")
Back to Journals » Drug Design, Development and Therapy » Volume 19
The Efficacy of Sodium Bicarbonate Ringer’s Solution and Lactate Ringer’s Solution in Patients Undergoing Long-Term Abdominal Open Surgery: A Multicenter Prospective Randomized Controlled Study
Authors Zhou S, Zhao K , Liu C, Luo H , Shi J, Liu C, Li X, Gao F, Wu X, Shen Q, Yuan W, Chai X, Wei X
Received 28 December 2024
Accepted for publication 28 May 2025
Published 1 June 2025 Volume 2025:19 Pages 4617—4628
DOI https://doi.org/10.2147/DDDT.S514725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Susu Zhou,1,2 Kai Zhao,1,2 Chunmei Liu,1,2 Hong Luo,3 Jun Shi,4 Chunhong Liu,5 Xiaoming Li,6 Fang Gao,7 Xiangnan Wu,8 Qin Shen,9 Wenhua Yuan,10 Xiaoqing Chai,1,2,* Xin Wei1,2,*
1Department of Anesthesiology, the First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China (USTC), Hefei, Anhui, People’s Republic of China; 2Department of Anesthesiology, Anhui Provincial Hospital, Hefei, Anhui, People’s Republic of China; 3Department of Anesthesiology, Hefei First People’s Hospital, Hefei, Anhui, People’s Republic of China; 4Department of Anesthesiology, the First Hospital of Anhui University of Science and Technology, Huainan, Anhui, People’s Republic of China; 5Department of Anesthesiology, Huainan Chaoyang Hospital, Huainan, Anhui, People’s Republic of China; 6Department of Anesthesiology, Affiliated Hospital of West Anhui Health Vocational College, Luan, Anhui, People’s Republic of China; 7Department of Anesthesiology, Bozhou People’s Hospital, Bozhou, Anhui, People’s Republic of China; 8Department of Anesthesiology, Anqing 116 hospital, Anqing, Anhui, People’s Republic of China; 9Department of Anesthesiology, Huainan Xinhua Hospital, Huainan, Anhui, People’s Republic of China; 10Department of Anesthesiology, General Hospital of Benxi iron and Steel Industry Group of Liaoning Health Industry Group, Benxi, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoqing Chai; Xin Wei, Department of Anesthesiology, The First Affiliated Hospital of USTC (Anhui Provincial Hospital), Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China, Tel +8613805518889; +86 13956975101, Email [email protected]; [email protected]
Purpose: Sodium bicarbonate Ringer’s solution (BRS) is an intravenous fluid that does not rely on hepatic or renal metabolism. It contains bicarbonate ions (HCO3−) and lacks lactate ions. This study hypothesizes that BRS is more effective in maintaining acid-base balance during prolonged open abdominal surgeries. The aim is to investigate the effects of sodium bicarbonate Ringer’s solution on lactate metabolism, acid-base balance, and clinical outcomes in patients undergoing extended-duration open abdominal surgery, with the objective of refining fluid replacement strategies for this patient population.
Patients and Methods: A multicenter randomized controlled trial was conducted involving 112 patients undergoing open abdominal surgery. Participants were randomly assigned to either the BRS group (n=55) or the lactated Ringer’s solution (LRS) group (n=57). The primary outcome was the incidence of postoperative hyperlactacidemia, while secondary outcomes included serum lactate (Lac), pH, base excess (BE), buffered base (BB), bicarbonate (HCO3−), blood glucose (Glu), electrolytes, postoperative liver and kidney function, and postoperative complications. Linear regression analysis was performed to identify factors influencing lactate concentration.
Results: The incidence of hyperlactic acidemia was lower in Group A compared to Group B (9.1% vs 19.3%, P = 0.177), although the difference did not reach statistical significance. No significant differences were observed in lactate (Lac), pH, base excess (BE), bicarbonate (BB), HCO₃⁻, glucose (Glu), or electrolytes between the two groups at any time point (Ptime < 0.001, Pgroup > 0.05, Ptime * group > 0.05). Linear regression analysis revealed that diabetes, hypotension and blood loss were significant factors influencing blood lactate concentration (R² = 0.349, P < 0.001).
Conclusion: Sodium bicarbonate Ringer’s solution and lactate Ringer’s solution are both safe options for fluid replacement during long-term open abdominal surgeries. There is no significant difference observed in perioperative lactate levels, acid-base balance, or clinical postoperative outcomes between the two solutions.
Keywords: sodium bicarbonate Ringer’s solution, lactate Ringer’s solution, open abdominal surgery, lactate levels
Introduction
Long-term open abdominal surgery results in significant trauma, substantial blood loss, prolonged exposure of the abdominal cavity, and considerable fluid inflow and outflow, which can easily lead to inadequate perfusion of tissues and organs. This is attributed to factors such as stringent intestinal preparation, anesthesia-induced vasodilation, inflammation-related capillary leakage, and intraoperative fluid loss.1 Consequently, patients are more susceptible to acid-base and electrolyte imbalances, with a risk of metabolic acidosis and hyperlactacidemia. Previous studies have reported that the incidence of postoperative hyperlactacidemia in patients undergoing major abdominal surgery ranges from 22.7% to 61.9%.2–5 The accumulation of lactate can lead to complications such as hypotension, inflammation, acid-base imbalance, and organ dysfunction.6 Therefore, effective fluid therapy and control of lactate concentration are crucial for patients undergoing prolonged abdominal open surgery.
Currently, research on ideal equilibrium crystal solutions in China is ongoing. Lactate Ringer’s solution (LRS) is the most commonly used equilibrium solution. However, prolonged and continuous infusion of large volumes of LRS has notable disadvantages, including increased lactate levels, acid-base imbalances, and electrolyte disturbances. It has been demonstrated to exacerbate intrinsic lactic acidosis and elevate aerobic demand.7,8 Sodium bicarbonate Ringer’s solution (BRS) is an innovative crystalline solution that closely resembles human plasma in its composition. It has a pH value and electrolyte content that align more closely with physiological levels, facilitates faster bicarbonate metabolism, and requires less oxygen and liver metabolism.9 Recent studies indicate that BRS is more effective in stabilizing the internal environment, reducing lactate concentrations, correcting acidosis, and decreasing the incidence of complications in patients experiencing shock.10–13
Currently, there is a notable absence of systematic research regarding the application of Balanced Ringer’s Solution (BRS) in patients undergoing prolonged open abdominal surgery. Consequently, we initiated a multicenter, prospective randomized controlled study aimed at comparing the efficacy of BRS with Lactated Ringer’s Solution (LRS) in this patient population.
Materials and Methods
This study is a prospective, multicenter, randomized controlled trial that adheres to the ethical standards outlined in the Helsinki Declaration and the CONSORT reporting guidelines. It has been approved by the Medical Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (Approval Number: 2019-KY-164) and is registered on ClinicalTrials.gov (ChiCTR2000030634). The study is centered on the medical treatment provided by the First Affiliated Hospital of the University of Science and Technology of China, along with eight additional institutions: Hefei First People’s Hospital, The First Hospital of Anhui University of Science and Technology, Huainan Chaoyang Hospital, the Affiliated Hospital of West Anhui Health Vocational College, Bozhou People’s Hospital, Anqing 116 hospital, Huainan Xinhua Hospital, and the General Hospital of Benxi Iron & Steel Industry Group of Liaoning Health Industry Group. Together, these nine hospitals form a multicenter research team.
Patients
Patients aged 18 to 80 years, classified as American Society of Anesthesiologists (ASA) grades I–III, who are undergoing elective open abdominal surgery with an estimated surgical duration exceeding three hours, including radical surgeries for gastrointestinal tumors, pancreaticoduodenectomy for pancreatic masses, hilar cholangiocarcinoma, gallbladder cancer, partial hepatectomy, gallstone surgery, and gynecological open abdominal surgeries for cervical, ovarian, and uterine diseases, were included in this study. All participants provided written informed consent prior to enrollment. Exclusion criteria: Patients with significant arrhythmias, severe heart disease (including moderate to severe heart valve disease, atrial fibrillation, and various arrhythmias necessitating pacemaker installation), severe cardiac dysfunction, liver dysfunction (Child-Pugh grades B and C), renal failure, severe functional impairment of the lungs and other organs, preoperative mental illness, hypermagnesemia, hypothyroidism, and those requiring emergency surgery are excluded from this study. Additionally, patients with incomplete data will also be excluded.
Randomization and Blinding
All enrolled patients were randomly assigned in a 1:1 ratio to either Sodium Bicarbonate Ringer’s Solution (Group A) or Lactated Ringer’s Solution (Group B) through computer-generated randomization. Sealed envelopes containing the designated patient numbers were opened on the day of surgery. A total of 188 patients were screened, and 134 were enrolled. Data were missing for 22 cases (4 lost to follow-up, with 2 in each group; and 18 cases with missing data during photo identification and data upload, including 10 in Group A and 8 in Group B). Ultimately, data from 112 patients were analyzed, comprising 55 in Group A and 57 in Group B. Due to the different packaging of Bicarbonate Ringer’s Solution (BRS) and Lactated Ringer’s Solution (LRS), although the anesthesiologists were unaware of the group assignments beforehand, they were cognizant of the infusion solutions. The personnel responsible for postoperative follow-up, data collection, and statistical analysis were blinded to the group assignments. Intraoperative and postoperative data were collected by medical students who were not involved in the trial.
Anesthetic Management and Intraoperative Fluid Replacement Plan
All patients should fast for at least 8 hours prior to surgery and complete the necessary preoperative preparations. A venous channel should be established, and an 18-G venous catheter must be inserted before entering the operating room. Standardized monitoring should include pulse oximetry (SpO2), electrocardiogram, invasive blood pressure, and the bispectral index (BIS) as provided by Aspect Medical Systems, Inc., United States. After preoxygenation, intravenous administration of midazolam (0.05 mg/kg), etomidate (0.3 mg/kg), sufentanil (0.5 µg/kg), and rocuronium bromide (0.9 mg/kg) was performed for induction. Anesthesia was maintained with propofol, remifentanil, and sevoflurane at concentrations ranging from 0.4% to 1.5%. The intraoperative BIS was maintained between 40 and 60. Mechanical ventilation parameters were set to maintain end-tidal carbon dioxide (PetCO2) close to 40 mmHg, with a tidal volume of 6 to 8 mL·kg−1. Nasopharyngeal temperature was monitored to ensure normal body temperature (core temperature > 36°C). Right internal jugular vein deep vein catheterization was performed, with intravenous infusion administered at a rate of 6 to 15 mL·kg−1·h−1, adjusted according to the patient’s volume status to maintain central venous pressure (CVP) between 5 and 12 mmHg. The intraoperative fluid replacement plan involved Group A receiving BRS (H20190021, specification 500 mL; Jiangsu Hengrui Pharmaceutical, China), while Group B received LRS (H20065323, specification 500 mL; Sichuan Pacific Pharmaceutical, China), based on randomization. Throughout the surgical procedure, the patient received a baseline infusion rate of 2 mL·kg−1·h−1. According to Robinson’s formula,14 the ideal body weight for fluid administration is defined as follows: males: 52 kg + 1.9 kg for every 2.5 cm above 150 cm, and females: 49 kg + 1.7 kg for every 2.5 cm above 150 cm. The total infusion volume for both groups should not exceed 15 mL·kg−1, with an infusion rate of 6 to 10 mL·kg−1·h−1. The infusion rate should be adjusted as necessary based on age, ideal body weight, and individual patient differences. The total infusion volume for both groups should not exceed 15 mL·kg−1, and the infusion rate should be maintained between 6 and 10 mL·kg−1·h−1. This rate should be adjusted as necessary based on the patient’s age, ideal body weight, and individual differences. In cases of hypotension, defined as a mean arterial pressure dropping below 65 mmHg within five minutes, intermittent administration of ephedrine or norepinephrine, or continuous administration of norepinephrine, is recommended. If the bleeding volume exceeds 800 mL, artificial colloids (hydroxyethyl starch 130/0.4 sodium chloride injection, 500 mL specification; manufactured by Fresenius Kabi, Germany, J20090065) should be supplemented in a 1:1 ratio according to the bleeding volume, ensuring the total volume remains below 1000 mL. According to the Chinese guidelines for perioperative patient blood management, “Whole Blood Transfusion and Blood Composition” WS/T 623–2018, when the hemoglobin level falls below 70 g/L, red blood cells should be infused to maintain a hemoglobin level of at least 70 g/L, and albumin should be administered if the albumin level is below 30 g/L. Postoperatively, all patients received Lactated Ringer’s Solution (LRS) as the maintenance fluid.
Result Measurement and Data Collection
The primary outcome of this study is the incidence of postoperative hyperlactacidemia. Hyperlactacidemia is typically defined as an arterial blood lactate concentration exceeding 2.0 mmol/L. Moderate hyperlactacidemia is characterized by a lactate concentration ranging from 2 to 5 mmol/L, while a lactate concentration greater than 5 mmol/L is classified as severe hyperlactacidemia.15
The secondary outcomes included changes in lactate (Lac), base excess (BE), beta-hydroxybutyrate (BB), pH, bicarbonate (HCO3−), and glucose (Glu) concentrations at each time point. Additionally, alterations in serum ion concentrations of potassium (K+), sodium (Na+), chloride (Cl−), and calcium (Ca2+) were assessed at various time intervals. Exploratory indicators consisted of liver and kidney function parameters on the first postoperative day, including albumin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TBIL), serum creatinine (SCr), and blood urea nitrogen (BUN). Safety indicators encompassed both intraoperative and postoperative complications.
Using various blood gas analyzers, including the Roche cobasb 123 (20,172,407,195), GEM 3500 (National Medical Equipment Administration: 20182221750), Radurei ABL90 (National Medical Equipment Administration: 2019221680), Shenzhen Libang (Guangdong Medical Equipment Administration: 20162220822), and Siemens Rapidlab 1200 (Food and Drug Administration: 20192213001), arterial blood was collected for gas analysis at multiple time points. Parameters measured included lactate (Lac), pH, base excess (BE), base bicarbonate (BB), bicarbonate (HCO3−), glucose (Glu), and electrolytes (K+, Na+, Cl−, Ca2+). These measurements were taken before liquid therapy (T0), surgery 1 hour (T1), at the end of surgery (T2), and 1 hour after surgery (T3). Intraoperative data recorded comprised infusion volume, bleeding volume, and urine volume; the proportion of intraoperative blood transfusions; administration of antihypertensive drugs; and use of vasopressors. The incidence of delayed postoperative recovery and the need for postoperative transfer to the ICU were also documented. On the first postoperative day, biochemical indicators were collected, including albumin, total bilirubin (TBIL), alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum creatinine (SCr), and blood urea nitrogen (BUN). During the follow-up period, clinical symptoms, examination reports, and medical records were collected for patients at 3 and 7 days post-surgery, with data summarized based on the surgeon’s report to diagnose postoperative complications. The incidence of postoperative hypotension, arrhythmia, pulmonary infection, myocardial infarction, and cerebral infarction was recorded.
Statistical Analysis
The sample size was calculated using PASS 11.0 (NCS-PASS 11), focusing on the comparison of randomized controlled rates to determine the required sample size. The incidence of postoperative hyperlactacidemia in patients undergoing abdominal open surgery with LRS fluid therapy ranged from 22.7% to 61.9%.2–5 Following fluid therapy, the incidence of hyperlactacidemia was observed to be 3.3% in the BRS group compared to 40.0% in the LRS group. 16 Our pre-trial results, derived from a pilot study conducted at the First Affiliated Hospital of USTC, involved 13 patients who met the composite inclusion criteria, of whom 1 developed hyperlactacidemia. This indicated an incidence of approximately 8% after BRS fluid therapy. Consequently, we estimated a sample size of 94 patients, with 47 in each group. The test power (1-β) was set at 90%, and the two-sided α level was established at 0.05. To account for a 15% dropout rate due to patient withdrawal, exclusion, and loss to follow-up, we determined that 54 patients were required in each group. Ultimately, a total of 188 patients were recruited for this study, with 134 included in the analysis, 4 lost to follow-up, and 18 cases of data loss. Data from 112 patients were ultimately analyzed, consisting of Group A (55 cases) and Group B (57 cases).
The analysis was conducted using SPSS version 25.0 statistical software. The final analysis included only participants who were randomly assigned and received all study interventions. The Shapiro–Wilk test was employed to assess the normality of continuous data. For normally distributed continuous variables, data are expressed as mean ± standard deviation (X ± S), with independent sample t-tests utilized for comparisons between two groups. Repeated measures analysis of variance was applied for comparisons at multiple time points between the two groups. Non-normally distributed continuous variables are represented by median and interquartile range, with comparisons between two groups conducted using the Mann–Whitney U-test. Categorical variables between two groups were compared using either the Pearson chi-square test or Fisher’s exact method. The relationship between lactate concentration and various independent variables was examined using both single-factor and multiple-factor linear regression analysis methods. All tests were two-sided, and a p-value of less than 0.05 was considered indicative of statistical significance. GraphPad Prism 9.0 (GraphPad Software, La Jolla, California, USA) was utilized for graphic construction.
Result
The study initially enrolled a total of 188 patients. Of these, 30 did not meet the inclusion criteria, 16 declined participation, and 8 withdrew for other reasons, resulting in 134 patients who were randomized. Subsequently, 22 patients were excluded from the final analysis: 4 were lost to follow-up, and 18 had incomplete data. Ultimately, 112 patients were included in the analysis, with 55 in Group A (BRS, Sodium Bicarbonate Ringer’s Solution) and 57 in Group B (LRS, Lactate Ringer’s Solution) (Figure 1).
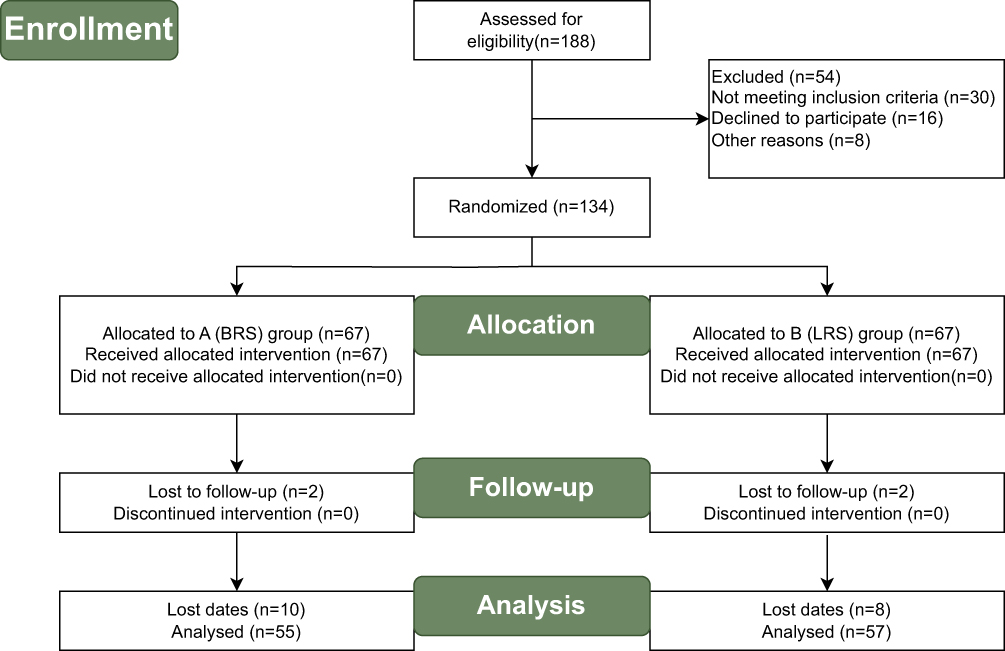 |
Figure 1 Flow Diagram of the Study. |
Baseline Characteristics and Surgical Data
There were no statistically significant differences in baseline characteristics and surgical data between the two groups (Table 1).
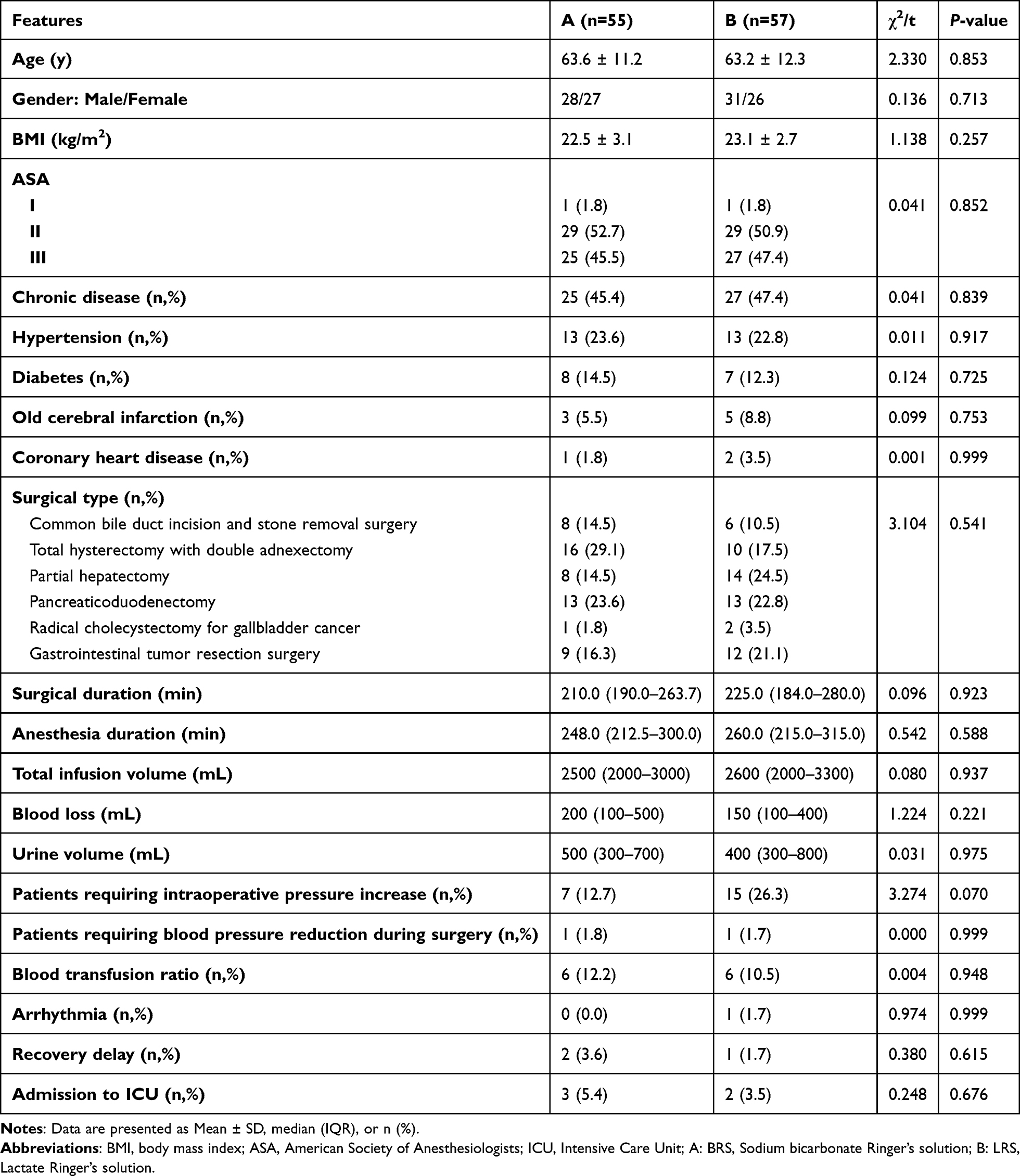 |
Table 1 Baseline Characteristics and Surgical Data |
Study Endpoints
The duration of surgery and anesthesia was comparable between the two groups, with no differences observed in fluid replacement, blood loss, urine output, the use of vasoactive drugs, blood component infusion, incidence of intraoperative center failure, delayed recovery, or postoperative ICU evacuation between the groups (P > 0.05) (Table 1).
Incidence of Postoperative hyperlactacidemia: Prior to fluid therapy, there was no statistically significant difference in lactate concentration between the two groups (Figure 2). Following fluid infusion, lactate concentration increased in Group B, whereas the increase in Group A was delayed and gradual. The incidence of hyperlactacidemia at the conclusion of surgery was 9.1% (5/55) in Group A and 19.3% (11/57) in Group B (P = 0.177, Table 2). Furthermore, hyperlactacidemia in both groups was predominantly moderate, with one instance of severe hyperlactacidemia observed in Group B. No statistically significant differences were found in lactate, pH, base excess (BE), bicarbonate (HCO3−), and glucose (Glu) levels between the two groups at any time point (Figure 2). Similarly, there were no statistically significant differences in electrolyte levels (K+, Na+, Cl−, Ca2+) between the two groups at any time point (Table 3).
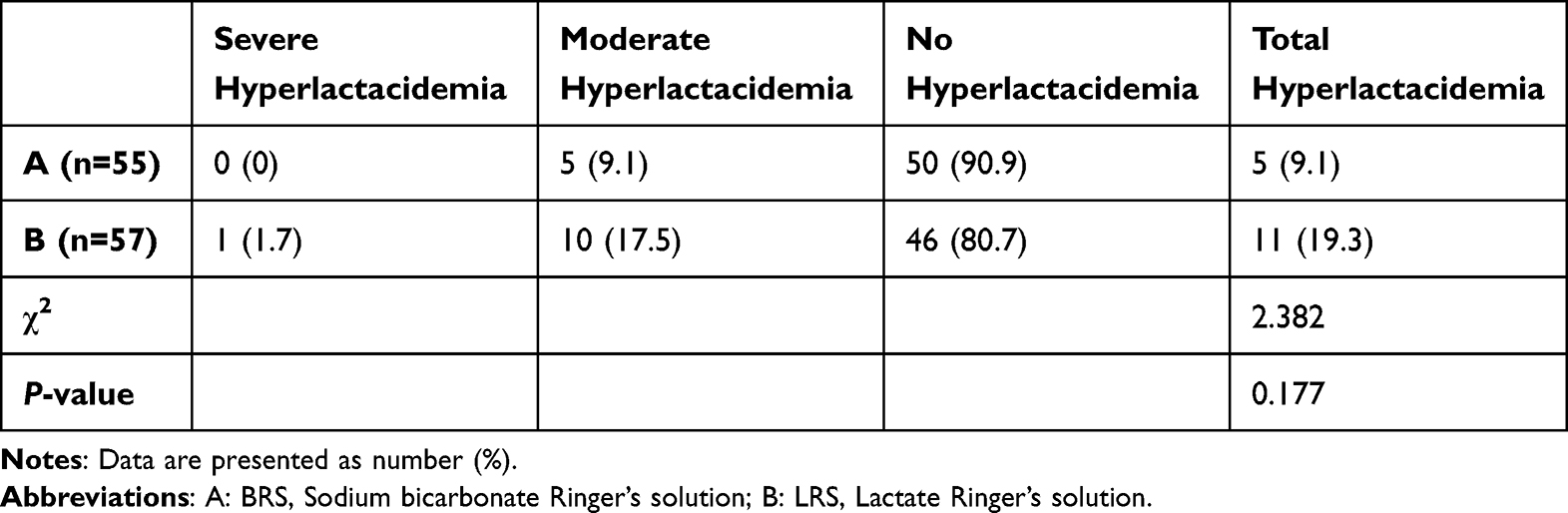 |
Table 2 Comparison of Postoperative Hyperlactic Acidosis Between Two Groups |
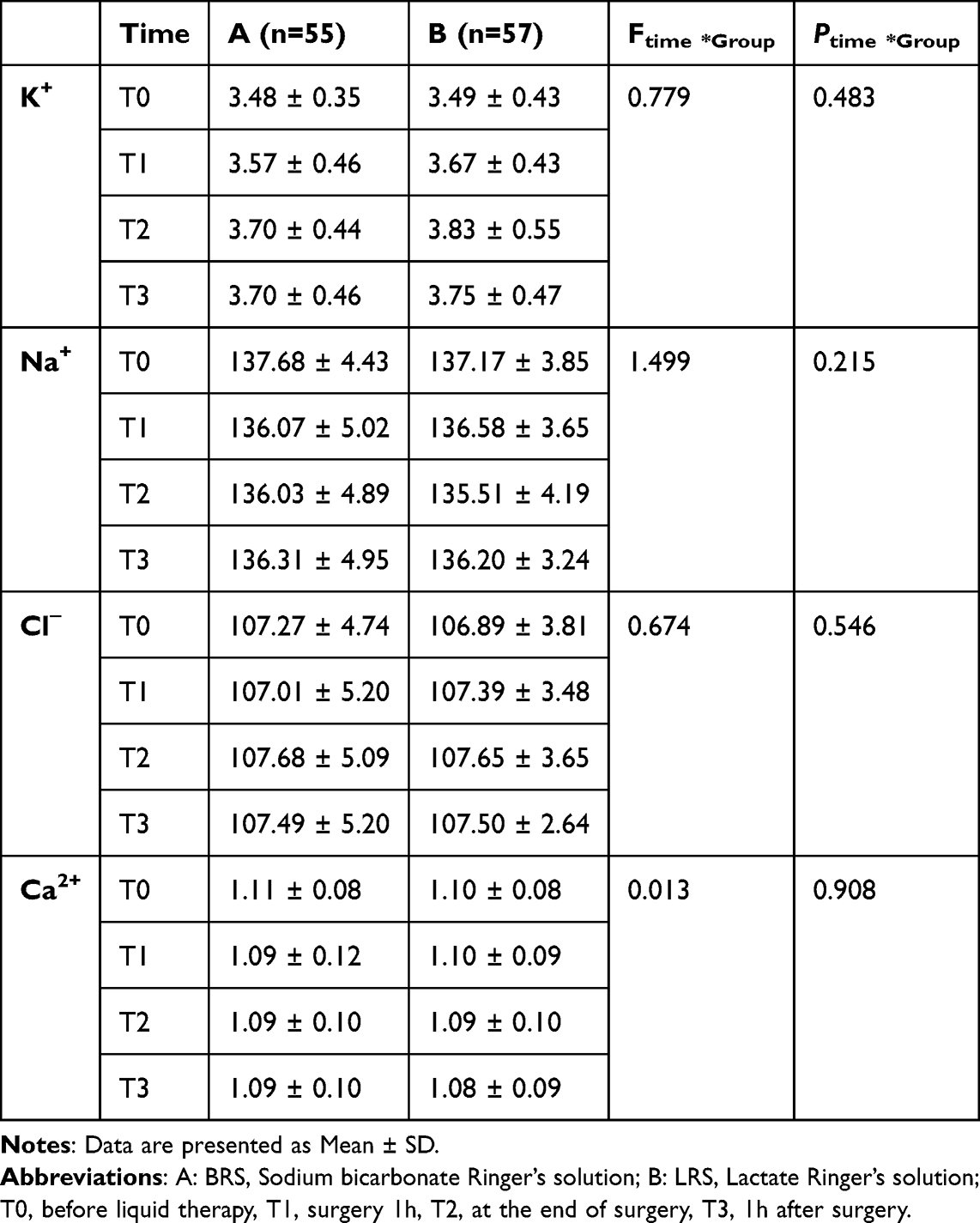 |
Table 3 Electrolytes (K+, Na+, Cl−, Ca2+) at Each Time Point of the Two Groups |
 |
Figure 2 Comparison of Lac, pH, BE, BB, HCO3−, and Glu Between Two Groups of Patients at Different Time Points. Abbreviations: BRS, Sodium bicarbonate Ringer’s solution; LRS, Lactate Ringer’s solution; Lac, lactate; BE, alkaline residue; BB, buffer base; HCO3−, bicarbonate; Glu, blood glucose. Notes: Data are presented as mean ± SD, (A) BRS; (B) LRS; T0: before liquid therapy, T1: surgery 1h, T2: at the end of surgery, T3: 1h after surgery. |
There was no statistically significant difference in biochemical indicators between the two groups 24 hours post-surgery (P > 0.05) (Table 4).
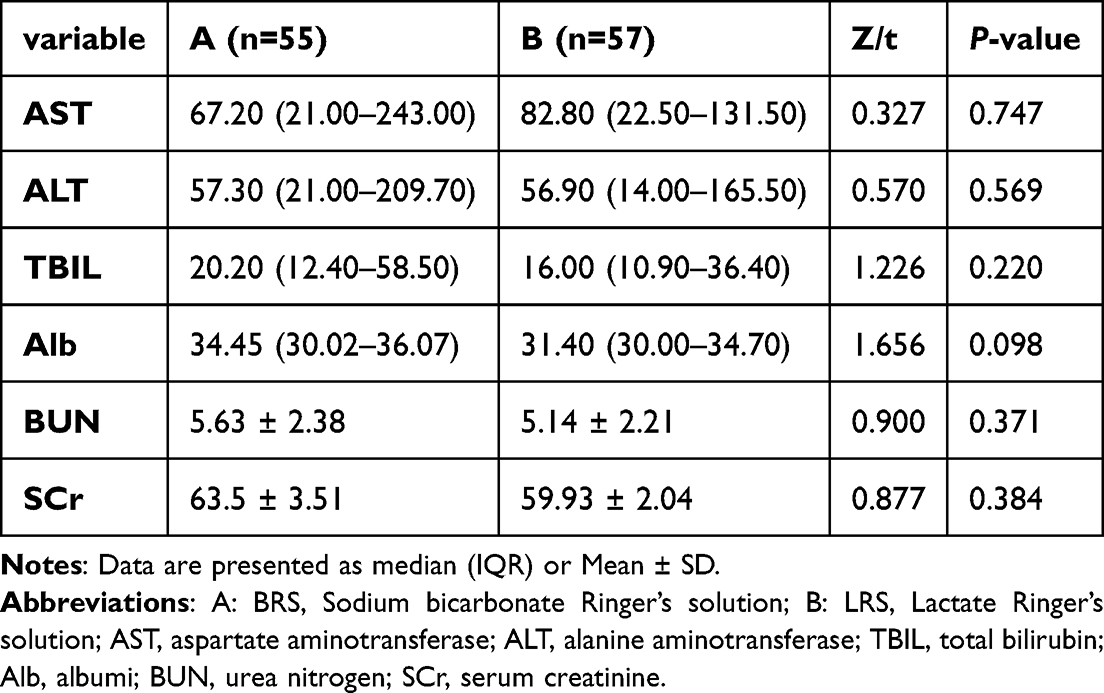 |
Table 4 Biochemical (Liver and Kidney Function) Indicators 24 hours After Surgery |
Additionally, there were no statistically significant differences in the incidence of related complications between the 3-day and 7-day follow-ups after surgery (Table S1, Supplementary). The results of the univariate linear regression analysis and the adjusted multivariate linear regression analysis of lactate concentration are presented in Supplementary (Table S2). Factors such as diabetes, intraoperative hypotension, and bleeding volume were found to affect blood lactate concentration (R²= 0.349, P < 0.001).
Discussion
Our findings indicate that BRS, when utilized as a crystalloid solution for fluid replacement during prolonged open abdominal surgery, resulted in a slower increase in lactate concentration compared to LRS. Additionally, BRS demonstrated a more gradual decrease in base excess (BE) and exhibited smaller fluctuations in pH values. However, these differences were not clinically significant. The incidence of hyperlactacidemia associated with LRS infusion was generally consistent with trends reported in previous studies, albeit slightly lower.16 Given that the carrier fluid was switched to LRS at the conclusion of the surgery and was not maintained for up to three days postoperatively or longer, we observed no significant differences in clinical outcomes between the two groups from one hour post-surgery through the recovery period. We plan to address this issue in future experimental design. Previous studies have reported statistical differences indicating that Balanced Ringer’s Solution (BRS) can reduce the incidence of metabolic acidosis during laparoscopic right hemihepatectomy and can slow the rate of lactate elevation during the early postoperative period.17 The pH and absolute base excess (BE) values of BRS undergo significant changes during liver reperfusion and immediately following liver transplantation reperfusion, necessitating a reduction in the infusion volume of 5% sodium bicarbonate.18 Compared to normal saline, sodium bicarbonate Ringer’s solution demonstrates a potential protective effect on renal function.12 Furthermore, early resuscitation in patients experiencing hemorrhagic shock can enhance coagulation function and blood gas analysis indicators affected by trauma, thereby better maintaining acid-base balance and hemodynamic stability, ultimately improving patient prognosis.19,20 Consequently, based on the aforementioned research findings, BRS may offer greater benefits for critically ill patients with liver and kidney impairment, such as those undergoing partial hepatic resection, liver transplantation, and experiencing shock.
However, considering lactate solely as a product of anaerobic metabolism does not fully align with reality. Even under fully aerobic conditions, our cells produce and utilize lactate in significant quantities. Lactate itself does not promote acidosis; it is non-toxic and serves as an important energy source.21 Some authors suggest that the lungs are one of the primary producers of lactate,22,23 while the release of lactate from internal organs is minimal.24 Currently, the goal is not to normalize lactate concentration but to interrupt the pathological processes that lead to its increase.21 This study, through general linear regression, identified that preoperative diabetes, intraoperative hypotension, and blood loss were factors influencing blood lactate concentration. The type of infusion fluid, whether BRS or LRS, and the total volume of fluid administered did not have a statistically significant impact on blood lactate outcomes. Therefore, it is more critical to avoid increasing exogenous lactate during the perioperative period.
Hepatic urea synthesis serves as the primary pathway for bicarbonate removal, with 70% of lactate metabolism occurring in the liver. This process participates in gluconeogenesis and the tricarboxylic acid cycle while generating HCO3−. For every 100g of protein metabolized, 1 mol of NH4+ is produced, and the metabolism of NH4+ consumes an equivalent amount of strong base HCO3−, which is then converted into urea and excreted by the kidneys.25 The extracellular acid-base status exerts sensitive and complex control over bicarbonate through hepatic urea production, establishing a feedback loop between acid-base status and the rate of bicarbonate elimination, known as the hepatic bicarbonate-homeostatic response.26 The kidneys utilize lactate via renal cortical uptake, rather than merely excreting it in urine, thereby playing a significant role in regulating acid-base balance.27,28 This study included patients with essentially normal liver and kidney functions; therefore, BRS did not demonstrate a significant advantage in improving acid-base balance during prolonged open abdominal surgery, and no clinically significant statistical differences were observed in lactate, HCO3−, pH, BE, BB, and Glu.
On the first postoperative day, the levels of ALT and AST were elevated in both patient groups, which may be related to the types of surgeries included in the study. Patients with intrahepatic and extrahepatic bile duct stones, partial hepatectomy, and pancreatic space-occupying lesions inevitably experienced liver tissue damage during the surgical procedures. The postoperative increase in transaminase levels may be attributed to various factors, including surgical stress, liver function impairment, and biliary tract injury.29 This study involved randomized grouping from various sub-centers, but detailed records of the surgical categories at each sub-center were not maintained. Only the liver and kidney function indicators on the first postoperative day were obtained, and there was no continuous monitoring on the 3rd and 7th postoperative days. In future clinical studies, it would be more insightful to compare surgical categories and patients with abnormal liver function (eg, Child-Pugh classification > B) and to conduct continuous monitoring of postoperative recovery indicators. This approach may better demonstrate the advantages of BRS in major surgeries for patients with abnormal liver function.
The ideal balanced crystalloid solution is isotonic, ensuring it can be well tolerated for peripheral administration while causing minimal disturbance to pH and tonicity. The emergence of the Stewart approach has provided a deeper understanding of the important design characteristics of ‘balanced’ crystalloids from the perspective of acid-base balance.30 BRS has a pH range of 6.8 to 7.8 and an osmolarity of 276 mOsm/L, featuring a HCO3− buffering system that can promptly correct acidosis. The reaction HCO3− + H+ → CO2 + H2O primarily facilitates respiratory excretion without increasing the burden on the liver and kidneys. Therefore, BRS appears to better meet the criteria of an ideal crystalloid solution compared to LRS.
Conclusion
However, there was no statistically significant difference between the two groups in this study. Both BRS and LRS, when applied to major open abdominal surgeries, showed no differences in perioperative lactate levels, acid-base balance, or clinical postoperative outcomes. Both can effectively maintain hemodynamic stability and are safe fluid choices. Under the principle of not increasing exogenous lactate, BRS can also be considered as a viable option for fluid therapy.
Data Sharing Statement
The individual participants’ data underlying the results reported in this article may be accessed with approval from the corresponding author six months after the publication of this study. Additionally, the study protocol, statistical analysis plan, and clinical study report will also be made available.
Acknowledgments
All authors appreciate the support from the relevant medical staff of the First Affiliated Hospital of USTC (Anhui Provincial Hospital) and other 8 hospitals.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bamboat ZM, Bordeianou L. Perioperative fluid management. Clin Colon Rectal Surg. 2009;22(1):28–33. doi:10.1055/s-0029-1202883
2. Xiaojuan Y, Xiaojia W, Xiaohong W, Xiaojun Y. Analysis of risk factor of hyperlactacidemia after gastrointestinal surgery: a clinical data analysis of 216 patients. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015;27(11):875–879.
3. Yu B, Park CM, Gil E, et al. Clinical impact of lactate on postoperative pancreatic fistula after pancreaticoduodenectomy: a single-center retrospective study of 1,043 patients. Pancreatology. 2023;23(3):245–250. doi:10.1016/j.pan.2023.02.001
4. Creagh-Brown BC, De Silva AP, Ferrando-Vivas P, Harrison DA. relationship between peak lactate and patient outcome following high-risk gastrointestinal surgery: influence of the nature of their surgery: elective versus emergency. Crit Care Med. 2016;44(5):918–925. doi:10.1097/CCM.0000000000001567
5. Sakamoto A, Funamizu N, Ito C, et al. Postoperative arterial lactate levels can predict postoperative pancreatic fistula following pancreaticoduodenectomy: a single cohort retrospective study. Pancreatology. 2022;22(5):651–655. doi:10.1016/j.pan.2022.04.002
6. Hayashi Y, Endoh H, Kamimura N, Tamakawa T, Nitta M. Lactate indices as predictors of in-hospital mortality or 90-day survival after admission to an intensive care unit in unselected critically ill patients. PLoS One. 2020;15(3):e0229135. doi:10.1371/journal.pone.0229135
7. Salinero A, Mitzova-Vladinov G. Battle of the crystalloids in the operating room: a literature review. J Perianesth Nurs. 2021;36(6):629–637. doi:10.1016/j.jopan.2021.03.012
8. Andersen LW, Mackenhauer J, Roberts JC, Berg KM, Cocchi MN, Donnino MW. Etiology and therapeutic approach to elevated lactate levels. Mayo Clin Proc. 2013;88(10):1127–1140. doi:10.1016/j.mayocp.2013.06.012
9. Xian H, Xie Q, Qin K, Ma X, Du X. Effect of sodium bicarbonate Ringer’s solution on intraoperative blood gas analysis and postoperative recovery time in liver transplantation: a single-center retrospective study. Ann Transplant. 2023;
10. Shafique MA, Shaikh NA, Haseeb A, Mussarat A, Mustafa MS. Sodium bicarbonate Ringer’s solution for hemorrhagic shock: a meta-analysis comparing crystalloid solutions. Am J Emerg Med. 2024;76:41–47. doi:10.1016/j.ajem.2023.11.003
11. Wu H, Meng G, Zuo C, et al. The Effects of sodium bicarbonate Ringer’s solution on acute kidney injury and the clinical outcomes after liver transplantation: a randomized controlled trial. Front Pharmacol. 2022;13:982472. doi:10.3389/fphar.2022.982472
12. Bian Y, Xu T, Le Y, Li S. The efficacy and safety of sodium bicarbonate Ringer’s solution in critically ill patients: a retrospective cohort study. Front Pharmacol. 2022;13:829394. doi:10.3389/fphar.2022.829394
13. Han SJ, Zhou ZW, Yang C, et al. Hemorrhagic, hypovolemic shock resuscitated with Ringer’s solution using bicarbonate versus lactate: a CONSORT-randomized controlled study comparing patient outcomes and blood inflammatory factors. Medicine. 2022;101(46):e31671. doi:10.1097/MD.0000000000031671
14. Pfortmueller CA, Funk GC, Reiterer C, Schrott A, Zotti O, Kabon B, Fleischmann E, Lindner G. Normal saline versus a balanced crystalloid for goal-directed perioperative fluid therapy in major abdominal surgery: a double-blind randomised controlled study. British J Anaesth. 2018;120(2):274–83.
15. Fleischmann E, Lindner G, Reiterer C. Normal saline versus a balanced crystalloid for goal-directed perioperative fluid therapy in major abdominal surgery: a double-blind randomised controlled study. Br J Anaesth. 2018;120(2):274–283. doi:10.1016/j.bja.2017.11.088
16. Liu J, Gao Y, He Z, Zhang H, Chen L. The efficacy of sodium bicarbonated Ringer’s solution versus lactated Ringer’s solution in elderly patients undergoing gastrointestinal surgery: a prospective randomized controlled trial. Am J Transl Res. 2023;15(8):5216–5227.
17. Song J, Liu Y, Li Y, et al. Comparison of bicarbonate Ringer’s solution with lactated Ringer’s solution among postoperative outcomes in patients with laparoscopic right hemihepatectomy: a single-centre randomised controlled trial. BMC Anesthesiol. 2024;24(1):152. doi:10.1186/s12871-024-02529-2
18. Li Q, Liu Y, Wang Y, et al. Bicarbonate ringer’s solution could improve the intraoperative acid-base equilibrium and reduce hepatocellular enzyme levels after deceased donor liver transplantation: a randomized controlled study. BMC Anesthesiol. 2023;23(1):418. doi:10.1186/s12871-023-02383-8
19. Yu LQ, Meng CC, Jin XS, Cai J. Clinical study of sodium bicarbonated Ringer’s solution on fluid resuscitation of patients with hemorrhagic shock. Eur Rev Med Pharmacol Sci. 2022;26(5):1535–1542. doi:10.26355/eurrev_202203_28218
20. Li Q, Yang Q, Tian C, et al. Effects of different types of Ringer’s solution on patients with traumatic haemorrhagic shock: a prospective cohort study. Eur J Med Res. 2024;29(1):215. doi:10.1186/s40001-024-01664-3
21. Müller J, Radej J, Horak J, et al. Lactate: the fallacy of oversimplification. Biomedicines. 2023;11(12):3192. doi:10.3390/biomedicines11123192
22. Opdam H, Bellomo R. Oxygen consumption and lactate release by the lung after cardiopulmonary bypass and during septic shock. Crit Care Resusc. 2000;2(3):181–187.
23. Kellum JA, Kramer DJ, Lee K, Mankad S, Bellomo R, Pinsky MR. Release of lactate by the lung in acute lung injury. Chest. 1997;111(5):1301–1305. doi:10.1378/chest.111.5.1301
24. Mizock BA. The hepatosplanchnic area and hyperlactatemia: a tale of two lactates. Crit Care Med. 2001;29(2):447–449. doi:10.1097/00003246-200102000-00047
25. Häussinger D, Steeb R, Gerok W. Ammonium and bicarbonate homeostasis in chronic liver disease. Klin Wochenschr. 1990;68(3):175–182. doi:10.1007/BF01649081
26. Häussinger D. Liver regulation of acid-base balance. Miner Electrolyte Metab. 1997;23(3–6):249–252.
27. Atkinson DE, Camien MN. The role or urea synthesis in the removal of metabolic bicarbonate and the regulation of blood pH. Curr Top Cell Regul. 1982;21:261–302. doi:10.1016/b978-0-12-152821-8.50014-1
28. Brosnan JT, Lowry M, Vinay P, Gougoux A, Halperin ML. Renal ammonium production—une vue canadienne. Can J Physiol Pharmacol. 1987;65(4):489–498. doi:10.1139/y87-084
29. Kwak JY, Kim HG, Han JH, Jeon H, Cha RR, Lee SS. Association of the etiology and peak level of markedly elevated aminotransferases with mortality: a multicenter study. Hepatol Commun. 2023;7(5):e0149. doi:10.1097/HC9.0000000000000149
30. Bianchetti DGAM, Amelio GS, Lava SAG, et al. D-lactic acidosis in humans: systematic literature review. Pediatr Nephrol. 2018;33(4):673–681. doi:10.1007/s00467-017-3844-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.