")
Back to Journals » Infection and Drug Resistance » Volume 18
The Inter-Relationships Among the Risk Factors for Pulmonary Infection and the Diagnostic Utility of Inflammatory Markers in Patients with Non-Small Cell Lung Cancer
Authors Qin W, You T , Guo T , Tian R, Cui X , Wang P
Received 12 September 2024
Accepted for publication 14 February 2025
Published 25 February 2025 Volume 2025:18 Pages 1111—1123
DOI https://doi.org/10.2147/IDR.S491507
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandip Patil
Wenwen Qin,* Tiebin You,* Tai Guo, Ruixin Tian, Xiaoman Cui, Ping Wang
Department of Respiratory Medicine, the Fourth Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ping Wang, Email [email protected]
Objective: To analyze independent risk factors and the distribution of pathogenic bacteria associated with pulmonary infection (PI) in patients with non-small cell lung cancer (NSCLC); and to explore the utility of peripheral blood-related inflammatory markers in the diagnosis of PI after comprehensive treatment of NSCLC.
Methodology: We retrospectively analyzed patients who were first diagnosed with NSCLC and received anti-tumor therapy from January 1, 2022 to December 31, 2022. There were 150 males and 50 females enrolled, and with a median age of 63 years. They were divided into PI (n=59) and non-PI (n=141) groups. The patients’ characteristics, treatment histories, and peripheral blood inflammatory indicators of the two groups were compared.
Results: Eighty-two strains of pathogens were isolated from 59 patients with NSCLC complicated by PI, of which 35 (42.7%) were Gram-negative and 29 (35.4%) were Gram-positive bacteria, 15 (18.3%) were fungi, and 3 (3.7%) were viruses. Logistic regression analysis revealed that ≥ 4 cycles of chemotherapy, radiotherapy, and higher neutrophil count before antineoplastic treatment were independent risk factors for PI in patients with NSCLC (P< 0.05). C-reactive protein (CRP) and CRP-to-albumin ratio (CAR) exhibited high area under the curve values of 0.807 and 0.791, respectively. CRP demonstrated high sensitivity (Cutoff Value:10.095, P< 0.001), whereas CAR had high specificity (Cutoff Value:0.747, P< 0.001) for the early diagnosis of PI in patients with NSCLC.
Conclusion: Gram-negative bacteria were the main pathogens causing PI in patients with NSCLC. Greater than or equal to 4 cycles of chemotherapy, radiotherapy, and elevated neutrophil count before antineoplastic treatment were independent risk factors for PI in patients with NSCLC. Elevated CRP levels and higher CAR demonstrated a certain diagnostic utility for PI in patients with NSCLC after antitumor treatment.
Keywords: non-small cell lung cancer, pulmonary infection, risk factors, inflammatory indicators
Introduction
Globally, lung cancer is the leading cause of cancer-related mortalities, accounting for 18% of all cancer-related deaths.1 According to the most recent statistics, the incidence of lung cancer is the highest in China, and lung cancer ranks first in terms of morbidity and mortality among both males and females. Lung cancer causes more deaths each year than colorectal, breast, and prostate cancers.2 Non-small cell lung cancer (NSCLC) is the most common type of lung cancer and accounts for approximately 85% of all lung cancer cases.3 Pulmonary infection (PI) is the most common cause of death in patients with lung cancer; the most common types of infections in these patient populations include pneumonia and sepsis, with Gram-negative bacilli being the most common pathogens.4 From a therapeutic point of view, pulmonary infection can complicate treatment. If the treatment of lung cancer such as radiotherapy and chemotherapy is being carried out, the infection may lead to the interruption or adjustment of these treatments, affecting the continuity and effect of lung cancer treatment. Several factors can lead to the development of PI in patients with NSCLC. This is particularly true for patients who have undergone chemotherapy, radiation therapy, or immune checkpoint inhibitor treatment.5 These treatments can weaken a patient’s immune system and result in infection.6,7
Although several factors can lead to the development of PI in patients with non-small cell lung cancer (NSCLC), making a determination about whether new patchy pulmonary lesions in such patients are due to disease progression, drug associated pneumonia, or infection is clinically challenging. Because this may lead to misdiagnoses, understanding the risk factors for PI in patients with NSCLC is essential to making an accurate diagnosis.The susceptibility factors for PIs in patients with NSCLC are many, including diabetes mellitus, radiation therapy, surgery (Chen et al), chemotherapy and exposure to gram-negative bacteria due to immunocompromise (Wang et al). It is, however, not clear if these factors act independently or interact with one another.8,9
To better understand the inter-relationships among the risk factors for PI, this study used data from patients diagnosed with NSCLC, analyzed the distribution of pathogens after PI and the risk factors for coinfection, and evaluated the diagnostic utility of different infection markers for PI. Although some blood inflammatory indices have been proposed for predicting tumor pathologic staging and to guide treatment for NSCLC patients (Zhai et al),10 we adopt a different approach by exploring different sets of biomarkers in patients with PI and NSCLC. Ultimately, this may help achieve clinical preventive purposes as well as earlier diagnosis.
Materials and Methods
Patient Population
The medical records of patients diagnosed with NSCLC for the first time in the Respiratory Department of the Fourth Hospital of Hebei Medical University (Hebei Province, China) between January 1, 2022, and December 31, 2022, were retrospectively analyzed. The inclusion criteria were as follows: ① Pathology-confirmed NSCLC; ② Antitumor treatment after diagnosis, such as surgery, chemotherapy, radiation therapy, immunotherapy, and/or targeted therapy; ③ Complete medical record information. The exclusion criteria were as follows: ① Other malignant tumors; ② PI before antitumor treatment; ③ Infections occurring in areas other than the lungs during the treatment process. Infections in organs other than the lungs (such as digestive tract infection, urinary tract infection and other infectious diseases that will affect the relevant indicators of this study) are diagnosed by the specialist of the corresponding department. This study was reviewed and approved by the Medical Ethics Committee of the Fourth Hospital of the Hebei Medical University (No. 2023KS206).
Baseline Patient Data
Two experienced physicians evaluated and selected patients who fulfilled the inclusion criteria. Patient data, including age, sex, pathological type, TNM stage, antitumor treatment, and laboratory investigation results, were collected from medical records and electronic databases.
Laboratory Investigations for Pathogens
Laboratory investigations included galactomannan (GM), 1-3-β-D-glucan, Cryptococcus capsular polysaccharide antigen, and the interferon-gamma release assay. Sputum and bronchoalveolar lavage fluid (BALF) examination results included Gram staining, acid-fast testing, hematoxylin, eosin, and hexamine silver staining, GM, and the Xpert Mycobacterium tuberculosis (MTB) test. Culture or metagenomic next-generation sequencing of sputum, BALF, and blood samples, and polymerase chain reaction (PCR) results for pathogen antigen in throat swabs were collected, which included the detection of viruses, mycoplasma, and chlamydia.
Determination of Positive Pathogen Detection Results
The criteria for determining positive results of pathogen testing were as follows. ① Bacteria (excluding mycobacteria): a positive result in blood, sputum culture, or BALF was considered to be positive. ② Mycobacterium tuberculosis: patients diagnosed with positive results needed to fulfill the criterion that the sputum or BALF smear was positive for acid-fast testing or the Xpert MTB test was positive. Diagnoses that conformed to official clinical practice guidelines of the American Thoracic Society/American College of Infectious Diseases/Centers for Disease Control and Prevention were considered to be positive.11 ③ Fungi: patients diagnosed with positive fungal infections needed to have ≥ 1 the host factor(s), clinical features, or mycological evidence, all of which were categorized as probable or proven according to the 2019 criteria from the European Organization for Research and Treatment of Cancer/Mycoses Study Group10. ④ Viruses, mycoplasma, and chlamydia: patients with a positive diagnosis tested positive for the pharyngeal swab antigen.
Inclusion Criteria for PI and Non-PI Patients
The inclusion criteria for the PI group were as follows: ① Presence of symptoms suggestive of PI, such as fever, cough, expectoration, and difficulty breathing; patchy, striped, or nodular pulmonary markings noted on chest computed tomography (CT); ② Positive results from laboratory pathogen testing. Patients in the non-PI group were required to have chest CT demonstrating no new inflammatory exudates, such as patchy or nodular shadows in the lungs. 200 patients were enrolled in the study and were divided into PI (n=59) and non-PI (n=141) groups. Relevant blood test data were collected from patients in the PI group at initial admission and at the time of infection, whereas blood test data from patients in the non-PI group were collected at initial admission and on the day of complete antitumor response or last hospitalization. These included neutrophil count, neutrophil percentage (N%), neutrophil-to-lymphocyte ratio (NLR), C-reactive protein (CRP), CRP-to-albumin ratio (CAR), procalcitonin (PCT), serum amyloid A (SAA), D-dimer, carcinoembryonic antigen (CEA), albumin, and white blood cell ratio.
Collection of Various Detection Markers Before and After Antitumor Treatment in Patients with NSCLC
Data regarding PCT, SAA, CRP, CAR, N%, NLR, albumin, white blood cell ratio, CEA, hemoglobin, and D-dimer levels were collected from patients in the PI and non-PI groups before and after antitumor treatment. Each group was divided into pre-treatment and post-treatment groups. The results of the above test indicators were collected from the pre-treatment group before undergoing antitumor treatment. Relevant blood test indicators in the post-treatment group were collected when infection occurred in those in the PI group, and collected in the non-PI group on the day of complete antitumor response or last hospitalization.
Statistical Methods
Statistical analyses were performed using SPSS version 27.0 (IBM Corporation, Armonk, NY, USA). Count data are expressed as rate or composition ratio, and intergroup comparisons were performed using the chi-squared test. Measurement data that conformed to normal distribution are expressed as mean ± standard deviation (SD), the t-test was used for inter-group comparisons. Variables with a skewed distribution are expressed as median (interquartile range [IQR], ie, P25 – P75), and a non-parametric test was used for intergroup comparisons. Risk factor analysis was performed using a logistic regression model. Diagnostic utility of the indicators was assessed using receiver operating characteristic (ROC) curves, and the area under the ROC curve (AUC) was used as the basis for evaluation. The detection value corresponding to the largest Youden index was selected as the cut-off value. In this study, a two tailed test was used, and P < 0.05 was considered statistically significant. A flow-diagram illustrating the research process is presented in Figure 1.
 |
Figure 1 Flow chart of this study design. |
Results
Patient Characteristics
All patients exhibited pathological evidence on bronchoscopy or CT-guided fine-needle biopsy. Based on whether PI occurred after antitumor treatment, patients were divided into 2 groups: PI (n=59) and non-PI (n=141). The clinical characteristics of the patients are summarized in Table 1.
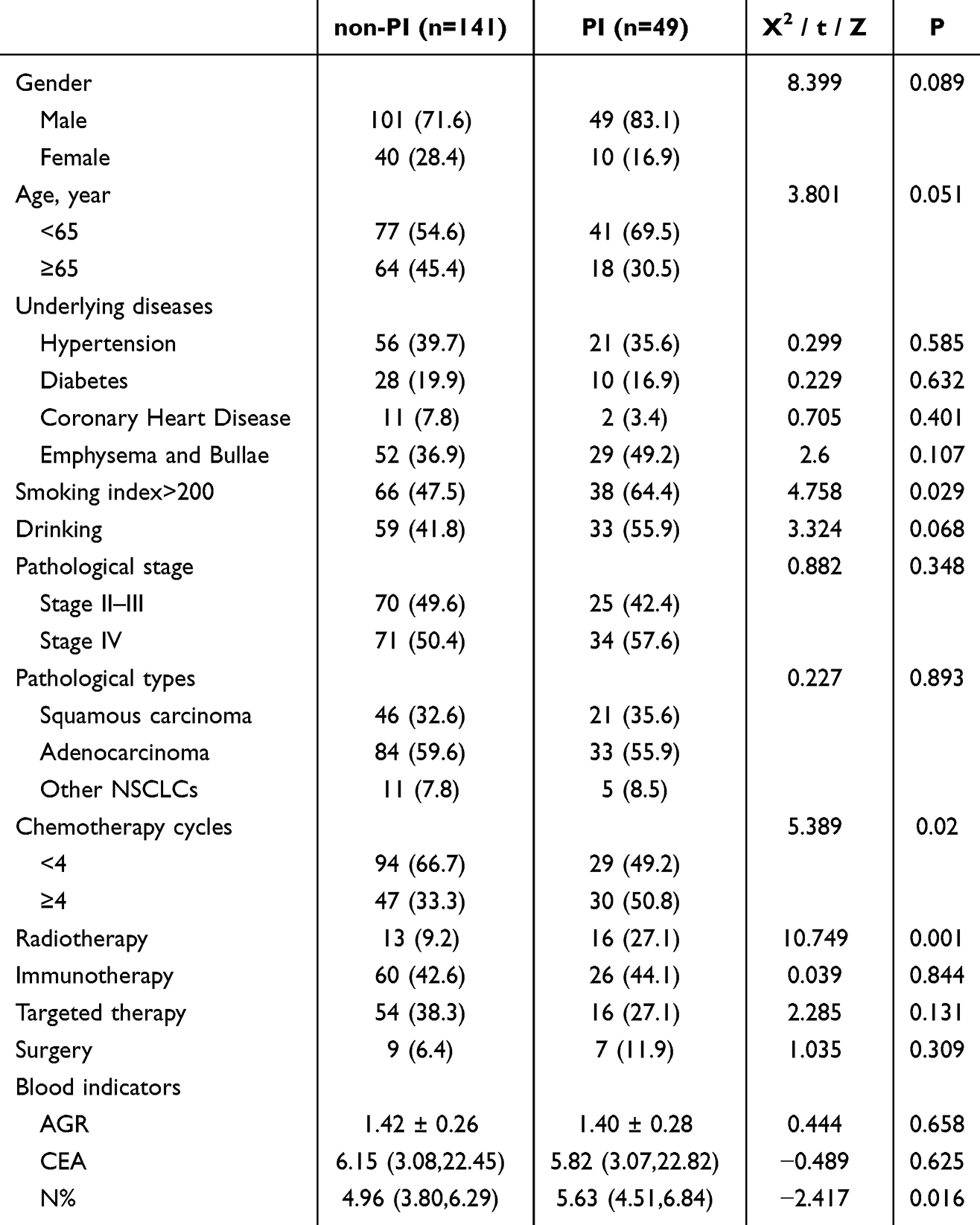 |
Table 1 Patient Characteristics |
There were 150 males and 50 females, ranging in age from 34 to 82 years, with a median age of 63 years (IQR 57–69 years). Underlying diseases among the cohort were distributed as follows: hypertension (n=77); diabetes (n=38); coronary heart disease (n=13); and imaging findings of pulmonary changes such as emphysema and bullae (n=81). Among these, 104 patients had a high smoking index and 92 had a history of drinking. According to TNM staging of lung cancer, 95 cases were classified as stages II and III, and 105 were classified as stage IV. Pathological types were distributed as follows: squamous cell carcinoma (n=67); adenocarcinoma (n=117); and other NSCLCs (such as large cell carcinoma, sarcomatoid carcinoma) (n=16). Treatment was distributed as follows: ≥ 4 cycles of chemotherapy (n=77); radiotherapy (n=29); immunotherapy (n=86); targeted therapy (n=70); and opportunity to undergo surgery at an early stage (n=16). Blood indicators were also collected from the patients before antitumor treatment.
Distribution of Pathogens
Data from 59 patients with NSCLC and PI were collected, and 82 pathogens were isolated. Among these, 35 (42.7%) were Gram-negative bacteria, including Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, Enterobacter cloacae and Acinetobacter baumannii. Twenty-nine (35.4%) strains were Gram-positive bacteria, including Streptococcus pneumoniae, Staphylococcus aureus, other bacilli, and M. tuberculosis. Fifteen (18.3%) strains were fungi, including Candida albicans, Candida tropicalis, Aspergillus and Penicillium. Three (3.7%) strains were viruses, including cytomegalovirus and Epstein-Barr virus. Nineteen patients is mixed infection in the PI group. The most common mixed infection is gram-negative bacteria and fungi. The distribution of pathogens is reported in Figure 2A. and Table 2.
 |
Table 2 Distribution of Pathogens |
 |
Figure 2 The distribution of pathogens and the results of time of occurrence of PI in patients with NSCLC. (A) Time of occurrence of PI in patients with NSCLC. (B) Distribution of pathogens. Abbreviations: PI, pulmonary infection; NSCLC, non-small cell lung cancer. |
Time of Occurrence of PI in Patients with NSCLC
The time from lung cancer diagnosis to the onset of PI was recorded. Thirty-three patients were diagnosed with PI within 6 months, 51 within 1.5 years, 58 within 2 years, and 59 within 2 years. The time is presented in Figure 2B.
Risk Factors for Infection
Based on whether PI occurred after antitumor treatment, patients were divided into 2 groups: PI (n=59) and non-PI (n=141). The clinical data of patients in the PI and non-PI groups were compared. As the parameters were compared between the 2 groups, single-factor analysis revealed that smoking index > 200 (P=0.029), ≥ 4 chemotherapy cycles (P=0.02), radiotherapy (P=0.001), and elevated neutrophil count (P=0.016) exhibited statistically significant results. Multiple-factor analysis revealed that ≥ 4 chemotherapy cycles (odds ratio [OR] 2.027, P=0.037), radiotherapy (OR 3.585, P=0.003), and elevated neutrophil count (OR 1.285, P=0.006) were independent risk factors for PI in patients with NSCLC. The results are presented in Figure 3A and Table S1.
 |
Figure 3 The results of risk factors for infection and ROC Curve. (A) Risk factors for infection. (B) The ROC Curve of neutrophil count before antitumor treatment. (C) Diagnostic role of peripheral blood inflammatory markers. |
Predictive Effect of Neutrophil Count on the Occurrence of PI
Multivariate analysis revealed that an elevated neutrophil count was a risk factor for PI. According to the ROC curve, the AUC was 0.609 (95% confidence interval [CI] 0.525–0.693; P=0.016). The best cut-off value for predicting the occurrence of nosocomial PI during NSCLC treatment was 4.255 × 109/L, with a corresponding sensitivity of 0.864, and a specificity of 0.353. The results are presented in Figure 3B.
Diagnostic Role of Peripheral Blood Inflammatory Markers
Relevant indicators of infection in the PI group were compared with various indicators of complete remission or last visit after anti-tumor treatment in the non-PI group and analyzed the diagnostic role of various inflammatory indicators in PI after anti-tumor treatment. Among PCT, SAA, CRP, N%, CAR, and NLR, the AUC values for each index for the diagnosis of PI in patients with NSCLC were all significantly higher than those in the non-PI group (P < 0.05). The AUC for CRP was highest (0.807), with a sensitivity and specificity of 92.6% and 61%, respectively. The AUC for CAR was 0.791, with a sensitivity and specificity of 62.2% and 85.4%, respectively. The AUC for SAA was 0.786, with a sensitivity and specificity of 85.2% and 51.1%, respectively. The AUC for PCT was 0.651, indicating a poor diagnostic performance. The results are presented Figure 3C. and summarized in Table 3.
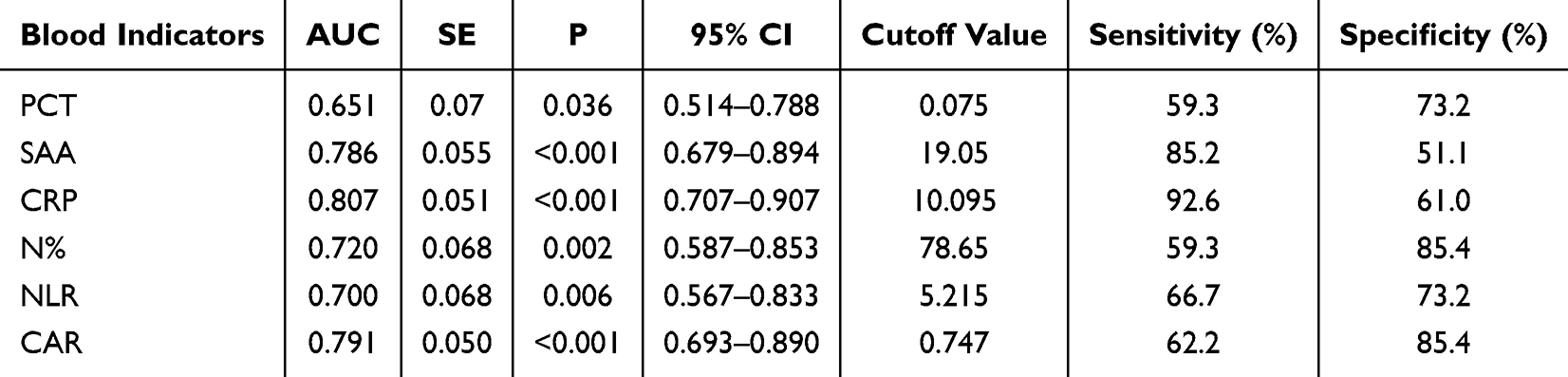 |
Table 3 Peripheral Blood Inflammatory Markers |
Changes in Relevant Indicators in Patients in the PI Group Before and After Antitumor Treatment
The laboratory indices of the 2 groups before and after antitumor treatment were compared. After antitumor treatment, the levels of albumin, albumin-to-globulin ratio (AGR), and hemoglobin in the peripheral blood of patients decreased, the level of D-dimer increased, and the differences were was statistically significant. The results are presented in Table 4.
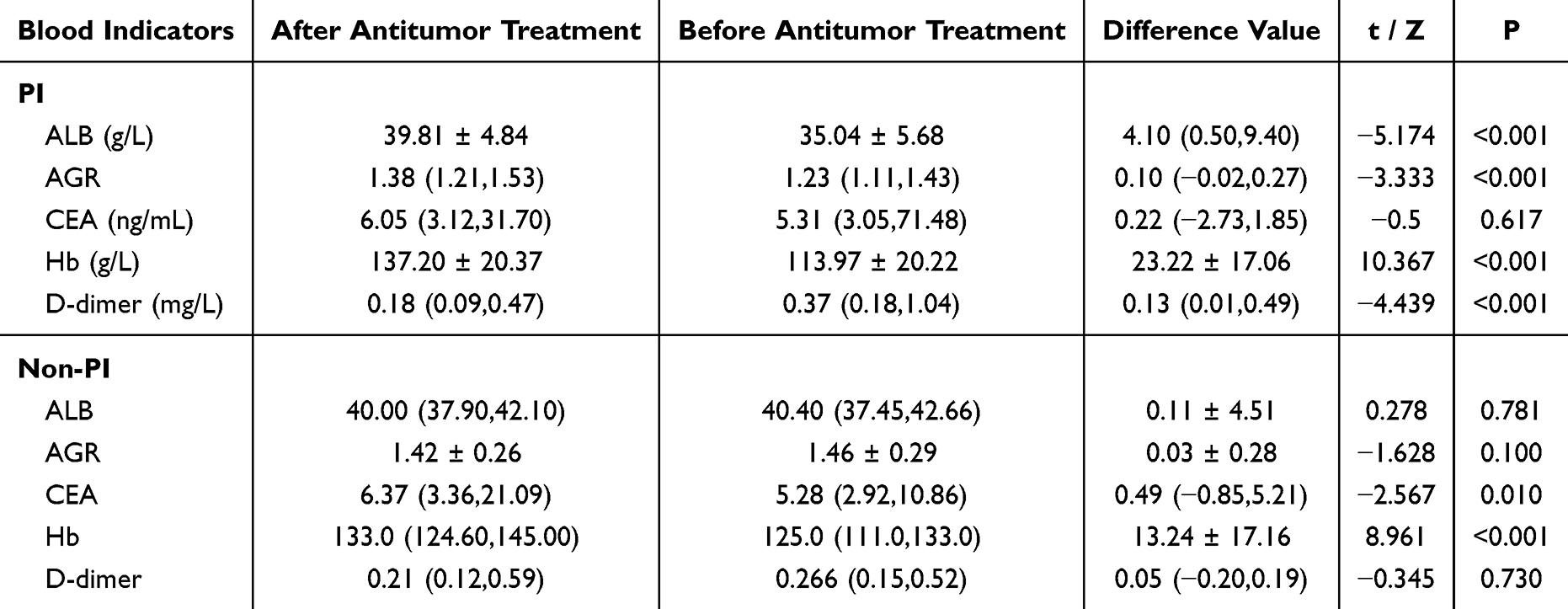 |
Table 4 Changes in Relevant Indicators in Patients in the PI and Non-PI Group Before and After Antitumor Treatment |
Changes in Relevant Indicators in Patients in the Non-PI Group Before and After Antitumor Treatment
After antitumor treatment, hemoglobin and CEA levels in the peripheral blood of patients decreased, and the difference was statistically significant. However, there was no significant difference in albumin, AGR, or D-dimer levels. The results are presented in Table 4.
Discussion
Patients with early-stage NSCLC can achieve good clinical benefits through comprehensive surgery-based treatment; however, the 5-year OS rate remains < 20%.12 The main reason is that the rate of early diagnosis is low; as such, > 75% of patients with NSCLC are clinically diagnosed as having progressed to the middle- to late-stage(s) and lose the opportunity for surgery to provide a radical cure. Chemotherapy, radiation therapy, and immune therapy remain the main treatments for advanced NSCLC. Although some patients achieve a complete response with these treatments,13–15 complications may occur such as infection, thrombosis, immune-related adverse reactions, and liver and kidney damage, and some are even life threatening.16–19 This underscores the benefit of developing a diagnostic markers that make early diagnosis and treatment possible, which can ultimately help prevent these treatment complications as well as comorbidities, while prolonging patient survival. Against this background, the present study investigated the relevant risk factors in patients with NSCLC and PIs and explored the potential diagnostic value of inflammatory markers in the peripheral blood.
PI is a common respiratory disease, presenting with symptoms including fever, cough, sputum production, chest pain, difficulty with breathing, and/or new patchy exudates in the lungs. This study enrolled 200 patients; of those with NSCLC, 59 had concurrent PI, which was based on PI diagnosis and pathogen testing. We were able to confirm that 82 pathogens were identified in 59 patients, and the pathogens mainly included Gram-negative bacteria, Gram-positive bacteria, fungi, and viruses.
In recent years, with advances in detection technologies, multiple studies have found that the common pathogens infecting lung cancer patients are Gram-positive bacteria, Gram-negative cocci, fungal infections, viruses, and tuberculosis.9,20–23 The results of related studies revealed that Gram-negative bacteria predominated among PIs. Early epidemiological data suggest that bacterial infections are common in patients with cancer, especially when the disease progresses, with an incidence rate of approximately 50%–70%.24 Our study evaluated the distribution of common pathogens in NSCLC after treatment, and provided diagnostic and therapeutic evidence for patients with PI during comprehensive treatment.
We divided the patients into PI and non-PI groups to evaluate risk factors for the development of PI in patients with NSCLC. To increase the authenticity and reliability of the evaluation, we limited the PI group to patients in whom pathogens were detected, while the non-PI group included patients who did not fulfill the criteria for clinical diagnosis of PI. Patients with suspected PIs were not included in any group. We found that history of ≥ 4 chemotherapy cycles, history of radiotherapy, and increased neutrophil count were independent risk factors for PI. Lower respiratory tract defense against infection includes mechanical defenses, such as coughing, barrier function of the mucus and epithelium, and mucociliary clearance, in combination with the innate immune response to help clear inhaled or inhaled substances, including infectious agents.25 The lower respiratory tract has defensive functions. When lung cancer occurs, airway compression and rupture of the alveoli occur, resulting in reduced defense functions and susceptibility to pneumonia. Because the chemotherapy regimen is basically 4–6 cycles, if the lesion does not progress, the patient will enter the observation period or maintenance treatment period. Therefore, selecting ≥ 4 cycles of chemotherapy will become a risk factor. When the immune system is weakened after radiotherapy or chemotherapy, infections are more likely to occur.26 Other studies have reported that radiotherapy and chemotherapy in patients with lung cancer can cause damage to epithelial cells and induce oxygen response, aging, and cell death.,27,28 including tumor necrosis factor, interleukin (IL)-1, IL-6, and IL-23, T lymphocytes, and infiltration inflammation of macrophages, neutrophils, and eosinophils in the alveoli (alveolitis), which leads to subsequent damage to the physiological condition of the lungs.29–31 Relevant studies pointed out that the occurrence of pulmonary bacterial infection in patients with non-small cell lung cancer receiving immunotherapy predicted better efficacy of immunotherapy, and immunotherapy was not a risk factor for pulmonary infection in this study.32
An elevated neutrophil count was also found to be an independent risk factor for the development of PI in patients with NSCLC. The AUC for neutrophil count in predicting PI was < 0.7, and the specificity of the neutrophil count as a predictor was low and, therefore, not ideal. Although neutrophil count before antineoplastic treatment was one of the risk factors in this study, and its AUC value was statistically significant, its AUC was < 0.7, indicating that its ability to predict the occurrence of PI was poor. Neutrophils are myeloid white blood cells that are one of the main mediators of acute inflammation in humans. Neutrophils account for 50%–70% of all circulating leukocytes, are generally believed to be present during the acute phase of inflammation, and play a role in killing pathogens.33 The neutrophil count in the PI group was higher than that in the non-PI group before antineoplastic treatment; however, its correlation with infection prediction was poor. This may be because the body has a mild inflammatory response when lung cancer is first diagnosed, but does not develop into specific organ infections. Neutrophil count reflects the inflammatory and immune status of the body over a short period rather than being a long-term indicator. Laboratory index changes affected by various factors are large and do not predict the need for anti-tumor treatment after infection. The AGR reflects the chronic inflammatory response in the body, and some studies have shown that it is closely related to the incidence and mortality of cancer.34 AGR is an important predictor of long-term mortality in patients with lung adenocarcinoma.35 However, the difference in the AGR in this study was not statistically significant before treatment.
In the diagnosis and treatment of NSCLC, when a patient develops a new lesion, it is necessary to determine whether the lesion represents tumor progression, infection, or interstitial pneumonia. Therefore, we often rely on blood test results for accurate judgments. Indicators frequently involved in inflammatory testing include PCT, CRP, SAA, white blood cell ratio, and neutrophil counts.36,37 The results for these inflammatory factors are easily obtainable in clinical practice, although whether these inflammatory factors play a diagnostic role in the occurrence of infection in patients with lung cancer requires further confirmation. Therefore, we collected these indicators from 200 patients at the time of diagnosis and at the end of follow-up. Patients with PI exhibited significantly higher levels of CRP, CAR, PCT, SAA, N%, and NLR than those in the non-PI group. Analysis revealed that CAR and PCT have high specificity but poor sensitivity, whereas the results for CRP are exactly the opposite. Related reports have also found that PCT, CRP, and CAR can be used as predictive indicators of concurrent infections in patients with lung cancer after radiotherapy and chemotherapy.38–40 However, CRP and CAR have better predictive performance.38,41 An increasing number of studies have suggested that CAR is the most effective early predictor of co-infection in patients with lung cancer.38,42 This is consistent with our results because we found that CRP and CAR had higher AUC values and sensitivities than PCT. In recent years, NLR has been widely investigated as a new inflammatory index. Some studies have reported that hospitalization for community-acquired pneumonia in patients with an elevated NLR is significantly prolonged.43,44 In recent years, some studies have suggested that NLR can serve as a predictor of targeted and immunotherapeutic effects for lung cancer, and the overall survival (OS) and progression-free survival of targeted therapy and immunotherapy are significantly reduced when the NLR is > 5.45,46 In recent studies, investigators have found that in the diagnosis of bacterial infection after chemotherapy, the diagnostic value of the NLR is higher than that of traditional routine blood indices, which is in agreement with the results of this study.47 In our study, although the NLR was significantly increased in the PI group, its sensitivity and specificity were poor, and its diagnostic significance for patients with lung cancer and concurrent infections was low. Therefore, CRP and CAR may be the best early diagnostic tools for co-infection in NSCLC.
To further explore the significance of blood tests in patients with PI, we compared albumin, white blood cell ratio, hemoglobin, CEA, and D-dimer levels before and after comprehensive treatment in the PI and non-PI groups. In the non-PI group, only a decrease in CEA level was observed after antitumor treatment, and no further changes were observed in the other indicators. In the PI group, the levels of albumin, white blood cell ratio, and hemoglobin decreased, changes in CEA were not significant, and D-dimer levels increased. This suggests that patients with PI may have decreased immune function due to the long-term depletion of albumin, white blood cell ratio, and hemoglobin. In addition, relevant reports have suggested that PI can cause an increase in D-dimer levels, which may be related to the damage caused by the infection of blood vessels.48,49 In a meta-analysis including 8452 patients, it was found that high D-dimer levels in patients with cancer led to reduced survival, and that D-dimer levels were an independent factor for poor prognosis.50 Related studies have shown that CEA levels gradually decrease during the remission of NSCLC. CEA levels help evaluate the therapeutic effect on NSCLC.51 After treatment, D-dimer levels in the infected group increased, whereas the CEA level in the non-infected group decreased. Therefore, it can be preliminarily inferred that the occurrence of infection may be associated with the effectiveness of antitumor therapy. Further research with larger sample sizes is necessary to determine the exact relationship between infection and oncological efficacy.
The present study had some limitations, the most significant of which was the more accurate collection of relevant indicators in the PI group. After careful consideration, we believe that test results at the last follow-up for patients without PI are more meaningful but may have introduced bias. In addition, the infected patients we enrolled were those who were found to have pathogens, excluding patients with lung cancer complicated by lung infection without clear pathogens. The main reason for the inclusion criteria was to exclude patients with radiation pneumonia and immune-related pneumonia in clinical practice.From the available records, the OS could not be determined, this should be listed as a limitation. A prospective, follow-up study which incorporates OS and PFS is warranted.
Conclusion
Gram-negative bacteria were the main pathogens causing PI in patients with NSCLC. More than 4 chemotherapy cycles, radiotherapy, and elevated neutrophil count before antineoplastic treatment were independent risk factors for PI in patients with NSCLC. Elevation of CRP levels and CAR had a certain diagnostic utility for PI in patients with NSCLC after anti-tumor treatment. Compared with the related indicators of tumor burden (CEA and D-dimer), the tumor burden of patients in the PI group was higher than that in the non-PI group. Pending its reproducibility and validation in a clinical population via a prospective study, our results suggest that the occurrence of PI may be a clinical indicator of the efficacy (or the lack of it) of antitumor treatment.
This study has some shortcomings, such as it is a retrospective single center study with a small sample size, no further analysis of different types of lung infections, and no long-term follow-up. We hope that in the future, we can conduct a multicenter, large sample prospective study with less bias to further find the risk factors of lung inflammation in lung cancer patients and the adverse impact of lung infection on the prognosis of lung cancer patients.
Ethical Approval and Consent to Participate
Before the commencement of the study, we obtained ethical clearance from the Ethics Review Committee of the Fourth Hospital of Hebei Medical University. Before data collection, we explained the study objectives to the heads of the hospital director and laboratory personnel who worked in the hospital. Since we used the secondary data obtained from previous clinical treatment for this study and didn’t require the patient’s informed consent. The informed consent of this study was waived by the Ethics Review Committee of the Fourth Hospital of Hebei Medical University (No. 2023KS206). We conducted the study following the Declaration of Helsinki.52 To ensure confidentiality of information from participant’s record, we didn’t record any personal identifiers on the data collection sheet, and secured data from participant records were not available to anyone except for the investigators.
Acknowledgments
We thank all the individuals, families, and physicians involved in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received the funding from S & T Program of Hebei (No. 22377715D).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL. et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49. doi:10.3322/caac.21820
3. Alexander M, Kim SY, Cheng H. Update 2020: management of non-small cell lung cancer. Lung. 2020;198(6):897–907. doi:10.1007/s00408-020-00407-5
4. Bodey GP. Infection in cancer patients. A continuing association. Am J Med. 1986;81(1a):11–26. doi:10.1016/0002-9343(86)90510-3
5. Burns EA, Gee K, Kieser RB, et al. Impact of infections in patients receiving pembrolizumab-based therapies for non-small cell lung cancer. Cancers (Basel). 2022;15(1):81. doi:10.3390/cancers15010081
6. Sharma A, Jasrotia S, Kumar A. Effects of chemotherapy on the immune system: implications for cancer treatment and patient outcomes. Naunyn Schmiedebergs Arch Pharmacol. 2024;397(5):2551–2566. doi:10.1007/s00210-023-02781-2
7. Zhai D, An D, Wan C, Yang K. Radiotherapy: brightness and darkness in the era of immunotherapy. Transl Oncol. 2022;19:101366. doi:10.1016/j.tranon.2022.101366
8. Chen J, Liu Y, Cai H, Zheng W. Risk factors for pulmonary infection in patients with non-small cell lung cancer: a Meta-analysis. BMC Pulm Med. 2024;24(1):353. doi:10.1186/s12890-024-03171-x
9. Wang Y, Li J, Wu Q, Chang Q, Guo S. Pathogen distribution in pulmonary infection in Chinese patients with lung cancer: a systematic review and meta-analysis. BMC Pulm Med. 2023;23(1):402. doi:10.1186/s12890-023-02681-4
10. Zhai Y, Wu J, Tang C, Huang B, Bi Q, Luo S. Characterization of blood inflammatory markers in patients with non-small cell lung cancer. Int J Clin Exp Pathol. 2024;17(5):165–172. doi:10.62347/iptw9741
11. Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention clinical practice guidelines: diagnosis of tuberculosis in adults and children. Clin Infect Dis. 2017;64(2):e1–e33. doi:10.1093/cid/ciw694
12. Doroshow DB, Sanmamed MF, Hastings K, et al. Immunotherapy in non-small cell lung cancer: facts and hopes. Clin Cancer Res. 2019;25(15):4592–4602. doi:10.1158/1078-0432.Ccr-18-1538
13. Riely GJ, Wood DE, Ettinger DS, et al. Non-small cell lung cancer, version 4.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2024;22(4):249–274. doi:10.6004/jnccn.2204.0023
14. Relli V, Trerotola M, Guerra E, Alberti S. Abandoning the notion of non-small cell lung cancer. Trends Mol Med. 2019;25(7):585–594. doi:10.1016/j.molmed.2019.04.012
15. Zhang C, Fu Y, Chen Q, Liu R. Risk factors for postoperative pulmonary infections in non-small cell lung cancer: a regression-based nomogram prediction model. Am J Cancer Res. 2024;14(11):5365–5377. doi:10.62347/bibd8425
16. Goldman JW, Dvorkin M, Chen Y, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, Phase 3 trial. Lancet Oncol. 2021;22(1):51–65. doi:10.1016/s1470-2045(20)30539-8
17. Wang W, Gu X, Wang L, et al. The prognostic impact of mild and severe immune-related adverse events in non-small cell lung cancer treated with immune checkpoint inhibitors: a multicenter retrospective study. Cancer Immunol Immunother. 2022;71(7):1693–1703. doi:10.1007/s00262-021-03115-y
18. Choi Y, Noh JM, Shin SH, et al. The incidence and risk factors of chronic pulmonary infection after radiotherapy in patients with lung cancer. Cancer Res Treat. 2023;55(3):804–813. doi:10.4143/crt.2022.1305
19. Khorana AA, Palaia J, Rosenblatt L, et al. Venous thromboembolism incidence and risk factors associated with immune checkpoint inhibitors among patients with advanced non-small cell lung cancer. J Immunother Cancer. 2023;11(1):e006072. doi:10.1136/jitc-2022-006072
20. Lira CAG, Peixoto Bittencourt D, Bicalho CDS, et al. Clinical profile and mortality predictors for tuberculosis disease among patients with solid tumours. Infect Dis (Lond). 2022;54(11):804–809. doi:10.1080/23744235.2022.2101690
21. Park M, Ho DY, Wakelee HA, Neal JW. Opportunistic invasive fungal infections mimicking progression of non-small-cell lung cancer. Clin Lung Cancer. 2021;22(2):e193–e200. doi:10.1016/j.cllc.2020.10.001
22. Wang Q, Berger NA, Xu R. Analyses of risk, racial disparity, and outcomes among us patients with cancer and COVID-19 infection. JAMA Oncol. 2021;7(2):220–227. doi:10.1001/jamaoncol.2020.6178
23. Chen Y, Wen F, Chen H, et al. Analysis of the pathogenic bacteria, drug resistance, and risk factors of postoperative infection in patients with non-small cell lung cancer. Ann Palliat Med. 2021;10(9):10005–10012. doi:10.21037/apm-21-2364
24. Akinosoglou KS, Karkoulias K, Marangos M. Infectious complications in patients with lung cancer. Eur Rev Med Pharmacol Sci. 2013;17(1):8–18.
25. Gopallawa I, Dehinwal R, Bhatia V, Gujar V, Chirmule N. A four-part guide to lung immunology: invasion, inflammation, immunity, and intervention. Front Immunol. 2023;14:1119564. doi:10.3389/fimmu.2023.1119564
26. Jiang J, Bai L, Yang W, et al. Metagenomic next-generation sequencing for the diagnosis of pneumocystis jirovecii pneumonia in non-HIV-infected patients: a retrospective study. Infect Dis Ther. 2021;10(3):1733–1745. doi:10.1007/s40121-021-00482-y
27. Wirsdörfer F, Jendrossek V. The role of lymphocytes in radiotherapy-induced adverse late effects in the lung. Front Immunol. 2016;7:591. doi:10.3389/fimmu.2016.00591
28. Piguet PF, Collart MA, Grau GE, Kapanci Y, Vassalli P. Tumor necrosis factor/cachectin plays a key role in bleomycin-induced pneumopathy and fibrosis. J Exp Med. 1989;170(3):655–663. doi:10.1084/jem.170.3.655
29. Piccinini AM, Midwood KS. DAMPening inflammation by modulating TLR signalling. Mediators Inflamm. 2010;2010:1–21. doi:10.1155/2010/672395
30. Kolb M, Margetts PJ, Anthony DC, Pitossi F, Gauldie J. Transient expression of IL-1beta induces acute lung injury and chronic repair leading to pulmonary fibrosis. J Clin Invest. 2001;107(12):1529–1536. doi:10.1172/jci12568
31. Ekstrand-Hammarström B, Wigenstam E, Bucht A. Inhalation of alkylating mustard causes long-term T cell-dependent inflammation in airways and growth of connective tissue. Toxicology. 2011;280(3):88–97. doi:10.1016/j.tox.2010.11.012
32. Cao Q, Wu X, Chen Y, et al. The impact of concurrent bacterial lung infection on immunotherapy in patients with non-small cell lung cancer: a retrospective cohort study. Front Cell Infect Microbiol. 2023;13:1257638. doi:10.3389/fcimb.2023.1257638
33. Liew PX, Kubes P. The neutrophil’s role during health and disease. Physiol Rev. 2019;99(2):1223–1248. doi:10.1152/physrev.00012.2018
34. Mori K, Janisch F, Mostafaei H, et al. Prognostic value of preoperative blood-based biomarkers in upper tract urothelial carcinoma treated with nephroureterectomy: a systematic review and meta-analysis. Urol Oncol. 2020;38(5):315–333. doi:10.1016/j.urolonc.2020.01.015
35. Duran AO, Inanc M, Karaca H, et al. Albumin-globulin ratio for prediction of long-term mortality in lung adenocarcinoma patients. Asian Pac J Cancer Prev. 2014;15(15):6449–6453. doi:10.7314/apjcp.2014.15.15.6449
36. Kanoh Y, Ohara T, Akahoshi T. Acute inflammatory biomarkers in cerebrospinal fluid as indicators of blood cerebrospinal fluid barrier damage in Japanese subjects with infectious meningitis. Clin Lab. 2011;57(1–2):37–46.
37. Kanoh Y, Ohtani H. Levels of interleukin-6, CRP and alpha 2 macroglobulin in cerebrospinal fluid (CSF) and serum as indicator of blood-CSF barrier damage. Biochem mol Biol Int. 1997;43(2):269–278. doi:10.1080/15216549700204051
38. Frey A, Martin D, D’Cruz L, Fokas E, Rödel C, Fleischmann M. C-reactive protein to albumin ratio as prognostic marker in locally advanced non-small cell lung cancer treated with chemoradiotherapy. Biomedicines. 2022;10(3):598. doi:10.3390/biomedicines10030598
39. Barlesi F, Vansteenkiste J, Spigel D, et al. Avelumab versus docetaxel in patients with platinum-treated advanced non-small-cell lung cancer (JAVELIN Lung 200): an open-label, randomised, phase 3 study. Lancet Oncol. 2018;19(11):1468–1479. doi:10.1016/s1470-2045(18)30673-9
40. Zhao Z, Li X, Zhao Y, et al. Role of C-reactive protein and procalcitonin in discriminating between infectious fever and tumor fever in non-neutropenic lung cancer patients. Medicine (Baltimore). 2018;97(33):e11930. doi:10.1097/md.0000000000011930
41. Norman-Bruce H, Umana E, Mills C, et al. Diagnostic test accuracy of procalcitonin and C-reactive protein for predicting invasive and serious bacterial infections in young febrile infants: a systematic review and meta-analysis. Lancet Child Adolesc Health. 2024;8(5):358–368. doi:10.1016/s2352-4642(24)00021-x
42. Matsubara T, Takamori S, Haratake N, et al. Identification of the best prognostic marker among immunonutritional parameters using serum C-reactive protein and albumin in non-small cell lung cancer. Ann Surg Oncol. 2021;28(6):3046–3054. doi:10.1245/s10434-020-09230-x
43. Chen Y, Wen S, Xia J, et al. Corrigendum: association of dynamic changes in peripheral blood indexes with response to PD-1 inhibitor-based combination therapy and survival among patients with advanced non-small cell lung cancer. Front Immunol. 2021;12:713268. doi:10.3389/fimmu.2021.713268
44. Tekin A, Wireko FW, Gajic O, Odeyemi YE. The neutrophil/lymphocyte ratio and outcomes in hospitalized patients with community-acquired pneumonia: a retrospective cohort study. Biomedicines. 2024;12(2):260. doi:10.3390/biomedicines12020260
45. Sebastian NT, Raj R, Prasad R, et al. Association of pre- and posttreatment neutrophil-lymphocyte ratio with recurrence and mortality in locally advanced non-small cell lung cancer. Front Oncol. 2020;10:598873. doi:10.3389/fonc.2020.598873
46. Yun NK, Rouhani SJ, Bestvina CM, et al. Neutrophil-to-lymphocyte ratio is a predictive biomarker in patients with Epidermal Growth Factor Receptor (EGFR) Mutated Advanced Non-Small Cell Lung Cancer (NSCLC) Treated with Tyrosine Kinase Inhibitor (TKI) Therapy. Cancers (Basel). 2021;13(6):1426. doi:10.3390/cancers13061426
47. Asik Z. The role of the NLR and PLR in urinary tract infection. Clin Lab. 2021;67(10). doi:10.7754/Clin.Lab.2021.210133
48. Khan N, Kumar V, Li P, et al. Inhibiting Eph/ephrin signaling reduces vascular leak and endothelial cell dysfunction in mice with sepsis. Sci Transl Med. 2024;16(744):eadg5768. doi:10.1126/scitranslmed.adg5768
49. Ackermann M, Verleden SE, Kuehnel M, et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in covid-19. N Engl J Med. 2020;383(2):120–128. doi:10.1056/NEJMoa2015432
50. Ma M, Cao R, Wang W, et al. The D-dimer level predicts the prognosis in patients with lung cancer: a systematic review and meta-analysis. J Cardiothorac Surg. 2021;16(1):243. doi:10.1186/s13019-021-01618-4
51. Bi H, Yin L, Fang W, Song S, Wu S, Shen J. Association of CEA, NSE, CYFRA 21-1, SCC-Ag, and ProGRP with clinicopathological characteristics and chemotherapeutic outcomes of lung cancer. Lab Med. 2023;54(4):372–379. doi:10.1093/labmed/lmac122
52. World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent. 2014;81(3):14–18.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Machine Learning for Prediction of Non-Small Cell Lung Cancer Based on Inflammatory and Nutritional Indicators in Adults: A Cross-Sectional Study
Wang Q, Liang T, Li Y, Liu X
Cancer Management and Research 2024, 16:527-535
Published Date: 30 May 2024