")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
The Role of Integrated Nursing Interventions in Traumatic Brain Injury Management in the Emergency Department: A Retrospective Study
Authors Zhou Y, Zhou L, Chen X
Received 17 December 2024
Accepted for publication 12 May 2025
Published 26 May 2025 Volume 2025:21 Pages 769—780
DOI https://doi.org/10.2147/TCRM.S512673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Yanli Zhou,1,* Linxia Zhou,2,* Xianxiang Chen1
1Department of Emergency Medicine The Second People’s Hospital of Hunan Province (Brain Hospital of Hunan Province), Changsha, Hunan Province, People’s Republic of China; 2Operating Room, The Second People’s Hospital of Hunan Province (Brain Hospital of Hunan Province), Changsha, Hunan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xianxiang Chen, Department of Emergency Medicine The Second People’s Hospital of Hunan Province (Brain Hospital of Hunan Province), No. 427, Furong Middle Road Section 3, Changsha, Hunan Province, People’s Republic of China, Email [email protected]
Background: Traumatic brain injury (TBI) is a leading cause of both disability and death, frequently necessitating treatment in emergency departments (ED). Integrated nursing interventions are critical in the management of TBI patients, but limited research has been conducted to evaluate their effectiveness in this setting. The aim of this article is to investigate and evaluate the impact of integrated nursing interventions on the management of TBI patients in the ED.
Method: A retrospective study was conducted among 216 patients with TBI who came to the ED between January 2022 and December 2022, of whom 120 were treated with nursing interventions and 96 were not treated with nursing interventions. The integrated interventions included rapid triage, continuous monitoring of neurological status, early rehabilitation involvement, patient and family education, and interdisciplinary care coordination. The medical records were reviewed to assess the utilization of nursing interventions and analyze the impact of these interventions on the short-term and long-term prognosis of TBI patients. Patient demographics, clinical characteristics, and outcomes were analyzed using descriptive statistics and logistic regression analysis.
Result: Among the 216 TBI patients, 96 (44.4%) received nursing interventions as part of their ED care. These patients had significantly lower rates of adverse events such as intracranial hemorrhage (3.3% vs 12.5%, P=0.018) and hospital stays (7 ± 2 days vs 10 ± 4 days, P< 0.001). Logistic regression analysis showed that nursing interventions were significantly associated with a decreased risk of adverse events (OR=0.25, 95% CI=0.10– 0.63, P=0.003).
Conclusion: Integrated nursing interventions are essential in the care of TBI patients in the emergency department. Early detection, swift treatment, continuous monitoring, assessment, and education for both patients and their families can enhance recovery and minimize the likelihood of complications. Implementation of nursing interventions should be encouraged in EDs to improve the quality of TBI care. Further studies are needed to investigate the optimal strategies and cost-effectiveness of nursing interventions in TBI management in the ED.
Keywords: traumatic brain injury, emergency department, nursing interventions, adverse events, prognosis, patient management
Introduction
Traumatic brain injury (TBI) represents a major public health issue, affecting approximately 69 million individuals globally every year.1,2 It is a leading cause of death and disability, particularly among young adults, and can lead to long-term physical, cognitive, and emotional sequelae. Previous studies have shown that emergency department (ED) care is often required for patients with TBI, and early intervention and prompt treatment are critical in improving patient outcomes.3,4 After traumatic brain injury (TBI) patients arrive at the Emergency Department (ED), rapid assessment, stabilization, and treatment are crucial for improving efficacy and reducing the risk of adverse events. In this context, nurses play a pivotal role in managing TBI patients within the ED. Their responsibilities extend throughout the patient’s entire hospitalization, and they collaborate closely with other healthcare professionals to ensure timely interventions and appropriate follow-up. The significance and necessity of our work lie in addressing the critical need for prompt and effective care during the initial stages of TBI presentation in the ED. Without comprehensive nursing interventions, potential consequences may include compromised patient outcomes, increased risks of adverse events, and suboptimal recovery trajectories.5 Therefore, elucidating the crucial role of nursing interventions in optimizing patient outcomes and reducing adverse events contributes to the comprehensive improvement of TBI care protocols assessment. Nurses play a key role in the management of TBI patients in the ED, providing care throughout the patient’s hospitalization and working collaboratively with other healthcare professionals to ensure timely interventions and appropriate follow-up. Through interdisciplinary nursing collaboration, comprehensive care refers to an integrated approach that goes beyond the emergency room setting.6,7 It involves inclusive communication, providing informational resources, and various interventions to support the rehabilitation of patients with traumatic brain injuries in different aspects, including language, memory, and motor function training. Such comprehensive care measures are necessary. For instance, A group randomized controlled trial by Saunders et al8 found that nurse-led interventions, such as fall prevention and pressure sore prevention education, significantly reduced the incidence of adverse events and length of stay in frail older patients and had the potential to prevent the progression of frailty in hospitalized older adults and improve patient prognosis. Similarly, Gamble et al9 examined the impact of early active care interventions on TBI outcomes and identified several key interventions, including improved monitoring and organized trauma systems and protocols, and patient/family education. Finally, the need to implement treatment strategies in resource-poor settings is emphasized.
The healthcare system in the region where this study was conducted is characterized by a significant role for nurses in emergency departments. Nurses in this region are responsible for a wide range of tasks, including triage, ongoing patient monitoring, early intervention, patient education, and coordination of care with other healthcare professionals. This broad scope of responsibilities allows for more integrated approaches to patient management, which is the focus of our study.
Despite the growing body of evidence on the effectiveness of nursing interventions in TBI care, there is still a need for further research to optimize their use in the ED setting. Few studies have specifically focused on the impact of nursing interventions on TBI patients in the ED, and there is a lack of standardized protocols for their implementation. Integrated Nursing Intervention is defined as a coordinated, multidisciplinary approach that combines nursing assessments, continuous monitoring of patients, early interventions, patient and family education, and close collaboration with other healthcare providers. This holistic approach aims to improve patient outcomes, particularly in the management of TBI cases within the emergency department setting. Therefore, this study aims to assess the effectiveness of integrated nursing interventions in improving the outcomes of TBI patients in the ED and provide insights into the optimal strategies for their implementation.
Materials and Methods
Study Design and Participants
This study will employ a retrospective cohort design to evaluate the effectiveness of nurse-led interventions in enhancing outcomes for TBI patients in the emergency department. It will include adult patients (18 years and older) who were diagnosed with TBI and required hospitalization after presenting to the ED during a specified time period (eg, January 2022 to December 2022). TBI is defined as brain injury resulting from external forces, including concussion (Patients initially diagnosed with concussion were carefully evaluated based on clinical presentation and imaging findings. If subsequent assessments indicated a more severe form of TBI, such as cerebral contusion or intracranial hematoma, those patients were reclassified under the appropriate subtype and excluded from the concussion subgroup.), brain contusion, traumatic epidural hemorrhage, traumatic subdural hematoma, and traumatic cerebral hemorrhage. The diagnosis will be confirmed by two imaging specialists who will jointly review CT and MRI results. Strict inclusion and exclusion criteria will be applied: Inclusion criteria include (1) patients aged 18 years or older at diagnosis; (2) TBI diagnosis based on imaging and physical examination; (3) absence of other major comorbidities. Exclusion criteria include (1) incomplete clinical data; (2) death within 24 hours of admission. The study will adhere to the Declaration of Helsinki and has been approved by the Ethics Committee of Brain Hospital Of Hunan Province. All patients provided informed consent.
Integrated Nursing Interventions
Integrated nursing interventions were initiated within the first hour of the patient’s admission to the emergency department, immediately following primary triage and stabilization procedures. To address concerns regarding the quantifiability and clarity of nursing interventions, specific details on frequency, duration, and methods for each intervention were incorporated:
Patient Education: Eligible patients and their families actively participated in expressing their views and received educational materials. The “Traumatic Brain Injury Guidebook” and a “cognitive rehabilitation instruction manual” were provided, adhering to established guidelines. Patient education sessions occurred twice weekly, each lasting 45 minutes, with content tailored to individual patient needs.
Quantifiable Language Training: Patients engaged in structured language training activities, including scheduled conversations with nursing staff three times a week for 30 minutes each session. Non-verbal communication techniques were taught, and patients participated in communication-enhancing activities such as role-playing and scenario discussions.
Structured Memory Training: Patients took part in a structured memory training program involving reading newspapers for 20 minutes daily, listening to the radio and music twice a week for 30 minutes, and engaging in intellectually stimulating games for 45 minutes, three times a week.
Documented Motor Function Training: To prevent complications, patients initiated documented motor function training. This included active and passive movements of affected limbs, starting within 48 hours post-admission. The frequency was three sessions per day, lasting 20 minutes each, progressively increasing the range of motion and incorporating joint flexion and extension, adduction, abduction, rotation, and other movements. This training was complemented by massage twice a week, hot compresses every other day, and acupuncture once a week.
Data Collection and Outcome Measures
Data will be extracted retrospectively from electronic medical records. The Glasgow Coma Scale (GCS) score was recorded for each patient at the time of admission to assess the level of consciousness and injury severity. Patients were subsequently stratified into mild (GCS 13–15), moderate (GCS 9–12), and severe (GCS ≤8) TBI categories. The primary emphasis of the outcome assessment lies in perioperative complications, complications associated with various physiological systems, and the duration of hospitalization. A survey of complications related to different physiological systems was conducted during the second week postoperatively. This comprehensive evaluation aims to provide a thorough understanding of the short-term effectiveness of Integrated Nursing Interventions. Secondary outcome measures include readmission rates, 30-day mortality, and 90-day mortality.
Circulatory System
We scrutinized complications related to the circulatory system, analyzing variables such as blood pressure, heart rate, and the occurrence of any cardiovascular events.
Urinary System
The assessment of complications related to the urinary system involved an examination of parameters such as urine output, kidney function, and the occurrence of urinary tract infections.
Digestive System
Complications associated with the digestive system, including gastrointestinal bleeding, bowel function, and nutritional issues, were thoroughly evaluated.
Coagulation System
We conducted a detailed examination of complications related to the coagulation system, considering variables such as clotting factors and the occurrence of thrombotic events.
The selection of these interventions was based on clinical guidelines and evidence-based practices previously demonstrated to be effective in the rehabilitation of patients with traumatic brain injury in emergency care settings.6,7
Data Analysis
Descriptive statistics will be used to summarize patient characteristics and outcome measures. The incidence of adverse events and other dichotomous outcomes will be compared between groups using chi-square tests or Fisher’s exact tests. Continuous outcomes such as hospital length of stay will be compared using t-tests or non-parametric tests as appropriate. Multivariable regression analysis will be used to adjust for potential confounders such as age, sex, injury severity, and comorbidities.
Data analysis was conducted using SPSS 25.0 (IBM, Armonk, New York, USA), with statistical significance set at P<0.05 (two-tailed). Graphs were created using R (version 4.0.5) and GraphPad Prism (version 8.0). Sample size estimation was performed prior to the study using PASS (version 11.0).
Follow-Up
All patients are discharged from the hospital and are followed up by two professional followers, who ask about the basic status of the patient and request the patient to come to the hospital for a review.
Results
Baseline Information of TBI with Integrated Nursing Interventions and without Integrated Nursing Interventions
The inclusion exclusion table is detailed in Figure 1. 216 patients with Traumatic Brain Injury (TBI) at admission, with 120 receiving Integrated Nursing Interventions and 96 receiving no such interventions. The two groups were similar in terms of gender distribution, age, spine trauma, use of hemostatic agents on admission, hypotension on arrival, GCS score on admission, hypoxia, surgical interventions, vital signs on admission, the mechanism of injury, type of TBI, injury site, and heart rate (P>0.05).
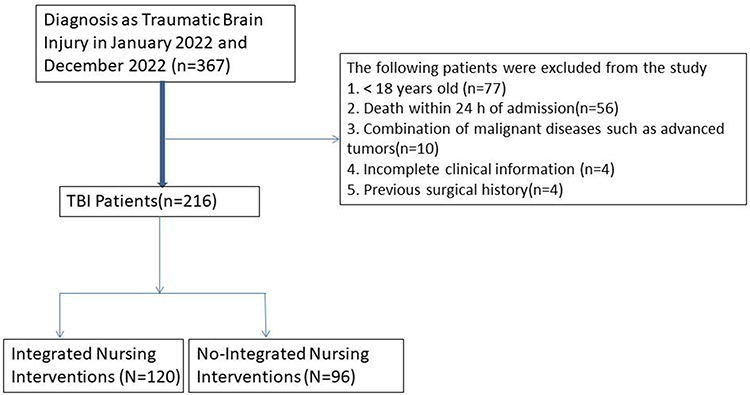 |
Figure 1 Inclusion and exclusion table for TBI patients. |
Specifically, the Integrated Nursing Interventions group had a higher proportion of traffic accidents (70.0% vs 62.5%), diffuse brain injury (55.0% vs 57.3%), and patients with a single-region injury (ie, TBI affecting only one anatomical brain area such as the frontal or temporal lobe) (71.7% vs 69.8%), but a lower proportion of high falls (15.0% vs 15.6%), focal brain injury (28.3% vs 37.5%), and injury site of ≥3 (5.0% vs 5.2%) than the No-Integrated Nursing Interventions group. The majority of patients had a GCS score within the moderate to severe range at admission, with 43.5% of patients in the Integrated Nursing Interventions group and 30.2% in the No-Integrated Nursing Interventions group presenting with severe TBI (GCS 3–8). Mild TBI (GCS 13–15) was observed in 50.5% and 48.0% of patients in the Integrated and No-Integrated groups, respectively. The distribution of GCS scores did not show significant differences between groups (P = 0.176).
The median values and interquartile ranges for systolic blood pressure, diastolic blood pressure, heart rate, and body temperature were not significantly different between the two groups (Table 1).
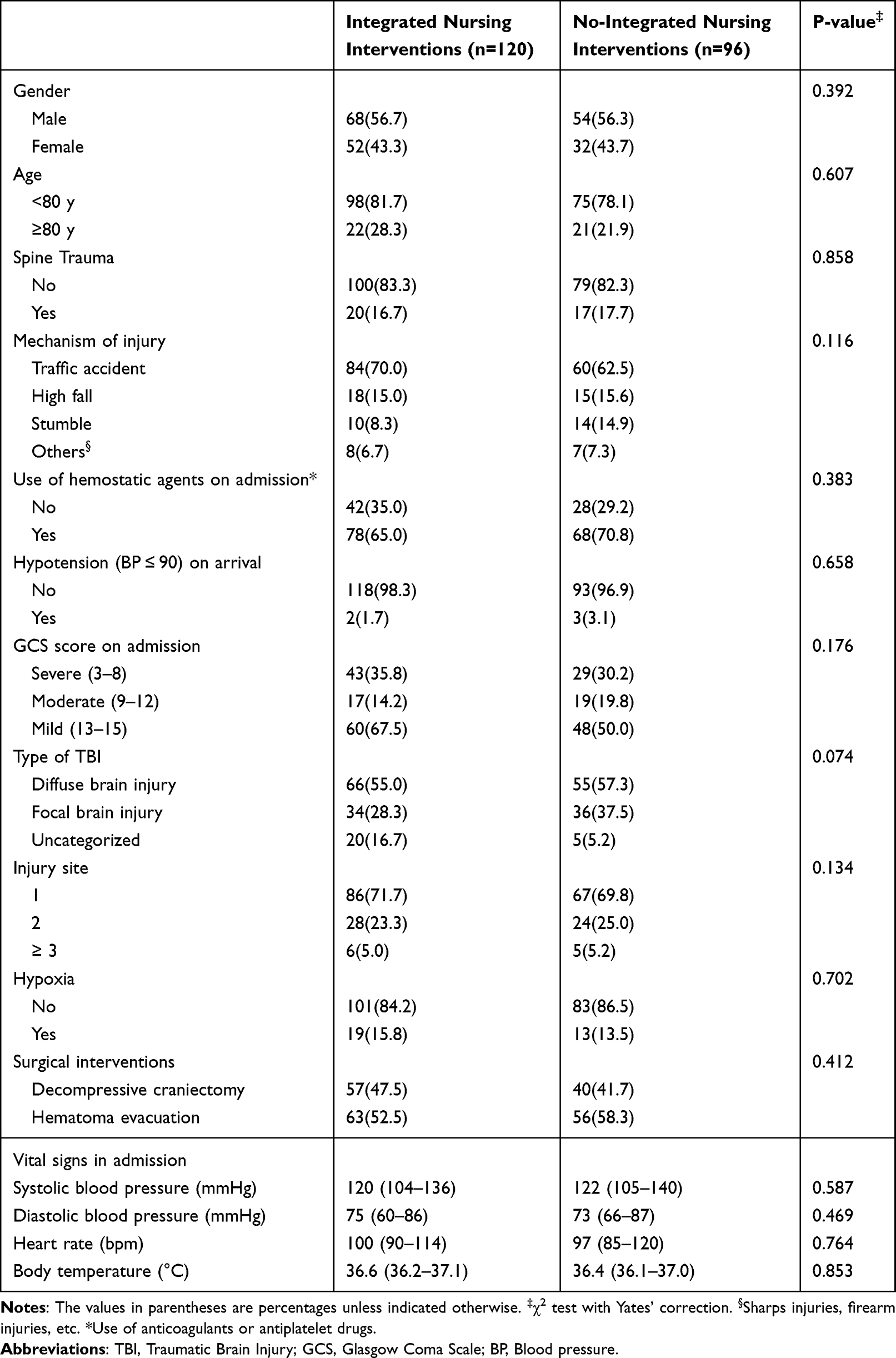 |
Table 1 Baseline Information of Patients with TBI at Admission (N = 216) |
Complications of TBI in Patients Receiving Comprehensive Nursing Interventions Versus Those Receiving No Comprehensive Care Interventions
Incidence of complications of traumatic brain injury (TBI) differs between patients receiving comprehensive care interventions and those receiving no comprehensive care interventions. The results showed that patients who received Integrated Nursing Interventions had a lower incidence of perioperative intracranial hemorrhage (3.3% vs 12.5%, P=0.018), shorter hospital stays (7±2 vs 10±4 days, P<0.001), and a lower incidence of respiratory infections (0.8% vs 9.4%, P=0.006) and postoperative infections (0% vs 3.4%, P<0.001) than those who did not receive such interventions.
Simultaneously, patients who underwent Integrated Nursing Interventions exhibited significantly lower postoperative GCS scores at two weeks, coupled with higher satisfaction levels.
There were no significant differences in circulatory, urinary, digestive, or coagulation complications between the two groups. These results suggest that Integrated Nursing Interventions may reduce the risk of certain TBI complications and lead to shorter hospital stays compared to No-Integrated Nursing Interventions (Table 2).
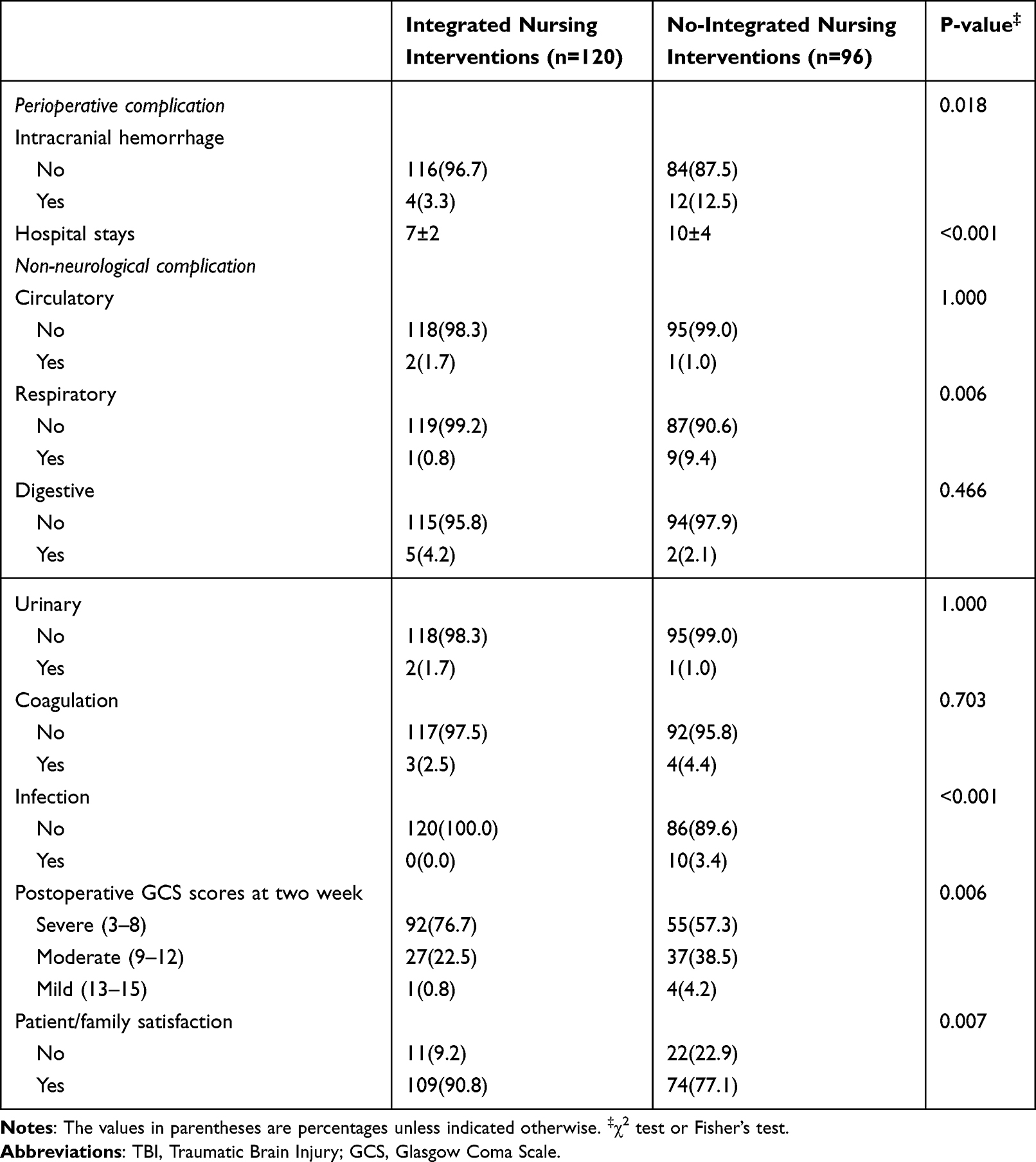 |
Table 2 Comparison of TBI Complications in Integrated Nursing Interventions Group and No-Integrated Nursing Interventions (N = 216) |
Univariate and Multivariate Cox Proportional Hazard Regression Analyses of Recurrence-Free Survival in TBI Patients
In the univariate analysis, age (p=0.043), hypotension on arrival (p=0.013), GCS score on admission (p<0.001), and integrated nursing interventions (p<0.001) were significantly associated with in-hospital mortality. In the multivariate analysis, age (p<0.001), hypotension on arrival (p=0.007), GCS score on admission (p<0.001), and integrated nursing interventions (p<0.001) remained significant predictors of in-hospital mortality.
Specifically, patients aged <80 years had a lower risk of in-hospital mortality compared to those aged ≥80 years (OR=0.843, 95% CI: 0.613–0.973). Patients without hypotension on arrival had a lower risk of in-hospital mortality compared to those with hypotension (OR=0.893, 95% CI: 0.785–0.912). Patients with mild (13–15) or moderate (9–12) GCS scores on admission had a lower risk of in-hospital mortality compared to those with severe (3–8) GCS scores (mild: OR=0.478, 95% CI: 0.348–0.792; moderate: OR=0.790, 95% CI: 0.641–0.891). Patients who received integrated nursing interventions had a higher risk of in-hospital mortality compared to those who did not (OR=1.828, 95% CI: 1.619–2.318).
Other variables such as gender, spine trauma, mechanism of injury, use of hemostatic agents on admission, admission destination, type of TBI, and injury site were not significantly associated with in-hospital mortality (Table 3).
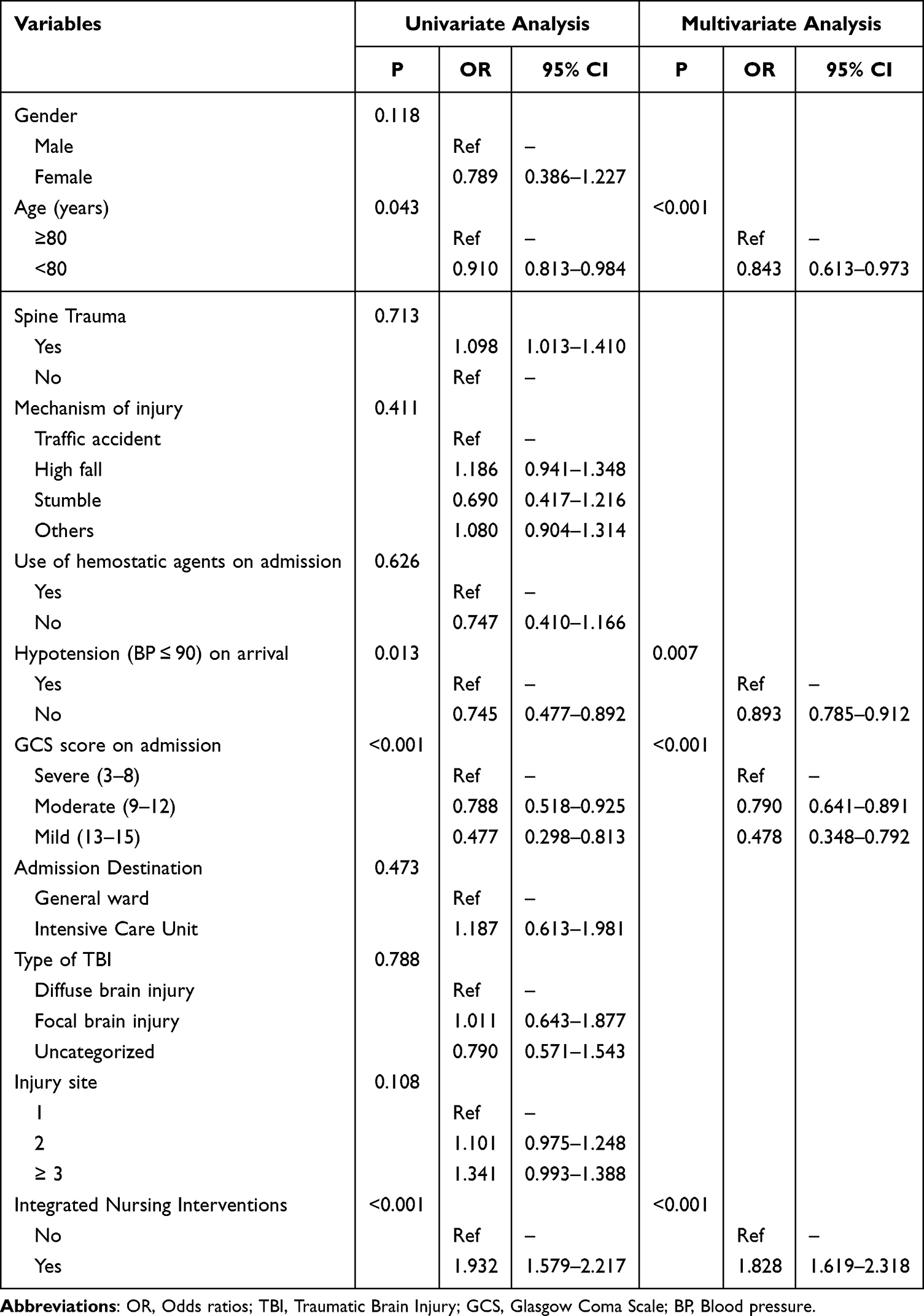 |
Table 3 Univariate and Multivariate Logistic Regression Analysis of Risk Factors Associated with in-Hospital Mortality in All TBI Patients |
Comparison of Clinical Prognostic of TBI Between Integrated Nursing Intervention Group and No Integrated Nursing Intervention Group
The results show that the integrated nursing intervention group had a lower 30-day mortality rate (5.8%) compared to the no-integrated nursing intervention group (14.6%), with a statistically significant difference (P=0.038). Similarly, the integrated nursing intervention group had a lower 90-day mortality rate (9.2%) than the no-integrated nursing intervention group (24.0%), with a statistically significant difference (P=0.004).
However, there was no statistically significant difference in readmission rates between the two groups, with 10.0% of patients in the integrated nursing intervention group and 15.6% of patients in the no-integrated nursing intervention group being readmitted within the study period (P=0.223). Overall, these findings suggest that integrated nursing interventions may improve short-term survival outcomes for patients with TBI (Table 4). The above data was represented through a bar proportion chart. After implementing comprehensive nursing interventions, as depicted in Figure 2, significant statistical differences are observed in readmission rates, 30-day mortality, and 90-day mortality (Figure 2).
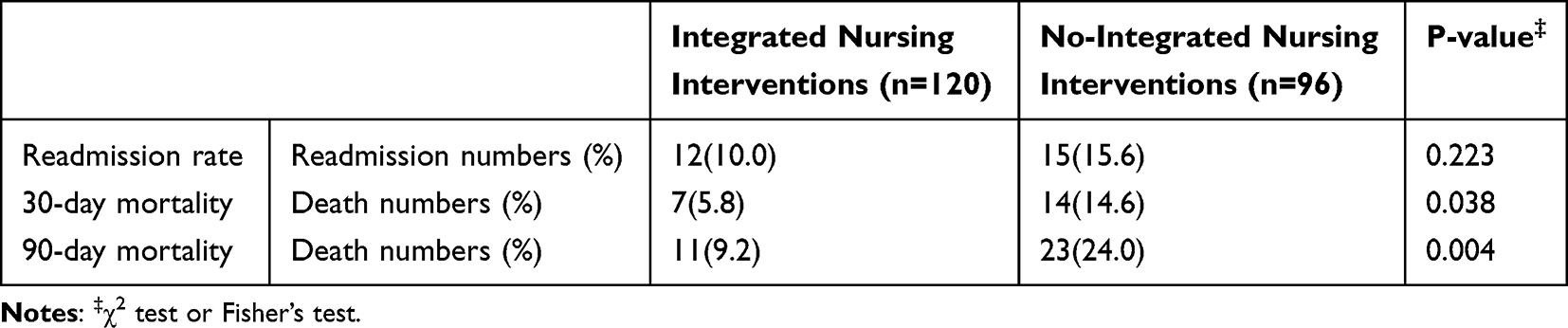 |
Table 4 Comparison of Clinical Prognostic of TBI Between Integrated Nursing Intervention Group and No Integrated Nursing Intervention Group (N = 216) |
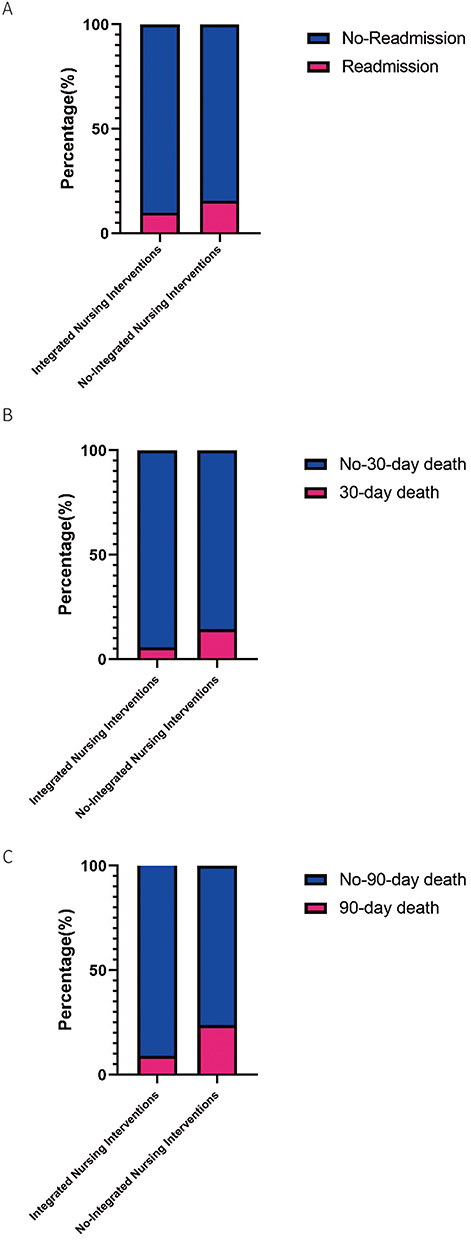 |
Figure 2 Comparison of Readmission and Mortality Outcomes Between Patients With and Without Integrated Nursing Interventions. (A) Hospital readmission rates. (B) 30-day mortality rates. (C) 90-day mortality rates. |
Discussion
Traumatic brain injury (TBI) can cause death and disability, so management strategies must focus on avoiding serious complications of TBI and reducing mortality.2,10,11 The aim of our study was to assess the impact of a comprehensive care intervention on patient outcomes in those with traumatic brain injury (TBI) in the emergency department (ED). Our results indicate that comprehensive care interventions are linked to improved short-term survival outcomes in TBI patients. It also reduces complications associated with TBI and reduces the length of hospital stay.
The emergency nursing care in the emergency department has always been a focal point of research. Different institutions utilize various approaches to demonstrate that certain nursing interventions for patients admitted through the emergency department can alter the short-term and long-term prognosis. Ridderikhof and colleagues found,12 in the emergency department, that nurse-initiated short-term and long-term pain management strategies for adult patients with traumatic injuries, particularly the use of fentanyl for severe pain, may enhance the long-term implications of pain for patients. For traumatic brain injury (TBI) patients, there is limited discussion among researchers regarding the pre-hospital ambulance service nursing capabilities before entering the emergency department. FALK and others,13 through a survey of 395 severely TBI-injured patients, discovered that the provision of ambulance personnel skills may better assess patient needs, although pre-hospital interventions and hospital mortality rates were not affected, there is a clear need for improvement in the management of emergency nursing care.
Our analysis revealed that patients who received integrated nursing interventions had significantly lower 30-day and 90-day mortality rates compared to those who did not receive these interventions. These results align with previous studies showing the positive impact of nurse-led interventions on patient outcomes across various clinical settings.14–16 For instance, research from three randomized trials in Ontario, Canada, led by Markle-Reid,17 demonstrated that nurse-led health promotion interventions resulted in significant improvements in health-related quality of life (HRQOL) for frail elderly home care clients, outperforming usual home care practices. Similarly, the results of a randomized controlled trial by Rasmussen et al18 suggest that family-centered interventions after traumatic brain injury may not be effective and that skilled nursing rehabilitation in a traumatic brain injury outpatient setting may be more preferable. A study by Blackmore et al19 identified the development, implementation and evaluation of a nurse-driven rapid reversal protocol for patients with TBI in the presence of pre-injury warfarin and that the protocol provided a more effective process of care for patients with TBI. Another recent study by Falk et al20 found that nurse-led discharge planning interventions were associated with reduced hospital readmissions and improved functional outcomes for patients with TBI.
The specific nursing interventions used in our study included early assessment and timely intervention, patient and family education, and collaborative care planning with other healthcare professionals. These interventions have been shown to be effective in improving patient outcomes in other clinical contexts.21 At the same time, postoperative patients may experience complications related to respiratory issues or infections. Previous researchers have also employed methods such as Incentive Spirometry to improve patient outcomes.22,23 Such approaches could potentially be applied in future nursing management systems. Our study adds to the existing literature by demonstrating their efficacy in the management of TBI in the ED.
Our findings also highlight the impact on some postoperative complications, especially infections and respiratory complications, with TBI patients who implemented comprehensive care measures having a lower proportion of hospitalized infections and respiratory complications (p<0.05), complications during hospitalization usually affect the prognosis and quality of life of TBI patients, thus necessitating comprehensive care measures to reduce complications.24,25 Longer hospitalization days are also a negative event for patients with TBI, which usually leads to higher consultation costs and a negative state of mind, and the length of hospitalization can also be reduced by this measure.26 Standardized protocols for implementing nursing interventions in the ED setting need to be taken into account. The lack of such protocols may lead to variations in the quality and effectiveness of care provided, which may lead to adverse patient outcomes. Further research is needed to develop and evaluate standardized protocols for nursing interventions for TBI management in the ED setting.
One limitation of our study is its retrospective design, which limits our ability to establish causality between nursing interventions and patient outcomes. Future studies using a prospective design and larger sample sizes are needed to confirm our findings. Additionally, our study was conducted at a single institution, limiting generalizability to other settings.
Conclusion
In conclusion, our study reveals a clear association between comprehensive care interventions and enhanced short-term survival outcomes, as well as a decrease in complications among patients with TBI in the ED. The implications of our findings strongly emphasize the urgent necessity for standardized protocols in implementing nursing interventions within the ED setting. Our research provides valuable insights into the optimal strategies for effective implementation, offering practical guidance for healthcare professionals. To fortify the evidence base and guide clinical practice, further research is imperative to validate our findings and contribute to the development of evidence-based guidelines for the management of TBI in the ED. Our recommendations are rooted in the demonstrated benefits of comprehensive care interventions and aim to enhance the overall quality of TBI care in emergency settings.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participation
Written informed consent was obtained from all participants. This research was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Brain Hospital of Hunan Province.
Consent for Publication
Written informed consent for publication was obtained.
Acknowledgments
Thanks to the nurses in the department for their help with the project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Khellaf A, Khan DZ, Helmy A. et al. Recent advances in traumatic brain injury. J Neurol. 2019;266(11):2878–2889. doi:10.1007/s00415-019-09541-4
2. Vella MA, Crandall ML, Patel MB, et al. Acute management of traumatic brain injury. Surg Clin N Am. 2017;97(5):1015–1030. doi:10.1016/j.suc.2017.06.003
3. Diaz-Arrastia R, Kochanek PM, Bergold P, et al. Pharmacotherapy of traumatic brain injury: state of the science and the road forward: report of the department of defense neurotrauma pharmacology workgroup. J Neurotrauma. 2014;31(2):135–158. doi:10.1089/neu.2013.3019
4. Hawryluk GWJ, Rubiano AM, Totten AM, et al. Guidelines for the management of severe traumatic brain injury: 2020 update of the decompressive craniectomy recommendations. Neurosurgery. 2020;87(3):427–434. doi:10.1093/neuros/nyaa278
5. Oyesanya TO, Thomas MA, Brown RL, et al. Nurses’ beliefs about caring for patients with traumatic brain injury. Western J Nurs Res. 2016;38(9):1114–1138. doi:10.1177/0193945916636629
6. Doneddu PE, Pensato U, Iorfida A, et al. Neuropathic pain in the emergency setting: diagnosis and management. J Clin Med. 2023;12(18):6028.
7. Flores-Sandoval C, Teasell R, MacKenzie HM, et al. Evidence-based review of randomized controlled trials of interventions for mental health management post-moderate to severe traumatic brain injury. J Head Trauma Rehabil. 2024;39(5):342–358. doi:10.1097/HTR.0000000000000984
8. Saunders R, Crookes K, Seaman K, et al. Effectiveness of nurse-led volunteer support and technology-driven pain assessment in improving the outcomes of hospitalised older adults: protocol for a cluster randomised controlled trial. BMJ open. 2022;12(6):e059388. doi:10.1136/bmjopen-2021-059388
9. Gamble M, Luggya TS, Mabweijano J, et al. Impact of nursing education and a monitoring tool on outcomes in traumatic brain injury. Afr J Emerg Med. 2020;10(4):181–187. doi:10.1016/j.afjem.2020.05.013
10. Bernardi E, et al. Traumatic brain injury. Emerg Med J. 2023;40:e2.
11. Sarmiento K, Kennedy J, Daugherty J, et al. Traumatic brain injury-related emergency department visits among American Indian and Alaska native persons-national patient information reporting system, 2005-2014. J Head Trauma Rehabil. 2020;35(5):E441–e9. doi:10.1097/HTR.0000000000000570
12. Ridderikhof ML, Schyns FJ, Schep NW, et al. Emergency department pain management in adult patients with traumatic injuries before and after implementation of a nurse-initiated pain treatment protocol utilizing fentanyl for severe pain. J Emergency Med. 2017;52(4):417–425. doi:10.1016/j.jemermed.2016.07.015
13. Falk AC, Alm A, Lindström V, et al. Has increased nursing competence in the ambulance services impacted on pre-hospital assessment and interventions in severe traumatic brain-injured patients? Scand J Trauma Resusc Emerg Med. 2014;22(1):20. doi:10.1186/1757-7241-22-20
14. Minen M, Jinich S, Vallespir Ellett G, et al. Behavioral therapies and mind-body interventions for posttraumatic headache and post-concussive symptoms: a systematic review. Headache. 2019;59(2):151–163. doi:10.1111/head.13455
15. Reuter-Rice K, Christoferson E. Critical update on the third edition of the guidelines for managing severe traumatic brain injury in children. Am J Crit Care. 2020;29(1):e13–e8. doi:10.4037/ajcc2020228
16. Sveen U, Guldager R, Soberg HL, et al. Rehabilitation interventions after traumatic brain injury: a scoping review. Disability Rehabil. 2022;44(4):653–660. doi:10.1080/09638288.2020.1773940
17. Markle-Reid M, Browne G, Gafni A, et al. Nurse-led health promotion interventions improve quality of life in frail older home care clients: lessons learned from three randomized trials in Ontario, Canada. J Eval Clin Pract. 2013;19(1):118–131. doi:10.1111/j.1365-2753.2011.01782.x
18. Rasmussen MS, Andelic N, Pripp AH, et al. The effectiveness of a family-centred intervention after traumatic brain injury: a pragmatic randomised controlled trial. Clin Rehabil. 2021;35(10):1428–1441. doi:10.1177/02692155211010369
19. Blackmore AR, Caputo LM, Bourg PW, et al. Developing, implementing, and evaluating a nurse-driven rapid reversal protocol for patients with traumatic intracerebral hemorrhage in the presence of preinjury Warfarin. J Trauma Nurs. 2016;23(3):138–143. doi:10.1097/JTN.0000000000000201
20. Falk AC. A nurse-led paediatric head injury follow-up service. Scand J Caring Sci. 2013;27(1):51–56. doi:10.1111/j.1471-6712.2012.00999.x
21. Winters BD, Weaver SJ, Pfoh ER, et al. Rapid-response systems as a patient safety strategy: a systematic review. Ann Internal Med. 2013;158(5_Part_2):417–425. doi:10.7326/0003-4819-158-5-201303051-00009
22. Mehrisadat Saremirad HY, Dalili A, Rastaghi S. Effect of motivational spirometry on severity of shoulder pain after laparoscopic cholecystectomy and its association with body mass index: a randomized clinical trial. J-Mazand-Univ-Med-Sci. 2021;31:61–70.
23. Saremirad M, Yazdimoghaddam H, Dalili A, et al. The impact of incentive spirometry on shoulder tip pain in laparoscopic cholecystectomy: a randomized clinical trial. Surg Laparosc Endosc Percutan Tech. 2021;32(1):14–20. doi:10.1097/SLE.0000000000001012
24. Blennow K, Brody DL, Kochanek PM, et al. Traumatic brain injuries. Nat Rev Dis Primers. 2016;2(1):16084. doi:10.1038/nrdp.2016.84
25. Gardner RC, Yaffe K. Epidemiology of mild traumatic brain injury and neurodegenerative disease. Molecular Cellular Neurosci. 2015;66:75–80. doi:10.1016/j.mcn.2015.03.001
26. Pasipanodya EC, Teranishi R, Dirlikov B, et al. Characterizing profiles of TBI severity: predictors of functional outcomes and well-being. J Head Trauma Rehabil. 2023;38(1):E65–e78. doi:10.1097/HTR.0000000000000791
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiology, Risk Factors and Etiology of Altered Level of Consciousness Among Patients Attending the Emergency Department at a Tertiary Hospital in Mogadishu, Somalia
Adan Ali H, Farah Yusuf Mohamud M
International Journal of General Medicine 2022, 15:5297-5306
Published Date: 30 May 2022
Serum NOX4 as a Promising Prognostic Biomarker in Association with 90-Day Outcome of Severe Traumatic Brain Injury
Jiang F, Chen Z, Hu J, Liu Q
International Journal of General Medicine 2022, 15:5307-5317
Published Date: 30 May 2022
Utility of Serum Growth Arrest-Specific Protein 6 as a Biomarker of Severity and Prognosis After Severe Traumatic Brain Injury: A Prospective Observational Study
Ni BK, Cai JY, Wang XB, Lin Q, Zhang XN, Wu JH
Neuropsychiatric Disease and Treatment 2022, 18:1441-1453
Published Date: 14 July 2022
A Rapid Prognostic Score Based on Bedside Arterial Blood Gas Analysis (ABG) Established for Predicting 60-Day Adverse Outcomes in Patients with Acute Pancreatitis in the Emergency Department
Lai Q, Wei W, He Y, Cheng T, Han T, Cao Y
Journal of Inflammation Research 2022, 15:5337-5346
Published Date: 15 September 2022
Prognostic Role of Serum Soluble Tim-3 in Severe Traumatic Brain Injury: A Prospective Observational Study
Zhang H, Lv QW, Zheng ZQ, Shen LJ, Zhou J, Guo M
Neuropsychiatric Disease and Treatment 2023, 19:153-169
Published Date: 18 January 2023