")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
The Role of Self-Efficacy Enhancement in Improving Self-Management Behavior for Type 2 Diabetes Mellitus Patients
Authors Jiang X , Jiang H , Li M
Received 26 February 2024
Accepted for publication 19 August 2024
Published 23 August 2024 Volume 2024:17 Pages 3131—3138
DOI https://doi.org/10.2147/DMSO.S460864
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Muthuswamy Balasubramanyam
Xinjun Jiang,1 Hua Jiang,2 Mingzi Li2
1International Nursing School, Hainan Medical University, Haikou, Hainan, People’s Republic of China; 2School of Nursing, Peking University, Beijing, People’s Republic of China
Correspondence: Mingzi Li, Email [email protected]
Background: The effectiveness of a self-efficacy-focused structured education program for patients with diabetes mellitus has been verified. However, changes in self-efficacy for the behavior change mechanism in patients who participated in the program require clarification.
Aim: To analyze the mechanism of self-management behavioral variations in patients with type 2 diabetes mellitus who underwent a self-efficacy-focused structured education program.
Methods: A secondary analysis of patients who received a self-efficacy-focused structured education program was conducted using data from a multicenter randomized controlled trial. The relationships among the 3-, 6-, and 12-month changes in diabetes knowledge, self-efficacy, diabetes distress, and self-management behaviors in patients with type 2 diabetes mellitus were studied using a structural equation model.
Results: Enhancement of self-efficacy among patients receiving a self-efficacy-focused structured education program directly influenced improvements in self-management behaviors at 3, 6 and 12 months. The increase in diabetes knowledge directly and indirectly improved self-management behaviors at 3 months, but the direct effect on behavior disappeared at 6 months and the indirect effect on behavior by enhancing self-efficacy only lasted until 6 months. The decrease in diabetes distress directly influenced improvement in self-management behaviors at 3 months. While it did not directly influence self-management behavior improvement at 6 and 12 months, it indirectly affected behavior improvement by enhancing self-efficacy.
Conclusion: The enhancement of self-efficacy plays a core role in improving and maintaining self-management behaviors in patients with type 2 diabetes mellitus who receive self-efficacy-focused structured education programs. Patients’ behaviors can be improved by gaining more diabetes knowledge and mitigating diabetes distress at the 3- and 6-month follow-up. Improvements in behaviors at the 12-month follow-up could be achieved by mitigating diabetes distress.
Keywords: diabetes mellitus, type 2, self efficacy, self-management behaviors, structured education, China
Introduction
Diabetes mellitus (DM) affects 10.5% of adults worldwide, or around 537 million people.1 It can cause disability, death, and seismic and economic challenges to healthcare systems. Good glycemic control can reduce diabetes-related complications2 and medical costs. Diabetes self-management behaviors (DSMB), including a reasonable diet, regular exercise, foot care, self-monitoring, and medication, are critical to managing the disease in daily life. Optimal DSMB are associated with better blood sugar level.3,4
A diabetes-structured education program is recommended by national and international guidelines to help patients improve their DSMB.5–7 However, some researchers suggest that the effects of diabetes-structured education programs on patients are not sustainable in the long term, and often attenuates between 6 and 12 months.8,9 This suggests the need for a detailed analysis of behavior change in patients who received structured education to identify the reasons for unmaintained behavior change. However, little research has been conducted in this area.
The self-efficacy-focused structured education program (SSEP) is one example of a self-efficacy-centered program that enhances diabetes self-efficacy of the patients.10,11 The effectiveness of the SSEP among patients with type 2 diabetes mellitus (T2DM) for improving diabetes self-efficacy (DSE), diabetes knowledge (DK), diabetes distress (DD), and DSMB has been verified.10–12 Moreover, the short- and long-term cost-effectiveness of the SSEP has been confirmed.13,14 However, no research currently reveals the mechanisms by which DSE, DK, and DD affect behavioral changes in patients with T2DM receiving SSEP.
DSE refers to a patient’s belief about his or her ability to successfully perform diabetes-related behaviors that lead to desired disease management outcomes.15 Our previous cross-sectional study found that diabetes self-efficacy was an important predictor of DSMB.16 A similar result was also found in other cross-sectional studies.17,18 Additionally, DSE mediated the associations between DK and DSMB,19 and between DD and DSMB in patients with T2DM.16 Thus, the SSEP included four structured modules that focused on four sources of information aiming to enhance DSE. However, whether SSEP affects DSMB through DSE is unclear, and the literature is scarce on the predictive ability of DSE improvement on changes in DSMB.
Previous studies also indicated that DK directly affects DSMB.16,20,21 DK refers to a patient’s understanding of DM information. One study found that most patients with DM lacked DK,22 which might have hindered DSMB implementation. DD is another factor that may affect DSMB.23,24 DD is a negative psychological reaction experienced by patients who bear an emotional burden and excessive concern regarding diabetes management and the prevention of complications. Therefore, in addition to promoting DSE enhancement in patients, an SSEP also increases DK and alleviates DD. However, it is not clear how changes of DK and DD affect DSMB at different follow-up points.
Given the scarcity of evidence regarding the influence of DSE, DK, and DD on DSMB, and the demonstrated difficulty in sustaining behavior change following participation in an SSEP, it is necessary to conduct an in-depth analysis of the mechanisms of behavioral changes in patients who have received structured education program. Of the available evidence on the four variables DSE, DK, DD, and DSMB, most studies have focused on a specific time point using a cross-sectional design. The relationships between the changes in DSE, DK, DD, and DSMB over time are unknown. This study aimed to analyze the associations between the enhancement of self-efficacy, increased diabetes knowledge, decreased diabetes distress, and improvement of self-management behaviors after individuals received self-efficacy-focused structured education program at the 3-month (T1), 6-month (T2), and 12-month (T3) follow-up timepoints.
Methods
Introduction of the Study
The design and Methods of the multicenter randomized controlled trial conducted from April 2017 to December 2018 in China have been described in detail elsewhere.10,11 The project was approved by the Institutional Review Board of Peking University (IRB00001052‐17,031). Briefly, the four-center trial recruited adult patients with T2DM who had not received insulin therapy in the last three months. A total of 265 patients were recruited by doctors and subsequently referred to nurses. After providing informed consent, patients were then randomly assigned to the intervention or control groups in a 1:1 ratio. Participants in the intervention and control groups received the SSEP and routine education, respectively. The SSEP is a structured educational program focused on enhancing patients’ self-efficacy to facilitate self-management behaviors. The four-module program covered the following topics: basic knowledge of diabetes mellitus, self-monitoring, dietary management, physical activities, foot care, medication, and complication screening. Four sources of information, namely performance accomplishments, vicarious experience, verbal persuasion, and physiological/emotional arousal, were embedded in the program. The program was delivered once a week continuously, and each module lasted approximately 60–90 minutes. A self-management behavioral change model was developed (Supplementary Figure S1) based on self-efficacy theory25 and previous studies.16,23,24
Indicators and Measurements
The indicators DSE, DK, DD, and DSMB were measured at T0, T1, T2, and T3 months. The data collection methods have been described in detail in previously published papers.10,11
Statistical Analysis
The statistical package SPSS 27.0 (IBM SPSS AMOS 27.0) was used for descriptive statistical analysis and Pearson correlation analysis. Descriptive statistical analysis as used to examine demographic information of the participants. The Pearson correlation analysis was used to examine the pairwise relationships between the changes in DSE, DK, DD, and DSMB. AMOS 23.0 (IBM SPSS AMOS 23.0) was used for structural equation model (SEM). SEM with multigroup path analysis was conducted to examine the relationships between the changes of DSE, DK, DD, and DSMB at different follow-up time points. Models at different follow-up time points were evaluated with the following requirements: χ2 with a non-significant P-value (P>0.05), GFI > 0.90, and NFI > 0.90 were recognized as a good model fit according to Wu30 and Hair.31 The critical ratio (absolute value) <1.96 between the parameters in multi-group path analysis could be considered equal, otherwise they were considered unequal and exerted significant difference.
Results
Study Population
There were 133 adults with a mean ± SD age of 57.35 ± 9.09 years who received the SSEP. A total of 58.65% of the participants were women and 94.74% were married. The proportion of retired participants was 66.17% and 42.11% had an educational level of primary school or below. Other characteristics of the participants who received SSEP are reported in detail in previous publications.10,11
Changes in Variables
The mean increases in DSE at T1, T2, and T3 follow-ups compared with T0 were 0.85 ± 0.95, 1.02 ± 1.01, 1.46 ± 1.14, respectively. The mean increases in DK at T1, T2, and T3 follow-ups compared with baseline were 4.02 ± 2.29, 4.07 ± 2.26, and 3.87 ± 2.57, respectively. The mean decreases in DD at T1, T2, and T3 follow-ups compared with baseline were 7.55 ± 14.26, 10.93 ± 16.26, and 17.63 ± 17.57, respectively. The mean increases in DSMB at T1, T2, and T3 follow-ups compared with baseline were 12.93 ±13.46, 11.86 ± 15.07, and 6.46 ± 15.31, respectively.
Relationship Between Changes in Variables
The Results showed no significant difference in the correlation between the changes in DD and DSE at the T1 follow-up (P>0.05). There was no significant difference in the correlation between the changes in DK and DSMB at the T3 follow-up (P>0.05). However, significant differences were observed in the correlations between the other variables at the T1, T2, and T3 follow-ups (P<0.05) (Supplementary Tables S1, S2, and S3).
Structural Modeling
Multigroup path analysis further analyzed the relationships between the variables at different follow-up points. Since the hypothesized theoretical model is a saturated model, the model showed a good fit to the data (χ2=0, GFI=1.000, NFI=1.000).
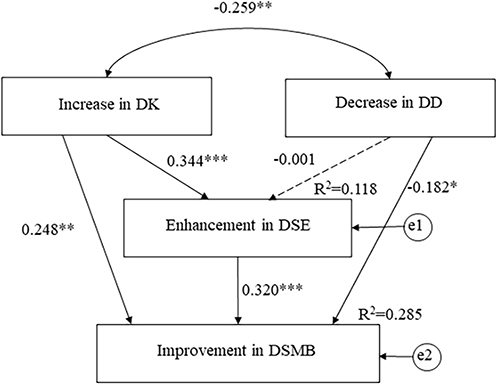 |
Figure 1 Behavior change model (changes in variables at T1 follow-up, *P<0.05, **P<0.01, ***P<0.001). |
 |
Figure 2 Behavior change model (changes in variables at T2 follow-up, *P<0.05, ***P<0.001). |
 |
Figure 3 Behavior change model (changes in variables at T3 follow-up, *P<0.05, ***P<0.001). |
Discussion
This study assessed the relationships between the 3-, 6-, and 12-month changes in diabetes knowledge, self-efficacy, diabetes distress, and self-management behaviors in a multicenter RCT of patients with T2DM who received SSEP. The results demonstrated that self-efficacy enhancement was a core predictor of improved DSMB at the T1, T2, and T3 follow-ups. The effects of the increase in diabetes knowledge on DSMB improvement were maintained only at the T1 and T2 follow-ups. The effects of the decrease in diabetes distress on DSMB improvement shifted from direct at the T1 follow-up to indirect at the T2 and T3 month follow-ups.
This study found that enhancing self-efficacy is crucial for improving patients’ DSMB. The enhancement of self-efficacy at 3, 6, and 12 months after the SSEP intervention directly improved patients’ DSMB. As the SSEP intervention time progressed, the impact of enhanced self-efficacy on the patients’ DSMB increased. However, there were no significant differences in the path coefficients among the three follow-up points. This indicates that enhancing the self-efficacy of patients can help establish and maintain patients’ DSMB. This is in line with the American Diabetes Association recommendation that health providers consider improving patient elf-efficacy for DSMB.32 The self-efficacy theory suggests that interventions based on the four sources of information can enhance patients’ self-efficacy and thus influence their behavior.25 This study supports the claims made by the self-efficacy theory, as SSEP based on the four sources of information can enhance patients’ self-efficacy and directly help improve DSMB. Additionally, the enhancement of self-efficacy plays a partial or complete mediating role, as an increase in diabetes knowledge and a decrease in diabetes distress both improve DSMB by enhancing self-efficacy. This further illustrates the importance of enhancing and maintaining self-efficacy in improving the DSMB of patients.
Interestingly, we found the direct and indirect effects of increased diabetes knowledge on the improvement in DSMB only lasted between 3 and 6 months. Additionally, there were significant differences in the path coefficients between the increase in diabetes knowledge and the improvement in DSMB among different follow-up periods. Unlike previous cross-sectional studies16,20,21 that focused solely on a single point in time, these findings indicate that an increase in diabetes knowledge indeed plays a significant role in improving DSMB in the short-term. As time progressed, patients developed a better understanding of how to manage the disease, which resulted in a plateau in diabetes knowledge growth. The effects of diabetes knowledge on DSMB will disappear in the long-term. Therefore, it is far from enough to only provide diabetes knowledge for patients to maintain DSMB.
Fortunately, the direct and indirect effects of decrease in distress on the improvement in DSMB were observed between 3 and 12 months. There were also significant differences in the path coefficients between the decrease in diabetes distress and the improvement in DSMB among different follow-up periods. In contrast to previous cross-sectional, single-timepoint studies,23,24 these findings highlight the dynamic nature of the relationship between decrease in diabetes distress and the improvement in DSMB. This suggests the importance of providing early and continuous psychological support to patients, especially from the 6-month time point. This is when the focus of the intervention program should shift towards psychological aspects, such as effectively coping with and adjusting to negative emotions that may arise during the diabetes management process, and maintaining confidence in DSMB.
In this study, increased diabetes knowledge in the SSEP group was consistently negatively correlated with a reduction in diabetes distress, indicating that the patients experienced emotional improvement as they gained more diabetes knowledge. The explanatory strength of the increase in diabetes knowledge and decrease in diabetes distress on the enhancement of self-efficacy increased slightly at 6 and 12 months after the SSEP intervention, mainly due to the effect of reducing diabetes distress. SSEP aims to help patients with diabetes understand the disease, arouse their internal motivation, and encourage them to consciously change their DSMB. The results showed that the explanatory strengths of increased diabetes knowledge, self-efficacy enhancement, and decrease in diabetes distress on the improvement of DSMB at the T1, T2 and T3 follow-up points were 28.5%, 20.7%, and 20.5%, respectively. This suggests that consciously and rationally arousing internal motivation in patients with diabetes positively affected the establishment and maintenance of DSMB. Marteau et al considered that interventions that only focus on improving individuals’ knowledge and beliefs have a limited effect on changing individuals’ behaviors because they overlook environmental impact.33,34 Most individuals’ decision-making behaviors are cued by unconscious and involuntary environmental stimuli.33,34 Therefore, changing the environment to reduce the triggers for unhealthy behaviors is likely to help patients achieve better DSMB. Future research should be conducted on the unconscious decision-making process of patients with diabetes, optimize intervention plans based on SSEP, and observe their effects to further elucidate mechanisms for improving patients’ DSMB.
Strengths and Limitations
This study explores the mechanism of DSMB changes in patients receiving SSEP. The results of the different models can be used as a framework to explain the process of self-management behavioral changes in T2DM patients who received SSEP, and the results of these models can be confirmed and enriched by the self-efficacy theory to some extent. These results can also guide the development of self-management support interventions after the SSEP.
Because the original study was a multicenter RCT, the study participants were from four hospitals in China. Thus, our results better reflect the characteristics of the Chinese population. However, the primary limitation of this study was that it used secondary data analysis of a multicenter RCT. The data for each variable was for the RCT rather than specifically designed for this study. Due to the strict inclusion and exclusion criteria in RCT, the generalizability of the results may be limited. Nevertheless, the measurements of these variables were conducted by the same trained researchers, which provided a foundation for obtaining high-quality data. Additionally, the explanatory strengths of the models in the study did not exceed 30%, which indicated that additional variables, such as unconscious factors, might be important for the improvement of patients’ DSMB. The patients’ DSMB may be better accounted for in the future when these variables are included.
Conclusions
The enhancement of self-efficacy has a direct positive effect on the improvement of self-management behavior and plays a partial or full mediating role in DSMB improvement at different follow-up time points. The direct and indirect effects of the increase in diabetes knowledge on the improvement in DSMB were maintained only at the 3-month and 6-month follow-ups. Whereas the effects of the decrease in diabetes distress on the improvement in DSMB shifted from direct function at the 3-month follow-up to indirect function at the 3-month and 6-month follow-ups. The results of the models can help explain the DSMB change mechanisms in T2DM patients who received SSEP and verify the self-efficacy-focused structured education program. Moreover, the findings can guide self-management support interventions at different follow-up time points after the SSEP to further maintain patients’ behavioral improvement.
Data Sharing Statement
Individual deidentified participant data beyond what is included in the manuscript and Supplementary materials will not be shared. Any additional questions should be directed to the corresponding author.
Funding
The work was supported by the Project of National Natural Science Foundation of China (82304262), and the Hainan Provincial Natural Science Foundation of China (820RC631).
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas 2021 | IDF Diabetes Atlas; 2021. Availabe from: https://diabetesatlas.org/atlas/tenth-edition/?dlmodal=active&dlsrc=https%3A%2F%2Fdiabetesatlas.org%2Fidfawp%2Fresource-files%2F2021%2F07%2FIDF_Atlas_10th_Edition_2021.pdf.
2. Fava MC, Reiff S, Azzopardi J, Fava S. Time trajectories of key cardiometabolic parameters and of cardiovascular risk in subjects with diabetes in a real world setting. Diabet Metabc Syndr Clinic Res Revie. 2023;17(6):102777. doi:10.1016/j.dsx.2023.102777
3. Ji M, Ren D, Dunbar-Jacob J, Gary-Webb TL, Erlen JA. Self-Management Behaviors, Glycemic Control, and Metabolic Syndrome in Type 2 Diabetes. NURSING RESEARCH. 2020;69(2):E9–E17. doi:10.1097/NNR.0000000000000401
4. Schmitt A, Bendig E, Baumeister H, Hermanns N, Kulzer B. Associations of depression and diabetes distress with self-management behavior and glycemic control. Health Psychol. 2021;40(2):113–124. doi:10.1037/hea0001037
5. Chinese Diabetes Society. Guidelines for the prevention and treatment of type 2 diabetes in China (2020 edition). Chin J Diabetes Mellitus. 2021;10(1):4–67. doi:10.3760/cma.j.issn.1674-5809.2018.01.003
6. National Institute for Health and Care Excellence. Type 2 diabetes in adults: management | guidance and guidelines | NICE; 2022. Availabe from: https://www.nice.org.uk/guidance/ng28.
7. A PM, K BJ, Cypress M, et al. Diabetes Self-management Education and Support in Adults With Type 2 Diabetes: a Consensus Report of the American Diabetes Association, the Association of Diabetes Care & Education Specialists. the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of Pas, the American Association of Nurse Practitioners, and the American Pharmacists Association. Scien Diabe Self Manag Care. 2021; 47(1):54–73. doi:10.1177/0145721720987936
8. Captieux M, Pearce G, L S PH, et al. Supported self-management for people with type 2 diabetes: a meta-review of quantitative systematic reviews. BMJ Open. 2018;8(12):e024262. doi:10.1136/bmjopen-2018-024262
9. He Q, Zhao X, Wang Y, et al. Effectiveness of smartphone application-based self-management interventions in patients with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. J Adv Nurs. 2022; 78(2):348–362. doi:10.1111/jan.14993
10. Jiang X, Jiang H, Chen Y, et al. The Effectiveness of a Self-Efficacy-Focused Structured Education Program (SSEP) in Improving Metabolic Control and Psychological Outcomes of Type 2 Diabetes Patients: a 12-Month Follow-Up of a Multicenter Randomized Controlled Trial. Diabe Metabolic Syndro Obes. 2021;14:305–313. doi:10.2147/DMSO.S290029
11. Jiang X, Jiang H, Lu Y, et al. The effectiveness of a self-efficacy-focused structured education programme on adults with type 2 diabetes: a multicentre randomised controlled trial. J Clin Nurs. 2019;28(17–18):3299–3309. doi:10.1111/jocn.14908
12. Yu X, Chau J, Huo L, et al. The effects of a nurse-led integrative medicine-based structured education program on self-management behaviors among individuals with newly diagnosed type 2 diabetes: a randomized controlled trial. BMC NURSING. 2022;21(1):217. doi:10.1186/s12912-022-00970-7
13. Jiang X, Jiang H, Tao L, Li M. The Cost-Effectiveness Analysis of Self-Efficacy-Focused Structured Education Program for Patients with Type 2 Diabetes Mellitus in Mainland China Setting. Front Public Health. 2021;9(9):767123. doi:10.3389/fpubh.2021.767123
14. Jiang X, Tao L, Li M. The structured education for type 2 diabetes patients without insulin therapy: a cost-effectiveness analysis. NURSING RESEARCH. 2022;36(7). doi:10.12102/j.issn.1009-6493.2022.07.027
15. Hurley AC, Shea CA. Self-efficacy: strategy for enhancing diabetes self-care. Diabet Educat. 1992;18(2):146–150. doi:10.1177/014572179201800208
16. Jiang X, Jiang H, Li M, Lu Y, Liu K, Sun X. The Mediating Role of Self‐Efficacy in Shaping Self‐Management Behaviors Among Adults With Type 2 Diabetes. World Evid-Ba Nur. 2019;16(2):151–160. doi:10.1111/wvn.12354
17. He Q, Liu Y, Lin K, Zhao F, Guo H, Shen Y. Diabetes self-management and its related factors among Chinese young adults with type 2 diabetes mellitus. Nursing Open. 2023;10:6125–6135. doi:10.1002/nop2.1834
18. Zhang A, Wang J, Wan X, et al. The mediating effect of self-efficacy on the relationship between diabetes self-management ability and patient activation in older adults with type 2 diabetes. Geriatric Nurs. 2023;51:136–142. doi:10.1002/nop2.1834
19. Liu H, Yao Z, Shi S, Zheng F, Li X, Zhong Z. The Mediating Effect of Self-Efficacy on the Relationship Between Medication Literacy and Medication Adherence Among Patients with Type 2 Diabetes. Patient Prefe Adheren. 2023;17:1657–1670. doi:10.2147/DMSO.S290029
20. Zhang Y, Zhang B, Chen C, Feng X, Song S, Wang H. The Mediation Effect of Attitude on the Association Between Knowledge and Self-Management Behaviors in Chinese Patients With Diabetes. Int J Public Health. 2023;68:1606022. doi:10.3389/ijph.2023.1606022
21. Lamptey R, Amoakoh-Coleman M, Djobalar B, Grobbee DE, Adjei GO, Klipstein-Grobusch K. Diabetes self-management education interventions and self-management in low-resource settings; a mixed methods study. PLoS One. 2023;18(7):e0286974. doi:10.1371/journal.pone.0286974
22. McElfish PA, Andersen JA, Rowland B, et al. Assessment of Diabetes-Related Health Disparities among the Marshallese Living in the Republic of the Marshall Islands. Hawaii J Health Soc Welf. 2021;80(10):235–241. doi:10.2105/ajph.91.9.1371
23. Gao Y, Xiao J, Han Y, et al. Self-efficacy mediates the associations of diabetes distress and depressive symptoms with type 2 diabetes management and glycemic control. Gene Hospl Psychi. 2022;78:87–95. doi:10.1016/j.genhosppsych.2022.06.003
24. Patra S, Patro BK, Padhy SK, Mantri J. Prevalence of diabetes distress and its relationship with self-management in patients with type 2 diabetes mellitus. Ind Psychiatry J. 2021;30(2):234–239. doi:10.4103/ipj.ipj_60_19
25. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. NJ: Prentice Hall; 1986.
26. Wei J (2013). Research on relationship between diabetes knowledge, self-efficacy and self-management among rural elderly patients. [Master thesis], Hangzhou Normal University, Hangzhou.
27. Liu YL (2016). A structured treatment and education program for patients with type 2 diabetes without insulin therap. development and practice.[Master thesis], Peking University, Beijing.
28. Li MZ. Study and application of depression screening methods in patients with diabetes. Peking Unive Beijing. 2012.
29. Wan QQ, Shang SM, Lai XB, Pan J. Study on the reliability and validity of summary of diabetes self-care activities for type 2 diabetes patients. Chin J Pracl Nurs. 2008;24(7):26–27. doi:10.3760/cma.j.issn.1672-7088.2008.07.009
30. Wu M. Structural Equation Modeling - Operation and Application of AMOS. Chongqing: Chongqing University Press; 2022.
31. Hair JF, Black WC, Babin BJ, Anderson RE. Multivariate Data Analysis. Englewood: Prentice Hall; 1998.
32. American Diabetes Association Professional Practice Committee. Facilitating Behavior Change and Well-being to Improve Health Outcomes: standards of Medical Care in Diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S60–S82. doi:10.2337/dc22-S005
33. Marteau TM. Changing minds about changing behaviour. Lancet. 2018;391(10116):116–117. doi:10.1016/S0140-6736(17)33324-X
34. Marteau TM, Hollands GJ, Fletcher PC. Changing human behavior to prevent disease: the importance of targeting automatic processes. SCIENCE. 2012;337(6101):1492–1495. doi:10.1126/science.1226918
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.