")
Back to Journals » Nature and Science of Sleep » Volume 17
The Sleep Patterns and Influencing Factors of Chronic Heart Failure Patients in China: A Latent Profile Analysis
Authors Li Y , Li J, Qin J, Zhou S, Gong K
Received 28 November 2024
Accepted for publication 12 March 2025
Published 8 April 2025 Volume 2025:17 Pages 571—581
DOI https://doi.org/10.2147/NSS.S509059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yan Li,1,2 Jiamin Li,1,2 Jingwen Qin,1 Sixin Zhou,1,2 Kaizheng Gong1
1Department of Cardiology, Affiliated Hospital of Yangzhou University, Yangzhou University, Yangzhou, People’s Republic of China; 2School of Nursing School of Public Health, Yangzhou University, Yangzhou, People’s Republic of China
Correspondence: Kaizheng Gong, Department of Cardiology, Affiliated Hospital of Yangzhou University, Yangzhou University, No. 368, Hanjiang Middle Road, Yangzhou, 225000, People’s Republic of China, Email [email protected]
Purpose: Sleep problems such as reduced sleep efficiency, difficulty initiating sleep, and increased sleep disturbances significantly affect the quality of life and health status of patients with chronic heart failure (CHF). However, the sleep patterns of CHF patients and their influencing factors need to be further studied. Therefore, this study aimed to explore the latent sleep patterns in patients with CHF and to analyze the factors influencing different sleep patterns.
Patients and Methods: A convenience sampling method was adopted to select 290 patients with CHF who were hospitalized in the Department of Cardiology of a tertiary hospital in Yangzhou City, Jiangsu Province, China, from January to August 2024. The investigation utilized a general information questionnaire, the Pittsburgh Sleep Quality Index (PSQI), and the Fear of Progression Questionnaire-Short Form (FoP-Q-SF). Utilizing Mplus version 8.3 for potential profile analysis, the influences on potential categorization were examined through univariate and multivariate logistic regression analyses.
Results: The sleep quality score of 290 patients with CHF was (12.00± 3.95). The findings from latent profile analysis indicated that the sleep quality patterns of patients with CHF were categorized into three distinct profiles: relatively good sleep group (n=87, 30.3%), low sleep efficiency-low medication use group (n=160, 54.9%), and sleep disorder-substance dependence group (n=43, 14.8%). Multiple logistic regression analysis showed that age, monthly income, number of hospitalizations for heart failure in a year, number of comorbidities, and fear of progression were influential factors (P < 0.05).
Conclusion: Sleep quality among patients with CHF exhibits distinct distributional profiles. Healthcare providers should implement tailored sleep management strategies and psychological interventions, aligning with the sleep patterns and influencing factors specific to patients with CHF. However, it is necessary to note that this study employed a cross-sectional design, and future research could benefit from a longitudinal design.
Keywords: chronic heart failure, sleep quality, latent profile analysis, fear of progression, influencing factors
Introduction
Chronic heart failure (CHF) is a significant clinical and public health challenge worldwide, with the current estimate suggesting that 64 million people are living with CHF worldwide.1 Approximately 8.9 million individuals in China are affected by CHF, and the prevalence continues to rise.2 In patients with CHF, common symptoms encompass dyspnea, peripheral edema, fatigue, and sleep disturbances.3 The prevalence of sleep disorders in CHF patients has been reported to range from 55.0% to 85.8%,4–8 often characterized by early awakening, difficulty in sleep initiation and maintenance, and insomnia.6,9 Inadequate quality sleep may trigger an inflammatory response and altered hormone levels, further aggravating the burden on the patient’s cardiac condition.10 This may contribute to a deterioration of health status and a diminished quality of life.11 A study showed that sleep efficiency was also associated with lower self-care maintenance.12 Furthermore, difficulty in falling asleep and early rising serves an essential function in the maintenance of cognitive health.13 Therefore, it is necessary to investigate the different sleep patterns of CHF patients and their relevant factors to decrease the underlying health hazards.
Several studies have delved into the sleep characteristics of CHF patients. The cross-sectional study conducted by Esnaasharieh et al6 revealed that patients with CHF exhibited shorter sleep duration and more frequent sleep disorders. Wang et al,14 on the other hand, reported low sleep efficiency and short nighttime sleep duration in patients with CHF. Javadi et al15 observed a significant prolongation of sleep latency in patients with CHF. Furthermore, some socio-demographic characteristics such as gender, education level, monthly income, occupational status,16 number of heart failure (HF) hospitalizations in the past year, number of HF medications, and NYHA classification are correlates of sleep in patients with CHF.4,6 In particular, Xiong et al4 have shown that fear of progression (FoP) accounts for 9.1% of the variance in poor sleep quality independently. However, the above studies have predominantly concentrated on the overall sleep quality of patients but were unable to reveal the diverse sleep patterns among different patients due to individual heterogeneity. Consequently, this makes it challenging for healthcare providers to implement precise and effective sleep management for CHF patients with distinct sleep patterns.
Currently, assessment tools for sleep disorders are categorized between objective assessment tools that are monitored using instrumentation and subjective assessment tools that are self-reported by the individual. Objective assessment tools, such as polysomnography (PSG) and actigraphy, are generally limited in their application among patients with CHF due to factors such as high cost, complexity, and stringent requirements for environmental and equipment settings.17,18 As compared to objective assessment methods, subjective assessment tools, such as the Pittsburgh Sleep Quality Index(PSQI), which are low-cost and user-friendly, are extensively used in the clinic.19 Although PSQI can determine whether a patient has a sleep problem and its severity, it is not possible to identify the specific sleep patterns of CHF patients. Therefore, using the PSQI, this study explores the sleep patterns and characteristics of different CHF patients based on the individual level, aiming to provide detailed insights into the specific sleep patterns in this population.
In contrast to traditional cluster analysis, Latent Profile Analysis (LPA) is an emerging method of individual-centered statistical analysis that identifies homogeneous subgroups characterized by similar distributions, rather than merely examining overall average trends. Consequently, the present study employed LPA to identify distinct subgroups within the sleep patterns of CHF patients exhibiting diverse phenotypes and to elucidate the influencing factors associated with each subgroup. Understanding the sleep patterns of CHF patients could aid healthcare professionals in delivering a precise and personalized sleep management strategy for patients with CHF.
Materials and Methods
Participants
This study utilized a cross-sectional design. A convenience sampling method was employed to recruit 290 patients with CHF hospitalized in the Department of Cardiology at the Affiliated Hospital of Yangzhou University from January to August 2024 as the study participants. The inclusion criteria were as follows: ① a physician’s diagnosis of HF; ② a stable condition; ③ age ≥ 18 years; ④ New York Heart Association (NYHA) class II–IV; ⑤ ability to understand questionnaire content; ⑥ provision of informed consent to voluntarily study participation. The exclusion criteria comprised: ① the presence of comorbid psychiatric disorders or cognitive dysfunction; ② a combination of other serious diseases and malignant tumors; ③ visual and hearing impairments. According to the requirements of the regression analysis model in G*Power 3.1, the medium effect size of 0.15, the alpha of 0.05, and the test efficacy of 0.95.20 A maximum of 21 predictor variables was included in this study, accounting for a potential 10% invalidated questionnaires. The resulting calculated sample size was at least 252 participants.
Measures
General Information Questionnaire
Use a general information questionnaire designed jointly by the researcher and members of the subject team based on a thorough reading of the literature. It included patients’ sociodemographic data: gender, age, education level, occupation, monthly income, caregiver and disease-related data: number of comorbidities, HF hospitalizations in the last year, number of medications, mean hospital duration, NYHA cardiac classification, and duration of HF.
The Pittsburgh Sleep Quality Index
The sleep quality was measured by the Pittsburgh Sleep Quality Index (PSQI). The PSQI was compiled by Buysse et al19 and Chineseized by Liu et al.21 The scale includes 19 items in seven dimensions: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, use of sleep medication, and daytime dysfunction, of which one item is not involved in the scoring. All dimensions were summed to obtain the total PSQI scale, ranging from 0 to 21 points, with higher scores indicating poorer sleep quality. In this study, a cutoff score of 7 was used, with scores above 7 suggesting the presence of a sleep disorder.21 The Cronbach’s alpha in this study was 0.773.
The Fear of Progression Questionnaire-Short Form
FoP was measured using the Fear of Progression Questionnaire-Short Form (FoP-Q-SF), which was simplified by Mehnert et al22 based on the original Fear of Progression Questionnaire (FoP-Q) and then simplified by Wu et al23 The scale consists of 12 entries in 2 dimensions: physical health and social family, and is scored on a 5-point Likert scale from “never” to “always”, with a total score range of 12–60 points. The higher the score, the more severe the fear, and 34 is the critical level. The Cronbach’s alpha coefficient was 0.838 in this study.
Data Collection
The investigators strictly followed the inclusion and exclusion criteria to select matched CHF patients. The investigators obtained documented informed consent from participants after thoroughly explaining the study’s objectives, procedures, and privacy protection statement. Patients completed the questionnaire questions independently, with the investigators providing clarification only upon request, thus not interfering with the answering process. When the patient is unable to answer the questionnaire independently, the investigators will dictate the questionnaire questions one-on-one without guiding questions and check the answers strictly according to the patient’s answers. The questionnaires were checked on-site after collection to ensure the completion and quality of the questionnaires.
Statistical Analysis
Descriptive statistics were analyzed using SPSS version 25.0. Kolmogorov–Smirnov (K-S) was used to test data normality. Continuous data were described by the means ± SD and categorical data were described by frequency (percentage). Group comparisons were performed using the chi-square test, Fisher’s exact test, and analysis of variance (ANOVA). We used boxplots via R version 4.4.1 to show differences in total PSQI scores by independent variable between potential classes.
In this study, the mean scores of the seven dimensions of the PSQI were used as exogenous variables for LPA using Mplus version 8.3. Starting with the assumption of a potential category of 1, the number of categories from 1 to 5 were sequentially selected for model fitting. The selection of the best model was a combination of model fitness evaluation metrics, model comparison metrics, and clinical realities. The model fitness evaluation metrics consist of the Akaike information criterion (AIC), Bayesian information criterion (BIC), and sample-size-adjusted Bayesian information criterion (aBIC). Lower values of AIC, BIC, and aBIC indicate a more favorable fit of the model. In addition, entropy is used to measure the accuracy of the model classification. Entropy ranges from 0 to 1, with values closer to 1 indicating more accurate classification and ≥ 0.8 suggesting a more satisfactory model fit. The comparative fit of various model categories was evaluated using the Lo-Mendell-Rubin Adjusted Likelihood Ratio Test (LMR) and the Bootstrap Likelihood Ratio Test (BLRT). Achieving statistical significance (P < 0.05) indicates that the model with k categories is significantly superior to the model with k-1 categories.
Multivariate logistic regression was applied with the categorical results of sleep patterns as the dependent variable and the variables with statistically significant differences in the between-group comparisons as the independent variables. P < 0.05 represents a statistically significant difference.
Results
Participants Characteristics
In the present study, a total of 312 patients were contacted, and 7 were rejected. An additional 15 questionnaires exhibiting monotonous responses were excluded, resulting in a final valid sample size of 290, yielding a response rate of 92.95%. Among the 290 participants with CHF in this study, the mean age was 73.84 (SD = 11.41) years. There were 136 males (46.9%) and 154 females (53.1%). FoP-Q-SF scale score was 29.68 (SD = 7.20). PSQI score was 12.00 (SD = 3.95). The socio-demographic characteristics and disease-related information of the CHF patients are shown in Table 1.
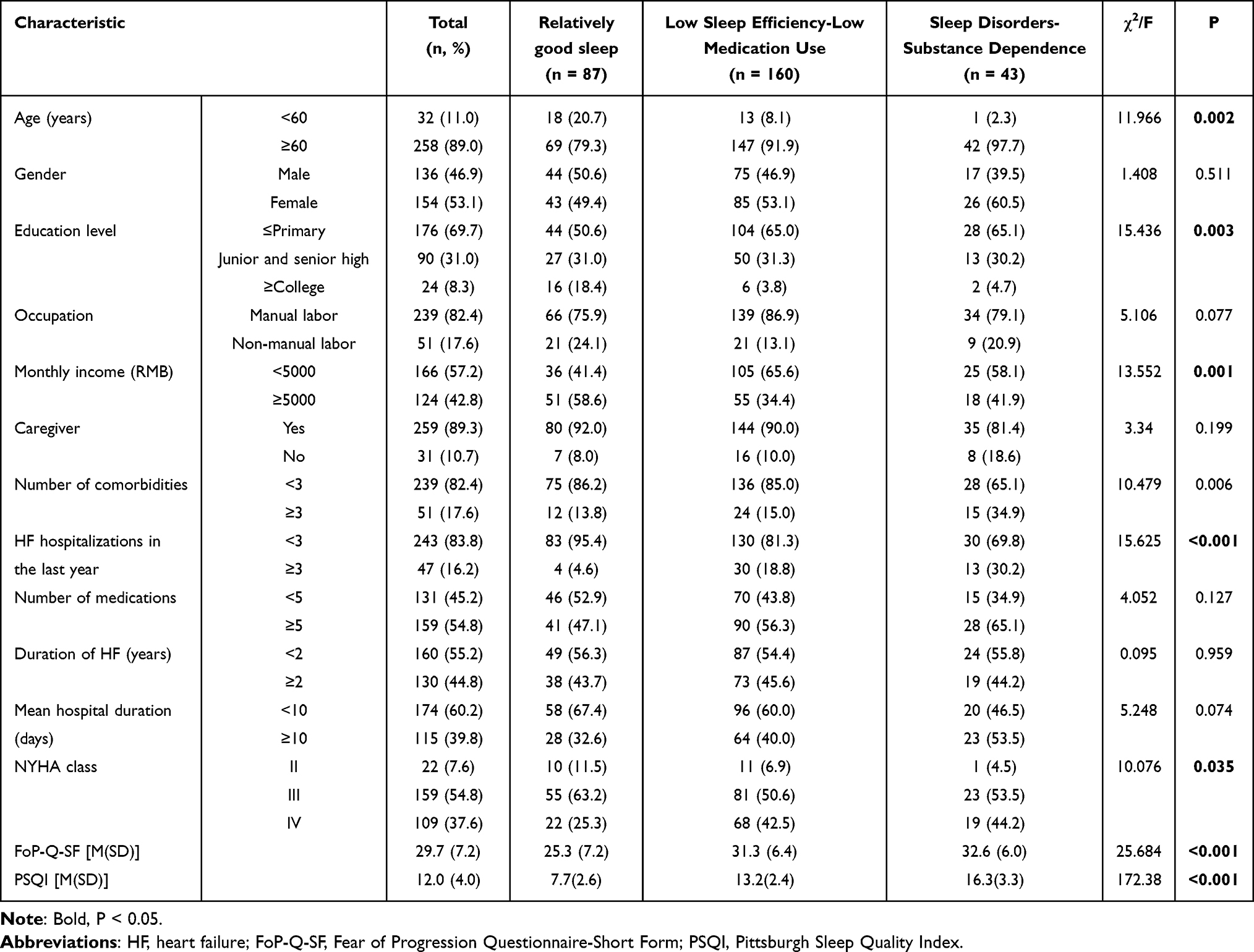 |
Table 1 General Data and Univariate Analysis of Potential Profiles of Sleep Characteristics in Patients with CHF |
Latent Classes and Naming of Sleep Patterns
In this study, latent class models of sleep patterns were analyzed sequentially for the number of classes 1–5, as shown in Table 2. As the number of classes increases sequentially from 1 to 5, AIC and aBIC gradually decrease, and the rate of decrease begins to plateau at the 3-class, suggesting that the model fit improves progressively. The BIC gradually decreased from 1-class to 4-class and began to increase slightly in 5-class, indicating a better model fit for 4-class. However, the LMR for 4-class was not statistically significant (P > 0.05), indicating that there was no significant improvement in the quality of the model fit when increasing from 3-class to 4-class. In addition, the entropy is all higher than 0.9 from 3-class onwards with a gradually increasing trend, indicating a potential risk of overfitting and decreasing clinical interpretability due to increased model complexity. Compared to 4-class, the sample exhibited a more uniform distribution across categories in 3-class, and both LMR and BLRT yielded statistically significant results (P < 0.05). For these reasons, 3-class was finally chosen as the optimal model, considering the potential overfitting and model simplicity.
 |
Table 2 Fit Indicators for Potential Profile Model |
Drawing a model diagram of the latent class model of sleep patterns for the 3-class model in Figure 1. Class 1 comprised 30.3% (n = 87) of the sample and exhibited the lowest mean PSQI scores across all dimensions compared to the other two classes; hence, it was designated as “relatively good sleep”. Class 2, comprising 54.9% (n = 160) of the sample, had the highest scores on the dimensions of sleep efficiency and sleep disorders and comparatively lower scores on the dimension of use of sleep medication. Consequently, this class was designated as “low sleep efficiency-low medication use”. The proportion of patients in class 3 was 14.8% (n = 43), exhibiting high scores on all dimensions, indicating a broad spectrum of sleep disturbances and a significant reliance on sleep medication. Consequently, this class was designated the “sleep disorders-substance dependence”. The differences in PSQI scores for all 3 classes were significant (P < 0.001), and post hoc comparative analyses showed that PSQI scores were Class 1 < Class 2 < Class 3, as shown in Table 1.
 |
Figure 1 Characteristic distribution of three latent classes of sleep patterns in patients with CHF. This figure shows the differences in sleep characteristics on the PSQI among CHF patients in the subgroups of the 3 classes of sleep patterns. Class 1 had the lowest scores on all dimensions indicative of superior sleep quality compared to Class 2 and 3. Class 2 demonstrated lower overall PSQI scores but had poorer sleep efficiency and more pronounced sleep disturbances compared to Class 3. |
Univariate Analysis of Latent Classes of Sleep Patterns in Patients with CHF
The results of the univariate analysis of the three sleep patterns classes showed statistically significant differences (P < 0.05) in age, education level, monthly income, number of comorbidities, HF hospitalizations in the last year, NYHA classification, and FoP-Q-SF scale scores, as shown in Table 1. In addition, the results of differences in PSQI scores for the independent variables between potential classes see Supplementary Figures S1–S13, where there were significant differences in total PSQI scores between potential classes for age and FoP (see Supplementary Figures S1 and S13).
Multifactorial Analysis of Latent Classes of Sleep Patterns in Patients with CHF
The covariance diagnostics showed that the variance inflation factor values of the independent variables ranged from 1.022 to 1.291 and the tolerances ranged from 0.774 to 0.978, indicating that there was no serious multicollinearity among the independent variables. Multivariate logistic regression analysis was performed with the three latent classes as the dependent variables, Class 1, labeled “relatively good sleep”, as the reference class, and the variables with significant differences in the univariate analysis of variance as the independent variables. Transform the categorical independent variables into dummy variables. The values assigned for the respective variables are shown in Table 3. The results of the multiple logistic regression are shown in Table 4. The results showed that patients with higher FoP-Q-SF scores (OR = 1.148, P < 0.001; OR = 1.198, P < 0.001), age ≥ 60 years (OR = 3.372, P = 0.023; OR = 12.189, P = 0.029), and HF hospitalizations in the last year ≥ 3 (OR = 3.367, P = 0.048; OR = 5.478, P =0.013) were more likely to be classified into Class 2 and Class 3. Patients with monthly income ≥ 5000 RMB (OR = 0.427, P = 0.010) had a lower likelihood of being attributed to Class 2 and a higher likelihood of being attributed to Class 1. Patients with the number of comorbidities ≥ 3 (OR = 3.055, P = 0.031) had a greater probability of being classified as Class 3 compared with Class 1.
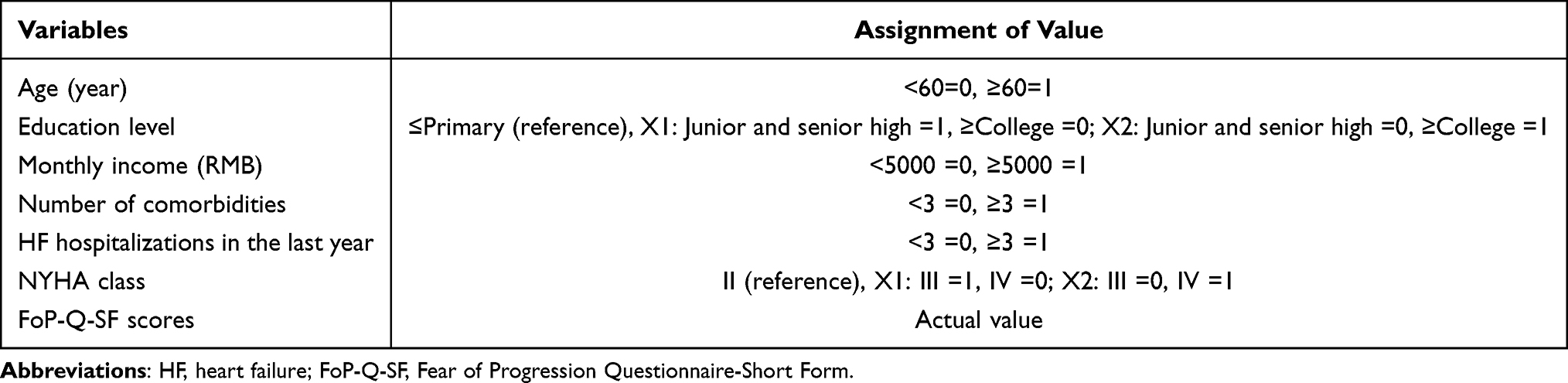 |
Table 3 Assignment Table for Multifactorial Analysis of Latent Classes of Sleep Patterns in Patients with CHF |
 |
Table 4 Multifactorial Analysis of Latent Classes of Sleep Patterns in Patients with CHF |
Discussion
To the best of our knowledge, this study is the first to identify the sleep patterns of CHF patients with the latent class method. Sleep patterns of CHF patients exhibited three subgroups: relatively good sleep, low sleep efficiency-low medication use, and sleep disorders-substance dependence. Factors affecting sleep characteristics included age, monthly income, number of comorbidities, HF hospitalizations in the last year, and FoP.
Subgroups of Sleep Patterns in CHF Patients
The findings of this study indicated that the relatively good sleep group comprised 30.3% of the sample, and the sleep quality within this group was comparatively favorable. This distinction may be attributed to the higher education level and stable condition of patients within this group. Patients demonstrated good self-care abilities, which enabled them to effectively manage their disease and control symptoms, resulting in less compromised sleep quality.24 Practitioners should encourage this group of patients to continue to maintain a healthy lifestyle and self-management program, thereby consolidating and further enhancing sleep quality.
The low sleep efficiency-low medication use group comprised 54.9% of patients, and the overall sleep quality of this group was better than that of patients in the sleep disorder-substance dependence group, but it had the lowest sleep efficiency and the most severe sleep disorders. It may be because patients in this category had more NYHA class III and IV patients with unfavorable health status and clinical symptoms.25 Sleep-disordered breathing (SDB) is one of the most common sleep disorders in patients with CHF and is associated not only with the progression of HF but also with reduced sleep quality and efficiency.17,26 The severity and persistence of sleep disturbances can disrupt the maintenance and continuity of sleep, ultimately impairing sleep efficiency.27,28 This is consistent with the results of Türoff et al17 using PSG. In addition, this group of patients had the lowest utilization of hypnotic drugs, and the reasons for this may be analyzed concerning drug literacy and medication adherence. The misunderstanding of hypnotic drugs caused the general low willingness of patients to take hypnotic drugs.29 Brief behavioral treatment is effective in improving sleep efficiency in patients with CHF.30 In addition, the cautious use of short-term, low-dose medication is advised, with monitoring of medication adherence and side effects. Adequate explanation of medication use is also recommended to minimize misunderstanding and anxiety.
The sleep disorder-substance dependence group, comprising 14.8% of the patient sample, was distinguished by disrupted multidimensional sleep patterns, severe impairment of daytime functioning, and elevated use of hypnotic medications. While hypnotics assist patients in falling asleep, prolonged usage may negatively affect their daytime functioning and disease management.31,32 Studies have indicated that long-term use of hypnotic drugs can disrupt sleep structure, such as difficulties in maintaining sleep and daytime sleepiness.33,34 Long-term use of benzodiazepines is associated with an increased risk of readmission.32 Interventions that rely on medication should be lessened for this group. Cognitive behavioral therapy for insomnia, which includes sleep hygiene education, cognitive treatment, and stimulus control, can promote the transition to healthy sleep patterns in patients.
Factors Influencing Subgroups of Sleep Patterns
The results of this present study demonstrated that patients with CHF aged < 60 years and HF hospitalizations in the last year < 3 had a high probability of being attributed to the relatively good sleep group compared to the low sleep efficiency-low medication use group and the sleep disorders-substance dependence group. These results are consistent with the studies conducted by He et al35 and Javadi et al,15 yet they contrast with those reported by Wang et al.14 This discrepancy may be attributed to variations in the sample demographics and clinical profiles. Results from Supplementary Figure S1 suggest that older patients could experience poorer sleep quality. Sleep patterns and structure change with age, and the presence of disease can further exacerbate these changes.36 Consequently, sleep problems such as decreased sleep efficiency and nighttime awakenings are more likely to manifest.37 In addition, fewer hospitalizations mean that HF is relatively well controlled and that patients can reduce their symptom burden through effective self-management, which in turn contributes to better sleep quality. Second, the environmental and medical practices of hospitalization, for instance, are also likely to cause sleep disruption and reduced sleep quality.38 The study by Edmiston et al39 also reported that CHF patients exhibited improved sleep quality post-discharge compared to their in-hospital stay. Consequently, healthcare providers should pay attention to sleep problems in elderly patients and implement strategies to enhance patient sleep and recovery during hospitalization, such as minimizing noise levels, optimizing lighting conditions, and centralizing treatment schedules. Additionally, intensive education on home self-management and sleep hygiene practices should be provided to CHF patients before discharge.
The findings of the present study showed that patients with lower FoP had a greater probability of belonging to the relatively good sleep group, which is consistent with the findings of the previous study.4 FoP is a common psychological response during the illness adaptation process. This adaptive mental state, when dysregulated, may lead to autonomic activation and imbalanced secretion of stress hormones such as cortisol, which can disrupt sleep quality.40 Furthermore, building on a comprehensive psychophysiological model of insomnia, persistent fear, and anxiety may result in cognitive hyperactivity that disrupts normal sleep patterns and the frequency of awakenings.41 Healthcare providers should promptly identify patients’ fears, facilitate the expression of their concerns and needs through the establishment of a trusting relationship, correct misconceptions about the disease, alleviate the FoP, and enhance their sleep quality.
The findings from this study indicated that patients with a monthly income of <5000 RMB had a greater probability of being categorized as a low sleep efficiency-low medication use group, which is in line with the research conducted by Chen.16 It is plausible that prolonged treatment and management may lead to significant financial strain for the patients, thereby potentially imposing a psychological burden that influences mood and sleep quality. Patients with lower monthly incomes may have inadequate access to quality medical care and may be less likely to utilize hypnotic medications for alleviating sleep disturbances, ultimately leading to exacerbated sleep problems.42 Therefore, healthcare professionals are counseled to consider the financial constraints of patients when choosing treatment options and to select affordable and effective treatment options that are within the patient’s financial capacity.
Moreover, the present study found that patients with ≥ 3 comorbidities had a greater likelihood of being classified as the sleep disorders-substance dependence group, which is in line with the results of the study by Javadi et al.15 However, this relationship was not significant in Souza’s findings.28 This may be due to the fact that the study only explored the overall sleep quality of CHF patients, which emphasizes the importance of assessing patients’ sleep patterns. An increase in the number of comorbidities implies a deterioration in the patient’s overall health, especially in the context of respiratory comorbidities. Patients may experience nocturnal exacerbation of dyspnea and increased nocturnal awakenings due to cardiopulmonary co-morbidities.43 The results of Ahmed et al44 also found that decreased cardiorespiratory fitness was associated with reduced sleep efficiency and difficulty falling asleep after awakening at night. Furthermore, patients are more likely to have sleep problems due to somatic symptoms, increasing the need for hypnotic drugs, which can cause other sleep issues as a side effect of long-term usage.45 Accordingly, healthcare providers should actively assess and manage patient comorbidities through a multidisciplinary team, including monitoring the patient’s functional status, metabolic health, and psychological status and reducing the use of medications that induce sleep disturbances or lead to polypharmacy-related adverse reactions.
Limitations and Prospects of This Study
Several limitations should be considered when interpreting the results of this study. First, the naming of sleep patterns in this study was based on the dimensional characteristics of the PSQI scale, and the accuracy and reliability need to be further verified in the future. Secondly, this present study is a cross-sectional study and causality cannot be confirmed due to the lack of longitudinal data. In addition, other potential confounding factors, such as the use of medications that affect sleep, may also affect patients’ sleep patterns, which were not fully considered in this study. Future longitudinal studies could be designed to observe the dynamics of sleep patterns with time in patients with CHF and assess possible confounders to determine the optimal time for intervention. Furthermore, the sleep assessment of CHF patients in this study was based exclusively on their subjective reports of the PSQI, which lacked the support of objective parameters to cover all aspects of sleep problems. To improve the rigor and validity of the findings, future studies should consider integrating the results of subjective and objective measures, such as PSG, to provide a more comprehensive analysis of sleep patterns. Finally, the sample was drawn from a single region, limiting the broad applicability of the findings. Future research should broaden the source and number of the center of the sample to improve the generalizability of the findings.
This study identified distinct three sleep patterns among patients with CHF, and this knowledge is critical for developing targeted interventions that address the specific sleep needs of patients with CHF. Healthcare professionals further implement targeted intervention programs by identifying patients at high risk for adverse sleep patterns. Pharmacologic and non-pharmacologic treatment programs may be suitable for patients with different sleep patterns, and thus integrating them into a clinical sleep management strategy may be beneficial to the patient’s sleep quality to a large extent.
Conclusion
The present study found that there was heterogeneity in the sleep quality of CHF patients, which could be classified into relatively good sleep group, low sleep efficiency-low medication use group, and sleep disorders-substance dependence group. Sleep patterns were affected by age, HF hospitalizations in the last year, monthly income, number of comorbidities, and FoP. Healthcare providers should prioritize the identification of distinct sleep typologies among patients with CHF and tailor interventions accordingly.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, K.G., upon reasonable request.
Ethics Approval and Informed Consent
The authors affirm that this present study follows the ethical principles outlined in the Declaration of Helsinki. Ethical approval for this study was granted by the Ethics Review Committee of the School of Nursing, School of Public Health, Yangzhou University (YZUHL20230052).
Author Contributions
Yan Li: writing - original draft, methodology, conceptualization, formal analysis, investigation, and writing-review and editing. Jiamin Li: formal analysis, project administration, and investigation. Jingwen Qin: conceptualization, methodology, and resources. Sixin Zhou: investigation and visualization. Kaizheng Gong: methodology, conceptualization, writing - review and editing, and supervision. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Jiangsu Provincial Medical Key Discipline Cultivation Unit (JSDW202251), the Yangzhou Medical Key Discipline Cultivation (YZYXZDXK-09), and the Yangzhou Basic Research Program (Joint Special Project, 2024-01-04).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lippi G, Sanchis-Gomar F. Global epidemiology and future trends of heart failure. AME Med J. 2020;5:15. doi:10.21037/amj.2020.03.03
2. Liu M, He X, Yang X, Wang Z. Interpretation of report on cardiovascular health and diseases in China 2023. J Clin Cardiol. 2024;40(8):599–616.
3. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
4. Xiong J, Qin J, Gong K. Association between fear of progression and sleep quality in patients with chronic heart failure: a cross‐sectional study. J Adv Nurs. 2023;79(8):3082–3091. doi:10.1111/jan.15657
5. Polanka BM, Yanek LR, Hays AG, et al. The association of multidimensional sleep health with adiposity in heart failure with preserved ejection fraction. Heart Lung. 2023;58:144–151. doi:10.1016/j.hrtlng.2022.12.005
6. Esnaasharieh F, Dehghan M, Mangolian Shahrbabaki P. The relationship between sleep quality and physical activity among patients with heart failure: a cross-sectional study. BMC Sports Sci Med Rehabil. 2022;14(1):20. doi:10.1186/s13102-022-00415-3
7. Batool SM, Shafqat A, Khan MF, Zubair UB, Ali SA, Zubair HB. Quality of sleep among the patients of congestive cardiac failure and factors associated with poor sleep quality. Med Forum. 2020;31(3):65–68.
8. Jorge-Samitier P, Durante A, Gea-Caballero V, Antón-Solanas I, Fernández-Rodrigo MT, Juárez-Vela R. Sleep quality in patients with heart failure in the Spanish population: a cross-sectional study. Int J Environ Res Public Health. 2020;17(21):7772. doi:10.3390/ijerph17217772
9. Cimluang J, Aungsuroch Y, Jitpanya C. Descriptors of insomnia among patients with heart failure. J Med Assoc Thai. 2017;100(4):403–409.
10. Mahmood A, Ray M, Dobalian A, Ward KD, Ahn S. Insomnia symptoms and incident heart failure: a population-based cohort study. Eur Heart J. 2021;42(40):4169–4176. doi:10.1093/eurheartj/ehab500
11. Ma X, Wang M, Xu W, et al. The influence of healthy lifestyle on the risk of re-hospitalization in patients with chronic heart failure in Qinghai-Tibet Plateau. Chin J Nurs. 2023;58(19):2373–2379.
12. Spedale V, Fabrizi D, Rebora P, et al. The association between self-reported sleep quality and self-care in adults with heart failure. J Cardiovasc Nurs. 2023;38(3):E98–E109. doi:10.1097/JCN.0000000000000929
13. Gharzeddine R, Yu G, McCarthy MM, Dickson VV. Associations of insomnia symptoms with cognition in persons with heart failure. West J Nurs Res. 2021;43(12):1105–1117. doi:10.1177/0193945920988840
14. Wang T, Lee S, Tsay S, Tung H. Factors influencing heart failure patients’ sleep quality. J Adv Nurs. 2010;66(8):1730–1740. doi:10.1111/j.1365-2648.2010.05342.x
15. Javadi N, Darvishpour A, Mehrdad N, Lakeh NM. Survey of sleep status and its related factors among hospitalized patients with heart failure. J Tehran Heart Cent. 2015;10(1):9–17.
16. Chen X. Research on the Status of Sleep Quality, Anxiety and Depression in Patients With Chronic Heart Failure in Changsha. Hunan Normal University; 2019.
17. Türoff A, Thiem U, Fox H, et al. Sleep duration and quality in heart failure patients. Sleep Breath. 2017;21(4):919–927. doi:10.1007/s11325-017-1501-x
18. Buendia R, Karpefors M, Folkvaljon F, et al. Wearable sensors to monitor physical activity in heart failure clinical trials: state-of-the-art review. J Card Fail. 2024;30(5):703–716. doi:10.1016/j.cardfail.2024.01.016
19. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
20. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
21. Liu X, Tang M, Hu L, et al. Reliability and validity of the Pittsburgh Sleep Quality Index. Chin J Psychiatry. 1996;29(2):103–107.
22. Mehnert A, Herschbach P, Berg P, Henrich G, Koch U. Progredienzangst bei Brustkrebspatientinnen - Validierung der Kurzform des progredienzangstfragebogens PA-F-KF/ Fear of progression in breast cancer patients – validation of the short form of the fear of progression questionnaire (FoP-Q-SF). Z Psychosom Med Psychother. 2006;52(3):274–288. doi:10.13109/zptm.2006.52.3.274
23. Wu Q, Ye Z, Li L, Liu P. Reliability and validity of Chinese version of fear of progression questionnaire-short form for cancer patients. Chin J Nurs. 2015;50(12):1515–1519.
24. Spedale V, Luciani M, Attanasio A, et al. Association between sleep quality and self-care in adults with heart failure: a systematic review. Eur J Cardiovasc Nurs. 2021;20(3):192–201. doi:10.1177/1474515120941368
25. Gharaibeh B, Al-Absi I, Abuhammad S, Gharaibeh M, Jarrah M. Sleep quality among different classes of heart failure patients in Jordan: a STROBE compliant cross-sectional study. Medicine. 2022;101(48):e32069. doi:10.1097/MD.0000000000032069
26. Oldenburg O, Lamp B, Faber L, Teschler H, Horstkotte D, Töpfer V. Sleep‐disordered breathing in patients with symptomatic heart failure A contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail. 2007;9(3):251–257. doi:10.1016/j.ejheart.2006.08.003
27. Javaheri S, Germany R. Sleep and breathing disorders in heart failure. Handb Clin Neurol. 2022;189:295–307. doi:10.1016/B978-0-323-91532-8.00009-4
28. de Souza JP, de Lima DFS, Leadebal ODCP, et al. Sleep quality of patients with heart failure and associated factors. Rev Bras Enferm. 2024;77(6). doi:10.1590/0034-7167-2024-0244
29. Cheng L, Zheng F, Hui M, Zhong Z. Influencing factors of home medication safety in patients with chronic heart failure: a qualitative study. Chin J Nurs. 2024;59(14):1713–1718.
30. Harris KM, Schiele SE, Emery CF. Pilot randomized trial of brief behavioral treatment for insomnia in patients with heart failure. Heart Lung. 2019;48(5):373–380. doi:10.1016/j.hrtlng.2019.06.003
31. Andrews LK, Coviello J, Hurley E, Rose L, Redeker NS. “I’d eat a bucket of nails if you told me it would help me sleep”: Perceptions of insomnia and its treatment in patients with stable heart failure. Heart Lung. 2013;42(5):339–345. doi:10.1016/j.hrtlng.2013.05.003
32. Sato Y, Yoshihisa A, Hotsuki Y, et al. Associations of benzodiazepine with adverse prognosis in heart failure patients with insomnia. J Am Heart Assoc. 2020;9(7):e013982. doi:10.1161/JAHA.119.013982
33. Choi NG, DiNitto DM, Marti CN, Choi BY. Too little sleep and too much sleep among older adults: associations with self‐reported sleep medication use, sleep quality and healthcare utilization. Geriatr Gerontol Int. 2017;17(4):545–553. doi:10.1111/ggi.12749
34. Conley S, Feder SL, Jeon S, Redeker NS. Daytime and nighttime sleep characteristics and pain among adults with stable heart failure. J Cardiovasc Nurs. 2019;34(5):390–398. doi:10.1097/JCN.0000000000000593
35. He D, Pan M. Serial multiple mediators in the relationship between symptom burden and sleep quality among patients with heart failure. Jpn J Nurs Sci. 2022;19(4):e12489. doi:10.1111/jjns.12489
36. Patel D, Steinberg J, Patel P. Insomnia in the elderly: a review. J Clin Sleep Med. 2018;14(06):1017–1024. doi:10.5664/jcsm.7172
37. Zuurbier LA, Luik AI, Leening MJG, et al. Associations of heart failure with sleep quality: the Rotterdam Study. J Clin Sleep Med. 2015;11(02):117–121. doi:10.5664/jcsm.4454
38. Koshy K, Gibney M, O’Driscoll DM, Ogeil RP, Young AC. Factors affecting sleep quality in hospitalised patients. Sleep Breath. 2024;28(6):2737–2740. doi:10.1007/s11325-024-03144-8
39. Edmiston EA, Hardin HK, Dolansky MA. Sleep quality in the advanced heart failure ICU. Clin Nurs Res. 2023;32(4):691–698. doi:10.1177/10547738231159045
40. Redeker NS, Conley S, Anderson G, et al. Effects of cognitive behavioral therapy for insomnia on sleep, symptoms, stress, and autonomic function among patients with heart failure. Behav Sleep Med. 2020;18(2):190–202. doi:10.1080/15402002.2018.1546709
41. Espie CA. Insomnia: conceptual issues in the development, persistence, and treatment of sleep disorder in adults. Annu Rev Psychol. 2002;53(1):215–243. doi:10.1146/annurev.psych.53.100901.135243
42. Conley S, Jeon S, Breazeale S, et al. Symptom cluster profiles among adults with insomnia and heart failure. Behav Sleep Med. 2023;21(2):150–161. doi:10.1080/15402002.2022.2060226
43. Benes J, Kotrc M, Jarolim P, et al. The effect of three major co‐morbidities on quality of life and outcome of patients with heart failure with reduced ejection fraction. ESC Heart Fail. 2021;8(2):1417–1426. doi:10.1002/ehf2.13227
44. Ahmed SI, Jonathan K, Billingsley H, et al. Reduced sleep quality is associated with worse cardiorespiratory fitness in heart failure with preserved ejection fraction. J Card Fail. 2023;29(4):592. doi:10.1016/j.cardfail.2022.10.115
45. Tanielian M, Antoun J, Sidani M, et al. Sleep pattern and predictors of daily versus as-needed hypnotics use in middle-aged and older adults with insomnia. BMC Prim Care. 2022;23(1):98. doi:10.1186/s12875-022-01707-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Changes in Depression Among Adolescents: A Multiple-Group Latent Profile Transition Analysis
Li G, Liu J, Wen H, Shen Q
Psychology Research and Behavior Management 2023, 16:319-332
Published Date: 8 February 2023
Latent Profile Analysis of Medication Beliefs in Patients with Type 2 Diabetes in the Hospital-Home Transition and Comparison with Medication Adherence
Jiang S, Luo T, Zhu Z, Huang Y, Liu H, Li B, Feng S, Zeng K
Patient Preference and Adherence 2024, 18:839-853
Published Date: 16 April 2024
Latent Profile Analysis and Determinants of Marital Adjustment in Patients with Breast Cancer
Chen XF, Shen C, Gu ZF, Dong C, Zhuang Y, Lu LH, Lu P, Li YJ
Journal of Multidisciplinary Healthcare 2024, 17:5799-5809
Published Date: 5 December 2024
Heterogeneity in Health-Related Quality of Life of Patients with Aplastic Anemia: A Latent Profile Analysis
Wu G, Li X, Ren X, Huang J, Zhang X, Liang T, Sun L, Hao M, Kuang Z, Li X, Zhang Q, Xu L, Zheng Y, Xie W
Patient Preference and Adherence 2025, 19:673-684
Published Date: 19 March 2025