")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Virtual Reality and Videogaming in Pulmonary Rehabilitation for Asthma: A Systematic Review of Clinical Outcomes and Engagement
Authors Darabseh MZ , Badran R, Alhasan EO, Shurrab AM, Amro AA, Mohmara YA, Al Oweidat K , Awwad S, Ledger SJ, Aburub A
Received 25 November 2024
Accepted for publication 26 March 2025
Published 24 April 2025 Volume 2025:18 Pages 2281—2292
DOI https://doi.org/10.2147/JMDH.S508524
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohammad Z Darabseh,1 Rahaf Badran,2 Eman Omar Alhasan,3 Ala’a M Shurrab,4 Anwaar A Amro,5 Yasser Alakhdar Mohmara,6 Khaled Al Oweidat,7 Shorooq Awwad,8 Sean James Ledger,9 Aseel Aburub5
1Department of Physiotherapy, The University of Jordan, Amman, Jordan; 2Department of Physiotherapy, Philadelphia University, Amman, Jordan; 3Department of Clinical Nutrition and Dietetics, Applied Science Private University, Amman, Jordan; 4Department of Basic Medical Science, Al-Balqa Applied University, Al salt, Jordan; 5Department of Physiotherapy, Applied Science Private University, Amman, Jordan; 6Department of Physiotherapy, University of Valencia, Valencia, Spain; 7Department of Internal Medicine, Respiratory and Sleep Medicine, The University of Jordan, Amman, Jordan; 8Department of Nursing, Middle East University, Amman, Jordan; 9Department of Physiotherapy, Central Queensland University, Rockhampton, QLD, Australia
Correspondence: Shorooq Awwad, Department of Nursing, Faculty of Nursing, Middle East University, Amman, 11831, Jordan, Email [email protected]
Abstract: Asthma is a chronic respiratory disease that significantly impacts quality of life. Pulmonary rehabilitation has been shown to improve lung function and symptoms in asthma, but its adoption is limited due to accessibility and patient engagement challenges. Virtual reality (VR) and videogaming technologies have emerged as potential tools to enhance pulmonary rehabilitation by providing an engaging and interactive environment. This systematic review aimed to evaluate the effectiveness, feasibility, safety, and patient engagement of VR and videogaming in pulmonary rehabilitation for individuals with asthma. A comprehensive search of seven electronic databases (PubMed, Embase, CINAHL, Cochrane, AMED, SPORTDiscus and PEDro) was conducted to identify studies that included VR and videogaming interventions. Studies included participants with asthma and used VR or videogaming as part of pulmonary rehabilitation. Data extraction focused on intervention types, clinical outcomes, patient engagement, and safety. Five studies were included in the final review and involved 104 participants. The studies implemented different digital tools, including the InSpire System, and games such as “Reflex Ridge” and “Serious Games”. VR and videogaming interventions improved asthma control, lung function, and exercise capacity. High levels of patient engagement and adherence were reported, with no adverse events across the trial. VR and videogaming show promise as effective, feasible, and safe tools to enhance pulmonary rehabilitation in individuals with asthma. However, the heterogeneity of studies limited the ability to draw definitive conclusions, with further research needed using standardized outcomes.
Keywords: asthma, pulmonary rehabilitation, virtual reality, videogaming, digital health technology, spirometry
Introduction
Asthma is a chronic respiratory condition characterized by airway inflammation and hyper responsiveness that affects millions of people globally.1 The disease leads to recurrent symptoms of wheezing, breathlessness, chest tightness, and coughing, which may significantly impair quality of life.2 Despite advances in pharmacological treatment, individuals with asthma experience poor symptom control, frequent exacerbations, and limitations in physical activity.3 As a result, non-pharmacological interventions, such as pulmonary rehabilitation, have emerged as valuable adjuncts to medical therapy, which aims to improve physical function, reduce symptoms, and optimize health outcomes.4
Pulmonary rehabilitation traditionally comprised of supervised exercise training, patient education and behavioral interventions has demonstrated efficacy in improving lung function and quality of life in people with asthma.5 However, several barriers, including limited access to rehabilitation programs, long waiting-lists, low patient engagement, and adherence issues, have hindered implementation.6 To overcome these challenges, researchers have increasingly turned to digital health technologies, such as tele-health, virtual reality (VR) and videogaming, as innovative tools to deliver and enhance pulmonary rehabilitation programs.7
VR and videogaming technologies offer interactive and immersive environments that may engage participants in rehabilitation exercises whilst providing real-time feedback on performance.8,9,10 These technologies have been shown to improve motivation, enhance adherence to exercise programs, and provide tailored rehabilitation experiences in various chronic conditions, including respiratory diseases.11 By gamifying the rehabilitation process, VR and videogaming systems may foster greater patient participation, making rehabilitation more enjoyable and accessible, particularly for pediatric and adolescent populations with asthma.12 Furthermore, VR and video games have the potential to simulate real-life environments and situations, which enable individuals with asthma to practice breathing techniques and physical activities in controlled, low-risk settings.
Although the use of VR and videogaming in pulmonary rehabilitation for asthma is a relatively new area of research, early studies have suggested promising benefits for lung function, asthma control, and exercise capacity.8 However, the evidence remains scant, with variations in the types of digital interventions, populations, and outcome measures assessed. Therefore, a comprehensive review of the available literature is warranted to consolidate current knowledge, identify gaps, and provide direction for future research.
The aim of this systematic review was to explore the use of VR and videogaming in pulmonary rehabilitation for people with asthma. Specifically, this review aimed to evaluate the effectiveness of these technologies to improve clinical outcomes, such as asthma control, lung function, and exercise capacity. Additionally, assessment of VR and videogaming feasibility, safety, and patient engagement was considered. Synthesis of this data may offer clinicians an insight into the potential role of VR and videogaming as mechanisms to enhance pulmonary rehabilitation in people with asthma.
Methodology
Study Design
The study was a systematic review that explored the use of VR and videogaming in pulmonary rehabilitation in people with asthma. The study protocol was registered using PROSPERO registry (registration number is: CRD42024582928).
Information Sources
A comprehensive search was conducted to identify studies published between January 1, 1970, and September 1, 2024. The search was conducted through EBSCO using the following seven electronic databases: PubMed (MEDLINE), Embase, CINAHL, Cochrane, AMED, SPORTDiscus, and PEDro. Additionally, citation tracking was conducted to identify other relevant trials. Search terms were adapted to meet the specific requirements of each database to ensure that all potentially relevant studies were captured. The search was limited to studies written in English and published in peer-reviewed journals.
Search Strategy
This review used a systematic search based on research questions aligned with medical subject headings (MeSH) terms, and combinations of synonyms with subjects on all items using Boolean (“AND” and “OR”) for each database. The systematic search was conducted using a combination of the following keywords: “asthma” OR “acute asthma” OR “asthma attack” OR “asthmatic” OR “asthma exacerbation” OR “wheeze” AND “virtual reality games” OR “virtual reality” OR “VR” OR “augmented reality” OR “AR” OR “mixed reality” OR “virtual reality therapy”; AND “spirometry test” OR “pulmonary functions test” OR “spirometer” OR “lung function” OR “lung test” OR “pulmonary function” OR “respiratory function”.
Inclusion and Exclusion Criteria
The inclusion criteria were studies that assessed the effectiveness of virtual reality games interventions for pulmonary rehabilitation in people with asthma. Exclusion criteria were studies that did not include virtual reality or video games, did not assess lung function using spirometry, were not written in English, or any study that included participants with any other respiratory, neurological, musculoskeletal, or cognitive disorders, or were conference abstracts or protocols only.
Study Selection
Initial Screening was conducted by the first reviewer (EA), who retrieved all studies from the initial database searches and exported them into EndNote 21 (Clarivate, USA). Trials were sorted chronologically, and duplicates were removed. Eligibility screening was also conducted by the first reviewer (EA), with trials screened for suitability by scanning titles and reading abstracts and assessment according to the predefined eligibility criteria. A second reviewer (AAm) independently screened the studies, with disagreements resolved by consulting a third reviewer (RB).
Data Extraction
Data from eligible studies were extracted, including author(s), year of publication, study design, sample size, participant characteristics (eg, age, sex), duration of follow-up period, physiological effects of virtual reality games in asthma rehabilitation (eg, spirometry data, dyspnea and quality of life). Additionally, the virtual reality technique used, game names (where applicable), and prescription of exercise (including frequency, intensity, type and duration) was recorded. The extracted data were then cross-checked by another reviewer (AAb), with any disagreements resolved by the lead author (MZD).
Risk of Bias of the Included Trials
The Cochrane Risk of Bias tool 2 (CROB 2) was used to evaluate the risk of bias of the included trials, where two independent reviewers (RB and AMS) assessed the risk of bias. The CROB 2 assessment encompassed the following: (1) bias stemming from randomization criteria; (2) bias due to deviations from intended interventions; (3) bias arising from missing outcome data; (4) bias in the measurement of outcomes; and (5) bias in the selection of reported results.
Results
Study Characteristics
The initial search identified n = 409 studies, with n = 3 records removed as they were duplicates. Consequently, n = 401 studies were excluded for the following reasons: n = 3 were conference abstracts, n = 4 were animal studies, n = 60 did not include people with asthma, n = 185 were not interventional studies, n = 79 did not use VR or videogaming, and n = 70 were protocols only. As a result, n = 58,12–15 trials were included in the review of which n = 1 was a feasibility trial, n = 1 was a randomized controlled trial, n = 1 was a cross-sectional trial, and n = 2 were pilot randomized controlled trials. Collectively, the included trials enrolled n = 104 participants with asthma with characteristics of each study shown in Table 1. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart for article selection is shown in Figure 1. A meta-analysis was not feasible due to the heterogeneity of the included trials.
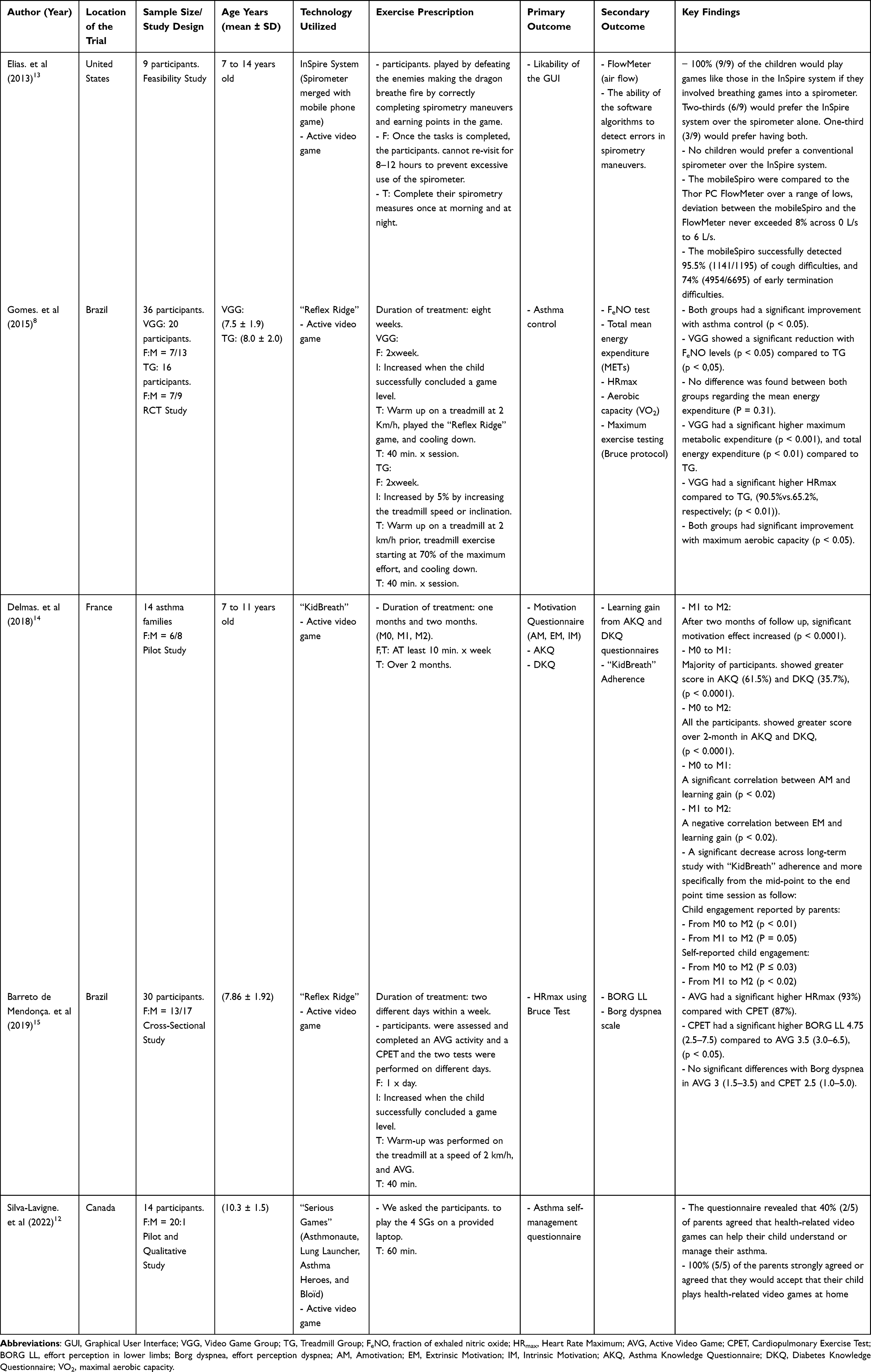 |
Table 1 Summary of Included Trials That Investigated the Effects of Using Virtual Reality and Games on Pulmonary Rehabilitation in Asthma |
 |
Figure 1 PRISMA diagram illustrating the article selection process. Adapted from Page M J, McKenzie J E, Bossuyt P M, Boutron I, Hoffmann T C, Mulrow C D et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372 :n71. Creative Commons.16 |
Risk of Bias
The risk of bias in the trials was independently assessed by two reviewers (RB and AMS) using the CROB2 tool. It showed that one trial was at a low risk of bias in one domain,8 two trials were at “some concern” of risk of bias in three domains,13,15 and two trials were at “some concern” of risk of bias in four domains.12,14 A summary of the CROB2 results is shown in Figure 2.
 |
Figure 2 Results of the Cochrane Risk of Bias (CROB2) for the included studies. |
Digital Health Technology Utilized
A wide range of digital health technologies were used in all studies1,8,13–15 and included smartphone applications and games using Xbox 360 Kinect and “Serious Games” systems. The InSpire System was used in n = 1 trial,15 which was an open-source, portable spirometer that connected with a mobile phone. This system was incorporated with a game; for example, participants were asked to defeat enemies in the game by making the dragon (Azmo) breathe fire by performing spirometry procedures correctly.
The game called “Reflex Ridge”, played on Xbox 360™ (Microsoft, Redmond, Washington, USA), was used in two trials,8,13 and participants played the games for 30-min. The “KidBreath” web application (Laboratoire Retines, Université Côte d’Azur, Nice, France) was used in one trial,14 and this was an e-learning gaming platform aimed at providing participants with asthma-related health information. The platform consisted of four categories with different games in each: (1) My Journey, (2) Discovering the Galaxy, (3) My Diary, and (4) My Profile. “Serious Games” were used in one trial,12 and this system consisted of four games that could be played using a laptop: “Asthmonautes”, “Lung Launcher”, “Asthma Heroes”, and “Bloïd”. All the games were educational and designed to help users understand their asthma symptoms and management.
Intervention Prescription
All five trials implemented different exercise prescriptions and educational programs dependent on the digital health technology. Elias et al15 asked participants to play a game that relied on spirometry sensors connected to a mobile phone such that each correct spirometry maneuver performed by the participants caused the dragon (called Azmo) to breathe fire, earning them points in the game. Once the spirometry maneuver was completed, users could not play the game again for between 8 and 12 hours to avoid overuse of the spirometer. Gomes et al8 instructed participants in two groups to train twice a week for 8-weeks. The video game training group completed a 5-minute warm-up on a treadmill at 2 km/h, followed by 30-min. of “Reflex Ridge” (10 × 3-minute rounds with a 30-second rest intervals), and a 5-minute cool-down. The intensity increased as participants concluded each gaming level. In contrast, the treadmill training exercise group completed a 5-minute warm-up on a treadmill at 2 km/h, followed by 30-min. of exercise training at 70% of maximum effort (based on a maximal exercise test), and a 5-minute cool-down, with the intensity increased through treadmill speed and inclination.
Delmas et al14 asked participants to use the “KidBreath” application for at least 10 minutes a week for 2-months. Between each month, participants received regular emails containing adherence questions that had to be answered before continuing. Barreto de Mendonça et al13 instructed participants to train for 2-days using active video games, and training consisted of a 10-minutes warm-up using the treadmill at a speed of 2 km/h before the session, followed by 30 minute of “Reflex Ridge” Game (10 three-minute matches with a 30-second rest interval) with the intensity increased gradually. Silva-Lavigne et al12 asked participants to play four “Serious Games” on a laptop for 60 min. (26-min. for “Asthmonautes”, 4-minutes for “Lung Launcher”, 26-minute. for “Asthma Heroes”, and 4-minutes for “Bloïd”). Parents were encouraged to motivate their children to explore the game, either alone or with their help.
Effects of the Digital Health Technology as an Intervention in Asthma
Gomes et al8 investigated the effects of gaming interventions (“Reflex Ridge” Game) on asthma control and reported significant improvements in both the intervention group and control group (p < 0.05). Elias et al15 investigated the effect of the InSpire System (mobileSpiro) on airflow and reported that the difference between the mobileSpiro and the FlowMeter never exceeded 8% (0L/s to 6 L/s). The ability of the software algorithms to detect difficulties in spirometry maneuvers was also reported by Elias et al,15 with the mobileSpiro software able to successfully detect 95.5% (1141/1195) of cough-related difficulties and 74% (4954/6695) of early termination difficulties.
Gomes et al8 examined the effects of the gaming intervention, “Reflex Ridge”, on fractional exhaled nitric oxide (FeNO) and reported a significant reduction (p < 0.05) in FeNO levels in the intervention group compared to the control group (p < 0.05). The study also measured the effect of the gaming intervention on total mean energy expenditure (MET), maximum MET, and maximum aerobic capacity, but found no significant difference (p = 0.31) between the two groups means energy expenditure. However, the intervention group had significantly higher maximum MET (p < 0.001) and total energy expenditure (p < 0.01) compared to the control group, whilst both groups saw significant (p < 0.05) improvements in maximum aerobic capacity.
Both Gomes et al8 and Barreto de Mendonça et al13 investigated the effect of gaming interventions on heart rate (HRmax). Gomes et al8 reported that their intervention group had a significantly higher HRmax compared to the control group (90.5% vs 65.2%, respectively; p < 0.01). However, Barreto de Mendonça et al13 reported that HRmax was significantly (p < 0.05) higher HRmax (93%) during a cardiopulmonary exercise test (CPET) than during the game (87%).
Only one study examined the effect of dyspnea and lower limb effort perception (Borg LL) using the Borg Dyspnea Scale during the gaming intervention. Barreto de Mendonça et al13 reported no significant differences in Borg dyspnea scores generated during the game (mean = 3; range: 1.5–3.5) and during CPET (mean = 2.5; range: 1.0–5.0). However, during CPET, a significantly higher (p < 0.05) BORG LL score (mean = 4.75; range: 2.5–7.5) was generated than during the game (mean = 3.5; range: 3.0–6.5).
Feasibility and Adherence
Elias et al15 reported that 100% (9/9) of participants would play games like those in the “InSpire” system if they involved breathing exercises with a spirometer and children reported no preference for use of a conventional spirometer over the “InSpire” system. Silva-Lavigne et al12 reported that 40% (2/5) of parents agreed that health-related video games could help their children understand or manage their asthma, whilst 100% (5/5) of parents neither strongly agreed nor agreed that they would allow their children to play health-related video games at home.
Delmas et al14 reported that most participants showed significantly (p < 0.0001) improved scores in the Asthma Knowledge Questionnaire (61.5%) and the Diabetes Knowledge Questionnaire (35.7%) [4]. This benefit was extended after completion of the study, with all participants demonstrating that they had further increased their scores in both the Asthma Knowledge Questionnaire and Diabetes Knowledge Questionnaire (p < 0.0001) at 2-month follow-up. Delmas et al14 also reported a significant improvement in motivation at the 2-month follow-up (p < 0.0001).
Despite these positive changes, Delmas et al14 reported that there was a significant decrease in adherence to “KidBreath” over time, especially between the midpoint and endpoint of the study. Child engagement, as reported by parents, also significantly decreased between baseline and the endpoint of the study (p < 0.05), and this was corroborated by children’s self-reported engagement, which dropped between baseline and the endpoint of the study (p < 0.02).
Safety of Digital Health Technology Interventions (Adverse Events)
No adverse events were reported in any of the trials.
Discussion
This systematic review has provided an insight into the emerging role of digital health technologies, specifically virtual reality (VR) and videogaming, in the pulmonary rehabilitation of individuals with asthma. The use of such technologies in healthcare has gained traction due to its potential to enhance patient engagement, increase adherence to rehabilitation programs, and improve clinical outcomes. In this review, all studies used various types of VR and gaming interventions to assess their impact on asthma-related outcomes. Although the evidence is still limited and heterogeneity was evident, the findings suggest promising benefits for people with asthma, particularly in terms of asthma control, lung function, and exercise capacity.
The heterogeneity across study designs and interventions presents a challenge when comparing outcomes. For instance, the interactive capabilities of Kinect, which require physical movement, might offer different therapeutic benefits compared to more passive, app-based interventions that rely on mobile platforms. Additionally, differences in the age and cognitive abilities of participants (such as children versus adolescents) may have led to varying degrees of engagement and possibly influenced the effectiveness of the interventions. These factors should be carefully considered when interpreting the results and generalizing the findings. Future research could benefit from exploring these variables in more detail to help standardize the methods and improve the reliability of conclusions drawn across studies.
Clinical Outcomes
The pooled data in this review may help clinicians looking to implement novel technologies to actively engage their participants in interventions that may help asthmatics. One of the key advantages of VR and videogaming was their ability to provide immersive and engaging environments that encouraged participants to adhere to their rehabilitation programs. The interactive nature of these interventions may help overcome some of the barriers associated with traditional pulmonary rehabilitation, such as boredom, lack of motivation, and low adherence. In the context of asthma, which often requires long-term management, these technologies may offer an innovative approach to sustaining patient engagement, particularly in pediatric populations.
Gomes et al8 reported improvements in asthma control and reductions in FeNO a marker of airway inflammation, in children participating in video game-based exercise training compared to controls. Similarly, Elias et al15 found that the use of the InSpire system, which incorporated spirometry into a gaming format, was effective in detecting airflow difficulties and improving spirometry performance in children. These findings align with previous research that underscores the potential of interactive digital interventions to improve clinical outcomes in chronic respiratory conditions such as asthma.
The feasibility and safety of the interventions were also assessed in the reviewed studies, with no adverse events reported across all trials. This is a critical consideration, as the safety of interventions is important when considered for inclusion in pulmonary rehabilitation programs. The high levels of patient and parent satisfaction reported in the studies support the acceptability of these digital interventions.
Despite the positive outcomes, challenges related to adherence were noted. Delmas et al14 reported a decline in engagement with the “KidBreath” application over time, which suggested that initial enthusiasm for digital interventions may be high, however maintaining long-term engagement may be a challenge. This issue is not unique to digital health technologies and has been observed in other forms of pulmonary rehabilitation where patient adherence tends to diminish over time. Clinicians may need to include a range of these technologies to sustain engagement.
The decline in engagement with digital interventions, as reported in studies like Delmas et al (2018) could be attributed to several psychological and contextual barriers. From a psychological perspective, users may experience a loss of interest or motivation over time, particularly when there is no novelty of the technology used. Additionally, if users do not perceive immediate or tangible benefits from the intervention, they may struggle to remain committed. Contextually, issues such as limited access to technology, lack of time, or family support can exacerbate disengagement. These factors may vary across different age groups and cultural contexts, highlighting the need for tailored interventions that address specific barriers to adherence. It is crucial that future studies explore these factors in more depth, identifying strategies to overcome them and improving long-term engagement with VR and gaming-based rehabilitation.
Implications for Future Research
The studies included in this review highlighted the potential of VR and videogaming as tools for pulmonary rehabilitation in asthma. Future research should focus on larger, well-designed randomized controlled trials that assess the long-term impact of VR and gaming interventions on asthma control, lung function, and quality of life. Moreover, standardized outcome measures should be defined for reporting and to allow for robust comparisons across studies. In addition, it is recommended to develop and implement VR-Based educational programs and conduct more multidisciplinary research to stay informed on technological advancements and improve the efficacy of this intervention in the field.
Limitations
Despite the evidence in this review that VR and videogaming are of interest and can potentially improve clinical outcomes in asthma management, but the evidence is still in its infancy. Most of the trials reviewed were small-scale, with small sample sizes that limited the generalizability of the findings. Additionally, the heterogeneity of the interventions and outcome measures used made it difficult to draw definitive conclusions about the overall effectiveness of these technologies. It should also be mentioned that specific demographic gaps such as adult populations or gender disparities can be considered as a limitation that should be taken into consideration.
Conclusion
VR and videogaming offer a promising environment for enhanced pulmonary rehabilitation in individuals with asthma. These technologies have the potential to improve clinical outcomes, increase patient engagement, and address barriers to traditional rehabilitation programs.
Clinicians are encouraged to use VR and videogaming more by assessing patient suitability through evaluating patients’ comfort with technology and ensuring they have no contraindications to VR use, and usage of the proper VR and videogaming tool/game. Researchers are also encouraged to design more rigorous studies, explore diverse VR applications and videogaming to fully understand the benefits and long-term sustainability of these technologies in the context of asthma management.
Data Sharing Statement
The data that support the findings of this study are available within the paper.
Acknowledgement
The authors would like to thank Middle East University in Jordan for their support in covering the publication fees for this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Global Initiative for Asthma. Global strategy for asthma management and prevention. Global Initiative for Asthma. 2024;2024:1–262.
2. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17–35. doi:10.1164/rccm.202109-2205PP
3. Bateman ED, Hurd SS, Barnes PJ, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31(1):143–178. doi:10.1183/09031936.00138707
4. Spruit MA, Singh SJ, Garvey C, et al. An official American thoracic society/European respiratory society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
5. Eijkemans M, Mommers M, Draaisma JMT, et al. Physical activity and asthma: a systematic review and meta-analysis. PLoS One. 2012;7(12):e50775. doi:10.1371/journal.pone.0050775
6. McCarthy B, Casey D, Devane D, et al. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2015(2):1.
7. McAnirlin O. Reflections on Co-Creating Nature-Based Virtual Reality Experiences for Adults Living With Severe COPD. Clemson University; 2023.
8. Gomes EL, Carvalho CR, Peixoto-Souza FS, et al. Active video game exercise training improves the clinical control of asthma in children: randomized controlled trial. PLoS One. 2015;10(8):e0135433. doi:10.1371/journal.pone.0135433
9. Alhusamiah B, Aldiqs M, Zeilani RS. The effectiveness of immersive virtual reality as a complementary approach and a new direction in cancer related fatigue management. Integr Cancer Ther. 2024;23:15347354241280272.
10. Alhusamiah BK, Zeilani RS, Haddad RH Using immersive and non-immersive virtual reality as an innovative and novel technology for managing depression, anxiety and psychological distress among patients with cancer. J Appl Psychol Enabling Technologies. 2025;19(1):42–62.
11. Laver K, Lange B, George S. Virtual reality for stroke rehabilitationCochrane. Database Syst Rev. 2017;11:1.
12. Silva-Lavigne N, Valderrama A, Pelaez S, et al. Acceptability of serious games in pediatric asthma education and self-management: pilot study. JMIR Pediatrics Parenting. 2022;5(2):e33389. doi:10.2196/33389
13. de Mendonça J B, Gomes EL, David M, et al. The intensity of physical activity in asthmatic children during active video game playing. EMJ Allergy Immunol. 2019:101–107. doi:10.33590/emjallergyimmunol/10311287.
14. Delmas A, Clement B, Oudeyer P, Sauzéon H. Fostering health education with a serious game in children with asthma: pilot studies for assessing learning efficacy and automatized learning personalization. Front Educ. 2018;3:1–22. doi:10.3389/feduc.2018.00099
15. Elias P, Rajan NO, McArthur K, Dacso CC. InSpire to promote lung assessment in youth: evolving the self-management paradigms of young people with asthma. Med 20. 2013;2(1):e1. doi:10.2196/med20.2014
16. Page MJ, McKenzie JE, Bossuyt PM, et al.The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of Symptoms Control, Pulmonary Function and Related Quality of Life in Asthmatic Patients Treated with Extrafine Beclomethasone Dipropionate/Formoterol Fumarate 100/6 μg pMDI: Results of a Multicenter Observational Study in Romania (ALFRESCO Study)
Ulmeanu R, Bloju S, Vittos O
Journal of Asthma and Allergy 2022, 15:919-933
Published Date: 8 July 2022
The Prevalence of Bronchodilator Responsiveness “Asthma” Among Adult Indigenous Australians Referred for Lung Function Testing in the Top End Northern Territory of Australia
Heraganahally SS, Howarth TP, Lloyd A, White E, Veale A, Ben Saad H
Journal of Asthma and Allergy 2022, 15:1305-1319
Published Date: 14 September 2022
Asthma Prevalence and Phenotyping in the General Population: The LEAD (Lung, hEart, sociAl, boDy) Study
Schiffers C, Wouters EF, Breyer-Kohansal R, Buhl R, Pohl W, Irvin CG, Breyer MK, Hartl S
Journal of Asthma and Allergy 2023, 16:367-382
Published Date: 8 April 2023
Advocating for Action: Exploring the Potential of Virtual Reality in Breathing Exercise – A Review of The Clinical Applications
Alhammad SA
Patient Preference and Adherence 2024, 18:695-707
Published Date: 19 March 2024
Detection of Inadequately Controlled Asthma in Adults Using Impulse Oscillometry and Fractional Exhaled Nitric Oxide
Yang X, Liu M, Shi H, Hu M, Lu Y, Chang X, Huang K
Journal of Asthma and Allergy 2025, 18:637-647
Published Date: 25 April 2025