")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
The Interface of a Leaky Gut with Reduced Sarcopenia-Related Quality of Life (SarQoL) in Patients with Chronic Obstructive Pulmonary Disease
Authors Qaisar R , Karim A , Muhammad T, Ahmad F, Marinho DA, Arkadianos I , Alkahtani S
Received 7 January 2025
Accepted for publication 20 May 2025
Published 24 June 2025 Volume 2025:20 Pages 2049—2059
DOI https://doi.org/10.2147/COPD.S511562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Rizwan Qaisar,1– 3 Asima Karim,1,4 Tahir Muhammad,5 Firdos Ahmad,1– 3 Daniel Almeida Marinho,6,7 Ioannis Arkadianos,8 Shaea Alkahtani9
1Department of Basic Medical Sciences, College of Medicine, University of Sharjah, Sharjah, 27272, United Arab Emirates; 2Space Medicine Research Group, Research Institute of Medical and Health Sciences, University of Sharjah, Sharjah, 27272, United Arab Emirates; 3Cardiovascular Research Group, Research Institute of Medical and Health Sciences, University of Sharjah, Sharjah, 27272, United Arab Emirates; 4Iron Biology Research Group, Research Institute of Medical and Health Sciences, University of Sharjah, Sharjah, 27272, United Arab Emirates; 5Department of Biochemistry, Gomal Medical College, Dera Ismail Khan, 29111, Pakistan; 6Department of Sport Sciences, University of Beira Interior, Covilhã, 6200-001, Portugal; 7Research Center in Sports Sciences, Health Sciences and Human Development, CIDESD, Covilhã, 6200-001, Portugal; 8Head Quarter Office, European Lifestyle Medicine Organization (ELMO), Geneva, 1201, Switzerland; 9Exercise Physiology Department, College of Sport Sciences and Physical Activity, King Saud University, Riyadh, 11451, Saudi Arabia
Correspondence: Shaea Alkahtani, Exercise Physiology Department, College of Sport Sciences and Physical Activity, King Saud University, Riyadh, 11451, Saudi Arabia, Tel +96611806304, Fax +966118063370, Email [email protected]
Purpose: Patients with chronic obstructive pulmonary disease (COPD) frequently exhibit intestinal leaks and age-related muscle impairment, termed sarcopenia. The sarcopenia-related quality-of-life (SarQoL) is a tool to evaluate the quality of life of sarcopenic patients. However, the association of intestinal leak with SarQoL in COPD patients remains unknown.
Methods: We recruited male controls (n=87, age=72.7± 6.7 years) and COPD patients (n=81, age=70.9± 5.8 years) to validate the Pashto version of SarQoL. This was followed by an investigation of the sarcopenia indices, including handgrip strength (HGS), skeletal mass index (SMI), and gait speed. We also measured plasma zonulin (a marker of intestinal leak) and lipopolysaccharides binding protein (LBP) (a marker of bacterial load).
Results: We first confirmed the reliability of Pashto SarQoL by demonstrating its internal consistency, test-retest reliability, and absence of a floor-and-ceiling effect. Next, we report that COPD patients had higher plasma zonulin and LBP levels and lower SarQoL, HGS, SMI, and gait speed than controls (all p< 0.05). Plasma zonulin demonstrated inverse correlations with SarQoL domains for locomotion, functionality, activities of daily living, and cumulative SarQoL scores in COPD patients (all p< 0.05). Further, higher LBP levels were correlated with lower scores on SarQoL domains for physical and mental health, locomotion, functionality, fear, and cumulative SarQoL scores (all p< 0.05).
Conclusion: In conclusion, intestinal leaks and associated bacterial load potentially contribute to reduced SarQoL in COPD patients. Future studies should investigate intestinal mucosal repair as a therapeutic option in COPD patients.
Keywords: zonulin, SarQoL, quality of life, handgrip strength, COPD
Introduction
Chronic obstructive pulmonary disease (COPD) is primarily a respiratory disease characterized by progressive airflow obstruction and systemic inflammation.1 COPD patients also exhibit a decline in multiple body organs, including skeletal muscle.1 Specifically, these patients demonstrate an advanced form of age-related muscle decline, termed sarcopenia. The characteristic features of sarcopenia in COPD include muscle weakness, wasting, and lower physical capacity than age-matched controls.1
The etiology of sarcopenia is multifactorial and includes a sedentary lifestyle, comorbidities, nutritional deficiencies, genetics, and hormonal defects.2,3 Recently, a pathological increase in intestinal permeability has been recognized as a critical cause of sarcopenia.4 Specifically, intestinal mucosal disruption and a leaky intestine allow the translocation of harmful bacteria and their products into blood, which damages skeletal muscle and exacerbates the sarcopenia phenotype.4 We have recently reported that COPD patients exhibit a higher intestinal permeability than age-matched controls.5 These patients also had higher plasma zonulin levels, a marker of intestinal leak. The intestinal barrier dysfunction in these patients may contribute to malabsorption of nutrients6 with detrimental effects on skeletal muscle mass and strength.7 This notion is supported by the established prevalence of malnutrition in COPD8 and its documented association with intestinal permeability.6 The malnutrition and sarcopenia phenotype observed in COPD manifests across multiple muscle groups, including the diaphragm.9 Diaphragmatic weakness in COPD is implicated in respiratory insufficiency, reduced diaphragmatic excursion during inspiration, and diminished tidal volume.9 Collectively, these pathological alterations in COPD can lead to impaired systemic oxygenation, potentially exacerbating the sarcopenic phenotype.10 Additionally, plasma zonulin levels in these patients correlate with sarcopenia phenotype and indicate the potential contribution of intestinal leak to muscle decline in COPD.5 These findings are generally consistent in sarcopenia patients with various age-related diseases.11,12
COPD patients frequently present with an impaired quality of life (QoL) than age-matched controls.13 Furthermore, the QoL worsens with increasing disease severity, duration, exacerbations, and hospitalization.13 Sarcopenia is also a critical factor for impaired QoL in these patients. This is partly because patients with sarcopenia exhibit physical and mental decline, which comprise their independent lifestyle and reduce QoL.14 It is also generally recognized that sarcopenic patients exhibit functional dependency, reduced leisure activities, reduced activities of daily living, and reduced locomotion.15 Most QoL tools are generic and do not consider these attributes associated with the sarcopenia phenotype. In this context, sarcopenia-related QoL (SarQoL) has recently been developed to evaluate multiple domains related to sarcopenia, including physical and mental health, locomotion, body composition, functionality, activities of daily living, leisure activities, and fear.16 The SarQoL exhibits adequate internal consistency and diagnostic potential for sarcopenia-related QoL domains.17–19
Several general and disease-specific tools have been developed to measure QoL in COPD patients.13 However, these tools generally overlook sarcopenia and related QoL domains. Thus, SarQoL may be a relevant tool for evaluating QoL associated with sarcopenia in COPD patients. However, no previous study has investigated SarQoL in COPD patients.
Our recent findings have demonstrated a causal link between a pathological increase in intestinal leak and postural instability in individuals with COPD.20 Specifically, a gradual increase in plasma zonulin levels shows a corresponding reduction in the ability to maintain postural balance.20 Postural imbalance is also independently correlated with sarcopenia phenotype in old age.21 However, the impact of intestinal leaks on the QoL in COPD patients remains unexplored. Due to its well-recognized association with sarcopenia, intestinal leak may also negatively affect the SarQoL domains in COPD patients. However, the association between a leaky gut and QoL remains elusive. Additionally, it is not known how plasma zonulin levels correlate with SarQoL in COPD patients.
We investigated the associations of plasma zonulin with individual SarQoL domains in COPD patients. In addition, we measured plasma markers of inflammation, oxidative stress, and bacterial load to dissect the mechanistic associations between intestinal leak and reduced SarQoL in COPD. We hypothesized that plasma zonulin may exhibit significant negative correlations with several domains of SarQoL. In addition, elevated systemic oxidative stress, inflammation, and bacterial load are associated with reduced SarQoL in COPD patients.
Materials and Methods
Study Design & Participants
After obtaining ethics approval from the hospital ethics committee, we randomly selected controls (n = 87) and COPD patients (n = 81) at the tertiary-care hospital of Gomal Medical College, Dera Ismail Khan (approval number: HREC-19-02-03-01). A sample size of 78–80 participants per group was calculated to achieve 80% power (alpha=0.05, beta = 0.2) in detecting a difference between control (SarQoL score = 80 ± 6) and COPD (SarQoL score = 78) groups. Thus, the sample size of 87 controls and 81 COPD patients ensured sufficient statistical power for the study. All participants were recruited from a parent cohort characterized elsewhere by us.5,22 COPD was diagnosed according to the guidelines of the global initiative for chronic obstructive lung disease.23 We excluded subjects with non-ambulance, major diseases, chronic bed rest, recent surgeries, and major organ failures.24 All participants were Caucasian men and provided written informed consent. The study was conducted following the declaration of Helsinki.25
SarQoL Measurement
The robustness and internal consistency of SarQoL is recently reported.18,26 We used a recently described version of SarQoL,26 translated for Pashto-speaking participants. We recently reported the validation of Pashto SarQoL.27 The validation process includes testing the internal consistency, test-retest reliability, construct validity, discriminative potential, and an absence of floor and ceiling effect.27 Following the validation, the Pashto SarQoL was categorized into seven domains as D1-D7, relevant to physical and mental health, locomotion, body composition, functionality, activities of daily living, leisure activities, and fear.28 The percent cumulative score of seven domains was also used for statistical analysis.
Assessment of Sarcopenia Indices
Sarcopenia was diagnosed according to the revised criteria of the European working group on sarcopenia in old people (EWGSOP2) for men.11 The criteria include concomitant presence of low handgrip strength (HGS) of < 27 kg, low skeletal muscle mass index (SMI) of < 7 kg/m2, and a low gait speed of ≤ 0.8 m/s for diagnosing sarcopenia.23 HGS was measured with a handgrip dynamometer (CAMRY, South El Monte, CA, USA), as described before.29,30 Briefly, the participants were requested to sit on a chair and use the maximal strength of their dominant hand to squeeze the dynamometer without changing their body posture. The highest of the three recordings was used for analysis. SMI and body fat content were measured with a bioelectrical impedance analysis (BIA) scale (RENPHO, Dubai, UAE).31 The gait speed was measured by asking the participants to walk over a straight line for six meters at their routine pace. The time taken to complete the test was divided by the distance to calculate the gait speed, as described before.32
Measurement of Plasma Biomarkers
All blood samples were collected from cubital veins in heparin syringes between 0900 and 1100 hours following an overnight fast. The samples were centrifuged at 3000 revolutions per minute for ten minutes to obtain plasma for storage at −80°C.33 We used ELISA kits to measure the plasma levels of zonulin (Cat # K5601, Immundiagnostik AG, Bensheim, Germany), lipopolysaccharides binding protein (LBP) (Cat # ab279407, Abcam, Biomedical Scientific Services LLC, Al-Ain, Abu Dhabi 69480, UAE) 8–isoprostanes (Cayman Chemical, Ann Arbor, MI, USA), and c-reactive proteins (CRP) (R&D Systems, Minneapolis, MN, USA), as described elsewhere.12,34,35
Statistical Analysis
The control and COPD patients were compared using an unpaired t-test. Associations of SarQoL with plasma LBP, zonulin, and sarcopenia indices were measured using correlation analysis. Data are presented as mean ± standard deviation, and a p-value of < 0.05 was considered statistically significant. We used GraphPad Prism 8 (Graph Stats Technologies Private Limited, Bangalore 560035, India) for statistical analysis.
Results
Characteristics of the Participants
There was no difference in the age of participants between controls and COPD patients (Table 1). However, COPD patients had higher BMI and lower HGS, SMI, and gait speed than controls (all p < 0.05). COPD patients also exhibited lower SarQoL scores than controls, when categorized according to sarcopenia status (p < 0.05) (Table 1). We also found lower proportions of non-smokers and higher systolic and diastolic blood pressures in COPD patients than in controls (all p < 0.05) (Table 1). COPD patients had higher plasma zonulin levels than controls (p < 0.05). These patients also exhibited higher levels of total cholesterol, 8-isoprostanes, CRP, and LBP while lower HDL-cholesterol levels than controls (all p < 0.05). Conversely, the plasma levels of hemoglobin and HbA1c were similar between the two groups (Table 1).
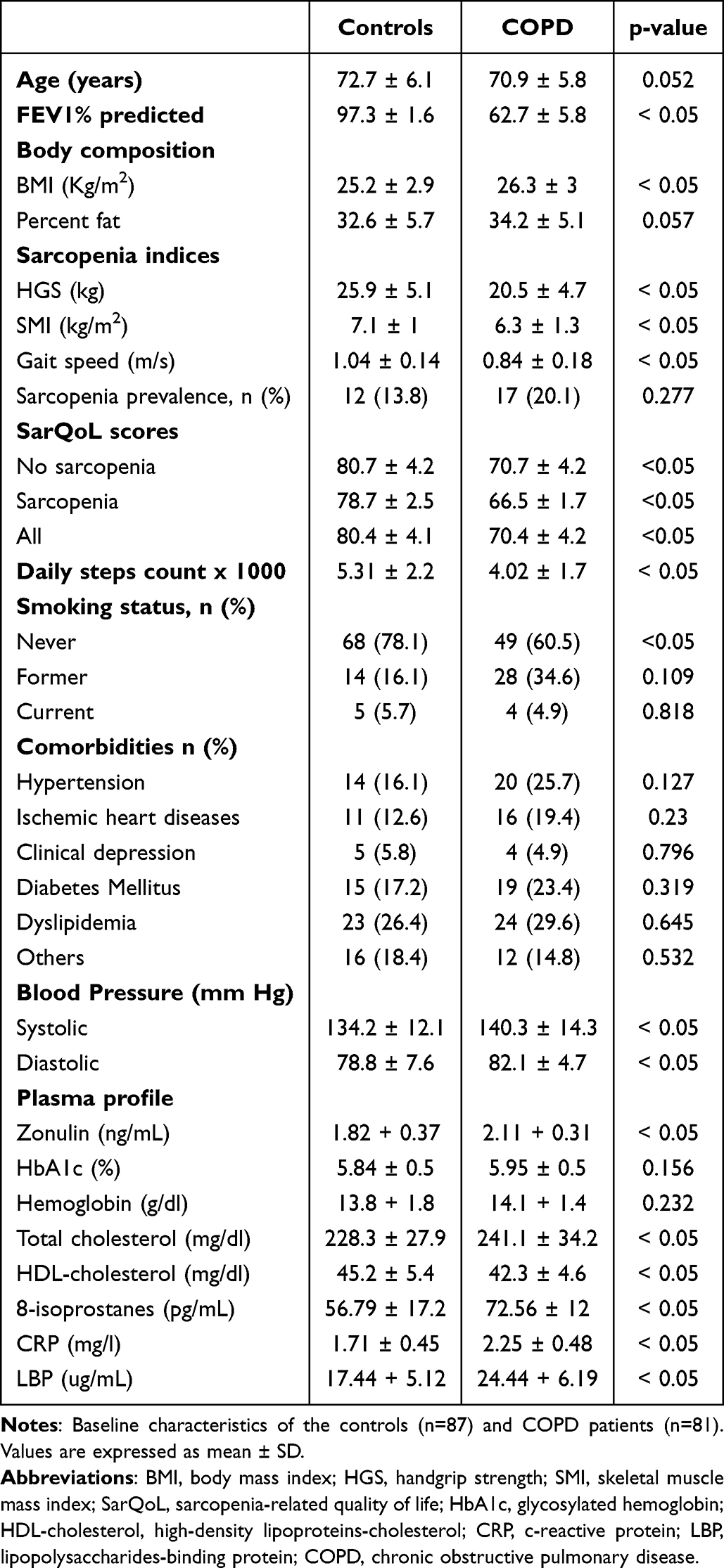 |
Table 1 Characteristics of the Study Population |
Validation of Pashto SarQoL
First, we confirmed the internal consistency of Pashto SarQoL by correlating the individual SarQoL domains with cumulative SarQoL scores in the study participants. All SarQoL domains exhibited positive correlations with cumulative SarQoL, confirming the internal consistency of the translated version (Table 2). Next, we confirmed the test-retest reliability of Pashto SarQoL by comparing a subset of sarcopenic patients with unchanged health over two weeks. All SarQoL domains exhibited significant ICCs, confirming the test-retest reliability of Pashto SarQoL (Table 2). Lastly, we confirmed the absence of floor-and-ceiling effect by finding that no patient obtained minimal or maximal scores on individual domains or cumulative SarQoL.
 |
Table 2 Validation of Pashto SarQoL |
SarQoL Scores
Next, we measured the scores for individual SarQoL domains among the two groups (Table 3). When compared to controls, COPD patients had significantly lower scores for physical and mental health (mean difference ± SEM = −14.18 ± 1.48, 95% C.I = −17.11 to −11.25, p-value = < 0.0001), locomotion (mean difference ± SEM = −9.74 ± 1.35, 95% C.I = −12.42 to −7.06, p-value = < 0.0001), body composition (mean difference ± SEM = −9.04 ± 1.91, 95% C.I = −12.83 to −5.27, p-value = < 0.0001), functionality (mean difference ± SEM = −14.1 ± 1.51, 95% C.I = −17.07 to −11.13, p-value = < 0.0001), and activities of daily living (mean difference ± SEM = −14.57 ± 1.9, 95% C.I = −18.33 to −10.82, p-value = < 0.0001). Conversely, the scores for leisure activities and fear were similar between the two groups. Lastly, the COPD patients had lower cumulative SarQoL scores than in controls (mean difference ± SEM = −10.01 ± 0.634, 95% C.I = −11.26 to −8.75, p-value = < 0.0001) (Table 3). We also found lower SarQoL scores in sarcopenic vs non-sarcopenic participants for controls (80.7 ± 4.2 vs 78.7 ± 2.5, p<0.05) and COPD patients (70.7 ± 4.2 vs 66.5 ± 1.7, p<0.05) (Table 1). Lastly, the COPD patients exhibited lower SarQoL scores than controls, when categorized according to the absence (80.7 ± 4.2 vs 70.7 ± 4.2, p<0.05) or presence (78.7 ± 2.5 vs 66.5 ± 1.7, p<0.05) of sarcopenia (Table 1).
 |
Table 3 SarQoL Scores of Controls and COPD Patients |
Associations of SarQoL with Plasma Zonulin
We next investigated the potential contributions of intestinal leak to reduced SarQoL by evaluating the associations of various SarQoL domains with plasma zonulin levels (Figure 1). The SarQoL domain for physical and mental health significantly correlated with plasma zonulin in the control group (r2 = 0.091, p = 0.004) but not in COPD patients (Figure 1A). Next, the SarQoL domain for locomotion exhibited significant correlations with plasma zonulin in controls (r2 = 0.073, p = 0.011) and COPD patients (r2 = 0.124, p = 0.001) (Figure 1B). No significant correlations were found between body composition and plasma zonulin (Figure 1C). However, the SarQoL domain for functionality exhibited significant correlations with plasma zonulin in controls (r2 = 0.168, p < 0.001) and COPD patients (r2 = 0.186, p < 0.001) (Figure 1D). The SarQoL domain for activities of daily living also exhibited significant correlations with plasma zonulin in controls (r2 = 0.112, p = 0.002) and COPD patients (r2 = 0.146, p = 0.004) (Figure 1E). However, the domains for leisure activities and fear exhibited no significant correlations with plasma zonulin (Figures 1F and G, respectively). Lastly, the cumulative SarQoL scores were significantly correlated with plasma zonulin in controls (r2 = 0.208, p < 0.001) and COPD patients (r2 = 0.163, p = 0.002) (Figure 1H).
 |
Figure 1 Correlations of plasma zonulin levels with SarQoL domains of physical and mental health (A), locomotion (B), body composition (C), functionality (D), activities of daily living (E), leisure activities (F), fear (G), and percent cumulative scores (H) in controls and COPD patients. Abbreviations: SarQoL, sarcopenia-related quality of life; COPD, chronic obstructive pulmonary disease. |
Associations of Cumulative SarQoL Scores with Sarcopenia Indices
We next asked if the reduction in SarQoL in COPD patients is potentially due to sarcopenia phenotype. Therefore, we evaluated the associations between cumulative SarQoL scores and sarcopenia indices of HGS, SMI, and gait speed. The cumulative SarQoL exhibited significant correlations with HGS in controls (r2 = 0.071, p = 0.012) and COPD patients (r2 = 0.088, p = 0.007) (Figure 2A). However, similar correlations of cumulative SarQoL scores with SMI were not found in the study cohort (Figure 2B). Conversely, cumulative SarQoL exhibited weak but statistically significant correlations with gait speed in controls (r2 = 0.052, p = 0.033) and COPD patients (r2 = 0.061, p = 0.025) (Figure 2C).
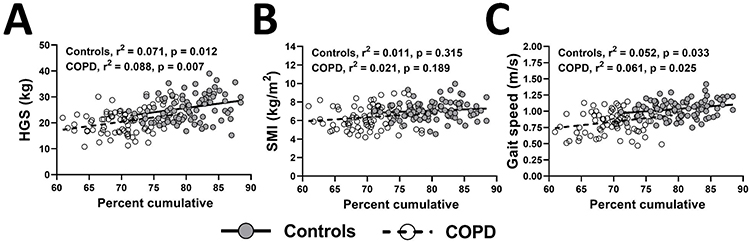 |
Figure 2 Correlations of percent cumulative SarQoL scores with sarcopenia indices of HGS (A), SMI (B), and gait speed (C) in controls and COPD patients. Abbreviations: SarQoL, sarcopenia-related quality of life; HGS, handgrip strength; SMI, skeletal mass index; COPD, chronic obstructive pulmonary disease. |
Associations of SarQoL Domains with Plasma Markers
Next, we dissected the potential mechanistic associations between intestinal leak and reduced SarQoL in COPD patients. An intestinal leak causes elevated systemic oxidative stress, inflammation, and bacterial load. Thus, we investigated the correlations of plasma 8-isoprostanes (markers of oxidative stress), CRP (marker of inflammation), and LBP (marker of bacterial load) with SarQoL domains (Table 4). Among different markers, plasma 8-isoprostanes exhibited significant correlations with SarQoL domains for physical and mental health, locomotion, functionality, and activities of daily living in controls and COPD patients (all p < 0.05) (Table 4). Conversely, plasma CRP did not exhibit significant correlations with any of the SarQoL domains in both groups. However, plasma LBP exhibited significant correlations with domains for physical and mental health, locomotion, functionality, and fear in COPD patients (all p < 0.05) (Table 4). Lastly, the cumulative SarQoL scores exhibited significant correlations with plasma 8-isoprostanes and LBP levels in controls and COPD patients (both p < 0.05) (Table 4).
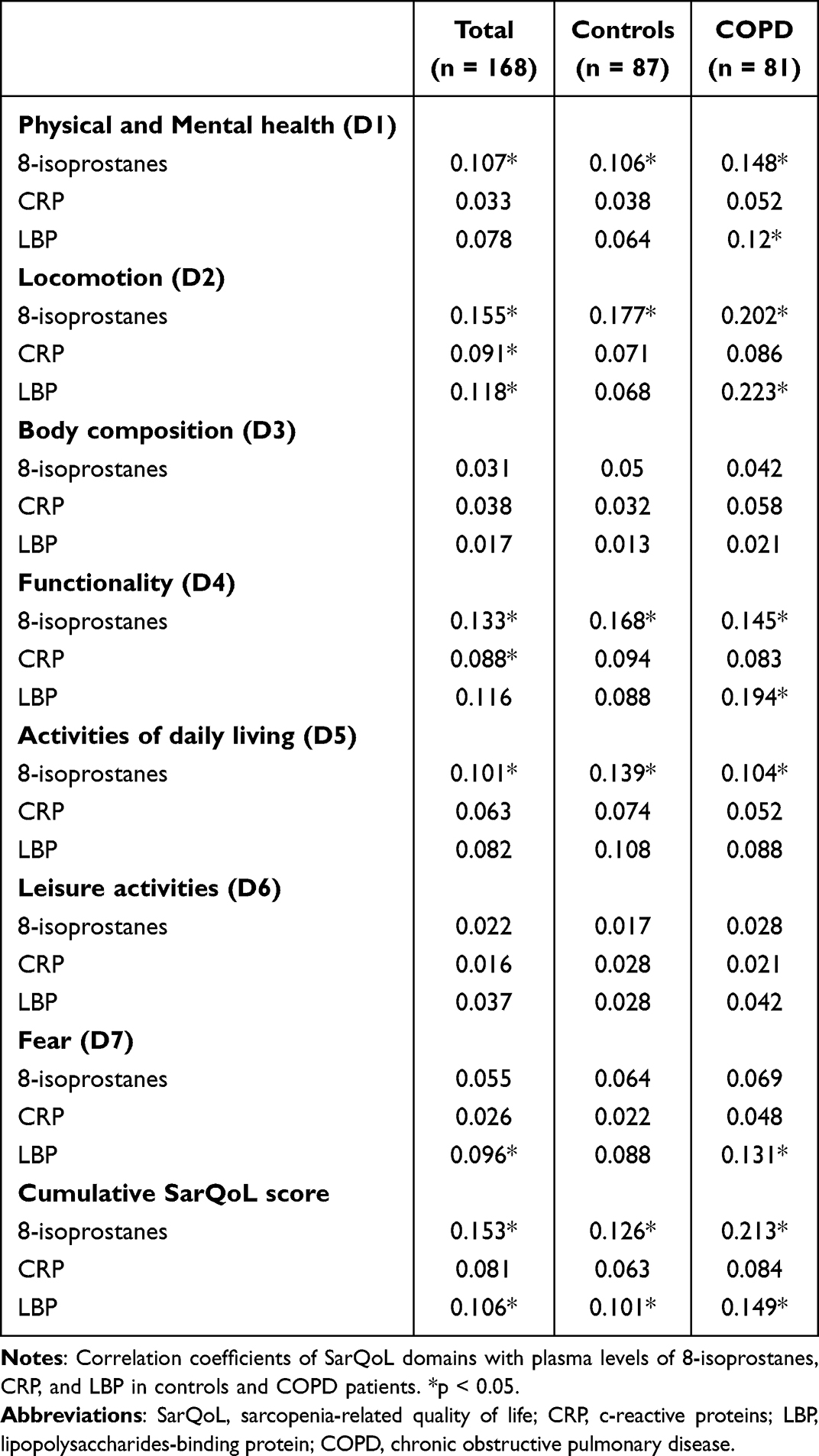 |
Table 4 SarQoL and Plasma Biomarkers |
Discussion
The major findings of our study include lower SarQoL scores and higher plasma zonulin levels in COPD patients than in controls. Plasma zonulin exhibited significant correlations with several SarQoL domains, including locomotion, functionality, activities of daily living, and cumulative SarQoL scores. We also found significant correlations of SarQoL with HGS and gait speed, validating the association between muscle decline and low SarQoL. Lastly, elevated plasma 8-isoprostanes and LBP may partly explain the mechanistic interface between a leaky gut and reduced SarQoL in COPD patients.
COPD patients exhibited lower scores on several domains of SarQoL, including physical and mental health, locomotion, body composition, functionality, and activities of daily living. These domains of daily life are primarily controlled by healthy skeletal muscle. For example, the optimal functioning of appendicular skeletal muscles is critical for maintaining locomotion and activities of daily living.15 Thus, patients with muscle weakness and/or atrophy exhibit a dependent lifestyle for daily activities. While no relevant data about SarQoL from COPD patients has been previously reported, the muscle decline in COPD patients indirectly supports and validates our findings. Specifically, we found lower HGS, SMI, and gait speed in COPD patients, translating into a reduced physical capacity and decline in several SarQoL domains associated with a functional lifestyle. Interestingly, COPD patients did not demonstrate a decline in leisure activities and fear. It is possible that the subjective nature of leisure activities and fear may be responsible for our observation. Additionally, fear is primarily associated with emotional health rather than physical health. Thus, the decline in physical health in COPD may not be coupled with emotional health. Interestingly, two recent studies did not find a decline in the fear domain of SarQoL despite the appearance of sarcopenia phenotype.17,26
Previous reports support our observation of higher plasma zonulin in COPD patients.5,23 This observation indicates the potential contribution of intestinal leak to disease phenotype in COPD. We have recently reported the contribution of intestinal leak to muscle weakness, wasting, and reduced physical capacity in patients with COPD23 and other age-related diseases.11,12 Together, these reports signify intestinal leak as a critical contributor to sarcopenia phenotype. Here, we extend these findings to report the potential contribution of intestinal leak to reduced SarQoL in COPD. We found robust correlations of plasma zonulin with SarQoL domains associated with functionality, locomotion, and activities of daily living. Interestingly, these domains are primarily governed by skeletal muscle and physical health. For example, people with skeletal muscle wasting and weakness exhibit reduced mobility and activities of daily living.15 Thus, it is imperative to think that the intestinal leak potentially impairs functionality, locomotion, and activities of daily living by negatively affecting skeletal muscle. Conversely, plasma zonulin demonstrated no significant correlations with domains for physical and mental health, body composition, leisure activities, and fear in COPD patients. These domains are partly subjective and are constructs of emotional health. Thus, it is possible that intestinal leak may not be a potential determinant of subjective attributes associated with emotional health.
Despite variations in individual domains, cumulative SarQoL exhibited significant correlations with plasma zonulin in COPD patients. These observations reflect the systemic detrimental effects of intestinal leaks on generalized health and QoL.36 While relevant studies are scarce, our findings agree with previous data on reduced subjective QoL in adults with increased intestinal permeability.37 However, intestinal leak negatively affects multiple body organs other than skeletal muscle. Therefore, the reduction in SarQoL in COPD patients may be independent of the sarcopenia phenotype. To further dissect the potential contribution of sarcopenia to reduced SarQoL, we performed a correlation analysis of sarcopenia indices with cumulative SarQoL scores. We found mild but significant correlations of cumulative SarQoL scores with HGS and gait speed in COPD patients. These observations validate and expand the interface of sarcopenia phenotype with SarQoL, as reported previously.19,38 However, SMI did not exhibit any significant correlation with plasma zonulin in COPD patients. A reduced SMI is considered a marker of muscle wasting. However, it is recently recognized that muscle weakness precedes muscle wasting in cachexia.39 Similarly, we have previously reported a greater decline in muscle strength than in muscle mass in various atrophying conditions.40,41 Lastly, muscle weakness may be a stronger predictor of reduced QoL than muscle wasting.
Plasma LBP levels reflect circulating bacterial load in patients with intestinal mucosal disruption.35 Thus, high LBP in patients with intestinal leak means a higher translocation of harmful bacteria from the gut into blood circulation with systemic negative consequences.35 We found higher plasma LBP levels in COPD patients, which are consistent with elevated plasma levels in these patients. LBP levels were also significantly correlated with SarQoL domains for physical and mental health, locomotion, and functionality. Plasma LBP and bacterial loads exhibit significant correlations with muscle strength and physical capacity in old age.42,43 Specifically, the composite scores of gait speed, ability to maintain postural balance, and rising from a chair were inversely correlated with plasma LBP levels.42 These physical attributes are critical for maintaining the functionality of everyday life. Thus, these findings support our observation of negative correlations of plasma LBP with SarQoL domains of functionality and locomotion. Plasma LBP is also an acute phase reactant positively associated with systemic inflammation.42 COPD is an inflammatory disease, and skeletal muscle is susceptible to damage by inflammatory cytokines. Thus, it is possible that the elevated bacterial load and systemic inflammation cause or contribute to sarcopenia and reduced SarQoL in COPD patients.
The elevated plasma 8-isoprostane levels in COPD patients reflect increased oxidative stress, a critical trigger of skeletal muscle decline.44 We have previously reported a positive correlation between plasma zonulin and 8-isoprostane levels, inferring the potential contribution of intestinal leak to systemic oxidative stress. It is generally recognized that elevated oxidative stress is a critical trigger of accelerated sarcopenia phenotype in old age.44,45 Here, we extend these findings to report the negative correlations of increased 8-isoprostane levels with reduced SarQoL scores in COPD patients. Specifically, 8-isoprostanes exhibited negative correlations with functionality, locomotion, and activities of daily living in these patients. Together, these findings show intestinal leak may trigger sarcopenia phenotype and reduce SarQoL by elevating systemic oxidative stress.
Due to the well-established respiratory insufficiency in COPD, diaphragm dysfunction may be more relevant for disease phenotype and QoL than the weakness of limb muscles. Diaphragm dysfunction is associated with poor spirometry performance in COPD with negative consequences for other body systems due to systemic hypoxia.9 It is possible that the intestinal leak affects diaphragm muscle by inducing malnutrition and systemic inflammation. The lower FEV1% in COPD patients suggest diaphragm dysfunction, which may have contributed to reduced SarQoL and sarcopenia phenotype.
Several strengths enhance the biological relevance of our study. The SarQoL is a simple, self-administered, and user-friendly tool that demonstrates similar efficacy to better-recognized tools, such as SARC-F.38 Measurement of plasma zonulin requires ≈ 15 µL of blood and can be performed in most clinical laboratories using a routine ELISA plate reader. HGS measurements require a simple dynamometer and no major technical expertise. All study participants had a consistent racial, cultural, and socioeconomic background.
The major limitation of this study is that we did not measure knee extensor strength, which may be more relevant to daily functioning and locomotion than HGS. However, in our experience, the HGS and testing of lower limb function show similar correlations in sarcopenic and non-sarcopenic men.11,32 We also found poor correlations of sarcopenia indices with SarQoL scores. However, sarcopenic patients exhibited lower SarQoL scores than the non-sarcopenic participants in both the controls and COPD patients. We did not investigate the diaphragm function, which may be more relevant to COPD phenotype than the limb muscles. We did not use dual X-ray absorptiometry (DXA) to measure muscle mass, which may be more accurate than BIA. However, adequate consistency has been reported between BIA and DXA for quantifying muscle mass.46 This study does not include women and may overlook the potential gender bias in our findings.
Altogether, we report higher plasma zonulin levels and lower SarQoL in COPD patients than in controls. Plasma zonulin also exhibited significant negative correlations with several SarQoL domains, including physical and mental health, locomotion, functionality, and activities of daily living. Our data indicate heightened circulating bacterial load and oxidative stress as potential mechanisms of reduced SarQoL due to intestinal leak. Future studies should use causal and mechanistic approaches to characterize the relationship between intestinal leak and SarQoL.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Statement of Ethics
The study was approved by the research ethics committee of the tertiary-care hospital of Gomal Medical College, Dera Ismail Khan (approval number: HREC-19-02-03-01).
Consent to Participate
Informed consent was obtained from all participants in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by a competitive grant (number: 24010901166) from the University of Sharjah to Rizwan Qaisar. The authors extend their appreciation to the Ongoing Research Funding Program (ORF - 2025 - 277), King Saud University, Riyadh, Saudi Arabia for funding this research. This work is supported by national funding through the Portuguese Foundation for Science and Technology, I.P., under project UIDB/04045/2020.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Gea J, Agusti A, Roca J. Pathophysiology of muscle dysfunction in COPD. J Appl Physiol. 2013;114(9):1222–1234. doi:10.1152/japplphysiol.00981.2012
2. Parvatiyar MS, Qaisar R. Editorial: skeletal muscle in age-related diseases: from molecular pathogenesis to potential interventions. Front Physiol. 2022;13:1056479. doi:10.3389/fphys.2022.1056479
3. Qaisar R, Ustrana S, Muhammad T, et al. Sarcopenia in pulmonary diseases is associated with elevated sarcoplasmic reticulum stress and myonuclear disorganization. Histochem Cell Biol. 2022;157(1):93–105. doi:10.1007/s00418-021-02043-3
4. Zhao J, Huang Y, Yu X. A narrative review of gut-muscle axis and sarcopenia: the potential role of gut microbiota. Int J Gen Med. 2021;14:1263–1273. doi:10.2147/IJGM.S301141
5. Karim A, Muhammad T, Shahid iqbal M, et al. A multistrain probiotic improves handgrip strength and functional capacity in patients with COPD: a randomized controlled trial. Arch Gerontol Geriatr. 2022;102:104721. doi:10.1016/j.archger.2022.104721
6. Kirschner SK, Deutz NEP, Jonker R, et al. Intestinal function is impaired in patients with chronic obstructive pulmonary disease. Clin Nutr. 2021;40(4):2270–2277. doi:10.1016/j.clnu.2020.10.010
7. Qaisar R, Karim A, Muhammad T, et al. Butyrate supplementation reduces sarcopenia by repairing neuromuscular junction in patients with chronic obstructive pulmonary disease. Respir Med. 2024;222:107510. doi:10.1016/j.rmed.2023.107510
8. Mete B, Pehlivan E, Gülbaş G, et al. Prevalence of malnutrition in COPD and its relationship with the parameters related to disease severity. Int J Chron Obstruct Pulmon Dis. 2018;13:3307–3312. doi:10.2147/COPD.S179609
9. Cesanelli L, Cesanelli F, Degens H, et al. Obesity-related reduced spirometry and altered breathing pattern are associated with mechanical disadvantage of the diaphragm. Respir Physiol Neurobiol. 2024;325:104267. doi:10.1016/j.resp.2024.104267
10. Wu JF, Jia J, Chen P, et al. Sarcopenia and its clinical correlation in elderly chronic obstructive pulmonary disease: a prospective cohort study. Eur Rev Med Pharmacol Sci. 2023;27(20):9762–9772. doi:10.26355/eurrev_202310_34150
11. Karim A, Iqbal MS, Muhammad T, et al. Elevated plasma zonulin and CAF22 are correlated with sarcopenia and functional dependency at various stages of Alzheimer’s diseases. Neurosci Res. 2022;184:47–53. doi:10.1016/j.neures.2022.08.004
12. Ahmad F, Karim A, Khan J, et al. Plasma zonulin correlates with cardiac dysfunction and poor physical performance in patients with chronic heart failure. Life Sci. 2022;311(Pt A):121150. doi:10.1016/j.lfs.2022.121150
13. Weldam SW, Schuurmans MJ, Liu R, et al. Evaluation of Quality of Life instruments for use in COPD care and research: a systematic review. Int J Nurs Stud. 2013;50(5):688–707. doi:10.1016/j.ijnurstu.2012.07.017
14. Beaudart C, Demonceau C, Reginster J-Y, et al. Sarcopenia and health-related quality of life: a systematic review and meta-analysis. J Cachexia, Sarcopenia Muscle. 2023;14(3):1228–1243. doi:10.1002/jcsm.13243
15. Wang DXM, Yao J, Zirek Y, et al. Muscle mass, strength, and physical performance predicting activities of daily living: a meta-analysis. J Cachexia, Sarcopenia Muscle. 2020;11(1):3–25. doi:10.1002/jcsm.12502
16. Beaudart C, Biver E, Reginster J-Y, et al. Development of a self-administrated quality of life questionnaire for sarcopenia in elderly subjects: the SarQoL. Age Ageing. 2015;44(6):960–966. doi:10.1093/ageing/afv133
17. Konstantynowicz J, Abramowicz P, Glinkowski W, et al. Polish Validation of the SarQoL((R)), a quality of life questionnaire specific to sarcopenia. J Clin Med. 2018;7(10):323. doi:10.3390/jcm7100323
18. Beaudart C, Locquet M, Reginster J-Y, et al. Quality of life in sarcopenia measured with the SarQoL(R): impact of the use of different diagnosis definitions. Aging Clin Exp Res. 2018;30(4):307–313. doi:10.1007/s40520-017-0866-9
19. Erdogan T, Eris S, Avci S, et al. Sarcopenia quality-of-life questionnaire (SarQoL)(R): translation, cross-cultural adaptation and validation in Turkish. Aging Clin Exp Res. 2021;33(11):2979–2988. doi:10.1007/s40520-020-01780-0
20. Qaisar R, Hussain S, Karim A, et al. A leaky gut contributes to postural imbalance in male patients with chronic obstructive pulmonary disease. Clin Nutr ESPEN. 2024;62:157–163. doi:10.1016/j.clnesp.2024.05.018
21. Kim AY, Lee JK, Kim SH, et al. Is postural dysfunction related to sarcopenia? A population-based study. PLoS One. 2020;15(5):e0232135. doi:10.1371/journal.pone.0232135
22. Qaisar R, Karim A, Muhammad T, et al. Degradation of neuromuscular junction contributes to muscle weakness but not physical compromise in chronic obstructive pulmonary disease patients taking lipids-lowering medications. Respir Med. 2023;215:107298. doi:10.1016/j.rmed.2023.107298
23. Karim A, Muhammad T, Ustrana S, et al. Intestinal permeability marker zonulin as a predictor of sarcopenia in chronic obstructive pulmonary disease. Respir Med. 2021;189:106662. doi:10.1016/j.rmed.2021.106662
24. Karim A, Muhammad T, Qaisar R. Prediction of sarcopenia using multiple biomarkers of neuromuscular junction degeneration in chronic obstructive pulmonary disease. J Pers Med. 2021;11(9):919. doi:10.3390/jpm11090919
25. World Medical A. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194.
26. Beaudart C, Edwards M, Moss C, et al. English translation and validation of the SarQoL(R), a quality of life questionnaire specific for sarcopenia. Age Ageing. 2017;46(2):271–276. doi:10.1093/ageing/afw192
27. Qaisar R, Iqbal MS, Karim A, et al. A leaky gut contributes to reduced sarcopenia-related quality of life (SarQoL) in geriatric older adults. Qual Life Res. 2023;33(2):551–559. doi:10.1007/s11136-023-03547-2
28. Guillamon-Escudero C, Diago-Galmés A, Zuazua Rico D, et al. SarQoL questionnaire in community-dwelling older adults under ewgsop2 sarcopenia diagnosis algorithm: a new screening method? Int J Environ Res Public Health. 2022;19(14):8473. doi:10.3390/ijerph19148473
29. Qaisar R, Karim A, Muhammad T. Circulating biomarkers of handgrip strength and lung function in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:311–321. doi:10.2147/COPD.S225765
30. Karim A, Muhammad T, Shah I, et al. A multistrain probiotic reduces sarcopenia by modulating Wnt signaling biomarkers in patients with chronic heart failure. J Cardiol. 2022;80(5):449–455. doi:10.1016/j.jjcc.2022.06.006
31. Ahmad F, Karim A, Khan J, et al. Plasma Galectin-3 and H-FABP correlate with poor physical performance in patients with congestive heart failure. Exp Biol Med. 2023;15353702231151980.
32. Karim A, Iqbal MS, Muhammad T, et al. Evaluation of sarcopenia using biomarkers of the neuromuscular junction in Parkinson’s disease. J Mol Neurosci. 2022;72(4):820–829. doi:10.1007/s12031-022-01970-7
33. Gupta A, Jayakumar MN, Saleh MA, et al. SARS-CoV-2 infection- induced growth factors play differential roles in COVID-19 pathogenesis. Life Sci. 2022;304:120703. doi:10.1016/j.lfs.2022.120703
34. Karim A, Muhammad T, Iqbal MS, et al. Elevated plasma CAF22 are incompletely restored six months after COVID-19 infection in older men. Exp Gerontol. 2023;171:112034. doi:10.1016/j.exger.2022.112034
35. Bindels LB, Neyrinck AM, Loumaye A, et al. Increased gut permeability in cancer cachexia: mechanisms and clinical relevance. Oncotarget. 2018;9(26):18224–18238. doi:10.18632/oncotarget.24804
36. Cammisuli DM, Fusi J, Scarfò G, et al. A minireview exploring the interplay of the muscle-gut-brain (MGB) axis to improve knowledge on mental disorders: implications for clinical neuroscience research and therapeutics. Oxid Med Cell Longev. 2022;2022(1):8806009. doi:10.1155/2022/8806009
37. Leech B, McIntyre E, Steel A, et al. the subjective well-being and health-related quality of life of Australian adults with increased intestinal permeability and associations with treatment interventions. J Altern Complement Med. 2021;27(12):1136–1146. doi:10.1089/acm.2021.0202
38. Geerinck A, Dawson-Hughes B, Beaudart C, et al. Assessment of the performance of the SarQoL((R)) questionnaire in screening for sarcopenia in older people. Aging Clin Exp Res. 2021;33(8):2149–2155. doi:10.1007/s40520-021-01913-z
39. Delfinis LJ, Bellissimo CA, Gandhi S, et al. Muscle weakness precedes atrophy during cancer cachexia and is linked to muscle-specific mitochondrial stress. JCI Insight. 2022;7(24). doi:10.1172/jci.insight.155147
40. Karim A, Muhammad T, Shah I, et al. Relationship of haptoglobin phenotypes with sarcopaenia in patients with congestive heart failure. Heart Lung Circ. 2022;31(6):822–831. doi:10.1016/j.hlc.2022.01.003
41. Qaisar R, Karim A, Elmoselhi AB. Muscle unloading: a comparison between spaceflight and ground-based models. Acta Physiol. 2020;228(3):e13431. doi:10.1111/apha.13431
42. Stehle JR, Leng X, Kitzman DW, et al. Lipopolysaccharide-binding protein, a surrogate marker of microbial translocation, is associated with physical function in healthy older adults. J Gerontol a Biol Sci Med Sci. 2012;67(11):1212–1218. doi:10.1093/gerona/gls178
43. Alamdari N, Toraldo G, Aversa Z, et al. Loss of muscle strength during sepsis is in part regulated by glucocorticoids and is associated with reduced muscle fiber stiffness. Am J Physiol Regul Integr Comp Physiol. 2012;303(10):R1090–9. doi:10.1152/ajpregu.00636.2011
44. Bhaskaran S, Pollock N, C. Macpherson P, et al. Neuron-specific deletion of CuZnSOD leads to an advanced sarcopenic phenotype in older mice. Aging Cell. 2020;19(10):e13225. doi:10.1111/acel.13225
45. Qaisar R, Bhaskaran S, Premkumar P, et al. Oxidative stress-induced dysregulation of excitation-contraction coupling contributes to muscle weakness. J Cachexia, Sarcopenia Muscle. 2018;9(5):1003–1017. doi:10.1002/jcsm.12339
46. Lee SY, Ahn S, Kim YJ, et al. Comparison between dual-energy X-ray absorptiometry and bioelectrical impedance analyses for accuracy in measuring whole body muscle mass and appendicular skeletal muscle mass. Nutrients. 2018;10(6):738.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Translation, Cultural Adaptation, and Validation of the Cantonese Version of SarQoL in Hong Kong’s Older Population: An Interviewer-Administered Questionnaire for Assessing Sarcopenia-Specific Quality of Life in Fieldwork Practice
Yu R, Lai D, Leung G, Tam LY, Cheng C, Kong S, Tong C, Lu Z, Leung JC, Chan A, Kwok T, Woo J
Clinical Interventions in Aging 2023, 18:1851-1861
Published Date: 9 November 2023
The Pathology of Intestinal Mucosal Disruption; Implications for Muscle Loss and Physical Dependency from Late Adolescence to Octogenarians
Qaisar R, Karim A, Iqbal MS, Muhammad T, Ahmad F, Alkahtani SA
International Journal of General Medicine 2024, 17:6117-6126
Published Date: 12 December 2024