")
Back to Journals » Journal of Pain Research » Volume 18
The Mechanism of Acupuncture Therapy for Migraine: A Systematic Review of Animal Studies on Rats
Authors An Y , Zhang J , Ren Q, Liu J, Liu Z, Cao K
Received 25 November 2024
Accepted for publication 7 January 2025
Published 25 January 2025 Volume 2025:18 Pages 473—487
DOI https://doi.org/10.2147/JPR.S504892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yuqiu An,1,2,* Jing Zhang,1,2,* Qiaosheng Ren,1,2 Jiaojiao Liu,1,2 Zhenhong Liu,1,2,* Kegang Cao1,2,*
1Department of Neurology, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, 100700, People’s Republic of China; 2Institute for Brain Disorders, Beijing University of Chinese Medicine, Beijing, 100700, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kegang Cao; Zhenhong Liu, Email [email protected]; [email protected]
Background: Acupuncture has long been used for migraine treatment as it is convenient for use and has remarkable efficacy. The acupuncture-based comprehensive treatment plan has been widely recognized for migraine prevention and treatment. However, the mechanism underlying acupuncture efficacy in migraine treatment is not yet completely understood. Our goal is to systematically analyze and evaluate this efficacy mechanism in migraine treatment-related basic research.
Methods: To retrieve animal experiments investigating the action mechanism of acupuncture in migraine treatment, We conducted a literature search in major databases, the search period was the inception of each database to April 1, 2024. Literature was screened and data were extracted independently based on predefined inclusion and exclusion criteria. The animal models, acupuncture points, and acupuncture methods specified in the included studies were statistically analyzed and summarized. Furthermore, the potential action mechanisms of acupuncture were discussed.
Results: In total, 20 animal experimental studies were included in the present analysis, and all of these studies used rats. In the order of frequency of use, the migraine animal models employed in the searched studies were the dural stimulation model, the nitroglycerin model, and the cortical spreading depression model. The primary acupuncture points selected were Fengchi (GB20) and Yanglingquan (GB34), and electroacupuncture was the most frequently used acupuncture method. The action mechanism of acupuncture underlying migraine treatment primarily involves regulating the descending pain modulatory system and inhibiting neurotransmitters such as CGRP, SP, and 5-HT, as well as microglial cell activation. It also reduces the levels of inflammatory cytokines, thereby mitigating neurogenic inflammation and improving central sensitization.
Conclusion: Acupuncture exerts its therapeutic effect on migraine by regulating neurotransmitter release, inhibiting inflammatory responses, modulating central analgesic mechanisms, and suppressing glial cell activation. However, further in-depth exploration is needed in the study of the mechanisms underlying acupuncture treatment for migraine.
Keywords: migraine, acupuncture, trigeminal neurovascular system, neurogenic inflammation, neurotransmitter
Introduction
According to the World Health Organization, migraine is the second leading cause of disabling neurological disorders globally.1 It afflicts more than 100 million individuals in China,2 thereby challenging public health and well-being substantially. The onset age for migraine is primarily 25–39 years,3 and the condition is characterized by high incidence and disability rates. Individuals with migraine experience up to 3.7 days of work or productivity loss per week because of disease episodes,4,5 which significantly diminishes their quality of life and causes substantial labor force losses. The global economic burden ascribed to migraine can reach upward of tens of billions of dollars annually. In addition to the direct burden of the disease itself, migraine can cause damage to cognitive and language functions and thus serve as a risk factor for various health problems such as stroke, epilepsy, anxiety, and depression.6 Therefore, migraine prevention and treatment have emerged as among the priority tasks in current medical research. At present, the therapeutic armamentarium for migraine predominantly includes non-steroidal anti-inflammatory drugs, triptans, calcitonin gene-related peptide (CGRP) receptor antagonists, and highly selective 5-hydroxytryptamine (5-HT) 1F receptor agonists such as ditans.7,8 Specific therapeutic agents targeting CGRP and its receptors have yielded promising clinical trial results, thus offering new hope for migraine treatment. Nevertheless, desired therapeutic outcomes have not yet been achieved for a subset of migraine patients in clinical practice.
Being a unique medical practice originating from China, knowledge about the application and benefits of acupuncture has spread to over 140 countries and regions, where it has played a major role in protecting the health and well-being of humanity at large and garnered extensive international recognition. Acupuncture has been proven to be effective against migraine and offers advantages such as rapid onset of action, high safety profile, minimal adverse reactions, and low cost. It is substantially beneficial to migraine patients experiencing inadequate pain relief even after using medications or are unwilling to undergo pharmacological treatment.9 Numerous clinical studies on acupuncture therapy for migraine have been published in prestigious international journals. For instance, regarding sustained pain relief, Ling Zhao reported that acupuncture exerts a lasting effect in terms of migraine prevention and treatment, thereby significantly outperforming sham acupuncture and wait-list control groups in reducing the frequency of attacks, number of attack days, and severity of attacks.10 Shabei Xu also confirmed the positive role of acupuncture in the prophylactic treatment of migraine.11 Furthermore, Ying Li et al discovered that acupuncture is advantageous in the acute management of migraine as it exerts superior analgesic effects when targeting acupoints along the Shaoyang meridian compared with non-meridian and non-acupoint locations.12 As a non-pharmacological therapy, acupuncture has been included in eight guidelines issued by organizations such as the French Headache Society and the Italian Headache Society,8,13 which marks a new direction in migraine treatment. Regarding mechanisms underlying acupuncture’s therapeutic effects on migraine, research has begun to explore this area. These studies have suggested that acupuncture modulates neurotransmitters and inflammatory factors, and alleviates pain sensitization to some extent, thereby improving migraine attacks. Systematic evaluation and evidence-based support are lacking.
This article highlights the urgent application needs in migraine diagnosis and treatment, particularly focusing on the challenge of elucidating complex mechanisms underpinning the substantial therapeutic effects of acupuncture in improving migraine symptoms. By conducting a thorough literature review, we probed into the potential mechanisms underlying acupuncture-induced analgesia. Given the substantial differences between humans and animals in acupoint localization, acupuncture depth, and other factors, direct systematic evaluations are associated with marked heterogeneity challenges. Animal experiments are evidently indispensable in acupuncture research. This research field is constantly expanding in breadth and depth, transcending across diverse animal species. This field comprehensively validates the diverse regulatory effects of acupuncture at multiple levels, spanning from behavioral manifestations and cellular activities to molecular levels, and dives deep into the underlying mechanisms. These studies offer a solid foundation for the scientific rationale of acupuncture therapy and unlock new avenues for optimizing migraine treatment strategies.
In this study, animal experiments were therefore used as the primary research approach, thus utilizing this precise and controllable methodology to more instinctively uncover the intrinsic action mechanisms of acupuncture in migraine treatment. The study findings contribute to improving our scientific understanding of the efficacy of acupuncture therapy. Therefore, This study contributes to further exploring the efficacy mechanism of acupuncture in treating migraine and provides directions for future research in this field.
Methods
This systematic review focused on animal experiments involving acupuncture intervention for migraine. The protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42024496359.
Search Strategy and Study Selection
The article rigorously adheres to the PRISMA statement14 in conducting an electronic literature search across the China National Knowledge Infrastructure (CNKI), Wanfang Data, PubMed, Embase, Cochrane Library, and Web of Science databases. The search was limited to the period from the inception of each database up until April 1, 2024. The search strategy employed a combination of subject headings and free-text terms. All search terms related to acupuncture were grouped using the “OR” function, and, similarly, all search terms associated with migraine were grouped using the “OR” function. Finally, the acupuncture-related and migraine-related search terms were combined using the “AND” function. Example search terms include: “Migraine Disorders”, “Migraine”, “Migraines”, “Migraine Headache”, “electroacupuncture”, “acupuncture”, among others.
Data Extraction
The retrieved research articles were imported into EndnoteX9 software for deduplication. Two independent researchers then conducted back-to-back screening and data extraction of the literature. In cases of disagreement, a third-party adjudicator was consulted for resolution. The literature screening process strictly adhered to the inclusion and exclusion criteria, with cross-checking performed based on a predefined data extraction form. Specific inclusion and exclusion criteria for the literature are detailed in Table 1.
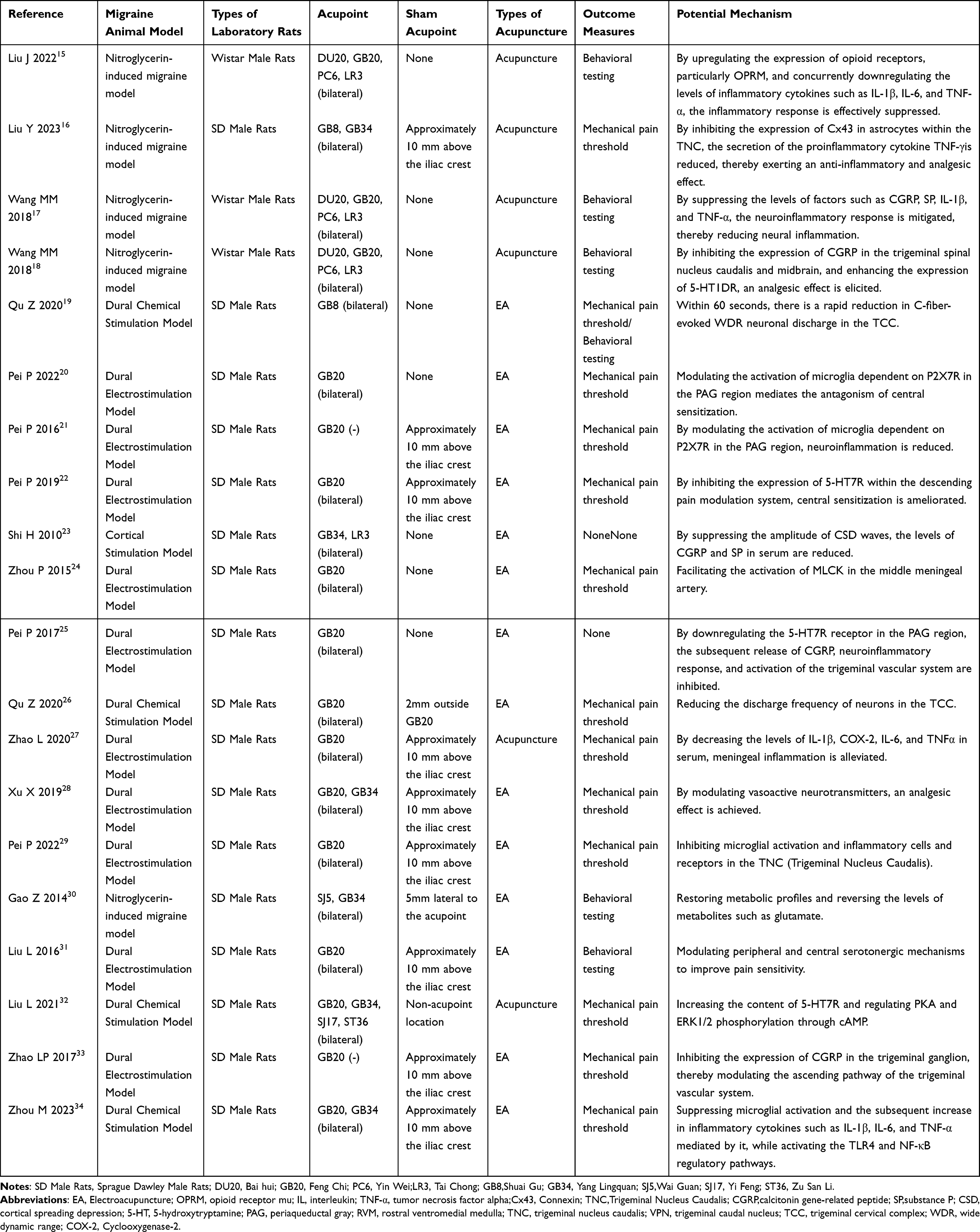 |
Table 1 Basic Characteristics of the Included Literature |
Results
The 2445 articles yielded in the initial search were imported into the NoteExpress software. After duplicates were removed, 633 articles remained. After the titles and abstracts were read, 96 articles were preliminarily selected for conducting full-text assessment. Based on strict inclusion and exclusion criteria, a total of 20 articles were finally included in the further analysis (Figure 1). All 20 articles were based on animal experiments. These experiments were conducted using rats, and the migraine animal models employed were sequentially the dura mater stimulation model (14/20), nitroglycerin model (5/20), and cortical spreading depression (CSD) model (1/20). The acupuncture points prominently used were Fengchi (GB20) and Yanglingquan (GB34), and electroacupuncture (EA) was the most frequently selected acupuncture method. The underlying action mechanisms can be categorized as follows: cortical spreading depression theory, trigeminovascular theory, and neurogenic inflammation theory.
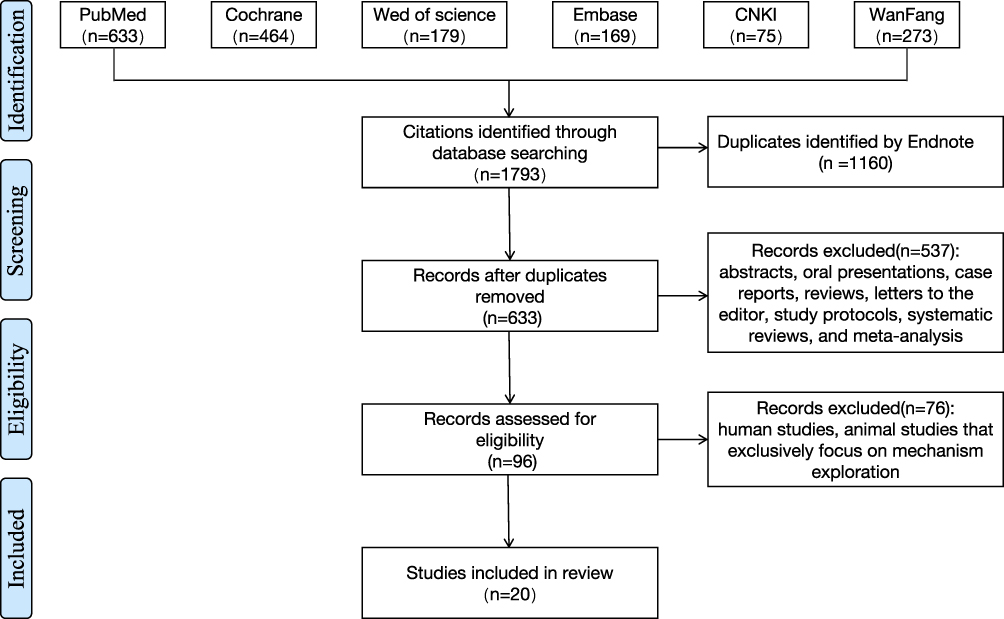 |
Figure 1 Flowchart of the systematic review. |
Animal Model of Migraine
Dural Irritation Model
The dural irritation model was most commonly used in the aforementioned experiments. This model is based on the trigeminovascular theory, which posits that, upon stimulation, migraine-associated pain signals are primarily transmitted from nociceptors located within intracranial and extracranial pain-sensitive tissues to the trigeminal nerve, and are ultimately conveyed to the cortex, thus triggering pain perception. The dura mater serves as the main pain-sensitive tissue within the intracranial space. In this space, numerous nerve endings from the ophthalmic branch of the trigeminal ganglion (TRG)are densely distributed around blood vessels. During a migraine attack, blood vessels expand into the dura mater, thus inducing inflammatory mediators and mechanical stress, which directly activate nociceptors and communicate pain signals to the TRG.35 Consequently, electrical or chemical stimulation methods can be used to directly irritate the dura mater, thereby causing inflammation and inducing migraine attacks.36 Among these methods, electrical stimulation is currently the most regularly used dural irritation model in acupuncture research.27 In this technique, the superior sagittal sinus region of the dura mater is electrically stimulated to evoke migraine-like responses. On the other hand, chemical stimulation involves injecting an inflammatory soup,19 which typically comprises bradykinin, 5-HT (serotonin), histamine, and prostaglandin E2. When this soup is administered as continuous stimulation, it can induce a chronic migraine model.37 The dura mater stimulation model offers the advantage of relatively low requirements regarding experimental equipment, and the rats used as a model exhibited notable behavioral changes while they were in a conscious state. However, the key drawbacks of this model lie in the complex surgical techniques required, which necessitate a high operational skill level. This can effortlessly lead to dura mater damage, leading to a relatively low success rate of modeling. Additionally, because of the shallow implantation of electrodes, they may fall off due to the animals’ grooming behaviors and daily activities. Furthermore, a risk of indirect activation of other non-nociceptive brain regions exists.
Nitroglycerin-Induced Migraine Model
The nitroglycerin model is a well-known animal model of migraine and is principally based on the vascular theory. Current studies have confirmed that NO, produced by nitroglycerin, directly activates the second messenger cyclic guanosine monophosphate and then leads to intracranial and extracranial vasodilation by controlling downstream signaling pathways. This process activates nociceptive neurons, thereby triggering migraine attacks.38 This model is usually established using intraperitoneal injections of nitroglycerin, although subcutaneous and intravenous injections can also be used for modeling.39 The nitroglycerin model is simple to establish, has a low cost, and has minimal requirements for experimental techniques and conditions. Furthermore, it demonstrates a high degree of similarity to human migraine symptoms, with stable pathological states and wide applicability, which renders this model among the most commonly used migraine models. However, nitroglycerin does not specifically target intracranial and extracranial vessels but rather affects the entire vascular system. This may result in symptoms and pathological changes not necessarily related to migraine.
Cortical Spreading Depression Model
The CSD model is an animal model based on the CSD theory. Three commonly used methods for establishing this model: electrical stimulation,40 chemical stimulation,41 and mechanical stimulation.42 This model can effectively mimic the pathogenesis of migraine aura symptoms, particularly cortical electrophysiological activities, with high stability and reproducibility, and is associated with relatively low modeling costs. However, its key limitations lie in the fact that animals are under anesthesia, which precludes the detection or observation of behavioral changes and the simulation of the pain processing mechanisms in migraine. Moreover, the model imposes high requirements on recording equipment.
Acupuncture Acupoints
Acupuncture was mainly applied to the Fengchi (GB20) and Yanglingquan (GB34) acupoints in the aforementioned experiments. According to traditional Chinese medicine theory, the principles of “where the meridian passes, its therapeutic effects reach” and “where the acupoint is located, its therapeutic effects are manifested” direct the practice of acupuncture therapy for migraine, principally focusing on the selection of distal and local acupoints. Acupoints from the Foot Shaoyang Gallbladder Meridian and the Foot Jueyin Liver Meridian are commonly selected for acupuncture treatment. Taichong (LR3) and Yanglingquan (GB34) are the most frequently used distal acupoints. Locally, Fengchi (GB20), Shuaigu (GB8), and Baihui (DU20) are predominantly targeted. In 2020, the China Association of Acupuncture-Moxibustion released the documentation “Names and Locations of Commonly Used Acupoints in Experimental Animals - Part 2: Rats”,43 which offers standardization for acupoint location in rats for acupuncture experiments. For instance, Taichong (LR3) is located in the depression between the first and second metatarsal bones on the hindlimb dorsum, and Yanglingquan (GB34) is located on the lateral side of the lower leg, that is, in the depression anterior and inferior to the fibular head, approximately 3-mm superior and lateral to Zusanli (ST36). The reasons for selecting the aforementioned acupoints are as follows: First, GB20 and GB34 are regularly employed in clinical practice for migraine treatment and have produced definitive therapeutic effects. Acupuncture at these acupoints can inhibit CGRP, 5-HT, and c-fos expression by modulating the endogenous analgesic system, thereby suppressing pain signal transmission.44 Second, GB20 shares similarities with its anatomical location and point-selection method in humans, which leads to a relatively high degree of extrapolatability for experimental results. Furthermore, acupuncturing acupoints located on the lower limbs and head of experimental rats facilitate their immobilization and the execution of acupuncture procedures.
Sham acupoints, which are usually non-acupoints and non-meridian locations, are selected as experimental controls. For instance, a location approximately 10 mm above the iliac crest may serve as a control for GB20. The neuroanatomical basis for the relative specificity of acupoints has been verified.45 However, acupoint sensitization may potentially influence the therapeutic effects of acupuncture, which needs to be explored further.
Acupuncture Method
In the aforementioned experiments, EA was frequently used as the key acupuncture method, with a current intensity of 0.5–1mA, primarily utilizing a sparse-dense wave pattern, often with frequencies of 2Hz/15Hz. As science and technology have advanced, EA has been widely used in both clinical and basic acupuncture research. On one hand, EA improves the stimulatory effects of conventional acupuncture, thereby allowing the intensity, frequency, and duration of stimulation at the acupuncture site to be precisely controlled, thus ensuring the consistency and standardization of experimental conditions. On the other hand, because of the effect of electrical current, EA differs from conventional acupuncture in its stimulatory signal pathway. Notably, some of the aforementioned studies have not described the specific parameters of the acupuncture method. As acupuncture techniques are being standardized, a unified set of parameters for conventional acupuncture and EA will be established for experimental research, which would enhance the comparability and reproducibility of future studies.
The Role of Acupuncture in Migraine
Cortical Spreading Depression
CSD refers to the stimulation-induced electrical inhibition zone generated in the cerebral cortex, which then spreads extensively throughout that area, thus causing neurons and glial cells to be transiently depolarized. This process triggers imbalances in ion channels and disruptions in neurotransmitter regulation and serves as the basis for migraine aura symptoms and neurological dysfunctions. Furthermore, several studies have demonstrated that CSD can activate the trigeminal-vascular system,46 thus inducing the release of neurotransmitters and vasoactive substances such as nitric oxide, CGRP, and substance P (SP), which participate in migraine attack onset. Shi H et al23 locally applied KCl to the cortex to induce CSD, thereby establishing a migraine rat model. Subsequently, they used EA to bilateral Yanglingquan (GB34) and Taichong (LR3) acupoints for 30 min and observed changes in the CSD amplitude and plasma CGRP and SP levels before and after EA. According to the results, EA significantly reduced the CSD amplitude, inhibited the duration and propagation speed of the wave amplitude, and concurrently decreased the plasma CGRP and SP levels. These findings hold major implications for elucidating the relationship between the time-effect and action mechanism of acupuncture in migraine treatment (Figure 2).
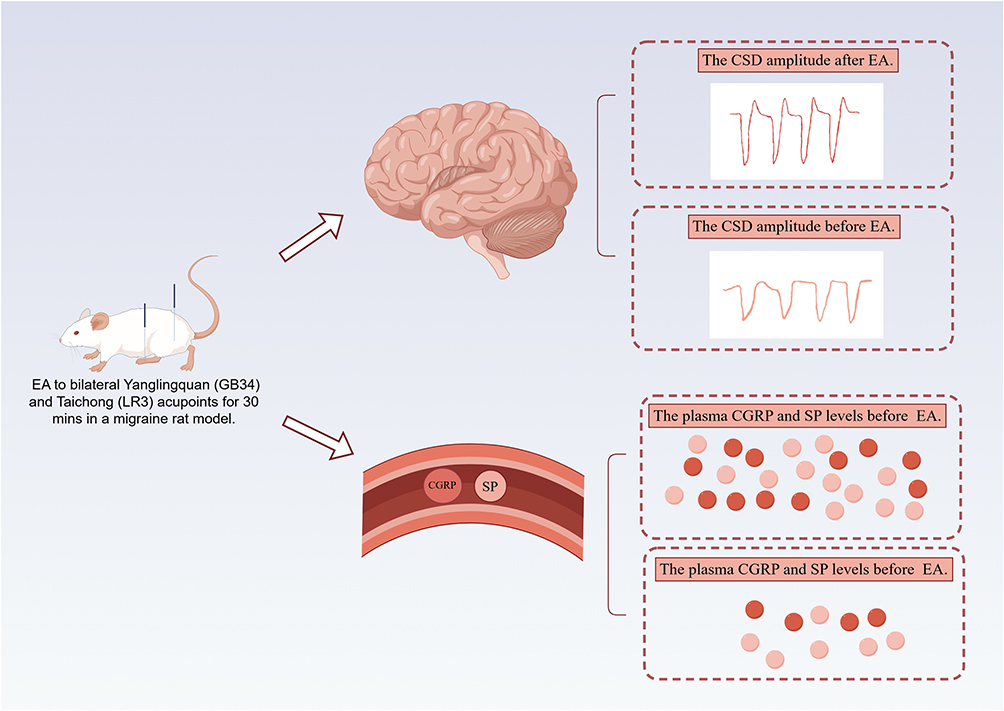 |
Figure 2 The mechanism of acupuncture through modulating cortical spreading depression. By Figdraw. Abbreviations: EA, electroacupuncture therapy; CSD, cortical spreading depression; CGRP, calcitonin gene-related peptide; SP, substance P. Notes: EA significantly reduced the CSD amplitude while also lowering the levels of CGRP and SP in the plasma. |
Trigeminal-Vascular System
When the TRG and its fibers are stimulated, vasoactive neuropeptides such as CGRP and SP are released. These neuropeptides, through a series of cascade reactions, promote vasodilatation, increase vascular permeability, and cause plasma protein extravasation, thereby leading to sterile inflammation. This, in turn, activates nociceptive receptors distributed around the dura mater and meningeal vessels. Pain signals are then transmitted to the central nervous system via trigeminal nociceptive afferent fibers, thus inducing migraine attacks (Figure 3).47
 |
Figure 3 The mechanism of acupuncture in treating migraine. By Figdraw. Abbreviations: PAG, periaqueductal gray; RVM, rostral ventromedial medulla; TNC, trigeminal nucleus caudalis; VPN, trigeminal caudal nucleus; TCC, trigeminal cervical complex; WDR, wide dynamic range. Notes: Acupuncture can inhibit the activation of microglia and astrocytes, as well as central inflammatory responses, and regulate central sensitization to exert an analgesic effect. |
Primary Sensory Fibers
Noxious stimulus-induced pain signals are transmitted by the fiber terminals of primary sensory neurons. They then synapse in the dorsal horn of the spinal cord. The signals later ascend through the anterolateral fasciculus of the spinal cord to reach the brainstem and thalamus, finally projecting to the cerebral cortex where the pain sensation is perceived. The unmyelinated C-fibers and thinly myelinated Aδ-fibers act as primary sensory neuronal fibers, which are involved in trigeminal nociceptive transmission. Serving as second-order neurons located in the dorsal horn of the spinal cord, wide dynamic range (WDR) neurons receive input from these primary sensory fibers and are crucial players in pain initiation and maintenance. Qu Z et al19 found that EA at Lǜgǔ (GB20) rapidly reduces the unmyelinated C-fiber-induced discharge of WDR neurons in the trigeminal cervical complex (TCC) within 60s, thereby activating the diffuse noxious inhibitory control system to exert an analgesic effect. When the same research team conducted electrophysiological experiments on TCC cells in vitro, they found that EA reduces neuronal discharge in the TCC region, elevates the mechanical pain threshold in the trigeminal periorbital area, and reverses abnormal cutaneous pain responses. The underlying mechanism may involve a reduction in the abnormal activation of thinly myelinated Aδ-fibers, a decrease in WDR neuron reactivity, and an improvement in pain sensitization.26
Vasoactive Neuropeptides
SP, vasoactive intestinal polypeptide (VIP), CGRP, and pituitary adenylate cyclase-activating polypeptide (PACAP) are currently identified vasoactive neuropeptides that exert potent vasodilatory effects, thus representing a major research direction in mechanisms underlying migraine. By establishing a migraine rat model through repeated electrical stimulation of the dura mater, Xu X et al28 conducted multi-acupoint electroacupuncture experiments. They found that EA reduces plasma CGRP, SP, VIP, and PACAP concentrations, thereby improving hyperalgesia and neurogenic inflammation.
Being the most prevalent and potent vasodilatory neuropeptide, CGRP has a pivotal role in migraine pathophysiology. It is predominantly distributed within the peripheral nervous system, including TRG, dorsal root ganglia, and nerve fibers innervating meningeal vessels. Furthermore, the presence of CGRP in the central nervous system has been documented, specifically in the TCC, hypothalamus, and PAG.48 Zhao LP et al reported that EA significantly reduces CGRP levels in the TRG, trigeminal caudate nucleus, and ventro posteromedial nucleus of the thalamus in a migraine rat model.33 The mechanism underlying this effect may be related to the activation of the MAPK signaling pathway. Similarly, Pei P and Wang MM also confirmed that acupuncture can decrease the CGRP content in the peripheral blood of rat models of migraine.17,18,23,25
Neurotransmitter
The brainstem descending inhibitory/dissociative system originates from the periaqueductal gray (PAG), which contains various neurotransmitters such as serotonin (5-HT), gamma-aminobutyric acid (γ-GABA), enkephalins, and substance P. Activation of neuronal activity within the ventrolateral region of the PAG sends descending projections to the rostral ventromedial medulla (RVM) and further projects to the caudal trigeminal nucleus (TNC). This pathway inhibits/facilitates the transmission of nociceptive information from the periphery and participates in the regulation of various types of pain, including migraine (Figure 3).
5-Hydroxytryptamine
5-HT, a neurotransmitter widely distributed throughout the nervous system, has vasoconstrictive properties. Notably, 5-HT levels in central and peripheral systems exhibit distinct patterns during the migraine pathophysiological process. During migraine attacks, 5-HT distribution in the central nervous system decreases, whereas its release in the periphery increases. EA alleviates pain by elevating 5-HT concentrations in the rostral ventromedial medulla (RVM) and trigeminal nucleus caudalis (TNC) regions.31 5-HT exerts inhibitory or facilitatory effects on pain modulation by binding to different receptors. For instance, 5-HT binding to 5-HT1B/1D receptors has an analgesic effect, whereas 5-HT binding to 5-HT2B or 5-HT7 receptors located in meningeal vascular endothelial cells facilitates pain transmission. Wang MM et al observed that acupuncture can increase 5-HT1DR expression in the spinal TNC and midbrain, thereby activating 5-HT to alleviate migraine attacks.18 Furthermore, studies have shown that when 5-HT acts on the 5-HT1DR receptor, it can reduce the levels of calcitonin gene-related peptide (CGRP) in the trigeminal ganglion and trigeminal spinal tract nucleus, thereby decreasing the incidence of migraine attacks. Based on the established finding that acupuncture improves central sensitization through descending pain pathways, Pei P et al further uncovered that acupuncture inhibits 5-HT7R expression in the PAG, rostral medulla, and TNC in rat models of migraine.22,25 Liu L et al found that EA significantly reduced 5-HT7R expression in the TNC and suggested that the ERK1/2 and PKA phosphorylation signaling pathways are the mechanisms responsible for this effect.32
Endogenous Opioid Peptides
Opioid receptors(OPRM), G-protein-coupled receptor family members, bind to agonists and activate GTP-binding proteins, thereby regulating downstream target molecules. This process involves the activation of K+ influx, inhibition of voltage-gated Ca2+ channels, mediation of extracellular signal transmission, induction of membrane potential hyperpolarization, and blockade of neural impulse transmission, which ultimately results in an analgesic effect. However, opioids are highly addictive, and their unreasonable use can cause medication-overuse headaches. Therefore, they are unsuitable as first-line therapeutic agents for migraine. Being a safe alternative therapy, acupuncture may potentiate the effects of opioids. By upregulating OPRM expression and downregulating the levels of inflammatory cytokines such as interleukin (IL)-1β, IL-6, and tumor necrosis factor (TNF)-α, acupuncture inhibits inflammatory responses and thus exerts an analgesic effect.15
Neurogenic Inflammation
Glial Cell
Glial cells participate in migraine pathogenesis by inducing neurogenic inflammation and oxidative stress (Figure 4).49 Microglia, the primary immune cells of the central nervous system, transform into a macrophage-like structure after activation and release inflammatory factors to eliminate pathogens and necrotic cells. However, excessive microglial activation can affect neuronal activity by releasing neurotransmitters and inflammatory mediators. The microglia–neuron interaction contributes to pain sensitization, thus playing a role in the occurrence of migraine.50 Microglial activation involves several pathways, including the adenosinergic signaling pathway, Toll-like receptor signaling pathway, and chemokine-chemokine receptor interactions.51 To construct a migraine rat model, Pei P et al repeatedly electrically stimulated the dura mater of rats.29 They observed that microglia in the TNC were abnormally activated, along with upregulated Iba1, IL-1β, and TNF-αexpression. EA at GB20 inhibited microglial activation and inflammatory factor release, decreased mechanical pain thresholds, and alleviated central sensitization. These effects were validated using the microglia inhibitor minocycline. The research team further revealed that EA can inhibit microglial activation in the PAG region. Further investigation into EA mechanisms unveiled that migraine can upregulate P2X7R expression in microglia, thereby participating in the regulation of inflammatory responses. EA acts as an antagonist, blocking P2X7R signaling and elevating pain thresholds in migraine rat models.20 Additionally, Zhou M et al reported that EA can reduce proinflammatory factors.34 They also found that it can inhibit microglial activation and the mediated inflammatory response through the TLR-4 receptor and its downstream inflammatory signaling pathway within the TLR family, thereby applying an analgesic effect.
 |
Figure 4 The mechanism of acupuncture in treating migraine through modulating neurovascular inflammation. ByFIgdraw. Abbreviations: PAG, periaqueductal gray; TNC, trigeminal nucleus caudalis; IL, interleukin; TNF, tumor necrosis factor; CSD, cortical spreading depression. Notes: Acupuncture can inhibit the activation of microglia and astrocytes, as well as central inflammatory responses, and regulate central sensitization to exert an analgesic effect. |
Astrocytes participate in processes such as blood-brain barrier regulation and neurotransmitter and ion metabolism, thereby aiding in sustaining neuronal function and the stability of the central nervous system.52 Abnormal astrocyte activation contributes to migraine pathogenesis and progression through mechanisms such as gap junction communication, synaptic glutamate, transporter proteins, and CSD. Connexins (Cx), the primary structural component of gap junctions, facilitate the interconnection between astrocytes, with Cx43 being the predominant isoform of connexins.Cx43 promotes the release of proinflammatory factors, including IL-1β, IL-6, and TNF-α, from activated astrocytes. These cytokines act on neurons, which leads to central sensitization. Liu Y et al observed that acupuncture inhibits Cx43 activation in astrocytes within the TNC region, thereby reducing the release of proinflammatory factors and exerting an analgesic effect.16
Inflammatory Cytokines
Inflammatory factors are various cytokines involved in the inflammatory process. Of them, TNF and IL are pivotal players in migraine pathophysiological processes. TNF-α, produced by macrophages, stimulates the release of prostaglandins and their compounds. Meanwhile, IL serves as a pain mediator in neurogenic inflammation, thus contributing to thermal and pain hypersensitivity. Both TNF-α and IL activate neutrophils and participate in the cascade of inflammatory responses in migraine. Serum TNF-α, IL-1β, and IL-6 levels were significantly elevated in the migraine rat models.17,27 EA, on the other hand, reduces the release of inflammatory factors and inhibits pain sensitization transmission. Moreover, EA reduces plasma COX-2 levels, thus elucidating the common link among inflammatory factors, COX-2, and CGRP in migraine pathogenesis. This offers a theoretical basis for further exploration of the mechanisms underlying migraine and the development of specific therapeutic agents.
Inflammatory Pathway
Nuclear transcription factor-κB (NF-κB) is a crucial fast-response transcription factor that mediates intracellular signal transduction. It is involved in inflammation, immunity, and pain responses.53 NF-κB is pivotal for the neurogenic inflammatory process of migraine. Pain stimuli activate the I-κB kinase complex, which results in IKB protein phosphorylation. This enables the nuclear translocation of NF-κB (P50/P65), and in the nucleus, it binds to inflammatory factor-associated gene loci. Subsequently, this cascade increases vascular permeability, allows for plasma albumin extravasation, promotes tissue edema, and improves pain sensitivity, collectively contributing to neurogenic inflammation.54
Omics Mechanisms
Multi-omics research integrates biological information across multiple levels, including proteomics, genomics, transcriptomics, and metabolomics, to drive the exploration of migraine pathogenesis and biomarkers, as well as the innovation of personalized drug therapies. For instance, a large-scale genome-wide association study identified differentially expressed genes enriched in both vascular and central nervous tissues, thus supporting the role of neurovascular theory.55 This finding offers a novel perspective for exploring the pathophysiological mechanisms underlying migraine. Omics research also has a pivotal role in migraine treatment, elucidating the action mechanisms of various drugs and aiding the development of precision-based therapeutic strategies.56 However, omics research on acupuncture therapy for migraine remains in its infancy. Differences have been noted in amino acid and lipid metabolism between migraine patients and healthy subjects. Gao Z et al applied EA therapy at both acupoints and non-acupoints in a nitroglycerin-induced migraine rat model.30 According to them, EA reduces plasma glutamate levels, whereas acupoint-specific EA restores the plasma metabolome, reverses changes in glutamate and lipids, and reduces cortical neuronal hyperexcitability and central sensitization, thus exerting an analgesic effect.
Conclusions and Future Perspectives
Internationally recognized high-quality clinical evidence has been gathered for acupuncture in the realm of pain relief. Thus, it emerges as an effective alternative approach in addressing the so-called “New Opioid War. “Migraine, as the most prevalent craniofacial pain disorder, is associated with the dire situation of inappropriate and excessive utilization of acute analgesic medications. By activating descending pain inhibitory pathways and modulating neurotransmitter levels, acupuncture therapy exerts its analgesic effects throughout the entire process of migraine occurrence and conduction. The analgesic mechanisms of acupuncture in mitigating migraine at both peripheral and central levels majorly include inhibition of abnormal activation of afferent nerves, modulation of ion channel expression, and alleviation of peripheral sensitization It also includes regulating the release of vasoactive neuropeptides and neurotransmitters, inhibiting glial cell activation, reducing the expression of inflammatory factors and pathways, and thus mitigating central sensitization.
As studies explore more about mechanisms underlying the therapeutic effects of acupuncture on migraine, current investigations primarily focus on neuroinflammation and neurovascular aspects. The current research mechanisms still possess certain limitations. For instance, in the CSD model, the rats are anesthetized, which prevents the detection or observation of behavioral changes and the simulation of pain processing mechanisms associated with migraine.However, additional studies are warranted to determine whether the intricate interplay among various inflammatory mediators, neurotransmitters, and cellular signaling molecules remains consistent. Moreover, with advancements in medical imaging technology, functional magnetic resonance imaging has emerged as pivotal for unraveling the neural mechanisms underlying the therapeutic effects of acupuncture on migraine. In future animal experiments, the mechanisms of acupuncture’s actions at the cerebral level must be determined, specifically on various brain functional regions and their associated neurotransmitters. In conclusion, modern neurobiological technologies must be used to study the intricate network mechanisms of acupuncture in migraine treatment from multiple layers, targets, and dimensions.
Abbreviations
PAG, Periaqueductal Gray; CGRP, Calcitonin Gene-Related Peptide; 5-HT, 5-Hydroxytryptamine; CSD, Cortical Spreading Depression; EA, Electroacupuncture; TRG, Trigeminal Ganglion; SP, Substance P; WDR, Wide Dynamic Range; TCC, Trigeminal Cervical Complex; VIP, Vasoactive Intestinal Polypeptide; PACAP, Pituitary Adenylate Cyclase-Activating Polypeptide; RVM, Rostral Ventromedial Medulla; TNC, Trigeminal Nucleus Caudalis; OPRM, Opioid Receptors; IL, Interleukin; TNF, Tumor Necrosis Factor; NF-κB, Nuclear transcription Factor-κB.
Acknowledgments
Yuqiu An and Jing Zhang are co-first authors for this study. We are grateful to figdraw for their excellent plotting software, which greatly facilitated our data visualization process.
Author Contributions
All authors have made substantial contributions to this work, spanning from its conception and study design to its execution, data acquisition, analysis, and interpretation. They have actively participated in drafting, revising, and critically reviewing the article, ensuring its accuracy and completeness. Furthermore, each author has given their final approval for the version to be published and has concurred on the journal’s selection for submission. They collectively accept accountability for all facets of this research endeavor.
Funding
China Capital Health Development Research Special Project (2024-2-4193).
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
2. Burch RC, Buse DC, Lipton RB. Migraine: epidemiology, burden, and comorbidity. Neurol Clin. 2019;37(4):631–649. doi:10.1016/j.ncl.2019.06.001
3. Ashina M. Migraine. N Engl J Med. 2020;383(19):1866–1876. doi:10.1056/NEJMra1915327
4. Liu R, Yu S, He M, et al. Health-care utilization for primary headache disorders in China: a population-based door-to-door survey. J Headache Pain. 2013;14(1):47. doi:10.1186/1129-2377-14-47
5. Takeshima T, Wan Q, Zhang Y, et al. Prevalence, burden, and clinical management of migraine in China, Japan, and South Korea: a comprehensive review of the literature. J Headache Pain. 2019;20(1):111. doi:10.1186/s10194-019-1062-4
6. Stovner LJ, Nichols E, Steiner TJ, GBD 2016 headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3
7. Marmura MJ, Silberstein SD, Schwedt TJ. The acute treatment of migraine in adults: the American headache society evidence assessment of migraine pharmacotherapies. Headache. 2015;55(1):3–20. PMID: 25600718. doi:10.1111/head.12499
8. Demarquay G, Mawet J, Guégan-Massardier E, et al. Revised guidelines of the French headache society for the diagnosis and management of migraine in adults. Part 3: non-pharmacological treatment. Rev Neurol. 2021;177(7):753–759. PMID: 34340809. doi:10.1016/j.neurol.2021.07.009
9. Li RR, Li XY, Li XH, et al. Clinical research progress and reflection on acupuncture treatment for migraine in recent 10 years. Zhejiang J Trad Chin Med. 2018;53(6):464–466.
10. Zhao L, Chen J, Li Y, et al. The Long-term Effect of Acupuncture for Migraine Prophylaxis: a Randomized Clinical Trial. JAMA Intern Med. 2017;177(4):508–515. PMID: 28241154. doi:10.1001/jamainternmed.2016.9378
11. Xu S, Yu L, Luo X, et al. Manual acupuncture versus sham acupuncture and usual care for prophylaxis of episodic migraine without aura: multicentre, randomised clinical trial. BMJ. 2020;368:m697. PMID: 32213509; PMCID: PMC7249245. doi:10.1136/bmj.m697
12. Li Y, Zheng H, Witt CM, et al. Acupuncture for migraine prophylaxis: a randomized controlled trial. CMAJ. 2012;184(4):401–410. PMID: 22231691; PMCID: PMC3291669. doi:10.1503/cmaj.110551
13. Sarchielli P, Granella F, Prudenzano MP, et al. Italian guidelines for primary headaches: 2012 revised version. J Headache Pain. 2012;13(Suppl 2):S31–70. PMID: 22581120; PMCID: PMC3350623. doi:10.1007/s10194-012-0437-6
14. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. doi:10.1136/bmj.b2700
15. Liu J, Wang MM, Yang DH, et al. [Mechanisms of liver-soothing and mind-regulating acupuncture mediating opioid receptor participated in the treatment of migraine]. Zhen Ci Yan Jiu. 2022;47(6):510–516. doi:10.13702/j.1000-0607.20210691
16. Liu Y, Zhou MD, Zheng YQ, et al. [Acupuncture relieves pain by inhibiting expression of Cx43 in astrocytes and release of interfe-ron-γ in neurons of trigeminal spinal nucleus in rats with migraine]. Zhen Ci Yan Jiu. 2023;48(2):118–124. doi:10.13702/j.1000-0607.20220967
17. Wang MM, Yu XH, Geng W, et al. [Effect of Manual Acupuncture Preconditioning on Behavior and Contents of Serum CGRP, SP, IL-1 β and TNF-α Levels in Migraine Rats]. Zhen Ci Yan Jiu. 2018;43(6):375–379. doi:10.13702/j.1000-0607.170415
18. Wang MM, Yu XH, Geng W, et al. [Manual Acupuncture Stimulation Regulates Expression of Receptor Activity-modifying Protein 1 and 5-HT 1 D Receptor Proteins and Genes in Migraine Rats]. Zhen Ci Yan Jiu. 2018;43(7):440–444. doi:10.13702/j.1000-0607.170346
19. Qu Z, Liu L, Yang Y, et al. Electro-acupuncture inhibits C-fiber-evoked WDR neuronal activity of the trigeminocervical complex: neurophysiological hypothesis of a complementary therapy for acute migraine modeled rats. Brain Res. 2020;1730:146670. doi:10.1016/j.brainres.2020.146670
20. Pei P, Chen HZ, Cui SW, et al. [Effects of electroacupuncture on ethology, microglia activation and P2X7 receptor expression in periaqueductal gray in rats with migraine]. Zhen Ci Yan Jiu. 2022;47(12):1054–1059. doi:10.13702/j.1000-0607.20211059
21. Pei P, Liu L, Zhao L, Cui Y, Qu Z, Wang L Effect of electroacupuncture pretreatment at GB20 on behaviour and the descending pain modulatory system in a rat model of migraine. Acupunct Med. 2016;34(2):127–135. doi:10.1136/acupmed-2015-010840
22. Pei P, Liu L, Zhao LP, et al. Electroacupuncture exerts an anti-migraine effect via modulation of the 5-HT7 receptor in the conscious rat. Acupunct Med. 2019;37(1):47–54. doi:10.1136/acupmed-2017-011410
23. Shi H, Li JH, Ji CF, et al. [Effect of electroacupuncture on cortical spreading depression and plasma CGRP and substance P contents in migraine rats]. Zhen Ci Yan Jiu. 2010;35(1):17–21.
24. Zhou P, Wang A, Li B, Liu C, Wang Y Effect of acupuncture at Fengchi (GB 20) on the activity of myosin light chain kinase in the middle meningeal artery of migraine modeled rats. J Tradit Chin Med. 2015;35(3):301–305. doi:10.1016/s0254-6272(15)30101-1
25. Pei P, Chen HZ, Wang YX, Yang WM, Liu L, Wang LP. [Effect of Electroacupuncture on Expression of 5-HT7 Receptor in Periaqueductal Gray and Plasma Calcitonin Gene-related Peptide in Migraine Rats]. Zhen Ci Yan Jiu. 2017;42(6):510–513. doi:10.13702/j.1000-0607.2017.06.008
26. Qu Z, Liu L, Zhao L, et al. Prophylactic electroacupuncture on the upper cervical segments decreases neuronal discharges of the trigeminocervical complex in migraine-affected rats: an in vivo extracellular electrophysiological experiment. J Pain Res. 2020;13:25–37. doi:10.2147/JPR.S226922
27. Zhao L, Liu L, Xu X, et al. Electroacupuncture inhibits hyperalgesia by alleviating inflammatory factors in a rat model of migraine. J Pain Res. 2020;13:75–86. doi:10.2147/JPR.S225431
28. Xu X, Liu L, Zhao L, et al. Effect of electroacupuncture on hyperalgesia and vasoactive neurotransmitters in a rat model of conscious recurrent migraine [published correction appears in Evid Based Complement Alternat Med. 2019 Jul 14;2019:8181245]. Evid Based Complement Alternat Med. 2019;2019:9512875. doi:10.1155/2019/9512875
29. Pei P, Cui S, Zhang S, Hu S, Wang L, Yang W. Effect of electroacupuncture at Fengchi on facial allodynia, microglial activation, and microglia-neuron interaction in a rat model of migraine. Brain Sci. 2022;12(8):1100. doi:10.3390/brainsci12081100
30. Gao Z, Liu X, Yu S, et al. Electroacupuncture at acupoints reverses plasma glutamate, lipid, and LDL/VLDL in an acute migraine rat model: a (1) H NMR-based metabolomic study. Evid Based Complement Alternat Med. 2014;2014:659268. doi:10.1155/2014/659268
31. Liu L, Pei P, Zhao LP, Qu ZY, Zhu YP, Wang LP. Electroacupuncture pretreatment at GB20 exerts antinociceptive effects via peripheral and central serotonin mechanism in conscious migraine rats. Evid Based Complement Alternat Med. 2016;2016:1846296. doi:10.1155/2016/1846296
32. Liu L, Xu XB, Qu ZY, et al. Determining 5HT7R’s involvement in modifying the antihyperalgesic effects of electroacupuncture on rats with recurrent migraine. Front Neurosci. 2021;15:668616. doi:10.3389/fnins.2021.668616
33. Zhao LP, Liu L, Pei P, Qu ZY, Zhu YP, Wang LP. Electroacupuncture at Fengchi (GB20) inhibits calcitonin gene-related peptide expression in the trigeminovascular system of a rat model of migraine. Neural Regen Res. 2017;12(5):804–811. doi:10.4103/1673-5374.206652
34. Zhou M, Pang F, Liao D, He X, Yang Y, Tang C. Electroacupuncture at Fengchi(GB20) and Yanglingquan(GB34) ameliorates Paralgesia through microglia-mediated neuroinflammation in a rat model of migraine. Brain Sci. 2023;13(4):541. doi:10.3390/brainsci13040541
35. Dyhring T, Jansen-Olesen I, Christophersen P, et al. Pharmacological profiling of KATP channel modulators: an outlook for new treatment opportunities for migraine. Pharmaceuticals. 2023;16(2):225. doi:10.3390/ph16020225
36. Melo-Carrillo A, Lopez-Avila A. A chronic animal model of migraine, induced by repeated meningeal nociception, characterized by a behavioral and pharmacological approach. Cephalalgia. 2013;33(13):1096–1105. doi:10.1177/0333102413486320
37. Miao S, Tang W, Li H, et al. Repeated inflammatory dural stimulation-induced cephalic allodynia causes alteration of gut microbial composition in rats. J Headache Pain. 2022;23(1):71. doi:10.1186/s10194-022-01441-9
38. Yu T, Yufang S, Yuan Z, et al. Research progress on animal models of migraine. Chin J Pain Med. 2023;29(10):766–773.
39. Casili G, Lanza M, Filippone A, et al. Dimethyl fumarate alleviates the nitroglycerin(NTG)-induced migraine in mice. J Neuroinflammation. 2020;17(1):59. doi:10.1186/s12974-020-01736-1
40. Andreou AP, Holland PR, Akerman S, et al. Transcranial magnetic stimulation and potential cortical and trigeminothalamic mechanisms in migraine. Brain. 2016;139(Pt 7):2002–2014. doi:10.1093/brain/aww118
41. Kurauchi Y, Haruta M, Tanaka R, et al. Propranolol prevents cerebral blood flow changes and pain-related behaviors in migraine model mice. Biochem Biophys Res Commun. 2019;508(2):445–450. doi:10.1016/j.bbrc.2018.11.173
42. Zhang X, Levy D, Kainz V, et al. Activation of central trigeminovascular neurons by cortical spreading depression. Ann Neurol. 2011;69(5):855–865. doi:10.1002/ana.22329
43. China Association of Acupuncture-Moxibustion, Common acupoint names and localization in experimental animals part 2: rats. Acupuncture Research. 2021;46(04):351–352.
44. Yu M, Zhou QW, Xu YH, et al. Effect of acupuncture on the endogenous analgesic system in CSD migraine rats. Guangxi J Trad Chin Med. 2018;41(02):62–65.
45. Liu S, Wang Z, Su Y, et al. A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis. Nature. 2021;598(7882):641–645. PMID: 34646018; PMCID: PMC9178665. doi:10.1038/s41586-021-04001-4
46. Kissoon NR, Cutrer FM. Aura and other neurologic dysfunction in or with migraine. Headache. 2017;57(7):1179–1194. doi:10.1111/head.13101
47. Moskowitz MA, Reinhard JF, Romero J, Melamed E, Pettibone DJ. Neurotransmitters and the fifth cranial nerve: is there a relation to the headache phase of migraine? Lancet. 1979;2(8148):883–885. doi:10.1016/s0140-6736(79)92692-8
48. Ashina H, Schytz HW, Ashina M. CGRP in human models of migraine. Handb Exp Pharmacol. 2019;255:109–120. doi:10.1007/164_2018_128
49. Amani H, Soltani Khaboushan A, Terwindt GM, Tafakhori A. Glia signaling and brain microenvironment in migraine. Mol Neurobiol. 2023;60(7):3911–3934. doi:10.1007/s12035-023-03300-3
50. Tozaki-Saitoh H, Tsuda M. Microglia-neuron interactions in the models of neuropathic pain. Biochem Pharmacol. 2019;169:113614. doi:10.1016/j.bcp.2019.08.016
51. Zhou YJ, Hu LY, Yang L, et al. Research progress on the role of microglia in primary headache. Chin J Clin Neurosci. 2022;30(06):656–660.
52. Chaboub LS, Deneen B. Astrocyte form and function in the developing central nervous system. Semin Pediatr Neurol. 2013;20(4):230–235. doi:10.1016/j.spen.2013.10.003
53. Ben-Neriah Y, Karin M. Inflammation meets cancer, with NF-κB as the matchmaker. Nat Immunol. 2011;12(8):715–723. doi:10.1038/ni.2060
54. Bowie A, O’Neill LAJ. The interleukin-1 receptor/Toll-like receptor superfamily: signal generators for pro-inflammatory interleukins and microbial products. J Leukoc Biol. 2002;67(4):508–514. doi:10.1089/152581600319513
55. Hautakangas H, Winsvold BS, Ruotsalainen SE, et al. Genome-wide analysis of 102,084 migraine cases identifies 123 risk loci and subtype-specific risk alleles. Nat Genet. 2022;54:152–160. doi:10.1038/s41588-021-00990-0
56. Ni N, Wang Q, Lin X, et al. Studies on the mechanism of glutamate metabolism in ntg-induced migraine rats treated with DCXF. Evid Based Complement Alternat Med. 2019;2019:1324797. doi:10.1155/2019/1324797
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.