")
Back to Journals » Journal of Pain Research » Volume 18
The Use of Electronic Consent (eConsent) Within the Ketamine for Long-Lasting Pain Relief After Surgery (KALPAS) Multicenter Trial
Authors Doan LV , Burr J , Perez R , Martinez H, Cuevas R, Watt K, Wang J
Received 27 July 2024
Accepted for publication 4 January 2025
Published 5 February 2025 Volume 2025:18 Pages 589—595
DOI https://doi.org/10.2147/JPR.S488917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert B. Raffa
Lisa V Doan,1,2 Jeri Burr,3 Raven Perez,1,2 Hamleini Martinez,1,2 Randy Cuevas,1,2 Kevin Watt,3 Jing Wang1,2,4
1Department of Anesthesiology, Perioperative Care, and Pain Medicine, New York University Grossman School of Medicine, New York, NY, USA; 2Interdisciplinary Pain Research Program, New York University Grossman School of Medicine, New York, NY, USA; 3Department of Pediatrics, University of Utah, Salt Lake City, UT, USA; 4Department of Neuroscience and Physiology, New York University Grossman School of Medicine, New York, NY, USA
Correspondence: Lisa V Doan; Jing Wang, Department of Anesthesiology, Perioperative Care, and Pain Medicine, New York University Grossman School of Medicine, New York, NY, USA, Email [email protected]; [email protected]
Background: The informed consent process has traditionally taken place in person. The introduction of electronic consent (eConsent) has made remote consenting processes possible. Use of eConsent has increased since the COVID-19 pandemic. It has streamlined the process of consenting patients and has been shown to benefit the research study team and participants.
eConsent in the Ketamine Analgesia for Long-Lasting Pain Relief After Surgery (Kalpas) Study: The KALPAS study is a multicenter, double-blind, randomized controlled study investigating the effectiveness of ketamine in reducing chronic post-mastectomy pain in women undergoing mastectomy for oncologic indication. The study uses a two-part consent form consisting of a master consent with information applicable to all sites and site-specific information. All potential participants receive the full two-part consent form for review. When signing the eConsent, however, all potential participants are provided with a concise summary of the informed consent document, an approach not widely used by multicenter studies. eConsent has been noted to be beneficial to research staff when trying to gather informed consent from participants who live far away from the hospital, want to include their family and friends, and for researchers who can approach patients outside of their clinical appointments.
Conclusion: The ability to consent patients remotely has allowed for a flexible workflow within sites and a more patient-centric process that focuses on including loved ones in the discussion and scheduling time to speak to a principal investigator. Demand for eConsent will likely continue in the post-COVID era, and use of a concise summary can allow for a more efficient consenting process.
Keywords: electronic consent, clinical trials, informed consent, concise summary
Introduction
The concept of informed consent in medicine began in the United States after a series of landmark court cases, including one in 1914 in which patient autonomy was legally established.1 This right guarantees patients the ability to make decisions about their medical care without experiencing any pressure or added influence from their healthcare providers. Meanwhile, the concept of protections for clinical research emerged after an inquiry into Nazi war crimes during World War II. Subsequently, guidelines such as the Nuremberg Code, the Declaration of Helsinki, and the Belmont Report set forth principles for the conduct of human subject research.1 Currently, in the United States, informed consent requirements are regulated by the US Department of Health and Human Services title 45 Code of Federal Regulations (CFR) 46 and by US Food and Drug Administration (FDA) title 21 CFR 50.2,3 Generally, an informed consent document must include a statement disclosing that the study involves research, the purpose of the research, study procedures, confidentiality, voluntary participation, right to withdraw, and more. The informed consent process includes giving ample information about the study in a language that is understandable to the potential participant, providing the opportunity for the potential participant to ask any questions or address any concerns, allowing the participant to consider all options, and ensuring that the potential participant has fully comprehended the study. Once the potential participant has been well educated on the risks and benefits of the study, the researcher must obtain the participant’s signature and date on the consent form. The researcher obtaining consent must also sign and date the consent form.
The informed consent process has traditionally taken place in person, with documentation of informed consent on paper forms. However, as technology has continued to advance, so too has the consent process. Recent advancements have made it possible for the consent process to be conducted remotely and with the use of electronic consent (eConsent) and electronic signatures. Electronic signatures in the United States became legal in 2000. In 2015, the FDA proposed its first ever guideline for implementing eConsent.4 The use of remote consent procedures and eConsent has increased in recent years, especially during and after the COVID-19 pandemic.5
Studies on the use of eConsent compared to traditional paper consent showed that participants reported good usability and acceptability with eConsent and ability to hold attention more with eConsent versus paper consent. Research teams also reported benefits, including easier participant recruitment, reduced administrative burden, and streamlined document management.6–9
Here, we share our experience with the use of eConsent in a large, Phase 3, multicenter, randomized controlled trial of perioperative ketamine for prevention of chronic post-mastectomy pain, including implementation, consenting process, and benefits.
The Ketamine Analgesia for Long-Lasting Pain Relief After Surgery (KALPAS) Study
Approximately, 20% of postoperative patients develop chronic post-surgical pain. Mastectomies have a particularly strong association with chronic post-surgical pain, and 25–60% of patients continue to experience pain more than three months after surgery.10–13 Ketamine is known to improve pain and reduce opioid use in the acute postoperative period.14 In addition, it has relatively long-lasting antidepressant and anxiolytic properties.15–18 By targeting pain and mood in the postoperative period, ketamine may be able to prevent the development of chronic post-surgical pain. The KALPAS study is a multicenter, double-blind, randomized controlled trial investigating the effectiveness of intravenous ketamine in reducing chronic post-mastectomy pain. Approximately 750 women undergoing mastectomy or prophylactic mastectomy will be randomized into one of three arms: the first arm consists of a continuous perioperative ketamine infusion (0.35mg/kg after induction, followed by 0.25mg/kg/hr infusion for up to a maximum of 6 hours intraoperatively and continued for 2 hours postoperatively); the second arm consists of a single-dose of ketamine (0.6mg/kg) administered immediately after surgery in the post-anesthesia care unit; and, lastly the third arm is placebo. The primary outcome is pain at the surgical site at three months. The KALPAS study is part of the National Institutes of Health Helping to End Addiction Long-term (HEAL) Initiative’s Pain Management Effectiveness Research Network. The study is overseen by the New York University (NYU) Grossman School of Medicine study team and the HEAL Resource Centers (HRCs), consisting of the Clinical Coordinating Resource Center (CCRC) led by the Duke Clinical Research Institute, the Data Coordinating Resource Center (DCRC) led by the University of Utah, the Statistical Coordinating Resource Center led by Johns Hopkins University, and the Recruitment Innovation Resource Center at Vanderbilt University Medical Center. The 16 participating study sites in the KALPAS study use the single Institutional Review Board (sIRB) at the University of Utah. The study is registered at ClinicalTrials.gov (Identifier NCT05037123; first posted 08/31/2021).
Consent Development Process
The study documents and research procedures for the KALPAS study were developed and finalized during the first two years of the COVID-19 pandemic, when the need for remote processes was clear and pressing. The KALPAS study utilizes the Research Electronic Data Capture (REDCap) system as the study database. REDCap provides a framework for eConsent, allowing the use of electronic informed consent forms (ICF). The Utah DCRC created a two-part consent document for use in the study, systematically gathering and generating site-specific information to include on each site’s informed consent forms. Part 1 consists of the master consent form, which outlines general study information. Part 2 consists of site-specific informed consent language, created from site staff responses to a survey sent by the DCRC. Federal policy on the protection of human subjects requires the use of key information. To meet this need, the research team developed concise key information presented at the beginning of the master consent form. This includes a clear statement that the consent is for research, and participation is voluntary. It states the purpose of the research, how long it will take, and what is expected from participants. It also includes potential risks, benefits, and other available options.19 Site-specific informed consent includes contact information of site principal investigators, institutional logos, language regarding the Certificate of Confidentiality, and language regarding Health Insurance Portability and Accountability Act (HPAA) authorization. MD Anderson, for example, is the only site that includes medical record numbers on their informed consent (Supplementary Figure 1). The resulting two-part informed consent document is provided to sites for local IRB review. During the consent development process, continued communications among the individual enrollment sites, the NYU leadership team, the CCRC, and the DCRC ensured both regulatory compliance and ease of use (see below). The eConsent process relies on current versions of the full informed consent document as well as the use of a concise summary document that lists the key information.
eConsent Process
The KALPAS study utilizes a novel eConsent approach that leverages the concise summary document of the key information. During the consent process, study participants are initially provided the full informed consent form, either electronically via an attachment per email or in a paper format during the initial approach by the study team (Figure 1). The REDCap eConsent platform, however, replicates the IRB approved concise summary document plus signature pages, which are used to capture the participant’s signature. Research staff electronically sign an attestation form. The attestation form confirms the participant’s identity has been verified and that the participant was given adequate time to review the information and opportunity to address questions and concerns. Only the concise summary document is viewed by participants in the REDCap eConsent platform, as opposed to the entire ICF previously provided to them. Potential participants can only sign the eConsent once they have confirmed they have read through the full informed consent document. The rationale for this approach is twofold. One, it supports the revised Common Rule requirement that the informed consent process must begin with a concise summary.20 Second, the concise summary is less likely to change with amendments or protocol updates throughout the study. Generally, if there are protocol revisions that affect the ICF, the concise summary is not affected and, therefore, no revisions are needed in the REDCap eConsent platform other than updating the IRB approval version date of the full informed consent. This approach offers several advantages, including increased efficiency for data managers, as the concise summary typically remains unchanged during study amendments. Additionally, it enhances the participant experience; most individuals prefer reading a brief summary over a lengthy document. Overall, this method represents a novel and efficient approach to eConsent, balancing regulatory compliance with user-friendly design while streamlining the consent process for both study teams and participants.
 |
Figure 1 eConsent Process Flowchart. Abbreviations: DOB, date of birth; ICF, informed consent form. |
Once the consent process has taken place, study participants sign the concise summary in the REDCap eConsent platform documenting their consent. Documentation includes the full ICF (unsigned) plus the concise summary, participant signature, and attestation form (electronically signed) in the REDCap eConsent platform (Supplementary Figure 2).
Ongoing Experience and Success of eConsent Across Participating Sites in the KALPAS Study
With the availability of eConsent, the KALPAS study allows for both remote and in-person recruitment processes. Thus, options include in-person discussion and hard copy signatures, in-person discussion and electronic signatures (utilizing the patient’s or research team’s electronic devices), and remote discussion and electronic signatures. As of November 26th, 2024, 724 participants have been consented for the KALPAS study (Table 1). Of these, 646 (89.2%) participants have consented with the use of electronic signatures. Whereas the majority of sites utilize the REDCap eConsent module, there are two external sites, Mayo Clinic and MD Anderson Cancer Center, which use their own alternative eConsent platforms due to institutional policy. MD Anderson Cancer Center uses its own eConsent platform which captures signatures and automatically uploads to the electronic medical record. Mayo Clinic uses its own approved method that allows patients to sign the complete informed consent document via DocuSign, which has been utilized for all 46 of its enrolled participants. Of the 78 uses of paper consent only, most were due to participant or study team preference and/or workflow. For instance, at a study site in which consent is obtained primarily during in-person office visits, logging into REDCap to access the eConsent module is cumbersome and interrupts clinic workflow; thus, paper consent is used. Higher proportions of patients who used paper consent preferred not to answer certain demographic questions such as race and ethnicity, making a comparison based on demographic characteristics a challenge. The majority of sites incorporate remote consent discussions and remote eConsent signatures. Only two uses of paper consent have been due to technical issues with the eConsent module within REDCap. The research coordinators at each site ensure that study participants are instructed on how to complete the eConsent online. User error on the participant’s end has contributed to a large portion of the issues we have encountered. This involved forgetting to enter date of birth (for subject verification purposes) or clicking the signature line expecting a box to pop up for signature. These were fixed with patient education. Aligning implementation of new consents during the study has not shown significant issues above and beyond the normal timing of IRB approval and getting the eConsent live. Even that was seamless with team communication.
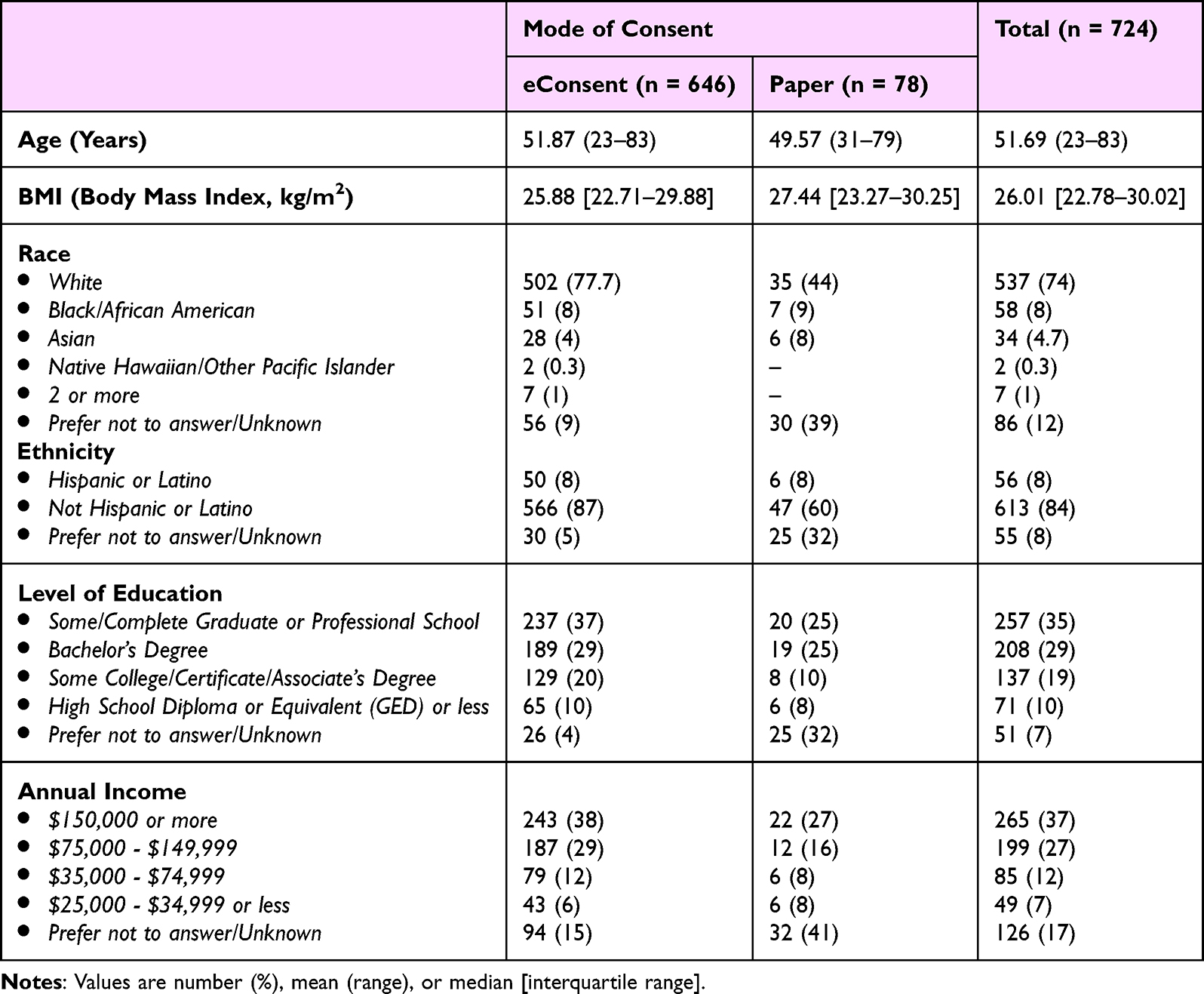 |
Table 1 Demographics of the Study Population |
After speaking with coordinators and study teams across different sites, we have identified both advantages and disadvantages of eConsent, which are listed in Table 2. For The KALPAS study, which targets a surgical study population, at some sites, potential participants have already had their visit with their surgeon prior to identification as a potential study participant. Remote recruitment processes increase possibility to contact potential participants and reduce travel-related costs.
 |
Table 2 KALPAS Study Team Experience With eConsent |
Conclusions
The availability of eConsent and the option to use remote discussion can potentially increase flexibility for recruitment processes and may provide participating sites the ability to develop site-specific workflows. Specifically, for our study, remote consenting provides a more patient-centric consent process that allows flexibility to schedule the conversation when the PI is available to answer questions and the person signing consent can include family members in the conversation. New innovative approaches to eConsent, like the concise summary method, are needed as the demand for eConsent in new studies post-COVID is on the rise. Considerations for future multicenter studies include use of the concise summary in the eConsent platform and appropriate education on eConsent use for both patients and research staff alike.
Abbreviations
CFR, Code of Federal Regulations; FDA, US Food and Drug Administration; eConsent, Electronic Consent; KALPAS, Ketamine Analgesia for Long-lasting Pain relief After Surgery; NIH, National Institutes of Health; HEAL, Helping to End Addiction Long-term; HRC, HEAL Resource Center; CCRC, Clinical Coordinating Resource Center; DCRC, Data Coordinating Resource Center; SIRB, Single Institutional Review Board; IRB, Institutional Review Board; REDCap, Research Electronic Data Capture; ICF, Informed Consent Form; NYU, New York University; COVID, Corona Virus Disease; PI, Principal Investigator.
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding
This research is supported by the National Institutes of Health through the NIH HEAL Initiative under award number UH3CA261067. Research reported in this publication is also supported by the NCATS Trial Innovation Network (TIN), under Award Numbers U24TR001608-05S3 (Clinical Coordinating Center), U24TR001597-06S1 (Data Coordinating Center), U24TR001579-06S1 (Recruitment Innovation Center), and U24TR001609 (Safety and Statistical Coordinating Center).
Disclosure
JW is a cofounder and scientific advisor for Pallas Technologies, Inc., and is an inventor of a pending US patent application of pain treatment technology. The authors report no other conflicts of interest in this work.
References
1. Bazzano LA, Durant J, Brantley PR. A modern history of informed consent and the role of key information. Ochsner J. 2021;21(1):81–85. doi:10.31486/toj.19.0105
2. Services, U.S.D.o.H.a.H. Available from: https://www.hhs.gov/ohrp/regulations-and-policy/guidance/faq/45-cfr-46/index.html#:~:text=Basic%20regulations%20governing%20the%20protection,were%20first%20published%20in%201974.
3. Administration, U.S.D.o.H.a.H.S.F.a.D. Available from: https://www.fda.gov/media/88915/download.
4. Administration, U.S.F.a.D.
5. Press, C.U. Available from: https://www.cambridge.org/core/journals/journal-of-clinical-and-translational-science/article/informed-consent-old-and-new-challenges-in-the-context-of-the-covid19-pandemic/E2493899FE1A9AE79BF1D6133823CFCF.
6. Cohen E, Byrom B, Becher A, et al. Comparative effectiveness of eConsent: systematic review. J Med Internet Res. 2023;25:e43883. doi:10.2196/43883
7. Skelton E, Drey N, Rutherford M, et al. Electronic consenting for conducting research remotely: a review of current practice and key recommendations for using e-consenting. Int J Med Inform. 2020;143:104271. doi:10.1016/j.ijmedinf.2020.104271
8. Mirza AB, Khoja AK, Ali F, et al. The use of e-consent in surgery and application to neurosurgery: a systematic review and meta-analysis. Acta Neurochir (Wien). 2023;165(11):3149–3180. doi:10.1007/s00701-023-05776-3
9. Chimonas S, Lipitz-Snyderman A, Gaffney K, et al. Electronic consent at US cancer centers: a survey of practices, challenges, and opportunities. JCO Clin Cancer Inform. 2023;7(7):e2200122. doi:10.1200/CCI.22.00122
10. Werner MU, Kongsgaard UE. I. Defining persistent post-surgical pain: is an update required? Br J Anaesth. 2014;113(1):1–4. doi:10.1093/bja/aeu012
11. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. doi:10.1016/S0140-6736(06)68700-X
12. Gewandter JS, Dworkin RH, Turk DC, et al. Research designs for proof-of-concept chronic pain clinical trials: IMMPACT recommendations. Pain. 2014;155(9):1683–1695. doi:10.1016/j.pain.2014.05.025
13. Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth. 2008;101(1):77–86. doi:10.1093/bja/aen099
14. Schwenk ES, Viscusi ER, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for acute pain management from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):456–466. doi:10.1097/AAP.0000000000000806
15. Zarate CA Jr, Singh JB, Carlson PJ, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry. 2006;63(8):856–864. doi:10.1001/archpsyc.63.8.856
16. Berman RM, Cappiello A, Anand A, et al. Antidepressant effects of ketamine in depressed patients. Biol Psychiatry. 2000;47(4):351–354. doi:10.1016/S0006-3223(99)00230-9
17. Ibrahim L, DiazGranados N, Franco-Chaves J, et al. Course of improvement in depressive symptoms to a single intravenous infusion of ketamine vs add-on riluzole: results from a 4-week, double-blind, placebo-controlled study. Neuropsychopharmacology. 2012;37(6):1526–1533. doi:10.1038/npp.2011.338
18. Diazgranados N, Ibrahim L, Brutsche NE, et al. A randomized add-on trial of an N-methyl-D-aspartate antagonist in treatment-resistant bipolar depression. Arch Gen Psychiatry. 2010;67(8):793–802. doi:10.1001/archgenpsychiatry.2010.90
19. Info, Gov. Available from: https://www.govinfo.gov/content/pkg/FR-2017-01-19/pdf/2017-01058.pdf.
20. Services, U.S.D.o.H.a.H. Available from: https://www.hhs.gov/ohrp/sachrp-committee/recommendations/attachment-c-november-13-2018/index.html.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.