")
Back to Journals » Journal of Pain Research » Volume 18
The Utilization of Ultrasound-Guided Regional Nerve Blocks in Anesthetic Management for Fracture Surgery
Authors Yi R, Li Z, Yang X, Huang T, Liu H, Zhang J
Received 19 August 2024
Accepted for publication 20 December 2024
Published 20 January 2025 Volume 2025:18 Pages 353—366
DOI https://doi.org/10.2147/JPR.S492151
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Ruofan Yi,1 Zeng Li,1 Xingjun Yang,2 Ting Huang,1 Hongjun Liu,1 Jun Zhang2
1Department of Anesthesiology, The 955th Hospital of Chinese People’s Liberation Army, Tibet, 854000, People’s Republic of China; 2Department of General Surgery, The 955th Hospital of Chinese People’s Liberation Army, Tibet, 854000, People’s Republic of China
Correspondence: Jun Zhang, Department of General Surgery, The 955th Hospital of Chinese People’s Liberation Army, No. 52, Gadong Street, Karuo District, Chamdo, Tibet, 854000, People’s Republic of China, Tel +86 0895 4820722, Email [email protected] Hongjun Liu Department of Anesthesiology, The 955th Hospital of Chinese People’s Liberation Army, No. 52, Gadong Street, Karuo District, Chamdo, Tibet, 854000, People’s Republic of China, Tel +86 0895-4820775, Email [email protected]
Abstract: Fracture surgeries are frequently accompanied by severe pain, necessitating efficacious pain management strategies to enhance postoperative recovery. Nerve block techniques, which are critical in mitigating pain, involve the targeted administration of local anesthetics to disrupt nerve signal transmission, thereby achieving significant analgesia. Traditionally, these techniques rely on anatomical landmarks and the clinician’s expertise, which can introduce variability and potential risks. The adoption of ultrasound-guided nerve blocks has increased, facilitated by advancements in imaging technology. This approach enables precise placement of anesthetics through real-time visualization of neural structures and adjacent tissues, significantly improving the accuracy and safety of the procedure. This review summarizes recent advancements in the application of ultrasound-guided nerve block techniques in fracture surgeries, particularly for rib, upper limb, thoracic, lumbar, and hip fractures. By precisely placing local anesthetics, these techniques not only improve the safety and efficiency of surgeries but also significantly reduce postoperative pain and recovery time. The widespread application of ultrasound-guided nerve blocks offers an efficient and low-side-effect anesthesia management strategy, enhancing post-surgical patient experience and recovery quality.
Keywords: ultrasound-guided nerve blocks, fracture surgery, postoperative pain management, anesthetic precision and safety
Introduction
Effective anesthetic management and analgesia are foundational to the successful execution of fracture-related surgical procedures.1 Fracture surgeries invariably involve intense pain, which, if inadequately managed, can significantly impede postoperative recovery.2 Consequently, the selection of a reliable, efficacious, and controlled anesthetic technique is pivotal in enhancing surgical outcomes. Nerve blocks, which directly interrupt pain transmission pathways, are extensively utilized in clinical settings due to their direct impact on pain perception.3
Depending on the location of the fracture, different nerve block techniques, like intercostal, sciatic, or femoral nerve blocks, are commonly used. These methods work by injecting local anesthetics near specific nerve trunks, which blocks nerve signals and provides significant pain relief.4 This approach helps manage pain during and after surgery, improves patient comfort, and supports faster recovery. However, traditional nerve block techniques often rely on anatomical landmarks and the clinician’s experience, which can lead to variability and potential risks.5
With the integration of technological advancements, ultrasound-guided methods have increasingly been adopted to enhance the precision and safety of nerve blocks.6 Ultrasound imaging facilitates real-time and detailed visualization of nerve structures, vascular formations, and adjacent tissues, thereby allowing for exact placement of local anesthetics.6 This precision reduces both the required dosage of anesthetics and the risk of complications, enhancing the overall safety profile of the procedure.7 Moreover, the consistency in analgesic effectiveness provided by ultrasound-guided techniques ensures a superior patient experience both during and following the surgical intervention.8 This review will collate recent advancements and explore the application, effectiveness, and future prospects of ultrasound-guided nerve blocks in anesthesia management for fracture surgeries.
Clavicle and Upper Limb Fractures
The brachial plexus primarily consists of the anterior branches from C5 to C8 and T1, occasionally including contributions from C4 and T2.9 With the widespread adoption of ultrasonography, new approaches and methods for continuous brachial plexus blocks (CBPB) have been developed, enhancing the traditional approaches and catheter placement techniques.10 Currently, approaches for CBPB include interscalene, supraclavicular, infraclavicular, and axillary routes, which are selected based on the anatomical course of the nerves.11 CBPB not only improves the efficacy of brachial plexus anesthesia but also offers distinct advantages in postoperative analgesia and pain management due to its precise analgesic effects, minimal systemic side effects, and the ability to improve local blood circulation through vasodilation.12 It is routinely employed for the diagnosis and treatment of acute and chronic pain, pain management in upper limb vascular reconstructions or ischemic conditions, treatment of cancer pain, and management of phantom limb syndrome in the upper extremities.13 Ultrasonography ensures accurate catheter placement, enhances the certainty of anesthesia and analgesia, and reduces the incidence of associated complications, potentially increasing patient satisfaction.14 The effectiveness of CBPB varies with the approach used, and there is a plethora of ongoing research on its methods and clinical applications.
Ultrasound-Guided Continuous Interscalene Brachial Plexus Block for Analgesia in Shoulder and Upper Humeral Surgeries
The interscalene brachial plexus block targets the upper trunk formed by C5-C6, extending to the middle and lower trunks, offering profound analgesia particularly suitable for shoulder and upper arm surgeries.15 This technique utilizes an ultrasound-guided anterolateral approach to accurately place the catheter, enhancing the efficacy and duration of analgesia beyond that provided by single-shot blocks.16 Studies have demonstrated its effectiveness not only in routine shoulder surgeries but also in specialized procedures like finger reattachment and pectoralis major tendon repairs.17
While the classic anterolateral approach remains standard, the posterior approach has gained favor for its stability and reduced risk of catheter displacement, crucial in dynamic regions.18 This approach navigates through deeper muscle layers, offering sustained analgesia with minimal risk of dislodgment.
Advanced Techniques in Upper Limb Anesthesia: Supraclavicular and Costoclavicular Blocks
The supraclavicular block and the costoclavicular approach are both effective techniques for providing anesthesia for upper limb surgeries, each with unique advantages and specific use cases. A randomized study compared the diaphragmatic and pulmonary functions following these blocks, showing that the costoclavicular approach preserves diaphragmatic function and pulmonary capacity better than the supraclavicular approach while maintaining similar efficacy.19 The costoclavicular block has also shown high success rates in pediatric populations, demonstrating excellent visualization and ease of application with minimal complications.20 Furthermore, in emergency settings, the costoclavicular block has proven to be an effective analgesic tool, providing dense, surgical anesthesia for upper extremity procedures, thereby avoiding the need for procedural sedation and reducing opioid use.21 Meta-analyses confirm the lower incidence of hemidiaphragmatic paralysis with the costoclavicular approach compared to other brachial plexus blocks, while maintaining comparable block performance parameters.22
Continuous Infraclavicular and Axillary Brachial Plexus Blocks
The infraclavicular block, axillary block, and supraclavicular block each have specific advantages and considerations for upper limb surgeries. A comparative study on ultrasound-guided infraclavicular block using bupivacaine alone versus bupivacaine combined with dexmedetomidine showed that the addition of dexmedetomidine hastened the onset and prolonged the duration of both sensory and motor blocks, providing better analgesia.23
The supraclavicular block’s effectiveness for upper limb surgeries has been enhanced by combining bupivacaine with ketamine.24 Ketamine, known for its NMDA receptor antagonism, may reduce central sensitization and inhibit pain signal transmission.25 When used as a perineural adjuvant, ketamine has been shown to improve the onset time and prolong the duration of nerve blocks, possibly by stabilizing nerve membranes and enhancing local anesthetic action through anti-inflammatory effects.24 While studies indicate these benefits, the exact mechanism of ketamine in prolonging regional anesthesia remains under investigation, and its efficacy compared to intravenous administration warrants further exploration. An observational study validated the use of the perfusion index (PI) as a reliable measure for postoperative pain assessment in patients undergoing upper limb surgeries under supraclavicular block.26 A comparison between ultrasound-guided supraclavicular and infraclavicular approaches found that the infraclavicular block had a faster onset of sensory blockade, although the block performance time was longer.27 Additionally, dexmedetomidine added to ropivacaine in supraclavicular blocks resulted in earlier onset and prolonged duration of sensory and motor blocks, enhancing postoperative analgesia.28
In conclusion, ultrasound-guided continuous interscalene brachial plexus blocks emerge as the preferred choice for shoulder and upper humeral surgeries due to their enhanced stability, especially with the posterior approach which mitigates the risk of catheter displacement (Table 1). Although the interscalene nerve block remains the gold standard for shoulder anesthesia due to its superior efficacy, the use of continuous supraclavicular brachial plexus blocks is expanding in shoulder surgeries attributed to their reduced risk of ipsilateral diaphragmatic paralysis, although they demonstrate limited efficacy in managing pain for elbow and more distal surgeries compared to continuous infraclavicular blocks. Meanwhile, continuous costoclavicular brachial plexus blocks excel in providing effective anesthesia and analgesia for elbow and distal procedures, surpassing the performance of supraclavicular, infraclavicular, and axillary approaches in terms of stability and effectiveness. The continuous axillary blocks, while easy and safe, are seeing a decline in usage due to anatomical constraints that affect their efficacy. CBPB remain a vital anesthesia and analgesia technique. Clinically, the choice of block technique and approach should be strategically selected based on the specific surgical requirements and patient conditions. Ultrasonography plays a critical role in enhancing the precision of catheter placement and block efficacy, significantly minimizing the potential for adverse effects and complications, thereby underscoring the need for broader clinical adoption and ongoing refinement in practice.
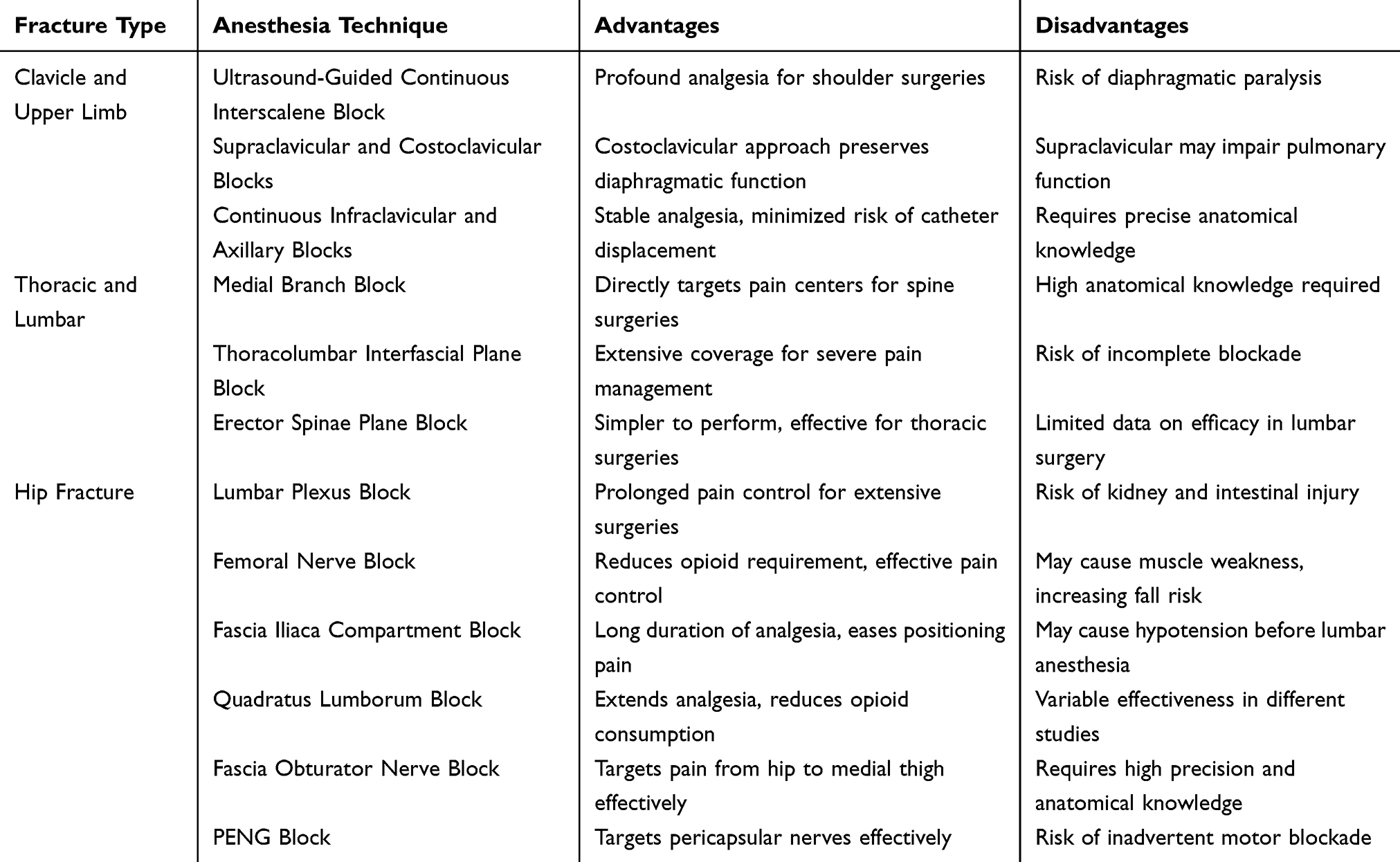 |
Table 1 Comparative Overview of Ultrasound-Guided Nerve Blocks Across Various Fracture Types |
Thoracic and Lumbar Fractures
The incidence of lumbar spine disorders, including fractures, has risen significantly in recent years, prompting the use of invasive surgeries that often lead to severe postoperative pain, impairing physiological functions and hindering early mobilization.29 To address this, a multimodal analgesia (MMA) strategy, incorporating various analgesic methods targeting different pain mechanisms, has become essential in managing acute postoperative pain effectively.30 This approach, particularly regional nerve blocks, has shown considerable success in reducing complications and facilitating quicker recovery in patients undergoing surgeries for spinal fractures (Table 1).
Medial Branch Block
The anatomical structure of the posterior branches of the spinal nerves is still under active investigation. Historically, the anatomy of these nerves was not precisely described for an extended period, and most anatomical textbooks depicted the posterior spinal nerve branches as consisting of two major subdivisions: the medial and lateral branches. Kozera et al31,32 building on a review of the literature, described the positioning and function of these branches, subdividing the posterior spinal nerve branches into posterior medial and lateral branches. Subsequently, dissections of eight cadavers from T1 to L5 confirmed that the posterior branches of the spinal nerves could consist of three primary branches: medial, lateral, and intermediate.33 The medial branch innervates the spinous muscles and the multifidus muscles, covering the area from the midline to the zygapophysial joints; the lateral branch innervates the area corresponding to the iliocostalis muscle; the intermediate branch covers the area between the medial and lateral branches, terminating at the longissimus muscle.34 The surgical treatment of lumbar spine disorders, including midline and paramedian approaches through the paraspinal muscles, may inadvertently damage or stimulate the posterior spinal nerve branches, leading to nerve root congestion, edema, and adhesion, which can result in postoperative muscle atrophy and subsequent lower back pain.35 Therefore, understanding the anatomical structure of the posterior spinal nerve branches is crucial for preserving the functionality of the paraspinal muscles. Despite ongoing debates over the anatomy of these branches, considering the distribution of thoracolumbar back muscles, the notion of three main branches in the posterior spinal nerve branches appears more plausible in practical applications.
The traction and stimulation of nerve roots during surgery can directly transmit to the pain centers, causing central pain.36 Selective blockade of the posterior spinal nerve branches at the site of injury can eliminate aseptic inflammation and interrupt pain transmission, providing effective analgesia.37 Five cases of posterior spinal nerve branch block used in lumbar spine laminectomy and internal fixation surgery involved surgical incisions positioned at the posterior midline of the L1 to L4 vertebrae.38 Under planar ultrasound guidance, patients in the prone position received 5 mL of 0.33% ropivacaine at each transverse process from T10 to L2, with five injections administered by moving the probe head or tail to change the needle direction without removing the needle from the skin, completing the injections at two skin puncture sites.39 The dosage of intravenous anesthetics and inhalation anesthetics used intraoperatively was reduced, and patients did not experience pain requiring remedial analgesia within 6 hours postoperatively; no adverse reactions associated with the blockade were observed.40 The report did not mention the impact of the blockade on postoperative analgesic medication dosage or prognosis. Considering the temporary effect of a single nerve block, a combination of local anesthetic infiltration around the surgical incision with the spinal nerve blockade can extend the effective duration of postoperative analgesia.
The clinical application of medial branch block is extensive, and apart from analgesia, it also plays a significant role in the treatment of lower back pain.41 However, the execution of medial branch block should consider the challenges of the blockade. Ultrasound-guided blocks require high anatomical knowledge from the practitioner and care should be taken to avoid injury due to the anatomical position and course of the posterior spinal nerve branches.42 For multi-segment surgeries, the demand for multiple block points increases the complexity of the procedure and the risk of infection. In contrast, direct visualization during nerve blocks appears safer, dependent on the surgeon, but concentrates local anesthetics around the nerves. No clear reports yet exist on the safe concentration of local anesthetics, and there is a risk of motor blockade from the infiltration of local anesthetics into the subarachnoid space. Further research is needed to explore the optimal dosage and minimum concentration of local anesthetics.
Thoracolumbar Interfascial Plane Block
The Thoracolumbar Interfascial Plane (TLIP) block, a novel interfascial blockade technique, has primarily been utilized in surgeries involving the lumbar and lower back regions.43 Initially reported in 2015 under ultrasound guidance, the TLIP block involves the injection of local anesthetics between the multifidus and longissimus muscles’ fascial planes, effectively blocking the posterior branches of the spinal nerves through fascial diffusion, thereby providing adequate analgesia for midline incisions in lumbar surgeries.43 In subsequent years, a series of studies demonstrated that local anesthetic injections into this interfascial plane effectively block the posterior spinal nerve branches.44,45 The bilateral TLIP block, when combined with general anesthesia, has been shown to significantly alleviate perioperative pain in patients undergoing lumbar laminoplasty, surpassing the analgesic efficacy of general anesthesia alone.46
However, the clinical application of TLIP blocks revealed challenges in accurately identifying the interfascial gap between the multifidus and longissimus muscles under ultrasound.47 This led researchers to propose a modified TLIP block, which involves ultrasound-guided injection of local anesthetics between the longissimus and iliocostalis muscles. The modified TLIP block offers several advantages, including a reduced risk of spinal cord injury by changing the needle trajectory from external to internal, and easier identification of the interfascial plane between the longissimus and iliocostalis, resulting in higher success rates of puncture.47 Subsequent studies have applied the modified TLIP block to various lumbar surgeries, such as multilevel lumbar surgery and posterior lumbar fusion, showing effective relief from static pain at 48 hours post-operation and dynamic pain at 24 hours post-operation, along with a reduction in opioid consumption at 24 hours.48 Ueshima et al reported on the successful use of combined conventional and modified TLIP blocks in surgeries, addressing the issue of incomplete blockade often encountered with a single blockade technique.49 The combined approach proved to be safer and easier to perform than the original TLIP block alone, suggesting its potential as a part of multimodal analgesic strategies for patients undergoing extensive lumbar surgeries.
While clinical data on TLIP block applications are sparse, primarily consisting of case reports with few complications related to the block reported, a retrospective study involving 175 cases noted only a single instance of hematoma with no reports of inadvertent vascular entry, infection, or other complications, underscoring its safety.50 The effectiveness of TLIP blocks largely depends on adequate diffusion of local anesthetics between the muscle fascial planes; common agents used include ropivacaine, levobupivacaine, and bupivacaine.51 Optimal volumes, concentrations, and types of local anesthetics for TLIP blocks have yet to be determined. Given its superficial injection site, the TLIP block is easy to implement and an excellent option for multimodal postoperative analgesia, particularly in patients with severe renal impairment.52 However, as a new technique, it demands high proficiency from the practitioner to accurately identify the fascial layers under ultrasound and ensure precise injection and sufficient diffusion of the anesthetic.
Erector Spinae Plane Block
The Erector Spinae Plane (ESPB) block, guided by ultrasound, represents a novel interfascial plane blockade technique that has been gaining prominence alongside the Thoracolumbar Interfascial Plane (TLIP) block.53 As the longest muscle in the back, the erector spinae lies adjacent to the spinal column’s spinous processes.54 Local anesthetics are injected deep into the erector spinae, where they can diffuse cranially and caudally through the potential spaces between muscles, effectively infiltrating and blocking both the dorsal and ventral branches of the spinal nerves.55 The use of ESPB for neuropathic pain achieved favorable outcomes and observing dye diffusion to the ventral and dorsal spinal nerve branches in dissections of fresh cadavers.56
In the years following, the clinical applications of ESPB have expanded, being employed for postoperative analgesia in various surgeries including abdominal,57 thoracic,58 and breast surgeries.59 As ESPB techniques have evolved, researchers have begun comparing ESPB with other regional nerve block techniques such as the transversus abdominis plane block for post-cholecystectomy pain management,60 and with local anesthetic infiltration around the shoulder joint for post-arthroscopy pain control.61 Randomized controlled trials have confirmed that ESPB provides more effective pain relief compared to other methods.62
There is growing clinical research on the use of ESPB for postoperative analgesia following lumbar surgery,63,64 yet extensive clinical studies are still required to explore its effectiveness comprehensively. Under ultrasound guidance, the injection of local anesthetics between the deep erector spinae and the transverse processes of the vertebrae allows for safer and more feasible observation of anesthetic spread.65,66 Compared to TLIP blocks, ESPB is simpler to perform under ultrasound as the transverse processes are easier to identify than the muscular interfascial gaps, where the spread of local anesthetics might be more restricted and the blockade range narrower.67 However, both techniques lack extensive randomized controlled trial data for post-lumbar surgery analgesia, mostly limited to case reports. Experiments comparing both techniques are warranted based on their proven benefits in managing postoperative pain.68 Furthermore, optimal protocols for the volume, concentration, and type of local anesthetics in ESPB remain undefined, necessitating extensive clinical research. There are case reports of continuous ESPB,69 but randomized controlled trials are yet to be seen; continuous ESPB may hold potential for opioid-free postoperative analgesia in the future. For patients undergoing single-segment lumbar surgeries, ESPB could potentially serve as the sole anesthetic technique, providing effective post-incisional pain relief while avoiding the incomplete blockade associated with local anesthetics and reducing medical resource waste and costs associated with general anesthesia, significantly advancing the development of patient-centered care.70
Hip Fracture
In recent years, the frequency of hip joint surgeries has steadily increased, establishing it as a common orthopedic procedure.71 A significant concern associated with these surgeries is perioperative pain, which can lead to a broad spectrum of complications, increased morbidity, and diminished overall patient satisfaction.72 This pain not only adversely affects surgical outcomes, such as intraoperative blood pressure fluctuations triggered by nociceptive stimuli but also negatively impacts long-term prognoses and the quality of life for patients.73 A prospective survey found that approximately 8% of patients were dissatisfied with the outcomes of total hip arthroplasty, with pain being the principal complaint, accounting for about 39% of all dissatisfaction factors.74
In the realm of anesthesia for hip surgeries, regional anesthesia facilitated by ultrasound-guided nerve blocks has become a recognized safe practice.75 The primary mechanism of nerve blocks is to interrupt the pathways of pain transmission and the associated vicious cycles, thereby improving blood circulation, nourishing nerves, and providing anti-inflammatory effects.76 Common nerve blocks utilized in hip surgeries include lumbar plexus block, femoral nerve block, quadratus lumborum block, obturator nerve block, and periarticular hip capsule block77 (Table 1).
Lumbar Plexus Block
The lumbar plexus, composed of the anterior branches of the T12 nerve and L1 to L4 spinal nerves embedded within the psoas major muscle, not only innervates the quadratus lumborum and iliacus muscles but also gives rise to branches such as the iliohypogastric, ilioinguinal, femoral, obturator, genitofemoral, and lateral femoral cutaneous nerves.78 These branches predominantly supply the anterior and medial aspects of the thigh, as well as the inguinal region. For lumbar plexus block (LPB), patients are typically positioned in the lateral decubitus position with the affected side up and hips and knees flexed for unilateral blocks; a prone position with a pillow under the abdomen to flatten the lumbar curvature is used for bilateral blocks. In the sagittal plane of the lumbar plexus, the ultrasound probe is placed parallel to the spine at the L3/4 spinous process level and scanned laterally.79 The psoas major muscle can be visualized in the space between adjacent transverse processes, with the lumbar plexus located deep within it. The spacing between the index, middle, and ring fingers can help locate the three transverse processes and the intermuscular septum of the psoas major, where a high-echoic region indicates the lumbar plexus and allows for measurement of the approximate distance from the skin to the nerves, thus minimizing the risk of adverse reactions and complications associated with nerve blocks.80 However, many clinicians consider this an out-of-plane technique that could potentially harm the kidneys and intestines.81 On the transverse section of the lumbar plexus, the position of the abdominal muscles is initially confirmed, then the probe is slowly moved dorsally and caudally inclined until a typical cloverleaf image comprising the L4 transverse process, psoas major, erector spinae, and quadratus lumborum is observed.82 At this point, within the posterior quarter quadrant of the psoas major, a high-echoic structure representing the lumbar plexus nerves can be seen. The probe is then stabilized, and the local anesthetic is injected 4 cm lateral to the L4 spinous process.83 LPB offers hemodynamic stability and prolonged postoperative maintenance, making it a preferred option for patients with unstable circulation.84 Compared to general anesthesia alone or epidural anesthesia, lumbar plexus nerve block has proven to be an effective method for controlling postoperative pain following hip joint reconstruction in cerebral palsy populations.85 Additionally, LPB combined with infiltration anesthesia can also reduce stress responses and postoperative pain in elderly patients undergoing hip replacement, enhancing anesthetic comfort.86 However, due to the deep placement of the lumbar plexus, the approach is prone to peritoneal injury during needle insertion and can occasionally result in unintended bilateral blocks causing epidural diffusion.87 Besides, due to the deep placement of the lumbar plexus and the requirement for relatively large volumes of local anesthetic, there is an elevated risk of local anesthetic systemic toxicity (LAST) if the anesthetic is inadvertently injected into vascular structures.88 Hence, although LPB provides effective analgesia in regional blocks for hip joint procedures, the operational risks and insufficient early postoperative mobility in patients necessitate further exploration of more effective blocking techniques.
Femoral Nerve Block
The femoral nerve, originating from the L2 to L4 nerve roots, descends between the psoas major and iliacus muscles, passing beneath the inguinal ligament into the femoral triangle.89 For ultrasound-guided femoral nerve blocks (FNB), the patient is positioned supine with the affected limb slightly externally rotated.90 The probe is placed at the midpoint of the inguinal ligament to locate a prominently pulsating artery, and the needle is inserted 1 cm laterally within the plane.91 The femoral nerve can be identified by a high-echoic shadow lateral to the femoral artery, where the local anesthetic is administered.92 FNB effectively alleviates pain while substantially reducing the need for opioid analgesics.92 Chul-Ho Kim demonstrated that FNB can prevent perioperative delirium in elderly patients with hip fractures who do not have pre-existing cognitive impairments.93 However, the blockade of the quadriceps muscles can increase the likelihood of postoperative falls, which is disadvantageous for early mobility recovery.
Fascia Iliaca Compartment Block
The iliofascial compartment represents a potential space in the inguinal region, bordered anteriorly by the iliac fascia, posteriorly by the iliacus muscle, medially by the lower lumbar and sacral vertebrae, and laterally by the inner lip of the iliac crest.94 Within this space, branches of the lumbar plexus, including the femoral nerve, the lateral femoral cutaneous nerve, and the obturator nerve, traverse. During ultrasound-guided Fascia Iliaca Compartment Block (FICB), the ultrasound probe is positioned horizontally just inferior to the inguinal ligament, lateral to the femoral artery where the broad fascia and iliac fascia appear as two distinct high-echoic lines.95 Special sonographic signs such as the “hourglass”, “bow-tie”, and “hill” help in rapidly locating the iliofascial space. The needle is inserted laterally to the thigh, extending 1 cm beyond the edge of the probe, using an in-plane technique from either the medial or lateral side of the femur, avoiding the femoral artery.96 A characteristic “pop” sensation felt twice, as the needle penetrates the fascia lata and iliac fascia, indicates entry into the iliofascial space.96 FICB can be performed via either a medial or lateral approach, with Tengchen Feng’s research on different approaches for FICB in total hip arthroplasty indicating that the medial approach provides better anesthesia, postoperative analgesia, reduced postoperative analgesic requirements, and a lower incidence of postoperative delirium compared to the lateral approach.97 In elderly patients undergoing hip replacement surgery, FICB is typically used before spinal anesthesia to alleviate the pain associated with positioning. A study investigating pre-spinal FICB found that the Visual Analogue Scale (VAS) scores decreased from 8.02 to 2.28.98 While FICB offers extended analgesia duration, it is noteworthy that it may reduce postoperative muscle strength and lead to hypotension before lumbar anesthesia.14 Additionally, studies have found that FICB can effectively reduce the incidence of early postoperative cognitive dysfunction in elderly, high-risk patients undergoing hip replacement.99 FICB not only reduces the reliance on opioid analgesics but also enhances patient satisfaction with pain management.100
Quadratus Lumborum Block
Depending on the injection site relative to the quadratus lumborum muscle, various approaches to quadratus lumborum block (QLB) are distinguished.101 The lateral QLB (QLB1) involves the deposition of local anesthetic laterally to the quadratus lumborum.102 The posterior QLB (QLB2) entails injections posterior to the quadratus lumborum muscle. The anterior QLB (QLB3), also known as the transmuscular approach, typically involves injecting at the level of the L4 vertebra, anterior to the quadratus lumborum muscle.102 The intramuscular QLB (QLB4) consists of injecting the local anesthetic within the quadratus lumborum muscle itself.102
The precise mechanism by which QLB provides analgesia is not fully understood; however, it is hypothesized that local anesthetics diffuse through the thoracolumbar fascia and intrathoracic fascia into the paravertebral space to exert their analgesic effects.103 Research suggests that QLB3 facilitates the spread of anesthesia through the medial and lateral arcuate ligaments into the thoracic paravertebral space, whereas the lumbar plexus nerves between the transversus abdominis and the psoas major are not affected.104 During ultrasound-guided QLB3, patients are positioned in the lateral decubitus position, with a low-frequency convex probe placed perpendicularly above the iliac crest.105 The puncture needle is inserted from the anteromedial direction through the quadratus lumborum until the tip lies between the quadratus lumborum and psoas major muscles, followed by the injection of the local anesthetic into the fascia.105
Moderate evidence suggests that the use of QLB in hip joint surgeries can significantly reduce pain scores and opioid consumption within the first 24 hours postoperatively, making QLB a viable option for postoperative analgesia following hip surgery.106 However, some argue that as part of a multimodal analgesic approach, QLB does not significantly benefit patients undergoing hip replacement in terms of opioid consumption or pain scores during rest and activity, and carefully designed trials are needed to validate these findings.107 A study evaluating the benefits of QLB in total hip arthroplasty within randomized controlled trials found that incorporating QLB with general or spinal anesthesia did not confer substantial benefits, thus not supporting the routine use of QLB as part of a multimodal analgesic regimen for total hip arthroplasty.108
Fascia Obturator Nerve Block
The obturator nerve, originating from the anterior branches of the second, third, and fourth lumbar nerves, descends through the psoas major muscle, traversing the obturator canal to extend to the anterior portion of the thigh.109 This nerve is a critical component of the lumbar plexus, providing sensory and motor innervation to the medial thigh.110 The Femoral Obturator Nerve Block (FONB) is a technique used to control pain by blocking the obturator nerve, which can be performed using either a distal or proximal approach.111 The distal approach involves injecting local anesthetic between the pectineus and the adductor brevis muscles, or between the long and short adductor muscles, using in-plane ultrasound guidance to block the anterior branch of the obturator nerve, followed by an injection between the adductor brevis and adductor magnus to block the posterior branch.112 The proximal approach, under ultrasound guidance, involves injecting the local anesthetic into the fascial plane between the pectineus and obturator externus muscles, effectively blocking both the anterior and posterior branches of the obturator nerve.113 Compared to the distal approach, the proximal approach requires a smaller volume of local anesthetic and is more likely to achieve successful nerve blockade.114
Both FONB and the Fascia Iliaca Compartment Block (FICB) offer effective pain control for elderly patients with hip fractures Notably, FONB has been shown to provide superior pain relief compared to FICB, significantly reducing pain levels and lowering the reliance on analgesic medications.115 These advantages highlight FONB as a valuable technique for managing pain in elderly patients with hip fractures, particularly when incorporated into a multimodal analgesic strategy.
PENG Block
The Pericapsular Nerve Group (PENG) block, first introduced in 2018 by Giron-Arango et al, represents a novel local analgesic technique primarily targeting the sensory branches of the femoral, obturator, and accessory obturator nerves that innervate the peri-capsular region of the hip joint.116 This technique is advantageous for perioperative analgesia in hip surgeries. Under ultrasound guidance, the PENG block involves positioning the probe transversely above the anteroinferior iliac spine and moving it downward to visualize the pubic ramus, subsequently displaying the femoral artery and ilium.117 Using an in-plane approach, the needle is advanced from lateral to medial, and local anesthetic is injected between the anterior aspect of the iliopsoas tendon and the posterior aspect of the ilium.118 PENG can serve as an alternative to femoral or lumbar plexus blocks, mitigating the risks of quadriceps weakness associated with these blocks and increasing patient comfort due to the supine position.119 Some studies have reported that extensive anesthetic injection during a PENG block might lead to obturator muscle motor blockade.120 Considering the proximity of the femoral nerve relative to the iliopsoas tendon, substantial volumes of local anesthetics might diffuse superficially, inadvertently resulting in a femoral or fascia iliaca compartment block (FICB).121 A meta-analysis comparing single-shot FNB with continuous FNB underscored the superiority of the continuous technique, enhancing the duration of analgesia and reducing opioid consumption.122 Prado-Kittel et al conducted continuous PENG blocks by placing a catheter between the pubic ramus and the iliopsoas tendon, finding that continuous PENG provided excellent analgesia, extending pain relief to the distal femoral region.123 However, the clinical efficacy of continuous or multi-dose PENG blocks requires further exploration. While anterior capsular innervation is the source of most hip joint-related pain, PENG blocks primarily provide analgesia to the anterior hip capsule, neglecting the posterior capsule. The posterior capsule, innervated by the nerve to the quadriceps and superior gluteal nerve from the sacral plexus, also plays a crucial role in complete analgesia of the hip joint.124 As some scholars have recently suggested, combining PENG blocks with sciatic nerve blocks or local infiltration analgesic techniques to enhance perioperative pain management in hip surgeries may gain wider application in the future.125
Conclusion and Perspective
In managing shoulder and upper limb fractures, the use of continuous brachial plexus blocks (CBPB) including interscalene, supraclavicular, infraclavicular, and axillary blocks has markedly enhanced the scope and efficacy of regional anesthesia. Employing ultrasound-guided techniques has catalyzed a significant shift towards more precise, effective, and safe anesthesia practices. This has improved the specificity of nerve targeting for different fracture types, offering tailored analgesia that enhances patient recovery and comfort while minimizing systemic side effects. Each anatomical route—interscalene, supraclavicular, infraclavicular, and axillary—has been fine-tuned to optimize postoperative outcomes through targeted analgesia, thus directly impacting surgical recovery trajectories and pain management strategies. Such specificity not only accelerates patient rehabilitation but also aligns closely with personalized medical care approaches.
For thoracic and lumbar fractures, the Thoracolumbar Interfascial Plane (TLIP) and Erector Spinae Plane (ESPB) blocks stand out for their extensive coverage and deep penetration of anesthesia, crucial in managing the severe pain associated with these fractures. These newer techniques provide extensive coverage and deep penetration of anesthesia, crucial for managing the severe pain associated with spinal fractures. By diffusing anesthetic effectively across multiple layers of back musculature, these blocks facilitate comprehensive postoperative pain control, which is pivotal in promoting early mobilization and reducing the risk of long-term disability.
In emergency medicine, where rapid and effective pain management is essential, supraclavicular and infraclavicular blocks, along with ESPB blocks, are frequently utilized due to their efficacy in both pre and post-operative care for patients with fracture surgeries. These blocks are preferred for their quick onset and effective management of pain, making them particularly useful in acute settings where treatment speed is critical. This tailored approach to anesthesia for fractures across different anatomical regions not only ensures effective pain management but also supports faster and safer recovery, embodying the advancements in ultrasound-guided nerve block techniques.
As we look to the future, the trajectory of regional anesthesia is poised to leverage the ever-evolving ultrasonography technology to further enhance the precision and efficacy of nerve blocks. Anticipated advancements are expected to refine these already sophisticated techniques and introduce novel anesthetic compounds that could offer longer durations of pain relief with minimal side effects. The ongoing integration of these advanced regional anesthesia techniques into multimodal analgesia strategies is set to revolutionize pain management in orthopedic surgeries. This progression will likely lead to a significant reduction in opioid dependency, aligning with broader healthcare goals of enhancing patient outcomes, optimizing surgical recovery, and personalizing pain management strategies.
Funding
There is no funding to report.
Disclosure
We declare no competing interests.
References
1. Serra S, Santonastaso DP, Romano G. Efficacy and safety of the serratus anterior plane block (SAP block) for pain management in patients with multiple rib fractures in the emergency department: a retrospective study. Eur J Trauma Emerg Surg. 2024;50:3177–3188. doi:10.1007/s00068-024-02597-6
2. Reyes BJ, Mendelson DA, Mujahid N, et al. Postacute management of older adults suffering an osteoporotic hip fracture: a consensus statement from the International Geriatric Fracture Society. Geriatr Orthop Surg Rehabil. 2020;11:2151459320935100. doi:10.1177/2151459320935100
3. Di Maio G, Villano I, Ilardi CR, et al. Mechanisms of transmission and processing of pain: a narrative review. Int J Environ Res Public Health. 2023;20(4):3064. doi:10.3390/ijerph20043064
4. Wang A, Kerolus K, Garry E, Li D, Desai A. Novel techniques and local anesthetics for perioperative pain management. Reg Anesth. 2023. https://www.intechopen.com/chapters/1170072.
5. Ma K, Uejima JL, Bebawy JF. Regional anesthesia techniques in modern neuroanesthesia practice: a narrative review of the clinical evidence. J Neurosurg Anesthesiol. 2024;36(2):109–118. doi:10.1097/ANA.0000000000000911
6. Li J, Krishna R, Zhang Y, Lam D, Vadivelu N. Ultrasound-guided neuraxial anesthesia. Curr Pain Headache Rep. 2020;24(10):59.
7. Albrecht E, Chin KJ. Advances in regional anaesthesia and acute pain management: a narrative review. Anaesthesia. 2020;75(Suppl 1):e101–e110.
8. Li Y, Zhang Q, Wang Y, et al. Ultrasound-guided single popliteal sciatic nerve block is an effective postoperative analgesia strategy for calcaneal fracture: a randomized clinical trial. BMC Musculoskelet Disord. 2021;22(1):735.
9. Singh R. Study about brachial plexus: comprehension of its anatomy and associated injuries. In: Issues and Developments in Medicine and Medical Research Vol 2. 2022. doi:10.9734/bpi/idmmr/v2/2226c
10. Tanaka N, Suzuka T, Kadoya Y, Kawaguchi M. 166 The efficacy of modified thoracoabdominal nerves block through perichondrial approach: a prospective observational study and a cadaveric evaluation. Reg Anesth Pain Med. 2021;70(Suppl 1):A86–A87.
11. Feigl GC, Litz RJ, Marhofer P. Anatomy of the brachial plexus and its implications for daily clinical practice: regional anesthesia is applied anatomy. Reg Anesth Pain Med. 2020;45(8):620–627. doi:10.1136/rapm-2020-101435
12. Ilfeld B, Eisenach J, Gabriel R. Clinical effectiveness of liposomal bupivacaine administered by infiltration or peripheral nerve block to treat postoperative pain. Anesthesiology. 2021;134(2):283–344. doi:10.1097/ALN.0000000000003630
13. Erlenwein J, Diers M, Ernst J, Schulz F, Petzke F. Clinical updates on phantom limb pain. Pain Rep. 2021;6(1):e888. doi:10.1097/PR9.0000000000000888
14. Abd Elhady MM, Mehanna AA, Maged NA. A randomized controlled study comparing the use of ultrasound versus the conventional method in thoracic epidural catheter insertion as a pain relief method in thoracic surgeries. Res Opin Anesth Intensive Care. 2023;10(1):75. doi:10.4103/roaic.roaic_22_17
15. Jones MR, Novitch MB, Sen S, et al. Upper extremity regional anesthesia techniques: a comprehensive review for clinical anesthesiologists. Best Pract Res Clin Anaesthesiol. 2020;34(1):e13–e29. doi:10.1016/j.bpa.2019.07.005
16. Pawar P, Shah M, Shah N, Tiwari A, Sahu D, Bagaria V. Surgeon administered direct adductor canal block is as good as ultrasound guided adductor canal block in pain management in knee replacements- A retrospective case-control study. J Orthop Traumatol. 2022;31:103–109.
17. Krishna Prasad GV, Khanna S, Jaishree SV. Review of adjuvants to local anesthetics in peripheral nerve blocks: current and future trends. Saudi J Anaesth. 2020;14(1):77. doi:10.4103/sja.SJA_423_19
18. Ghasemi M, Janparvar A, Behnaz F, Taheri F. Evaluation of analgesia using perineural dexamethasone compound in interscalene brachial plexus block after shoulder surgery. Anesth Pain Med. 2024;14(1):e142635. doi:10.5812/aapm-142635
19. Saraswat RK, Deganwa M, Verma K, Bharadwaj A. Diaphragmatic and pulmonary functions following an ultrasound-guided supraclavicular approach versus a costoclavicular approach of a brachial plexus block: a randomized study. Cureus. 2024;16(6):e62586. doi:10.7759/cureus.62586
20. Ashwin M, Kumar KR, Sinha R, et al. Ultrasound guided costoclavicular block in pediatric population: a prospective observational study. Paediatr Anaesth. 2024;34(6):538–543. doi:10.1111/pan.14889
21. Reeves MT, O’Neil K, Slesinger TL. Costoclavicular brachial plexus block facilitates painless upper extremity reduction: a case report. Clin Pract Cases Emerg Med. 2023;7(4):221–226. doi:10.5811/cpcem.59091
22. Koo CH, Hwang I, Shin HJ, Ryu JH. Hemidiaphragmatic paralysis after costoclavicular approach versus other brachial plexus blocks in upper limb surgery: a meta-analysis. Korean J Anesthesiol. 2023;76(5):442–450. doi:10.4097/kja.22718
23. Sivasankar K, Sureshkumar K, Silambarasan S. Ultrasound-guided single injection infraclavicular brachial plexus block using bupivacaine alone or combination combined with dexmedetomidine for pain control in upper limb surgery. Int J Acad Med Pharm. 2023;5(2):111–114.
24. Soliman FI, Mabood AMA, Mahmoud AG, Mohamed KA. Comparative study between ketamine-bupivacaine versus bupivacaine with intravenous ketamine infusion in supraclavicular brachial plexus block during upper limb surgeries. Res Opin Anesth Intensive Care. 2023;10(4):279. doi:10.4103/roaic.roaic_25_23
25. Ma X, Yan J, Jiang H. Application of ketamine in pain management and the underlying mechanism. Pain Res Manag. 2023;2023:1928969. doi:10.1155/2023/1928969
26. Bihani P, Pandey A, Jha M, Paliwal N, Jaju R, Solanki R. Comparing perfusion index and visual analogue scores for postoperative pain assessment following upper limb surgeries under supraclavicular brachial plexus block: an observational study. Cureus. 2024;16(3):e55529. doi:10.7759/cureus.55529
27. Guru A, Desingh DC, Jayakumar V, Kuppusamy SK. A comparison between ultrasound-guided supraclavicular and infraclavicular approaches to brachial plexus block for elective upper limb surgery. Cureus. 2023;15(10):e46656. doi:10.7759/cureus.46656
28. Singh DP, Rai SK, Maurya RG, et al. Analgesic efficacy of dexmedetomidine as an adjuvant to ropivacaine in supraclavicular brachial plexus block for upper limb surgeries: a prospective randomized study. Indian J Pain. 2023;37(Suppl 1):S22–S27. doi:10.4103/ijpn.ijpn_38_23
29. Alshammari HS, Alshammari AS, Alshammari SA, Ahamed SS. Prevalence of chronic pain after spinal surgery: a systematic review and meta-analysis. Cureus. 2023;15(7):e41841. doi:10.7759/cureus.41841
30. Sampognaro G, Harrell R. Multimodal postoperative pain control after orthopaedic surgery. In: StatPearls. StatPearls Publishing; 2023.
31. Kozera K, Ciszek B. Posterior branches of lumbar spinal nerves - part I: anatomy and functional importance. Ortop Traumatol Rehabil. 2016;18(1):1–10. doi:10.5604/15093492.1198827
32. Kozera K, Ciszek B, Szaro P. Posterior branches of lumbar spinal nerves - part II: lumbar facet syndrome - pathomechanism, symptomatology and diagnostic work-up. Ortop Traumatol Rehabil. 2017;19(2):101–109. doi:10.5604/15093492.1237716
33. Zhang Z, Liu J, Xu Y, et al. Anatomical study and clinical significance of the posterior ramus of the spinal nerve of the lumbar spine. Front Cell Dev Biol. 2022;10:1019309. doi:10.3389/fcell.2022.1019309
34. Shuang F, Hou SX, Zhu JL, et al. Clinical anatomy and measurement of the medial branch of the spinal dorsal ramus. Medicine. 2015;94(52):e2367. doi:10.1097/MD.0000000000002367
35. Palpan Flores A, García feijoo P, Isla Guerrero A. Paraspinal muscle atrophy after posterior lumbar surgery with and without pedicle screw fixation with the classic technique. Neurocir. 2019;30(2):69–76. doi:10.1016/j.neucir.2018.11.006
36. Huang XL, Chen YC, Kuo CC, Tsai ST. Potential benefits of spinal cord stimulation treatment on quality of life for paralyzed patients with spinal cord injury. Tzu Chi Med J. 2023;35(2):131–136. doi:10.4103/tcmj.tcmj_102_22
37. Sayed D, Grider J, Strand N, et al. The American Society of Pain and Neuroscience (ASPN) evidence-based clinical guideline of interventional treatments for low back pain. J Pain Res. 2022;15:3729–3832.
38. Kozera K, Ciszek B, Szaro P. Posterior branches of lumbar spinal nerves – part III: spinal dorsal ramus mediated back pain – pathomechanism, symptomatology and diagnostic work-up. Ortop Traumatol Rehabil. 2017;19(4):315–321.
39. Zhang P, Chang H, Yang T, et al. Study on MEV90 of 0.5% ropivacaine for US-guided caudal epidural block in anorectal surgery. Front Med. 2022;9:1077478. doi:10.3389/fmed.2022.1077478
40. Wong SSC, Choi SW, Lee Y, Irwin MG, Cheung CW. The analgesic effects of intraoperative total intravenous anesthesia (TIVA) with propofol versus sevoflurane after colorectal surgery. Medicine. 2018;97(31):e11615. doi:10.1097/MD.0000000000011615
41. Liu M, Shaparin N, Nair S, Kim RS, Hascalovici JR. Chronic low back pain: the therapeutic benefits of diagnostic medial branch nerve blocks. Pain Physician. 2021;24(4):E521–E528.
42. Chakraborty A, Khemka R, Datta T. Ultrasound-guided truncal blocks: a new frontier in regional anaesthesia. Indian J Anaesth. 2016;60(10):703–711. doi:10.4103/0019-5049.191665
43. Abdildin YG, Salamat A, Omarov T, Sultanova M, Krassavina Y, Viderman D. Thoracolumbar interfascial plane block in spinal surgery: a systematic review with meta-analysis. World Neurosurg. 2023;174:52–61. doi:10.1016/j.wneu.2023.02.140
44. Liu T, Yang J, Wang Y, et al. Interfascial plane block: a new anesthetic technique. Anesthesiol Perioperative Sci. 2023;1(4):31. doi:10.1007/s44254-023-00028-0
45. Dontukurthy S, Mofidi R. The role of interfascial plane blocks in paediatric regional anaesthesia: a narrative review of current perspectives and updates. Anesthesiol Res Pract. 2020;2020:8892537. doi:10.1155/2020/8892537
46. Eltaher E, Nasr N, Abuelnaga ME, Elgawish Y. Effect of ultrasound-guided thoracolumbar interfascial plane block on the analgesic requirements in patients undergoing lumbar spine surgery under general anesthesia: a randomized controlled trial. J Pain Res. 2021;14:3465–3474. doi:10.2147/JPR.S329158
47. Patel TD, McNicholas MN, Paschell PA, Arnold PM, Lee CT. Thoracolumbar Interfascial Plane (TLIP) block verses other paraspinal fascial plane blocks and local infiltration for enhanced pain control after spine surgery: a systematic review. BMC Anesthesiol. 2024;24(1):122. doi:10.1186/s12871-024-02500-1
48. Hu L, Shen Z, Pei D, et al. Ultrasound-guided modified thoracolumbar fascial plane block in Tianji robot-assisted lumbar internal fixation: a prospective, randomized, and non-inferiority study. J Pain Res. 2023;16:543–552. doi:10.2147/JPR.S395677
49. Hu Z, Han J, Jiao B, et al. Efficacy of thoracolumbar interfascial plane block for postoperative analgesia in lumbar spine surgery: a meta-analysis of randomized clinical trials. Pain Physician. 2021;24(7):E1085–E1097.
50. Gajapure SJ, Chakole V. Exploring the thoracolumbar interfascial plane (TLIP) block as a novel approach for improved pain management after spine surgery: a comparative review. Cureus. 2024;16(5):e59531. doi:10.7759/cureus.59531
51. Long G, Liu C, Liang T, Zhan X. The efficacy of thoracolumbar interfascial plane block for lumbar spinal surgeries: a systematic review and meta-analysis. J Orthop Surg Res. 2023;18(1):318. doi:10.1186/s13018-023-03798-2
52. Saini S, Sharma A, Gupta A, Mankotia DS, Boruah T. Analgesic efficacy of thoracolumbar interfascial plane block versus standard care in patients undergoing lumbar spinal surgeries—A randomized controlled trial. J Neuroanaesth Crit Care. 2024. doi:10.1055/s-0044-1782506
53. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
54. Bonnel F, Dimeglio A. Vertebral column: muscles, aponeurosis, and fascia. In: Spinal Anatomy. Springer International Publishing; 2020:279–320.
55. Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth. 2021;68(3):387–408. doi:10.1007/s12630-020-01875-2
56. Abdella AMMR, Arida EEAEM, Megahed NA, El-Amrawy WZ, Mohamed WMA. Analgesia and spread of erector spinae plane block in breast cancer surgeries: a randomized controlled trial. BMC Anesthesiol. 2022;22(1):321. doi:10.1186/s12871-022-01860-w
57. Liheng L, Siyuan C, Zhen C, Changxue W. Erector spinae plane block versus transversus abdominis plane block for postoperative analgesia in abdominal surgery: a systematic review and meta-analysis. J Invest Surg. 2022;35(9):1711–1722. doi:10.1080/08941939.2022.2098426
58. Ciftci B, Ekinci M, Celik EC, Tukac IC, Bayrak Y, Atalay YO. Efficacy of an ultrasound-guided erector spinae plane block for postoperative analgesia management after video-assisted thoracic surgery: a prospective randomized study. J Cardiothorac Vasc Anesth. 2020;34(2):444–449.
59. Elsabeeny WY, Shehab NN, Wadod MA, Elkady MA. Perioperative analgesic modalities for breast cancer surgeries: a prospective randomized controlled trial. J Pain Res. 2020;13:2885–2894.
60. Park YJ, Chu S, Yu E, Joo JD. Comparison of the efficacy of erector spinae plane block according to the difference in bupivacaine concentrations for analgesia after laparoscopic cholecystectomy: a retrospective study. Journal of Yeungnam. 2023;40(2):172–178.
61. Voss A, Pfeifer CG, Kerschbaum M, Rupp M, Angele P, Alt V. Post-operative septic arthritis after arthroscopy: modern diagnostic and therapeutic concepts. Knee Surg Sports Traumatol Arthrosc. 2021;29(10):3149–3158.
62. Mirkheshti A, Raji P, Komlakh K, Salimi S, Shakeri A. The efficacy of ultrasound-guided erector spinae plane block (ESPB) versus freehand ESPB in postoperative pain management after lumbar spinal fusion surgery: a randomized, non-inferiority trial. Eur Spine J. 2024;33(3):1081–1088.
63. Xiao X, Zhu T, Wang L, Zhou H, Zhang Y. Efficacy of postoperative analgesia by erector spinal plane block after lumbar surgery: a systematic review and meta-analysis of randomized controlled trials. Comput Math Methods Med. 2022;2022:3264142.
64. Rizkalla JM, Holderread B, Awad M, Botros A, Syed IY. The erector spinae plane block for analgesia after lumbar spine surgery: a systematic review. J Orthop. 2021;24:145–150.
65. Lucente M, Ragonesi G, Sanguigni M, et al. Erector spinae plane block in children: a narrative review. Korean J Anesthesiol. 2022;75(6):473–486.
66. Fusco P, Stecco C, Maggiani C, Ciaschi W. Erector spinae plane block with warm saline solution for treating chronic myofascial pain. Minerva Anestesiol. 2024;90(3):217–218.
67. Wang L, Wu Y, Dou L, Chen K, Liu Y, Li Y. Comparison of two ultrasound-guided plane blocks for pain and postoperative opioid requirement in lumbar spine fusion surgery: a prospective, randomized, and controlled clinical trial. Pain Ther. 2021;10(2):1331–1341.
68. Sundaram Venkatesan G, Thulasiraman SV, Kesavan B, Chinnaraju N, Manoharan EV, Kesavan P. An observational study to assess postoperative pain control and formulate a comprehensive approach to the implementation of policy change for pain control in postoperative units. Cureus. 2022;14(12):e33026.
69. Hyland SJ, Brockhaus KK, Vincent WR, et al. Perioperative pain management and opioid stewardship: a practical guide. Healthcare (Basel). 2021;9(3):333.
70. Tsaousi G, Tsitsopoulos PP, Pourzitaki C, Palaska E, Badenes R, Bilotta F. Analgesic efficacy and safety of local infiltration following lumbar decompression surgery: a systematic review of randomized controlled trials. J Clin Med. 2021;10(24):5936.
71. Fontalis A, Epinette JA, Thaler M, Zagra L, Khanduja V, Haddad FS. Advances and innovations in total Hip arthroplasty. SICOT J. 2021;7:26.
72. Shellito AD, Dworsky JQ, Kirkland PJ, et al. Perioperative pain management issues unique to older adults undergoing surgery: a narrative review. Ann Surg Open. 2021;2(3):e072.
73. Hirose M, Okutani H, Hashimoto K, et al. Intraoperative assessment of surgical stress response using nociception monitor under general anesthesia and postoperative complications: a narrative review. J Clin Med. 2022;11(20):6080.
74. Yousef M, Zheng H, Yang W, Ayers DC. Predictive factors of pain and functional outcome 5 years following total hip arthroplasty: a prospective function and outcomes research for comparative effectiveness in total joint replacement cohort study. J Arthroplasty. 2024. doi:10.1016/j.arth.2024.02.050
75. Scholzen EA, Silva JB, Schroeder KM. Unique considerations in regional anesthesia for emergency department and non-or procedures. Int Anesthesiol Clin. 2024;62(1):43–53.
76. Jiang W, Tang M, Yang L, et al. Analgesic alkaloids derived from traditional Chinese medicine in pain management. Front Pharmacol. 2022;13:851508.
77. Casas Reza P, Gestal Vázquez M, López Álvarez S. New ultrasound-guided capsular blocks for hip surgery: a narrative review. Rev Esp Anestesiol Reanim. 2022;69(9):556–566.
78. Warner T, Tubbs RS, Chapter 6 - Lumbar Plexus. In: Surgical Anatomy of the Lateral Transpsoas Approach to the Lumbar Spine. Tubbs RS, Iwanaga J, Oskouian RJ, Moisi M, editors. Elsevier; 2020:45–81.
79. Lee TY, Chung CJ, Park SY. Comparing the pericapsular nerve group block and the lumbar plexus block for Hip fracture surgery: a single-center randomized double-blinded study. J Clin Med. 2023;13(1). doi:10.3390/jcm13010122
80. Refai N, Tadi P. Anatomy, bony pelvis and lower limb, thigh femoral nerve; 2020. Available from: https://europepmc.org/article/nbk/nbk556065.
81. Situ-LaCasse E, Javedani P, Devis P, Arif-Tiwari H. Ultrasound-guided percutaneous drainage procedures. In: Adhikari S, Blaivas M, editors. The Ultimate Guide to Point-of-Care Ultrasound-Guided Procedures. Springer International Publishing; 2020:205–223.
82. Jelínek L, Gogna S, Ferguson T. Anatomy, abdomen and pelvis, anterolateral abdominal wall fascia. 2019. Available from: https://europepmc.org/article/nbk/nbk557605.
83. Zhang J, He Y, Wang S, et al. The erector spinae plane block causes only cutaneous sensory loss on ipsilateral posterior thorax: a prospective observational volunteer study. BMC Anesthesiol. 2020;20(1):88.
84. Abebe MM, Arefayne NR, Temesgen MM, Admass BA. Incidence and predictive factors associated with hemodynamic instability among adult surgical patients in the post-anesthesia care unit, 2021: a prospective follow up study. Ann Med Surg. 2022;74(103321):103321.
85. Trionfo A, Zimmerman R, Gillock K, Budziszewski R, Hasan A. Lumbar plexus nerve blocks for perioperative pain management in cerebral palsy patients undergoing hip reconstruction: more effective than general anesthesia and epidurals. J Pediatr Orthop. 2023;43(1):e54–e59.
86. Zhang J, Li Y, Sun X, Ren W. Effects of lumbar plexus block combined with infiltration anesthesia on anesthesia comfort scores and stress responses in elderly patients undergoing hip replacement. Dis Markers. 2022;2022:8692966.
87. Roldan PS, Mora AC, Cruz PA, Zambrano LG, Paredes G, Cajamarca AC. Ultrasound-guided regional analgesia for post-cesarean pain. Topics in Regional Anesthesia. 2022;69. doi:10.5772/intechopen.101465
88. Fung G, Liu SE. Regional anaesthesia for orthopaedic procedures. Anaesth Intensive Care Med. 2021;22(1):13–18.
89. Vojvodić A, Matic A, Mihailović J, et al. Anatomical and functional study of the psoas major muscle and femoral nerve in correlation with pelvic diameters. Vojnosanit Pregl. 2023. doi:10.2298/vsp221129025v
90. Meti V, Lohit K, Amarappa G, Babu R, Balaraju T, Lavanya S. Usefulness of ultrasonography guided femoral and lateral femoral cutaneous nerve blocks in providing analgesia before giving spinal anaesthesia in patients undergoing surgery for intertrochanteric fracture of femur: a randomized clinical trial. J Anaesthesiol Clin Pharmacol. 2022;38:469–473.
91. Shim JG, Cho EA, Gahng TR, et al. Application of the dynamic needle tip positioning method for ultrasound-guided arterial catheterization in elderly patients: a randomized controlled trial. PLoS One. 2022;17(8):e0273563.
92. Fukui S, Rokutanda R, Kawaai S, et al. Current evidence and practical knowledge for ultrasound-guided procedures in rheumatology: joint aspiration, injection, and other applications. Best Pract Res Clin Rheumatol. 2023;37(1):101832.
93. Kim CH, Yang JY, Min CH, Shon HC, Kim JW, Lim EJ. The effect of regional nerve block on perioperative delirium in hip fracture surgery for the elderly: a systematic review and meta-analysis of randomized controlled trials. Orthop Traumatol Surg Res. 2022;108(1):103151.
94. Eshag MME, Hasan LOM, Elshenawy S, et al. Fascia iliaca compartment block for postoperative pain after total hip arthroplasty: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2024;24(1):95.
95. Kong B, Zabadayev S, Perese J, Panag A, Jafry Z. Ultrasound-guided fascia iliaca compartment block simulation training in an emergency medicine residency program. Cureus. 2024;16(1):e52411.
96. Nidgundi N, Rao MS, Mukund M. Ultrasound-guided preoperative fascia iliaca compartment block for pain relief during positioning for spinal anesthesia in patients with hip fracture. Cureus. 2023;15(12):e51185.
97. Zheng T, Hu B, Zheng CY, Huang FY, Gao F, Zheng XC. Improvement of analgesic efficacy for total hip arthroplasty by a modified ultrasound-guided supra-inguinal fascia iliaca compartment block. BMC Anesthesiol. 2021;21(1):75.
98. Aoki Y, Sugiura S, Nakagawa K, et al. Evaluation of nonspecific low back pain using a new detailed visual analogue scale for patients in motion, standing, and sitting: characterizing nonspecific low back pain in elderly patients. Pain Res Treat. 2012;2012:680496.
99. Chen L, Liu S, Cao Y, Yan L, Shen Y. Effect of perioperative ultrasound guided fascia iliaca compartment block in elderly adults with Hip fractures undergoing arthroplasty in spinal anesthesia-a randomized controlled trial. BMC Geriatr. 2023;23(1):66.
100. Mou Z, Xiang L, Ni Y. Comparative effectiveness of pericapsular nerve group block versus fascia iliac compartment block on postoperative wound pain management in patients undergoing hip fracture surgery: a systematic review and meta-analysis. Int Wound J. 2024;21(2):e14637. doi:10.1111/iwj.14637
101. Abdeltawab AM, Abo-Elkhair SA, Radi MS, Ataa AMAA. Quadratus lumborum block versus transversus abdominis plane block for analgesia after caesarean section. SJMS. 2023;2(3):88–95. doi:10.55675/sjms.v2i3.57
102. Elsharkawy H, Bendtsen TF. Ultrasound-guided transversus abdominis plane and quadratus lumborum nerve blocks. NYSORA [Online|| 2022 | Cited: June 30, 2022]; 2023. Available from: https://www.nysora.com/topics/regional-anesthesia-forspecific-surgical-procedures/abdomen/ultrasound-guided-transversus-abdominis-plane-quadratus-lumborum-blocks.
103. Akerman M, Pejčić N, Veličković I. A review of the quadratus lumborum block and ERAS. Front Med. 2018;5:44. doi:10.3389/fmed.2018.00044
104. Long X, Yin Y, Guo W, Tang L. Ultrasound-guided quadratus lumborum block: a powerful way for reducing postoperative pain. Ann Med Surg. 2023;85(10):4947–4953. doi:10.1097/MS9.0000000000001209
105. Jadon A, Jain P, Dhanwani L. Bilateral transmuscular quadratus lumborum block performed in single lateral decubitus position without changing position to the contralateral side. Indian J Anaesth. 2018;62(4):314. doi:10.4103/ija.IJA_750_17
106. Xiong H, Chen X, Zhu W, Yang W, Wang F. Postoperative analgesic effectiveness of quadratus lumborum block: systematic review and meta-analysis for adult patients undergoing Hip surgery. J Orthop Surg Res. 2022;17(1):282. doi:10.1186/s13018-022-03172-8
107. Park HJ, Park KK, Park JY, Lee B, Choi YS, Kwon HM. Peripheral nerve block for pain management after total hip arthroplasty: a retrospective study with propensity score matching. J Clin Med. 2022;11(18):5456. doi:10.3390/jcm11185456
108. Hussain N, Brull R, Speer J, et al. Analgesic benefits of the quadratus lumborum block in total Hip arthroplasty: a systematic review and meta-analysis. Anaesthesia. 2022;77(10):1152–1162. doi:10.1111/anae.15823
109. Tshabalala ZN, Human-Baron R, van der Walt S, Louw EM, van Schoor AN. The anatomy of the obturator nerve and its branches in a South African cadaver sample. Transl Res Anatomy. 2022;27:100201. doi:10.1016/j.tria.2022.100201
110. Liyew WA. Clinical presentations of lumbar disc degeneration and lumbosacral nerve lesions. Int J Rheumatol. 2020;2020:2919625. doi:10.1155/2020/2919625
111. Kang C, Hwang DS, Song JH, et al. Clinical analyses of ultrasound-guided nerve block in lower-extremity surgery: a retrospective study. J Orthop Surg. 2021;29(1):2309499021989102. doi:10.1177/2309499021989102
112. Harmon CM, Davidson KS, Helander E, Eng MR, Kaye AD. Ultrasound guided nerve blocks for lower extremity. In: Li J, Ming-Der Chow R, Vadivelu N, Kaye AD, editors. Ultrasound Fundamentals: An Evidence-Based Guide for Medical Practitioners. Springer International Publishing; 2021:149–160.
113. Yoshida T, Nakamoto T, Kamibayashi T. Ultrasound-guided obturator nerve block: a focused review on anatomy and updated techniques. Biomed Res Int. 2017;2017:7023750. doi:10.1155/2017/7023750
114. Malik A, Thom S, Haber B, et al. Regional anesthesia in the emergency department: an overview of common nerve block techniques and recent literature. Curr Emerg Hospital Med Rep. 2022;10(3):54–66. doi:10.1007/s40138-022-00249-w
115. Hao C, Li C, Cao R, et al. Effects of perioperative fascia iliaca compartment block on postoperative pain and hip function in elderly patients with hip fracture. Geriatr Orthop Surg Rehabil. 2022;13:21514593221092884. doi:10.1177/21514593221092883
116. Johnson ELH, Kelly TL, Wolf BJ, et al. Comparison of pericapsular nerve group and lateral quadratus lumborum blocks for analgesia after primary total hip arthroplasty: a randomized controlled trial. bioRxiv. 2024. doi:10.1101/2024.07.18.24310628
117. Girón-Arango L, Peng P. Pericapsular nerve group (PENG) block: what have we learned in the last 5 years? Reg Anesth Pain Med. 2024:
118. Albano D, Gitto S, Serpi F, Aliprandi A, Maria Sconfienza L, Messina C. Ultrasound-guided musculoskeletal interventional procedures around the hip: a practical guide. J Ultrason. 2023;23(92):15–22. doi:10.15557/JoU.2023.0003
119. Kukreja P, Schuster B, Northern T, Sipe S, Naranje S, Kalagara H. Pericapsular nerve group (PENG) block in combination with the quadratus lumborum block analgesia for revision total hip arthroplasty: a retrospective case series. Cureus. 2020;12(12):e12233. doi:10.7759/cureus.12233
120. Yeoh SR, Chou Y, Chan SM, Hou JD, Lin JA. Pericapsular nerve group block and iliopsoas plane block: a scoping review of quadriceps weakness after two proclaimed motor-sparing hip blocks. Healthcare. 2022;10(8). doi:10.3390/healthcare10081565
121. Crutchfield CR, Schweppe EA, Padaki AS, et al. A practical guide to lower extremity nerve blocks for the sports medicine surgeon. Am J Sports Med. 2023;51(1):279–297. doi:10.1177/03635465211051757
122. Yurutkina A, Klaschik S, Kowark P, et al. Pain levels and patient comfort after lower limb arthroplasty comparing i.v. patient-controlled analgesia, continuous peripheral nerve block and neuraxial analgesia: a retrospective cohort analysis of clinical routine data. J Orthop Surg Res. 2022;17(1):381. doi:10.1186/s13018-022-03277-0
123. Prado-Kittel C, Zumelzu-Sánchez P, Palma-Licandeo A, Faúndez-Lillo G, Ellenberg-Oyarce K, Jorquera-Adarme B. Continuous pericapsular nerve group blockade as analgesia for fracture of the posterior column and wall of the acetabulum; a case report and description of infusion regimen for extending analgesic effect to the distal femoral area. Rev Esp Anestesiol Reanim. 2020;67(3):159–162. doi:10.1016/j.redar.2019.12.005
124. Thorp LE. Hip anatomy. In: Hip Arthroscopy and Hip Joint Preservation Surgery. Springer International Publishing; 2022:3–15.
125. Zheng J, Du L, Chen G, Zhang L, Deng X, Zhang W. Efficacy of pericapsular nerve group (PENG) block on perioperative pain management in elderly patients undergoing hip surgical procedures: a protocol for a systematic review with meta-analysis and trial sequential analysis. BMJ Open. 2023;13(1):e065304. doi:10.1136/bmjopen-2022-065304
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.