")
Back to Journals » Journal of Pain Research » Volume 18
Ultrasound-Guided vs Non-Guided Pharmacopuncture for Cervical Myofascial Pain Syndrome: A Multi-Center Prospective Comparative Study Protocol
Authors Kim K , Song J, Chu H , Kwon R, Park S, Kwon J, Hong HJ, Lee Y, Kwon S, Kang K, Leem J , Kim CH
Received 24 December 2024
Accepted for publication 12 March 2025
Published 19 March 2025 Volume 2025:18 Pages 1417—1431
DOI https://doi.org/10.2147/JPR.S509236
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Kwangho Kim,1 Juhwan Song,1 Hongmin Chu,1,2 Robin Kwon,1,3 Seongjun Park,1,4 Junhui Kwon,1,5 Hyeon Joon Hong,1,6 Youngyun Lee,1,7 Sanghyuk Kwon,1,3 Kyungho Kang,1,8 Jungtae Leem,9,10 Cheol-Hyun Kim1,11
1The Academy of Korean Medicine Clinical Anatomy, Seoul, Korea; 2Mapo Hongik Korean Medicine Clinic, Seoul, Korea; 3Department of Korean Medicine, Jinjeop Hanyang Hospital, Namyangju, Korea; 4Mullae Majubom Korean Medicine Clinic, Seoul, Korea; 5Anjung Korean Medicine Clinic, Seoul, Korea; 6Gwanghwamun Kyung Hee Korean Medicine Clinic, Seoul, Korea; 7Kangnyung Korean Medicine Clinic, Anyang, Korea; 8Yangjae Chungwoo Korean Medicine Clinic, Seoul, Korea; 9Research Center of Traditional Korean Medicine, College of Korean Medicine, Wonkwang University, Iksan, Korea; 10Department of Diagnostics, College of Korean Medicine, Wonkwang University, Iksan, Korea; 11Department of Internal Medicine, College of Korean Medicine, Wonkwang University, Iksan, Korea
Correspondence: Jungtae Leem, Department of Diagnostics, College of Korean Medicine, Wonkwang University, Iksan, Korea, Tel +82-63-850-6984, Fax +82-63-850-6985, Email [email protected] Cheol-Hyun Kim, Department of Internal Medicine, College of Korean Medicine, Wonkwang University, Iksan, Korea, Tel +82-62-670-6412, Fax +82-62-670-6492, Email [email protected]
Purpose: Cervical Myofascial Pain Syndrome (CMPS) is a common musculoskeletal disorder that significantly impacts daily life due to pain and restricted movement. This study focuses on Ultrasound-Guided Pharmacopuncture(UGP) to release fascial restrictions and alleviate nerve compression. By utilizing real-time ultrasound imaging, UGP is expected to enhance treatment accuracy, reduce adverse events, and improve clinical outcomes. This study aims to assess the efficacy and safety of UGP compared to Non-Guided Pharmacopuncture (NGP) in patients with acute CMPS.
Patients and Methods: This multi-center prospective observational comparative study evaluates the efficacy and safety of UGP versus NGP in patients with acute CMPS. A minimum of 100 patients with acute CMPS (≤ 7 days since symptom onset) will be recruited from two hospitals and five Korean medicine clinics. Participants will be randomly assigned to either the UGP group (receiving ultrasound-guided pharmacopuncture with Hominis Placenta(HP) solution) or the NGP group (receiving non-guided pharmacopuncture with HP solution). A single treatment session will be conducted, with pre- and post-treatment assessments using the Numerical Rating Scale (NRS), Pressure Pain Threshold (PPT), and Range of Motion (ROM). Additionally, a follow-up safety assessment will be conducted via telephone 24– 36 hours post-treatment.
Discussion and Conclusion: This study is the first to evaluate the efficacy and safety of ultrasound-guided HP pharmacopuncture for acute CMPS in a multi-center prospective comparative study. The findings are expected to provide comprehensive evidence supporting ultrasound-guided pharmacopuncture as an effective treatment for myofascial pain and may expand its clinical applications, particularly in Korean medicine clinics.
Keywords: ultrasonography, acupuncture therapy, pharmacopuncture, myofascial pain syndrome, needle guidance technique
Introduction
Visual Display Terminal (VDT) Syndrome, sometimes referred to as a modern occupational disease, encompasses Cervical Myofascial Pain Syndrome (CMPS) as one of its manifestations.1 In 2019, approximately 7.8 million individuals in South Korea received treatment for VDT Syndrome, incurring total medical expenses of 824.8 billion KRW.1
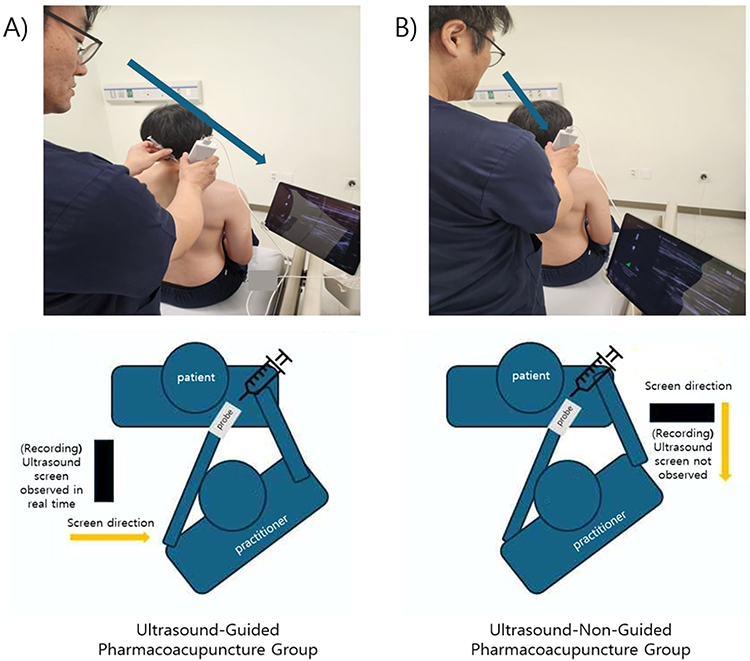 |
Figure 1 Treatment Methods of Ultrasound-Guided Pharmacopuncture(UGP) Group and ultrasound-Non-Guided Pharmacopuncture (NGP) Group: The arrows in the figure indicate the direction the practitioner is looking at during the procedure. (A) In the UGP Group, the patient is unable to see the ultrasound screen while the practitioner performs the procedure by looking at the ultrasound screen. (B) In the NGP Group, both the practitioner and the patient do not view the ultrasound screen during the procedure. The practitioner depicted in the image has provided informed consent for the publication of this figure. |
 |
Figure 2 Location Information of the Participating Institutions: A total of seven medical facilities are participating in this study, including two hospitals and five Korean medicine clinics located in South Korea. |
 |
Figure 3 The Contact of the Ultrasound Transducer with the Affected Site: The ultrasound probe is placed on the SLS (Splenius Capitis, Levator Scapulae, and Serratus Posterior Superior) Triangle area to perform the ultrasound scan. |
 |
Figure 4 Ultrasound Screen Image of SLS (Splenius Capitis, Levator Scapulae, and Serratus Posterior Superior) Triangle: (A) The practitioner confirms the positions of the Splenius Capitis, Levator Scapulae, and Trapezius muscles through the ultrasound screen. (B) The Needle Guiding System (NGS) detects both the position and direction of the magnetized needle while the probe is in place in the SLS Triangle area. |
Myofascial Pain Syndrome (MPS) is a common musculoskeletal condition, with an estimated lifetime prevalence of up to 85% in the general population, varying between males and females.2 It has been identified as a major cause of chronic pain, accounting for 54.6% of chronic head and neck pain cases.3 Additionally, studies have reported that MPS affects approximately 85% of patients attending chronic pain clinics and 30% of those visiting internal medicine clinics.3
CMPS, a subtype of MPS, is a prevalent musculoskeletal pain condition characterized by both acute and chronic pain, as well as discomfort resulting from stress-induced stiffness in the muscles and fascia surrounding the neck.1,4 One of the primary causes of this syndrome is the shortening of the Levator Scapulae muscle.1,5 A shortened Levator Scapulae can lead to internal rotation and elevation of the scapula, which places continuous strain on the shoulder muscles and joints.5 This strain can potentially result in movement disorders and muscle deformities.5
CMPS has a significant impact on individuals, their families, communities, healthcare systems, and businesses.6 One study indicates that when CMPS becomes chronic, it can significantly diminish quality of life and lead to considerable disability and economic costs.4 Furthermore, a recent projection of disease burden and life expectancy to 2050 indicates that the global health status will increasingly be affected by Non-Communicable Diseases (NCDs), with the proportion of the disease burden attributable to NCDs expected to grow considerably.7 These findings emphasize that prompt and effective management of CMPS is essential for reducing the global healthcare burden.
Ultrasound-Guided Acupuncture (UGA) has been increasingly utilized worldwide due to its effectiveness and safety.8 Research efforts have focused on improving procedural accuracy and minimizing complications.9–11 In 2018, The Korea Institute of Oriental Medicine in South Korea published the “High-Risk Area Ultrasound-Guided Acupuncture Handbook”, which introduced ultrasound applications to enhance needling safety from the initial insertion stage.12
By providing real-time visualization of anatomical structures, UGA improves treatment precision while reducing potential adverse effects.8 In this study, UGA is expected to provide a safer and more precise intervention compared to Non-Guided Acupuncture (NGA) and other major invasive procedures.
According to a study on ultrasound-guided procedures, ultrasound guidance enables real-time visualization of anatomical structures, allowing for the identification of the Spinal Accessory Nerve (SAN) within the interfascial plane between the Levator Scapulae and Trapezius muscles, as well as the Dorsal Scapular Nerve (DSN) located beneath the Levator Scapulae and Rhomboid muscles. This plays a crucial role in preventing nerve injury during procedures. In fact, the application of ultrasound guidance in local procedures is expected to reduce the risk of unintended iatrogenic injury.13
Building on these advancements, the authors of this study have focused on methods for releasing fascial restrictions to alleviate Dorsal Scapular Nerve compression, which occurs between muscles and leads to pain and restricted motion. Previous case reports have documented the effectiveness of this approach, particularly in treating movement limitations and pain.14–16
In 2024, the authors published a case report in the Korean Journal of Acupuncture, emphasizing the successful application of Ultrasound-Guided Pharmacopuncture (UGP) at the interfascial space of the Splenius Capitis, Levator Scapulae, and Serratus Posterior Superior muscles (known as the “SLS triangle”) for the treatment of acute CMPS.1
Although various studies have investigated UGA for CMPS, research on UGP remains limited on a global scale. Most existing studies are single-center trials or retrospective analyses, which lack large-scale comparative data. To overcome these limitations, this study has been designed as a multi-center prospective comparative study involving two hospitals and five Korean medicine clinics. By providing a broader evaluation of UGP in primary care settings, this research aims to validate its safety and efficacy while expanding its clinical applications in ultrasound-guided interventions.
Materials and Methods
Study Registration
The This study was registered with the Clinical Research Information Service (CRIS) of the Korea National Institute of Health (NIH), Republic of Korea (KCT0009932, Trial Status: Protocol version 1.2 (2024.09.06)).
Study Design
The aim of this prospective comparative observational study is to evaluate the efficacy and safety of UGP treatment in patients with acute MPS complaining of neck and shoulder muscle pain. The treatment involves injecting the Hominis Placenta (HP) Pharmacopuncture solution into the interfascial space at the intersection of the Splenius Capitis, Levator Scapulae, and Serratus Posterior Superior muscles (SLS Triangle) under ultrasound guidance.
Subjects who voluntarily sign a written informed consent form after receiving sufficient explanation about the study will undergo screening through an assessment of inclusion and exclusion criteria. The screening process will include consent acquisition, determination of eligibility based on criteria, demographic data collection, and medical history assessment. If deemed suitable as a prospective comparative observational study patient after screening, the first intervention will be conducted immediately following the acquisition of consent. Eligible subjects will then be assigned to the registry.
Eligible subjects will be assigned to either the Ultrasound-Guided Pharmacopuncture (UGP) Group or the Non-Guided Pharmacopuncture (NGP) Group for this study. This clinical study will be conducted in a primary outpatient department setting as a foundational observational prospective study aimed at calculating effect size for future Randomized Controlled Trial (RCT) design. Site-based allocation will be implemented, with each institution assigning a different recruitment group.
Both groups will have a single treatment visit, during which evaluations of pain will be conducted using the Numerical Rating Scale (NRS), Pressure Pain Threshold (PPT), and Range of Motion (ROM) both before and immediately after the ultrasound-guided Pharmacopuncture treatment. Additionally, a follow-up assessment for adverse reactions will be conducted via telephone between 24 and 36 hours after the treatment. The detailed study procedure is shown in Table 1.
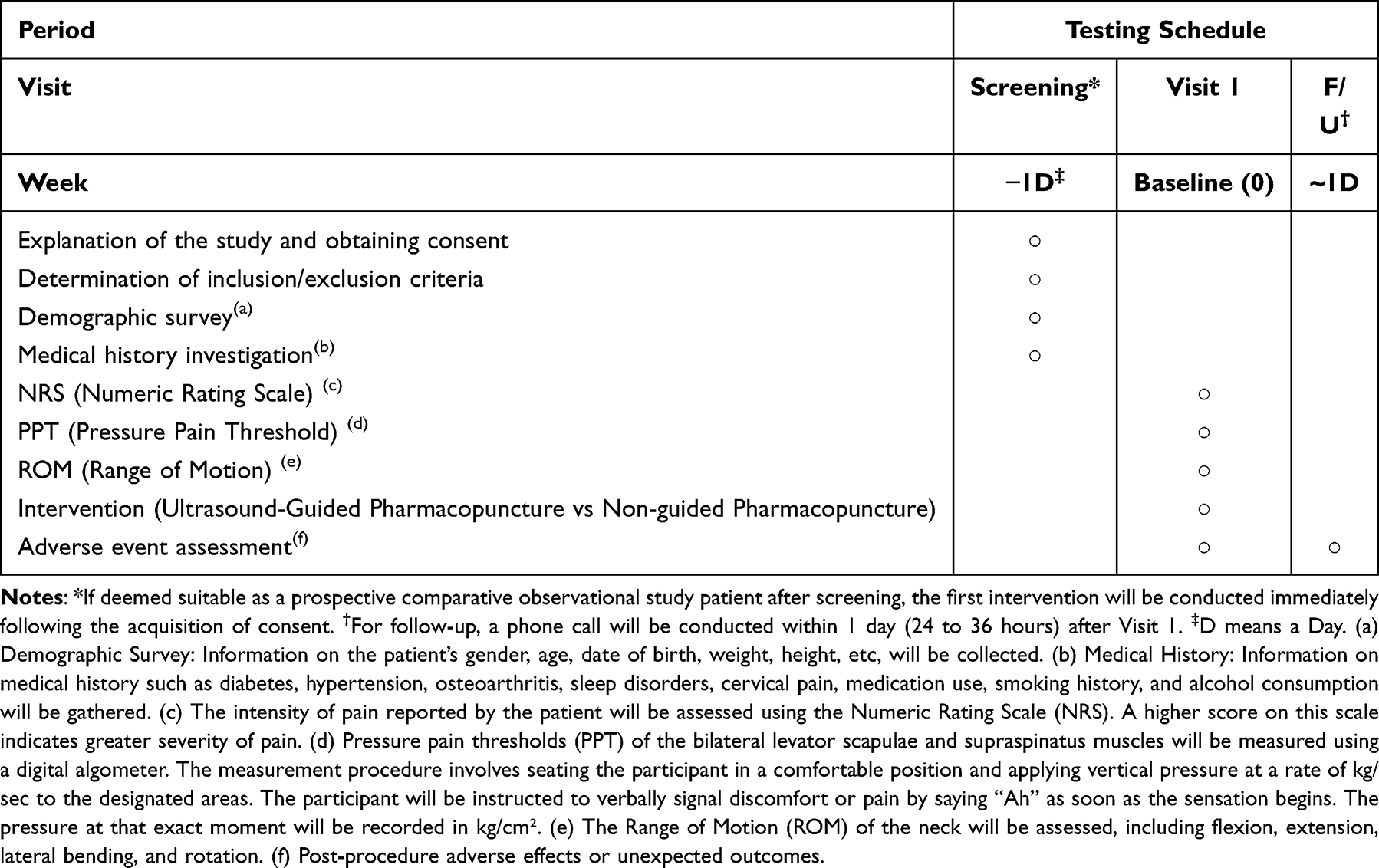 |
Table 1 Prospective Clinical Research Progress |
In both groups, only HP Pharmacopuncture treatment will be administered to consenting patients. In the UGP Group, the practitioner will visualize the ultrasound screen and injects the solution at the SLS triangle area, which is located in the interfascial plane between the three muscles. During this process, the practitioner will monitor the ultrasound screen, while the patient will not have access to it. In the NGP Group, the practitioner will estimate the location of the SLS Triangle through palpation, then apply the ultrasound probe to that location before administering the Pharmacopuncture treatment. In this case, neither the practitioner nor the patient will view the ultrasound screen. The methods for Pharmacopuncture treatment in both groups are illustrated in Figure 1.
The study protocol has been approved by the Institutional Review Board (IRB) of Wonkwang University Gwangju Medical Center (approval number: WKIRB-2024/10-3), and informed consent will be obtained from each participant.
The clinical trial will be conducted from the enrollment of the first patient and will continue until 100 participants have been recruited. The IRB has approved a study period of one year from the date of approval, concluding on December 31, 2025. However, the study will be terminated early if participant recruitment is completed ahead of schedule.
Participants
This study will be conducted on patients with acute myofascial pain syndrome in the cervical region. In this context, all aspects of the study’s purpose, potential adverse reactions, and safety will be thoroughly explained to the clinical research participants before the study begins. Written consent will be obtained from the participants, indicating their voluntary decision to participate in the research.
In this study, patients with Cervical Myofascial Pain Syndrome (CMPS) with symptom onset within the past seven days will be included.
MPS is classified as either acute or chronic, with chronic cases tending to be more widespread and involving additional factors such as anxiety and depression.17,18 Since chronic MPS presents confounding factors that may influence pain perception and treatment response, this study is designed specifically to focus on acute-phase cases.18,19 This approach ensures a more homogeneous study population and enhances the accuracy of treatment effect assessments.
While there is some controversy regarding the definition of acute pain, with previous studies defining it as lasting either 4 or 6 weeks, this study adopts a 7-day symptom onset limit to establish a clearly defined acute-phase population and prevent transitions into the subacute phase, which may introduce variability in treatment responses.18
This criterion aligns with previous studies that have assessed acute MPS within strict timeframes, including those that set a 48-hour limit for Acute Low Back Pain and a 7-day inclusion criterion for Upper Trapezius MPS.20,21 In contrast, research on subacute and chronic neck pain has used a minimum duration of 2 weeks as an inclusion criterion.22
Establishing this 7-day inclusion criterion ensures methodological consistency and enhances the validity of the study’s outcome assessments.
Setting
This study will be conducted in two hospitals and five Korean medicine clinics located in the Republic of Korea. All subjects will be recruited from the outpatient department of the participating medical institutions. The locations of the hospitals and clinics are shown in Figure 2.
Only medical professionals who are members of The Academy of Korean Medicine Clinical Anatomy, a specialized ultrasound research society composed exclusively of Korean medicine doctors, and who have completed at least three formal training sessions on ultrasound-guided pharmacopuncture, are eligible to participate in this study.
Inclusion Criteria
All study participants can only participate in the prospective comparative observational study if they meet all of the following criteria:
(1) Adults aged 20 to 64 years.
(2) Individuals who have experienced acute cervical pain within the past 7 days and are complaining of cervical pain and range of motion restrictions.
(3) Individuals diagnosed with acute cervical myofascial pain syndrome at the outpatient clinic of the conducting medical institution or other medical facilities.
(4) Individuals who have not received treatment for acute cervical myofascial pain syndrome at other hospitals after being diagnosed.
(5) Individuals who voluntarily decide to participate in this study and sign an informed consent form.
Exclusion Criteria
(1) Individuals who have taken medication or received related treatments for muscle pain or discomfort in the neck or shoulder area that occurred within the past 7 days (including both Western and Korean medicine).
(2) Individuals with a surgical history in the cervical area within the past 3 months.
(3) Individuals who have experienced a sprain in the cervical area due to trauma, such as a traffic accident or contusion, within the past 3 months.
(4) (For women only) Individuals who are pregnant or have given birth within the past 6 months.
(5) Individuals with symptoms such as edema due to diseases of the renal endocrine system.
(6) Patients currently taking anticoagulants.
(7) Individuals whose cognitive function is impaired, making it difficult to understand the consent form and provide voluntary consent.
(8) Individuals taking psychiatric medications due to reasons such as depression.
(9) Any other individuals deemed unsuitable for participation in the study by the medical staff.
Early Termination Criteria
If the research team determines that the circumstances observed during the study involving the prospective comparative observational study participant make it difficult to continue the study.
(1) If there are safety issues with the medical device or if the medical device’s item approval is revoked.
(2) If violations of GCP, the prospective comparative observational study protocol, contractual agreements, or relevant laws and regulations by the conducting institution or research team raise concerns about the continuation of the study.
(3) Other administrative reasons that may significantly impact the continuation of the prospective comparative observational study.
If the prospective comparative observational study is discontinued, the principal investigator must compile the case records of participants up to the point of discontinuation, along with the study’s progress and results, and provide this information to the study sponsor. Additionally, all study-related materials (case records, medical devices used in the study, and the investigator’s brochure) must be returned to the study sponsor.
Dropout Criteria
(1) If the prospective comparative observational study participant (or their guardian) expresses a refusal to participate in the study (withdrawal of consent).
(2) If the participant is unable to comply with the scheduled visit or investigation dates during the study period (in this prospective comparative observational study, arrangements can be made for visits within ±1 day of the planned visit date).
(3) If the participant receives the following medications or treatments during the study period:
- Medications: Non-steroidal anti-inflammatory drugs (NSAIDs), narcotic or non-narcotic analgesics, muscle relaxants, and other pharmaceuticals and over-the-counter products that act on musculoskeletal discomfort.
- Treatments: Interventions or therapies such as traditional treatments (Chuna, acupuncture, etc.) and physical therapy (manual therapy, etc.) that act on improving musculoskeletal discomfort.
(3) If the participant is deemed unsuitable for study continuation due to accidental complications.
(4) If the participant is unable to continue in the study due to death or the onset of illness.
Management of Early Termination and Dropout
In all cases of study termination and dropout, the reasons and dates of termination or dropout must be recorded in the case records and the participants’ medical records. To determine whether the reason for the participant’s dropout is related to an adverse event, a follow-up investigation should be conducted if possible. In the case of an adverse event, the results must be reported according to the safety evaluation criteria, assessment methods, and reporting procedures that include the adverse events. Additionally, if side effects arising from the prospective comparative observational study occur, the participant will receive supportive treatment according to the treatment guidelines of the respective institution. Participants who drop out cannot rejoin the prospective comparative observational study.
Participant Recruitment Plan
Announcements will be posted in hospitals and local communities near the clinical research institution. Additionally, patient recruitment will be conducted through online advertising, including blogs.
Registration of Participants
Patients with acute myofascial pain syndrome will be the focus of this clinical study. After receiving a comprehensive explanation of the study, patients who voluntarily sign the informed consent form for a prospective comparative observational study will undergo an assessment to determine their eligibility based on inclusion and exclusion criteria. Those who meet these criteria will be enrolled in the registry. Following their enrollment, participants’ medical information related to their treatment will be collected throughout the course of their care.
Intervention
AcuViz Pocket Ultrasound Device (FCU Corp., Korea) and Magnetic Needle
The AcuViz Pocket is an ultrasound diagnostic device equipped with a magnet sensor that can track a magnetized acupuncture needle. This Needle Guiding System (NGS) detects both the position and direction of the magnetized needle while the probe is in place, displaying this information in relation to the ultrasound image. Consequently, the spatial position of the needle on the ultrasound image is updated in real-time, assisting the operator in visualizing the needle more effectively during ultrasound-guided needling procedures. When utilized by skilled healthcare professionals under optimal operating conditions, the AcuViz Pocket needle guidance system can achieve a precision of up to ±2 mm.
The Magnetic Needle (YONG CHANG Co., LTD., Korea) is an acupuncture-tracking device with a thickness of 26 gauge and a length of 60 mm. This needle is used for insertion at the treatment site and for injecting the Pharmacopuncture solution before removal. In this study, the procedure is conducted at the interfascial space of the Splenius Capitis, Levator Scapulae, and Serratus Posterior Superior muscles, referred to as the SLS Triangle. This location is situated near the Gyeonoesu (SI14, Jianwaishu in Chinese) along the crossing line of the Splenius Capitis and Levator Scapulae, specifically targeting an area of pain within a zone approximately 5 cm in diameter, where tenderness is most pronounced.
Hominis Placenta Pharmacopuncture Solution
The Pharmacopuncture solution used in this study is the Hominis Placenta(HP) Pharmacopuncture solution, produced by Anjung Korean Medicine Clinic Extramural Herbal Dispensary in South Korea.
Pharmacologically, HP is a biologically active product derived from the hydrolyzed villous tissue of the placenta obtained from healthy pregnant women.23 It contains a rich array of bioactive substances, including polydeoxyribonucleotides, RNA, DNA, peptides, amino acids, enzymes, and trace elements.24 Furthermore, HP is known to contain several cell growth factors, various interferons, and colony-forming stimulating factors, which contribute to its regenerative and therapeutic properties.25
In clinical practice, HP is typically injected into major acupuncture points along meridians, as well as alarm and transport points, to treat various conditions.26 Studies have reported that HP possesses therapeutic properties such as anti-inflammatory, antiviral, antioxidant, anti-mutagenic, and analgesic effects.26,27 These characteristics make HP pharmacopuncture a valuable treatment option for pain-related disorders.
During the HP Pharmacopuncture treatment process, there is a possibility of adverse effects such as bruising, urticaria, nausea, hypersensitivity with tingling sensations, fatigue, and localized pain.28
In this study, the HP Pharmacopuncture will be administered within a 5 cm diameter zone near the Gyeonoesu (SI14), specifically targeting the SLS Triangle, which is located in the interfascial plane between the Splenius Capitis, Levator Scapulae, and Serratus Posterior Superior muscles, where tenderness is most pronounced.
Procedure
The process of identifying and performing the procedure on the SLS Triangle via ultrasound is as follows:
- Identify the affected side’s Levator Scapulae muscle using ultrasound.
- Locate the intersection of the Levator Scapulae and Splenius Capitis muscles.
- Track the Levator Scapulae, Splenius Capitis, and Trapezius (which is located above the Serratus Posterior Superior muscle) while ensuring that the SLS Triangle, the interfascial space between these muscles, is clearly visible.
- Upon identifying the SLS Triangle, move the ultrasound transducer in the cranial direction.
- Observe the hyperechoic fascia on the ultrasound image, which forms the boundaries of the interfascial space containing fat tissue and part of the Dorsal Scapular Nerve.29
- Prepare a disposable 5 cc syringe (Bukwang Medical, Yangju-si, Gyeonggi-do, Korea) containing 2 cc of Placenta Pharmacopuncture solution. Using a 26-gauge × 60 mm guiding needle (Yongchang Co., Gimpo-si, Gyeonggi-do, Korea), inject the pharmacopuncture solution at the junction where the Splenius Capitis, Levator Scapulae, and Trapezius muscles meet under ultrasound guidance.
Figures demonstrate various aspects of the procedure: Figure 3. shows the contact of the ultrasound transducer with the affected site; Figure 4. displays standard ultrasound imaging of the SLS Triangle region.
Outcomes
In this study, we will assess the Numerical Rating Scale (NRS) for pain reported by patients before and after the Pharmacopuncture procedure during Visit 1. Additionally, we will measure the Pressure Pain Threshold (PPT) of the left and right Levator Scapulae and Supraspinatus muscles, as well as the Range of Motion (ROM) for cervical spine flexion, extension, lateral flexion, and rotation.
To ensure the reliability of assessors and consistency in outcome measurement, standardized criteria for NRS, PPT, and ROM measurements have been established. Before the study begins, all participating medical staff will undergo pre-study training on outcome measurement methods to ensure standardized data collection.
NRS will be used as a clinical tool to objectively measure pain by recording patients’ subjective responses. The NRS is a well-established assessment tool known for its high sensitivity and effectiveness in detecting changes in pain levels.30 The scale ranges from 0 (indicating no pain) to 10 (representing unbearable pain), with higher scores indicating greater pain intensity.
For PPT measurements, all medical staff will use a uniform digital algometry device to ensure consistency. The measurement sites will be standardized to the bilateral Levator Scapulae and Supraspinatus muscles, and a consistent measurement protocol will be followed to minimize errors. During the assessment, the participant will be seated comfortably, and the digital algometry device will be applied perpendicularly at a controlled speed (kg/sec). Participants will be instructed to vocalize “Ah” upon experiencing discomfort or pain, at which point the device will record the pressure value in kg/cm² to ensure objective and reproducible data collection. Furthermore, a study has reported that PPT evaluation using an electronic algometer is both reliable and effective in distinguishing individuals with and without neck and low back pain, with minimal measurement error. This highlights the validity and reliability of PPT as a measurement tool in this study.31
ROM measurements will be conducted using identical goniometers at all study sites to ensure consistency. These measurements will follow the American Medical Association (AMA) guidelines and will assess Active Range of Motion (A-ROM), which evaluates voluntary cervical spine movement without external assistance. Improvement in ROM is one of the most direct methods for assessing pre- and post-treatment differences in pain management. One study reported that adopting a standardized measurement protocol when using a goniometer for ROM assessment can enhance its reliability.32 Additionally, another study found that Active Cervical A-ROM measured with a universal goniometer demonstrated excellent intra-rater and inter-rater reliability, confirming its validity as a reliable assessment tool in clinical practice.33
Outcome assessors in this study will not be blinded to the treatment groups. Since the study will be conducted in a real-world clinical setting, it will not be feasible to ensure complete blinding of the evaluators. However, to minimize potential bias, all measurements will be conducted following a standardized assessment protocol across all study sites. Additionally, efforts will be made to maintain consistency and objectivity in data collection by providing pre-study training to evaluators. While these measures will help reduce bias, the possibility of measurement bias cannot be entirely eliminated, and results should be interpreted with caution.
Sample Size and Statistical Analysis
Given that no prior studies have been conducted under identical conditions—namely, using ultrasound-guided acupuncture as the intervention with the NRS as the primary outcome—we based our effect size estimation on research with similar conditions. To evaluate the efficacy of ultrasound-guided acupuncture, the Numeric Rating Scale (NRS) was employed as the primary outcome measure. Previous studies have reported a minimum clinically important difference (MCID) of 2.17 points for the NRS, and the standardized effect size (Cohen’s d) comparing groups that received ultrasound-guided acupuncture with those that did not was approximately 1.3.34 These findings indicate that the observed difference is not only clinically meaningful—exceeding the MCID—but also far surpasses the threshold for a “large effect” (≥0.6). Consequently, this study assumed a large effect size (≥0.6) for the purpose of sample size estimation, supporting the adequacy of a total of 100 participants to achieve sufficient statistical power.
Statistical analysis will be conducted using the Statistical Package for the Social Sciences (SPSS) for Windows, version 20.0. The independent variable in this study will be the assigned treatment method (UGP vs NGP), while the dependent variables include the NRS, PPT, and ROM values, which will be measured twice—before and after the procedure—in both groups.
A two-way mixed ANOVA will be conducted to analyze the differences in treatment effects between groups (UGP vs NGP) and across time (pre- and post-procedure), as well as to examine their interaction effects. Effect sizes will be calculated using partial eta-squared (η²) for ANOVA models.
For continuous data, descriptive statistics will be used to calculate the mean, standard deviation, minimum, and maximum values. Additionally, a Student’s t-test will be applied, with effect sizes reported using Cohen’s d to quantify the magnitude of differences between groups. Categorical variables will be analyzed for absolute and relative frequencies using the Chi-square test or Fisher’s exact test.
Additionally, after confirming any differences in baseline characteristics between groups, if these differences are found to be related to the study variables or the evaluation of treatment effects, they will be regarded as confounding factors. Consequently, subgroup analysis or multivariate analysis (eg, ANCOVA or multiple regression models) will be conducted. Effect sizes, adjusted R² (for regression), and 95% confidence intervals will be reported for all model parameters.
All statistical tests will be two-tailed, and a p-value of < 0.05 will be considered statistically significant.
Data Collecting, Processing, and Monitoring
The management of clinical research data will be conducted in accordance with the latest standard operating procedures of the Clinical Research Center at the affiliated hospital. For any matters not specified in these standard operating procedures, the ICH-GCP guidelines will be followed. Data must be entered into the case report form (or electronic case report form) immediately upon availability. If data has not been recorded by the end of the case, an appropriate reason for the omission must be documented. Even after data entry, source documents, case report forms, and materials from the electronic case report form database will be retained to allow for verification upon request. Upon the conclusion of the study, in accordance with clinical research management regulations, written personal and sensitive information will be stored in a secure location equipped with a locking mechanism for three years. Additionally, personal data stored in electronic file format will be encrypted to ensure safe storage.
Ethics and Dissemination
Ethical Approval
This study has been approved by the Institutional Review Board (IRB) of Wonkwang University in Iksan, South Korea (WKIRB-2024/10-3). This clinical research will be conducted in accordance with ethical principles based on the “Declaration of Helsinki” and the “Good Clinical Practice (GCP)” guidelines, ensuring the rights, welfare, and safety of clinical research participants to the greatest extent possible.
Consent Statement and Obtaining Written Consent
Before entering the clinical study, all aspects of the research purpose, potential adverse reactions, and safety will be explained to the participants. Their voluntary consent to participate in the study will be obtained.
In particular, if staff members of the clinical research institution wish to participate, it will be limited to subjects unrelated to the study. Sufficient explanations about the research will be provided to those staff members who have a voluntary motivation to participate, and consent will only be obtained after they agree to participate, guiding them to complete the written consent form.
If the research participants or their legal representatives are unable to read the consent form, clinical research participant information sheet, or other documented information, a neutral third party will be present throughout the entire consent process to obtain consent.
Compensation for Severe or Emergency Adverse Events
This clinical study utilizes the existing medical device and the commonly used placenta Pharmacopuncture in Korean medicine institutions for patient treatment. While it is anticipated that there will be minimal risk during the research process, compensation regulations for potential harm will be established as a precaution. In the event of an emergency, every effort will be made to provide treatment for the participants. Naturally, participants can withdraw their registration at any time.
Adverse Events
This study involves a single administration of the Pharmacopuncture solution. Given that HP Pharmacopuncture is commonly used in clinical practice, it is expected to be safe. However, participants will be informed in advance about potential mild adverse effects such as bruising, localized pain, and fatigue following the procedure.
Additionally, specific adverse reactions related to the Magnetic Needle used in Pharmacopuncture will be closely monitored. Potential adverse effects of needling may include localized pain at the insertion site, hypersensitivity reactions such as tingling sensations, minor bleeding, or hematoma formation. In rare cases, skin hypersensitivity reactions, infections, dizziness, syncope, nausea, or headaches may occur.
Furthermore, ultrasound guidance enhances procedural safety by preventing unintentional injury to key neurovascular structures in the cervical region. The superficial branch of the transverse cervical artery (TCA), located beneath the trapezius, and the deep branch of the TCA, which runs alongside the dorsal scapular nerve, can be clearly visualized and avoided.35 Unlike blind injections, which pose risks of vascular injury and nerve damage, ultrasound guidance enables precise needle placement, reducing complications such as bleeding and inadvertent nerve injury.
To ensure patient safety, adverse reactions will be assessed immediately post-procedure and via phone follow-up the next day. In the event of any adverse effects or safety incidents, immediate notification to the principal investigator will be required. All adverse reactions—including symptoms, onset date, duration, and other relevant details—will be thoroughly recorded and reported by the researchers.
Discussion and Conclusion
Ultrasound-guided procedures have gained significant attention as a method that enhances both safety and therapeutic efficacy by providing real-time visualization of the treatment area. Unlike blind procedures, ultrasound guidance enables direct visualization of muscles, nerves, and blood vessels, facilitating more precise and targeted interventions.9–11 In addition to its advantages over blind procedures, ultrasound-guided techniques have shown superior efficacy compared to fluoroscopy-guided procedures, particularly regarding patient satisfaction and reduced procedural pain.36,37
Recently, research on the application of ultrasound-guided procedures in traditional Korean medicine, including acupuncture and pharmacopuncture, has been increasing. Studies have reported that ultrasound-guided acupuncture not only improves accuracy, effectiveness, and safety but also facilitates more precise access to and assessment of deep anatomical structures.1,8,38 Given this expanding interest, this study is designed as a multi-center prospective comparative observational study to evaluate the effectiveness of Ultrasound-Guided Pharmacopuncture(UGP) for acute Myofascial Pain Syndrome(MPS) in patients experiencing neck and shoulder pain.
This study collects clinical data from two hospitals and five Korean medicine clinics, where patients will receive Hominis Placenta (HP) pharmacopuncture injections at the interfascial space of the Splenius Capitis, Levator Scapulae, and Serratus Posterior Superior muscles, known as the SLS Triangle, under ultrasound guidance. To evaluate treatment outcomes, pain assessments will be conducted using the Numerical Rating Scale (NRS), Pressure Pain Threshold (PPT), and Range of Motion (ROM) both before and immediately after the intervention.
Additionally, this study investigates the therapeutic effects of HP pharmacopuncture at the SI14 acupoint in patients with Acute Cervical Myofascial Pain Syndrome (CMPS) who have experienced symptom onset within the past seven days. The SI14 acupoint is located within the SLS Triangle, where the Splenius Capitis, Levator Scapulae, and Serratus Posterior Superior muscles intersect.1 The Dorsal Scapular Nerve passes through this region, and excessive tension in these muscles can compress the nerve, potentially leading to CMPS.1 Therefore, pharmacopuncture injection at this site is hypothesized to relieve nerve compression and improve symptoms.
In this protocol study, HP solution, which contain several cell growth factors, various interferons, and colony-forming stimulating factors, which contribute to its anti-inflammatory, antiviral, antioxidant, and analgesic effects.25 Clinically, HP is administered at major acupuncture points along meridians, as well as at alarm points, to treat various conditions.26 In particular, its pain-modulating and tissue-regenerative effects make it a valuable therapeutic option for musculoskeletal disorders and pain-related conditions.
Building on this understanding, This study aims to evaluate the pain-modulating effects of HP pharmacopuncture in conjunction with ultrasound guidance, providing insights into its therapeutic efficacy.
Recent advances in ultrasound-guided interventions have highlighted the significance of targeting interfascial planes for precise and effective pain management.39 In addition to traditional intramuscular trigger point injections, ultrasound-guided interfascial injections enable selective nerve blocks and adhesion release, thereby enhancing therapeutic outcomes.39
With the assistance of ultrasound guidance, the injection site and dosage of the HP solution can be adjusted according to the patient’s fascial condition, pain distribution, and degree of nerve compression within the SLS Triangle. This tailored approach allows for individualized treatment, optimizing therapeutic efficacy while minimizing unnecessary interventions.
Given these research objectives, this study protocol is designed with several strengths that enhance its clinical relevance and reliability.
First, This study will be the first registered study to confirm the effectiveness of ultrasound-guided HP Pharmacopuncture in relieving muscle pain and improving cervical range of motion in CMPS patients.
Second, this study utilizes the Acuviz Pocket, a portable ultrasound device equipped with a needle-tracking function. Most previous studies involving ultrasound have primarily focused on fixed console-type ultrasounds, which, despite their excellent performance, limit mobility during clinical practice. If meaningful results are obtained, this study may expand the applicability of ultrasound-guided procedures in Korean medicine clinics.
Third, this study is a multi-center prospective comparative study, conducted across two hospitals and five primary care clinics, enhancing the generalizability and reliability of its findings. With an expected enrollment of over 100 patients, this study is structured to compare two groups: the UGP group and the NGP group, allowing for a direct comparison of treatment outcomes based on the presence or absence of ultrasound guidance. This design provides valuable insights into the clinical effectiveness of ultrasound-guided procedures.
Finally, the results of this study are expected to provide comprehensive evidence on the effectiveness and safety of UGP, with a particular focus on pain relief and range of motion improvements in CMPS patients.
This study protocol has several limitations. However, despite these limitations, the study design remains methodologically meaningful, and appropriate measures have been taken to address potential concerns.
First, this study was designed as a prospective comparative observational study, rather than a Randomized Controlled Trial (RCT), meaning that selection bias due to non-random group allocation cannot be entirely ruled out. Future research should adopt a more rigorous controlled study design with randomized allocation to enhance methodological validity and improve the reliability of comparative analyses.
Second, this study specifically targets patients with acute CMPS within seven days of symptom onset, whereas previous studies have defined acute phase as lasting 4 to 6 weeks.18 This discrepancy indicates that the 7-day inclusion criterion in this study represents a more restrictive definition of the acute phase, which may limit the inclusion of patients with symptom onset within the broader acute-phase range. However, this study aims to focus on early acute-phase CMPS to minimize the influence of subacute-phase transitions or other confounding variables on pain levels. Furthermore, previous studies have successfully conducted research targeting MPS patients within a 7-day onset period, supporting the methodological consistency of this approach.20,21
Third, this study primarily focuses on evaluating the short-term therapeutic effects of UGP, as it does not include long-term follow-up assessments. Future studies should incorporate follow-up evaluations to assess the long-term efficacy of UGP beyond its immediate effects. Such studies would help determine whether the therapeutic benefits of UGP persist over time.
As a multi-center study conducted across two hospitals and five primary care clinics, this study is expected to enhance the generalizability of its findings. Future research should further evaluate the applicability of UGP in diverse clinical settings to establish broader clinical evidence for its efficacy and safety.
Abbreviations
CMPS, Cervical Myofascial Pain Syndrome; MPS, Myofascial Pain Syndrome; NCDs, Non-Communicable Diseases; UGA, Ultrasound-Guided Acupuncture; NGA, Non-Guided Acupuncture; SAN, Spinal Accessory Nerve; DSN, Dorsal Scapular Nerve; UGP, Ultrasound-Guided Pharmacopuncture; SLS Triangle, Splenius Capitis, Levator Scapulae, Serratus Posterior Superior Triangle; CRIS, Clinical Research Information Service; NIH, National Institute of Health; HP, Hominis Placenta; NGP, Non-Guided Pharmacopuncture; RCT, Randomized Controlled Trial; NRS, Numerical Rating Scale; PPT, Pressure Pain Threshold; ROM, Range of Motion; IRB, Institutional Review Board; NGS, Needle Guiding System; AMA, American Medical Association. A-ROM, Active Range of Motion; SPSS, Statistical Package for the Social Sciences.
Acknowledgments
We gratefully thank all the collaborating investigators and subjects for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by grants from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant numbers: RS-2024-00442030), and by a grant from the National Institute for Korean Medicine Development (NIKOM) for the Korean medicine industry advancement support project funded by the Ministry of Health & Welfare, Republic of Korea (grant number: 24R433). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Chu H, Park S, Nam T, et al. Case report on three patients with cervical myofascial pain syndrome showing improvement with ultrasound-guided pharmacopuncture: proposal of the ‘SLS Triangle’ treatment protocol. Korean J Acupunct. 2024;41(3):101–109. doi:10.14406/acu.2024.012
2. Galasso A, Urits I, An D, et al. A comprehensive review of the treatment and management of myofascial pain syndrome. Curr Pain Headache Reports. 2020;24(8):43. doi:10.1007/s11916-020-00877-5
3. Urits I, Charipova K, Gress K, et al. Treatment and management of myofascial pain syndrome. Best Pract Res Clin Anaesth. 2020;34(3):427–448. doi:10.1016/j.bpa.2020.08.003
4. Ezzati K, Ravarian B, Saberi A, et al. Prevalence of cervical myofascial pain syndrome and its correlation with the severity of pain and disability in patients with chronic non-specific neck pain. Arch Bone Joint Surg. 2021;9(2):230–234. doi:10.22038/abjs.2020.48697.2415
5. Sahrmann S, Azevedo DC, Dillen LV. Diagnosis and treatment of movement system impairment syndromes. Brazilian J Physical Ther. 2017;21(6):391–399. doi:10.1016/j.bjpt.2017.08.001
6. Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res. 2010;24(6):783–792. doi:10.1016/j.berh.2011.01.019
7. GBD 2021 Forecasting Collaborators. Burden of disease scenarios for 204 countries and territories, 2022–2050: a forecasting analysis for the global burden of disease study 2021. Lancet. 2024;403(10376):2204–2256. doi:10.1016/S0140-6736(24)00685-8
8. Chu H, Park S, Kang K, et al. Current insights and updates in ultrasound-guided acupuncture: a comprehensive review and status report. J Korean Med Soc Acupotomol. 2023;7(2):121–130. doi:10.54461/JAcupotomy.2023.7.2.121
9. Xu H, Zhang Y, Wang C. Ultrasound-guided hydrodilatation of glenohumeral joint combined with acupotomy for treatment of frozen shoulder. J Back Musculoskeletal Rehab. 2022;35(5):1153–1160. doi:10.3233/BMR-210272
10. Lin S, Lai C, Wang J, et al. Efficacy of ultrasound-guided acupotomy for knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2023;102(2):e32663. doi:10.1097/MD.0000000000032663
11. Liang Y, Chen L, Cui Y, Du C, Xu Y, Yin L. Ultrasound-guided acupotomy for trigger finger: a systematic review and meta-analysis. J Orthopaedic Surg Res. 2023;18(1):678. doi:10.1186/s13018-023-04127-3
12. Lee S, Kim JH, Chu H. High-Risk Area Ultrasound-Guided Acupuncture Handbook. Dajeon (Korea): Korea Institute of Oriental Medicine; 2018.
13. Ricci V, Mezian K, Chang K, et al. Ultrasound imaging and guidance for cervical myofascial pain: a narrative review. Int J Environ Res Public Health. 2023;20(5):3838. doi:10.3390/ijerph20053838
14. Alagha B. Chiropractic and rehabilitation management of a patient with extraforaminal entrapment of L4 nerve with balance problem. J Back Musculoskeletal Rehab. 2015;28(3):603–607. doi:10.3233/BMR-140557
15. Sucher BM. Myofascial manipulative release of carpal tunnel syndrome: documentation with magnetic resonance imaging. J Osteopathic Med. 1993;93(12):1273–1278. doi:10.7556/jaoa.1993.93.12.1273
16. Sucher BM. Thoracic outlet syndrome—a myofascial variant: part 2. Treatment J Am Osteopathic Assoc. 1990;90(9):810–823. doi:10.1515/jom-1990-900917
17. Unalan H, Majlesi J, Aydin FY, Palamar D. Comparison of high-power pain threshold ultrasound therapy with local injection in the treatment of active myofascial trigger points of the upper trapezius muscle. Arch Phys Med Rehabil. 2011;92(5):657–662. doi:10.1016/j.apmr.2010.11.030
18. Lugo LH, García HI, Rogers HL, Plata JA. Treatment of myofascial pain syndrome with lidocaine injection and physical therapy, alone or in combination: a single blind, randomized, controlled clinical trial. BMC Musculoskeletal Disord. 2016;17(101). doi:10.1186/s12891-016-0949-3
19. Gerwin RD. Classification, epidemiology, and natural history of myofascial pain syndrome. Curr Pain Headache Reports. 2001;5(5):412–420. doi:10.1007/s11916-001-0052-8
20. Kocak AO, Ahiskalioglu A, Sengun E, Gur STA, Akbas I. Comparison of intravenous NSAIDs and trigger point injection for low back pain in ED: a prospective randomized study. Am J Emergency Med. 2019;37(3):457–461. doi:10.1016/j.ajem.2019.01.015
21. Ay S, Tur BS, Karakaş M, Gökmen D, Altınbilek T, Evcik D. Comparison of kinesio taping, trigger point injection, and neural therapy in the treatment of acute myofascial pain syndrome: a randomized controlled study. Agri. 2023;35(3):134–141. doi:10.14744/agri.2022.39259
22. Groeneweg R, Kropman H, Leopold H, et al. The effectiveness and cost-evaluation of manual therapy and physical therapy in patients with sub-acute and chronic non-specific neck pain: rationale and design of a randomized controlled trial (RCT). BMC Musculoskeletal Disord. 2010;11(1):14. doi:10.1186/1471-2474-11-14
23. Lee KH, Cho YY, Kim S, Sun SH. History of research on pharmacopuncture in Korea. J Pharmacopuncture. 2016;19(2):101–108. doi:10.3831/KPI.2016.19.010
24. Ryoo DW, Kim HG, Kim SJ, et al. Systematic review of hominis placenta pharmacopuncture in English and Korean literature. J Acupuncture Res. 2017;34(4):153–158. doi:10.13045/jar.2017.02236
25. Lee GJ. Pharmacopuncturology. Seoul (Korea): Hanmi; 2019:247.
26. Park Y, Ahn CB, Park Y, et al. Comparative observational study on the effects of intra-articular hominis placenta pharmacopuncture and acupoint hominis placenta pharmacopuncture for knee osteoarthritis patients. J Acupuncture Res. 2021;38(1):60–65. doi:10.13045/jar.2020.00451
27. Kim JW, Kim CY, Choi SP, Han SW, Lee JC, Kim DH. The case report of trigger finger improved with hominis placenta pharmacopuncture treatment. J Pharmacopuncture. 2010;13(4):139–147. doi:10.3831/KPI.2010.13.4.139
28. Chun HS. Literature review of domestic randomized controlled trials for hominis placenta pharmacopuncture. J Acupuncture Res. 2024;41:228–244. doi:10.13045/jar.24.0028
29. Hung C, Wang B, Chang H, et al. Pictorial essay on ultrasound and magnetic resonance imaging of paraspinal muscles for myofascial pain syndrome. Life. 2024;14(4):499. doi:10.3390/life14040499
30. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14(7):798–804. doi:10.1111/j.1365-2702.2005.01121.x
31. Zicarelli CAM, Santos JPM, Poli-Frederico RC, et al. Reliability of pressure pain threshold to discriminate individuals with neck and low back pain. J Back Musculoskeletal Rehab. 2021;34(3):363–370. doi:10.3233/BMR-181208
32. Gajdosik RL, Bohannon RW. Clinical measurement of range of motion: review of goniometry emphasizing reliability and validity. Physical Ther. 1987;67(12):1867–1872. doi:10.1093/ptj/67.12.1867
33. Farooq MN, Bandpei MAM, Ali M, Khan GA. Reliability of the universal goniometer for assessing active cervical range of motion in asymptomatic healthy persons. Pakistan J Med Sci. 2016;32(2):457–461. doi:10.12669/pjms.322.8747
34. Ceballos-Laita L, Medrano-de-la-Fuente R, Estébanez-De-Miguel E, et al. Effects of dry needling in teres major muscle in elite handball athletes. a randomised controlled trial. J Clin Med. 2021;10(18):4260. doi:10.3390/jcm10184260
35. Ricci V, Özçakar L. Ultrasound imaging of the upper trapezius muscle for safer myofascial trigger point injections: a case report. Physic Sports Med. 2019;47(3):247–248. doi:10.1080/00913847.2019.1589105
36. Hofmeister M, Dowsett LE, Lorenzetti DL, Clement F. Ultrasound- versus fluoroscopy-guided injections in the lower back for the management of pain: a systematic review. Eur Radiol. 2019;29(7):3401–3409. doi:10.1007/s00330-019-06065-3
37. Byrd JW, Potts EA, Allison RK, Jones KS. Ultrasound-guided Hip injections: a comparative study with fluoroscopy-guided injections. Arthroscopy. 2014;30(1):42–46. doi:10.1016/j.arthro.2013.09.083
38. Kang K, Oh K, Kim J, Chu H. Protocol for ultrasound-guided acupotomy procedure at ligament flavum. J Acupotomy. 2023;7(1):1–6.
39. Wu W, Chang K, Ricci V, Özçakar L. Ultrasound imaging and guidance in the management of myofascial pain syndrome: a narrative review. J Yeungnam Med Sci. 2024;41(3):179–187. doi:10.12701/jyms.2024.00416
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.