay, resulting in permanent disability, or requiring medical intervention to prevent suffering. SAEs will be promptly reported to the safety committee for proactive management. Information regarding treatment discontinuation, outcomes, and timing will be recorded concurrently in CRFs for comprehensive statistical analysis.
Data Management and Quality Control
Researchers will be instructed to record data for screening and assessment on the original paper CRFs to follow the protocol. To ensure the accuracy of the study data, researchers will promptly record evaluation, outcome measures, baseline, and other trial data on the CRFs for regular verification. If there are corrections, explicit labeling should be illuminated according to the correction instructions in the CRF. For fMRI data, the researchers will be responsible for recording on DVDs and converting the format of obtained data timely, meanwhile checking the completeness of images and head motions. All original data and CRFs will be safely stored by our specific study members in a locked filing cabinet for loss avoidance. Additionally, the results of this study may be published in medical journals, and all the patients’ information will be kept confidential legally except for requirements by relevant laws.
Rigorous inclusion and detailed protocol will be conducted to persist in strictness. Before the formal trial, clinical training will be provided to familiarize researchers with the process, operation of acupuncture, and implementation of scales. The protocol will be on-site trained to make the performance of acupuncture standardized. Monitoring and spot checks for every 4 subjects included will be regularly applied.
Statistical Analysis
Clinical Data Analysis
Statistical analysis will be performed using SPSS software (version 26.0, SPSS Inc., Chicago, IL, United States). All statistical tests with a P-value of ≤0.05 will be considered statistically significant. For measurement data that conforms to normal distribution, the independent samples t-test is employed for comparisons between groups, whereas the paired samples t-test is utilized for within-group analyses. The results are typically presented as mean ± standard deviation; For measurement data that do not follow a normal distribution, non parametric rank sum test is used, described by median (interquartile range). The Chi-Square Test is utilized to analyze categorical variables, with percentages (n%) serving as the descriptive statistic.
Equilibrium analysis of baseline values: Independent sample t-test or chi-square test will be used to compare demographic data and other baseline indicators to evaluate the balance between the two groups. Paired t-test will be used to assess the differences within each group compared to the baseline values during the screening period.
Sensitivity analysis: In the per-protocol analysis (PP) for the primary outcome measure after 4 weeks of treatment, patients who underwent a minimum of 10 acupuncture treatments and completed the requisite questionnaire will be included.
fMRI Data Analysis
All neuroimaging data analysis will be conducted on the MATLAB 2017b platform. Based on the SPM12 toolkit (http://www.fil.ion.ucl.ac.uk/spm) and DPARSF tool (http://rfmri.org/DPARSF), the data preprocessing will include converting DICOM format, removing the first 10 time points, slice timing correction, motion correction (deleting subjects with translation > 2mm or rotation > 2°), spatial normalization (resampling to 3.0 mm×3.0 mm×3.0 mm), removing linear drift, low-frequency filtering (0.01–0.1Hz), and regressing out covariates (24 Friston head motion model parameters, cerebrospinal fluid, white matter, and global mean signal).
After all pre-processed resting-state fMRI images from the different groups into one group, Independent Component Analysis (ICA) will be performed using the GIFT v3.01 toolkit (https://trendscenter.org/software/gift). Researchers employ ICA combined with fMRI to extract spatial independent components (ICs) to enable the assessment of functional connectivity between the resting-state networks. Relevant ICs associated with chronic pain will be selected based on literature. After ICA, a single-sample t-test will be performed on the 3D spatial map of each IC. Pearson correlation will be used to calculate the correlation coefficients between pairs of time series for functional connectivity and to construct patients’ functional brain network. The SPM12 and SPSS software will be used to determine the statistical analysis of brain functional connectivity, which refers to the cerebral responses to acupuncture. Intra-group comparisons will be conducted using paired t-tests, while inter-group comparisons will utilize independent sample t-tests. Functional connectivity strength maps will be subjected to independent sample t-tests with covariates such as age, gender, education duration, and head motion parameters. Regions with statistically significant differences will be identified based on corrected P-values, and these specific brain regions will be considered to have a resting-state FC with the based seed spots. The correlation between brain structure and function and the variables among different groups will be reflected in the results above.
Discussion
Knee Osteoarthritis (KOA) is one of the clinically common degenerative osteoarticular diseases, characterized by high prevalence and high disability rate.42 Increasing clinical evidence supports acupuncture as an effective treatment method for improving chronic pain in KOA.20,43 Therefore, utilizing modern technological means to comprehensively investigate the central mechanism of acupuncture treatment for chronic pain in KOA has important practical significance in improving the clinical efficacy of acupuncture analgesia and advancing the theory of acupuncture analgesia.
Currently, the research on the central mechanism of acupuncture improving chronic pain in KOA mainly focuses on certain brain regions of interest and the short-term effect mechanism of acupuncture.26,27,44 Therefore, based on previous studies, this study further integrates modern fMRI techniques and adopts a brain functional networks perspective to effectively correlate the central brain mechanism of acupuncture analgesia intervention with the central sensitization and neuroplasticity implicated in the onset and progression of chronic pain in KOA. Through the identification of optimal neural markers for chronic pain in KOA and acupuncture analgesia, this study explores the relationship between changes in these markers, while also observing the enduring central regulatory impact of acupuncture intervention on chronic pain in KOA. This study may provide favorable evidence support for clinical investigations on acupuncture analgesia.
The advantages of this study are mainly reflected in the following aspects. Firstly, it focuses on connectivity patterns derived from brain functional networks to explore the link between chronic pain occurrence in KOA and aberrant functional connectivity patterns within the brain network. Subsequent analysis delves into the central mechanism of acupuncture analgesia, with a longitudinal period set to delve into the sustained central mechanisms of acupuncture analgesia effects. Secondly, This study leverages the technical advantages of fMRI and utilizes the functional brain network analysis method of ICA to identify potential central targets for the occurrence of chronic pain in KOA from a brain functional network perspective. It further analyzes and compares the short-term and long-term effect targets of acupuncture. Thirdly, to observe the abnormal functional connectivity patterns in the brain networks of KOA patients, HC will be included. By comparing the fMRI data from KOA patients and HC subjects, we aim to identify KOA-specific abnormal brain functional networks. Building on this, the study will delve into the short and long-term effects of both true acupuncture and sham acupuncture on the abnormal brain network connectivity patterns in KOA patients. Furthermore, quality control provides the favorable conditions for improving the reliability of results. The protocol and implementation in this study will strictly adhere to existing standards. Other measures will be taken such as strict criteria, separate treatment facilities, unified training, and the same examination machine to ensure homogeneity and stability. The assessment of blinding credibility will be conducive to avoiding the severe bias of breaking and unblinding.
The following are the limitations of this study. First, chronic pain and negative emotions such as anxiety and depression are increasingly gaining attention from researchers.45–47 This study primarily focuses only on the relief of pain symptoms with acupuncture and does not look into the improvement of emotional states or the neurological processes that underpin acupuncture’s benefits. Future study should explore more deeply into the relationship between pain and emotion. Second, in terms of acupuncture intervention methods, the sham acupuncture group employed superficial needling at non-meridian points. Recent studies on the non-penetration of the sham needles have yielded inconsistent results.48 Some researchers contend that superficial needling can produce specific acupuncture effects, resulting in false negatives.49,50 However, recent research suggests that skin-penetrating sham needles can be used as inert placebo controls in randomized controlled trials.31,51,52 Given that patients have some history of acupuncture treatments, they expect certain sensations during the acupuncture procedure. Taking into account this and other relevant evidence, this study will utilize superficial needling with sham needles not inserted through meridians or acupoints.
Conclusion
The main purposes of this study are to investigate the abnormal functional connectivity patterns in the brain networks of KOA patients treated with acupuncture, and to identify potential central targets where acupuncture may improve chronic pain in KOA. Through this study, we aim to initially explore the correlation between chronic pain in KOA and abnormal connectivity patterns in brain functional networks. Based on this pattern, we hypothesize that there exist different central mechanisms of action for the short-term and long-term effects of acupuncture intervention. This study is guided by traditional acupuncture theory while incorporating modern medical imaging techniques, providing significant reference value for clinical studies on the effects of acupuncture analgesia.
Abbreviations
KOA, knee osteoarthritis; fMRI, functional magnetic resonance imaging; RCT, randomized controlled trials; fALFF, fractional amplitude of low-frequency fluctuation; PCC, posterior cingulate cortex; HC, healthy controls; TA, true acupuncture; SA, sham acupuncture; CONSORT, Consolidated Standards of Reporting Trials; STRICTA, Standards for Reporting Interventions in Clinical Trials of Acupuncture; SPIRIT, Standard Protocol Items: Recommendations for Intervention Trials; NRS, numerical rating scale; CRF, case report files; SAE, serious adverse event; EPI, echo planar imaging; TR, repetition time; TE, echo time; FOV, field of view; FA, flip angle; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; STAI, State-Trait Anxiety Inventory; ReHo, regional homogeneity; FC, functional connectivity; ICA, independent component analysis; AEs, Adverse Events; MRI, magnetic resonance imaging; IC, independent component.
Data Sharing Statement
The data obtained and analyzed in this study will be published in peer-reviewed international journals. If you need the original data, please contact the email: [email protected].
Ethics and Dissemination
This study has been approved by the ethics committee of the Affiliated Hospital of Shandong University of Traditional Chinese Medicine (Ethics Reference Number:(2024) Lunshen No. (028) - KY). Furthermore, the study was registered with the Chinese Clinical Trial Registry (ChiCTR2400083695). The researchers should provide explicit informed consent which has been authorized by the ethics committee and render subjects sufficient time to consider. Written informed consent will be obtained from every participant before study initiation.
Author Contributions
All authors contributed significantly to the work reported, whether in the study design, study supervision, data collection, analysis, neuroimaging, and statistical analyses, or in all of these areas; participated in drafting, modifying, or critically reviewing the the study protocol; gave final approval to the version to be published; and agreed to be accountable for all aspects of their work.
Funding
The study was supported by the National Natural Science Foundation of China Youth Fund (No: 82305406), Shandong University of Traditional Chinese Medicine Postdoctoral Program.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393:1745–1759. doi:10.1016/S0140-6736(19)30417-9
2. Roos EM, Arden NK. Strategies for the prevention of knee osteoarthritis. Nat Rev Rheumatol. 2016;12:92–101. doi:10.1038/nrrheum.2015.135
3. Loeser RF, Goldring SR, Scanzello CR, et al. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012;64(6):1697–1707. doi:10.1002/art.34453
4. Garcia J, Mennan C, McCarthy HS, et al. Chondrogenic potency analyses of donor-matched chondrocytes and mesenchymal stem cells derived from bone marrow, infrapatellar fat pad, and subcutaneous fat. Stem Cells Int. 2016;2016:6969726. doi:10.1155/2016/6969726
5. Felson DT, Lawrence RC, Dieppe PA, et al. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann Intern Med. 2000;133:635–646. doi:10.7326/0003-4819-133-8-200010170-00016
6. Blagojevic M, Jinks C, Jeffery A, et al. Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2010;18:24–33. doi:10.1016/j.joca.2009.08.010
7. Heidari B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: part I. Casp J Intern Med. 2011;2:205–212.
8. Giorgino R, Albano D, Fusco S, et al. Knee osteoarthritis: epidemiology, pathogenesis, and mesenchymal stem cells: what else is new? An update. Int J Mol Sci. 2023;24(7):6405. doi:10.3390/ijms24076405
9. Li D, Li S, Chen Q, et al. The prevalence of symptomatic knee osteoarthritis in relation to age, sex, area, region, and body mass index in China: a systematic review and meta-analysis. Front Med. 2020;7:304. doi:10.3389/fmed.2020.00304
10. Culliford D, Maskell J, Judge A, et al. Future projections of total hip and knee arthroplasty in the UK: results from the UK clinical practice research datalink. Osteoarthritis Cartilage. 2015;23(4):594–600. doi:10.1016/j.joca.2014.12.022
11. Liew JW, King LK, Mahmoudian A, et al. OARSI early osteoarthritis classification criteria task force. A scoping review of how early-stage knee osteoarthritis has been defined. Osteoarthritis Cartilage. 2023;31(9):1234–1241. doi:10.1016/j.joca.2023.04.015
12. Bijlsma JWJ, Berenbaum F, Lafeber FPJG. Osteoarthritis: an update with relevance for clinical practice. Lancet. 2011;377(9783):2115–2126. doi:10.1016/S0140-6736(11)60243-2
13. Buttgereit F, Burmester G-R, Bijlsma JWJ. Non-surgical management of knee osteoarthritis: where are we now and where do we need to go? RMD Open. 2015;1(1):e000027. doi:10.1136/rmdopen-2014-000027
14. Sharma L. Osteoarthritis of the Knee. N Engl J Med. 2021;384(1):51–59. doi:10.1056/NEJMcp1903768
15. Buchbinder R, Richards B, Harris I. Knee osteoarthritis and role for surgical intervention: lessons learned from randomized clinical trials and population-based cohorts. Curr Opin Rheumatol. 2014;26(2):138–144. doi:10.1097/BOR.0000000000000022
16. National Institute for Health and Care Excellence (NICE). Osteoarthritis in Over 16s: Diagnosis and Management. London: National Institute for Health and Care Excellence (NICE); 2022.
17. The Joint Surgery Group of the Orthopedics Branch of the Chinese Medical Association. Chinese guidelines for the diagnosis and treatment of osteoarthritis (2021 edition). Chin J Orthop. 2021;41(18):24.
18. Berman BM, Lao L, Langenberg P, et al. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med. 2004;141(12):901–910. doi:10.7326/0003-4819-141-12-200412210-00006
19. Witt C, Brinkhaus B, Jena S, et al. Acupuncture in patients with osteoarthritis of the knee: a randomised trial. Lancet. 2005;366(9480):136–143. doi:10.1016/S0140-6736(05)66871-7
20. Mavrommatis CI, Argyra E, Vadalouka A, et al. Acupuncture as an adjunctive therapy to pharmacological treatment in patients with chronic pain due to osteoarthritis of the knee: a 3-armed, randomized, placebo-controlled trial. Pain. 2012;153(8):1720–1726. doi:10.1016/j.pain.2012.05.005
21. Tu JF, Yang JW, Shi GX, et al. Efficacy of intensive acupuncture versus sham acupuncture in knee osteoarthritis: a randomized controlled trial. Arthritis Rheumatol. 2021;73(3):448–458. doi:10.1002/art.41584
22. Lin X, Huang K, Zhu G, et al. The effects of acupuncture on chronic knee pain due to osteoarthritis: a meta-analysis. J Bone Joint Surg Am. 2016;98(18):1578–1585. doi:10.2106/JBJS.15.00620
23. Baliki MN, Mansour AR, Baria AT, et al. Functional reorganization of the default mode network across chronic pain conditions. PLoS One. 2014;9(9):e106133. doi:10.1371/journal.pone.0106133
24. Pinto CB, Bielefeld J, Barroso J, et al. Chronic pain domains and their relationship to personality, abilities, and brain networks. Pain. 2023;164(1):59–71. doi:10.1097/j.pain.0000000000002657
25. Barroso J, Wakaizumi K, Reis AM, et al. Reorganization of functional brain network architecture in chronic osteoarthritis pain. Hum Brain Mapp. 2021;42(4):1206–1222. doi:10.1002/hbm.25287
26. Gao N, Shi H, Hu S, et al. Acupuncture enhances dorsal raphe functional connectivity in knee osteoarthritis with chronic pain. Front Neurol. 2022;12:813723. doi:10.3389/fneur.2021.813723
27. Chen X, Spaeth RB, Freeman SG, et al. The modulation effect of longitudinal acupuncture on resting state functional connectivity in knee osteoarthritis patients. Mol Pain. 2015;11:67. doi:10.1186/s12990-015-0071-9
28. Wang X, Li JL, Wei XY, et al. Psychological and neurological predictors of acupuncture effect in patients with chronic pain: a randomized controlled neuroimaging trial. Pain. 2023;164(7):1578–1592. doi:10.1097/j.pain.0000000000002859
29. American College of Rheumatology Subcommittee on Osteoarthritis Guidelines, Recommendations for the medical management of osteoarthritis of the Hip and knee: 2000 update. Arthritis Rheum. 2000;43(9):1905–1915. doi:10.1002/1529-0131(200009)43:9<1905::AID-ANR1>3.0.CO;2-P
30. Mumford JA, Nichols TE. Power calculation for group fMRI studies accounting for arbitrary design and temporal autocorrelation. Neuroimage. 2008;39(1):261–268. doi:10.1016/j.neuroimage.2007.07.061
31. Jia J, Yan C, Zheng X, et al. Central mechanism of acupuncture treatment in patients with migraine: study protocol for randomized controlled neuroimaging trial. J Pain Res. 2023;16:129–140. doi:10.2147/JPR.S377289
32. Sun N, Wang LQ, Shao JK, et al. An expert consensus to standardize acupuncture treatment for knee osteoarthritis. Acupunct Med. 2020;38(5):327–334. doi:10.1177/0964528419900789
33. Zhao JS. [Research and identification of the concept and terminology of “tender-point” and “Ashi-point”]. Zhen Ci Yan Jiu. 2010;35(5):388–390. Chinese.
34. Zhao L, Chen J, Li Y, et al. The long-term effect of acupuncture for migraine prophylaxis: a randomized clinical trial. JAMA Intern Med. 2017;177(4):508–515. doi:10.1001/jamainternmed.2016.9378
35. Hawker GA, Mian S, Kendzerska T, et al. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(Suppl 11):S240–52. doi:10.1002/acr.20543
36. Liang D, Guo X, Zhang J, et al. Pain characteristics of patients with fibromyalgia: a comparison between gender and different emotional states. Pain Physician. 2024;27(1):E109–E118. doi:10.36076/ppj.2024.27.E109
37. Li D, Hang R, Meng L, et al. Co-treatment with oral duloxetine and intraarticular injection of corticosteroid plus hyaluronic acid reduces pain in the treatment of knee osteoarthritis. Pain Physician. 2024;27(1):E45–E53. doi:10.36076/ppj.2024.27.E45
38. Rodríguez-Aragón M, Barranco-Rodríguez D, de Mora-Martín M, et al. The effects of global postural re-education on sleep quality and stress in university women lecturers: a randomized controlled trial. Front Psychiatry. 2024;14:1321588. doi:10.3389/fpsyt.2023.1321588
39. Guillén-Riquelme A, Buela-Casal G. Metaanálisis de comparación de grupos y metaanálisis de generalización de la fiabilidad del cuestionario State-Trait Anxiety Inventory (STAI) [Meta-analysis of group comparison and meta-analysis of reliability generalization of the State-Trait Anxiety Inventory Questionnaire (STAI)]. Rev Esp Salud Publica. 2014;88(1):101–112. Spanish. doi:10.4321/S1135-57272014000100007
40. Song Y, Xu W, Chen S, et al. Functional MRI-specific alterations in salience network in mild cognitive impairment: an ALE meta-analysis. Front Aging Neurosci. 2021;13:695210. doi:10.3389/fnagi.2021.695210
41. Xiang Y, Xing X, Hua X, et al. Resting-state brain network remodeling after different nerve reconstruction surgeries: a functional magnetic resonance imaging study in brachial plexus injury rats. Neural Regen Res. 2025;20(5):1495–1504. doi:10.4103/NRR.NRR-D-23-00493
42. Tonge DP, Pearson MJ, Jones SW. The hallmarks of osteoarthritis and the potential to develop personalised disease-modifying pharmacological therapeutics. Osteoarthritis Cartilage. 2014;22(5):609–621. doi:10.1016/j.joca.2014.03.004
43. Wang H, Yang G, Wang S, et al. The most commonly treated acupuncture indications in the United States: a cross-sectional study. Am J Chin Med. 2018:1–33. doi:10.1142/S0192415X18500738
44. Sun R, Yang Y, Li Z, et al. Connectomics: a new direction in research to understand the mechanism of acupuncture. Evid Based Complement Alternat Med. 2014;2014:568429. doi:10.1155/2014/568429
45. Fonseca-Rodrigues D, Rodrigues A, Martins T, et al. Correlation between pain severity and levels of anxiety and depression in osteoarthritis patients: a systematic review and meta-analysis. Rheumatology. 2021;61(1): 53–75. doi:10.1093/rheumatology/keab512
46. Sugai K, Takeda-Imai F, Michikawa T, et al. Association between knee pain, impaired function, and development of depressive symptoms. J Am Geriatr Soc. 2018;66(3):570–576. doi:10.1111/jgs.15259
47. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
48. Paterson C, Britten N. Acupuncture as a complex intervention: a holistic model. J Altern Complement Med. 2004;10(5):791–801. doi:10.1089/acm.2004.10.791
49. Vase L, Baram S, Takakura N, et al. Can acupuncture treatment be double-blinded? An evaluation of double-blind acupuncture treatment of postoperative pain. PLoS One. 2015;10(3):e0119612. doi:10.1371/journal.pone.0119612
50. Lund I, Näslund J, Lundeberg T. Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist’s perspective. Chin Med. 2009;4:1. doi:10.1186/1749-8546-4-1
51. Liu L, Lyu TL, Fu MY, et al. Changes in brain connectivity linked to multisensory processing of pain modulation in migraine with acupuncture treatment. Neuroimage Clin. 2022;36:103168. doi:10.1016/j.nicl.2022.103168
52. Zhang Y, Wang Z, Du J, et al. Regulatory effects of acupuncture on emotional disorders in patients with menstrual migraine without aura: a resting-state fMRI study. Front Neurosci. 2021;15:726505. doi:10.3389/fnins.2021.726505
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture for Pain and Function in Patients with Nonspecific Low Back Pain: Study Protocol for an Up-to-Date Systematic Review and Meta-Analysis
Li Y, Liu Y, Zhang L, Zhai M, Li L, Yuan S, Li Y
Journal of Pain Research 2022, 15:1379-1387
Published Date: 10 May 2022
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
The Effectiveness of Pharmacopuncture in Patients with Lumbar Spinal Stenosis: A Protocol for a Multi-Centered, Pragmatic, Randomized, Controlled, Parallel Group Study
Lee JY, Park KS, Kim S, Seo JY, Cho HW, Nam D, Park Y, Kim EJ, Lee YJ, Ha IH
Journal of Pain Research 2022, 15:2989-2996
Published Date: 23 September 2022
Central Mechanism of Acupuncture Treatment in Patients with Migraine: Study Protocol for Randomized Controlled Neuroimaging Trial
Jia J, Yan C, Zheng X, Shi A, Li Z, Xu L, Hui Z, Chen Y, Cao Z, Wang J
Journal of Pain Research 2023, 16:129-140
Published Date: 18 January 2023