")
Back to Journals » Infection and Drug Resistance » Volume 17
The Impact of Early Antibiotic Use on Clinical Outcomes of Patients Hospitalized with COVID-19: A Propensity Score-Matched Analysis
Authors Duan Y , Ren J, Wang J, Wang S, Zhang R, Zhang H, Hu J, Deng W, Li W , Chen B
Received 24 May 2024
Accepted for publication 29 July 2024
Published 9 August 2024 Volume 2024:17 Pages 3425—3438
DOI https://doi.org/10.2147/IDR.S470957
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sandip Patil
Yishan Duan,1,* Jing Ren,2,* Jing Wang,3,* Suyan Wang,4 Rui Zhang,1 Huohuo Zhang,1 Jinrui Hu,1 Wen Deng,1 Weimin Li,1,3,4 Bojiang Chen1,3
1Department of Respiratory and Critical Care Medicine, West China Hospital of Sichuan University, Chengdu, Sichuan Province, 610041, People’s Republic of China; 2The Integrated Care Management Center, West China Hospital of Sichuan University, Chengdu, Chengdu, Sichuan Province, 610041, People’s Republic of China; 3Precision Medicine Center, West China Hospital, Sichuan University, Chengdu, Sichuan Province, 610041, People’s Republic of China; 4Frontiers Science Center for Disease-Related Molecular Network, West China Hospital, Sichuan University, Chengdu, Sichuan Province, 610041, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bojiang Chen; Weimin Li, Email [email protected]; [email protected]
Purpose: Early empiric antibiotics were prescribed to numerous patients during the Coronavirus disease 2019 (COVID-19) pandemic. However, the potential impact of empiric antibiotic therapy on the clinical outcomes of patients hospitalized with COVID-19 is yet unknown.
Methods: In this retrospective cohort study, early antibiotics use cohort was defined as control group, which was compared with no antibiotic use and delayed antibiotic use cohorts for all-cause mortality during hospitalization. The 1:2 propensity score matched patient populations were further developed to adjust confounding factors. Survival curves were compared between different cohorts using a Log rank test to assess the early antibiotic effectiveness.
Results: We included a total of 1472 COVID-19 hospitalized patients, of whom 87.4% (1287 patients) received early antibiotic prescriptions. In propensity-score-matched datasets, our analysis comprised 139 patients with non-antibiotic use (with 278 matched controls) and 27 patients with deferred-antibiotic use (with 54 matched controls). Patients with older ages, multiple comorbidities, severe and critical COVID-19 subtypes, higher serum infection indicators, and inflammatory indicators at admission were more likely to receive early antibiotic prescriptions. After adjusting confounding factors likely to influence the prognosis, there is no significant difference in all-cause mortality (HR=1.000(0.246– 4.060), p = 1.000) and ICU admission (HR=0.436(0.093– 2.04), p = 0.293), need for mechanical ventilation (HR=0.723(0.296– 1.763), p = 0.476) and tracheal intubation (HR=1.338(0.221– 8.103), p = 0.751) were observed between early antibiotics use cohort and non-antibiotic use cohort.
Conclusion: Early antibiotics were frequently prescribed to patients in more severe disease condition at admission. However, early antibiotic treatment failed to demonstrate better clinical outcomes in hospitalized patients with COVID-19 in the propensity-score-matched cohorts.
Keywords: Coronavirus disease 2019, COVID-19, early antibiotics use, bacterial co-infections, clinical outcomes
Introduction
The Coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has infected over 700 million people and resulted in over 6 million related fatalities worldwide since December 2019.1 As is known to us all, bacterial co-infection is a common complication of many respiratory viral tract infections and is associated with increased disease severity and mortality.2,3 Patton’s study reported a double 30-day mortality of COVID-19 patients with confirmed bacterial co-infections when compared to influenza virus with bacterial co-infections.4 In the setting of COVID-19, bacterial co-infections were observed to have a profound impact on an increased risk of in-hospital mortality, intensive care unit (ICU) admission, and the need for mechanical ventilation.5,6 During the COVID-19 pandemic, the incidence of gram-positive and gram-negative bacteria co-infections (especially multidrug resistant bacteria) continued to grow.7 Among the bacterial species found in COVID-19 patients, Enterobacteria and carbapenemase-resistant A. baumanni showed high rates of colonization and superinfection, which were associated with high mortality especially in ICU super-infection.8
Whereas, it is challenging to accurately distinguish between viral infection alone and viral combined with bacterial co-infections based on symptoms, clinical-biological or radiological examinations. In addition, COVID-19 itself could lead to increased inflammatory markers (such as procalcitonin (PCT) and C-reactive protein (CRP)) typically associated with bacterial co-infection, which made it more difficult for physicians to diagnose bacterial co-infection at hospital admission.9,10 Considering the increased risk of death and disease progression in COVID-19 patients with bacterial co-infection, nearly three-quarters of patients with COVID-19 have received early empiric antibacterial therapy in the first 6 months of the global pandemic.11,12 Another large, multicenter study also reported that early antibiotics use in patients with COVID-19 accounts for 27% to 84% across different hospitals.11
The COVID-19 pandemic had resulted in a sharp rise in antibiotic usage. Overuse or misuse of antibiotics can lead to an increased risk of adverse events, Clostridium difficile infection and global antimicrobial resistance. Adequate antibiotic management is urgently required to reduce the overprescription of antibiotics. As for different countries and different subtypes of COVID-19 viruses, there have not come to a consensus among the various guidelines on the prescription of antibiotics in hospitalized patients with COVID-19. While some guidelines recommended early empiric antibiotic therapy in severe COVID-19 patients, the 2021 UK National Institute for Health and Care Excellence (NICE) rapid guideline on managing COVID-19 demonstrated that the only recommendation for antibiotics use is when there is a strong clinical or paraclinical suspicion of bacterial infection.13–16 Previous studies have put more emphasis on the rates of antibacterial therapy and microbiologically proven co-infection but ignored the potential impact of early antibiotic therapy on the clinical outcomes of patients hospitalized with COVID-19.17 It is high time to emphasize the appropriate use of antibiotics among patients with COVID-19, and more studies are urgently needed to assess if early antibiotic therapy work to improve the prognosis and survival rate of hospitalized patients with COVID-19.
We conducted a retrospective analysis aimed to evaluate whether early antibacterial therapy is beneficial to improve the prognosis (including mortality, rate of ICU admission, need for tracheal intubation and mechanical ventilation, and length of hospital stays) of hospitalized COVID-19 patients, which could help clinicians to establish better antimicrobial strategy, reduce unnecessary antibiotic exposure and prevent worsening antimicrobial resistance within global healthcare systems.
Methods
Study Design and Patients
We conducted a retrospective cohort study in West China Hospital of Sichuan University, which comprised hospitalized patients with positive real-time reverse transcription polymerase chain reaction (RT-PCR) or rapid antigen test results from an oronasopharyngeal swab for SARS-CoV-2 infection at admission during the period from Dec 2nd, 2022 to Mar 15th, 2023.
This is a retrospective study for follow-up observation of clinical features and prognosis of COVID-19 cohort. All data in this study was extracted from the Electronic Medical Record. The West China Hospital of Sichuan University Ethics Review Committee, in accordance with the principles of the Helsinki Declaration II, approved this research. The authors only had access to anonymized data and had no interaction with patients or patient samples, so The West China Hospital of Sichuan University Ethics Review Committee has approved the waiver for individual patient-informed consent. All analysis was performed in accordance with relevant guidelines and regulations.
We included patients aged ≥16 years old in both the ICU and non‐ICU settings. Patients were eligible for inclusion if their positive oronasopharyngeal swab was identified before hospitalization. Exclusion criteria include: (1) patients discharged within 24 h of admission and patients who were still in hospitalization as of March 15, 2023; (2) positive tests for COVID-19 during hospitalization; (3) patients whose antibiotics course was < 48h; (4) patients who were incidentally admitted during this period (eg, for surgery), and were found to be asymptomatic cases of COVID-19; (5) patients with confirmed positive bacterial culture before admission; and (6) antibiotics were prescribed by confirmed proof of a non-pulmonary microbiological infection (eg, for bacterial skin infections).
Data Collection
Electronic medical records for each patient were collected, including demographic characteristics, body mass index (BMI), former or current smoker, comorbidity (including diabetes, hypertension, chronic kidney disease, chronic hepatic disease, chronic lung diseases, cardiovascular disease, immune system disease, and malignancy), antibiotics prescription records, and disease severity for COVID-19. Laboratory parameters on admission included serum lymphocyte count, PCT, CRP, interleukin-6 (IL-6), D-dimer level, CD4+ T cells, and CD8+ T cells count.
Patients with antibiotic exposure (this study included antibiotics intended for systemic use, which does not include topical antibiotics; and antibiotics in our study pertains to antibacterials drug used to inhibit bacterial growth and kill bacteria) were classified as non-early antibiotic use cohort and early antibiotic use cohort based on whether or not to commence antibiotics within 48 h of hospital admission. Non-early antibiotic use cohort was further categorized as non-antibiotic use cohort and Delayed-antibiotic use according to antibiotics prescription record. Delayed-antibiotic use refers to antibiotic Initial used more than 48 h of hospital admission, yet non-antibiotic use refers to cases that never received antibiotics during their hospital stay.
According to World Health Organization (WHO) definitions of disease severity, COVID-19 has been classified as critical COVID-19, severe COVID-19, and non-severe COVID-19.15 All patients were followed until death in hospital or hospital discharge. The primary outcome was all-cause mortality during hospitalization. Secondary outcomes included initiating mechanical ventilation (including tracheal intubation and non-invasive ventilator), the need for tracheal intubation, ICU admission, and the length of hospital stays.
Propensity Score Matching
Propensity score matching (PSM) refers to the screening of experimental and control groups by certain statistical methods, so that the selected subjects are comparable in terms of potential confounders (applicable to both continuous variables and categorical variables).18 In our study, PSM was used to balance the differences in baseline variables that might confound the impact of early antibiotic use on clinical outcomes of hospitalized COVID-19 patients.18 The following baseline variables were included for propensity score matching: demographic characteristics (age and gender), BMI, current or former smoker, comorbidities, and disease severity for COVID-19. We excluded patients with missing data on any of these baseline variables. Considering great higher number of early-antibiotic treated patients, matched study groups were created using nearest-neighbor 1:2 matching without replacement (each patient with non-antibiotic use and delayed-antibiotic use were matched exactly with two patients with early-antibiotic use).19
Statistical Analyses
All statistical learning methods in our research were chosen based on statistical learning theory. Categorical data were expressed as counts and frequencies (%) and analyzed using Fisher’s exact test or chi-squared test depending on the data. Quantitative variables were expressed as means ± standard deviations (SD) and analyzed by independent‐samples T-test or Mann–Whitney U-test when appropriate. Wilcoxon rank-sum tests or Spearman correlation test was selected by ranked data.
The 1:2 propensity score matched patient populations were established based on the Greedy algorithm using the package MatchIt (Nonparametric Preprocessing for Parametric Causal Inference) in R 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). Balance was assessed within the matched cohorts using the standardized mean difference, with a standardized mean difference <0.100 indicating sufficient balance. Hazard ratios (HRs) with a 95% confidence interval (CI) for each outcome parameter used were estimated using univariate binary logistic regression. Survival curves were generated by the group using the Kaplan–Meier estimator and compared using a Log rank test.
SPSS Statistics Version 26.0 (Armonk, NY) was used for statistical analysis before and after matching. For all comparisons, differences were tested using two-tailed tests, and P < 0.05 was considered to indicate statistical significance.
Results
We identified 4999 patients with a confirmed diagnosis of SARS-CoV-2 infection who were admitted to West China Hospital between Dec 2nd, 2022, and Mar 15th, 2023. A total of 1472 patients were eligible for inclusion and 1287 patients (87.4%) received early antibiotic treatments (Figure 1). Besides, the delayed-antibiotic use cohort and non-antibiotic use cohort include 36 patients and 149 patients, respectively, (The detailed baseline characteristics and laboratory parameters of three cohorts after propensity score matching were listed in Table S1). Beta-lactam antibiotic was the most commonly used antibiotics in our study population. Patients with early antibiotic use were defined as controls.
 |
Figure 1 Identification of delayed-antibiotic use, non-antibiotic use and their matched controls (early-antibiotic use) among patients hospitalized with COVID-19 during the study period. |
The Early Antibiotic Consumption Trending in Patients Hospitalized with COVID-19 Before Propensity Score Matching
Baseline characteristics of three cohorts before 1:2 propensity-score matching are presented in Table 1. Before matching, the non-antibiotic use cohort had a significantly lower age (61.42 ± 19.00 vs 71.24 ± 16.95, p < 0.001) than the controls. More than 50% of the patients were male in all three cohorts. In comparison with the control cohort, the non-antibiotic use cohort had lower prevalence rates of diabetes, chronic kidney disease, chronic lung disease, and cardiovascular disease. Fewer patients with more than 2 types of comorbidities were found in patients with non-antibiotic use (28.2% vs 55.7%, p < 0.001) and delayed-antibiotic use cohort (38.9% vs 55.7%, p = 0.045) than controls. The proportion of patients belonged to severe COVID-19 and critical COVID-19 was identified to be 39.4% and 23.5%, respectively, in the early antibiotic use cohort, which was much higher than that of both delayed-antibiotic use cohort (p<0.001) and non-antibiotic use cohort (p<0.001).
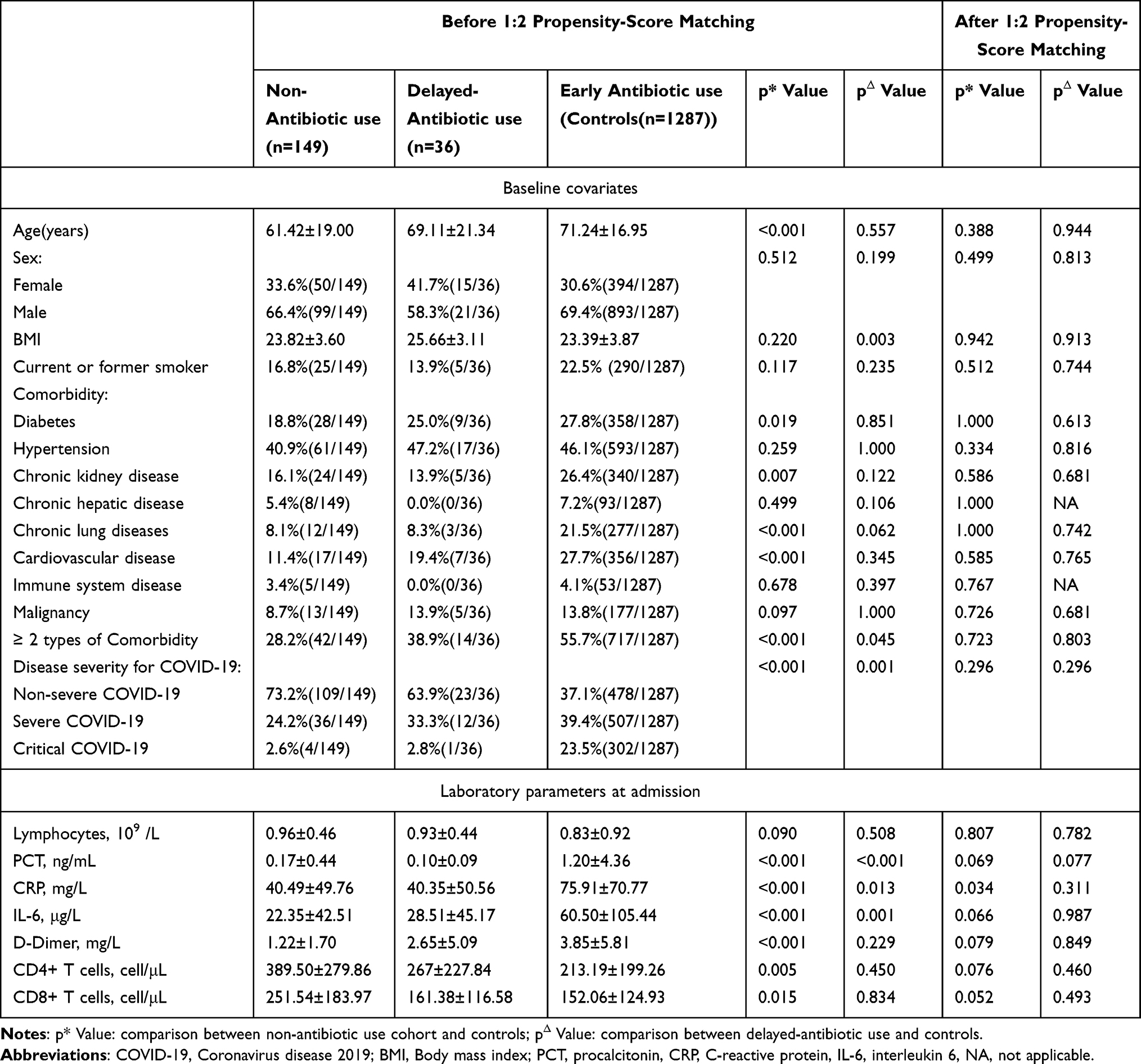 |
Table 1 Baseline Characteristics and Laboratory Parameters of Patients Hospitalized with COVID-19 Before and After Propensity Score Matching |
Among patients with non-antibiotic use, several infectious indicators and inflammatory indicators (including serum PCT (0.17 ± 0.44 VS 1.20 ± 4.36, p < 0.001), CRP (40.49 ± 49.76 VS 75.91 ± 70.77, p < 0.001), IL-6 (22.35 ± 42.51 VS 60.50 ± 105.44, p < 0.001), D-dimer (1.22 ± 1.70 VS 3.85 ± 5.81, p < 0.001)) at admission were much lower than that of control cohort. Furthermore, immune indicators (CD4+T cells (389.50 ± 279.86 VS 213.19 ± 199.26, p = 0.005) and CD8 + T cells count (251.54 ± 183.97 VS 152.06 ± 124.93, p = 0.015)) of patients with non-antibiotic use were observed to be greatly higher than controls. Compared with patients with early antibiotic use, similar lower serum PCT (p < 0.001), CRP (p = 0.013), and IL-6 (p = 0.001) levels were also seen in the delayed-antibiotic use cohort.
During the study period, 190 of the 1287 patients (14.8%) with early antibiotic use died, which was greatly higher than 3.1% of the non-antibiotic use cohort (0.194(95% CI: 0.085–0.443), p < 0.001) (Table 2). What’s more, patients with non-antibiotic use were found to stay in the hospital for a significantly shorter time than controls (10.56 ± 5.89 VS 15.74 ± 10.15, p < 0.001). Among patients with non-antibiotic use, the risk of ICU admission (0.091(95% CI: 0.022–0.369), p = 0.001), need for mechanical ventilation (0.149(95% CI: 0.077–0.285), p < 0.001) and tracheal intubation (0.132(95% CI: 0.032–0.541), p = 0.005) were identified to be much lower than controls. However, there was no significant difference in all-cause mortality, length of hospital stays, and the risk of tracheal intubation between the delayed-antibiotic use cohort and the early antibiotic use cohort. In comparison with the control cohort, a lower risk of ICU admission (p = 0.018) and mechanical ventilation (p = 0.006) were shown in the delayed-antibiotic use cohort.
 |
Table 2 Comparison of Outcomes Parameters Between Patients with Non-Antibiotic Use and Early Antibiotic Use Before and After Propensity Score Matching |
Early Antibiotic Effectiveness in Patients Hospitalized with COVID-19 After Propensity Score Matching
After propensity score matching, our analysis included 139 patients with non-antibiotic use (with 278 matched controls) and 27 patients with delayed-antibiotic use (with 54 matched controls). The baseline characteristics of the case cohorts and matched control cohort were balanced with no significant difference (Table 1). The standard mean differences were greater than 0.1, indicating good balance. With the above methods, 332 patients with early antibiotic use (Figure S1 and Table S2) and 278 patients with antibiotic use (Figure S2 and Table S3) were successfully matched to 166 patients with non-early antibiotic use and 139 patients with non-antibiotic use, respectively. After matching for baseline characteristics, laboratory parameters at admission in the delayed-antibiotic use cohort and non-antibiotic use cohort were found to be not significantly different from corresponding matched controls (except for lower serum CRP level in patients with non-antibiotic use).
Comparison of Outcome Parameters Between Patients with Non-Antibiotic Use, Delayed-Antibiotic Use, and Matched Controls
Further analysis was conducted in propensity-score-matched datasets and observed no evidence of improved outcome parameters in patients who received early antibiotics treatment. Compared with the non-antibiotic use cohort, matched controls did not have lower all-cause mortality (HR = 1.000(0.246–4.060), P = 1.000), lower risk of ICU admission (HR = 0.436(0.093–2.047), P = 0.293), mechanical ventilation (HR = 0.723(0.296–1.763), P = 0.476) and tracheal intubation (HR = 1.338(0.221–8.103), P = 0.751) (Table 2). Similar results were observed in the comparison of outcome parameters between patients with deferred-antibiotic use and matched controls (Table 3). However, patients with non-early antibiotic use, who had a less serious disease condition, tend to stay in the hospital for a significantly shorter time period than matched controls (10.55 ± 5.81 VS 13.88 ± 7.38, P < 0.001).
 |
Table 3 Comparison of Outcomes Parameters Between Patients with Delayed-Antibiotic Use and Early Antibiotic Use Before and After Propensity Score Matching |
In propensity score matching cohorts analysis, Log rank test for comparison of survival curves in the non-antibiotic use cohort versus matched controls (HR = 1.522(95% CI: 0.339–7.109, p = 0.522), delayed-antibiotic use cohort versus matched controls (HR=1.014(95% CI: 0.169–6.086), p = 0.988) had no statistical difference (Figure 2).
 |
Figure 2 Survival curves of patients with the early antibiotic use cohort versus non-antibiotic use cohort, delayed-antibiotic use cohort, non-early antibiotic use cohort, and antibiotic use cohort versus non-antibiotic use cohort. |
Comparison of Outcome Parameters Between Patients with and without Early Antibiotic Use, and Patients with and without Antibiotic Use
The above comparison of outcome parameters was conducted between patients with and without early antibiotic use and patients with and without antibiotic use in propensity-score-matched cohorts. Similarly, both the non-early antibiotic use cohort (Table 4) and the non-antibiotic use cohort (Table 5) showed no statistical difference in all-cause mortality, the risk for ICU admission, mechanical ventilation, and tracheal intubation from that of their respective matched controls.
 |
Table 4 Comparison of Outcomes Parameters Between Patients with and without Early Antibiotic Use Before and After Propensity Score Matching |
 |
Table 5 Comparison of Outcomes Parameters Between Patients with and without Antibiotic Use Before and After Propensity Score Matching |
Survival curves in Figure 2 did not find any significant difference between patients with and without early antibiotic use (HR = 1.143(95% CI: 0.386–3.386), p = 0.387), patients with and without antibiotic use (HR = 1.281(95% CI: 0.393–4.171), p = 0.804).
Discussion
In conclusion, early-antibiotic use was associated with older age, multiple comorbidities, severe and critical COVID-19 subtype, higher serum infectious indicators, and inflammatory indicators at admission. Compared to patients with delayed-antibiotic use and non-antibiotic use cohorts, early antibiotics use in patients hospitalized with COVID-19 had no beneficial effect on all-cause mortality, risk of ICU admission, need for tracheal intubation, and mechanical ventilation after adjusting for baseline characteristics.
The morbidity of bacterial co-infection was highly variable between different respiratory viruses. Other respiratory viral pathogens, such as influenza virus and rhinovirus, may be susceptible to bacterial invasion due to impaired physical barrier, dysregulation of an inflammatory response, and immune response.20 The impact of SARS-CoV-2 on bacterial co-infection remains unclear now. In a meta-analysis of hospitalized ICU and non-ICU COVID-19 patients, only 7% of the patients combined with bacterial co-infection, which was significantly lower than the influenza co-infection rate.21 Consistent with other research, most reported epidemiological investigations from China and Spain also showed similarly low bacterial co-infection rates.22–24 However, it’s worth noting that the proportion of hospitalized COVID-19 patients who received antibiotics far exceeds the reported prevalence of microbiologically proven co-infection.11,25
As high as 87.4% of hospitalized patients with COVID-19 in our study received early-antibiotic treatments, with an all-cause mortality of 14.8%. The higher reported rate of antibiotic use may be due to that our study excluded asymptomatic COVID-19 patients and mild COVID-19 patients who did not require hospitalization, so that severe and critical COVID-19 accounted for a high proportion of our study population. Our data showed that antibiotics were frequently prescribed in patients with older age, multiple comorbidities, severe and critical COVID-19 subtype, higher serum infectious indicators, and inflammatory indicators at admission. Especially the severity of COVID infection was reported as an important factor related with mortality regardless of antibiotic use and bacteria co-infection.8 Both hyperinflammation and immune dysfunction are reported to play a necessary role in COVID-19-related pathogenesis and clinical outcomes.26 Abnormally increased inflammation markers (such as CRP\IL-6\PCT) and decreased immune associated markers (such as Lymphocytes \CD4+ T cell\CD8+ T cell count) were observed in all groups, especially in patients with early antibiotic use. Patients with the above characteristics were regarded as population with high risk for death, and antibiotics prescribing in these patients was believed to be conducive for preventing secondary bacterial super-infection and improving prognosis initially.3,16 However, simple COVID-19 infection also could cause abnormalities of immune and inflammation markers, our another research found that only critical COVID-19 subtype was an independent risk factor for both co-infection and secondary infection.27
Current clinical trials on the efficacy of antibiotics in patients with COVID-19 are mainly limited to azithromycin for its supposed immunomodulatory and pro-inflammatory cytokines downregulation action. Nevertheless, subsequent research failed to demonstrate a significant clinical benefit of azithromycin against SARS-CoV-2.28,29 Our study raises questions about the effectiveness of early antibiotic therapy on improving clinical outcomes, and we found that patients with early antibiotic use had worse outcomes, including increased all-cause mortality, prolonged length of hospital stay, higher risk of ICU admission, mechanical ventilation, and tracheal intubation before adjusting to patients’ baseline characteristics. However, this apparent deterioration in outcomes should not be crudely attributed to early antibiotic treatment.30 We concluded that the poor prognosis was due to the fact that early antibiotic therapy was more common in patients with older age and multiple comorbidities (including diabetes, chronic lung, and kidney diseases, and cardiovascular disease), those with more severe disease conditions of COVID-19 (a large proportion of patients belonged to severe or critical subtype (62.9%)) and higher inflammatory markers level, rather than due to the effect of the antibiotic therapy itself. Considering that patients with the above characteristics were reported to have a higher risk of disease progression and death,31,32 empiric antibiotic therapy was initiated at hospital admission.
Whereas, after carefully adjusting to these confounding factors likely to influence the prognosis, no significant correlation between early antimicrobial use and outcomes parameters was seen. Early antibiotic treatment failed to demonstrate a clear positive effect on all-cause mortality, the risk for ICU admission, mechanical ventilation, and tracheal intubation. These conclusions could apply to all subtypes of COVID-19 and all age groups. Furthermore, additional subgroup analyses in our supplement came to the same results. Buetti’s research conducted in critically ill patients with COVID-19 also came to a similar conclusion that early administered antibiotics do not impact neither mortality or delayed hospital-acquired infections.33 In the LEOSS cohort, compared with patients without antibiotic therapy, antibiotics therapy in SARS-CoV-2-infected patients did not illustrate a significant benefit for all-cause mortality or disease progression.34 Compared with the first wave of COVID-19 (spring of 2020), less antimicrobial use was observed in the second wave (winter of 2020), which did not significantly affect mortality in critically ill patients.35 With deeper knowledge of COVID-19, more and more data were reported to support our point that early antibiotic prescription does not appear to worsen nor improve the prognosis in the context of COVID-19.36,37
There are several limitations to our study. Firstly, this is a monocentric, retrospective study, and the number of patients without early antibiotic use was small. Secondly, viral in this study mainly included the COVID-19-Omicron variant for the study period limited from Dec 2022 to Mar 2023. Thirdly, COVID-19 patients without early antibiotic use (including delayed antibiotic use and non-antibiotics use) majorly belonged to non-severe COVID-19 patients, which needs more data to strengthen the credibility of this conclusion in severe and critical COVID-19 patients. In addition, inactivated vaccine and recombinant protein vaccine were the main types of vaccines for Chinese population. However, we ignored to make a detailed record of every patient’s vaccination to explore the impact of vaccination on antibiotic prescription. And lack of comparison of antiviral drugs for COVID-19 between groups was another limitation of our study. Lastly, we need to further supplement the data on bacteria distribution and risk factors associated with bacterial co-infection during hospitalization in these patients to better understand the association between COVID-19 and bacterial co-infection.
Conclusion
Antibiotic consumption trending in our data indicated that early antibiotics were frequently prescribed in patients with more severe disease conditions (including older age, multiple comorbidities, severe and critical COVID-19 subtype, higher serum infectious indicators, and inflammatory indicators) at admission. However, compared with delayed antibiotics therapy or non-antibiotics therapy, early antibiotics therapy in hospitalized patients with COVID-19 does not successfully demonstrate better clinical outcomes in the propensity-score-matched cohorts. Therefore, our study did not recommend early antibiotic therapy for COVID-19 patients at hospital admission to prevent worsening worldwide antimicrobial resistance. The prescription of early empiric antimicrobial treatment should be restricted and carefully evaluated at hospital admission to reduce unnecessary antibiotic use and guide proper antibiotic management.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Bojiang Chen is funded by the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (2017-046, ZYJC21028), and the Key R & D plan of Sichuan Provincial Department of Science and Technology (2021YFS0072).
Disclosure
Yishan Duan, Jing Ren, and Jing Wang are co-first authors for this study. Weimin Li and Bojiang Chen are co-last authors for this study. The authors declare that they have no competing interests in this work.
References
1. World Health Organization. WHO coronavirus disease (COVID-19) dashboard. Available from: https://covid19.who.int/.
2. Rawson TM, Moore LSP, Zhu N, et al. Bacterial and fungal coinfection in individuals with coronavirus: a rapid review to support COVID-19 antimicrobial prescribing. Clin Infect Dis. 2020;71(9):2459–2468. doi:10.1093/cid/ciaa530
3. Rouze A, Martin-Loeches I, Povoa P, et al. Early bacterial identification among intubated patients with COVID-19 or influenza pneumonia: a European multicenter comparative clinical trial. Am J Respir Crit Care Med. 2021;204(5):546–556. doi:10.1164/rccm.202101-0030OC
4. Patton MJ, Orihuela CJ, Harrod KS, et al. COVID-19 bacteremic co-infection is a major risk factor for mortality, ICU admission, and mechanical ventilation. Crit Care. 2023;27(1):34. doi:10.1186/s13054-023-04312-0
5. Westblade LF, Simon MS, Satlin MJ. Bacterial coinfections in coronavirus disease 2019. Trends Microbiol. 2021;29(10):930–941. doi:10.1016/j.tim.2021.03.018
6. Goncalves Mendes Neto A, Lo KB, Wattoo A, et al. Bacterial infections and patterns of antibiotic use in patients with COVID-19. J Med Virol. 2021;93(3):1489–1495. doi:10.1002/jmv.26441
7. Abubakar U, Al-Anazi M, Alanazi Z, Rodríguez-Baño J. Impact of COVID-19 pandemic on multidrug resistant gram positive and gram negative pathogens: a systematic review. J Infect Public Health. 2023;16(3):320–331. doi:10.1016/j.jiph.2022.12.022
8. Casale R, Bianco G, Bastos P, et al. Prevalence and impact on mortality of colonization and super-infection by carbapenem-resistant gram-negative organisms in COVID-19 hospitalized patients. Viruses. 2023;15(9):1934. doi:10.3390/v15091934
9. Kasugai D, Jingushi N, Omote N, Shindo Y, Goto Y. The Mystery of Futility of Appropriate Antibiotics for Coinfection in COVID-19. Am J Respir Crit Care Med. 2021;204(12):1489. doi:10.1164/rccm.202107-1656LE
10. Nasir N, Rehman F, Omair SF. Risk factors for bacterial infections in patients with moderate to severe COVID-19: a case-control study. J Med Virol. 2021;93(7):4564–4569. doi:10.1002/jmv.27000
11. Vaughn VM, Gandhi TN, Petty LA, et al. Empiric antibacterial therapy and community-onset bacterial coinfection in patients hospitalized with coronavirus disease 2019 (COVID-19): a multi-hospital cohort study. Clin Infect Dis. 2021;72(10):e533–e541. doi:10.1093/cid/ciaa1239
12. Sieswerda E, de Boer MGJ, Bonten MMJ, et al. Recommendations for antibacterial therapy in adults with COVID-19 - an evidence based guideline. Clin Microbiol Infect. 2021;27(1):61–66. doi:10.1016/j.cmi.2020.09.041
13. Shah W, Heightman M, O’Brien S. UK guidelines for managing long-term effects of COVID-19. Lancet. 2021;397(10286):1706. doi:10.1016/S0140-6736(21)00847-3
14. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
15. Lamontagne F, Agarwal A, Rochwerg B, et al. A living WHO guideline on drugs for covid-19. BMJ. 2020;370:m3379.
16. Bendala Estrada AD, Calderon Parra J, Fernandez Carracedo E, et al. Inadequate use of antibiotics in the covid-19 era: effectiveness of antibiotic therapy. BMC Infect Dis. 2021;21(1):1144. doi:10.1186/s12879-021-06821-1
17. Milas S, Poncelet A, Buttafuoco F, Pardo A, Lali SE, Cherifi S. Antibiotic use in patients with Coronavirus disease 2019 (COVID-19): outcomes and associated factors. Acta Clin Belg. 2022;77(3):579–587. doi:10.1080/17843286.2021.1916300
18. Rubin DB. Using propensity scores to help design observational studies: application to the tobacco litigation. Health Services Outcomes Res Methodol. 2001;2(3):169–188. doi:10.1023/A:1020363010465
19. Hansen BB, Klopfer SO. Optimal full matching and related designs via network flows. J Comput Graph Stat. 2006;15(3):609–627. doi:10.1198/106186006X137047
20. Tsai YW, Tsai CF, Wu JY, Huang PY, Liu TH, Lai CC. The risk of methicillin-resistant Staphylococcus aureus infection following COVID-19 and influenza: a retrospective cohort study from the TriNetX network. J Infect. 2023;86(3):256–308. doi:10.1016/j.jinf.2023.01.006
21. Moreno-Garcia E, Puerta-Alcalde P, Letona L, et al. Bacterial co-infection at hospital admission in patients with COVID-19. Int J Infect Dis. 2022;118:197–202. doi:10.1016/j.ijid.2022.03.003
22. Lansbury L, Lim B, Baskaran V, Lim WS. Co-infections in people with COVID-19: a systematic review and meta-analysis. J Infect. 2020;81(2):266–275. doi:10.1016/j.jinf.2020.05.046
23. Langford BJ, So M, Raybardhan S, et al. Antibiotic prescribing in patients with COVID-19: rapid review and meta-analysis. Clin Microbiol Infect. 2021;27(4):520–531. doi:10.1016/j.cmi.2020.12.018
24. Chedid M, Waked R, Haddad E, Chetata N, Saliba G, Choucair J. Antibiotics in treatment of COVID-19 complications: a review of frequency, indications, and efficacy. J Infect Public Health. 2021;14(5):570–576. doi:10.1016/j.jiph.2021.02.001
25. Murillo-Zamora E, Trujillo X, Huerta M, et al. Empirical antibiotic prescribing in adult COVID-19 inpatients over two years in Mexico. Antibiotics. 2022;11(6). doi:10.3390/antibiotics11060764
26. Merad M, Blish CA, Sallusto F, Iwasaki A. The immunology and immunopathology of COVID-19. Science. 2022;375(6585):1122–1127. doi:10.1126/science.abm8108
27. Duan Y, Wang J, Wang S, et al. Risk factors, outcomes, and epidemiological and etiological study of hospitalized COVID-19 patients with bacterial co-infection and secondary infections. Europ J Clin Microbiol Infect Dis. 2024;43(3):577–586. doi:10.1007/s10096-024-04755-5
28. Oldenburg CE, Pinsky BA, Brogdon J, et al. Effect of oral azithromycin vs placebo on COVID-19 symptoms in outpatients with SARS-CoV-2 infection: a randomized clinical trial. JAMA. 2021;326(6):490–498. doi:10.1001/jama.2021.11517
29. O’Connor S. In patients hospitalized with COVID-19, adding azithromycin to usual care did not reduce 28-d mortality. Ann Internal Med. 2021;174(6):Jc64. doi:10.7326/ACPJ202106150-064
30. Garcia-Vidal C, Sanjuan G, Moreno-García E, et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: a retrospective cohort study. Clin Microbiol Infect. 2021;27(1):83–88. doi:10.1016/j.cmi.2020.07.041
31. Ng TM, Ong SWX, Loo AYX, et al. Antibiotic therapy in the treatment of COVID-19 pneumonia: who and when? Antibiotics. 2022;11(2). doi:10.3390/antibiotics11020184
32. Pinte L, Ceasovschih A, Niculae CM, et al. Antibiotic prescription and in-hospital mortality in COVID-19: a prospective multicentre cohort study. J Pers Med. 2022;12(6). doi:10.3390/jpm12060877
33. Buetti N, Mazzuchelli T, Lo Priore E, et al. Early administered antibiotics do not impact mortality in critically ill patients with COVID-19. J Infect. 2020;81(2):e148–e149. doi:10.1016/j.jinf.2020.06.004
34. Schons MJ, Caliebe A, Spinner CD, et al. All-cause mortality and disease progression in SARS-CoV-2-infected patients with or without antibiotic therapy: an analysis of the LEOSS cohort. Infection. 2022;50(2):423–436. doi:10.1007/s15010-021-01699-2
35. Chan XHS, O’Connor CJ, Martyn E, et al. Reducing broad-spectrum antibiotic use in intensive care unit between first and second waves of COVID-19 did not adversely affect mortality. J Hosp Infect. 2022;124:37–46. doi:10.1016/j.jhin.2022.03.007
36. Pettit NN, Nguyen CT, Lew AK, et al. Reducing the use of empiric antibiotic therapy in COVID-19 on hospital admission. BMC Infect Dis. 2021;21(1):516. doi:10.1186/s12879-021-06219-z
37. Iosub MI, Balan ES, Pinte L, Draghici AM, Baicus C, Badea C. The impact of antibiotic use on mortality in patients hospitalized in a COVID-19 centre from Romania: a retrospective study. Medicina. 2022;58:11.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.