")
Back to Journals » Clinical Ophthalmology » Volume 19
The Impact of Comfort Eluting Agents and Replacement Frequency on Enhancing Contact Lens Performance
Authors Phan CM , Hui A, Shi XC , Zheng Y , Subbaraman LN , Wu J , Jones L
Received 14 December 2024
Accepted for publication 25 February 2025
Published 12 March 2025 Volume 2025:19 Pages 857—873
DOI https://doi.org/10.2147/OPTH.S512246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Chau-Minh Phan,1,2 Alex Hui,1,3 Xinfeng Charlie Shi,4 Ying Zheng,4 Lakshman N Subbaraman,4 James Wu,4 Lyndon Jones1,2
1Centre for Ocular Research & Education (CORE), School of Optometry and Vision Science, University of Waterloo, Waterloo, Canada; 2Centre for Eye and Vision Research (CEVR), Science Park, Hong Kong; 3School of Optometry and Vision Science, Faculty of Medicine and Health, UNSW Sydney, Sydney, NSW, Australia; 4Alcon Research LLC, Fort Worth, TX, USA
Correspondence: Chau-Minh Phan, Email [email protected]
Abstract: This review explores the development and clinical implications of soft contact lenses designed to elute comfort agents, emphasizing their role in enhancing user experience and ocular health. As discomfort remains one of the primary reasons for discontinuation of lens wear, this concept aims to address this challenge by gradually releasing these agents over their period of use. This review also explores the effectiveness, safety, and user satisfaction associated with frequent replacement schedules of these lenses. Clinical trials demonstrate that lenses with eluting comfort agents significantly reduce dryness and irritation, leading to improved wear-time and overall comfort. The findings suggest that frequent replacement not only enhances lens hygiene but also maximizes the therapeutic benefits of the eluted agents, promoting a healthier ocular environment. The implications for practice highlight a shift towards more patient-centered approaches in contact lens design and management, aiming to improve adherence and satisfaction among users. This research paves the way for future innovations in contact lens technology, focusing on personalized solutions that cater to individual comfort needs.
Keywords: comfort, contact lens, replacement frequency, wettability
Introduction
Since their conception in the early 1960s, soft contact lenses (CL) have become a highly successful biomedical device, with an estimated 150 million wearers worldwide.1 However, this success has involved overcoming numerous challenges, many of which continue to persist today. The first generation of CLs was crafted from the hydrogel material polyhydroxyethyl methacrylate (PHEMA)2 and commercialised in the early 1970’s. These lenses were well tolerated for daily wear, but due to their relatively low oxygen permeability, extended or continuous overnight use resulted in a variety of hypoxia-related complications.3–5 The late-1990s saw the commercialisation of the first silicone hydrogel (SiHy) CL materials, which provided superior oxygen transmissibility and resolved many of the issues associated with hypoxia for extended and continuous wear.6–9 However, the first-generation SiHy materials were more hydrophobic than hydrogel materials due to the large amount of siloxane-based monomers incorporated, resulting in increased lipid deposition,10 and relatively poor in vitro wettability.11 Increased lipid deposition on CLs has been shown to increase the likelihood of tear film breakup and promote dewetting of CL surfaces.12,13 Companies have used a variety of surface modifications or the incorporation of internal wetting agents to mask the underlying hydrophobic components of the CL material from the tear film.14–17
When a clinician is selecting an appropriate CL for a patient, in addition to choosing between hydrogel or SiHy-based materials, they must choose an appropriate frequency of replacement. The mid-1980’s saw the introduction of frequent replacement lenses, with most lenses being replaced every two or four weeks. These lenses exhibited significant clinical advantages over soft lenses that had traditionally been replaced annually or longer, especially with respect to comfort, vision, deposition, number of unscheduled visits and overall complications.18–21 However, reusable CLs still exhibited complications due to poor compliance with cleaning, frequency of replacement and poor case hygiene.22,23 Some of these issues were addressed with the introduction of the daily disposable CL modality in the mid 1990s.24–26 Although they are relatively more expensive, daily disposable replacement schedules offer greater convenience, exhibit fewer adverse events and have improved compliance compared to lenses which need to be regularly cleaned and reconditioned.23–30 Indeed, the current market trend favors the use of daily disposables.31 However, this shift has raised growing concerns about waste generation and environmental sustainability and incurs an increased cost for the wearer.
The evolution of CL materials remains dynamic, as the industry continues to develop materials with superior performance to previous generations.16,17 However, this evolutionary progress has resulted in an immense catalogue of CLs available today. This multitude of choices can be both beneficial but also challenging for clinicians, as selecting the optimal lens type for a particular patient is not always straightforward.
The success of CL wear is heavily influenced by lens performance on the eye, particularly with respect to comfort,32,33 which is the primary reason for discontinuing CL wear in long term wearers.33–35 However, understanding CL comfort is a complex matter influenced by numerous factors, including lens fit, design, modulus, wettability, friction, lubricity, water content, oxygen permeability, ocular responses, tear film interactions, lens deposition, and the uptake and release of components from multipurpose solutions (MPS) for reusable lenses, as well as demographic factors.23,32,34,36–40 Several comprehensive reviews have been published addressing CL discomfort,23,32,34,37–39,41–46 but there is still no consensus regarding the exact mechanisms that drive CL discomfort and the factors needed to alleviate this.
There are two factors worthy of consideration that have received relatively little discussion. The first relates to the possibility of incorporating wetting agents into CL materials that are released slowly and that act as “comfort agents”. Some commercial lenses already incorporate wetting agents into the blister packaging solution to enhance initial comfort,47 while others incorporate these agents directly into the lens material during their manufacture.39 The release of these agents could help improve CL performance by improving comfort and reducing dryness associated with CL wear. The second factor is determining the optimal frequency of replacement for a patient, as it is entirely possible that optimal performance may decline well before the scheduled replacement.48
This article provides a review of current research exploring the enhancement of CL performance by focusing on the release of wetting agents and the influence of lens replacement frequency on comfortable CL wear, with a particular emphasis on how this may impact materials designed to release wetting agents.
Methods
This review was conducted using information sourced from a wide variety of databases, including PubMed, Scopus, Web of Science, and ScienceDirect. Additional online resources, such as Contact Lens Spectrum, were referenced where necessary. The search strategy was designed to achieve the objective of the review: examining the impact of comfort-eluting agents and replacement frequency on enhancing CL performance.
Release of Wetting Agents
The concept of using CLs for the sustained release of a wetting agent shares many similarities to that seen in the design of CL materials for topical ocular drug delivery.49 The use of CLs to deliver topical drugs or comfort agents offers two key benefits. First, any agent released from the lens into the post-lens tear film experiences less influence from removal mechanisms such as blinking and tear drainage, resulting in an extended residence time and contact with the cornea. Second, soft CLs naturally absorb water and other compounds, including drugs. These absorbed agents can interact with the lens polymer, creating a drug reservoir that can be tuned to be released in a sustained manner.49–51 Different strategies, such as modifying the polymer composition or incorporating nanoparticles, liposomes, and coatings, can be employed to control and prolong the release duration of the drug from the CL material.49–52
Similarly, wetting agents, such as surfactants, can be added to the lens during the manufacturing process, with the intention of releasing them during wear to enhance CL performance.52–63 By increasing lens surface wettability with a wetting agent, the surface tension is lowered, facilitating the spreading of the tear fluid over the lens. Increased lens wettability is also associated with reducing friction between the lid and the lens surface, which is believed to enhance CL comfort.39 Additionally, wetting agents can also interact with the tear film, increasing tear film stability and preventing dewetting of the lens surface.64
Several methods have been explored to load wetting agents into lenses, including their incorporation into blister pack solutions,47,53–56,58,65–71 incorporating them into the lens material,53–62 adding wetting agents to MPS that soak reusable lenses overnight,72–81 and applying rewetting drops over the lens surface.37,39,82–86 In most cases, the wetting agents are rapidly released from the CL within a few hours,56,65,70 thus the overall comfort boost may only be temporary. In an attempt to prolong comfort, manufacturers are investigating designing lens materials that can provide sustained release of agents for longer periods.58,87
Table 1 summarizes the various wetting agents that are released from CL materials to enhance their performance. Only studies that included measuring the release of a wetting agent or its effect over at least two time points have been included.
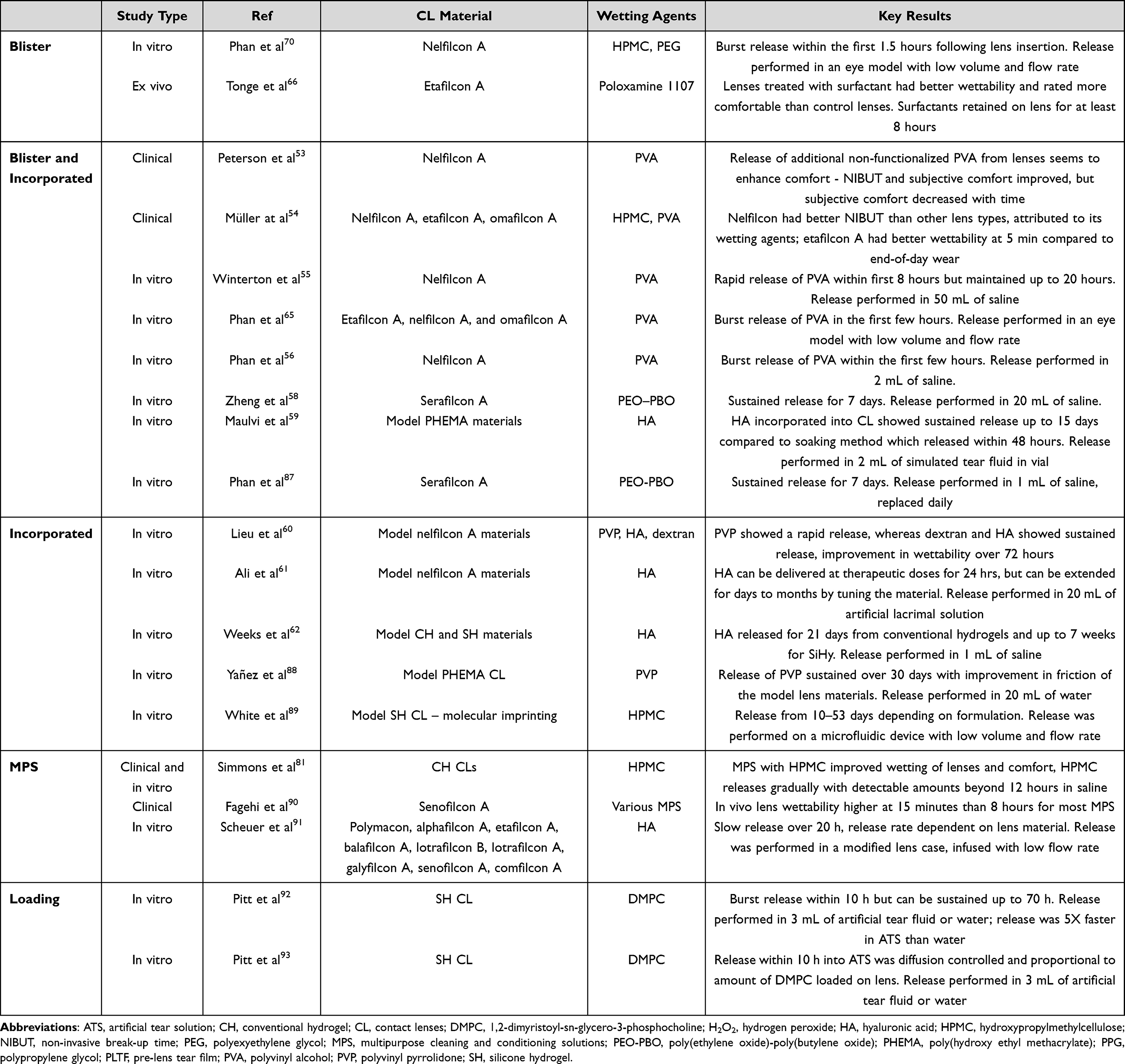 |
Table 1 Summary of Wetting Agents Released From CLs to Improve Lens Performance |
There are four broad ways by which wetting agents can be “added” to a CL material: Incorporating them into the blister packaging; incorporating them into the lens material; incorporation into the multipurpose solution or incorporating them into an ocular lubricant.
Wetting Agents Incorporated into the Blister Packaging
Historically, blister pack solutions consisted of buffered saline.94 These solutions have evolved over time to include various other components, including wetting agents. The specific wetting agents used in the blister pack are often not explicitly mentioned on the packaging or the package inserts, making it a challenge to determine their exact composition. Some identified components in commercial products include polyethylene glycol (PEG),66,70 polyvinylpyrrolidone (PVP),66 polyvinyl alcohol (PVA),53–57,65 poloxamines (Tetronics®),66,69 hydroxypropyl-methylcellulose (HPMC),54,70 hyaluronic acid (HA),59 and poly(oxyethylene)-co-poly(oxybutylene) (PEO-PBO).58 A wide range of wetting agents have been used by different manufacturers, but a single “best” agent is yet to be identified. Unsurprisingly, due to variations in components, the surface tension of commercial blister pack solutions has been shown to vary greatly, between 22–70 dynes/cm.47,67 The ideal range that is suggested to promote comfortable CL wear is between 42–46 dynes/cm,95 and a large portion of blister pack solutions appear to fall in this range.
The release of wetting agents from CL that are merely soaked in a blister pack solution is typically temporary, providing only an initial comfort boost following initial CL insertion. Studies investigating the hydrogel material etafilcon A that was soaked in a solution of wetting agents including poloxamine, PEG, and PVP have shown increased subjective comfort within the first 30 minutes of wear, which also correlated with a reduced measured surface tension during this same time period.66 Clinical studies with the PVA-based nelfilcon A hydrogel material that contains non-polymerized PVA that “leaks” into the blister pack have demonstrated improved non-invasive break-up time (NIBUT) and subjective comfort on lens insertion, although comfort ratings decreased over time.53 In vitro studies with PVA, HPMC, and PEG and various CL materials have indicated that the majority of the release from the lenses occurs within the first few hours of wear.56,65,70 These observations, which follow a burst release, are in line with those of therapeutics released from commercial CLs that have not been specifically designed for sustained delivery.49 Notably, wetting agents incorporated into the blister pack solution are thought to be primarily surface-bound, as washing or rinsing the blister pack solution from lenses has been shown to reduce the lens wettability as compared to when lenses are removed directly from the packaging.71 Interestingly, one study has shown sustained release of a high molecular weight, amphiphilic, non-ionic, wetting agent, PEO-PBO, from a blister pack for up to one week.58 This innovative technique allows for up to 80% of the absorbed wetting agent to become irreversibly trapped within the lens material (serafilcon A) while the remaining portion is available for release over a period of up to one week,58 although its impact on sustained comfort is unknown. In another in vitro study, Phan et al showed that serafilcon A released a fluorescently tagged version of PEO-PBO over 7 days in a simulated wear and cleaning regimen.87
Currently, there is limited research on leveraging the uptake and release of wetting agents from blister packs, with most studies suggesting that these agents are only used to provide improved comfort within a short period after CL insertion.
Wetting Agents Incorporated into the Lens Material
Silicone hydrogel CLs, due to their siloxane components, can exhibit poor wetting properties compared with hydrogel materials. To address this issue, wetting agents can be incorporated into the lens material or added as a surface treatment during the lens manufacturing process to enhance the intrinsic wettability of the material.14,16,39 Various compounds have been successfully employed for this purpose, including PVA, PEG, HPMC, HA, N-vinyl pyrrolidone (NVP), PVP, methacrylic acid (MA), poly-2-ethyl-2-oxazoline, glycidyl methacrylate, dextran, phosphorylcholine, phosphocholine, phosphatidylcholine, and poloxamers.16,39,60,92,93,96–98 The majority of these agents become embedded within the lens material itself as internal wetting agents, whereas others modify the surface wettability.14,16,39,96,97 Only a very small fraction of these wetting agents, in particular PVA,53–57,65 HA,60 PVP,60 dextran,60 and phosphocholine92,93 have been shown to be released from the lens rather than remaining fixed within the lens.
PVA has garnered the most attention among these releasable wetting agents, particularly in relation to its release from the nelfilcon A material.53–57,65 PVA has a wide range of biomedical applications due to its biocompatibility and lubrication properties.99 Nelfilcon A is made from photo cross-linked PVA and non-polymerized PVA is released from the material into the blister pack and subsequently from the lens onto the ocular surface during wear.53,55,57,63 Several clinical studies have demonstrated that nelfilcon A CLs do indeed provide enhanced comfort, which can be attributed to the release of PVA.53,54 Initial in vitro studies with nelfilcon A suggested that PVA is released from the CL over 8 hours.55,63 However, later studies showed that the majority of the PVA is released within a few hours,56,65 limiting its impact over the course of the day. However, it may be possible that the released PVA becomes trapped beneath the post-lens tear film, resulting in longer than expected residence time on the eye. The nelfilcon A material also releases two other wetting agents, PEG and HPMC.70 It is thought that the HPMC provides initial comfort immediately after lens application, PEG release provides an early-day comfort boost, and PVA release is sustained for a longer period.57
Aside from PVA, there have been limited attempts in the industry to develop CLs capable of releasing other wetting agents. Some studies have focused on incorporating HA59–61 and phosphocholine92,93 into model CL materials. HA is a hydrophilic polymer commonly used in ophthalmic applications for its wetting properties and ability to stabilize the tear film.100,101 Studies have demonstrated sustained release of HA from model CL materials ranging from 24 hours to several weeks.59–62 Molecularly imprinted CLs with HPMC showed that these lenses can provide release of the wetting agent for up to 53 days in vitro.89 Model hydrogel CLs made from HEMA with PVP showed that this lens material could release PVP for up to 30 days, with measured improvements in the friction of the lens material surface.88 These findings suggest that HA, 1.2-dimyristoyl-sn-glycero-3-phosphocholine (DMPC) and HPMC, may be potential wetting agent candidates for release from a CL, but studies thus far have only been performed on model CL materials in the laboratory. Moreover, the uptake and release of these agents from a simple soaking procedure already seem to be sufficient for a daily wear modality, so incorporating them into the lens material for a longer release duration may not be needed.59
Wetting Agents Incorporated into Multipurpose Solutions
A multipurpose solution (MPS) plays a crucial role in restoring the performance of reusable CLs by effectively cleaning, disinfecting, and restoring the lens to a usable state following an overnight soak. Contemporary MPS formulations are complex, comprising a combination of buffers, biocides, surfactants, chelating agents, and hydrating agents for soft CL storage.39,43 Similar to that seen with respect to the situation described previously relating to blister pack solutions, CLs can also uptake components from the MPS, including biocides, surfactants and wetting agents.36,39,43,102,103 These sorbed components can be subsequently released onto the corneal surface during lens wear, potentially impacting the overall clinical performance, positively or negatively, of the CL on the eye.36,43,102,103 While the majority of studies have focused on the negative effects of CL uptake and subsequent release of biocides or other components from the MPS,36,39,41,43,102–107 it is equally important to recognize the potential opportunity for MPS to enhance CL performance with a fresh supply of wetting agents.34,43
Wetting agents commonly found in MPS vary among manufacturers and include poloxamers (Pluronics®),90,108 poloxamines (Tetronics®),77,90,108 PEO-PBO,78,80 hyaluronic acid, aloe vera,73 and PVP.73 These wetting agents can be absorbed into the bulk of the lens material or adsorbed onto the lens surface, depending on the presence of a surface coating.109 Numerous studies have demonstrated that the use of MPS generally enhances lens wettability and performance.37,39,72–81,90,91,110 A study also showed that an MPS containing wetting agents demonstrated improved ocular comfort, reduced blink frequency, enhanced visual performance, and improved tear film quality compared to an MPS without wetting agents.79 Some studies have also suggested that certain wetting agents, such as PEO-PBO, may offer slightly superior comfort compared to others,78,80 while agents such as aloe vera or PVP may not have significant effects on wettability.73 While there is substantial evidence supporting the positive effect of wetting agents in MPS on lens wettability,37,72–81,90,91,110 only a few have examined the release of these agents from the CL over time.81,90,91
Similar to blister pack solutions, it can be postulated that the release of wetting agents sorbed onto a lens from an MPS would likely occur rapidly,56,65,70 resulting in only an initial impact on comfort, with little sustained benefit. Studies observing the uptake and release of biocides from MPS have shown that the release of biocides occurs rapidly, within the first few hours.102,111–113 Although limited studies have investigated the release of wetting agents following an MPS soak, the available evidence indirectly suggests that the majority of the release is also within hours.39 A clinical study using tear interferometry conducted with senofilcon A using various MPS solutions demonstrated that in vivo lens wettability was higher at 15 minutes compared to 8 hours.90 The decline in wettability may have already occurred within the first few hours, but the study did not measure this time point.
Some studies, however, have suggested that the release of wetting agents can be sustained from a lens exposed to an MPS soak. A study investigating the uptake and release of a HPMC-containing MPS reported improved lens wettability and comfort, with detectable levels of HPMC released even beyond 12 hours.81 An in vitro study looking at the retention of fluorescently tagged HA to commercial CLs also showed that while there is a burst release within 4 hours, almost all of the materials tested could release HA for up to 20 hours.91 Studies with radiolabeled DMPC demonstrated that these phospholipids can be absorbed into a SiHy material and then subsequently released from the lens materials for up to 70 hours, although a burst release does occur within the first 10 hours, with more elution of the drug into an artificial tear solution than water.92,93
To date, there is clearly a lack of studies on the uptake and release of wetting agents from MPS to enhance CL performance, highlighting the need for further research in this area.
Wetting Agents Incorporated into Ocular Lubricants
One strategy to improve CL performance is through the use of rewetting drops, which are commonly referred to as lubricating drops or comfort drops.39 These drops are frequently recommended for CL wearers experiencing dryness and discomfort, and can be applied just before or during lens wear.83,114 Rewetting drops contain a variety of wetting agents, such as HPMC, PVA, PVP, HA, poloxamines (Tetronics®), PEG, carboxymethylcellulose (CMC), dextran, and povidone, each with distinct molecular weights, shear strengths, viscosities, and mucoadhesive properties that impact their performance.39,82,115,116
It is worth noting that the efficacy of rewetting drops can differ between materials, with some studies suggesting greater improvements in wettability for hydrogel CLs compared to SiHy lenses, where wettability improvement may be inconsistent or even diminished.83,117 A study investigating the impact of a rewetting drop containing two surface active agents (RLM-100 and Tetronic® 1304) on a SiHy material (lotrafilcon A) when used on a 30-day continuous wear basis found that the rewetting drop provided greater subjective satisfaction, reduced lysozyme and total protein deposition, and reduced denatured lysozyme than a rewetting drop containing saline alone, each applied four times daily.118 Notably, one study found that HA, HPMC, and CMC had greater comfort properties than other agents tested.116 Several strategies have been proposed to improve the performance of rewetting drops, such as increasing viscosity at low shear rates without exceeding the blur threshold, or using a high molecular weight wetting agent with low polydispersion index.83,119 A study with HA showed that formulations with 0.1% HA improved the in vivo wettability of hydrogel CLs for 5 minutes, whereas a more viscous 0.3% HA solution improved the wettability for 30 minutes.83
Most rewetting drops typically have a very short residence time on the eye.84,115 Improvements after instilling a rewetting drop during CL wear are typically transient, lasting less than 10 minutes.37,39,84,85 Moreover, while subjects may experience improved subjective comfort after using the rewetting drop, there is currently no other evidence suggesting enhanced tear film stability or optical quality.120 The benefits of using a rewetting drop are also not immediate and may take months to manifest for CL wearers.86 A study also indicated uncertainty as to whether the improved comfort was due to the specific wetting agent used or if saline solution alone would suffice.121 Nonetheless, most studies suggest that rewetting drops do improve comfort and reduce ocular symptoms associated with CL wear.82,118,121–124
To date, there have been no studies that have actively examined the release of wetting agents from rewetting drops when applied to CLs in-situ, and this may be an area of future exploration. Existing research has indicated that certain components in ophthalmic formulations can be absorbed by soft lenses and gradually released onto the ocular surface over time. A noteworthy example is benzalkonium chloride (BAK), a commonly used preservative in glaucoma medications, which can unintentionally be absorbed by a soft CL material and subsequently released on the eye, potentially leading to adverse effects on the ocular surface.125 In such scenarios, it is recommended to allow a minimum of 15 minutes between instilling medication and wearing lenses.125 Rather than presenting a negative impact, these underlying mechanisms could also be leveraged to deliver wetting agents to improve CL performance.
A notable limitation in the current literature is the reliance on in vitro studies to measure the release of wetting agents from lenses, often using non-standardized, vial-based models. The release medium’s environment has been shown to significantly impact release rates.92,126,127 For instance, DMPC was released five times faster in an artificial tear solution compared to water.92 Additionally, drug delivery studies with CL materials indicate much slower release in advanced in vitro models with low tear volume and flow than in vials.126,127 The lack of standardization and use of different models complicate comparisons across studies and underscore the importance of also carefully considering system parameters before extrapolating results to predict the performance on the eye.
In reviewing the literature on wetting agents, it is clear that the incorporation of surface-active agents into the blister pack, into the lens material itself, in the MPS used to disinfect and clean reusable lenses overnight or by direct application over the CL can all bring potential benefits to lens wearers and enhance the wearing experience. However, these approaches can be impacted by the lens material used and the frequency with which the lens is replaced. What evidence exists that can assist the prescribing practitioner on the most appropriate lens replacement period, and how could that be linked to the potential incorporation of wetting agents? The literature on wetting agent release from soft lenses remains limited, highlighting the need for further studies to advance sustained-release technologies and assess their clinical impact on lens comfort. Research into using multipurpose solutions or ocular lubricants to enhance comfort with wetting agents would also be valuable.
Replacement Frequency and Contact Lens Comfort
Increasing the frequency of replacement is widely recognized as advantageous for promoting ocular health and enhancing lens wearer comfort.34,41 Indeed, there is a growing trend towards the prescribing of daily disposable CLs.31,128 However, the daily disposable modality comes with significantly increased costs for full-time wearers129 and growing concerns regarding their environmental impact.130 Reusable modalities address these shortcomings but, in turn, have their own challenges. For this reason, the optimal replacement frequency varies between patients, as it depends on several factors, including CL performance, cost, and patient compliance.
Current Wear Modalities and Performance
There are two primary modalities for soft CL wear, namely daily disposable and reusable, with the latter requiring lenses to be removed, disinfected overnight and replaced after a certain period. Reusable lenses are typically replaced after 2 weeks or 1 month, with some lenses being replaced for durations exceeding 1 month.31,128 The preference for each modality varies based on geographic location, with daily disposables being more popular in Australia, Canada, the UK, and Japan, while reusable lenses are more commonly fit in France and The Netherlands.31 There has been a noticeable shift towards an increase in daily disposable lens wear such that there is now an almost 50:50 split of reusable to daily disposable fits (see Figure 1).31,128,131–134 In 2018, daily disposable CLs accounted for approximately 32% of fittings, rising rapidly over the past 6 years. Among daily disposable lenses, SiHy options are increasingly becoming the preferred choice, now accounting for 73% of all daily disposable materials fit.31
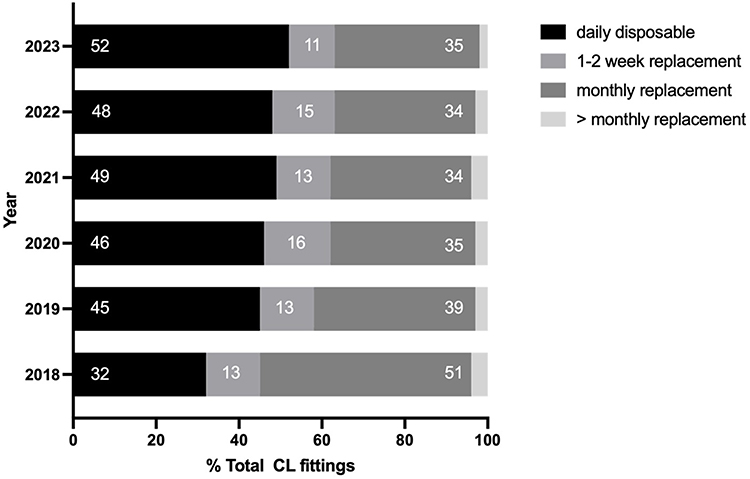 |
Figure 1 Contact lens fitting modalities worldwide from 2018 to 2023. |
The increasing preference for daily disposable CLs may be attributed to their advantages over reusable CLs. Daily disposables offer greater convenience, improved ocular health, fewer adverse events, and better compliance with replacement schedules compared to lenses that require regular cleaning and reconditioning.29,30,135 Reusable lenses have an increased risk of corneal infiltrates compared with daily disposable lenses,136–138 and silicone hydrogel reusables show an approximate 2x increased risk of infiltrates compared with hydrogel reusable materials.136,137,139,140 Disinfection and overnight cleaning with MPS may also result in unwanted uptake of biocides and other agents, which can result in poor lens performance and corneal staining.30,36,39,41,43,102,103,107
One of the primary drawbacks of using daily disposable CL relates to the higher cost, but advancements in manufacturing methods may address this concern in the future. Another factor to consider is that manufacturers need to tackle the challenge of increased packaging waste, particularly for the daily disposable modality.130,141 Full-time daily disposable wearers generate 27% more waste annually compared to their reusable counterparts.130 Fortunately, most of the waste associated with CL, for both daily disposable and reusable modalities, can be recycled with the appropriate infrastructure for waste collection in place.130 However, to date, there is no information on whether the majority of CL waste ends up in landfills or is actually recycled through programs.
The data in Figure 1 was collected from various countries, and the reported percentages are based on the global average. The fitting modality percentages for individual countries may vary from the average. There is a trend shift from monthly reusables to daily disposables.31,131–134,142
Based on economic factors alone, monthly replacement should be the most popular fitting option, since they are least expensive for full time wear, even when factoring in the cost of solutions.129 However, in many countries daily disposables have the highest CL fitting rate,31 suggesting that cost considerations may no longer be a significant barrier for the adoption of daily disposables CL for many wearers. In comparison, based on CL performance, it would be natural to assume that daily disposables would be the most widely fit modality, followed by 1–2 week lenses, and then monthly replacement. In a survey-based study, a daily disposable modality recorded higher end of day comfort than a 2-week or 1-month replacement frequency.143 Daily disposables also offer convenience for patients, as they eliminate the need for cleaning solutions and storage cases.29,144 Clinical trials with daily disposables show fewer ocular adverse events and better comfort compared to their reusable counterparts.29 Review of the overall data from various studies suggests that there are relatively small differences in performance between 2-week and monthly modalities. However, monthly fittings are currently more than double that seen for 1–2 week lenses,31 suggesting there are other key factors than performance that drive practitioners to fit monthly replacement lenses, including cost and availability of products.
Patient Non-Compliance
Non-compliance with lens-wearing schedules, replacement schedules, and lens care regimens continues to pose a challenge, leading to reduced CL performance, complications and an increased chance of CL dropout.143,145 Although manufacturers do provide specific instructions for optimal performance, these details can become unclear or lost as they are passed from practitioners to patients.146 Not surprisingly, patients who are compliant, in particular replacing their lenses based on the recommended schedule, achieve improved CL subjective performance for both comfort and vision.143 However, effectively managing and ensuring patient compliance remains a complex endeavour that requires further attention and innovative approaches.143,145,146
Non-compliance with CL wear and care is extremely high, with reported rates ranging from 50% to 99%, and it exists even in situations where patients are aware of the risks associated with non-compliance.22,40,145,147–154 However, despite these issues, there is a lack of comprehensive data on strategies to improve compliance. Studies have shown that compliance varies among different replacement modalities, with daily disposables demonstrating the highest compliance with replacement frequency, followed by monthly lenses, with 2-week lenses showing the poorest compliance for replacing lenses on time.148,152,155–157 Reasons for noncompliance include “forgetting” to replace lenses and saving money.29,155–157 These findings are not surprising, as replacing lenses daily or on the same date each month is inherently easier to remember than tracking a 2-week schedule.
Determining Optimal Replacement Frequencies
Determining an optimal replacement frequency is challenging due to complex factors, including the material interactions with tear film components, MPS and wetting agents.39 The lens material characteristics also play a crucial role in determining the optimal frequency of replacement.158 Additionally, individual patient factors and compliance with cleaning and maintenance instructions further contribute to variability in lens performance.143,145 Moreover, each patient physiology is also different, and so responses to CL wear may also vary greatly, and personal preferences may also play a role.
To maintain optimal lens performance, the recommended replacement frequency for most patients can range anywhere from 1 week to several months.48 For symptomatic patients, a shorter replacement interval down to 1 week has been suggested.48 In vitro studies with reusable CLs show increased deposition of proteins and lipids over time, with more deposits at 1 month than 2 weeks.10,159–164 In vivo studies on protein and lipid deposition indicate that there may be an optimum point for hydrogel lens replacement between 1 and 7 days: protein deposition stabilizes within 7 days, while lipid deposition reaches a maximum within 1 day on group IV lenses but gradually increases on group II materials over 4 weeks.159 However, the direct link between increased deposition and clinical discomfort remains unclear, and further investigation is required.41 Nonetheless, for a reusable lens wearer, a replacement schedule of 1 week or less may be optimal in order to mitigate the potential issues associated with longer replacement intervals.
The 2-week replacement modality was initially chosen for the etafilcon A material when it was not prescribed on an extended wear, one-week replacement schedule.165 There is no clinical data or publications to suggest why this particular replacement schedule was originally determined. Once daily disposable lenses became available, the 2-week modality continued to be widely used to strike a balance between the convenience of daily disposables and the lower cost of monthly lenses. However, as detailed above, in terms of compliance, the 2-week modality can create problems with remembering when to replace the lenses,29,155–157 leading to potential impacts on lens performance. In addition, many practitioners opt to advise patients to replace their 2-week replacement materials every month.155,157
To-date, there is no widespread availability of a 1-week replacement frequency, daily wear material.87 However, intuitively, the replacement frequency would be simple to remember (as is 1 day and 1 month) and the clinical performance should conceptually be closer to that seen with daily disposables, while still offering the cost advantages of reusable lenses. Ideally, practitioners would be able to “personalize” a replacement schedule for a specific material for each wearer, with the lens being replaced prior to a reduction in performance. Such an approach would hopefully improve the wearer’s experience, reduce the risk of complications and optimize the cost to the wearer. Indeed, previous work has shown that patient deposition is highly individual166–168 and that adopting a blanket replacement schedule for a particular material is not an ideal approach. However, while indeed ideal, such an approach is fraught with difficulties relating to what key metrics would drive the decision and how such a system would be administered by the prescribing practitioner. Given this, then an option to replace a lens on a weekly basis may be a viable consideration.
Summary
CL performance, particularly in terms of comfort, is influenced by a multitude of factors.34,35,44–46,169–171 Existing research has primarily focused on investigating the physical properties of CLs, their interactions with the tear film and ocular surface, as well as the impact of MPS on CL performance over time.23,32,34,37–39,41,172,173 This review has investigated two specific aspects that also play a crucial role in enhancing CL performance: the interaction and release of wetting agents from CL materials and their replacement frequency.
The release of wetting agents from CL materials, particularly nelfilcon A that is based on PVA, has been associated with improved comfort.53–57,65 However, a challenge in achieving sustained release is the tendency for these wetting agents to be released within a few hours.55,56,65 While methods used for CL drug delivery could potentially enhance the duration of wetting agent release,52,59–61,88,89 this approach would introduce additional complexity to the manufacturing process, resulting in increased costs for both manufacturers and wearers. Moreover, designing CLs specifically for delivering wetting agents may subject them to the same regulatory scrutiny as lenses intended for drug delivery.49
Several methods have been explored to incorporate wetting agents into CL materials, including their inclusion in blister pack solutions,47,53–56,58,65–71 MPS,72–81 and rewetting drops.37,39,82–86 Overall, the longer the incubation period and the higher the concentration of the wetting agent, the longer its effect is felt. Hence, blister packs and MPS have demonstrated better outcomes compared to rewetting drops. However, the consensus is that these wetting agents only provide temporary relief, with effects lasting minutes to at most an hour.39 Thus, end-of-day comfort for CLs continues to remain an issue that cannot be addressed with the current release technology approaches used to deliver wetting agents. Recent research has demonstrated that it is possible to release wetting agents such PEO-BEO for up to one week,58,87 but to-date there are no published clinical studies to validate whether this release is correlated to improved comfort. The investigation of wetting agent release from CLs remains a relatively unexplored area of research, presenting a valuable opportunity for further exploration around methods to enhance CL performance.
Despite the known importance of replacement frequency for ensuring optimal CL performance,41 there is a lack of comprehensive research investigating its impact, in particular with contemporary materials. It is intuitive that simply replacing a CL frequently would address issues related to tear film deposition and interactions with tear film components over time. This is reflected in the increasing popularity of daily disposable CLs over the past decade,128,131–134,142 which accounted for nearly 50% of all CL fittings in 2023.31 Daily disposables offer numerous advantages, including convenience, improved ocular responses, fewer adverse events, and enhanced patient compliance.29,30 However, it is worth considering the increased costs associated with daily disposables. Moreover, since these lenses are disposed of each day, there is less incentive and more cost constraints to designing more advanced CL materials. Advanced lens materials refer to those with more complex polymer chemistries, incorporating internal wetting agents and modified surfaces for improved wettability, interaction with the tear film, and compatibility with multipurpose solutions.
Among the reusable CL modality, the monthly replacement schedule has emerged as the dominant choice worldwide, significantly surpassing the popularity of the 2-week replacement schedule.31,128 The preference for a monthly modality is likely driven by cost savings and factors related to non-compliance with replacement schedule, which is better for monthly replacement than 2-week replacement.148,152,155–157 Studies have demonstrated that patients show higher levels of non-compliance with 2-week replacement lenses, often attributed to forgetfulness.29,155–157 Indeed, the challenges associated with remembering to change lenses every 2 weeks can easily be understood, considering the irregular gaps within the replacement frequency. A 1-week replacement schedule balances the cost advantages of reusables and the benefits of frequent lens replacement. While it may improve patient compliance compared to a 2-week modality, it would likely not be as good as daily disposables. It also shares drawbacks with other reusables, such as the need for a cleaning regimen, lens case, and solution. With only one lens currently approved for weekly use,87 more time is needed to assess its adoption by practitioners and its potential to compete with daily disposables and monthly replacement lenses.
A deeper understanding of the impact of replacement frequency on comfort, particularly through additional clinical studies, could help guide the field in determining the optimal frequency that balances lens performance with cost and environmental considerations. Much of the existing evidence relies on intuition and logic rather than scientific substantiation. While the ideal replacement frequency will inevitably vary between patients, a new modality between daily disposables and reusable lenses may offer the advantages of both. If the field can determine an optimal frequency for most of the population, then manufacturers and researchers can more effectively focus on developing technologies to sustain the release of wetting agents during that period. At present, it remains unclear whether to prioritize release technologies for daily disposables or reusables; a more targeted focus would ensure commercialization success. Overall, further research in these areas will help establish a stronger framework for manufacturers and practitioners to develop and prescribe CL with higher comfort.
Funding
This work was funded by Alcon Research LLC and the Hong Kong Special Administrative Region Government and InnoHK.
Disclosure
Alex Hui reports grants from Alcon, during the conduct of the study; grants and/or personal fees from Johnson and Johnson and Labtician Thea, outside the submitted work. Xinfeng Charlie Shi, Ying Zheng, Lakshman N Subbaraman, and James Wu are employees of Alcon. Lyndon Jones reports grants and/or personal fees from Alcon, Azura Ophthalmics, Bausch & Lomb, CooperVision, Hoya, IMedPharma, Integral Biosystems, Johnson & Johnson Vision, Menicon, Novartis, Ophtecs, Santen, SightGlass, SightSage, Topcon, Visioneering Tech, and Essilor Luxottica, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Akerman D. Our greatest opportunity. Cont Lens Anterior Eye. 2018;41:319–320. doi:10.1016/j.clae.2018.05.007
2. Wichterle O, Lim D. Hydrophilic gels for biological use. Nature. 1960;185:117–118. doi:10.1038/185117a0
3. Zantos S, Holden B. Ocular changes associated with continuous wear of contact lenses. Aust J Optom. 1978;61:418–426.
4. Holden BA, Mertz GW. Critical oxygen levels to avoid corneal edema for daily and extended wear contact lenses. Invest Ophthalmol Vis Sci. 1984;25:1161–1167.
5. Dillehay SM. Does the level of available oxygen impact comfort in contact lens wear?: a review of the literature. Eye Cont Lens. 2007;33:148–155. doi:10.1097/01.icl.0000245572.66698.b1
6. Sweeney DF. Have silicone hydrogel lenses eliminated hypoxia? Eye Cont Lens. 2013;39:53–60. doi:10.1097/ICL.0b013e31827c7899
7. Sweeney DF. Clinical signs of hypoxia with high-Dk soft lens extended wear: is the cornea convinced? Eye Cont Lens. 2003;29:S22–5; discussionS26–9, S192–4. doi:10.1097/00140068-200301001-00007
8. Stretton S, Jalbert I, Sweeney DF. Corneal hypoxia secondary to contact lenses: the effect of high-Dk lenses. Ophthalmol Clin North Am. 2003;16:327–40, v. doi:10.1016/S0896-1549(03)00053-1
9. Dumbleton K, Keir N, Moezzi A, Feng Y, Jones L, Fonn D. Objective and subjective responses in patients refitted to daily-wear silicone hydrogel contact lenses. Optom Vis Sci. 2006;83:758–768. doi:10.1097/01.opx.0000237547.35542.b8
10. Lorentz H, Jones L. Lipid deposition on hydrogel contact lenses: how history can help us today. Optom Vis Sci. 2007;84:286–295. doi:10.1097/OPX.0b013e3180485d4b
11. Keir N, Jones L. Wettability and silicone hydrogel lenses: a review. Eye Cont Lens. 2013;39:100–108. doi:10.1097/ICL.0b013e31827d546e
12. Bhamla MS, Chai C, Rabiah NI, Frostad JM, Fuller GG. Instability and breakup of model tear films. Invest Ophthalmol Vis Sci. 2016;57:949–958. doi:10.1167/iovs.15-18064
13. Bhamla MS, Balemans C, Fuller GG. Dewetting and deposition of thin films with insoluble surfactants from curved silicone hydrogel substrates. J Colloid Interface Sci. 2015;449:428–435. doi:10.1016/j.jcis.2015.01.002
14. Jones L, Subbaraman LN, Rogers R, Dumbleton K. Surface treatment, wetting and modulus of silicone hydrogels. Optician. 2006;232:28–34.
15. Teichroeb JH, Forrest JA, Ngai V, Martin JW, Jones L, Medley J. Imaging protein deposits on contact lens materials. Optom Vis Sci. 2008;85:1151–1164. doi:10.1097/OPX.0b013e31818e8ad6
16. Tighe BJ. A decade of silicone hydrogel development: surface properties, mechanical properties, and ocular compatibility. Eye Cont Lens. 2013;39:4–12. doi:10.1097/ICL.0b013e318275452b
17. Musgrave CSA, Fang F. Contact lens materials: a materials science perspective. Materials. 2019;12:261. doi:10.3390/ma12020261
18. Poggio EC, Abelson MB. Complications and symptoms with disposable daily wear contact lenses and conventional soft daily wear contact lenses. CLAO J. 1993;19:95–102.
19. Jones L, Franklin V, Evans K, Sariri R, Tighe B. The spoilation and clinical performance of monthly versus three monthly disposable contact lenses. Optom Vis Sci. 1995;72:147. doi:10.1097/00006324-199512001-00245
20. Pritchard N, Fonn D, Weed K. Ocular and subjective responses to frequent replacement of daily wear soft contact lenses. CLAO J. 1996;22:53–59.
21. Malet F, Schnider CM. Influence of replacement schedule and care regimen on patient comfort and satisfaction with daily wear frequent-replacement contact lenses. CLAO J. 2002;28:124–127.
22. Wu YT, Willcox M, Zhu H, Stapleton F. Contact lens hygiene compliance and lens case contamination: a review. Cont Lens Anterior Eye. 2015;38:307–316. doi:10.1016/j.clae.2015.04.007
23. Stapleton F, Bakkar M, Carnt N, et al. BCLA CLEAR-contact lens complications. Cont Lens Anterior Eye. 2021;44:330–367. doi:10.1016/j.clae.2021.02.010
24. Nason RJ, Boshnick EL, Cannon WM, et al. Multisite comparison of contact lens modalities. Daily disposable wear vs. conventional daily wear in successful contact lens wearers. J Am Optom Assoc. 1994;65:774–780.
25. Nilsson SEG, Söderqvist M. Clinical performance of a daily disposable contact lens: a 3-month prospective study. J Br Cont Lens Assoc. 1995;18:81–86. doi:10.1016/S0141-7037(95)80012-3
26. Solomon OD, Freeman MI, Boshnick EL, et al. A 3-year prospective study of the clinical performance of daily disposable contact lenses compared with frequent replacement and conventional daily wear contact lenses. CLAO J. 1996;22:250–257.
27. Hamano H, Watanabe K, Hamano T, Mitsunaga S, Kotani S, Okada A. A study of the complications induced by conventional and disposable contact lenses. CLAO J. 1994;20:103–108.
28. Young G. Diligent disinfection in 49 steps. Cont Lens Spectr. 2012;27:53.
29. Sulley A, Dumbleton K. Silicone hydrogel daily disposable benefits: the evidence. Cont Lens Anterior Eye. 2020;43:298–307. doi:10.1016/j.clae.2020.02.001
30. Cho P, Boost MV. Daily disposable lenses: the better alternative. Cont Lens Anterior Eye. 2013;36:4–12. doi:10.1016/j.clae.2012.10.073
31. Morgan PB, Efron N, Woods CA, Jones D, Jones L, Nichols JJ. International trends in daily disposable contact lens prescribing (2000–2023): an update. Cont Lens Anterior Eye. 2024;47:102259. doi:10.1016/j.clae.2024.102259
32. Dumbleton K, Caffery B, Dogru M, et al; Members of the TIWoCLD. The TFOS International Workshop on Contact Lens Discomfort: report of the subcommittee on epidemiology. Invest Ophthalmol Vis Sci. 2013;54:TFOS20–36. doi:10.1167/iovs.13-13125
33. Sulley A, Young G, Hunt C, McCready S, Targett MT, Craven R. Retention rates in new contact lens wearers. Eye Cont Lens. 2018;44(Suppl 1):S273–S282. doi:10.1097/ICL.0000000000000402
34. Nichols JJ, Willcox MD, Bron AJ, et al; Members of the TIWoCLD. The TFOS International Workshop on Contact Lens Discomfort: executive summary. Invest Ophthalmol Vis Sci. 2013;54:TFOS7–TFOS13. doi:10.1167/iovs.13-13212
35. Pucker AD, Tichenor AA. A review of contact lens dropout. Clin Optom. 2020;12:85–94. doi:10.2147/OPTO.S198637
36. Jones L, Powell CH. Uptake and release phenomena in contact lens care by silicone hydrogel lenses. Eye Cont Lens. 2013;39:29–36. doi:10.1097/ICL.0b013e31827d4f25
37. Craig JP, Willcox MD, Argueso P, et al.; Members of TIWoCLD. The TFOS International Workshop on Contact Lens Discomfort: report of the contact lens interactions with the tear film subcommittee. Invest Ophthalmol Vis Sci. 2013;54:TFOS123–56. doi:10.1167/iovs.13-13235
38. Efron N, Jones L, Bron AJ, et al; Members of the TIWoCLD. The TFOS International Workshop on Contact Lens Discomfort: report of the contact lens interactions with the ocular surface and adnexa subcommittee. Invest Ophthalmol Vis Sci. 2013;54:TFOS98–TFOS122. doi:10.1167/iovs.13-13187
39. Willcox M, Keir N, Maseedupally V, et al. BCLA CLEAR-contact lens wettability, cleaning, disinfection and interactions with tears. Cont Lens Anterior Eye. 2021;44:157–191. doi:10.1016/j.clae.2021.02.004
40. Cope JR, Collier SA, Rao MM, et al. Contact lens wearer demographics and risk behaviors for contact lens-related eye infections—United States, 2014. MMWR Morb Mortal Wkly Rep. 2015;64:865–870. doi:10.15585/mmwr.mm6432a2
41. Jones L, Brennan NA, Gonzalez-Meijome J, et al; Members of the TIWoCLD. The TFOS International Workshop on Contact Lens Discomfort: report of the contact lens materials, design, and care subcommittee. Invest Ophthalmol Vis Sci. 2013;54:TFOS37–70. doi:10.1167/iovs.13-13215
42. Morgan PB, Sulley AL. Challenges to the new soft contact lens wearer and strategies for clinical management. Cont Lens Anterior Eye. 2023;46:101827. doi:10.1016/j.clae.2023.101827
43. Kuc CJ, Lebow KA. Contact lens solutions and contact lens discomfort: examining the correlations between solution components, keratitis, and contact lens discomfort. Eye Cont Lens. 2018;44:355–366. doi:10.1097/ICL.0000000000000458
44. Stapleton F, Tan J. Impact of contact lens material, design, and fitting on discomfort. Eye Cont Lens. 2017;43:32–39. doi:10.1097/ICL.0000000000000318
45. Chalmers R. Overview of factors that affect comfort with modern soft contact lenses. Cont Lens Anterior Eye. 2014;37:65–76. doi:10.1016/j.clae.2013.08.154
46. Guillon M. Are silicone hydrogel contact lenses more comfortable than hydrogel contact lenses? Eye Cont Lens. 2013;39:86–92. doi:10.1097/ICL.0b013e31827cb99f
47. Menzies KL, Jones L. In vitro analysis of the physical properties of contact lens blister pack solutions. Optom Vis Sci. 2011;88:493–501. doi:10.1097/OPX.0b013e3181ff9d39
48. Guillon M, Allary J-C, Guillon J-P, Orsborn G. Clinical management of regular replacement: part I. Selection of replacement frequency. Intl Cont Lens Clinic. 1992;19:104–120. doi:10.1016/0892-8967(92)90038-F
49. Jones L, Hui A, Phan CM, et al. CLEAR - Contact lens technologies of the future. Cont Lens Anterior Eye. 2021;44:398–430. doi:10.1016/j.clae.2021.02.007
50. Rykowska I, Nowak I, Nowak R. Soft contact lenses as drug delivery systems: a review. Molecules. 2021;26:5577. doi:10.3390/molecules26185577
51. Yang Y, Lockwood A. Topical ocular drug delivery systems: innovations for an unmet need. Exp Eye Res. 2022;218:109006. doi:10.1016/j.exer.2022.109006
52. Guzman-Aranguez A, Fonseca B, Carracedo G, Martin-Gil A, Martinez-Aguila A, Pintor J. Dry eye treatment based on contact lens drug delivery: a review. Eye Cont Lens. 2016;42:280–288. doi:10.1097/ICL.0000000000000184
53. Peterson RC, Wolffsohn JS, Nick J, Winterton L, Lally J. Clinical performance of daily disposable soft contact lenses using sustained release technology. Cont Lens Anterior Eye. 2006;29:127–134. doi:10.1016/j.clae.2006.03.004
54. Muller C, Marx S, Wittekind J, Sickenberger W. Subjective comparison of pre-lens tear film stability of daily disposable contact lenses using ring mire projection. Clin Optom. 2020;12:17–26. doi:10.2147/OPTO.S235167
55. Winterton LC, Lally JM, Sentell KB, Chapoy LL. The elution of poly (vinyl alcohol) from a contact lens: the realization of a time release moisturizing agent/artificial tear. J Biomed Mater Res B Appl Biomater. 2007;80:424–432. doi:10.1002/jbm.b.30613
56. Phan CM, Subbaraman LN, Jones LW. Uptake and release of polyvinyl alcohol from hydrogel daily disposable contact lenses. Optom Vis Sci. 2019;96:180–186. doi:10.1097/OPX.0000000000001351
57. Pruitt J, Lindley K, Winterton L. Triple-action moisturisers for increased comfort in daily disposable lenses. Optician. 2007;234:27–28.
58. Zheng Y, Dou J, Wang Y, et al. Sustained release of a polymeric wetting agent from a silicone-hydrogel contact lens material. ACS Omega. 2022;7:29223–29230. doi:10.1021/acsomega.2c03310
59. Maulvi FA, Soni TG, Shah DO. Extended release of hyaluronic acid from hydrogel contact lenses for dry eye syndrome. J Biomater Sci Polym Ed. 2015;26:1035–1050. doi:10.1080/09205063.2015.1072902
60. Liu L, Jones L, Sheardown H. Wetting agent release from contact lenses. Invest Ophthalmol Vis Sci. 2005;46:908. doi:10.1167/iovs.04-0362
61. Ali M, Byrne ME. Controlled release of high molecular weight hyaluronic Acid from molecularly imprinted hydrogel contact lenses. Pharm Res. 2009;26:714–726. doi:10.1007/s11095-008-9818-6
62. Weeks A, Subbaraman LN, Jones L, Sheardown H. Physical entrapment of hyaluronic acid during synthesis results in extended release from model hydrogel and silicone hydrogel contact lens materials. Eye Cont Lens. 2013;39:179–185. doi:10.1097/ICL.0b013e318281ae06
63. Mahomed A, Tighe B. Contact lenses and comfort enhancers: in vivo and in vitro release of soluble PVA. Ophthalmic Res. 2004;36:34.
64. Suja VC, Verma A, Mossige E, et al. Dewetting characteristics of contact lenses coated with wetting agents. J Colloid Interface Sci. 2022;614:24–32. doi:10.1016/j.jcis.2022.01.075
65. Phan CM, Walther H, Riederer D, et al. Analysis of polyvinyl alcohol release from commercially available daily disposable contact lenses using an in vitro eye model. J Biomed Mater Res B Appl Biomater. 2019;107:1662–1668. doi:10.1002/jbm.b.34259
66. Tonge S, Jones L, Goodall S, Tighe B. The ex vivo wettability of soft contact lenses. Curr Eye Res. 2001;23:51–59. doi:10.1076/ceyr.23.1.51.5418
67. Lin MC, Svitova TF. Contact lenses wettability in vitro: effect of surface-active ingredients. Optom Vis Sci. 2010;87:440–447. doi:10.1097/OPX.0b013e3181dc9a1a
68. Menzies KL, Rogers R, Jones L. In vitro contact angle analysis and physical properties of blister pack solutions of daily disposable contact lenses. Eye Cont Lens. 2010;36:10–18. doi:10.1097/ICL.0b013e3181c5b385
69. Ketelson HA, Meadows DL, Stone RP. Dynamic wettability properties of a soft contact lens hydrogel. Colloids Surf B Biointerfaces. 2005;40:1–9. doi:10.1016/j.colsurfb.2004.07.010
70. Phan CM, Walther H, Smith RW, et al. Determination of the release of PEG and HPMC from nelfilcon A daily disposable contact lenses using a novel in vitro eye model. J Biomater Sci Polym Ed. 2018;29:2124–2136. doi:10.1080/09205063.2018.1514192
71. Maldonado-Codina C, Morgan PB. In vitro water wettability of silicone hydrogel contact lenses determined using the sessile drop and captive bubble techniques. J Biomed Mater Res A. 2007;83:496–502. doi:10.1002/jbm.a.31260
72. Kitamata-Wong B, Yuen T, Li W, Svitova T, Zhou Y, Lin MC. Effects of lens-care solutions on hydrogel lens performance. Optom Vis Sci. 2017;94:1036–1046. doi:10.1097/OPX.0000000000001125
73. Pinto-Fraga J, Blazquez Arauzo F, Urbano Rodriguez R, Gonzalez-Garcia MJ. Evaluation of safety and efficacy of a new multipurpose disinfecting solution on silicone hydrogel contact lenses. J Optom. 2015;8:40–47. doi:10.1016/j.optom.2014.07.004
74. Tilia D, Lazon de la Jara P, Weng R, Naduvilath T, Willcox MD. Short-term clinical comparison of two dual-disinfection multipurpose disinfecting solutions. Eye Cont Lens. 2014;40:7–11. doi:10.1097/01.ICL.0000436270.08502.d3
75. Guillon M, Maissa C, Wong S, Patel T, Garofalo R. Effect of lens care system on silicone hydrogel contact lens wettability. Cont Lens Anterior Eye. 2015;38:435–441. doi:10.1016/j.clae.2015.06.007
76. Lira M, Silva R. Effect of lens care systems on silicone hydrogel contact lens hydrophobicity. Eye Cont Lens. 2017;43:89–94. doi:10.1097/ICL.0000000000000247
77. Stiegemeier MJ, Friederichs GJ, Hughes JL, Larsen S, Movic W, Potter WB. Clinical evaluation of a new multi-purpose disinfecting solution in symptomatic contact lens wearers. Cont Lens Anterior Eye. 2006;29:143–151. doi:10.1016/j.clae.2006.03.006
78. Corbin GS, Kading DL, Powell SM, et al. Clinical evaluation of a new multi-purpose disinfecting solution in symptomatic wearers of silicone hydrogel contact lenses. Clin Optom. 2012;4:13.
79. Yang SN, Tai YC, Sheedy JE, Kinoshita B, Lampa M, Kern JR. Comparative effect of lens care solutions on blink rate, ocular discomfort and visual performance. Ophthalmic Physiol Opt. 2012;32:412–420. doi:10.1111/j.1475-1313.2012.00922.x
80. Muya L, Scott A, Alvord L, Nelson J. Wetting substantivity of a new hydrogen peroxide disinfecting solution on silicone hydrogel contact lenses. Cont Lens Anterior Eye. 2018;41:S15–S16. doi:10.1016/j.clae.2018.04.128
81. Simmons PA, Donshik PC, Kelly WF, Vehige JG. Conditioning of hydrogel lenses by a multipurpose solution containing an ocular lubricant. CLAO J. 2001;27:192–194.
82. Pucker AD. A review of the compatibility of topical artificial tears and rewetting drops with contact lenses. Cont Lens Anterior Eye. 2020;43:426–432. doi:10.1016/j.clae.2020.04.013
83. Pastrana C, Carpena-Torres C, Rodriguez-Pomar C, Martin-Gil A, Carracedo G. Improvement of soft contact lens wettability after the instillation of hyaluronic acid eye drops. Eye Cont Lens. 2023;49:120–126. doi:10.1097/ICL.0000000000000955
84. Golding TR, Efron N, Brennan NA. Soft lens lubricants and prelens tear film stability. Optom Vis Sci. 1990;67:461–465. doi:10.1097/00006324-199006000-00011
85. Chen Q, Wang J, Tao A, Shen M, Jiao S, Lu F. Ultrahigh-resolution measurement by optical coherence tomography of dynamic tear film changes on contact lenses. Invest Ophthalmol Vis Sci. 2010;51:1988–1993. doi:10.1167/iovs.09-4389
86. Nichols JJ, Lievens CW, Bloomenstein MR, Liu H, Simmons P, Vehige J. Dual-polymer drops, contact lens comfort, and lid wiper epitheliopathy. Optom Vis Sci. 2016;93:979–986. doi:10.1097/OPX.0000000000000878
87. Phan CM, Wy Chan V, Drolle E, et al. Evaluating the in vitro wettability and coefficient of friction of a novel and contemporary reusable silicone hydrogel contact lens materials using an in vitro blink model. Cont Lens Anterior Eye. 2024;47:102129. doi:10.1016/j.clae.2024.102129
88. Yanez F, Concheiro A, Alvarez-Lorenzo C. Macromolecule release and smoothness of semi-interpenetrating PVP-pHEMA networks for comfortable soft contact lenses. Eur J Pharm Biopharm. 2008;69:1094–1103. doi:10.1016/j.ejpb.2008.01.023
89. White CJ, McBride MK, Pate KM, Tieppo A, Byrne ME. Extended release of high molecular weight hydroxypropyl methylcellulose from molecularly imprinted, extended wear silicone hydrogel contact lenses. Biomaterials. 2011;32:5698–5705. doi:10.1016/j.biomaterials.2011.04.044
90. Fagehi R, Pearce EI, Oliver K, Abusharha AA, Tomlinson A. Care solution effects on contact lens in vivo wettability. Clin Exp Optom. 2017;100:623–632. doi:10.1111/cxo.12518
91. Scheuer CA, Fridman KM, Barniak VL, Burke SE, Venkatesh S. Retention of conditioning agent hyaluronan on hydrogel contact lenses. Cont Lens Anterior Eye. 2010;33(Suppl 1):S2–6. doi:10.1016/j.clae.2010.10.003
92. Pitt WG, Jack DR, Zhao Y, Nelson JL, Pruitt JD. Loading and release of a phospholipid from contact lenses. Optom Vis Sci. 2011;88:502–506. doi:10.1097/OPX.0b013e31820e9ff8
93. Pitt WG, Jack DR, Zhao Y, Nelson JL, Pruitt JD. Transport of phospholipid in silicone hydrogel contact lenses. J Biomater Sci Polym Ed. 2012;23:527–541. doi:10.1163/092050611X554174
94. Lum E, Perera I, Ho A. Osmolality and buffering agents in soft contact lens packaging solutions. Cont Lens Anterior Eye. 2004;27:21–26. doi:10.1016/j.clae.2003.11.002
95. Nagyova B, Tiffany JM. Components responsible for the surface tension of human tears. Curr Eye Res. 1999;19:4–11. doi:10.1076/ceyr.19.1.4.5341
96. Goda T, Ishihara K. Soft contact lens biomaterials from bioinspired phospholipid polymers. Expert Rev Med Devices. 2006;3:167–174. doi:10.1586/17434440.3.2.167
97. Li Z, Cheng H, Ke L, et al. Recent advances in new copolymer hydrogel‐formed contact lenses for ophthalmic drug delivery. ChemNanoMat. 2021;7:564–579. doi:10.1002/cnma.202100008
98. Willis SL, Court JL, Redman RP, et al. A novel phosphorylcholine-coated contact lens for extended wear use. Biomaterials. 2001;22:3261–3272. doi:10.1016/S0142-9612(01)00164-8
99. Baker MI, Walsh SP, Schwartz Z, Boyan BD. A review of polyvinyl alcohol and its uses in cartilage and orthopedic applications. J Biomed Mater Res B Appl Biomater. 2012;100:1451–1457. doi:10.1002/jbm.b.32694
100. Rah MJ. A review of hyaluronan and its ophthalmic applications. Optometry. 2011;82:38–43. doi:10.1016/j.optm.2010.08.003
101. Salwowska NM, Bebenek KA, Zadlo DA, Wcislo-Dziadecka DL. Physiochemical properties and application of hyaluronic acid: a systematic review. J Cosmet Dermatol. 2016;15:520–526. doi:10.1111/jocd.12237
102. Powell CH, Lally JM, Hoong LD, Huth SW. Lipophilic versus hydrodynamic modes of uptake and release by contact lenses of active entities used in multipurpose solutions. Cont Lens Anterior Eye. 2010;33:9–18. doi:10.1016/j.clae.2009.10.006
103. Green JA, Phillips KS, Hitchins VM, et al. Material properties that predict preservative uptake for silicone hydrogel contact lenses. Eye Cont Lens. 2012;38:350–357. doi:10.1097/ICL.0b013e318272c470
104. Jones L, Jones D, Houlford M. Clinical comparison of three polyhexanide-preserved multi-purpose contact lens solutions. Cont Lens Anterior Eye. 1997;20:23–30. doi:10.1016/S1367-0484(97)80032-X
105. Jones L, MacDougall N, Sorbara LG. Asymptomatic corneal staining associated with the use of balafilcon silicone-hydrogel contact lenses disinfected with a polyaminopropyl biguanide-preserved care regimen. Optom Vis Sci. 2002;79:753–761. doi:10.1097/00006324-200212000-00007
106. Willcox MD, Phillips B, Ozkan J, et al. Interactions of lens care with silicone hydrogel lenses and effect on comfort. Optom Vis Sci. 2010;87:839–846. doi:10.1097/OPX.0b013e3181f3e2fc
107. Khan TF, Price BL, Morgan PB, Maldonado-Codina C, Dobson CB. Cellular fluorescein hyperfluorescence is dynamin-dependent and increased by Tetronic 1107 treatment. Int J Biochem Cell Biol. 2018;101:54–63. doi:10.1016/j.biocel.2018.05.011
108. Jones L, Senchyna M. Soft contact lens solutions review: part 1 - components of modern care regimens. Optometry Pract. 2007;8:45–56.
109. Huo Y, Ketelson H, Perry SS. Ethylene oxide-block-butylene oxide copolymer uptake by silicone hydrogel contact lens materials. Appl Surf Sci. 2013;273:472–477. doi:10.1016/j.apsusc.2013.02.064
110. Nichols JJ, Mitchell GL, King-Smith PE. The impact of contact lens care solutions on the thickness of the tear film and contact lens. Cornea. 2005;24:825–832. doi:10.1097/01.ico.0000157904.52305.29
111. Morris CA, Maltseva IA, Rogers VA, et al. Consequences of preservative uptake and release by contact lenses. Eye Cont Lens. 2018;44(Suppl 2):S247–S255. doi:10.1097/ICL.0000000000000480
112. Yee A, Phan CM, Chan VWY, Heynen M, Jones L. Uptake and release of a Multipurpose Solution Biocide (MAP-D) from hydrogel and silicone hydrogel contact lenses using a radiolabel methodology. Eye Cont Lens. 2021;47:249–255. doi:10.1097/ICL.0000000000000724
113. Yee A, Phan CM, Jones L. Uptake and release of polyhexamethylene biguanide (PHMB) from hydrogel and silicone hydrogel contact lenses using a radiolabel methodology. Cont Lens Anterior Eye. 2022;45:101575. doi:10.1016/j.clae.2022.101575
114. McDonald M, Schachet JL, Lievens CW, Kern JR. Systane(R) ultra lubricant eye drops for treatment of contact lens-related dryness. Eye Cont Lens. 2014;40:106–110. doi:10.1097/ICL.0000000000000018
115. Snibson GR, Greaves JL, Soper ND, Tiffany JM, Wilson CG, Bron AJ. Ocular surface residence times of artificial tear solutions. Cornea. 1992;11:288–293. doi:10.1097/00003226-199207000-00003
116. White CJ, Thomas CR, Byrne ME. Bringing comfort to the masses: a novel evaluation of comfort agent solution properties. Cont Lens Anterior Eye. 2014;37:81–91. doi:10.1016/j.clae.2013.07.004
117. Iwashita H, Itokawa T, Suzuki T, Okajima Y, Kakisu K, Hori Y. Evaluation of in vitro wettability of soft contact lenses using tear supplements. Eye Cont Lens. 2021;47:244–248. doi:10.1097/ICL.0000000000000698
118. Subbaraman LN, Bayer S, Glasier MA, Lorentz H, Senchyna M, Jones L. Rewetting drops containing surface active agents improve the clinical performance of silicone hydrogel contact lenses. Optom Vis Sci. 2006;83:143–151. doi:10.1097/01.opx.0000204513.76568.57
119. Aragona P, Simmons PA, Wang H, Wang T. Physicochemical properties of hyaluronic acid-based lubricant eye drops. Transl Vis Sci Technol. 2019;8:2. doi:10.1167/tvst.8.6.2
120. Asharlous A, Mirzajani A, Jafarzadehpur E, KhabazKhoob M, Ostadimoghaddam H. Objective and subjective assessing efficacy of a lubricating drop in eyes wearing silicone hydrogel contact lenses. J Curr Ophthalmol. 2016;28:69–74. doi:10.1016/j.joco.2016.03.007
121. Coles ML, Brennan NA, Shuley V, et al. The influence of lens conditioning on signs and symptoms with new hydrogel contact lenses. Clin Exp Optom. 2004;87:367–371. doi:10.1111/j.1444-0938.2004.tb03096.x
122. Efron N, Golding TR, Brennan NA. The effect of soft lens lubricants on symptoms and lens dehydration. CLAO J. 1991;17:114–119.
123. Caron P, St-Jacques J, Michaud L. Clinical discussion on the relative efficacy of 2 surfactant-containing lubricating agents in removing proteins during contact lens wear. Optometry. 2007;78:23–29. doi:10.1016/j.optm.2006.06.017
124. Ozkan J, Papas E. Lubricant effects on low Dk and silicone hydrogel lens comfort. Optom Vis Sci. 2008;85:773–777. doi:10.1097/OPX.0b013e3181819f37
125. Chandrinos A, Tzamouranis D. Dry eye, contact lenses and preservatives in glaucoma medication. Clin Ophthalmol J. 2019;1:1003.
126. Phan CM, Bajgrowicz M, Gao H, Subbaraman LN, Jones LW. Release of fluconazole from contact lenses using a novel in vitro eye model. Optom Vis Sci. 2016;93:387–394. doi:10.1097/OPX.0000000000000760
127. Bajgrowicz M, Phan CM, Subbaraman LN, Jones L. Release of ciprofloxacin and moxifloxacin from daily disposable contact lenses from an in vitro eye model. Invest Ophthalmol Vis Sci. 2015;56:2234–2242. doi:10.1167/iovs.15-16379
128. Morgan PB, Efron N. Global contact lens prescribing 2000–2020. Clin Exp Optom. 2022;105:298–312. doi:10.1080/08164622.2022.2033604
129. Efron N, Efron SE, Morgan PB, Morgan SL. A ‘cost-per-wear’ model based on contact lens replacement frequency. Clin Exp Optom. 2010;93:253–260. doi:10.1111/j.1444-0938.2010.00488.x
130. Smith SL, Orsborn GN, Sulley A, Chatterjee NB, Morgan PB. An investigation into disposal and recycling options for daily disposable and monthly replacement soft contact lens modalities. Cont Lens Anterior Eye. 2022;45:101435. doi:10.1016/j.clae.2021.03.002
131. Morgan PB, Woods CA, Tranoudis IG, et al. International contact lens prescribing in 2022. Cont Lens Spectr. 2023;38:28–35.
132. Morgan PB, Woods CA, Tranoudis IG, et al. International contact lens prescribing in 2018. Cont Lens Spectr. 2019;34:26–32.
133. Morgan PB, Woods CA, Tranoudis IG, et al. International contact lens prescribing in 2019. Cont Lens Spectr. 2020;35:26–32.
134. Morgan PB, Woods CA, Tranoudis IG, et al. International contact lens prescribing in 2020. Cont Lens Spectr. 2021;36:26–32.
135. Muhafiz E, Bayhan HA, Sahin S, Gocmen AY, Aslan Bayhan S, Gurdal C. Evaluation of the ocular surface in different contact lens replacement schedules. Cornea. 2019;38:587–594. doi:10.1097/ICO.0000000000001870
136. Chalmers RL, Keay L, McNally J, Kern J. Multicenter case-control study of the role of lens materials and care products on the development of corneal infiltrates. Optom Vis Sci. 2012;89:316–325. doi:10.1097/OPX.0b013e318240c7ff
137. Chalmers RL, Wagner H, Mitchell GL, et al. Age and other risk factors for corneal infiltrative and inflammatory events in young soft contact lens wearers from the Contact Lens Assessment in Youth (CLAY) study. Invest Ophthalmol Vis Sci. 2011;52:6690–6696. doi:10.1167/iovs.10-7018
138. Steele KR, Szczotka-Flynn L. Epidemiology of contact lens-induced infiltrates: an updated review. Clin Exp Optom. 2017;100:473–481. doi:10.1111/cxo.12598
139. Radford CF, Minassian D, Dart JK, Stapleton F, Verma S. Risk factors for nonulcerative contact lens complications in an ophthalmic accident and emergency department: a case-control study. Ophthalmology. 2009;116:385–392. doi:10.1016/j.ophtha.2008.09.053
140. Szczotka-Flynn L, Diaz M. Risk of corneal inflammatory events with silicone hydrogel and low dk hydrogel extended contact lens wear: a meta-analysis. Optom Vis Sci. 2007;84:247–256. doi:10.1097/OPX.0b013e3180421c47
141. Yeung KK, Davis R. The environmental impact of contact lens waste. Cont Lens Spectr. 2019;34:27–30.
142. Morgan PB, Woods CA, Tranoudis IG, et al. International contact lens prescribing in 2021. Cont Lens Anterior Eye. 2022;37:32–38.
143. Dumbleton K, Woods C, Jones L, Richter D, Fonn D. Comfort and vision with silicone hydrogel lenses: effect of compliance. Optom Vis Sci. 2010;87:421–425. doi:10.1097/OPX.0b013e3181d95aea
144. Efron N. All soft contact lenses should be silicone hydrogel daily disposables. Clin Exp Optom. 2024;2024:1–3.
145. Donshik PC, Ehlers WH, Anderson LD, Suchecki JK. Strategies to better engage, educate, and empower patient compliance and safe lens wear: compliance: what we know, what we do not know, and what we need to know. Eye ContLens. 2007;33:430–3; discussion434. doi:10.1097/ICL.0b013e318157f62a
146. McMonnies CW. Improving patient education and attitudes toward compliance with instructions for contact lens use. Cont Lens Anterior Eye. 2011;34:241–248. doi:10.1016/j.clae.2011.06.007
147. Bui TH, Cavanagh HD, Robertson DM. Patient compliance during contact lens wear: perceptions, awareness, and behavior. Eye Cont Lens. 2010;36:334–339. doi:10.1097/ICL.0b013e3181f579f7
148. Yeung KK, Forister JF, Forister EF, Chung MY, Han S, Weissman BA. Compliance with soft contact lens replacement schedules and associated contact lens-related ocular complications: the UCLA Contact Lens Study. Optometry. 2010;81:598–607. doi:10.1016/j.optm.2010.01.013
149. Hickson-Curran S, Chalmers RL, Riley C. Patient attitudes and behavior regarding hygiene and replacement of soft contact lenses and storage cases. Cont Lens Anterior Eye. 2011;34:207–215. doi:10.1016/j.clae.2010.12.005
150. Robertson DM, Cavanagh HD. Non-compliance with contact lens wear and care practices: a comparative analysis. Optom Vis Sci. 2011;88:1402–1408. doi:10.1097/OPX.0b013e3182333cf9
151. Cope JR, Collier SA, Nethercut H, Jones JM, Yates K, Yoder JS. Risk behaviors for contact lens-related eye infections among adults and adolescents - United States, 2016. MMWR Morb Mortal Wkly Rep. 2017;66:841–845. doi:10.15585/mmwr.mm6632a2
152. Rueff EM, Wolfe J, Bailey MD. A study of contact lens compliance in a non-clinical setting. Cont Lens Anterior Eye. 2019;42:557–561. doi:10.1016/j.clae.2019.03.001
153. Wolffsohn JS, Dumbleton K, Huntjens B, et al. CLEAR - evidence-based contact lens practice. Cont Lens Anterior Eye. 2021;44:368–397. doi:10.1016/j.clae.2021.02.008
154. Alonso S, Yela S, Cardona G. Are patients sufficiently informed about contact lens wear and care? Optom Vis Sci. 2022;99:853–858. doi:10.1097/OPX.0000000000001964
155. Dumbleton K, Woods C, Jones L, Fonn D, Sarwer DB. Patient and practitioner compliance with silicone hydrogel and daily disposable lens replacement in the United States. Eye Cont Lens. 2009;35:164–171. doi:10.1097/ICL.0b013e3181ac4a8d
156. Dumbleton K, Richter D, Woods C, Jones L, Fonn D. Compliance with contact lens replacement in Canada and the United States. Optom Vis Sci. 2010;87:131–139. doi:10.1097/OPX.0b013e3181ca32dc
157. Richter D, Dumbleton K, Guthrie S, Woods C, Jones L, Fonn D. Patient and practitioner compliance with silicone hydrogel and daily disposable lens replacement in Canada. Can J Optom. 2010;72:10.
158. Sapkota K, Franco S, Lira M. Daily versus monthly disposable contact lens: which is better for ocular surface physiology and comfort? Cont Lens Anterior Eye. 2018;41:252–257. doi:10.1016/j.clae.2017.12.005
159. Jones L, Mann A, Evans K, Franklin V, Tighe B. An in vivo comparison of the kinetics of protein and lipid deposition on group II and group IV frequent-replacement contact lenses. Optom Vis Sci. 2000;77:503–510. doi:10.1097/00006324-200010000-00004
160. Walther H, Lorentz H, Heynen M, Kay L, Jones LW. Factors that influence in vitro cholesterol deposition on contact lenses. Optom Vis Sci. 2013;90:1057–1065. doi:10.1097/OPX.0000000000000022
161. Omali NB, Subbaraman LN, Coles-Brennan C, Fadli Z, Jones LW. Biological and clinical implications of lysozyme deposition on soft contact lenses. Optom Vis Sci. 2015;92:750–757. doi:10.1097/OPX.0000000000000615
162. Chow LM, Subbaraman LN, Sheardown H, Jones L. Kinetics of in vitro lactoferrin deposition on silicone hydrogel and FDA group II and group IV hydrogel contact lens materials. J Biomater Sci Polym Ed. 2009;20:71–82. doi:10.1163/156856208X393509
163. Subbaraman LN, Glasier MA, Senchyna M, Sheardown H, Jones L. Kinetics of in vitro lysozyme deposition on silicone hydrogel, PMMA, and FDA groups I, II, and IV contact lens materials. Curr Eye Res. 2006;31:787–796. doi:10.1080/02713680600888799
164. Subbaraman LN, Jones L. Kinetics of lysozyme activity recovered from conventional and silicone hydrogel contact lens materials. J Biomater Sci Polym Ed. 2010;21:343–358. doi:10.1163/156856209X415873
165. Bergenske P. The winning combination: disposable lenses for daily wear. Cont Lens Spectr. 1990;5:72–74.
166. Jones L, Franklin V, Evans K, Sariri R, Tighe B. Spoilation and clinical performance of monthly vs. three monthly Group II disposable contact lenses. Optom Vis Sci. 1996;73:16–21. doi:10.1097/00006324-199601000-00003
167. Jones L, Evans K, Sariri R, Franklin V, Tighe B. Lipid and protein deposition of N-vinyl pyrrolidone-containing group II and group IV frequent replacement contact lenses. CLAO J. 1997;23:122–126.
168. Tighe BJ, Jones L, Evans K, Franklin V. Patient-dependent and material-dependent factors in contact lens deposition processes. Adv Exp Med Biol. 1998;438:745–751.
169. Fonn D. Targeting contact lens induced dryness and discomfort: what properties will make lenses more comfortable. Optom Vis Sci. 2007;84:279–285. doi:10.1097/OPX.0b013e31804636af
170. McMonnies CW. Mechanisms for the symptoms of dryness in soft contact lens wearers. Expert Rev Ophthalmol. 2023;18:327–335. doi:10.1080/17469899.2023.2259613
171. Rueff EM. Visual discomfort and contact lens wear: a review. Cont Lens Anterior Eye. 2023;46:101872. doi:10.1016/j.clae.2023.101872
172. Papas EB, Ciolino JB, Jacobs D, et al; Members of the TIWoCLD. The TFOS International Workshop on Contact Lens Discomfort: report of the management and therapy subcommittee. Invest Ophthalmol Vis Sci. 2013;54:TFOS183–203. doi:10.1167/iovs.13-13166
173. Morgan PB, Murphy PJ, Gifford KL, et al. BCLA CLEAR-effect of contact lens materials and designs on the anatomy and physiology of the eye. Cont Lens Anterior Eye. 2021;44:192–219. doi:10.1016/j.clae.2021.02.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comfort After Refitting Symptomatic Habitual Reusable Toric Lens Wearers with a New Daily Disposable Contact Lens for Astigmatism
Wan K, Mashouf J, Hall B
Clinical Ophthalmology 2023, 17:3235-3241
Published Date: 30 October 2023