")
Back to Journals » Journal of Pain Research » Volume 18
The Mediating Role of Depression in the Relationship Between Perceived Injustice and Pain Intensity Among Fibromyalgia Patients
Authors Raev S, Aloush V, Gilam G , Elkana O
Received 19 January 2025
Accepted for publication 9 May 2025
Published 19 June 2025 Volume 2025:18 Pages 3077—3085
DOI https://doi.org/10.2147/JPR.S518357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Sheer Raev,1 Valerie Aloush,2,3 Gadi Gilam,4 Odelia Elkana1
1Behavioral Sciences, Academic College of Tel Aviv-Yaffo, Tel Aviv, Israel; 2Institute of Rheumatology and Internal Medicine, Tel Aviv Sourasky Medical Center, Tel Aviv-Yaffo, Israel; 3A Gray School of Medicine, Tel Aviv University, Tel Aviv, Israel; 4The Institute of Biomedical and Oral Research, Faculty of Dental Medicine, Hebrew University of Jerusalem, Jerusalem, Israel
Correspondence: Odelia Elkana, The Academic College of Tel Aviv-Yafo (MTA), P.O.B 8401, Tel-Aviv-Jaffa, 61083, Israel, Tel +972-3 6802525, Fax +97236802526, Email [email protected], [email protected] Gadi Gilam, Institute of Biomedical and Oral Research, Faculty of Dental Medicine, Hebrew University of Jerusalem, Jerusalem, 91120, Israel, Tel +972-54 5335986, Fax +97226757078, Email [email protected]
Background: Fibromyalgia (FM) patients often perceive heightened levels of injustice, which can be associated with depressive symptoms. Despite this connection, the mediating role of depression between perceived injustice and pain intensity in FM patients remains unexplored.
Aim: This study explored whether depression mediates the relationship between perceived injustice and pain intensity in FM.
Methods: Data were collected through an online survey distributed to FM patients at the Tel Aviv Sourasky Medical Center, Israel. A total of 161 FM patients completed the survey, with perceived injustice assessed using the Injustice Experience Questionnaire, depression evaluated using the Patient Health Questionnaire, and pain intensity measured with the numerical Pain Intensity Rating Scale. Statistical analyses included analysis of variance and bootstrap-based mediation models.
Results: FM patients reported elevated levels of pain, perceived injustice, and depression. The study found that depression significantly mediated the association between perceived injustice and pain intensity in FM patients (P < 0.001, CI = 0.024, 0.312).
Conclusion: The link between perceived injustice and pain intensity in FM is partially explained by the level of depression. Individuals with higher perceived injustice scores are more susceptible to depression, subsequently experiencing increased pain. These findings suggest that intervention programs targeting depression may mitigate the impact of perceived injustice on pain intensity in FM, potentially enhancing health-related quality of life.
Plain Language Summary: This study explores the connection between feelings of unfairness, depression, and pain levels in people with fibromyalgia, a chronic condition that causes widespread pain and emotional distress. Fibromyalgia patients often report experiencing a sense of injustice, such as feeling misunderstood or treated unfairly, which can worsen their mental and physical health.
We aimed to investigate whether depression plays a role in linking perceived injustice to the intensity of pain experienced by these patients. To do this, we surveyed 161 individuals with fibromyalgia using online questionnaires. Participants rated their feelings of injustice, symptoms of depression, and pain intensity. Statistical methods were used to analyze how these factors interact.
Our findings showed that people who felt a higher sense of injustice were more likely to experience symptoms of depression. This depression, in turn, contributed to higher levels of pain. In other words, depression served as a bridge connecting feelings of injustice to increased pain intensity.
These results highlight the importance of addressing depression in fibromyalgia treatment. By helping patients manage depressive symptoms, healthcare providers may reduce the impact of perceived injustice on pain, potentially improving patients’ quality of life. This study emphasizes the need for psychological interventions to complement traditional pain management strategies for fibromyalgia patients.
By understanding how mental health influences physical pain, this research supports a more comprehensive approach to care for people living with fibromyalgia.
Keywords: fibromyalgia, perceived injustice, depression, pain intensity, psychological distress, injustice experience questionnaire
Introduction
Fibromyalgia Syndrome (FM) is a centralized pain condition affecting up to 5% of the global population and is more prevalent in women than in men.1,2 FM is characterized by widespread musculoskeletal pain, sleep disturbances, fatigue, notable cognitive impairment symptoms, and a high incidence of functional disability.2,3 Despite extensive research, the precise cause and pathophysiology of FM remain elusive. However, abnormal central pain processing is identified as one of the primary mechanisms, manifested as heightened responses to experimental stimuli (sensitization), increased neuronal activity in pain-processing brain regions, and alterations in pain-related neurotransmitter levels.4–7 FM patients often suffer from fatigue, emotional distress, and maladaptive coping strategies.8–12
FM is associated with increased negative affect, including distress and aversive emotions such as sadness, fear, anger, and guilt. Individuals with FM also frequently report elevated stress levels, heightened anger, and pain catastrophizing tendencies.13
Depression and anxiety are among the most prevalent psychiatric comorbidities, significantly impacting patients’ quality of life.11,14 Compared to the general population, individuals with FM demonstrate higher rates of a broad range of mental health conditions, including generalized anxiety disorder, panic attacks, phobias, obsessive-compulsive disorder, post-traumatic stress disorder, major depressive disorder, dysthymia, and bipolar disorder.13,15–20
Depression is the most prevalent comorbidity associated with FM, with a lifetime prevalence estimated at 63%.14 Most research has predominantly turned to “diathesis-stress” models to elucidate how depressive symptoms may emerge following the onset of a pain condition. These models propose that psychological factors interact with the stress induced by pain to increase the likelihood of experiencing depressive symptoms.21 Any element amplifying the perceived threat or the weight of associated losses from pain could potentially act as a diathesis for symptoms of depression.22
One of the challenges in managing FM is the absence of clinically valid tests for diagnosis and assessment.23 Moreover, the ongoing debate in the medical community about the nature of FM complicates patients’ understanding and management of their illness and associated pain. Research suggests that FM patients encounter greater difficulty in comprehending and articulating their pain compared to individuals with other chronic pain conditions like Rheumatoid Arthritis (RA).10 The International Association for the Study of Pain (IASP) defines pain as “An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage”.24 Indeed, the experience of pain is a complex result of interactions between physiological and psychological factors,25 the latter reflecting cognitive, emotional, and social components.26 An individual’s beliefs and the meaning they attribute to pain, especially chronic pain, are recognized as key modulators of their pain experience.25,27–29
Recent evidence highlights the significant role of perceived injustice (PI) in shaping pain experiences and related psychological outcomes in individuals with fibromyalgia. PI is a multifaceted psychological construct involving appraisals of unfairness, blame, and the severity and irreparability of pain-related loss.21,29,30 In FM, these perceptions may be intensified by the lack of clear diagnostic biomarkers, frequent misdiagnosis, and skepticism from healthcare providers, which can contribute to patients feeling invalidated or dismissed.10,31,32 Elevated levels of PI have been associated with increased pain intensity, pain behaviors, functional disability, and poorer psychological adjustment. Importantly, PI has also been linked to greater levels of depression and emotional distress, suggesting that it may not only exacerbate physical symptoms but also worsen mental health outcomes. Understanding the role of PI in FM is therefore crucial, as it may offer novel targets for intervention, especially in cases where standard pharmacological treatments are insufficient. By analyzing PI within a mediational framework, this study aims to shed light on the psychological mechanisms through which feelings of injustice may amplify suffering in FM patients.
FM patients have been observed to report higher levels of PI compared to those with other chronic pain conditions like RA, possibly due to the lack of clear pathophysiological explanations and biomarkers for FM, which may heighten feelings of injustice.10,33
The relationship between PI, depression, and pain intensity in FM is complex. While it is plausible that PI could directly influence pain intensity, we hypothesize that depression may serve as a critical mediator in this relationship. Depression is known to alter cognitive processes, leading to an increased focus on negative thoughts and cognitive distortions, which could amplify the perception of pain.21,34 Moreover, depression may enhance sensitivity to feelings of injustice by heightening perceptions of loss and unfairness.35 In this context, depression could represent a key pathway through which PI impacts pain intensity, making it a logical mediator in our model.
The objective of the current study was to examine whether PI is associated with pain intensity in individuals with fibromyalgia, and whether depression mediates this relationship. By investigating depression as a mediator, we aim to elucidate the pathways through which psychological factors, particularly PI, influence pain experiences in FM. Identifying depression as a mediating factor could provide valuable insights into intervention targets and inform more comprehensive approaches to pain management in this population.
Methods
Procedure
The study was conducted in accordance with the Declaration of Helsinki, and all procedures were approved by the Tel Aviv-Yaffo Institutional Ethics Committee (2021037) and the Tel Aviv Sourasky Medical Center Institutional Review Board (reference number 0494-21-TLV) for clinical patients. The research department of the Sourasky Medical Center contacted patients from the Rheumatology Department via Email or text message, inviting them to participate in the study and providing a link to the online questionnaire. Upon clicking the link, participants were first asked to review and sign an electronic informed consent form. They were then directed to complete a set of self-report questionnaires, including demographic information. Participation was voluntary, and participants could stop the survey at any point.Data collection took place between April 2021 and January 2022 via the Qualtrics online survey platform.
Participants
Data was collected from patients diagnosed with FM in the Rheumatology Department at the Tel Aviv Sourasky Medical Center, Israel. A total of 203 FM patients volunteered to participate, of whom 42 (20.69%) did not complete the survey. A total of 161 FM patients completed the survey (48.17, SD ± 13.05 years; 138 female [85.2%]). Inclusion criteria were: age above 18 years, confirmed diagnosis of FM, native Hebrew speakers, and currently living in Israel. Exclusion criteria included a comorbid diagnosis of both FM and rheumatoid arthritis (RA), which led to the exclusion of 46 individuals. All patients were treated at the Sourasky Medical Center between 2015–2021.
Measures
Primary Measures
Perceived Injustice
The Injustice Experience Questionnaire (IEQ) was used to measure pain-related perceptions of injustice.29 The IEQ was developed based on two theoretical factors, labeled “severity/irreparability of loss” and “blame/unfairness”, though statistically, it comprises one single scale of 12 items. Participants rate the frequency with which they experienced each of these items on a 5-point scale, ranging from 0 (never) to 4 (all the time). Examples of items from the first factor include: “Most people do not understand how severe my condition is” and “My life will never be the same”. Examples of items related to the latter factor include: “I am suffering because of someone else’s negligence” and “It all seems so unfair”. All scores are summed to obtain a global score ranging from 0 to 48. The Hebrew version of the Injustice Experience Questionnaire (IEQ), which we translated and validated,36 was used in the current study to assess perceived injustice among the participants. In the current sample, internal consistency was α=0.93.
Pain Intensity
Participants were asked to rate their current level of pain on a single-item Numerical Rating Scale (NRS) ranging from 0 (no pain) to 10 (excruciating pain). Although internal consistency cannot be computed for a single-item measure, the NRS has been shown to have good reliability and validity in assessing pain intensity across various clinical populations.37
Depression
The Patient Health Questionnaire-9 (PHQ-9), a 9-item depression module from the complete PHQ questionnaire,38 was used to assess depression. For each item, patient responses range from 0 (not at all) to 3 (nearly every day). For example, a sample item is “feeling down, depressed, or hopeless”. The questionnaire was translated into Hebrew and validated.39 All scores are summed to obtain a global score ranging from 0 to 27. The Cronbach’s α, as reported by the developers, was 0.89 and 0.86 in the validation studies of the PHQ-9.38 In the current sample, the internal consistency was α=0.88.
Although additional psychological questionnaires were administered to the same sample (ie, GAD-7, STAXI-2, and PCS), these measures were not analyzed in this study and are reported elsewhere (Gilam et al, 2024).
Analysis Strategy
Prior to the main analyses, the data were screened for univariate outliers and assessed for normality. Visual inspections of histograms and Q–Q plots, along with the Shapiro–Wilk test, indicated no substantial deviations from normality for the primary variables (perceived injustice, depression, and pain intensity). Scatterplots were also examined to confirm linear relationships between variables. Given the sample size and the robustness of Pearson’s correlation to minor violations of normality, parametric tests were deemed appropriate. Therefore, Pearson correlation coefficients were used to assess bivariate associations among the main study variables. An alpha level of.05 was used throughout. Based on these correlations, we tested the hypothesis for a mediation model, conducting bootstrapped-based mediation using PROCESS40 macro for SPSS (IBM Corp., Armonk, NY, U.S.A.). We ran the mediation model with IEQ as the predictor, depression as the mediator, and pain intensity as the outcome using IBM SPSS. Bias-corrected 95% confidence intervals were produced using 10,000 bootstrap resamples, and the total and indirect effects were considered significant if zero was not included in the confidence interval. To assess the potential influence of demographic variables, we re-estimated the mediation model using the PROCESS macro (Model 4), controlling for gender and years of education. These covariates were entered into the model alongside the primary variables to evaluate whether they modified the indirect effect of perceived injustice on pain intensity via depression.
Results
The demographic and clinical characteristics of the sample are presented in Table 1. The sample’s mean age was 48.17, SD ± 13.05 years; 85.2% (N=138) were female, and 14.2% (N=23) were male. Nearly half of the sample had 12 years of education (46%, 29.2% 13–16 years of education, 24.8% 17 years and higher). On average, the patients who participated in the study had suffered from FM for 8.22 years (SD: 6.03 years; range 20).
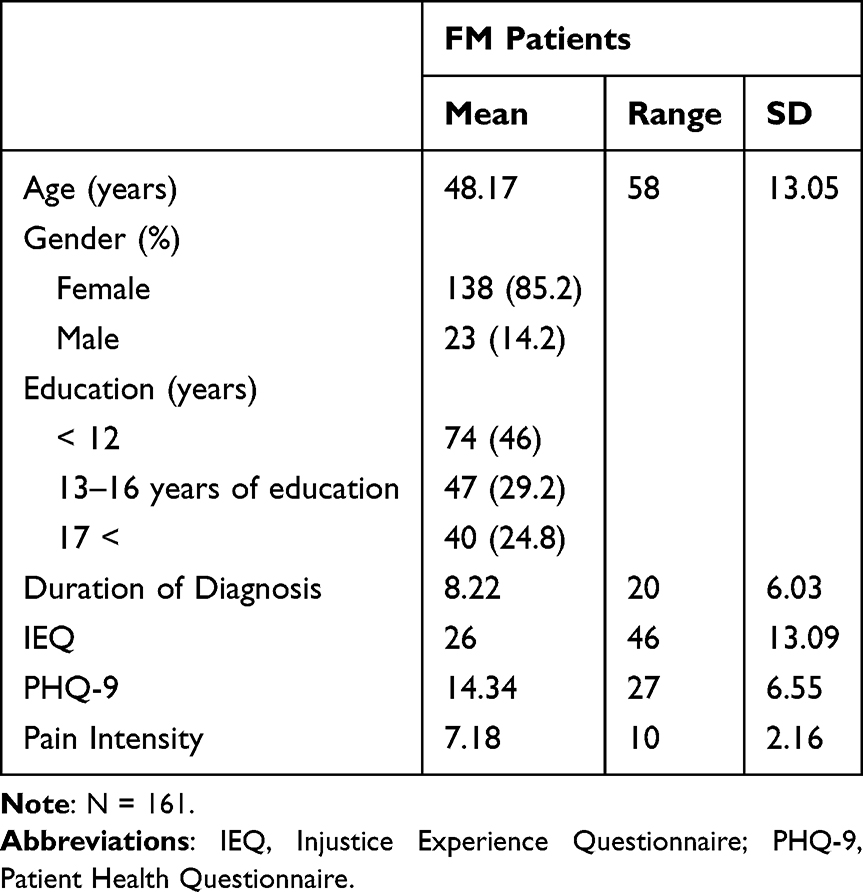 |
Table 1 Sample Characteristics |
The mean total IEQ score was 26 (SD 13.09; range 46). The mean total for depression was 14.34 (SD 6.55; range 27). The mean pain intensity score was 7.18 (SD 2.16; range 10) Table 1.
Mediation Analysis
The bivariate correlation matrix for the variables used in the mediation analysis (ie, PI, depression, and pain intensity) is presented in Table 2 and supports the predicted relationships among these variables Table 2. In line with our hypothesis, we observed significant positive correlations between IEQ, depression, and pain intensity. The IEQ demonstrated moderate-to-strong positive correlations with all related constructs. Next, we conducted a mediation analysis (Figure 1). The results indicate a significant positive association between IEQ and depression (β= 0.70, t(159)= 12.31, p<0.001, R2= 0.49). As well as a positive association between IEQ and pain intensity (β= 0.25, t(158)= 2.53, p<0.001, R2= 0.20). The relationship between depression and pain intensity was positive and significant (β= 0.24, t(158)= 2.31, p<0.05). The 95% confidence interval (CI) for the indirect mediating effect of IEQ on pain intensity through depression was significant and ranged from 0.024 to 0.311 (β=0.17, p<0.05; 10,000 bootstrap resamples). Hence, depression partially mediated the relationship between IEQ and pain intensity Figure 1. To account for potential demographic influences, we re-ran the mediation analysis while controlling for gender and education. The indirect effect of IEQ on pain intensity through depression remained statistically significant (β = 0.16, 95% CI [0.019, 0.298]), confirming that the mediation pathway is robust even when demographic covariates are taken into account.
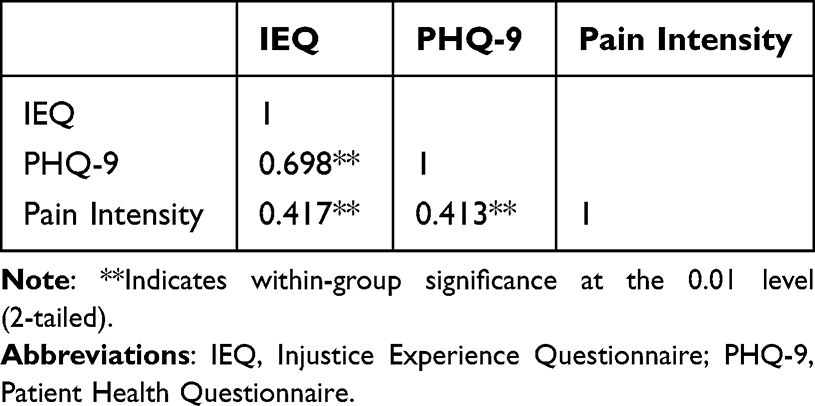 |
Table 2 Correlation Matrix of IEQ and Related Factors |
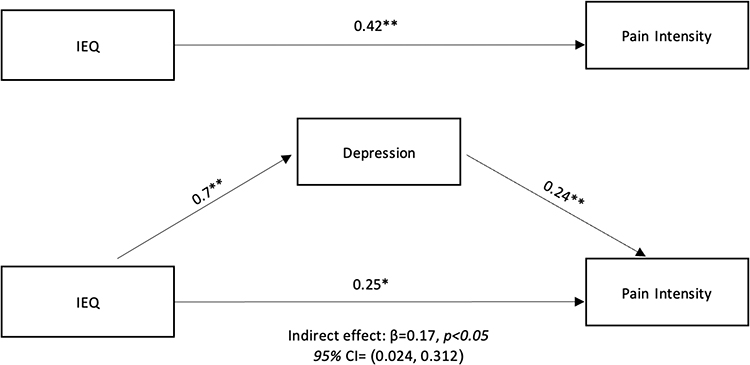 |
Figure 1 Mediation model showing that depression partially mediates the relationship between perceived injustice (IEQ) and pain intensity. All paths were significant ( < 0.05; p < 0.001). Bootstrap sample = 10,000. Abbreviation: IEQ, Injustice Experience Questionnaire. Note: **Indicates significance at p<0.001. |
Discussion
The primary objective of our study was to investigate the intricate relationship among PI, depression, and pain intensity in individuals diagnosed with FM. We specifically examined whether depression acted as a mediator in the well-established link between PI and pain intensity. Our study results align with existing research, consistently revealing significant correlations between PI, depression, and pain intensity.10,14,21,31,34,35 Additionally, we observed a positive correlation between depression and pain intensity.
While our findings are consistent with previous research showing significant correlations among PI, depression, and pain intensity, the present study provides a novel contribution by empirically testing and confirming a mediation model in which depression explains, at least in part, the association between perceived injustice and pain intensity in individuals with fibromyalgia. To our knowledge, this is among the first studies to demonstrate this pathway in a well-characterized clinical FM sample.
Importantly, the direct association observed between perceived injustice and pain intensity in our sample highlights the independent contribution of PI to the pain experience. PI is known to activate cognitive and emotional processes that may heighten the perception of pain. For example, chronic appraisals of unfairness and loss can lead to sustained stress activation, increased pain vigilance, and reduced pain tolerance. In individuals with FM—who often face stigmatization, diagnostic ambiguity, and invalidation—these appraisals may become internalized, contributing to a heightened pain experience even in the absence of overt physiological changes. Furthermore, PI may interfere with the development of adaptive coping strategies, such as acceptance or self-efficacy, and instead promote emotional responses such as resentment, helplessness, and anger, all of which are known to exacerbate pain perception. These processes may help explain why PI correlates directly with pain intensity in our findings, beyond its indirect effect through depression.
Interactions Between Perceived Injustice and Depression
PI may interact with depression in several ways, thus intensifying pain symptoms. The unique impact of PI on depressive symptoms can be attributed to various underlying processes. Efforts to find meaning in situations of injustice have the potential to trigger social comparison mechanisms that negatively affect individuals’ self-esteem. Individuals may interpret their suffering as stemming from their shortcomings, deviations, or feelings of unworthiness compared to those with a well-defined diagnosis or without pain. These unfavorable self-other comparisons may contribute to the development of depressive symptoms.41 Another aspect of PI that influences these symptoms involves thoughts of assigning blame. Studies suggest that attributing blame is likely to trigger feelings of anger,30,42 potentially leading to confrontations with insurance representatives, healthcare providers, or family members. Such confrontational relationships could be linked to elevated stress levels and a decrease in the quality of support, both of which are associated with depressive symptoms.21,43,44
Moreover, the assessment of the severity and irreparability of loss has been identified as a crucial aspect of PI.29 Losses resulting from pain, such as diminished functionality, reduced independence, and financial instability, may predominantly influence PI. Furthermore, loss plays a central role in triggering and sustaining depressive symptoms, as the irreparability of the loss can lead to feelings of hopelessness or helplessness, which are associated with depressive symptoms.21 FM patients experience various losses due to their diagnosis, ranging from physical, psychological, and social functions to a loss of quality of life and self-fulfillment. These losses, combined with the lack of understanding FM patients often encounter, the lack of validation, the methods and mechanisms used to determine outcomes, and the procedures related to the assessment of compensation claims and medical treatment could heighten PI.8,45,46 This, in turn, may lead to heightened depressive symptoms and, consequently, intensified pain levels.
Clinical Implications
PI stands out from other psychological factors due to its diverse range of origins.32 The influence of personal, social, and systemic cognitions on PI makes it one of the most complex risk factors to address in clinical settings.47 While the management and treatment of PI in individuals experiencing persistent musculoskeletal pain, such as FM patients, have not been extensively researched, acceptance-based interventions appear to be a promising approach.48,49 Acceptance and Commitment Therapy (ACT) for chronic pain, for example, helps patients accept their pain and commit to living a meaningful life despite it. ACT has been shown to reduce the impact of pain on daily functioning and improve overall quality of life by encouraging psychological flexibility and reducing pain-related distress.50 Additionally, Emotional Awareness and Expression Therapy (EAET) targets the emotional aspects of chronic pain by helping patients identify and express suppressed emotions that may contribute to their pain.51 EAET has been particularly effective in reducing pain severity and improving emotional well-being in individuals with FM and other chronic pain conditions. These therapies address the cognitive and emotional components of PI, helping patients manage their feelings of loss, unfairness, and helplessness, which may otherwise exacerbate depressive symptoms and pain intensity.
Psychological therapies such as Cognitive Behavioral Therapy (CBT) and interpersonal therapy are also commonly employed to treat major depression and alleviate depressive symptoms in individuals with chronic pain. CBT for major depression involves challenging negative cognitions related to the world (pessimism), the future (hopelessness), and the self (low self-worth). It also focuses on mindfulness and behavior change, including increasing engagement in pleasurable activities.52,53 These approaches have demonstrated effectiveness in reducing depressive symptoms in FM patients.54,55
Given the similarities between the treatment of PI and depression, and the mediating relationship found between PI, depression, and pain severity, further research is needed to determine the effects of treating PI on both depression and pain intensity. The integration of pain-focused psychotherapies like ACT and EAET, alongside traditional therapies like CBT, may provide a more comprehensive approach to managing both psychological distress and pain in FM patients.
Limitations
Several limitations should be considered when interpreting our findings. Our study focused specifically on PI in individuals with FM, and as such, the generalizability of these findings to other chronic pain populations is still being determined. While previous research has suggested that PI may serve as a general risk factor for chronic pain patients, the mediating role of depression warrants consideration in future research involving various chronic pain populations. Additionally, all study variables were assessed using self-report measures instead of a structured clinical interview. Because high scores on self-report measures do not necessarily indicate the presence of a diagnosable depressive disorder, it is not clear whether the relationships observed in the present study would apply to individuals with a clinical diagnosis. Due to the cross-sectional nature of our study, caution should be exercised when concluding the direction of the relationships studied. Although our correlations demonstrated notable strength and consistency, future research employing intervention-based approaches could provide valuable insights into PI, examining its influence on pain intensity. Additionally longitudinal studies should be conducted to provide a more in-depth analysis. Further, the study included FM patients using medical treatment for depression. The use of medication could have an effect of levels of depression reported. Moreover, our sample consisted mostly of females (85.2%). Future studies should aim for the inclusion of a more equal sex distribution.
Beyond these considerations, the study was conducted in a single medical center, which may reduce the ecological validity of the results.
Conclusion
Despite the study’s limitations, our findings offer a novel contribution to the understanding of psychological mechanisms involved in chronic pain, particularly in fibromyalgia. By demonstrating that depression partially mediates the relationship between perceived injustice and pain intensity, this study highlights a potential pathway through which emotional and appraisal-related processes exacerbate the pain experience. These results not only deepen our theoretical understanding of the interplay between injustice appraisals and pain but also underscore the importance of targeting perceived injustice and depression in clinical interventions. Tailoring treatment approaches to address these psychological dimensions may ultimately improve outcomes for individuals living with fibromyalgia.
Data Sharing Statement
Anonymized patient data will be made available upon request to the corresponding authors.
Acknowledgments
We thank all participants and patients for the participation in the study. Sheer Raev and Valerie Aloush Shared first authorship; Gadi Gilam and Odelia Elkana Shared last authorship.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ruschak I, Montesó-Curto P, Rosselló L, Martín CA, Sánchez-Montesó L, Toussaint L. Fibromyalgia syndrome pain in men and women: a scoping review. Healthcare. 2023;11(2):223. doi:10.3390/healthcare11020223
2. Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010;62(5):600–610. doi:10.1002/acr.20140
3. Costa IDS, Gamundí A, Miranda JGV, França LGS, De Santana CN, Montoya P. Altered functional performance in patients with fibromyalgia. Front Hum Neurosci. 2017;11:14. doi:10.3389/fnhum.2017.00014
4. Bair MJ, Krebs EE. Fibromyalgia. Ann Intern Med. 2020;172(5):ITC33–ITC48. doi:10.7326/AITC202003030
5. Crofford LJ, Pillemer SR, Kalogeras KT, et al. Hypothalamic–pituitary–adrenal axis perturbations in patients with fibromyalgia. Arthritis Rheum. 1994;37(11):1583–1592. doi:10.1002/art.1780371105
6. Gür A, Karakoc M, Nas K, Cevik R, Sarac J, Demir E. Efficacy of low power laser therapy in fibromyalgia: a single-blind, placebo-controlled trial. Lasers Med Sci. 2002;17:57–61. doi:10.1007/s10103-002-8267-4
7. Siracusa R, Paola RD, Cuzzocrea S, Impellizzeri D. Fibromyalgia: pathogenesis, mechanisms, diagnosis and treatment options update. Int J Mol Sci. 2021;22(8):3891. doi:10.3390/ijms22083891
8. Bucourt E, Martaill V, Goupille P, et al. A comparative study of fibromyalgia, rheumatoid arthritis, spondyloarthritis, and Sjö gren’s syndrome; impact of the disease on quality of life, psychological adjustment, and use of coping strategies. Pain Med. 2021;22(2):372–381. doi:10.1093/pm/pnz255
9. Everest J. Fibromyalgia and workers’ compensation: controversy, problems, and injustice. Ala L Rev. 2008;60:1031.
10. Ferrari R, Russell AS. Perceived injustice in fibromyalgia and rheumatoid arthritis. Clin Rheumatol. 2014;33:1501–1507. doi:10.1007/s10067-014-2552-z
11. Galvez-Sánchez CM, Reyes DEl Paso GA, Duschek S. Cognitive impairments in fibromyalgia syndrome: associations with positive and negative affect, alexithymia, pain catastrophizing and self-esteem. Front Psychol. 2018;9:377. doi:10.3389/fpsyg.2018.00377
12. Laursen BS, Bajaj P, Olesen AS, Delmar C, Arendt-Nielsen L. Health related quality of life and quantitative pain measurement in females with chronic non-malignant pain. Eur J Pain. 2005;9(3):267–275. doi:10.1016/j.ejpain.2004.07.003
13. Galvez-Sánchez CM, Duschek S, Reyes DEl Paso GA. Psychological impact of fibromyalgia: current perspectives. Psychol Res Behav Manag. 2019;Volume 12:117–127. doi:10.2147/PRBM.S178240
14. Kleykamp BA, Ferguson MC, McNicol E, et al. The prevalence of psychiatric and chronic pain comorbidities in fibromyalgia: an ACTTION systematic review. In: Seminars in Arthritis and Rheumatism. Vol. 51. Elsevier; 2021:166–174.
15. Pando-Fernández MP. Fibromyalgia and psychotherapy. Rev Digit Med Psicosom Psicoter. 2011;1:1–42.
16. Coppens E, Van Wambeke P, Morlion B, et al. Prevalence and impact of childhood adversities and post‐traumatic stress disorder in women with fibromyalgia and chronic widespread pain. Eur J Pain. 2017;21(9):1582–1590. doi:10.1002/ejp.1059
17. Galek A, Erbslöh-Möller B, Köllner V, et al. Mental disorders in patients with fibromyalgia syndrome: screening in centres of different medical specialties. Der Schmerz. 2013;27:296–304. doi:10.1007/s00482-013-1323-0
18. Steiner JL, Bigatti SM, Slaven JE, Ang DC. The complex relationship between pain intensity and physical functioning in fibromyalgia: the mediating role of depression. J Appl Biobehav Res. 2017;22(4):e12079. doi:10.1111/jabr.12079
19. Alciati A, Sarzi-Puttini P, Batticciotto A, et al. Overactive lifestyle in patients with fibromyalgia as a core feature of bipolar spectrum disorder. Clin Exp Rheumatol. 2012;30(6 Suppl 74):122–128.
20. MORRISO11 MCDIT, CARI1CI F, LESSIA1I3 G, SPI1AS E. Fibromyalgia and bipolar disorder: extent of comorbidity and therapeutic implications. J Biol Regul Homeost Agents. 2017;31(1):17–20.
21. Scott W, Sullivan M. Perceived injustice moderates the relationship between pain and depression. J Pain. 2011;12(4):P81. doi:10.1016/j.jpain.2011.02.330
22. Banks SM, Kerns RD. Explaining high rates of depression in chronic pain: a diathesis-stress framework. Psychol Bull. 1996;119(1):95.
23. Elkana O, Falcofsky AK, Shorer R, Bar-On Kalfon T, Ablin JN. Does the cognitive index of the symptom severity scale evaluate cognition? Data from subjective and objective cognitive measures in fibromyalgia. Clin Exp Rheumatol. 2019;37(Suppl 116):S51–7.
24. Rajaa SN, Carrb DB, Cohenc M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Development. 2020;7:19.
25. Arntz A, Claassens L. The meaning of pain influences its experienced intensity. Pain. 2004;109(1–2):20–25. doi:10.1016/J.PAIN.2003.12.030
26. Gilam G, Gross JJ, Wager TD, Keefe FJ, Mackey SC. What is the relationship between pain and emotion? Bridging constructs and communities. Neuron. 2020;107(1):17–21. doi:10.1016/j.neuron.2020.05.024
27. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581. doi:10.1037/0033-2909.133.4.581
28. Moseley GL, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain. 2015;16(9):807–813. doi:10.1016/j.jpain.2015.05.005
29. Sullivan MJL, Adams H, Horan S, Maher D, Boland D, Gross R. The role of perceived injustice in the experience of chronic pain and disability: scale development and validation. J Occup Rehabil. 2008;18:249–261. doi:10.1007/s10926-008-9140-5
30. Carriere JS, Pimentel SD, Yakobov E, Edwards RR. A systematic review of the association between perceived injustice and pain-related outcomes in individuals with musculoskeletal pain. Pain Med. 2020;21(7):1449–1463. doi:10.1093/pm/pnaa088
31. Scott W, Trost Z, Bernier E, Sullivan MJL. Anger differentially mediates the relationship between perceived injustice and chronic pain outcomes. Pain. 2013;154(9):1691–1698. doi:10.1016/j.pain.2013.05.015
32. Sullivan MJL, Yakobov E, Scott W, Tait R. Perceived injustice and adverse recovery outcomes. Psychol Inj Law. 2014;7:325–334. doi:10.1007/s12207-014-9209-8
33. Ferrari R. Quantitative assessment of the “inexplicability” of fibromyalgia patients: a pilot study of the fibromyalgia narrative of “medically unexplained” pain. Clin Rheumatol. 2012;31:1455–1461. doi:10.1007/s10067-012-2029-x
34. Beck AT. The evolution of the cognitive model of depression and its neurobiological correlates. Am J Psychiatry. 2008;165(8):969–977. doi:10.1176/appi.ajp.2008.08050721
35. Lynch J, Fox S, D’Alton P, Gaynor K. A systematic review and meta-analysis of the association between perceived injustice and depression. J Pain. 2021;22(6):643–654. doi:10.1016/j.jpain.2020.12.009
36. Gilam G, Silvert J, Raev S, et al. Perceived injustice and anger in fibromyalgia with and without comorbid mental health conditions: a hebrew validation of the injustice experience questionnaire. Clin J Pain. 2024;40(6):356–366. doi:10.1097/AJP.0000000000001204
37. Safikhani S, Gries KS, Trudeau JJ, et al. Response scale selection in adult pain measures: results from a literature review. J Patient Rep Outcomes. 2018;2(1):1–9. doi:10.1186/s41687-018-0053-6
38. Kroenke K, Bair MJ, Damush TM, et al. Optimized antidepressant therapy and pain self-management in primary care patients with depression and musculoskeletal pain: a randomized controlled trial. JAMA. 2009;301(20):2099–2110. doi:10.1001/jama.2009.723
39. Geulayov G, Jungerman T, Moses S, Friedman N, Miron R, Gross R. Validation of the Hebrew version of the PHQ-9, a screening instrument for depression in primary care. Isr J Psychiatry. 2009;46:45.
40. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford Publications; 2017.
41. Kendler KS, Hettema JM, Butera F, Gardner CO, Prescott CA. Life event dimensions of loss, humiliation, entrapment, and danger in the prediction of onsets of major depression and generalized anxiety. Arch Gen Psychiatry. 2003;60(8):789–796. doi:10.1001/archpsyc.60.8.789
42. Mikula G, Scherer KR, Athenstaedt U. The role of injustice in the elicitation of differential emotional reactions. Pers Soc Psychol Bull. 1998;24(7):769–783. doi:10.1177/0146167298247009
43. Hammen C. Stress and depression. Annu Rev Clin Psychol. 2005;1(1):293–319. doi:10.1146/annurev.clinpsy.1.102803.143938
44. Roose E, Lahousse A, Robbeets A, et al. The prevalence of perceived injustice and factors associated with perceived injustice in people with pain: a systematic review with meta-analysis. Pain Physician. 2023;26(2):E1. doi:10.36076/ppj.2023.26.E1
45. McParland JL, Eccleston C, Osborn M, Hezseltine L. It’s not fair: an interpretative phenomenological analysis of discourses of justice and fairness in chronic pain. Health. 2011;15(5):459–474.
46. DeGood DE, Kiernan B. Perception of fault in patients with chronic pain. Pain. 1996;64(1):153–159. doi:10.1016/0304-3959(95)00090-9
47. Sullivan MJL. Introduction to the special issue on justice-related appraisals and recovery outcomes. Psychol Inj Law. 2016;9(1):1–5. doi:10.1007/s12207-016-9250-x
48. Hayes SC, Strosahl KD, Wilson KG. Acceptance and Commitment Therapy. Vol. 6. New York: Guilford Press; 1999.
49. Sullivan MJL, Scott W, Trost Z. Perceived injustice: a risk factor for problematic pain outcomes. Clin J Pain. 2012;28(6):484–488. doi:10.1097/AJP.0b013e3182527d13
50. McCracken LM, Vowles KE. Acceptance and commitment therapy and mindfulness for chronic pain: model, process, and progress. Am Psychologist. 2014;69(2):178. doi:10.1037/a0035623
51. Lumley MA, Schubiner H, Lockhart NA, et al. Emotional awareness and expression therapy, cognitive behavioral therapy, and education for fibromyalgia: a cluster-randomized controlled trial. Pain. 2017;158(12):2354–2363. doi:10.1097/j.pain.0000000000001036
52. Amutio A, Franco C, Pérez-Fuentes MDC, Gázquez JJ, Mercader I. Mindfulness training for reducing anger, anxiety, and depression in fibromyalgia patients. Front Psychol. 2015;5:1572. doi:10.3389/fpsyg.2014.01572
53. Holmes A, Christelis N, Arnold C. Depression and chronic pain. Med J Aust. 2013;199(6):S17–S20. doi:10.5694/mja12.10589
54. Häuser W, Jones G. Psychological therapies for chronic widespread pain and fibromyalgia syndrome. Best Pract Res Clin Rheumatol. 2019;33(3):101416. doi:10.1016/J.BERH.2019.05.001
55. Hoffman BM, Papas RK, Chatkoff DK, Kerns RD. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol. 2007;26(1):1. doi:10.1037/0278-6133.26.1.1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.