")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Tracing Missing Surgical Specimens: A Quality Improvement Strategy for Adverse Events Based on Root Cause Analysis
Authors Huang LL, Yang JH, Hong WW , Wang BL, Chen HF
Received 8 March 2025
Accepted for publication 23 June 2025
Published 27 June 2025 Volume 2025:18 Pages 2139—2150
DOI https://doi.org/10.2147/RMHP.S527015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Li-Li Huang,1 Ju-Hong Yang,2 Wei-Wen Hong,3 Bin-Liang Wang,4 Hai-Fei Chen5
1Department of Quality Management, Huangyan Hospital Affiliated to Wenzhou Medical University, Taizhou, Zhejiang, People’s Republic of China; 2Infusion Room, Taizhou First People’s Hospital, Huangyan, Zhejiang, People’s Republic of China; 3Department of General Surgery, Taizhou First People’s Hospital, Taizhou, Zhejiang, People’s Republic of China; 4Department of Hospital, Taizhou First People’s Hospital, Taizhou, Zhejiang, People’s Republic of China; 5Operating Room, Taizhou First People’s Hospital, Taizhou, Zhejiang, People’s Republic of China
Correspondence: Hai-Fei Chen, Operating Room, Taizhou First People’s Hospital, Taizhou, Zhejiang, China, No. 218, Hengjie Road, Huangyan District, Taizhou, Zhejiang, 318020, People’s Republic of China, Tel +86-13575807288, Email [email protected] Bin-Liang Wang, Hospital Department, Taizhou First People’s Hospital, No. 218, Hengjie Road, Huangyan District, Taizhou, Zhejiang, 318020, People’s Republic of China, Email [email protected]
Background: In 2022, a critical incident occurred at a Chinese hospital where a surgical specimen from a rectal prostate procedure was misplaced, necessitating repeat surgery for the patient. This event underscored systemic vulnerabilities in specimen handling processes and catalyzed an investigation into how healthcare systems manage medical errors to uphold patient safety.
Methods: Using root cause analysis (RCA), we dissected the workflow gaps and organizational factors contributing to the specimen loss. Key failures identified included unclear role delineation among staff, inadequate specimen labeling protocols, and lack of real-time tracking mechanisms. Three interventions were implemented: (1) Redesigning specimen handling workflows with explicit role responsibilities; (2) Developing standardized, color-coded specimen bottles and racks to improve visual identification; (3) Integrating an electronic tracking system for closed-loop management of specimens.
Results: Post-intervention, the recognition rate of post-use specimen vials improved from 0% to 100% after implementing a dual-color sealing system (white cap with red ring), enabling visual confirmation of proper sealing. Over two years, no surgical pathology specimens were lost post-intervention.
Conclusion: The RCA-driven reforms effectively addressed systemic flaws in specimen management, demonstrating that targeted process redesign, ergonomic tools, and digital tracking can mitigate risks of medical errors. This case highlights the importance of analyzing localized workflow failures within broader systemic contexts to build resilient, patient-centered medical care systems.
Keywords: rectal prostate specimens, medical errors, root cause analysis, patient safety, quality improvement
Introduction
Patient safety has remained a pivotal concern in healthcare since seminal reports such as the Institute of Medicine’s “To Err is Human: Building a Safer Health System”.1 The mishandling of surgical specimens, in particular, poses significant risks, including delayed diagnoses, inappropriate treatments, and unnecessary repeat procedures. Globally, studies estimate that approximately 6% of specimen errors directly result in adverse clinical outcomes.2 Moreover, over half of these errors can be attributed to identifiable systemic factors, including ambiguous protocols and insufficient safeguards.2 These challenges persist despite decades of efforts to improve safety frameworks, underscoring the urgency of addressing latent organizational flaws that perpetuate errors.3
In 2022, a sentinel event at a Chinese hospital exemplified these systemic gaps: a misplaced rectal prostate biopsy specimen led to a patient undergoing repeat surgery. This incident not only caused physical and psychological harm but also exposed critical weaknesses in specimen management workflows, including inconsistent labeling practices, fragmented role responsibilities, and a lack of real-time tracking mechanisms. Such failures align with prior findings that more than half of errors involve preventable systemic oversights.2 Yet this case uniquely highlights the cascading consequences of these gaps in a high-stakes clinical setting.
RCA is a structured, systematic process designed to identify the fundamental reasons behind adverse events rather than merely addressing the immediate causes.4 It typically begins with a detailed reconstruction of the event timeline, involving the collection of data from various sources such as incident reports, interviews with involved personnel, and review of relevant policies and procedures.5,6 One of the key techniques used in RCA is the “5 Whys” method, where the team repeatedly asks “why” about each identified factor contributing to the event.5,6 Which categorizes potential causes into groups like people, methods, machines, materials, and environment, allowing the team to visualize and analyze the complex web of factors contributing to the event.6,7
In other healthcare contexts, RCA has been highly successful. For example, in the area of hospital - acquired pressure ulcers.8 Similarly, in surgical site infection prevention, RCA has helped uncover issues like ineffective pre - operative skin preparation, improper sterilization of surgical instruments, and breakdowns in communication among the surgical team. Corrective actions based on RCA findings have led to a substantial decrease in surgical site infections.9 These examples illustrate the versatility and effectiveness of RCA, highlighting the potential for its application in addressing specimen - related errors. RCA has been recognized as a powerful theoretical tool, capable of identifying fundamental issues such as outdated protocols and technological deficiencies.10,11
However, despite its well-established theoretical utility, its practical application to specimen-related errors, which can have significant consequences for patient care, remains notably underexplored. Specimen - related errors, which can lead to incorrect diagnoses, inappropriate treatment, and potential harm to patients, often stem from complex interactions between human factors, such as fatigue, lack of attention and system - level issues, such as inefficient processes and outdated technology. Human factors engineering, which focuses on optimizing the interaction between humans and systems, and digital solutions, which can automate and streamline processes, have the potential to address these root causes effectively.12,13 However, the practical application of these approaches in the context of specimen - related errors, guided by a rigorous RCA framework, remains largely unexplored. This study aims to fill this gap by demonstrating how a comprehensive RCA can identify the root causes of specimen - related errors and inform the development and implementation of targeted interventions based on human factors engineering principles and digital solutions, thereby contributing to the broader goal of improving patient safety in healthcare systems globally.
Methods
Study Design
This quality improvement project investigated a 2022 sentinel event at a tertiary hospital in Zhejiang Province, China, where a misplaced rectal prostate biopsy specimen necessitated repeat surgery. The hospital, with 1,200 beds and ~17,000 annual surgeries, processes ~8,000 surgical specimens yearly. The RCA followed national guidelines, focusing on systemic failures in specimen handling rather than individual blame.14
Team Composition
A multidisciplinary RCA team (vice president, a quality manager, an operating room head nurse, a urologist, and a pathologist), reviewed workflows, and mapped the specimen journey (shown in Figure 1). The head nurse of the operating room was the leader of the team. Staff involved in the incident were excluded to minimize bias.15 Each team member brought unique expertise to the project. All team members were trained and passed an RCA course of at least 8 hours prior to joining. Regular team meetings were held to discuss findings, share ideas, and make decisions.
 |
Figure 1 The event story map. |
Event-Specific Analysis Framework
System Failure Identification
Using the Incident Decision Tree (IDT),16,17 we evaluated whether systemic factors rather than individual error enabled the specimen loss. The “substitution test” confirmed that even competent staff would likely err under existing conditions due to:
- Ambiguous preoperative order protocols.
- Lack of visual verification tools for specimen bottle sealing.
- Absence of real-time tracking between operating rooms and pathology labs.
Semi-Structured Face-to-Face Interviews
We conducted semi-structured interviews with 12 hospital staff members, including nurses, doctors, technicians and administrative personnel directly involved in the specimen handling process (excluding those directly related to sentinel incidents to minimize bias). Due to the sensitivity of the issue, no interviews were conducted with the patients and their families in this study. Sample questions included: “Can you describe the steps you take to ensure specimen integrity during the handoff between the operating room and the pathology lab?”; “Have you encountered any challenges with the current specimen labeling or sealing protocols, and if so, what were they?”; and “In your opinion, what aspects of the specimen handling workflow could be improved to prevent errors?” These questions aimed to uncover systemic issues in the specimen handling process, rather than focusing on individual performance.
“Swiss Cheese” Conceptual Model Analysis
We conducted a qualitative error analysis using James Reason’s “Swiss cheese” model to explore the interaction between surgical specimen loss and its systemic implications.18,19 In the analysis, by applying the Swiss cheese model, various “holes” that led to the loss of surgical specimens at different system levels were identified, as shown in Figure 2. These included issues such as specimen bottle status unconfirmed, unconfirmed specimen count status and records, failure to send specimens to the herbarium, and specimen bottles not labelled. Each of these represented gaps or failures in specific processes. The model posits that when such holes across different levels (eg, preoperative, intraoperative, postoperative workflows) align, they create a pathway for errors like specimen loss to occur.
 |
Figure 2 The Swiss cheese conceptual model analysis. |
Root Cause Identification
We identified 13 systemic root causes (shown in Table 1). The analysis identified three interdependent systemic vulnerabilities contributing to the specimen loss (identify root cause contributing factors as shown in Figure 3). Material deficiencies were evident in non-intuitive specimen labeling designs, which increased the risk of misidentification during high-pressure workflows. Process gaps further compounded risks, as the absence of closed-loop tracking systems allowed specimens to bypass critical checkpoints undetected. Human factor limitations exacerbated these issues, with inadequate staff training on updated protocols leading to inconsistent adherence to safety measures. Together, these flaws created alignment in the system’s “Swiss cheese” defenses, enabling the specimen to slip through multiple layers of safeguards.
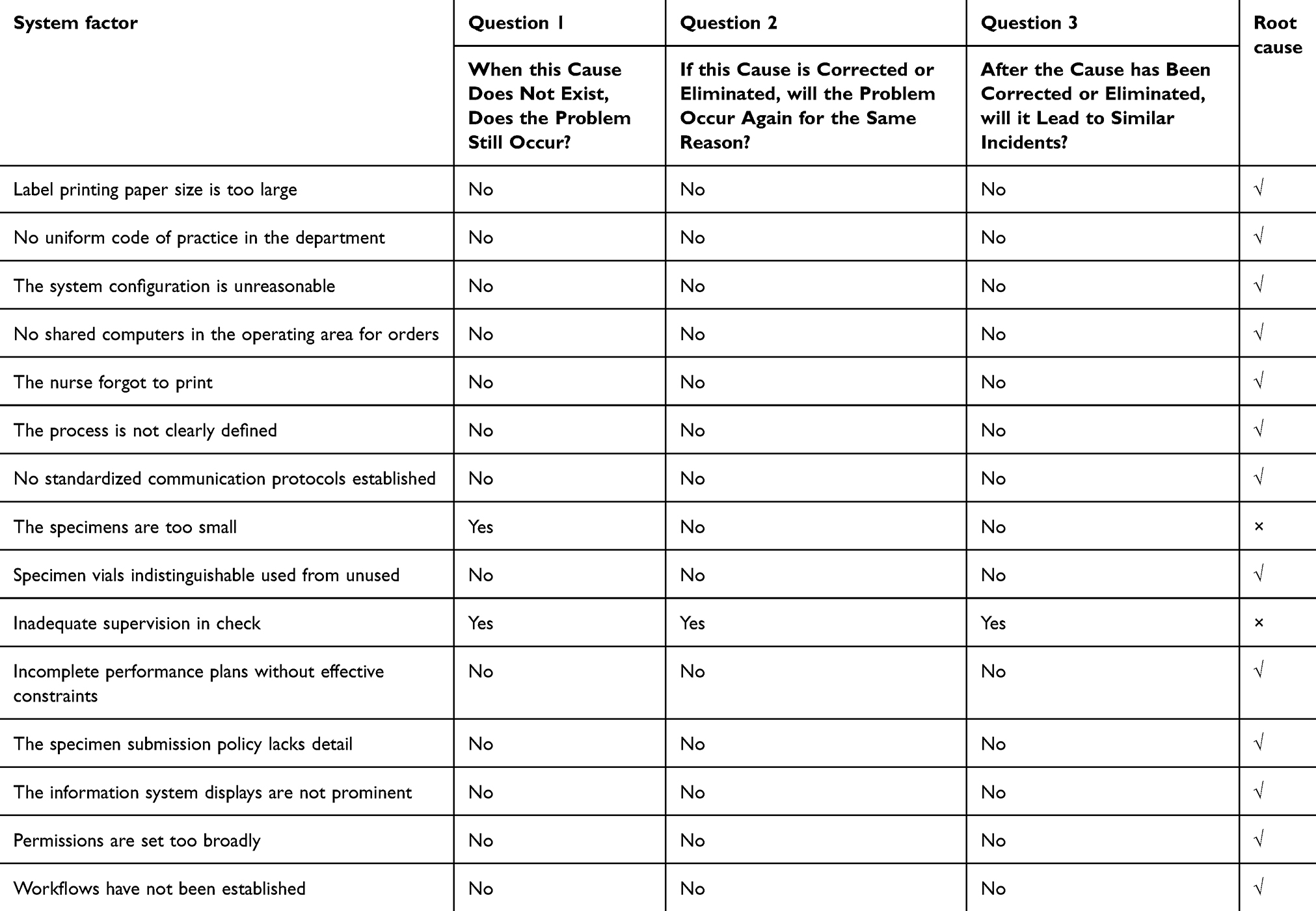 |
Table 1 Systemic Root Cause Analysis |
 |
Figure 3 Identify root cause contributing factors. |
Interventions
As shown in Table 2, to address the root causes, inspired by previous studies, we have formulated three targeted intervention measures: Process redesign established mandatory preoperative pathology orders, alongside clear cross-departmental role delineation for specimen handling;20 Ergonomic innovations introduced dual-color sealing rings (white cap/red ring) on specimen bottles, enabling instant visual verification of proper sealing status;21 and digital closed-loop management integrated barcode tracking into the hospital information system, with automated alerts flagging unlogged specimens to prevent oversight.22
 |
Table 2 Developing and Implementing Improvement Actions |
However, the implementation of these interventions was not without challenges. For the process redesign, some staff resisted the changes due to concerns about increased workload and the need to adapt to new procedures. To overcome this, we organized in - depth training sessions that included both theoretical explanations of the importance of the new protocols and practical demonstrations of how to follow them. For the ergonomic innovation of dual - color sealing rings, there were initial concerns about the cost implications and compatibility with existing specimen bottles. We addressed these by conducting thorough cost - benefit analyses and collaborating closely with suppliers to ensure that the new sealing rings could be seamlessly integrated into the existing workflow. When implementing digital closed - loop management, technical glitches during system integration emerged as a major hurdle. Our IT department worked closely with the system developers, conducting extensive testing and troubleshooting to optimize the system and ensure its smooth operation. Training sessions were conducted for all these employees to ensure understanding and adherence to the new protocols, ergonomic changes, and digital tracking systems. A total of 287 employees, including surgeons, nurses, lab technicians, and administrative staff, whose roles directly impacted specimen handling workflows, were included in the interventions.These measures collectively fortified safeguards across the entire specimen journey, spanning preoperative protocols to postoperative tracking, thereby closing systemic gaps identified in the RCA.
Evaluation Metrics
The intervention’s effectiveness was evaluated through a structured, hierarchical framework aligned with the RCA-identified systemic vulnerabilities.
Clinical Outcome Metrics
Clinical outcome metrics centered on ensuring specimen integrity and safety throughout the handling process. Specimen integrity preservation was evaluated by systematically monitoring recurrence rates of loss events, while safety verification efficacy was assessed through enhancements in the reliability of sealing confirmation mechanisms, ensuring tamper-evident protocols were consistently maintained. These dual metrics collectively validated the intervention’s capacity to safeguard specimens from pre-collection to final analysis.
Process Compliance Metrics
Process compliance metrics evaluated specimen workflow standardization. Preoperative protocol adherence was measured through pathology order compliance, while documentation accuracy focused on labeling error tracking to mitigate traceability risks. These metrics ensured procedural fidelity and resolved preoperative-postoperative coordination gaps.
System-Level Impact Metrics
System-level impact metrics focused on organizational and translational impact. Staff competency was tracked through participation in updated protocol training, while scalability was monitored via external partnerships adopting RCA innovations like dual-color sealing systems and closed-loop tracking.
Results
Inspection Results
Members of the RCA quality management team collected data on indicators related to the loss of pathological specimens during two sampling periods (9 September to 27 September 2022 and 12 February to 26 February 2023). We examined 96 patients undergoing transrectal prostate biopsy procedures.
Evaluation of Direct Quantitative Indicators Before and After the Implementation of RCA
After adopting the split design for the sealing ring of specimen vials, the post-use recognition rate of specimen vials increased from 0% before the implementation of RCA to 100% after the implementation of RCA, which is an effective improvement measure. Our joint hospital information research and development centre introduced a closed-loop management design based on the existing pathology specimen management information system. After the implementation of the following three measures, ie, the implementation of the information system’s anti-defective settings, the setting of the information alert function, and the design of the registration page for pathology specimens using the “colour differentiation method”. There has been no adverse event of loss of surgical pathology specimen for 2 years since the occurrence of the adverse event. The printing rate of specimen identification codes has increased from 97% to 100%, the issuance rate of preoperative pathology orders has increased from 14% to 100%, and the rate of pre-pricing surgical pathology specimens has decreased from 100% to 0%. Significant improvements were achieved in all the above quantitative indicators. (The results as shown in Table 3)
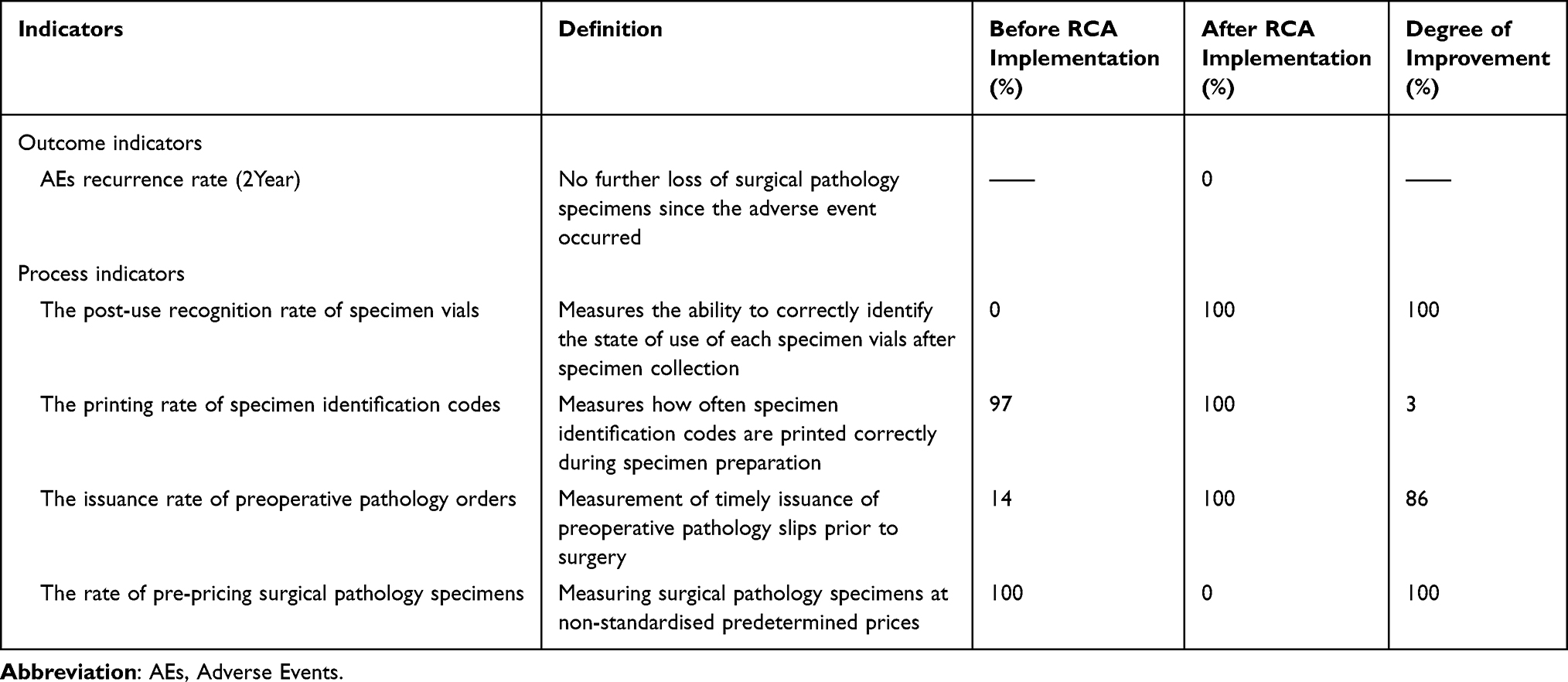 |
Table 3 Evaluation of Direct Quantitative Indicators Before and After the Implementation of RCA |
Evaluation of Indirect Derived Indicators Before and After the Implementation of RCA
The quality management department, in collaboration with the hospital quality and safety management committee, organized three training sessions for surgeons, nurses, lab technicians, and administrative staff to disseminate the findings of the RCA report on “missing” pathology specimens that led to a patient undergoing a repeat prostate biopsy. A total of 1,500 surgical and clinical managers attended these post - intervention training sessions, The trainings were a part of the post - intervention efforts to enhance awareness and improve practices related to specimen handling across the hospital.
We also promoted the innovative split design of sample vial seals and the application of the color differentiation method on the pathology specimen registration page. These innovations have been shared with 14 healthcare institutions. The RCA report was awarded the gold medal at the 2024 hospital quality management competition in Zhejiang Province, Mainland China, highlighting its practical significance in improving patient safety culture.
To further strengthen the rigor of our study and assess the long term effectiveness of the interventions, we are conducting a follow up evaluation. We plan to collect data six months and one year after the implementation of the interventions, focusing on process compliance, staff feedback, and the recurrence rate of specimen related errors. This follow up will provide more comprehensive evidence of the sustainability of the RCA - based improvements.
Discussion
Clinical Implications
Our study successfully addressed the issue of lost surgical pathology specimens through systematic improvements and innovations. The investigation utilized RCA, a quality improvement tool, to examine how local specimen handling processes interact with systemic medical error management. By implementing a dual-color sealing ring system and integrating closed-loop management into our pathology specimen information system, we achieved a significant enhancement in specimen recognition and management efficiency. Following these interventions, we observed a marked increase in specimen identification accuracy and operational effectiveness across multiple quantitative metrics. Moreover, our comprehensive training initiatives and knowledge sharing efforts further reinforced these improvements within our institution and beyond, impacting a wide range of healthcare facilities. These outcomes underscore the efficacy of proactive quality management strategies in mitigating risks and enhancing patient safety in surgical pathology practices.
Surgical specimen management is a multifaceted and error - prone process from the time the surgeon identifies the need to collect a surgical specimen.23 There are multiple steps and people involved in the specimen handling process. Errors can occur at any stage of the process, but most occur during the pre - analytical stage, ie, the period before the surgical specimen is collected until it is sent to the laboratory.2 One study showed that the incidence of errors related to surgical specimens in the pre - analytical phase ranged from 45% to 71%.24 Further studies have found that the most common error causing loss of surgical specimens is mixing of specimens between two patients.25 The surgical specimen error addressed in this study also falls under the issue of specimen mixing between two patients. This is an enduring and popular topic that has prompted researchers to continue to explore and make discoveries.
Previous studies have shown that concerns about the problem of lost surgical pathology specimens usually focus on process management and joint multidisciplinary management.26,27 To reduce this problem, previous studies have focused on measures such as overall process optimisation and improved communication.26,27 However, these studies have mostly focused on the outcome facet indicator of surgical specimen loss rate in the presentation of results, and less on process facet specific indicators.26–28 The innovation of this study is that it focuses on the development and implementation of systematic measures that focus on the root causes, not only optimising the process but also focusing on addressing the development of assistive technology at the operational level.
Such innovative reform measures face challenges in implementation.29 Firstly, technological integration posed a significant hurdle. Integrating the digital closed - loop management system into the existing hospital information system required extensive technical support and coordination between different departments.30 Compatibility issues with legacy systems led to initial delays, and ensuring data security during the transition was a constant concern. Secondly, staff resistance to change was another major challenge.31 The introduction of new tools like the dual - color sealing rings and the revised specimen handling protocols meant that employees had to unlearn old habits and adapt to new ways of working. Some staff members were skeptical about the effectiveness of these new measures, and training them to use the new systems proficiently required substantial time and resources. Thirdly, financial constraints played a role.32 Developing and purchasing the new sealing rings and implementing the digital tracking system required a significant investment, which had to be carefully justified within the hospital’s budgetary limitations.
These challenges were highly relevant to our study as they highlight the real - world complexities of translating theoretical RCA - based solutions into practical, sustainable improvements. Understanding and addressing these barriers were essential for the successful implementation of our interventions and for ensuring that the improvements were not only effective in the short - term but also sustainable in the long - run. Unlike previous studies, our study presents findings through a three - level synthesis: outcome - level indicators, process - level indicators, and educational outreach. This multilevel presentation helps to comprehensively understand and assess all aspects of the reform measures, which in turn can more effectively promote the continuous improvement of healthcare quality management and patient safety culture.
Clinical Practices
In previous quality improvement studies of lost surgical specimens, the choice of improvement tools has shown diversity, usually including Failure mode and effect analysis (FMEA),23 Quality Improvement (QI)26,27 and Plan-Do-Check-Act (PDCA).29 In this study, RCA was chosen as an improvement tool, and the methodology for applying RCA emphasises systematic analysis rather than individual responsibility, aiming to accumulate empirical data on the occurrence of events and their causes. Although many healthcare professionals have a broad understanding of RCA, there is a relative lack of practical experience.33 Therefore, it is necessary to train the team members involved in this project on RCA-related knowledge before the study was initiated to ensure that the team was able to quickly reach a consensus and move forward with the improvement project in a robust manner.34
The “Swiss cheese” conceptual model and the brainstorming methodology were applied in the discussions of the quality management team. During the discussion, all team members were actively involved in analysing and determining the causes of missing surgical pathology specimens. This discussion transformed the team members from passive performers to active participants. While RCA can improve closed-loop management of surgical pathology specimens in the short term, we are more concerned with continually tracking the effects of improvement. Our long term goal is to achieve continuous improvement in organisational planning.35
The people involved in the RCA process need to have high standards and resource-intensive qualities.36 This allows for a comprehensive grasp and multiple coordination when optimising the process and coordinating its advancement. The RCA team members for this project included a quality manager with a senior quality manager qualification for healthcare organisations, proficiency in RCA and other management tools, and a background in healthcare education, who was responsible for the overall facilitation and coaching of the project. Therefore, careful trade-offs are required when undertaking a comprehensive RCA improvement project in a staff-constrained organisation.
Limitations
This study has a number of limitations, as described below. First, this study was based on a single case RCA at a hospital level, and the findings are not easily transferable to a different setting or hospital. These strategies can serve as a template for other institutions to diagnose and address analogous systemic failures, even as broader validation is warranted. Future research should prioritize multi-center studies to further assess the interventions’ broader feasibility. Second, the evaluation period for the effectiveness of the interventions was limited to six months, which may not fully reflect the long-term sustainability of the improvements. Third, during the research process, we did not interview patients and their families. This was mainly due to ethical and practical concerns. The sentinel event had already brought emotional stress to the patient and family, and we worried that additional interviews might cause further harm. In future research, we will design a more comprehensive approach, guided by ethics committees, to incorporate the perspectives of patients and families, aiming to gain a more complete understanding of the incident and improve our quality improvement measures from the patient - experience perspective.
Conclusion
The RCA-driven reforms effectively addressed systemic flaws in specimen management, demonstrating that targeted process redesign, ergonomic tools, and digital tracking can mitigate risks of medical errors. While the single-hospital setting and short evaluation period limit generalizability, the study highlights the value of systemic workflow analysis and provides a replicable template for other institutions to address similar issues, with broader validation needed via future multi-center research.
Data Sharing Statement
All data underlying the findings are within the paper.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki. All research methods were performed in accordance with relevant guidelines and regulations. The study was approved by the Ethics Committee of Taizhou First People’s Hospital [Ethical Approval No. 2024-KY034-01]. All participants gave verbal informed consent to participate in this study. The medical ethics committee of the authors’ institution approved the verbal informed consent procedure for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported from the medical quality (evidence-based) management by the Institute of Hospital Management, National Health Commission (Project Number: YLZLXZ24G132), and the sustainable development of kang’enbei research project of zhejiang provincial hospital association (2023ZHA-KEB335). The funding bodies observed during some data collection but was not involved in the study design, analysis of data, interpretation of fndings, or writing the manuscript. No funding was received. There was no additional financial support from public or private sources.
Disclosure
The authors have declared that there are no conflicts of interest, given their final approval, and agreed to be responsible for all aspects of the work that ensures accuracy and integrity.
References
1. Donaldson MS, Corrigan JM, Kohn LT. To Err Is Human: Building a Safer Health System. National Academies Press; 2000.
2. Vm S, Williams TL, Szekendi MK, Halverson AL, Dintzis SM, Pavkovic S. Surgical specimen management: a descriptive study of 648 adverse events and near misses. Arch Pathol Lab Med. 2016;140(12):1390–1396. doi:10.5858/arpa.2016-0021-OA
3. Kellogg KM, Hettinger Z, Shah M, et al. Our current approach to root cause analysis: is it contributing to our failure to improve patient safety? BMJ Qual Saf. 2017;26(5):381–387. doi:10.1136/bmjqs-2016-005991
4. The Joint Commission. Framework for conducting a root cause analysis and action plan. The Joint Commission. 2018. https://www.jointcommission.org/resources/sentinel-event/.
5. NHS England Patient Safety Domain. Serious Incident Framework. England: NHS; 2015.
6. National Patient Safety Agency (NPSA). National framework for reporting and learning from serious incidents requiring investigation. NPSA, 2009.
7. South Australia Health. Root Cause Analysis. Government of South Australia. 2016. Available from: https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa +health+internet/clinical+resources/safety+and+quality/governance+for +safety+and+quality/root+cause+analysis+rca.
8. Abela G. Root cause analysis to identify contributing factors for the development of hospital acquired pressure injuries. J Tissue Viability. 2021;30(3):339–345. doi:10.1016/j.jtv.2021.04.004
9. Mezemir R, Seid A, Gishu T, Demas T, Gize A. Prevalence and root causes of surgical site infections at an academic trauma and burn center in Ethiopia: a cross-sectional study. Patient Saf Surg. 2020;14:3. doi:10.1186/s13037-019-0229-x
10. Peerally MF, Carr S, Waring J, Dixon-Woods M. The problem with root cause analysis. BMJ Qual Saf. 2017;26(5):417–422. doi:10.1136/bmjqs-2016-005511
11. Card AJ, Ward J, Clarkson PJ. Successful risk assessment may not always lead to successful risk control: a systematic literature review of risk control after root cause analysis. J Healthc Risk Manag. 2012;31(3):6–12. doi:10.1002/jhrm.20090
12. Rakha EA, Clark D, Chohan BS. Efficacy of an incident-reporting system in cellular pathology: a practical experience. J Clin Pathol. 2012;65(7):643–648. doi:10.1136/jclinpath-2011-200453
13. Foglia E, Garagiola E, Ferrario L, Plebani M. Performance evaluation of the introduction of full sample traceability system within the specimen collection process. Clin Chem Lab Med. 2024;63(4):723–733. doi:10.1515/cclm-2024-0854
14. China Hospital Quality Circle Alliance. Root Cause Analysis, 2022. Available from: http://www.cfhqcc.org.cn.
15. Rooney JJ, Heuvel LN. Root cause analysis for beginners. Qual Progr. 2004;37(7):45–56.
16. Meadows S, Baker K, Butler J. The incident decision tree: guidelines for action following patient safety incidents. In: Henriksen K, Battles JB, Marks ES, Lewin DI, editors.Advances in Patient Safety: From Research to Implementation (Volume 4: Programs, Tools, and Products);Rockville (MD);Agency for Healthcare Research and Quality (US);2005.
17. Senders JW. FMEA and RCA: the mantras of modern risk management. Qual Saf Health Care. 2004;13(4):249–250. doi:10.1136/qhc.13.4.249
18. Reason JT. Human Error. Cambridge, England: Cambridge University Press; 1990.
19. Stein JE, Heiss K. The Swiss cheese model of adverse event occurrence--Closing the holes. Semin Pediatr Surg. 2015;24(6):278–282. doi:10.1053/j.sempedsurg.2015.08.003
20. Letelier P, Guzmán N, Medina G, et al. Workflow optimization in a clinical laboratory using Lean management principles in the pre-analytical phase. J Med Biochem.;40(1):26–32. doi:10.5937/jomb0-26055.
21. Bix L, Seo DC, Ladoni M, Brunk E, Becker MW. Evaluating varied label designs for use with medical devices: optimized labels outperform existing labels in the correct selection of devices and time to select. PLoS One. 2016;11(11):e0165002. doi:10.1371/journal.pone.0165002
22. Norgan AP, Simon KE, Feehan BA. Radio-frequency identification specimen tracking to improve quality in anatomic pathology. Arch Pathol Lab Med. 2020;144(2):189–195. doi:10.5858/arpa.2019-0011-OA
23. Link T. Guidelines in Practice: specimen Management. AORN J. 2021;114(5):443–455. doi:10.1002/aorn.13518
24. ECRI Institute. Where Do Most Lab Errors Occur? Not the Lab. PSO Monthly Brief. West Conshohocken (PA): ECRI Institute; 2012.
25. Troxel DB. Error in surgical pathology. Am J Surg Pathol. 2004;28(8):1092–1095. doi:10.1097/01.pas.0000126772.42945.5c
26. Holstine JB, Samora JB. Reducing surgical specimen errors through multidisciplinary quality improvement. Jt Comm J Qual Patient Saf. 2021;47(9):563–571. doi:10.1016/j.jcjq.2021.04.003
27. Morris AM. A multidisciplinary approach for reducing lost surgical specimens. AORN J. 2020;111(6):691–698. doi:10.1002/aorn.13061
28. Valenstein PN, Raab SS, Walsh MK. Identification errors involving clinical laboratories: a College of American Pathologists Q- Probes study of patient and specimen identification errors at 120 institutions. Arch Pathol Lab Med. 2006;130(8):1106–1113. doi:10.5858/2006-130-1106-IEICL
29. Minato H, Nojima T, Nakano M, Yamazaki M. Safety management in pathologylaboratory: from specimen handling to confirmation of reports. Rinsho Byori. 2011;59(3):299–304.
30. Albulushi A, Al Kindi DI, Moawwad N. Digital health technologies in enhancing patient and caregiver engagement in heart failure management: opportunities and challenges. Int J Cardiol. 408;132116. doi:10.1016/j.ijcard.2024.132116
31. Xue Z, M NNS, Cheng Y, et al. Overcoming resistance to innovation: strategies and change management. J Business Innovation. 2024;9(1):32.
32. Alexander JA, Weiner BJ, Griffith J. Quality improvement and hospital financial performance. J Organizational Behav. 2006;27(7):1003–1029. doi:10.1002/job.401
33. Balakrishnan K, Brenner MJ, Gosbee JW, Schmalbach CE. Patient safety/quality improvement primer, part ii: prevention of harm through root cause analysis and action (RCA2). Otolaryngol Head Neck Surg. 2019;161(6):911–921. doi:10.1177/0194599819878683
34. Gottula JL, Hope ER, Wood TA, Medla SA, Saunders RD, Keyser EA. rapid root cause analysis: improving OBGYN resident exposure to quality improvement and patient safety curricula. Cureus. 2024;16(3):e56881. doi:10.7759/cureus.56881
35. Jiang S, Yi L, Chen Y, Hu R. Optimizing sterilization packaging through root cause analysis: an exploration into sealing defects of paper-plastic pouches. Med Sci Monit. 2023;29:e940342. doi:10.12659/MSM.940342
36. Liepelt S, Sundal H, Kirchhoff R. Team experiences of the root cause analysis process after a sentinel event: a qualitative case study. BMC Health Serv Res. 2023;23(1):1224. doi:10.1186/s12913-023-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Literature Review of Safety Culture in Hemodialysis Settings
Albreiki S, Alqaryuti A, Alameri T, Aljneibi A, Simsekler MCE, Anwar S, Lentine KL
Journal of Multidisciplinary Healthcare 2023, 16:1011-1022
Published Date: 11 April 2023
Public Perception of Medical Errors and Confusion About Medical Complications: Implications for Healthcare Safety in Saudi Arabia
Alhewiti A
International Journal of General Medicine 2025, 18:2093-2106
Published Date: 12 April 2025